
Abstract
Introduction
Safe and high-quality health care involves respecting people's wishes and choices about their health and clinical care during their illness trajectory and at the end of their life. 1 A lack of awareness of a person's wishes for their end-of-life care (EOLC) may result in unnecessary or nonbeneficial treatment, loss of dignity and autonomy of the person during a vulnerable time, and additional distress for the patient, their family members and health professionals. 2 To facilitate safe and high-quality EOLC in health services, the Australian National Consensus statement on safe and high-quality EOLC (Consensus Statement) outlines 10 recommendations encompassing processes of care and organizational prerequisites (Table 1).
10 Recommendations of the Consensus Statement for EOLC.
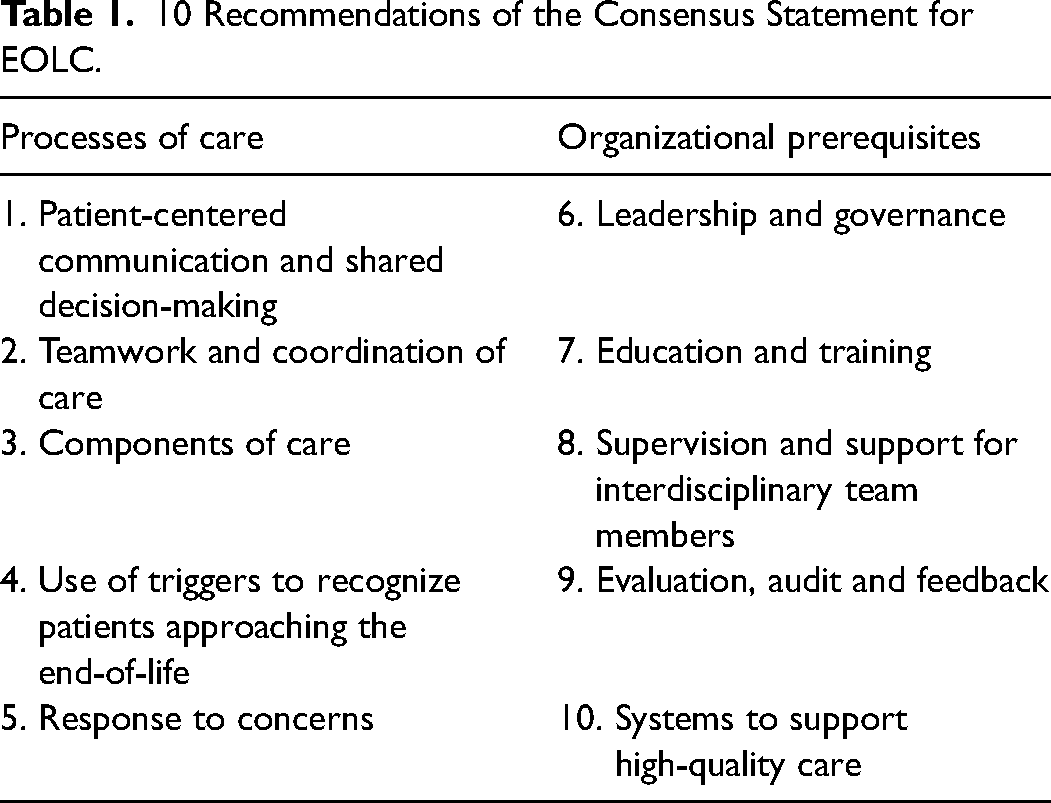
The process of clinical care requires that conversations about EOLC are adequately documented when life limiting conditions are diagnosed, so that when needed in urgent situations, the information is readily available to act in a manner that respects the wishes and care preferences of the unwell patient. 2
Cancer diagnoses commonly have a distinct trajectory of a functional decline and more predictable prognostication compared to noncancer diagnoses.3,4 Therefore, cancer diagnoses, ideally well before the advanced stages, may be an opportune time to engage in optimal and supportive EOLC discussions. Furthermore, cancer is a leading cause of death in Australia: cancer was the cause of approximately 49 000 deaths in 2021, an average of 135 deaths every day. 5 It is estimated that 151 000 people will have a new cancer diagnosis every year and one in two Australians will be diagnosed with cancer by the age of 85 years. 5 Additionally, an increasing number of people with cancer live with multiple chronic conditions, or multimorbidity, which can contribute to intensive and unnecessary hospital care at the end of life. 6
Hospital clinicians are expected to proactively engage in EOLC discussions with people who have been diagnosed with cancer and whose prognosis is limited to less than one year to increase the likelihood of delivering high-quality EOLC aligned with the patient's values and preferences. 2 However, mainstream assumptions about death and dying, and health care professionals’ familiarity with patients and their families as decision-makers may be misaligned in some cultures, increasing the risk of deviating from person-centered care.7,8 Additionally, discussions about EOLC between patients, their family members and health professionals may not occur9,10 or, if they do, they are often poorly documented or undocumented. 11 Inadequate documentation of EOLC wishes can have negative consequences on the quality of care, especially if a person becomes unable to make or communicate their care preferences or appoint a decision-maker due to a lack of opportunity, illness progression or treatment side-effects. The underlying assumption is that if EOLC discussions are not documented in patients’ medical records, the information is not available to all clinicians, and patient's wishes and preferences for EOLC may not be delivered. Therefore, medical records that provide easy access to documented EOLC preferences are essential for optimal EOLC.
