
Abstract
Introduction
Advance care planning (ACP) is an ongoing process for conscious individuals to express their values, goals, and preferences for future medical treatment and care, and discuss these with medical personnel, surrogate decision maker, and their family.1,2 ACP not only assists patients and their families in making healthcare decisions, but it also encourages the use of high-quality treatment and healthcare services.3,4 In addition to reducing unneeded treatments and improving patients’ quality of life in their later years, ACP enables patients’ treatment preferences to be expressed and respected.5,6 ACP may help family members prepare for the death of a loved one, take the stress out of making decisions for them, and reduce negative feelings such as stress, worry, and grief.7,8 When patients lack the ability to make decisions, ACP can raise the probability that healthcare personnel will understand and comply with their patients’ medical care choices, as well as lower the risk of doctor-patient disagreements developing.9,10 For society, ACP can reduce patient hospitalization rates, reduce the waste of medical resources, and promote the development of hospice care. 11 As the Chinese aging society is coming, an increasing number of individuals and families will suffer from illnesses and deaths. However, in the context of the death taboo and family joint decision-making in China, the phenomenon of excessive medical treatment is intensifying with the continuous innovation of medical technology. 12 Patients have few opportunities to express their preferences for terminal treatment. Meanwhile, excessive medical treatment against one's will increases the suffering and loss of dignity in patients, 13 aggravates the doctor–patient conflict, 14 and wastes a certain amount of healthcare resources. 3 Therefore, the new challenge for healthcare professionals is how to help patients ensure the quality of life at the end of life and reduce the incidence of overtreatment, which highlights the need for ACP.
With the development of the ACP global movement and the promotion of nonprofit organizations and professional groups, the concepts related to ACP are gradually gaining popularity. In China, ACP is still in its early stages. In 2013, the Living Will Promotion Association, a nonprofit organization located in Beijing, launched the first public welfare website “Death with Dignity” and a text of “My Five Wishes” to promote ACP in mainland China. 15 ACP has received a lot of attention as an important component of hospice and palliative care since the Chinese National Health Commission published the Practice Guidelines for Hospice Care (Trial) in 2017. 16 It is worth noting that the Medical Treatment Regulations of Shenzhen Special Economic Zone (Revised) were officially passed in June 2022, which clearly states that medical institutions should follow the requirements of patients’ advance directives (ADs). 17 This is the first time that ADs have been incorporated into the legal system in mainland China, indicating ACP has been preliminarily promoted by government. The government then led the development of “Communication guidelines for advanced care planning” as a local standard of Zhuhai. 18 The ACP conversation process is clearly presented in the guidelines, which includes: establishing a communication team, evaluating before communication, conducting communication, dealing unexpected problems during the communication process follow emergency plans, and documenting files. The communication process contains 3 steps: video introduction of ACP, interview of illness experience, and interview of end-of-life treatment intention. As China's ACP is in the primary stage, more research is needed to develop standardized ACP operating mechanisms and processes in the context of Chinese culture.
As 1 crucial member of the ACP conversation in China, physicians usually play roles as important initiators, organizers, and educators of ACP.19,20 There are existing tools to assess physicians’ knowledge, attitude, behavioral intentions, and practice related to ACP in China, but these tools are not comprehensive enough.21–26 Furthermore, the previous research 27 suggested that self-efficacy of ACP participators, rather than their knowledge, is associated with the ACP engagement. Self-efficacy refers to an individual's beliefs in his or her ability to complete a specific task. 28 Physicians’ ACP self-efficacy mainly refers to their self-efficacy in the field of ACP practice, which is a subjective judgment of their competence in ACP practice.29–31 ACP self-efficacy is an essential indicator to predict the participation of physicians in ACP practice and to measure the effectiveness of professional training.29,30
Currently, there has been a tool for measuring ACP self-efficacy among nurses in China. 29 However, this tool may be not suitable for the physician population due to the physicians and nurses have discrepant duties in medical work. In general, physicians dominated in informing patients and making medical decisions, which make them indispensable in ACP conversation. In this study, we aimed to translate the ACP self-efficacy scale (ACP-SE) into Chinese, which was developed by Baughman in 2016, 31 and tested its psychometric features to evaluate the physicians’ ACP self-efficacy level.
Methods
This study was carried out in 2 phases: (1) translation and revision of the ACP-SE; (2) evaluation of the reliability and validity of the ACP self-efficacy scale into Chinese (ACP-SEc).
Sample and Setting
A convenience sampling method was used to select eligible physicians to evaluate the reliability and validity of the ACP-SEc from May to June 2021. The physicians came from 7 tertiary care hospitals in Shanghai, Wuhan, Shenzhen, Guangzhou, and Kunming. Inclusion criteria: (a) having a license to practice medicine; (2) participating in clinical work for more than 1 year; (3) informed consent. According to the requirements of the scale test, the sample size usually needs to be 10 times the number of items. 32 The ACP-SEc contained 17 items, Considering the sample size loss and sampling error, this study planned to expand the sample size by 20%. Therefore, the minimum sample size of this study was 204. To improve the response rate of the questionnaire, we abandoned the online questionnaire. Instead, after obtaining consent from the head of the relevant hospital administration and the head of the department, the department appointed the office nurse in charge to issue and collect the paper questionnaires and mailed to the research group. For the test-retest reliability, we randomly selected physicians who completed the questionnaire in Shanghai to re-fill the questionnaire 2 weeks after the questionnaire was collected. Survey completion was accepted as informed consent.
Ethical Considerations
This research was one of the contents of the project “Construction of Military civilian-trinity house hospice care center,” which is exempt from ethical approval. All participants were informed of the purpose, significance, voluntary and anonymous nature of the study by the homepage of the survey questionnaire. Survey completion was accepted as informed consent. The office nurse kept the completed questionnaire confidential and prohibited other personnel from browsing.
