
Abstract
Background
Existential distress, marked by hopelessness, loss of meaning, and spiritual suffering, is prevalent among patients with advanced illness, and is associated with psychological burden and a wish to hasten death (WTHD).
Purpose
This systematic review aimed to synthesize current evidence on meaning in life (MIL) in adult palliative care (PC) populations, focusing on its associations with quality of life (QOL), mental health, existential and spiritual well-being (SWB), and WTHD.
Methods
MEDLINE, Web of Science, Scopus, and the Cochrane Library were searched for eligible studies (English, 2016-2024) involving adult cancer patients receiving PC. MIL was examined as a central intervention component or outcome. Risk of bias was assessed: findings were synthesized narratively. The review was registered in PROSPERO.
Results
Eight studies (n = 1733 participants) were included: four cross-sectional, two randomized controlled trials, one longitudinal observational study, and one qualitative study. Several studies had small samples and substantial attrition. Risk of bias was high (n = 7), and moderate in one cross-sectional study. MIL was inversely associated with depression, anxiety, demoralization, and WTHD; and positively associated with QOL and SWB. MIL may also mediate psychological outcomes (eg, purpose, coherence, and personal values). However, heterogeneity in MIL conceptualization and measurement, combined with low methodological quality, limited comparability and certainty of findings.
Conclusion
MIL may be relevant to psychosocial/existential outcomes in PC. Conclusions are constrained by a small and methodologically weak evidence base. Further high-quality, longitudinal research is needed before MIL-centered interventions can be recommended for routine clinical practice.
Keywords
Introduction
Rationale
Advances in medicine and public health have extended life expectancy, increasing the prevalence of chronic, progressive, life-limiting conditions such as advanced cancer, neurodegenerative disorders, and end-stage organ failure. 1 These shifts challenge healthcare systems to move beyond curative models and embrace holistic, person-centered approaches. Meeting not only physical but also psychological, social, spiritual, and existential needs has become essential, particularly at the end-of-life (EOL).
Palliative care (PC) explicitly aims to relieve suffering and improve quality of life (QOL) for patients and families facing life-threatening illness. 2 However, access to PC remains uneven, particularly in low- and middle-income countries, compounding disparities in care. 3 Beyond physical symptoms, many patients experience existential distress—feelings of hopelessness, purposelessness, and loss of meaning—that are closely associated with depression, demoralization, and the wish to hasten death (WTHD).4,5
Emerging evidence identifies meaning in life (MIL)—defined as the sense that life is coherent, purposeful, and significant, 6 —as a key protective factor in serious illness. is increasingly recognized as fundamental to emotional and spiritual resilience. 7 As Viktor Frankl famously posited, suffering becomes intolerable when perceived as meaningless. 8 In palliative settings, helping patients find or preserve meaning is not only therapeutic—it is an ethical imperative.
Several psychotherapeutic models, including Meaning-Centered Psychotherapy and Dignity Therapy seek to restore a sense of meaning, dignity, and legacy near the EOL.5,9 A 2016 systematic review of twelve studies reported that MIL-focused interventions in cancer patients improved various outcomes, including purpose, QOL, spiritual well-being (SWB), optimism, hopelessness, depression, and WTHD. 10 However, the evidence base has expanded substantially since then and remains heterogeneous and fragmented. MIL is variably conceptualized—as a psychological construct, a spiritual dimension, or an existential need—and the outcomes assessed range widely across studies.
Moreover, many existing reviews have focused narrowly on specific interventions, without synthesizing the broader evidence on how MIL relates to core patient outcomes in PC. There remains a pressing need to clarify these relationships using a structured, quality-appraised, and updated synthesis. Addressing this gap is essential to inform more integrated, evidence-based existential support within PC.
Objectives
This systematic review aimed to synthesize and appraise the empirical evidence on MIL-centered interventions in adult patients with advanced cancer receiving PC. Specifically, we sought to examine how MIL-based interventions relate to outcomes such as QOL, mental health, WTHD, and existential or SWB. While not exhaustive of all MIL research, our focus on interventional and directly MIL-centered studies allows for a more targeted understanding of clinical utility, and sets the stage for future trials and implementation research.
Methods
This systematic review followed the recommendations of the “Cochrane Handbook for Systematic Reviews of Interventions,” 11 and was reported in accordance with the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” guidelines. 12
Eligibility Criteria
Selected articles met the following criteria:
Participants: Adult patients with advanced cancer receiving PC. Any definition of “advanced cancer” and PC used by the original authors was accepted, including early PC, hospice care, and EOL care.
Exposure/Intervention: Studies examining MIL either as a central intervention component or as a primary psychological construct, including its role as an exposure, outcome, correlate, or mediator.
Comparators: Any comparator, if applicable. Usual care was accepted as a control condition.
Outcomes: QOL, mental health, WTHD, and existential or SWB.
Study design: Quantitative, qualitative, and mixed-methods primary studies were eligible, including interventional, observational, and qualitative designs. Reviews, editorials, academic theses, and commentaries were excluded.
Articles not accessible through our Faculty's subscriptions were excluded.
Information Sources
MEDLINE (via PubMed), Web of Science, Cochrane Library and Scopus were searched for articles published between January 1, 2016, and December 31, 2024. The final search was conducted on January 2, 2025.
This date range was chosen to capture the most recent decade of research and to reflect the growing integration of existential care into PC practice, while recognizing that earlier foundational studies may have been excluded.
Search Strategy
The search combined free-text terms with database-specific subject headings: (“palliative care” OR “terminal care” OR “hospice care” OR “end-of-life care”) AND (cancer* OR malign* OR neoplasm*) AND (“meaning in life” OR “purpose in life” OR “meaning of life” OR “purpose of life”). Only English-language publications were included, and grey literature or trial registries were not searched, which may have introduced language or publication bias. Full database search strategies are provided in Supplementary Table 1.
Selection Process
Both authors independently screened titles and abstracts, followed by full-text assessment. Disagreements were resolved by discussion and consensus. No automation tools were used.
Data Collection Process
Data extraction was performed independently by two reviewers. Study authors were not contacted for additional information.
Data Items
Extracted data included study characteristics, design, objectives, participant characteristics, MIL conceptualization, intervention/exposure details, outcome measures, and main findings.
Study Risk of Bias Assessment
Risk of bias was assessed using the revised Cochrane Risk of Bias tool (RoB 2) for randomized controlled trials (RCT), 13 and ROBINS-I V2 for observational studies. 14 Visual summaries were generated using the Risk-of-Bias VISualization (Robvis) tool. 15 The Joanna Briggs Institute checklists were used for analytical cross-sectional and qualitative studies.16,17 For qualitative studies, overall quality was calculated as the proportion of “Yes” items; because no standard cut-offs exist, thresholds (low <0.5; moderate 0.5-0.7; high >0.7) were defined a priori for consistent interpretation.
Effect Measures
The effect measures reported by the original authors were accepted and used for both the synthesis and the presentation of results.
Synthesis Methods
A meta-analysis was not conducted due to the limited number of studies and the heterogeneity of interventions and outcomes, which precluded meaningful quantitative synthesis. Findings were synthesized narratively by outcome domain.