Following recommendations from the Consensus Statement, hospitals across the country have developed their own standards to guide the delivery of EOLC. The extent to which these standards are followed has not been formally established. Assessing which EOLC standards are documented in patients’ medical records can help identify areas that are performed well and areas where improvements are needed, with the notion that adequately documented care is conducive to higher quality of care. 12 This study therefore aimed to describe EOLC documentation as per hospital standards among cancer decedents. A secondary analysis explored differences between EOLC documentation by hospital settings, namely specialist palliative care unit, sub-acute/rehabilitation care settings, acute care wards and intensive care units.
Methods
Design
A retrospective cross-sectional study design was used to collect data from patients with a cancer diagnosis who died during an inpatient stay between 1 Jan 2019 and 31 Dec 2019.
Setting
The study was conducted in six hospitals from one of Australia's largest metropolitan public health services. Services available across these hospitals included tertiary acute care, metropolitan and regional secondary services, geriatric medicine, and rehabilitation services. Specialist palliative care services were offered via a hospital-based palliative care consultation team and a specialist palliative care inpatient unit. The hospital-based palliative care consultation team consisted of nursing and medical staff. Referrals to spiritual care, an allied health team, and psychology services on the wards were made on a need-basis. The specialist palliative care inpatient unit included nursing and medical staff, social work, physiotherapy, occupational therapy, spiritual care, and psychology services as well as volunteers and pet therapy.
The key organizational standards supporting EOLC at the participating hospitals included advance care planning, resuscitation planning, goals of care, care of the dying person, and grief and bereavement care. Appendix 1 provides a definition for each of these guidelines, except for the Goals of Care guideline as it was not implemented in 2019. This aspect of EOLC was therefore not formally included in our study.
Advance Care Plans (ACPs) can be documented in patients’ medical records and/or in an advance care directive (ACD). Advance care planning supports person-centered care and shared decision-making by providing a mechanism for patients to discuss their wishes, values, and beliefs regarding their current and anticipated future health status including EOLC. 2 Documenting patients’ EOLC wishes in an ACP can improve the outcomes of patients at the end of life. 13 Resuscitation planning involves the completion of a form on admission which describes the appropriate ceiling of resuscitation. This form is often changed during the course of the admission according to changes in the patient's condition and is used to guide care in case of clinical deterioration. The absence of documented resuscitation planning may affect appropriate end-of-life care and expose the patient to potentially unnecessary interventions that are highly likely to increase the patient's suffering.14,15 Care of the Dying Person (CPDP) requires clinicians to recognize and diagnose imminent dying (the patient is likely to die within hours to days) and communicate this to the patient and their family to actively support them in this phase of the illness. 16 The CPDP prompts appropriate management of the dying person and documents care in the one place. Grief and bereavement care recommends access to psychosocial spiritual and cultural support to empower patients and their families as they grieve before and after death. 17
These four standards are supported by key clinical practice guidelines and several indicators pertaining to EOLC provision should be documented in patients’ medical records. A list of the corresponding practice guidelines and EOLC indicators is provided in Appendix 1.
The EOLC supporting standards were integrated into clinical practices through organizational education and training packages for hospital staff, coordination of care through effective teamwork, and ongoing organization monitoring and improvement strategies.