Measurement Instruments
A general information questionnaire, designed by the researchers themselves, including age, gender, ethnicity, marital status, religion, education, professional title, department, years of experience in the specific setting, experience in the medical rescue of relatives and friends, experienced the death of relatives and friends.
ACP-related information questionnaire, designed by the researchers themselves, including knowledge level of ACP (know nothing about it, don’t know much about it, know it, familiar with it, know it very well), palliative care or ACP-related training experience (participated in palliative /hospice care training, participated in ACP training, participated none of them), attitude toward ACP (Support, uncertain/ neutral, against), whether have discussed ACP with patients, whether be willing to initiate ACP discussions with patients, whether have discussed ACP with family and friends, whether be willing to initiate ACP conversations with family and friends.
General Self-Efficacy Scale (GSES), was developed by Schwarzer and Jerusalem 33 and then introduced to China by Zhang. 34 The Chinese version contains 10 items rated on a 4-point Likert scale (1 = Not at all true, 4 = Very true). The higher the score, the higher the self-efficacy level.
ACP-SE Scale, was developed by Baughman for evaluating physicians’ ACP-SE level in 2016. The scale contained 17 items rated on a 5-point Likert scale (1 = Not at all confident, 5 = Very confident) and a single dimension that explained 58.38% of the total variation. The Cronbach's α of the scale was .95. 31 Subsequently, the ACP-SE scale was translated into Spanish for evaluating the ACP self-efficacy level of primary care providers and social workers, containing 19 items, showing the Cronbach's α of .95 and a unidimensional dimension that explained 56.2% of the total variance. 30 Recently, it was translated into Chinese and adapted for evaluating the ACP self-efficacy level of nurses, including 14 items, showing Cronbach's α of .896 and a 3 dimension that explained 61.131% of the total variance. 29 The ACP-SE was considered a specific and brief tool to assess physicians’ ACP self-efficacy level.
Procedures
Phase I: Culture Adaptation and Revision
With the approval of the original author, we followed the adaptation of Brislin's model 35 to translate the ACP-SE into Chinese. Firstly, the scale was translated into Chinese separately by 2 professionals who are proficient in English, respectively. These included an oncologist and an expert in palliative and hospice care. Secondly, members of the research group organized the 2 translators to compare the 2 versions of Chinese with the original scale and negotiated to modify the difference to create a single Chinese version. Thirdly, 2 other bilingual translators who did not know the original scale independently translated the Chinese version of the scale into English. Finally, a second group discussion was held in which all translators agreed on the cultural equivalence between the English and Chinese versions.
To revise and confirm the content validity of the draft of ACP-SEc, 7 experts with a strong research base or extensive experience in the field of palliative care or hospice care were invited, including 2 medical oncologists, 1 head nurse of intensive care unit (ICU), 1 head nurse of general surgery, 1 hospice nurse specialist and 2 clinical nursing professors. 32 All experts met the following criteria: (1) at least 8 years of hospice or palliative care study; (2) at least a bachelor degree; (3) at least an intermediate title; (4) voluntary participants in the study. A 4-point rating scale was used to assess the relevance of each item, ranging from 1 (not relevant) to 4 (very relevant). Apart from the ratings, they were asked to make suggestions on how to rephrase the items if they were deemed unclear or irrelevant.
To ensure that the revised draft of ACP-SEc was comprehensible and properly for the target population, a purposive sample of eleven physicians working in different departments (eg, oncology, cardiology, respiratory, and ICU) was recruited at the Third Affiliated Hospital of the Naval Medical University (a tertiary hospital in Shanghai, China). All participants were asked to select whether the item content and scale descriptions were clear, and they were asked to make suggestions for the unclear parts. If more than 20% of the participants felt that an item on the scale was unclear, the item would be reassessed or revised. 32
Phase II Evaluation of the Reliability and Validity of the Scale
Item Analysis
The critical ratio was used to evaluate the discrimination of the scale's items among different physicians. In this study, the total scores of the ACP-SEc scale of all participants were ranked in order of high and low, with the high group being the top 27% of the total score and the low group being the last 27% of the total score, and an independent sample t-test was performed between the top-low groups. If the CR > 3.00 and P < .05, the item was considered to be well discriminated and was retained, otherwise it was removed. 36
The item-total correlation coefficient was used to test the homogeneity of each item with the scale, if the correlation coefficient < 0.40 or P > .05 between the items and total scores, the items would be removed. 32
After deleting each item, Cronbach's coefficient was calculated to determine the item's quality. We required that Cronbach's coefficient of scale not rise if the item was removed. 37
Validity and Reliability Analysis
The content validity index of the scale and each item were calculated based on the scoring results from experts. The content validity of the scale was good when the content validity index of the item(I-CVI)> 0.78, the universal agreement content validity index of scale (S-CVI/UA) > 0.80, and the average content validity index of scale (S-CVI /Ave) > 0.90. 38
Construct validity was evaluated by using exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). Randomly divided the sample population into Sample Set 1 and Sample Set 2, with Sample Set 1 used for EFA and Sample Set 2 used for CFA. Bartlett's test of sphericity was significant (P < 0.05) and the Kaiser–Meyer–Olkin (KMO) coefficient > 0.60, indicating that sample set 1 was suitable for EFA. The factor composition of the scales and the factor attribution of each item were analyzed by principal component analysis and maximum variance rotation, the number of common factors was determined by eigenvalues > 1.00, and factor loadings of 0.40 were used to determine the factor attribution of each item. If the factor loading of the item < 0.4 or there was cross-loading, the item would be removed. The cumulative explanatory variation of all common factors should exceed 40.0%. 39 On this basis, combined with CFA to explore whether the factor model met theoretical expectations. The maximum likelihood method was used to Sample set 2 data was fitted using a series of model fitting indices to measure the degree of fit of the model. The criteria for fitting indices are as follows: (1) the chi-square degree of freedom (χ2/df) ≤ 3.000; (2) the root mean square of approximation error (RMSEA) ≤ .100; (3) the goodness of fit index (GFI) ≥ 0.800, (4) the tucker lewis index (TLI) ≥ 0.900; (5) the compare fitting indices (CFI) ≥ 0.900. 40 If the theoretical model did not fit well with the observed data, it was necessary to make appropriate modifications to the model.