Results were synthesized by predefined outcomes: the impact of MIL-centered interventions on: 1) QOL; 2) mental health; 3) WTHD; and 4) existential and SWB.
Summary tables were used to aid comparison: Table 1 details study characteristics; Table 2, main results; Tables 3–5, risk of bias by study type; and Table 6, certainty and confidence of evidence.
Characteristics of the Included Studies (n = 8).
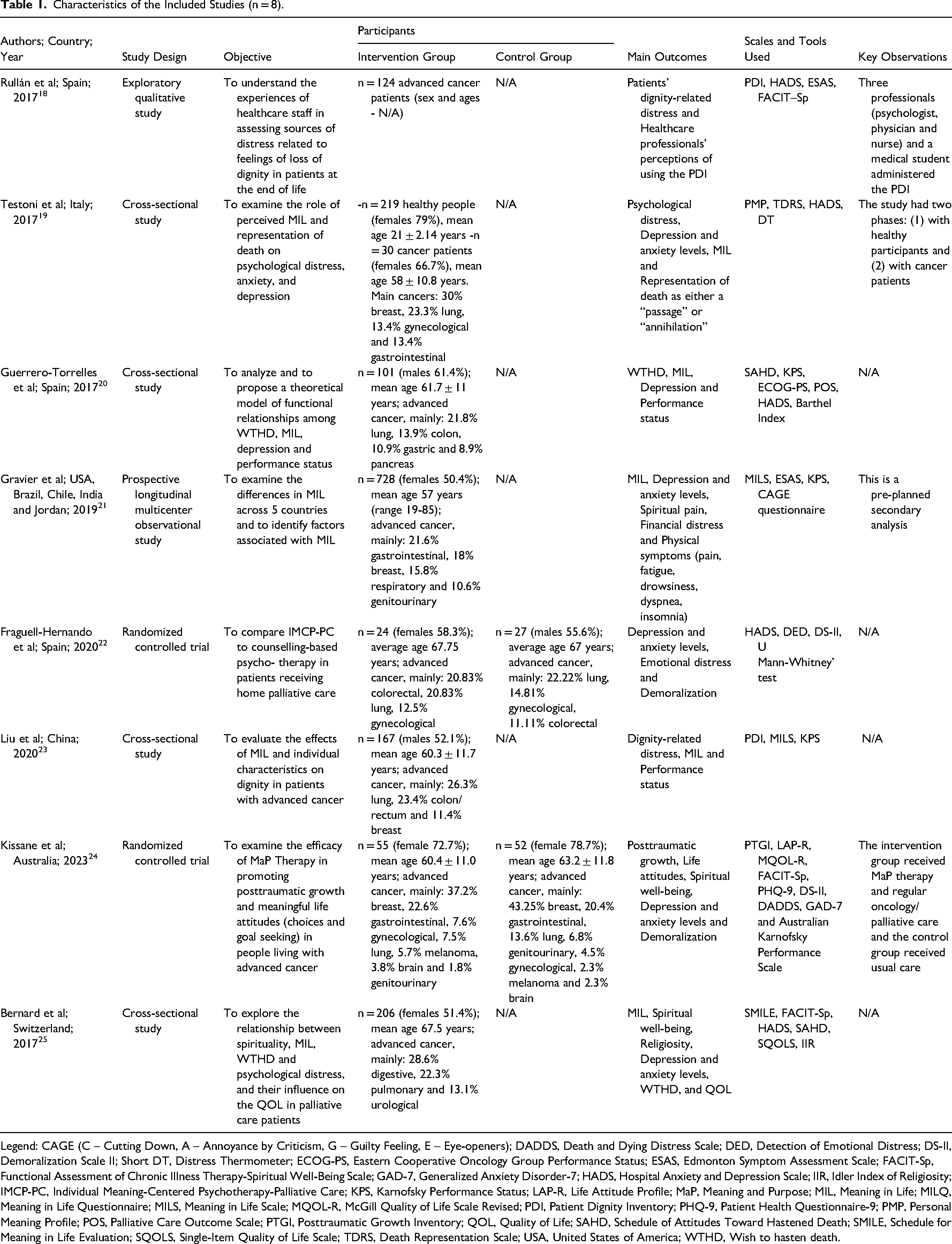
Legend: CAGE (C – Cutting Down, A – Annoyance by Criticism, G – Guilty Feeling, E – Eye-openers); DADDS, Death and Dying Distress Scale; DED, Detection of Emotional Distress; DS-II, Demoralization Scale II; Short DT, Distress Thermometer; ECOG-PS, Eastern Cooperative Oncology Group Performance Status; ESAS, Edmonton Symptom Assessment Scale; FACIT-Sp, Functional Assessment of Chronic Illness Therapy-Spiritual Well-Being Scale; GAD-7, Generalized Anxiety Disorder-7; HADS, Hospital Anxiety and Depression Scale; IIR, Idler Index of Religiosity; IMCP-PC, Individual Meaning-Centered Psychotherapy-Palliative Care; KPS, Karnofsky Performance Status; LAP-R, Life Attitude Profile; MaP, Meaning and Purpose; MIL, Meaning in Life; MILQ, Meaning in Life Questionnaire; MILS, Meaning in Life Scale; MQOL-R, McGill Quality of Life Scale Revised; PDI, Patient Dignity Inventory; PHQ-9, Patient Health Questionnaire-9; PMP, Personal Meaning Profile; POS, Palliative Care Outcome Scale; PTGI, Posttraumatic Growth Inventory; QOL, Quality of Life; SAHD, Schedule of Attitudes Toward Hastened Death; SMILE, Schedule for Meaning in Life Evaluation; SQOLS, Single-Item Quality of Life Scale; TDRS, Death Representation Scale; USA, United States of America; WTHD, Wish to hasten death.
Main Results of the Included Studies (n = 8).