Sample
A list of patients with a cancer diagnosis (active or in remission) who died during an inpatient stay at one of the six hospitals during the study period was provided by the health service data management team. Patients were excluded if they were <18 years and/or had an unconfirmed cancer diagnosis. Data were collected until trends in EOLC documentation became apparent, whereby EOLC indicators were consistently or rarely documented.
Data Collection
An electronic data collection tool was created in the REDCap™ for the purpose of this study. The development of the tool was informed via the four organizational standards and panel discussions with clinicians and researchers. The panel was composed of three clinician researchers experienced in emergency, general medical and palliative care, two researchers experienced in patient experience and supportive care, and one consumer representative.
The data collection tool was pilot tested by two members of the research team who independently collected data from four medical records. Data was compared to ensure interrater reliability. Minor changes were made to the tool prior to the commencement of the data collection phase. All study data were collected by one member of the research team (RH).
The data were de-identified and coded electronically at the time of collection. The following information was collected for each patient: patient characteristics (age, sex, date of death, country of birth, language spoken at home, interpreter requirement, marital status, religious belief/affiliation, and living arrangement), clinical characteristics (type of cancer, disease stage, other comorbidities), care characteristics of the final admission (length of stay, site of admission and type of care received), and the presence or absence of EOLC indicators. Evidence of referral to specialist palliative care and indicators of palliative care interventions such as symptom and pain management, and psychosocial and spiritual support (including family care) was collected, as well as preferences and values regarding the place and nature of care from the patient's final admission records. Patient clinical files, electronic medical records, and progress notes from the patient's final admission were inspected to collect evidence of EOLC provision.
Data Analysis
The data were exported from the REDCap™ to the MS Excel for cleaning and consistency checks and analyzed using the SPSS version 26. Descriptive statistics including frequencies and percentages were used to summarize the study data. Associations between EOLC documentation and hospital settings, ie, specialist palliative care units, sub-acute/rehabilitation care settings, acute care wards and intensive care units, were explored using chi-square test or Fisher's exact test as appropriate. Sub-acute/rehabilitation care settings, acute care wards and intensive care units were combined into one variable (“nonpalliative care”) to assess the difference between EOLC documentation in specialist palliative care units and all other settings. Post hoc chi-square tests further explored associations between referral to the hospital-based Palliative Care Consultation Team (HPCCT) and EOLC documentation in nonpalliative care settings.
Ethical Considerations
Ethics approval and a waiver of consent were granted by the relevant institutional Human Research Ethics Committees (Eastern Health LR20/047 and Deakin University 2021-321). We used the STROBE cohort checklist to guide our reporting. 18
Results
A collection of 562 medical records was identified by the hospital data management team. Following data collection of 254 medical records (45.2%), a trend in hospital setting specific EOLC documentation became apparent, indicating data saturation. Of the 254 records, 14 (5.5%) were excluded because cancer diagnosis was not confirmed, leading to a final sample size of 240 medical records included in the analysis. The distribution of the 240 patients across all six hospitals was proportionate to the patient distribution in the full (562) dataset.
The mean age of our study population was 75.3 years (SD 11.8) ranging between 29 and 105 years. Approximately half of the patients (n = 125; 52%) were female. Most were born in an Anglo-Saxon country (n = 180; 74.5%), spoke English at home (n = 220; 91.6%), lived with other adults or carers (n = 177; 73.7%) and were affiliated to a religion (n = 142; 59.9%) (Table 2).
Patient Characteristics (n = 240).