Criterion validity was evaluated by calculating the Spearman correlation coefficient between the ACP-SEc scale and the GSES.
Known-group validity was evaluated by a nonparametric test comparing the difference of the total scores of known groups on ACP-SEc according to the result of ACP-related information questionnaire.
Cronbach's α coefficient and Guttman split-half reliability coefficient were used to evaluate the internal consistency reliability of the scales. The intraclass correlation coefficient (ICC) was calculated to assess the test–retest reliability. The reliability of the scale was good when Cronbach's α coefficient, Guttman split-half reliability, and ICC were 0.70 or above, respectively.39,41
Statistical Analysis
All the data were examined and organized by 2 individuals. The data were analyzed by SPSS (version 25.0) and AMOS (version 25.0) statistical software. Univariate normality was evaluated for the total score of the ACP-SEc by the Kolmogorov–Smirnov test, and the results showed that it did not conform to the normal distribution. Categorical data were expressed as frequencies and percentages; measurement data are expressed by quartile [P50 (P25, P75)]. P < .05 was statistically significant. Data analysis included descriptions of the participants’ demographic profiles, and physicians’ ACP self-efficacy levels, as well as determinations of item analysis, reliability, and validity of ACP-SEc.
Result
Sample Characteristics
In this study, 408 questionnaires were finally distributed and 348 valid responses were received (response rate: 85.29%). The sample consists of 217 males and 131 females with an average age of (36.01 ± 8.15). Physicians’ ACP-SEc scores ranged from 17 to 85, with a Quartiles score of [65 (51, 69)]. More details were shown in Table 1.
General Information and the ACP-SEc Scores of 348 Physicians.
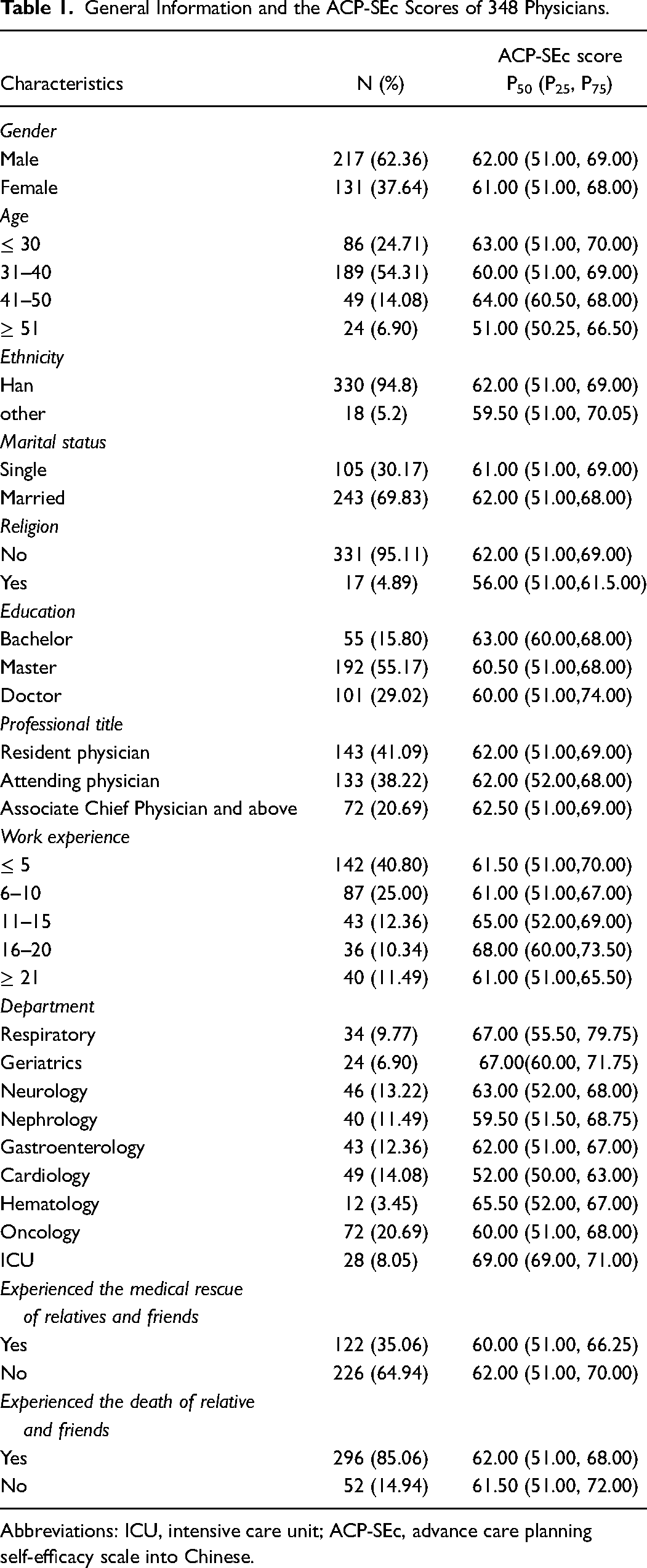
Abbreviations: ICU, intensive care unit; ACP-SEc, advance care planning self-efficacy scale into Chinese.