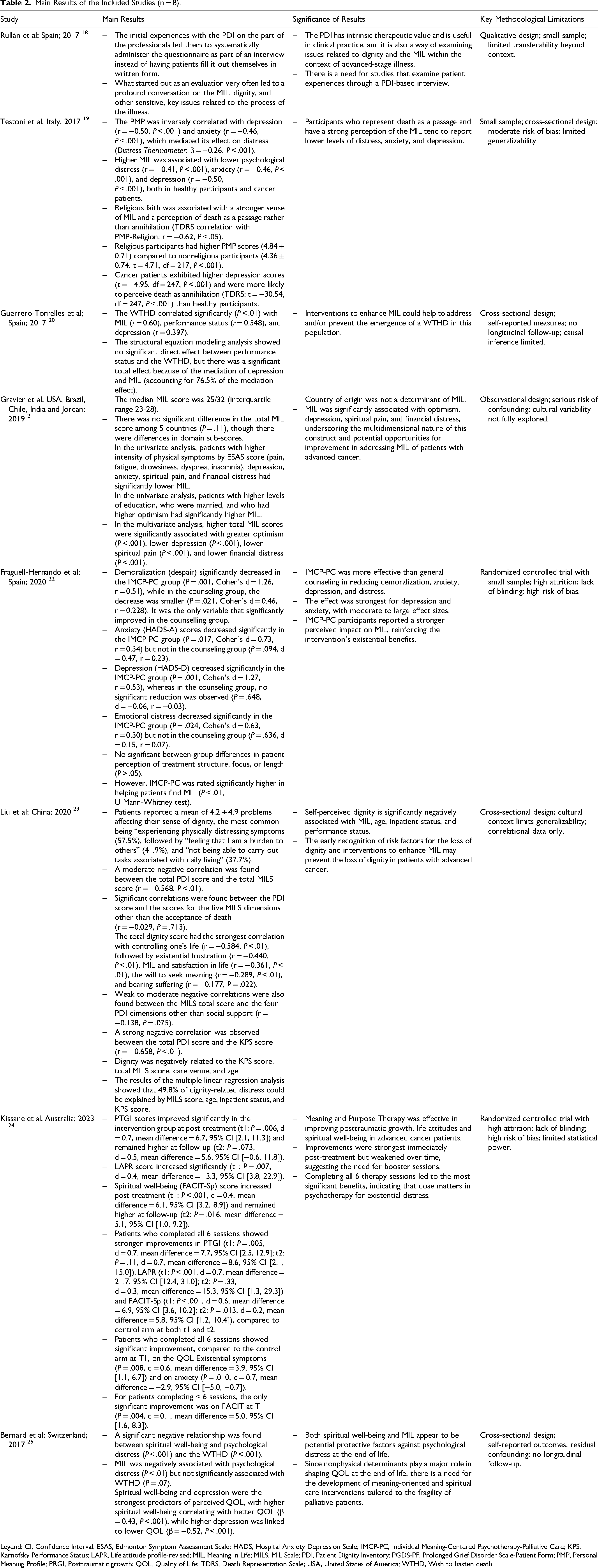
Legend: CI, Confidence Interval; ESAS, Edmonton Symptom Assessment Scale; HADS, Hospital Anxiety Depression Scale; IMCP-PC, Individual Meaning-Centered Psychotherapy-Palliative Care; KPS, Karnofsky Performance Status; LAPR, Life attitude profile-revised; MIL, Meaning In Life; MILS, MIL Scale; PDI, Patient Dignity Inventory; PGDS-PF, Prolonged Grief Disorder Scale-Patient Form; PMP, Personal Meaning Profile; PRGI, Posttraumatic growth; QOL, Quality of Life; TDRS, Death Representation Scale; USA, United States of America; WTHD, Wish to hasten death.
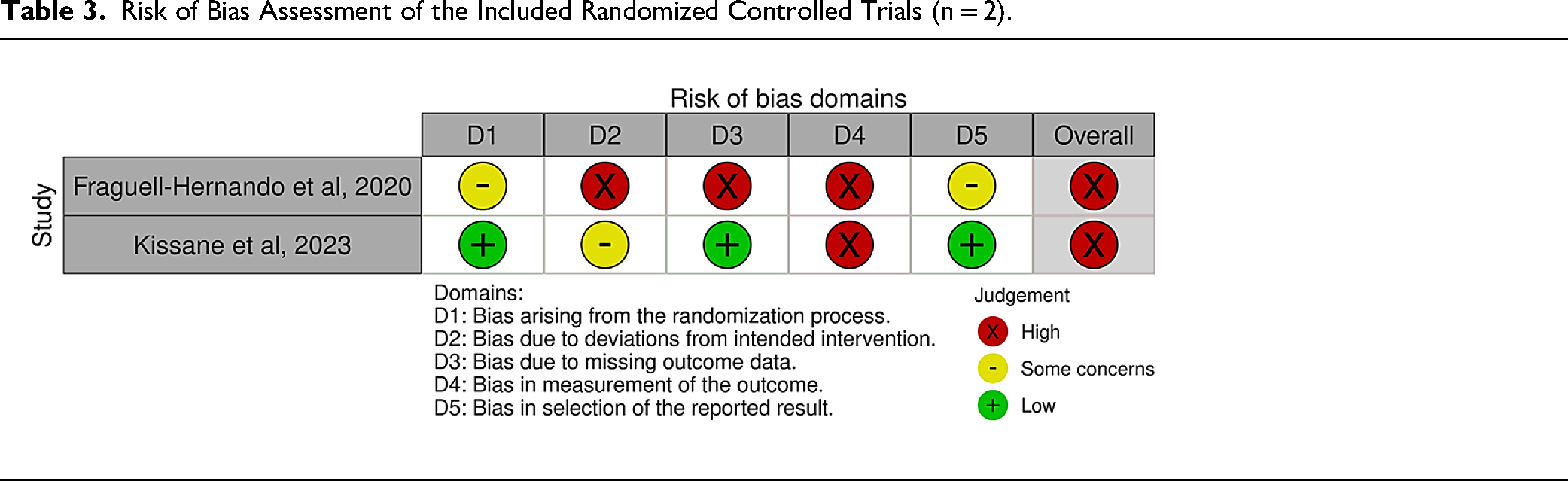
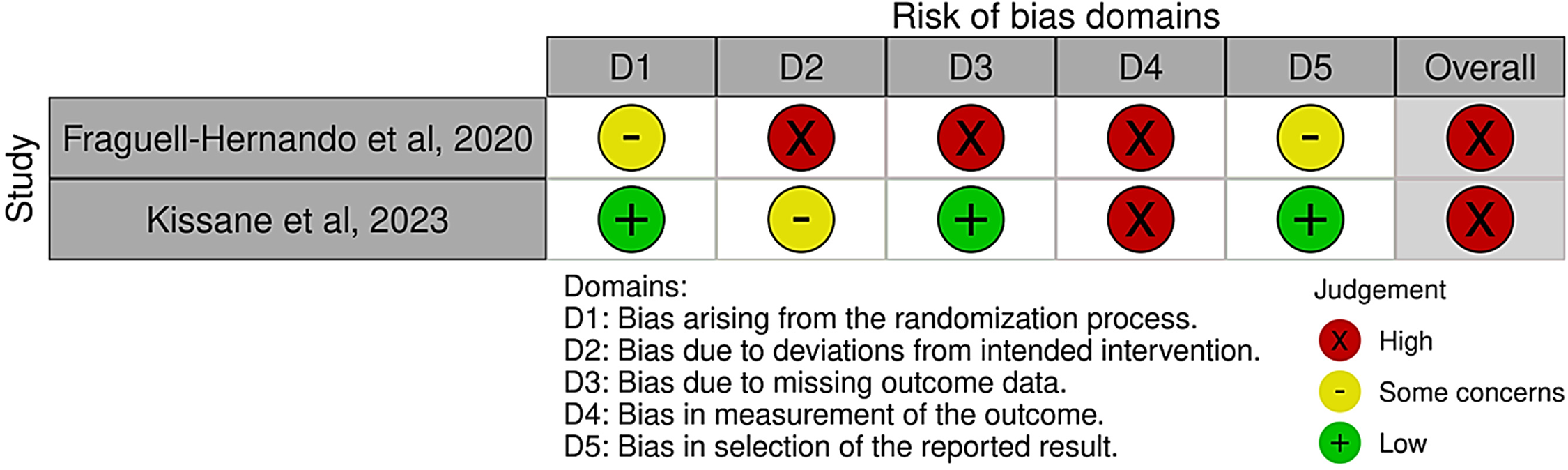
Risk of Bias Assessment of the Included Randomized Controlled Trials (n = 2).