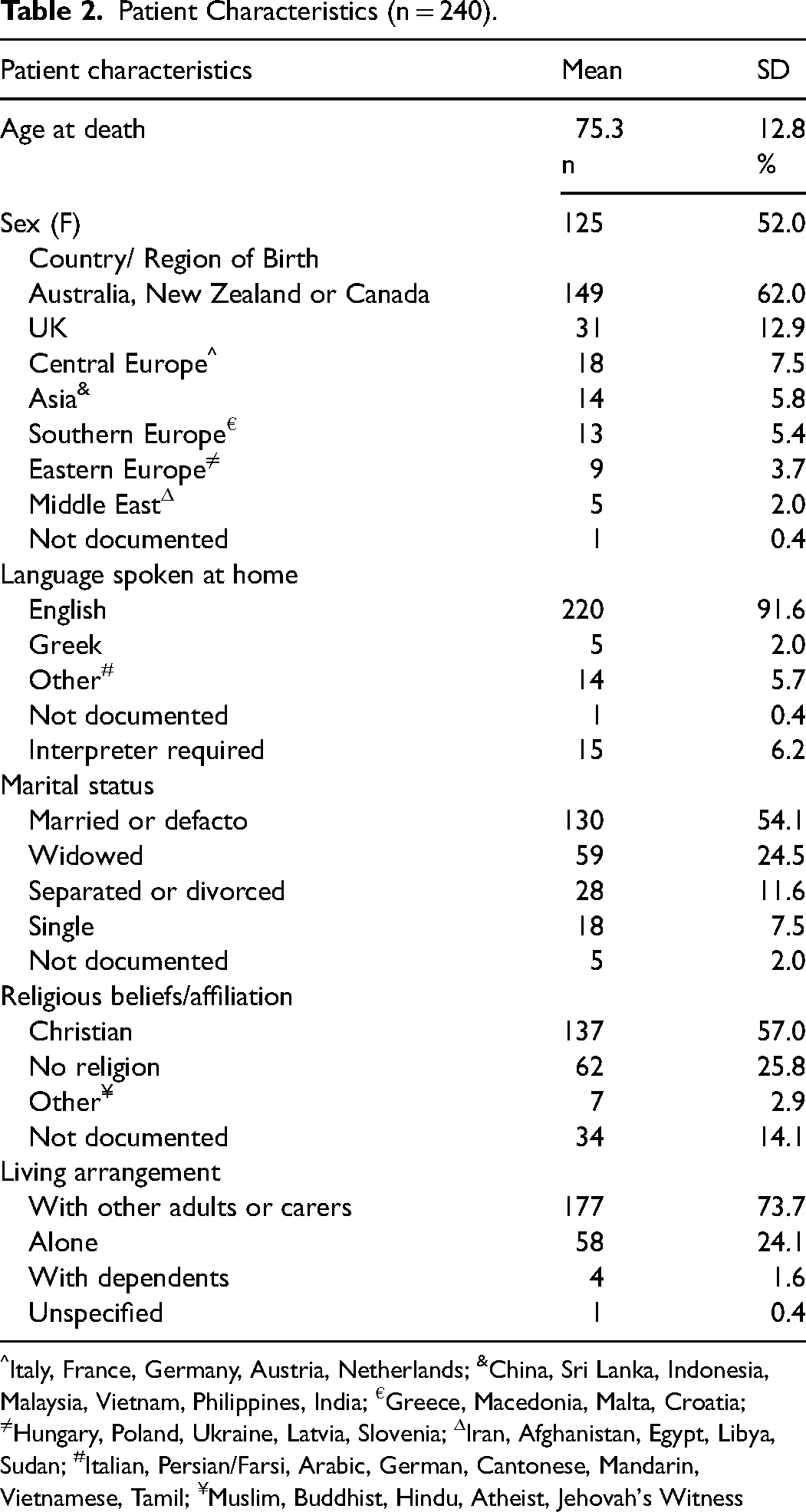
Italy, France, Germany, Austria, Netherlands; &China, Sri Lanka, Indonesia, Malaysia, Vietnam, Philippines, India; €Greece, Macedonia, Malta, Croatia; ≠Hungary, Poland, Ukraine, Latvia, Slovenia; ΔIran, Afghanistan, Egypt, Libya, Sudan; #Italian, Persian/Farsi, Arabic, German, Cantonese, Mandarin, Vietnamese, Tamil; ¥Muslim, Buddhist, Hindu, Atheist, Jehovah's Witness
Clinical characteristics of the patient cohort are shown in Table 3. The most frequent cancers were those affecting the gastrointestinal system (n = 60; 25%), followed by lung cancer (n = 54; 22.5%) and breast cancer (n = 24; 10%). Of those diagnosed with comorbidities (n = 210; 87.5%), the majority had at least 2 comorbidities (n = 192; 81.7%), with cardiovascular diseases present in nearly a half of the patients (n = 101; 48.0%).
Patient Clinical Characteristics.