Scale Translation and Revision
Considering that there was no ACP-related legislation in mainland China, most medical institutions have not implemented ACP and even different departments in the same institution have different degrees of ACP practice, we merged “Ensure that patient's treatment preferences will be honored at your facility” and “Ensure that patient's treatment preferences will be honored at a hospital if a patient is hospitalized” into “Ensure that patient's treatment preferences will be honored at your department.”
According to the current clinical practice in our context, the Chinese tended to measure the family as a hub for joint decision-making had occasionally led to overriding patient autonomy in medical decision-making, we added 1 item to the original scale: Respect patient's wishes when patient and their families have differences of opinions. After a preliminary survey using the revised draft of the ACP-SEc, all 11 physicians reported that each item of the scale was easy to understand and answer. Then the pretest version of ACP-SEc with 17 items was finally developed.
Analysis of the Item
The CR of the items ranged from 12.533 to 23.306(P < .001) and the item-total correlation coefficients ranged from 0.619 to 0.839 (P < .001). After each item was deleted, Cronbach's α of the ACP-SEc ranged from 0.956 to 0.959(<0.960), so all items were retained.
Analysis of the Validity and Reliability
Content Validity
The I-CVIs of ACP-SEc ranged from 0.86 to 1.00. The S-CVI/UA was 0.88 and average scale-level content validity index (S-CVI/Ave) was 0.98, respectively.
Construct Validity
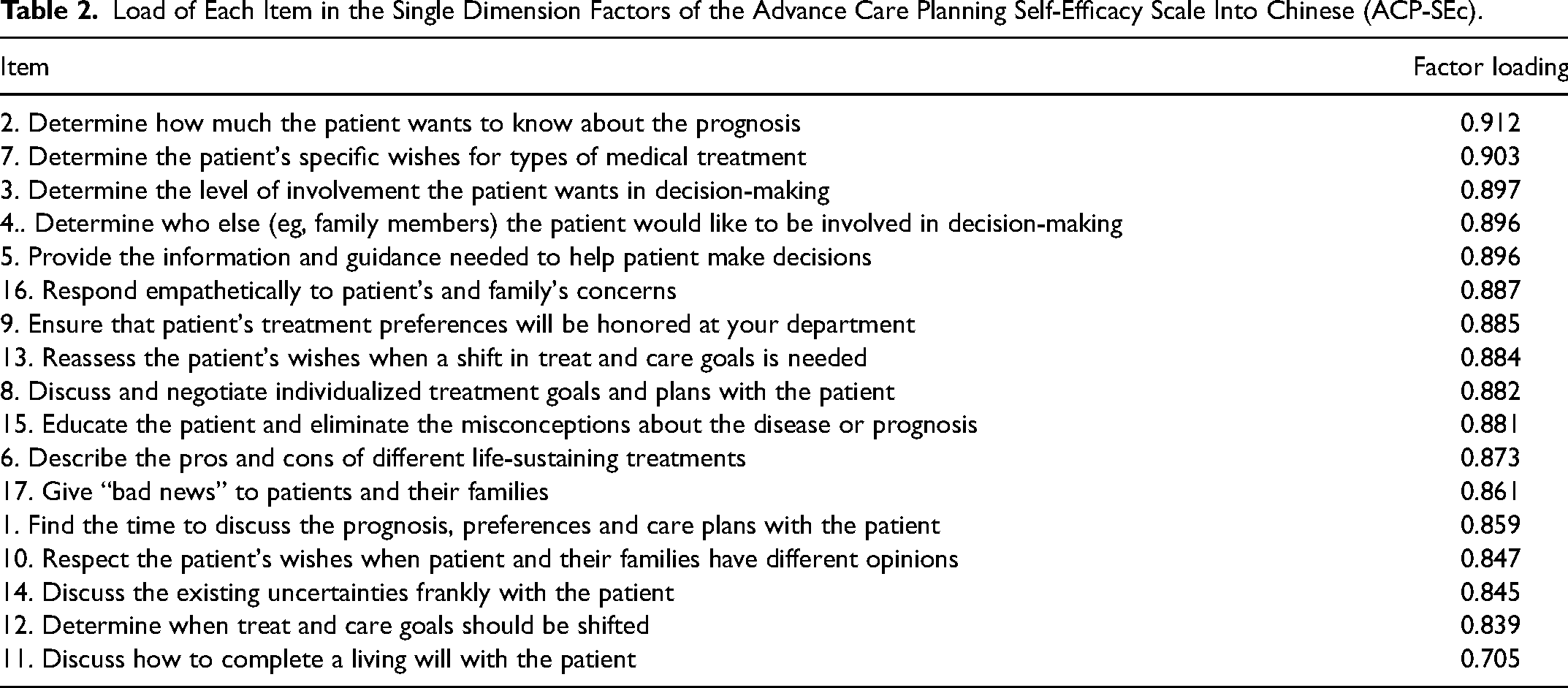
Referring to the standard of EFA with a minimum sample size of 100, 40 148 samples (Sample set 1) were randomly selected from the population for analysis. Factor analysis was determined to fit the data because the KMO value was 0.960, and Bartlett's sphericity test was significant (χ2 = 3202.92, P < .001). After principal component analysis and maximum variance orthogonal rotation, the single factors accounting for 75.507% of the total variance were extracted using the eigenvalue greater than the 1.00 criterion (Figure 1). The load values of each item on the common factor ranged from 0.705 to 0.912 (Table 2). The extracted common factors were consistent with the assumptions of the original scale designer.
