
Abstract
Introduction
Cancer is a leading cause of death for adolescents and young adults, with intensive and complex care requirements.1–5 Adolescence is a time of emotional, social, and physical growth. However, when an adolescent or young adult is diagnosed with advanced cancer it impacts their identity, relationships, and psychological, social, and cognitive development given their impending death.6,7 There is a major care focus on the needs of the adolescents, managing pain, and other symptoms to ensure what is perceived to be a “good death” with minimal suffering.8,9
There are also impacts on those caring for adolescents and young adults with advanced cancer. Care is potentially taxing with risks of emotional burnout underpinned by a sense of failure.10,11 Healthcare workers express major concerns relating to helping people to accept palliative care, uncertainty about family involvement, and profound concerns about the workers own sense of tragedy and emotional proximity.10,12–15 Recent research reinforced issues of emotional confrontation and helplessness, questioning of professional skills, navigating uncertainty, and organizational obstacles. 16
Research that explores the perspectives of healthcare workers remains scant, and especially work focused on workers specializing in hospice and palliative care, where these issues may be particularly pertinent. Previous research has primarily focused on acute care settings.10,14 Therefore, the aim of this study is to explore the lived experiences of hospice healthcare workers who care for adolescents and young adults with a diagnosis of advanced cancer who are receiving palliative care. This study was completed as part of a PhD and is reported according to COREQ guidelines. 17
Methods
Design
This study was conducted throughout according to the principles of interpretative phenomenological analysis (IPA). The study is situated within an interpretivist and constructivist philosophical stance. 18 It takes a phenomenological, hermeneutic, idiographic stance. 18 Interpretative phenomenological analysis enables an in-depth understanding of lived experience, where the researcher also makes sense of the lived experience.
Population
A homogeneous population of hospice healthcare workers who work with adolescents (aged 10-19) and young adults (20-24) was sought. 19 Full inclusion and exclusion criteria are presented in Table 1.
Inclusion and Exclusion Criteria of the Study.
Setting
Pediatric hospices within Canada were selected as the setting for the study. Pediatric hospices in Canada provide palliative care support to children, adolescents and young adults to the age of 18 years. While there are 13 pediatric palliative care programs (mostly located in tertiary and acute care settings) and 6 pediatric hospices in Canada, 20 the focus on hospice settings both facilitated broadening the current acute care evidence base and enhanced homogeneity.
Sampling
A purposive approach congruent with IPA was used to identify a homogeneous group of those working as specialists in palliative care within similar hospice settings who would have rich experiences to share. 18 While it is acknowledged that they had varying characteristics including professional background, age, and gender, they shared an experience of the core phenomena under study. In IPA, sufficiency of the sample is determined through assessment of the richness of the data, and data facilitating comparison. 18
Recruitment
Study information was circulated to potential participants by an identified study contact within each hospice. If interested, potential participants contacted the research team to discuss the study and arrange a mutually convenient time for the interview.
Ethical Considerations
Research Ethics Committee approval was granted by Lancaster University, the Faculty of Health and Medicine Research Ethics Committee (FHMREC) (October 18, 2019, FHMREC18014), and the Health Research Ethics Board through the University of Alberta (February 26, 2019, Pro00079604).
Data Collection
In-person interviews were conducted by NP within the hospice settings. As the aim was to produce rich, meaningful, and detailed experiences of this phenomenon. 21 Open-ended and nondirective questions provided the foundation for the interviews, congruent with the IPA approach. 22 Each interview began with the question, “Can you please tell me about the experience of providing palliative care to adolescents and young adults living with cancer?.” Beginning with this one question allowed the participant to guide the interview based on their experiences. Probing and nonleading questions were asked to further explore the participants’ experiences. Reflective field notes were produced to capture the essence of each interview.