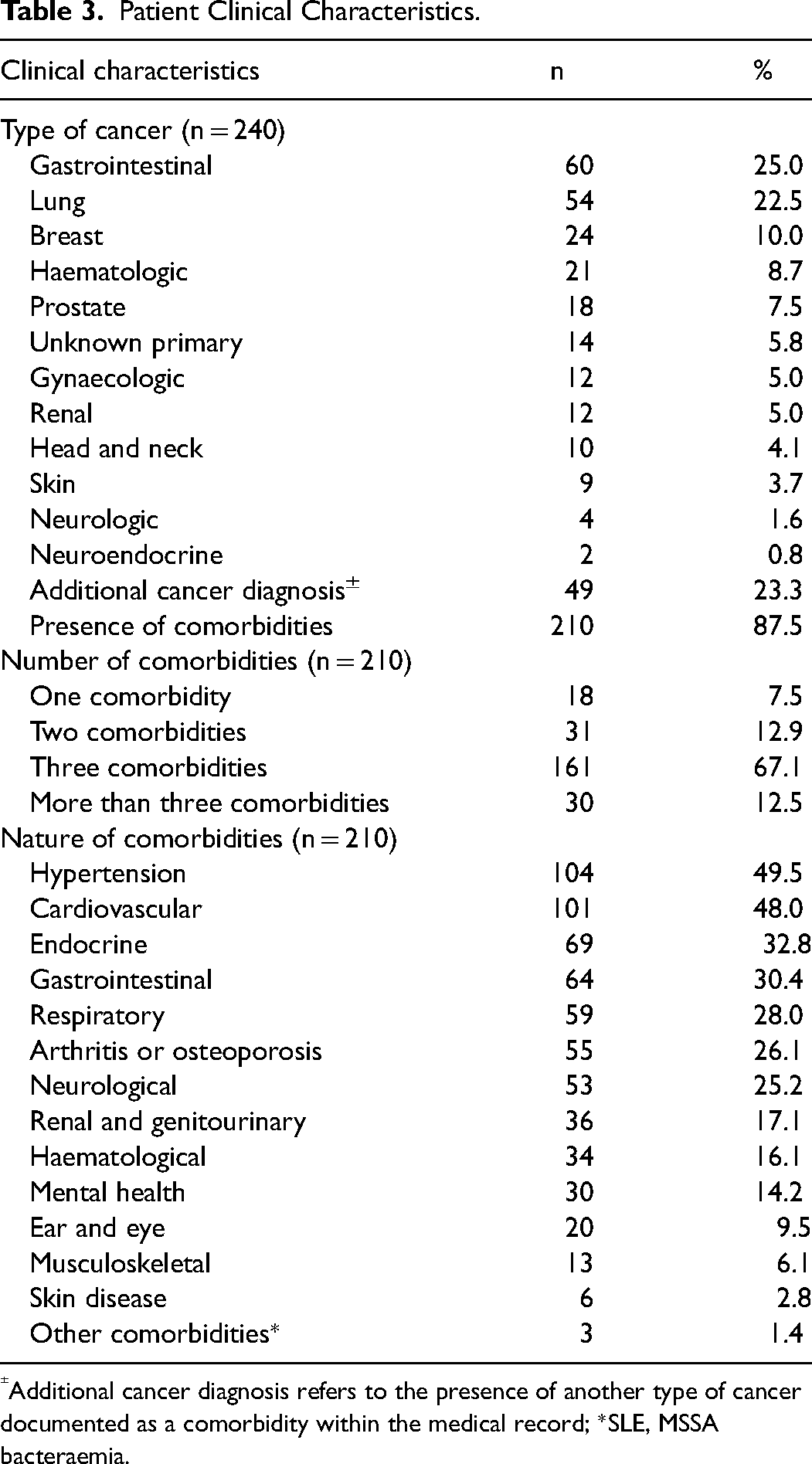
Additional cancer diagnosis refers to the presence of another type of cancer documented as a comorbidity within the medical record; *SLE, MSSA bacteraemia.
The mean length of stay of the final hospital admission was 15.86 days (SD = 8.6). Nearly a half of the patients died in the palliative care unit or acute care settings (n = 114; 47.5% and n = 113; 47%, respectively) (Table 4).
Care Characteristics at Final Admission (n = 240).