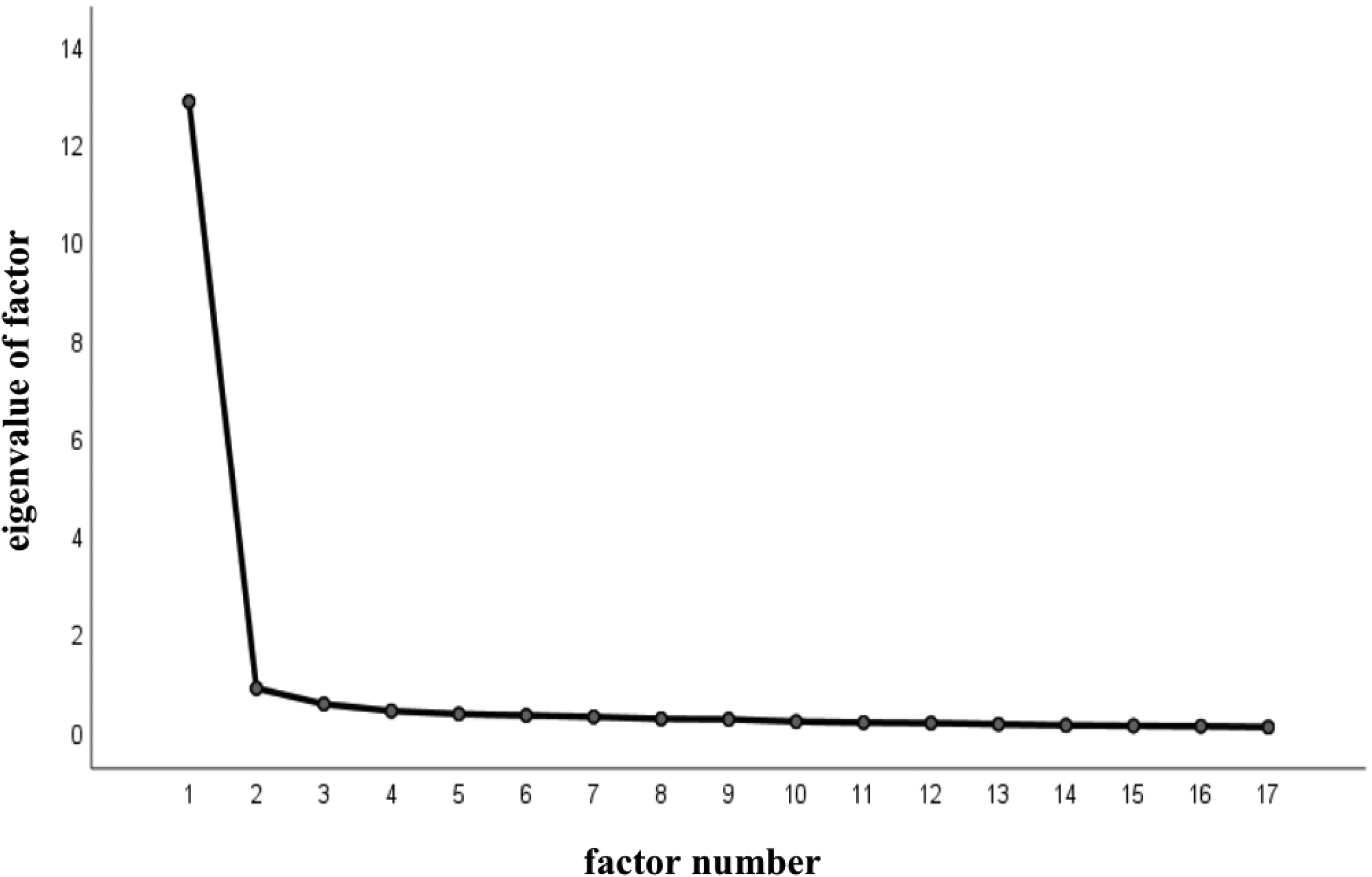
The Scree Plot for advance care planning self-efficacy scale into Chinese (ACP-SEc).
Load of Each Item in the Single Dimension Factors of the Advance Care Planning Self-Efficacy Scale Into Chinese (ACP-SEc).
Referring to the standard of CFA with a minimum sample size of 200, 40 200 samples (Sample set 2) were randomly selected from the population for analysis, performing CFA on the single factor models in EFA. Established an initial model (M1) and use the maximum likelihood method to fit the data. The results showed that the M1 fitting indices were not ideal (Table 3), χ2/df > 3.000、RMSEA > 0.100、GFI < 0.800, TLI < 0.900, CFI < 0.900. Revised the model according to the modification indices, increased the covariance correlation between error variables e12 and e13, e15 and e16, e15 and e17, and establish a modified standardized single-factor structural equation model (M2) (Figure 2). In M2, all fitting indicators are within an acceptable range (Table 3). The standardized regression coefficient (factor loading) ranges from 0.775 to 0.902.