Data Analysis
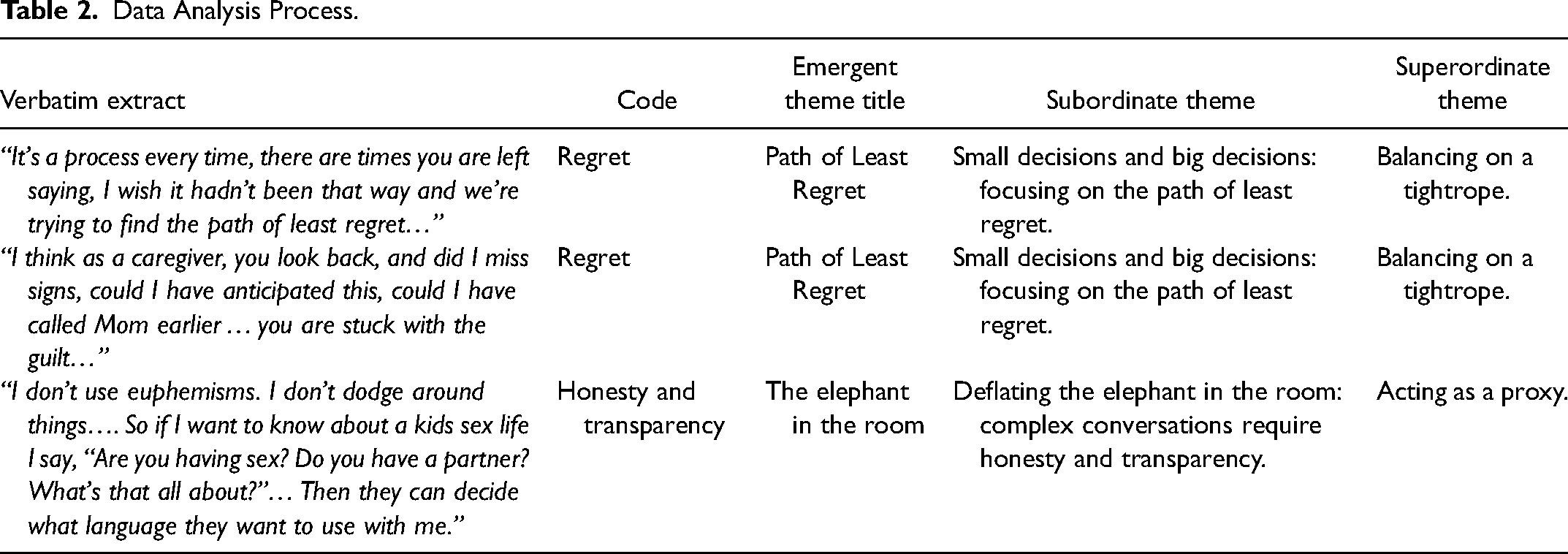
Interviews were audio-recorded and transcribed verbatim. Interpretative phenomenological analysis is iterative and cyclical involving 4 stages: a first encounter with the text, preliminary themes being identified, grouping themes into clusters, and tabulating the themes into a summary table. 23 Each transcript was read twice to ensure accuracy and to capture the essence and meaning of each interview. 24 NVivo 12 was used to help organize data. Through the second reading initial notes were turned into codes and then emergent theme titles by focusing on the theoretical framework of IPA and the voices of the participants. 25 The developing themes were clustered and given an overarching name and these represented the subordinate themes. 25 All participants were pseudonymized. Table 2 illustrates the data analysis process.
Data Analysis Process.
Reflexivity in IPA is a key part of the research process. 26 NP has a social work background and works in the field of palliative care with an in-depth knowledge of the provision of palliative care in Ontario, Canada. However, the experiences related to the phenomenon being explored were limited. As a reflexive research practitioner, the intersections of power and knowledge, coupled recognition of the experience of working in palliative care were acknowledged. A self-reflective journal was kept throughout the research process to address positionality and intersectionality. This journal ensured that personal biases and assumptions were managed. There were multiple critical thinking discussions with two PhD supervisors, CW and SB.