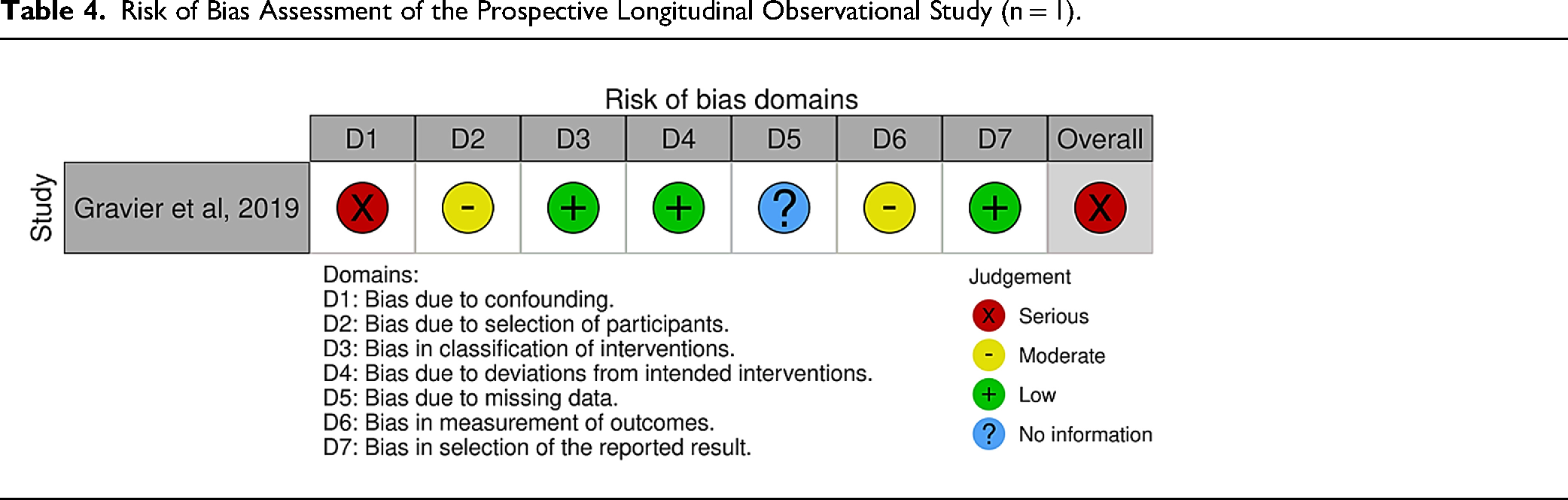
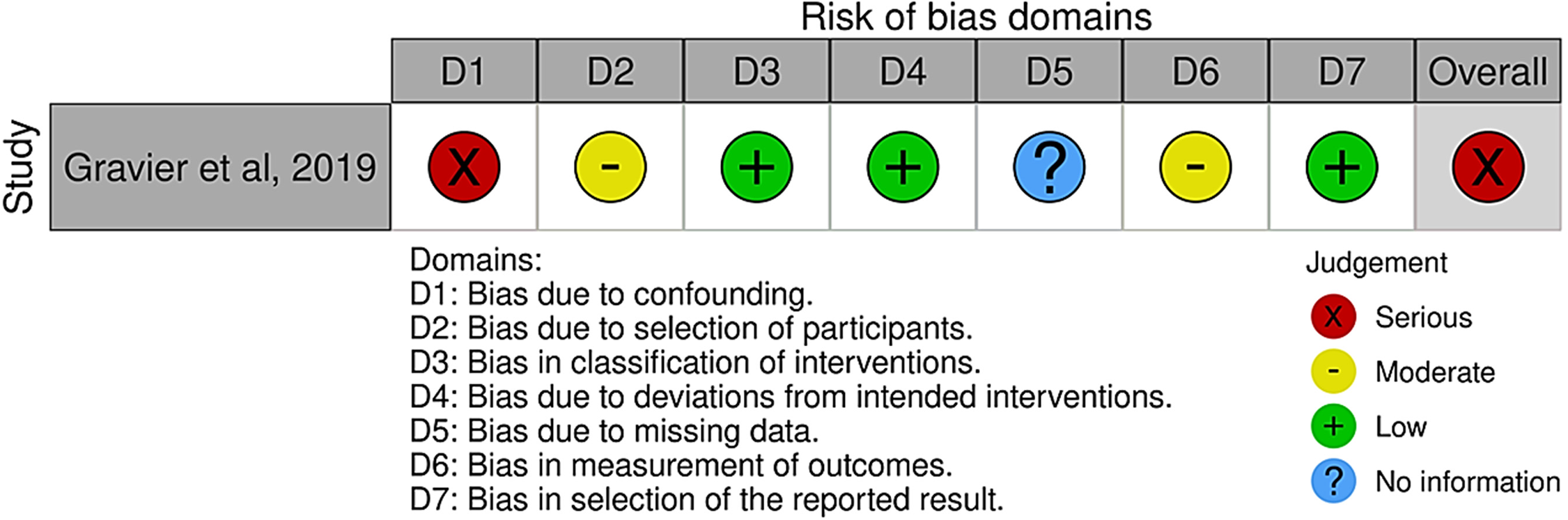
Risk of Bias Assessment of the Prospective Longitudinal Observational Study (n = 1).
Risk of Bias of Qualitative and Cross-Sectional Studies (n = 5).

Certainty and Confidence of Evidence: Summary of Findings (n = 8).
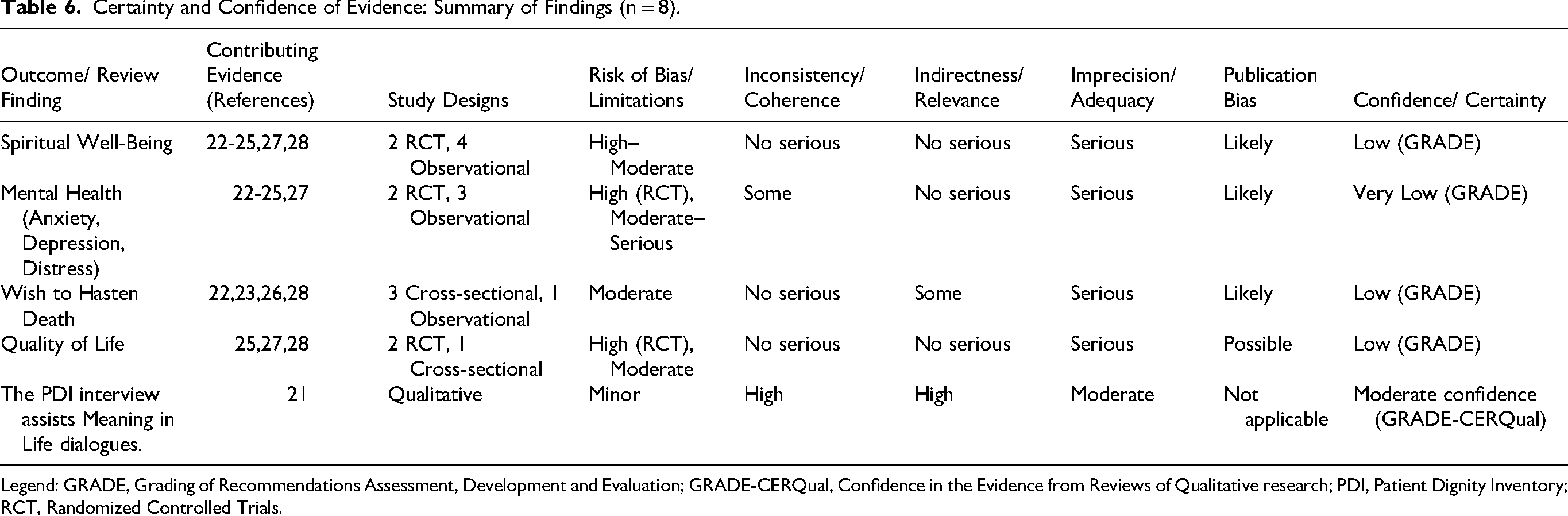
Legend: GRADE, Grading of Recommendations Assessment, Development and Evaluation; GRADE-CERQual, Confidence in the Evidence from Reviews of Qualitative research; PDI, Patient Dignity Inventory; RCT, Randomized Controlled Trials.