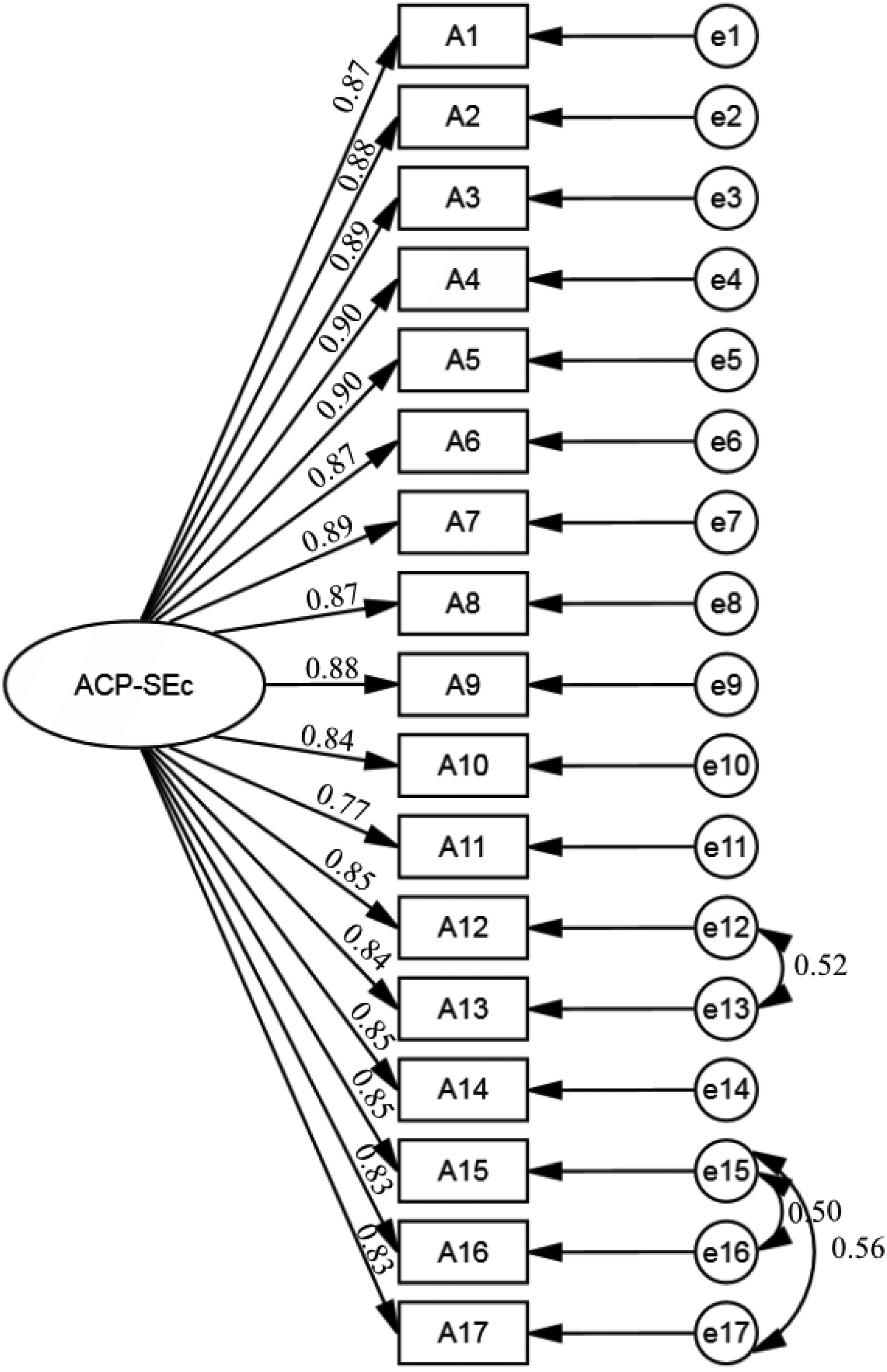
Standardized single-factor model of the advance care planning self-efficacy scale into Chinese (ACP-SEc).
the Fitting Indicators and Reference Standards Before and After the Model Correction of ACP-SEc.
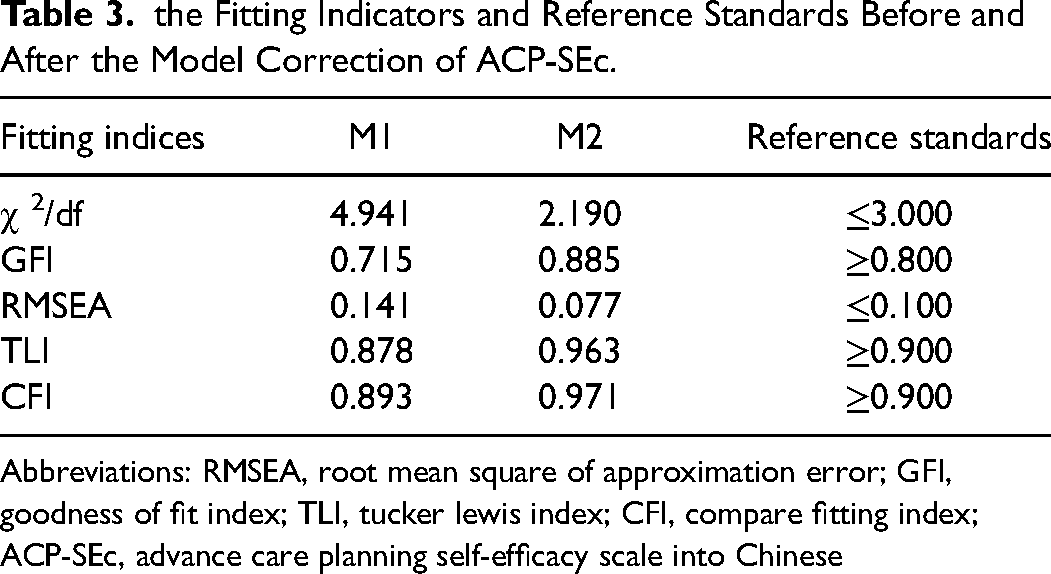
Abbreviations: RMSEA, root mean square of approximation error; GFI, goodness of fit index; TLI, tucker lewis index; CFI, compare fitting index; ACP-SEc, advance care planning self-efficacy scale into Chinese
Criterion Validity
The ACP-SEc was positively and significantly correlated with the GSES (r = 0.675, P<.001).