Results
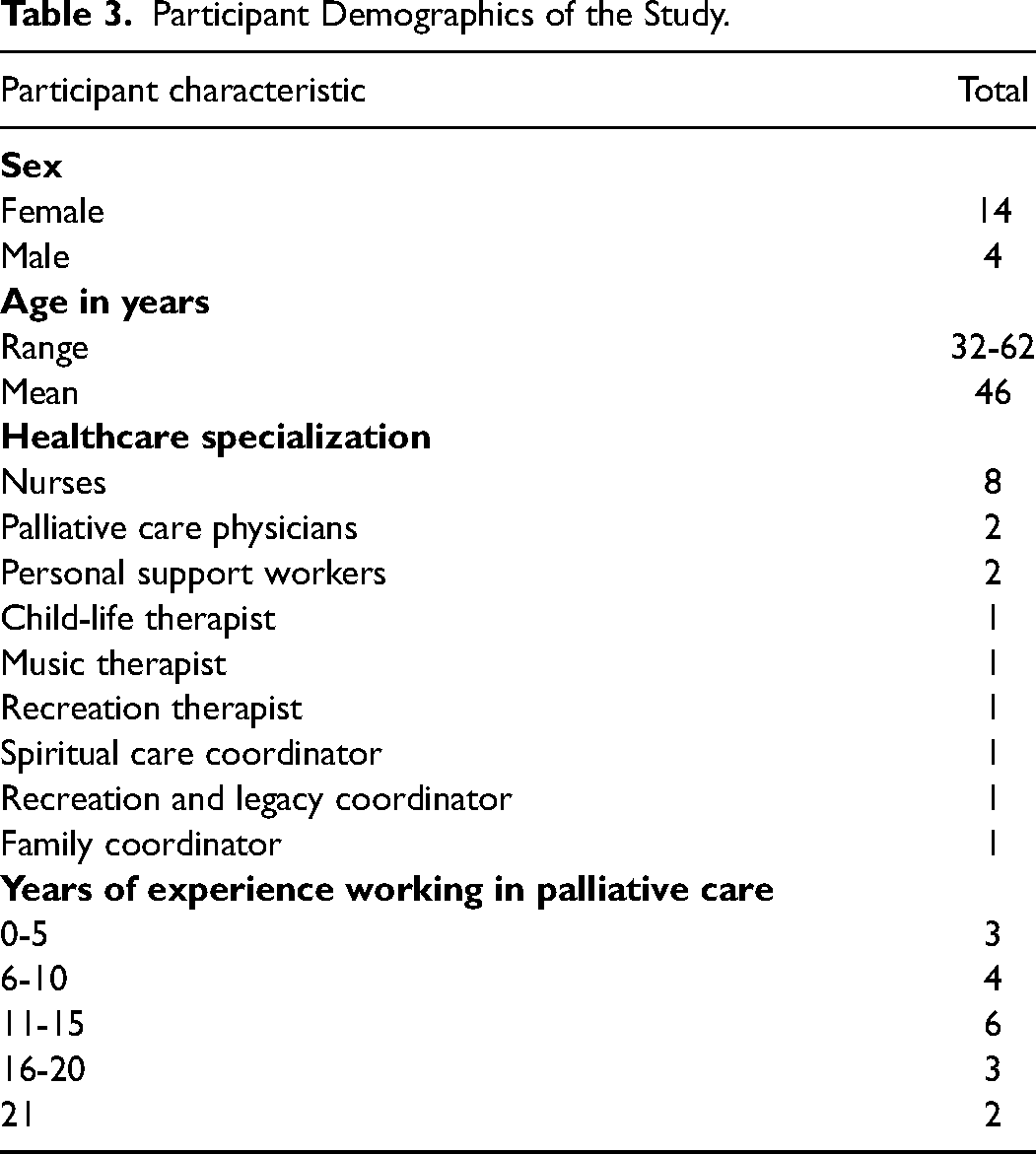
Eighteen hospice healthcare workers participated from four pediatric hospices across Canada. During July to November 2018, interviews were conducted and lasted between 43 and 59 min (mean 52 min). Table 3 provides detailed participant demographics:
Participant Demographics of the Study.