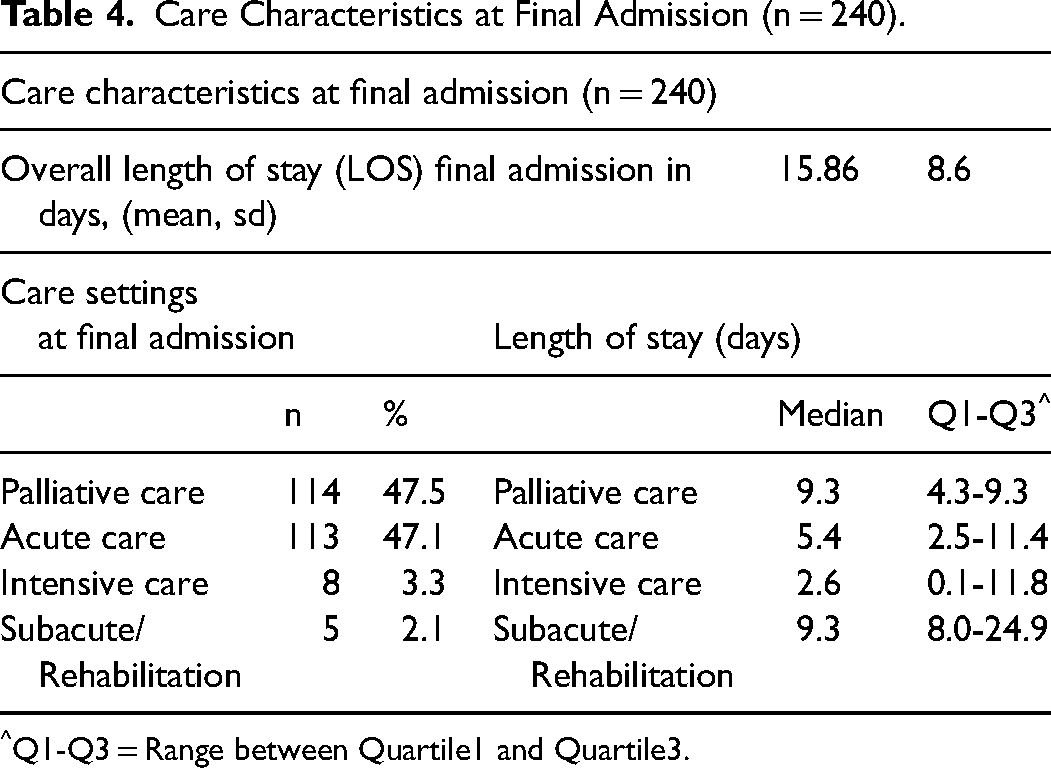
Q1-Q3 = Range between Quartile1 and Quartile3.
Documentation of EOLC
Advance care planning was formally documented for 73 (30.4%) patients, evidenced by the presence of an advance care directive in 9 (3.8%) patient records, a substitute decision maker for 45 (18.8%) patients, and both indicators for 19 patients (7.9%). Discussions about aspects of patient values, instructions, or treatment preferences during their final admission were documented in the progress notes for all patients (n = 240; 100%).
Resuscitation planning was documented in all (100%) patient records, mainly through completed ‘consensus resuscitation plans’ (n = 231; 96.2%). Medical Emergency Team (MET) calls were documented for 42 patients (17.5%) during their final admission and modifications to MET call criteria were made at least 72 h before death for 52 patients (21.6%). Of 52 patients with MET modifications recorded, three (5.8%) had specific MET call criteria modified, and the remaining 49 patients (94.2%) had MET modification directions to cease physiological observations or had been documented as not for MET calls or MET calls for distress only. Risk factors for deterioration or dying were documented in 240 (100%) patient records.
Indicators of Care for the Dying Person were document in 235 (97.6%) patient records. While a CPDP was present in 102 (42.5%) patient records, it was not often completed throughout all sections by all disciplines required.
Grief and bereavement care was documented in 96 (40%) patient records. Table 5 provides further details on the type of EOLC documentation.
Type of EOLC Documentation (n = 240).