Known-Group Validity
By comparing the total scores of ACP-SEc between the known groups, the ACP-SEc can distinguish the ACP self-efficacy level between different knowledge levels of ACP, palliative care or ACP-related training experience, attitude toward ACP, whether be willing to initiate ACP discussions with patients, whether have discussed ACP with family and friends, whether be willing to initiate ACP discussions with family and friends (P < .05) ; There was no statistically difference in the total scores of ACP-SEc among physicians on whether have discussed ACP with patients (P > .05) . All are shown in Table 4.
Comparison of ACP-SEc Scores among Known Groups (N = 348).
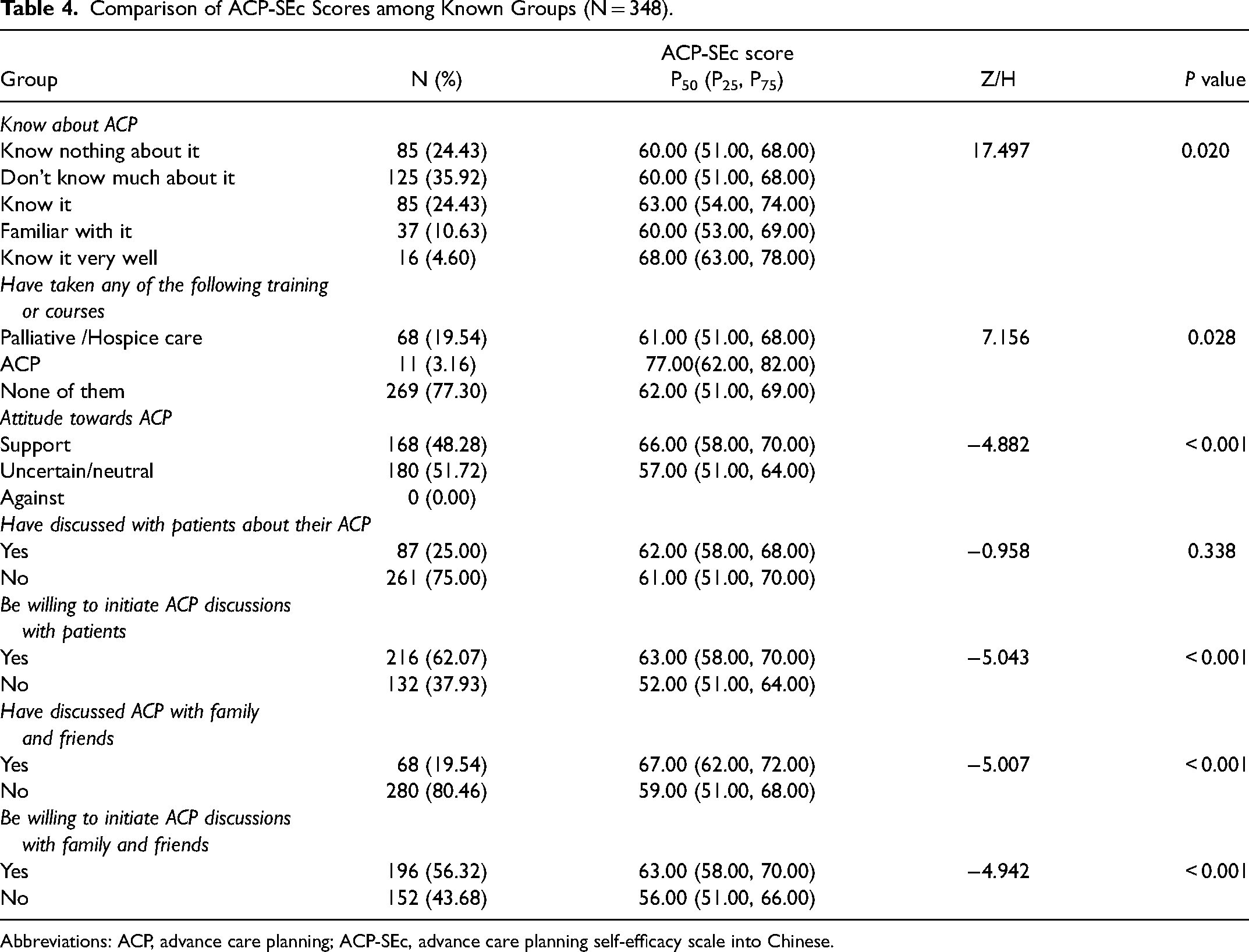
Abbreviations: ACP, advance care planning; ACP-SEc, advance care planning self-efficacy scale into Chinese.
Reliability
The total Cronbach's α coefficient and Guttman split-half reliability coefficient of the scale were .960 and .917, respectively.
A total of 40 physicians were randomly invited to fill out the ACP-SEc again, and 31 valid questionnaires were finally received for test-retest. The ICC for the 2-week test-retest reliability was 0.976 (95% CI:0.951-0.989).
Discussion
Scholars from various countries have demonstrated that ACP-SE can comprehensively, accurately, and quickly assess the ACP self-efficacy level of healthcare professionals. After a rigorous review, revision, and evaluation of the scale, we developed the ACP-SEc with a single dimension and 17 items. Only minor changes were made to improve its clarity and suitability for use in Chinese hospitals. Through testing in clinical physicians, the scale was considered scientific and suitable for Chinese culture.