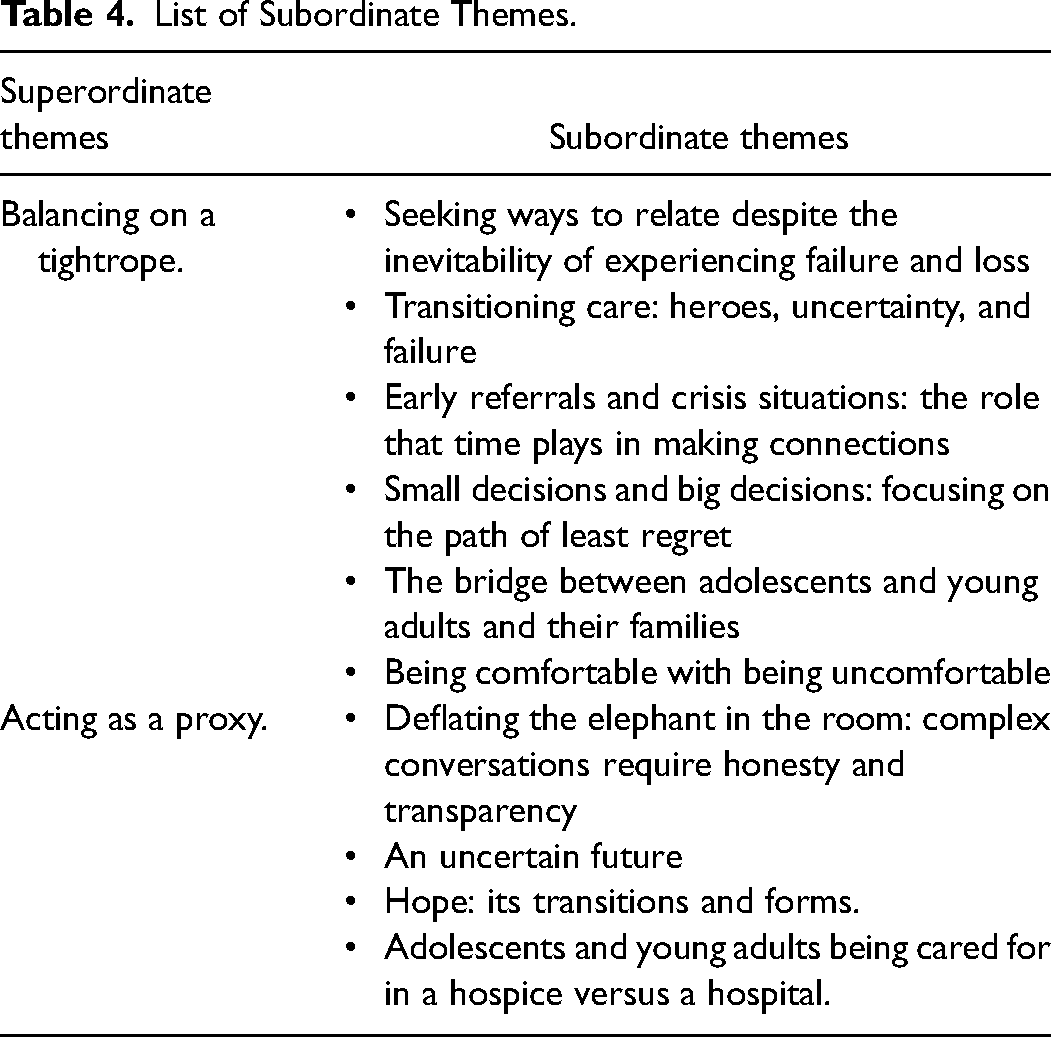
Two overarching superordinate themes were identified: balancing on a tightrope and acting as a proxy. These were created from 10 subordinate themes identified during the IPA analysis. Table 4 provides a list of the subordinate themes.
List of Subordinate Themes.
Balancing on a Tightrope
Finding ways of relating to adolescents and young adults played an important role in the delivery of care. Healthcare workers worked hard at building connections that supported the hopes and wishes of adolescents and young adults: The critical role that we play really is through relationships. If we can develop a relationship with a family or a patient, we can understand and translate for them the medical tools that will serve their hopes and wishes better. (Palliative Care Physician Kurt)
Concerns were raised that the relative lack of shared interests with the adolescents and young adults for whom they cared could lead to challenges with connections. Healthcare workers felt they needed to find unique ways of connecting with this population. Taking the extra time to find ways of being less medical and more personal was viewed as being important. A typical doctor thing is to say, “How are you? How is your pain today?” “And I'll come in and say,” Wow. “What music are you listening to?” “Oh. I don't know that band tells me about it.”… I'll go home and I'll YouTube it and I'll listen to it and…then I'll be able to have a conversation with them. (Palliative Care Physician Howard)
Healthcare workers play an important role in decision-making with adolescents and young adults and their families. They place pressure on themselves to do the best that can and hope for decisions that would cause them the least regret. It's…a process every time, and … there are times when you are left saying, “I wish it hadn't had to have been that way … and we're trying to find the path of least regret … so when it comes down to hospice…we are all of us trying to do what we think is best…” (Palliative Care Physician Kurt)
Nurse Kim shared a story of an adolescent whom she supported who died suddenly while in the middle of making a wish come true. Nurse Kim shared this story with such guilt and regret as things did not go as planned: I was by myself … and then Mom was honestly like grief stricken and angry and it didn't go the way that I would have ever wanted it to go..I don't even think looking back like anything would have necessarily changed or gone any different but … then you go through all the emotions … like they didn't get to say goodbye and I didn't get to hold him, and I didn't get to say, “I love you.”…
Healthcare workers made it their responsibility to do their best when caring for adolescents and young adults. Healthcare workers often found it difficult to cope with their own discomfort when decisions were made that they did not support. However, when things worked out, healthcare workers shared these stories with relief and thankfulness. There was a young man … he was 17…he needed to see his mother. So, it wasn’t easy because he had a lot of … medication and he had to go alone…we weren’t sure if…he could make it … we arranged everything and then he was over there with his mother…he had …a satellite phone…and when I talked to him, he was like, “This is the best day of my life. I’m with my mom … she's with me. I’m in … her arms” … and so for me, that was great, you know … and he came back, he died a few days after that…. (Nurse Alissa)
Acting as a Proxy
Being honest and sharing accurate information was felt to enable the establishment of trust between healthcare workers and adolescents and young adults. Using euphemisms was not felt to be a good way of communicating with adolescents and young adults. Rather being direct while also being compassionate while leading complex conversations was viewed as important. I don't use euphemisms. I don't dodge around things…. So if I want to know about a kids sex life I say, “Are you having sex? Do you have a partner? What's that all about?”… Then they can decide what language they want to use with me. (Palliative Care Physician Howard)