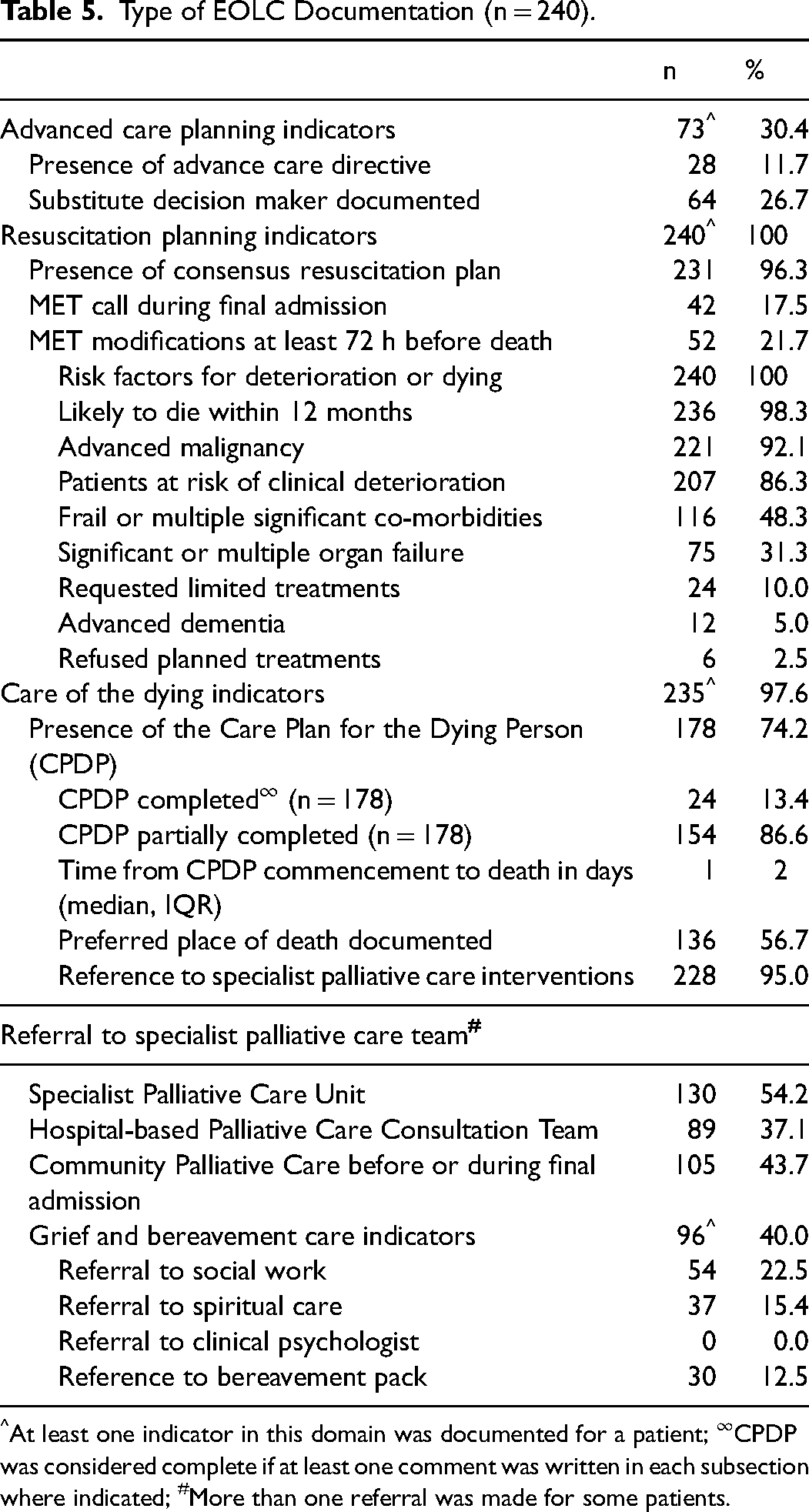
At least one indicator in this domain was documented for a patient; ∞CPDP was considered complete if at least one comment was written in each subsection where indicated; #More than one referral was made for some patients.
Documentation of End-of-Life Care by Patient Characteristics
Patients living with other adults or carers were less likely to have a documented ACP than those living alone or with dependents (OR 0.48; 95% CI 0.26-0.89). Other patients’ characteristics such as sex, marital status, country of birth, religious affiliation, and number of co-morbidities were not associated with the way EOLC was documented.
Patients who died in palliative care settings were more likely to have a referral documented to the hospital-based Palliative Care Consultation Team than those who died in other settings (61.8% vs 38.2%; P < .001).
Documentation of End-of-Life Care by Care Setting
EOLC documentation was more frequently observed in palliative and sub-acute/rehabilitation care settings than that in acute care wards and intensive care units (Figure 1).