The Scientificity of the ACP-SEc
In item analysis, the CR of each item met the reference standard, indicating that each item of the scale has good discrimination. The item-total correlation coefficients also met the reference standard, suggesting that each item is closely related to the scale. Cronbach's α coefficient on the scale did not increase when the item was deleted, indicating that 17 items in the ACP-SEc have high homogeneity. Based on the above findings, the items of ACP-SEc have considerable applicability, which is consistent with the Chinese version of ACP-SE for nurse. 29
In the validity analysis, the I-CVI, S-CVI/UA, and S-CVI/Ave of the ACP-SEc all met the reference standard, indicating a good content validity of the scale. The total variation was well explained by the single-factor structure extracted from EFA, consistent with the hypothesis of the original version and the Spanish version.30,31 The expected theoretical model was further confirmed by CFA, and the model fitting indexes were satisfied. The above results strongly suggest an appropriate construct validity of the ACP-SEc. The moderate correlation between the ACP-SEc and the GSES also demonstrated that the scale has suitable criterion validity. The total score of ACP-SEc among physicians significantly varied by knowledge level of ACP, palliative care or ACP-related training experience, attitude toward ACP, willingness to initiate ACP discussions with patients, experience of having discussed ACP with family and friends, and willingness to initiate ACP discussions with family and friends (P < .05), indicating that ACP-SEc shows satisfied known-group validity, which consistent with the original and Spanish version.30,31 In this study, there was no statistical difference in total ACP-SEc scores among physicians regarding whether they had discussed ACP with patients, which contradicted the Spanish version and our expected hypothesis. 30 We hypothesized the reason is most physicians encountered obstacles in ACP conversations and lacked sufficient successful experience, lowering physicians’ ACP self-efficacy.
In reliability analysis, Cronbach's α coefficient of ACP-SEc in the study sample demonstrated good internal consistency. The result also match those of the original and Spanish versions, which both reported a Cronbach's α of .95.30,31 The original version 31 did not report test-retest reliability, but the Spanish version did, with an ICC of 0.88 (95% CI: 0.83-0.91). 30 Compared to the Spanish version, the higher test-retest reliability of the Chinese version could be attributed to the shorter test–retest reliability interval time (14 days vs 37 days), and the smaller sample size (31 vs 157).
the Chinese Cultural Adaptation of the ACP-SEc
Under the traditional concept of emphasizing life and avoiding death in China, a general notion is that life is the way to realize self-worth and social value, while death is the negation and termination of life.42,43 People are less willing to discuss death, especially before they die. ACP can be utilized as a death education tool to help the Chinese talk about death in a more tranquil and mild manner. 44 In contrast to the Western emphasis on individual rights and liberties, Chinese people are tightly tied in the form of family.45,46 When suffering from serious diseases, the Chinese people may respond differently from the Western people in medical decision-making and bad news disclosure.47–49 To alleviate the potential impact on patients, physicians prefer to inform the family members with the disease condition rather than the patients themselves.50,51 Likewise, some families may choose to conceal bad news from the patient. However, it not only interferes with patients’ rights to know the truth, but also limits patients’ participation in medical decision-making. 52 In addition, most patients rely on their children or spouses to make medical decisions on their behalf, making family decision-making rights prior to patients’ rights.46,53 As a result, some medical decisions may conflict with patients’ values and preferences. Under such traditional family culture and default social rules, Chinese physicians face some unique challenges in promoting and applying ACP.54–56 To some extent, the development of ACP may alleviate the negative impact of traditional Chinese family culture in the medical field.
To adapt to China's clinical practice in medical decision-making, we added the item “Respect the patient's wishes when patients and their families have different opinions”. We believe that the ACP-SEc is in accordance with the Chinese culture and the public expectations for future medical decisions.
The Application Prospects of ACP-SEc
Patients prefer physician-initiated ACP conversations in China. 54 Physicians are responsible for bridging the gap between family members and patients, enabling patients to know more about their true condition, assisting patients in expressing their wishes and preferences, making decisions for medical planning, and helping family members to find a balance between respecting the patient's autonomy and not harming the patient.55,57 Physicians with a low ACP self-efficacy may be reluctant to lead or participate in ACP conversations with patients and their family members, or to expend effort in developing ACP skills and addressing barriers to ACP conversations. 29 Therefore, it is particularly important to cultivate the confidence of physicians in ACP by developing culturally and realistically appropriate ACP training programs in China.20,58
The ACP-SEc with good reliability and validity can be an effective tool for assessing ACP-SE among physicians. This tool not only provides a foundation for the development of ACP training programs for physicians but also assesses the effectiveness of ACP training programs. Based on the scale scores, we can select physicians with higher self-efficacy to participate in ACP training and clinical practice.
Limitation
Considering the differences between the West and China in terms of economy, culture, social security, legislation, and healthcare system, further verification is required, particularly whether the cultural characteristics reflected by ACP-SEc are highly compatible with the cultural characteristics of the mainland. Besides, all study participants were from tertiary hospitals in 5 Chinese cities, and the applicability of ACP-SEc among physicians in primary medical institutions needs to be investigated.
Conclusions
The ACP-SE scale developed by Baughman was translated and cross-culturally adapted into Chinese. It provides a fundamental study for evaluating ACP self-efficacy in Chinese physicians. The content validity, construct validity, criterion validity, internal consistency, and test–retest reliability of the ACP-SEc were all satisfied. In addition, the scale not only provides a practicable tool to conduct comparative analysis with other similar work in different countries but also assists us to improve physicians’ ACP self-efficacy in our country.
Footnotes
Availability of Data and Materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Construction of Military Civilian-Trinity House Hospice Care Center (2020-jdyxzdfcxk-01).
Ethical Approval
This research was one of the contents of the project “Construction of Military civilian-trinity house hospice care center”, which is exempt from ethical approval. All participants were informed of the purpose, significance, voluntary and anonymous nature of the study by the homepage of the survey questionnaire. Survey completion was accepted as informed consent. The office nurse kept the completed questionnaire confidential and prohibited other personnel from browsing.
Informed Consent
Survey completion was accepted as informed consent.