Adolescents and young adults were described as at an age where they were thinking about the future and such things as university, marriage, and planning their goals. Healthcare workers found they often had to be ready to answer the practical questions of how life could go on as “normal.” When conversations about death were had, adolescents and young adults often thought about how this would impact their future. Adolescents are very quick to ask. How is this going to affect my life? How's this going to affect my self-esteem? How is this gonna affect my English class? How is this going to affect that … degree I wanted to pursue at this university? (Nurse Sabrina)
As healthcare workers often felt as if they had to have all of the answers, it took bravery to be present and not speak. Having a silent presence was viewed as important. Being present and listening also supported healthcare workers to reflect on their own personal practice and identify their personal needs. Being a compassionate presence was important involving empathy, observation, and opening space for multiple emotions. So sometimes you just don't say anything. You just listen … you have to have big ears and a … small mouth … you have to listen to them… (Family Coordinator Alexandra)
When working with adolescents and young adults, the healthcare team tried to ensure that the adolescent or young adult's wishes were achieved. Experiences were described around special milestones with this population, such as holidays, prom, graduating from school, being sexually active, and getting married. Supporting the completion of these wishes helped the healthcare workers cope with their own grief and experience feelings of satisfaction when wishes were met. When situations do not go as planned, there was a need for healthcare workers to forgive themselves as a way of working through their sense of failure and suffering. Reflecting on personal vulnerabilities played a role in forgiveness. I think I've become a lot more … forgiving of my humaneness … I can't get it right all the time … having compassion, not just for the vulnerabilities I see but also for my own … humaneness and vulnerabilities. (Music Therapist Kelsey)
Healthcare workers found it difficult to support this population. Death at their age was explained to be unfair. It was important for healthcare workers to find ways of coping. Your heart … is going to be broken in this work. The difference is some people repair it with steel and some people prepare it with gold. Some people have hearts of steel, and some people have hearts of gold, and it's the way in which we allow ourselves to heal from that … because we're going to break. These are kids who are dying. (Recreation and Legacy Coordinator Helen)
Discussion
Inherent within both superordinate themes is a need for or call to action. The steps taken and gestures made by hospice healthcare workers reflect this action-focused orientation: the need to do. Hospice healthcare workers ensure that when they are supporting decision-making they focus on the well-being of the adolescent and young adult and decisions made so that they can later feel comfortable with themselves. Protection of self, however, was identified as important, forming a key part of the cycles of protection (whereby hospice healthcare workers want to protect themselves, adolescents, and young adults and their families; adolescents and young adults seek to protect their families; and their families want to protect adolescents and young adults).