Certainty Assessment
Certainty and confidence of evidence were assessed separately for quantitative and qualitative findings. Two reviewers independently applied the “Grading of Recommendations Assessment, Development and Evaluation” (GRADE) approach to evaluate the certainty of evidence for quantitative outcomes. 26 Certainty ratings began at “high” for RCT and “low” for observational studies, and were rated down based on risk of bias, inconsistency, indirectness, imprecision, and publication bias. For the qualitative study, we used the “Confidence in the Evidence from Reviews of Qualitative research” (GRADE-CERQual) approach,27,28 assessing confidence based on methodological limitations, coherence, adequacy of data, and relevance. Narrative summary-of-findings statements were produced for all domains, as most studies did not report variances or provide effect estimates compatible with meta-analysis (Table 6).
GRADE and GRADE-CERQual assessments were applied post hoc. This methodological decision was made to enhance interpretability but is acknowledged as a limitation of the review.
Results
Study Selection
Eighty-four studies were identified. After removing 16 duplicates, 68 records were screened. Forty-eight were excluded based on title and abstract screening, leaving 20 for full-text review. One could not be retrieved due to subscription restrictions. Of the 19 assessed, 11 were excluded: nine for involving irrelevant populations (eg, healthcare professionals, students, or patients without advanced cancer), and two for evaluating non-aligned outcomes. Eight studies met all inclusion criteria and were included.18–25 The study selection process is summarized in Figure 1.
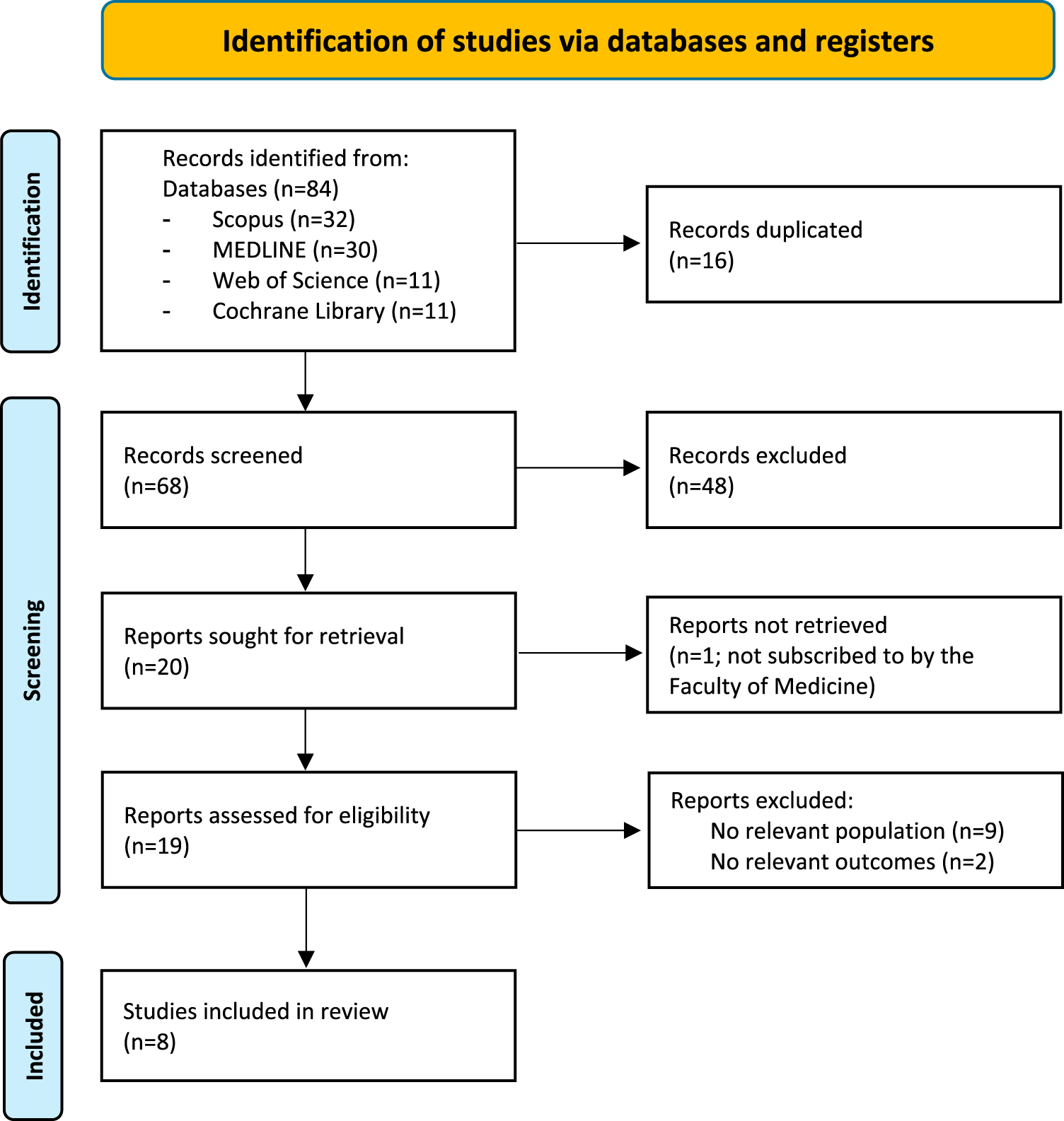
Flow diagram of the study selection process.
Study Characteristics
Eight studies were included: three from Spain, and one each from Italy, Switzerland, China, Australia, and a multicenter study across the United States of America, Brazil, Chile, India, and Jordan. Study designs comprised four cross-sectional studies,19,20,23,25 two RCT,22,24 one prospective longitudinal observational study, 21 and one qualitative study. 18 Across all studies, there were 1733 participants: 1514 advanced cancer patients and 219 healthy individuals. Table 1 summarizes the characteristics of the included studies.
Risk of Bias
All studies were assessed as having a high risk of bias, except Testoni et al., 19 which was rated as having a moderate risk of bias.