Doing for Rather Than Being With
The theme of walking on a tightrope fits the need to balance doing for and being with. Hospice healthcare workers strive to do their best, often through attempting wish fulfillment. Wish fulfilment can be viewed as enriching life, maintaining hope, easing suffering, and adding joy.27,28 Wishes are viewed as being different from a goal; wishes are meant to be magical experiences which go above and beyond day-to-day experiences, a way of making dreams a reality. 28 Wish fulfilment by health and social care workers is also suggested as a way of being with by meeting needs and listening to how families are adapting and coping.27,29 However, wish fulfillment for hospice healthcare workers may be rooted in the notion of doing for, to help hospice healthcare workers do their best while taking the path of least regret for themselves. The notion of “doing” is not intrinsically “wrong” but can lead to negative outcomes for healthcare workers when the intended result does not occur or when healthcare workers are unable to acknowledge their limitations and their own expectations.
Doing More to Achieve a “Good Death”
When supporting adolescents and young adults, there is a connection between grand gestures and how a good death is defined. The concept of a good death for adolescents and young adults is often questioned due to the uncertainty of defining and achieving it.30,31 However, experiences leading up to death can result in adolescents and young adults having meaningful moments contributing to what some would consider a good death journey. 32 Healthcare workers going beyond their call of duty by carrying out gestures have been described as rooted in compassion. 33 However, these grand gestures were described as an indicator to understand better if these actions are from a place of altruism or an internal motivator for external recognition. 33 Nurse Kim and Nurse Alissa shared stories of grand gestures they did to achieve a good death. The notion of grand gestures and aiming for a “good death” may go beyond both altruism and recognition, it may be a way of coping with the emotional challenges hospice healthcare workers experience while caring for this population.
The Cycles of Protection
This need for healthcare workers to protect themselves from emotional proximity can be related to the notion of distancing, in which healthcare workers create boundaries to protect themselves from getting too involved and to prevent burnout.34–36 This cycle of protection through actions of doing was found to be necessary to this study; however, the literature spoke to such things as meditation, spiritual practices, and specialized training in emotional management as protective factors related to working in palliative care.37–39 Hospice healthcare workers develop personal approaches to managing the demands of doing this work instead of relying on the resources and practices organizations should have in place to support their workers.37–39 There is a need for a shift in policies to better protect healthcare workers’ wellness.
The Transitioning of the Hero Narrative and the Need for Personal Protection
Hospice healthcare workers believe that they must change the hero narrative associated with adolescents with cancer; however, the work of hospice healthcare workers is also rooted in being the hero, just in a different way. The healthcare workers within this study shared their experiences of being called heroes when they were able to carry our grand gestures. The heroic actions of healthcare workers are grand gestures, acts that are morally excellent and go above and beyond.40,41 This need to be the hero was interpreted as a protective factor that hospice healthcare workers used to cope.
To cope with the vulnerability of this work and face the difficulty of supporting this population, hospice healthcare workers placed a protective shell around themselves. Pediatric palliative care healthcare workers address the multiple needs of their patients while trying to protect their own well-being. 42 This protective shell is also manifested as doing and demonstrates coping mechanisms created by hospice healthcare. Vulnerability is often viewed as a weakness, and if healthcare workers are vulnerable, they are at risk of exposing their need for support. 43 Hospice healthcare workers fulfilling wishes prevent the need to focus on being vulnerable, and diverting stressors and overall supports the concept of coping.
Strengths and Limitations of the Study
Globally, this is one of the first studies to explore the experiences of hospice healthcare workers providing care to adolescents and young adults with advanced cancer. A particular strength is the IPA approach that enabled an in-depth understanding of experiences of these hospice workers. As with all IPA studies, this is a homogeneous sample, based on palliative care specialization and location of work, with little variability in ethnicity and gender. Such variation is not a feature of IPA but may require further exploration in subsequent studies. While data for this study were collected in 2018, they remain relevant to contemporary healthcare practice as such lived experiences are a constant in healthcare practice. Given the diversity of Canada, including only English-speaking Healthcare Workers is also a limitation of this study.
Conclusion
Healthcare workers experience conflict between the need to “do for” adolescents and young adults, and the need to protect themselves. A better understanding of the coping mechanisms, and how to support, healthcare workers who provide palliative care to adolescents and young adults needs to be explored. Further research could focus on how best to support workers in their grief and loss, considering issues such as compassion fatigue and burnout.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.