Randomized Controlled Trials
Fraguell-Hernando et al. were rated as high risk of bias (Table 3). 22 Major concerns included insufficient details on randomization and allocation concealment, significant deviations from intended interventions (per-protocol analysis with notable non-adherence), high attrition (37% did not complete the study), and subjective self-reported outcomes without blinding.
Kissane et al. were also judged as high risk. 24 While the randomization process and handling of missing data (via multiple imputation) were sound, the lack of blinding among participants and therapists raised concerns about deviations from the intended intervention and subjective outcome reporting, which likely influenced responses.
Observational Study
Gravier et al. were assessed as having a serious overall risk of bias, primarily due to confounding (Table 4). 21 Key determinants of MIL (eg, performance status, social support, QOL) were not included in the analysis. Moderate risk was noted in participant selection and outcome measurement. Information on missing data was insufficient.
Cross-Sectional Studies
Guerrero-Torrelles et al. were rated high quality (Table 5). 20 The study had well-defined inclusion criteria, valid tools, and appropriate statistical methods, including structural equation modeling. Limitations included its cross-sectional design and reliance on a single-item MIL measure.
Testoni et al. were rated moderate quality. 19 Inclusion criteria for cancer patients were clear, but less so for healthy participants. While settings, measures, and tools were generally appropriate, confounding factors were not fully addressed.
Liu et al. achieved high quality, meeting all eight criteria. 23 The study clearly described its population, used valid measures, identified confounders, and applied sound statistical techniques.
Bernard et al. were rated high quality, though identification and handling of confounders were rated “unclear.” 25 Inclusion criteria, measurements, and statistical analyses (including regression and Bonferroni correction) were appropriate.
Qualitative Study
Rullán et al. were also rated high quality (Table 5). 18 There was strong alignment between philosophical framework, methodology, and analysis. Participants’ voices were well represented through direct quotes, and ethical approval was obtained. Areas for improvement included a more explicit statement on the researchers’ theoretical positioning and influence on the research process.
Results of Individual Studies
The results of individual studies are summarized in Table 2.
Results of Syntheses
“Meaning in Life”-Centered Interventions and Quality of Life
Three of the eight included studies examined QOL in relation to MIL-centered interventions.22,24,25 Across these studies, SWB was consistently associated with higher QOL. Bernard et al. reported that SWB was a strong positive predictor of QOL (β = 0.43, P < .001), whereas depression was inversely associated with QOL (β = −0.52, P < .001). 25 However, the cross-sectional design precludes causal inference.
Kissane et al. observed improvements in posttraumatic growth, life attitude, and SWB following a MIL-centered intervention, indicating changes in psychological and existential outcomes over time. 24 Similarly, Fraguell-Hernando et al. found that participants receiving “Individual Meaning-Centered Psychotherapy-Palliative Care” (IMCP-PC) reported significant improvements in perceived MIL (P < .01) and emotional outcomes. 22 These findings suggest a possible relationship between MIL-focused interventions and QOL-related domains rather than definitive treatment effects. Interpretation of these results is limited by important methodological constraints. Bernard et al. relied on correlational data, 25 while both RCT were rated as high risk of bias due to substantial attrition, lack of blinding, and small sample sizes.22,24
Applying the GRADE framework, the certainty of evidence for QOL was rated as very low, driven by serious concerns regarding risk of bias, indirectness, and imprecision (Table 6). Accordingly, although the findings are consistent with a potential association between MIL-centered approaches and improved QOL-related outcomes, conclusions must remain cautious and tentative.
“Meaning in Life”-Centered Interventions and Mental Health
Six of the eight included studies examined the relationship between MIL and mental health outcomes.19–22,24,25 In cross-sectional analyses, Testoni et al. 19 reported strong inverse correlations between MIL and both depression and anxiety (r = −0.50, P < .001), while Bernard et al. 25 found that higher SWB was associated with lower psychological distress (P < .001). Similarly, in a large multinational study, Gravier et al. found that higher levels of depression (estimate = −0.45, P < .001) and anxiety (estimate = −0.36, P < .001) were significantly associated with lower MIL in univariate analyses. 21 These findings indicate consistent associations but do not permit conclusions about directionality or causation. Guerrero-Torrelles et al. further reported that depression was positively correlated with WTHD (r = 0.397, P < .01), highlighting the clinical relevance of psychological distress in PC, although the cross-sectional design and absence of longitudinal follow-up limit causal interpretation. 20 Interventional studies suggested short-term improvements in mental health outcomes following MIL-centered approaches. Fraguell-Hernando et al. reported statistically significant reductions in depression (P = .001, d = 1.27) and anxiety (P = 0.017, d = 0.73) among participants receiving IMCP-PC, whereas no comparable changes were observed in the control group. 22 Similarly, Kissane et al. reported moderate-to-large effect sizes in reducing depression (P = .008, d = 0.6) and demoralization (P = .003, d = 0.7) following “Meaning and Purpose” therapy. 24 However, both trials were rated as high risk of bias due to small sample sizes, lack of blinding, and substantial attrition, which may have inflated effect estimates.22,24
Overall, the certainty of evidence for mental health outcomes was rated as very low using GRADE, reflecting serious concerns related to risk of bias, imprecision, and potential publication bias (Table 6). While the findings are consistent with a possible protective role of MIL in relation to psychological distress, confidence in the magnitude and durability of these effects remains limited.
“Meaning in Life”-Centered Interventions and Wish to Hasten Death
Four studies examined associations between existential variables and the WTHD.19,20,23,25 Bernard et al. found a significant inverse correlation between SWB and WTHD (P < .001), 25 indicating that higher SWB was associated with lower endorsement of a WTHD. Guerrero-Torrelles et al. similarly found that depression and loss of meaning statistically mediated the relationship between physical impairment and WTHD. 20 While this modeling highlights potential pathways linking physical and existential distress to WTHD, the observational design limits causal interpretation and may not account for unmeasured confounding.20,25 Testoni et al. 19 further reported that higher MIL was associated with a reduced tendency to conceptualize death as annihilation (r = −0.62, P < .05), a cognitive representation that has been linked to attitudes toward death and dying. However, these findings were derived from a small sample (n = 30), substantially limiting statistical power and precision. 19 Liu et al. also observed inverse correlations between dignity-related distress and MIL (r = −0.568, P < .01), suggesting an association between perceived meaning and existential suffering. 23 Interpretation of these findings should consider the cultural and healthcare context of the study population, which may limit generalizability. 23
Across studies, evidence regarding WTHD is derived exclusively from correlational or model-based analyses, precluding conclusions about directionality or intervention effects. Applying the GRADE framework, the certainty of evidence for WTHD outcomes was rated as very low, reflecting serious concerns related to indirectness, risk of bias, imprecision, and potential residual confounding (Table 6). Collectively, the findings are consistent with a possible buffering role of MIL and SWB in relation to WTHD; however, stronger longitudinal and interventional evidence is required to substantiate this hypothesis.
“Meaning in Life”-Centered Interventions and Existential/Spiritual Well-Being
Six studies explored associations between MIL and existential or SWB.19–22,24,25 In cross-sectional analyses, Bernard et al. found that SWB was significantly associated with both perceived meaning and overall QOL (P < .001), 25 while Testoni et al. found that religious affiliation correlated with higher MIL scores (P < .001), suggesting that spiritual frameworks may contribute to existential grounding. 19 Guerrero-Torrelles et al. identified loss of meaning as a mediator between physical impairment and existential distress, 20 further underscoring the potential role of meaning in shaping psychological responses to illness. Gravier et al., in a cross-cultural sample, reported that spiritual pain was a key correlate of MIL, though the study did not explore cultural variations in detail. 21
Intervention studies offered additional, though limited, insight. Fraguell-Hernando et al. reported that participants receiving IMCP-PC experienced a significant increase in perceived meaning (P < .01), 22 and Kissane et al. observed improvements in SWB and life attitude following “meaning and purpose” therapy (P < .001 and P = .007, respectively). 24 However, both RCT were rated at high risk of bias due to high attrition and lack of blinding,22,24 and small sample sizes further reduced the certainty of effect estimates. Cross-sectional studies,19,20,25 and Gravier et al.'s observational design 21 also limit the ability to infer causality or directionality.
Applying the GRADE approach, the certainty of evidence for existential and SWB outcomes was rated as very low, due to serious concerns about risk of bias, methodological heterogeneity, and limitations in study design (Table 6). While conclusions must remain cautious, the overall pattern of associations across diverse contexts suggests that existential and spiritual dimensions are consistently linked with perceived meaning and may be relevant targets for MIL-centered care.
Certainty of Evidence
Certainty of evidence for quantitative findings ranged from low (QOL, WTHD, SWB) to very low (mental health outcomes), primarily due to high risk of bias, imprecision, and potential publication bias.
The sole qualitative study, Rullán et al., 18 was appraised using GRADE-CERQual, resulting in moderate confidence in its core findings about the therapeutic and existential value of “Patient Dignity Inventory”-facilitated conversations.
Discussion
Summary of Evidence
This systematic review synthesized empirical evidence on the role of MIL in PC settings. Eight studies met inclusion criteria, spanning diverse methodologies: four cross-sectional studies, two RCT, one longitudinal observational study, and one qualitative study. The total sample included 1733 participants, the majority of whom were patients with advanced cancer.
Several studies reported associations between MIL-centered interventions and outcomes such as improved QOL, reduced emotional distress, enhanced existential and SWB, and decreased WTHD. However, these findings must be interpreted with caution. The empirical literature remains limited and heterogeneous, with marked variation in how MIL is conceptualized, operationalized, and integrated into interventions. Moreover, only two studies employed randomized designs, both of which were rated at high risk of bias. Observational and cross-sectional studies comprised the majority of the evidence base, restricting causal inference.
While the findings tentatively suggest that attending to MIL may hold value in PC, the overall certainty of the evidence was judged to be very low, particularly across quantitative outcomes. Our application of GRADE and GRADE-CERQual highlighted methodological shortcomings, including small sample sizes, lack of blinding, high attrition, and unmeasured confounding. These limitations constrain the strength of any conclusions regarding effectiveness. Although studies were conducted across diverse cultural settings, differences in the conceptualization and measurement of MIL were insufficiently examined, precluding meaningful cross-cultural comparison.
Nevertheless, the review highlights a consistent thematic signal across diverse settings: MIL and existential concerns are relevant to the lived experience of patients with advanced cancer. Future research should prioritize conceptually coherent interventions, methodologically robust designs, and longitudinal evaluations to clarify causal pathways and inform holistic, person-centered models of care at the EOL.
General Interpretation of Results
The evidence synthesized in this review suggests that MIL may be an important contributor to QOL in PC, but the overall strength of this evidence remains limited. Interventions focused on MIL yielded improvements in overall well-being and QOL. 29 These findings are partially supported by the wider literature. A meta-analysis by Dietrich et al. 30 confirmed that meaning-centered psychotherapies have a large effect on improving QOL. This connection is further reinforced by evidence that MIL exerts a significant indirect effect on QOL through pathways involving SWB and depression in patients with terminal cancer, underscoring its potential role in enhancing EOL experiences. 31 Similarly, family and interpersonal relationships were identified as key sources of MIL among Spanish patients with advanced cancer, contributing to higher satisfaction and QOL. 32 In addition, a positive correlation between spiritual transcendence, MIL, and global QOL was observed in Polish EOL cancer patients, highlighting the universality of meaning as a fundamental human need across diverse cultural contexts. 33 This connection is so fundamental that foundational frameworks like Ferrell's QOL model explicitly include the spiritual domain—encompassing meaning—as a pillar equal in importance to physical and psychological well-being. 29
This review highlights MIL's possible role as a buffer against psychological distress, particularly depression, 19 anxiety, 19 and demoralization. 24 The significant impact on demoralization is especially noteworthy, as it aligns with the work of Dong et al. and others who identify demoralization—a state of existential anguish and hopelessness—as a primary target for MIL-based therapies. 34 A broader meta-analysis by Izgu et al. reinforces this, concluding that spiritual interventions, often centered on meaning, are effective in reducing psychological distress in this population. 35 “Meaning of Life” Therapy, a culturally adapted intervention, elicited themes of family, identity, and reconciliation, effectively addressing psycho-existential needs and reducing distress in Portuguese PC patients. 36 Among Chinese lung cancer patients undergoing radiochemotherapy, MIL was significantly associated with lower psychological distress, with mood state and social support identified as key contributing factors. 37 Demoralization, marked by hopelessness and a loss of meaning, was reported in 13%–18% of cancer patients and was significantly linked to inadequately treated depression and anxiety. 4 Meaning-Centered Group Psychotherapy significantly reduced depression and anxiety scores in patients with advanced urological tumors, further reinforcing the therapeutic potential of MIL-focused interventions. 38 While these findings are promising, our GRADE analysis rated the certainty of evidence for mental health outcomes as very low, requiring cautious interpretation.4,5
A critical finding of this review is that a stronger sense of meaning may help mitigate the WTHD by addressing its existential roots. The study by Guerrero-Torrelles et al. illustrates this mechanism, showing that the loss of MIL was the most significant mediator between physical impairment and the WTHD. 20 This suggests that it is not physical decline itself, but the resulting loss of purpose, that may drive the WTHD. This is corroborated by Bernard et al., who found a significant inverse correlation between SWB and WTHD, 25 and Liu et al., who linked dignity-related distress—a proxy for lost meaning—to higher WTHD. 23 These findings echo the conclusions of major reviews by Rodríguez-Prat et al. and Monforte-Royo et al., which identify existential distress as a more potent driver of WTHD than physical symptoms.39,40 Spanish patients with advanced cancer prioritized interpersonal relationships as key sources of MIL, which may foster a sense of connection and purpose. 32 Consequently, MIL-centered interventions, by aiming to restore a sense of purpose, dignity, and value, may play a role in reducing WTHD. A recent systematic review on the WTHD in patients with life-limiting conditions identified depression, pain, functional impairment, diminished sense of MIL, perceived burden on others, and reduced QOL as the most commonly reported associated factors. 41 Nonetheless, our review rated the overall certainty of evidence for WTHD as very low, limiting the strength of conclusions.
Finally, this review affirms that MIL and SWB are deeply intertwined and mutually reinforcing constructs. The multinational study by Gravier et al. found that spiritual pain was a significant negative predictor of MIL.
21
Conversely, interventions focused on meaning were shown to improve SWB.
24
Rullán et al. observed that the very process of discussing dignity and meaning was inherently therapeutic and enhanced SWB.
18
A meta-analysis by Bauereiß et al.
42
confirmed that existential interventions have a moderate positive effect on SWB (g = 0.52). “Meaning of Life” Therapy, which incorporates elements such as forgiveness and legacy documents, significantly enhanced SWB by addressing existential needs in PC patients.
36
SWB and MIL were shown to significantly mediate the impact of depression on QOL, reinforcing their interconnected roles.
31
Spirituality and religion were identified as important sources of MIL, with the overall sample reporting high satisfaction scores, suggesting both cultural and developmental influences on SWB.
43
Additionally, 86% of advanced cancer patients endorsed spiritual concerns; thinking about meaning was significantly associated with poorer psychological QOL, yet addressing these concerns was considered critical for improving both SWB and overall QOL.
44
These findings support the framework proposed by Ferrell, which underscores that addressing spiritual needs and sources of meaning is not optional but a fundamental, evidence-based component of PC.
45
Although spiritual care is widely recognized as a cornerstone of PC, many healthcare professionals report difficulties in integrating it into clinical practice. The
Limitations
The principal limitation of this review is that its conclusions are necessarily based on a small and methodologically weak body of evidence. Only eight studies met inclusion criteria, and the majority were affected by substantial design limitations. Only two studies were RCT, both of which were rated as having a high risk of bias, primarily due to non-blinded outcomes and high attrition. Most included studies were cross-sectional, precluding conclusions about causality or long-term effects. Sample sizes varied considerably, with several studies involving fewer than 50 participants, limiting statistical power and increasing the risk of imprecise effect estimates. These limitations were reflected in our GRADE assessments, which rated the certainty of evidence for all quantitative outcomes as very low.
In addition, there was marked heterogeneity in how MIL was conceptualized and measured across studies. A wide range of instruments was used, each capturing different dimensions of meaning. This variability complicates comparisons across studies and substantially limits the feasibility of quantitative synthesis (eg, meta-analysis). Furthermore, outcomes were predominantly self-reported, which may be influenced by social desirability bias or by patients’ psychological state at the time of assessment. Nevertheless, self-report measures remain standard in existential research, given the inherently subjective nature of constructs such as MIL and SWB.
Several review-level limitations should also be acknowledged. Although the review was conducted rigorously and followed PRISMA 2020 guidelines, the search was restricted to four databases and to English-language publications from 2016 to 2024. This may have excluded relevant studies published earlier or in other languages, introducing potential language and publication bias. The search strategy was developed by the authors without the involvement of an information specialist or medical librarian, which may have affected comprehensiveness. Grey literature, conference abstracts, and dissertations were not included; while this may enhance internal validity, it further reduces the breadth of the evidence base.
Finally, due to substantial heterogeneity in study design, populations, and outcome measures, no meta-analysis could be conducted. Although narrative synthesis was appropriate, it is inherently more subjective and less robust than quantitative approaches. The application of GRADE and GRADE-CERQual frameworks was performed post hoc and was not pre-specified in the PROSPERO registration; while these assessments improve interpretability, their retrospective application represents an additional limitation.
Implications for Practice, Policy, and Future Research
The findings of this review suggest that existential suffering, including concerns related to MIL, is a relevant dimension of patient experience in PC. However, given the very low certainty of evidence identified using GRADE and GRADE-CERQual, these findings should be interpreted cautiously. At present, the evidence supports awareness and recognition of existential distress rather than the routine implementation of MIL-centered interventions. Healthcare professionals may benefit from training to identify existential concerns and to initiate supportive conversations or appropriate referrals, particularly when patients express distress related to meaning, purpose, or legacy. Brief, structured conversations about meaning may be acceptable and potentially supportive, but their therapeutic impact remains insufficiently established.
Therapeutic models such as IMCP-PC and “meaning and purpose” therapy have shown promising associations with improvements in existential and psychological outcomes in small and methodologically limited studies. However, the current evidence base does not justify their integration into routine care, and their use should remain confined to research settings or specialized services until more robust evidence becomes available.
From a policy perspective, this review does not support immediate changes to clinical pathways or mandates for implementation. Rather, it underscores the importance of recognizing existential and spiritual dimensions as areas warranting further investigation within PC. Policies should prioritize support for high-quality research, training initiatives aimed at improving clinicians’ competence in addressing existential distress, and the development of culturally sensitive frameworks to guide future intervention design.
This review emphasizes the need for more rigorous trials on MIL-centered interventions in advanced illness. Future studies should: Use larger, diverse samples and longitudinal designs to examine the sustainability of benefits; Standardize outcome measures to allow for comparability and meta-analysis; Explore mechanisms of change in meaning-centered therapy; Examine cultural factors influencing the experience and relevance of MIL; Evaluate the feasibility, cost-effectiveness and scalability of interventions in real-world PC settings.
Addressing these gaps is essential before meaningful clinical or policy recommendations can be made.
Conclusions
This systematic review identified consistent associations between MIL and key psychological and existential outcomes in patients with advanced cancer receiving PC. Across the eight included studies—most of which were small, affected by high attrition, and methodologically limited—MIL was reported to be inversely associated with depression, anxiety, demoralization, and WTHD, and positively associated with QOL and SWB. These patterns emerged across diverse clinical and cultural contexts, suggesting that MIL may be a relevant and potentially beneficial focus of care in serious illness.
However, the overall certainty of evidence was very low. Findings should therefore be interpreted as preliminary and hypothesis-generating. At present, MIL support remains a promising but unproven adjunct to comprehensive PC, rather than an established standard of care. The results underscore the urgent need for high-quality research, including adequately powered trials and longitudinal studies, to determine the effectiveness, mechanisms, and appropriate implementation of MIL-centered interventions.
Addressing patients’ need for meaning, dignity, and purpose may hold therapeutic potential, but more rigorous evidence is needed before existential care can be fully integrated into routine PC practice.
Key Message
In this systematic review (n = 8), fostering MIL in palliative care correlated with higher quality of life, lower emotional distress, greater existential and spiritual well-being, and a reduced wish to hasten death, highlighting the urgent need for standardized tools to assess meaning.
Supplemental Material
sj-docx-1-pal-10.1177_08258597261426760 - Supplemental material for Meaning in Life in Palliative Cancer Care: Psychosocial and Existential Outcomes—A Systematic Review
Supplemental material, sj-docx-1-pal-10.1177_08258597261426760 for Meaning in Life in Palliative Cancer Care: Psychosocial and Existential Outcomes—A Systematic Review by Francisco Rodrigues-Fouto and Paulo Reis-Pina in Journal of Palliative Care
Footnotes
List of Abbreviations and Acronyms
Acknowledgements
None.
Authors Contributions
This study was conceptualized by FRS and PRP. FRS and PRP conducted searches and screening of articles, analyzed data, designed the review protocol, wrote the manuscript, reviewed it, and approved the definitive version of the paper.
Ethical Considerations
Not applicable. It is a systematic review.
Consent to Participate
Not applicable. It is a systematic review.
Consent for Publication
Not applicable. It is a systematic review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data relevant to this study are included within the article. No additional datasets, code, or materials were generated or used.
Registration and Protocol
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.