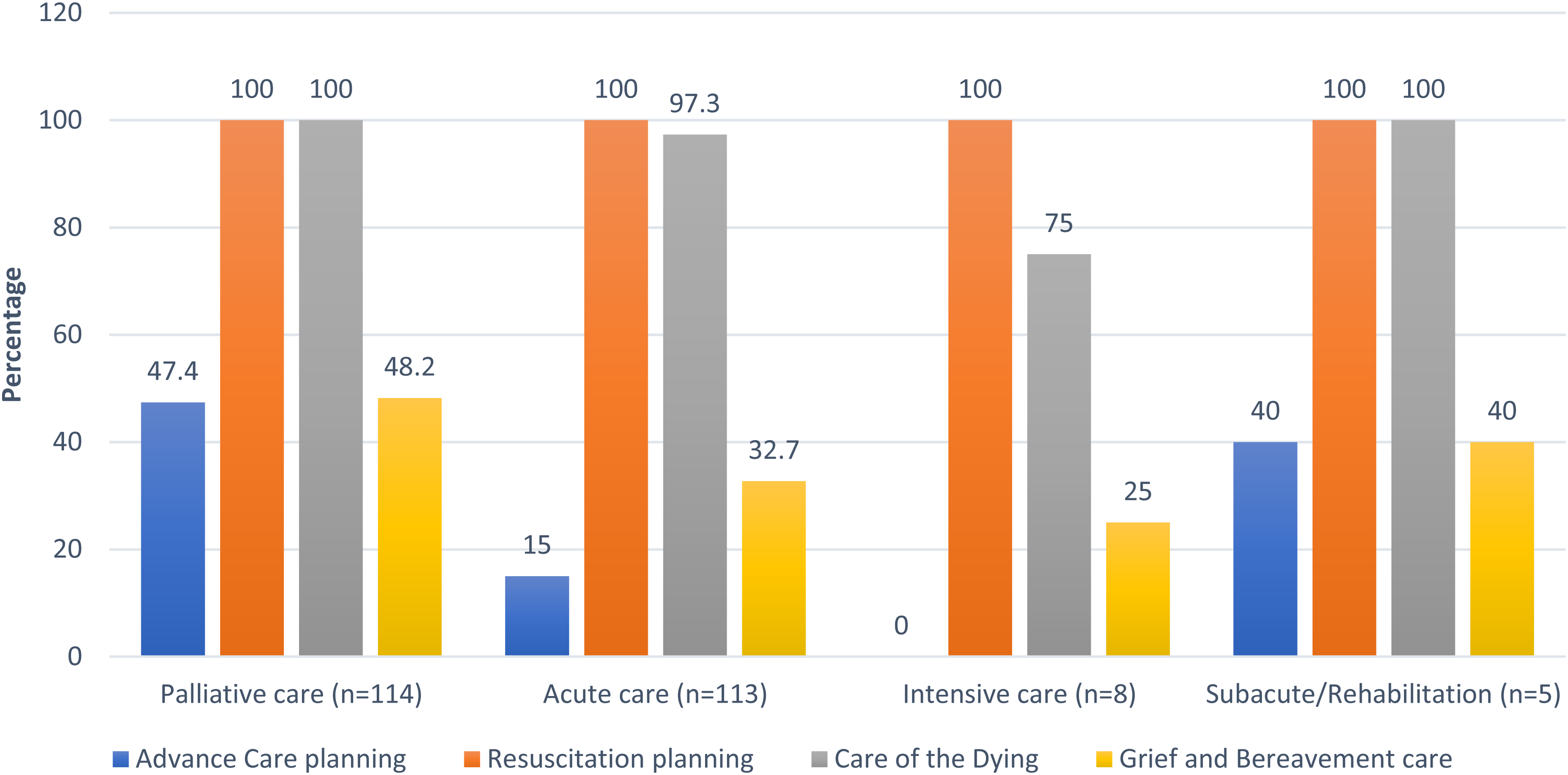
Distribution of EOLC documentation across hospital settings.
Documentation of EOLC relating to advance care planning, care of the dying person, and grief and bereavement care was significantly greater in palliative care settings than that in other hospital settings (P < .001, P = .032 and P = .013, respectively) (Table 6).
EOLC Documentation in Palliative Care and non-Palliative Care Settings.
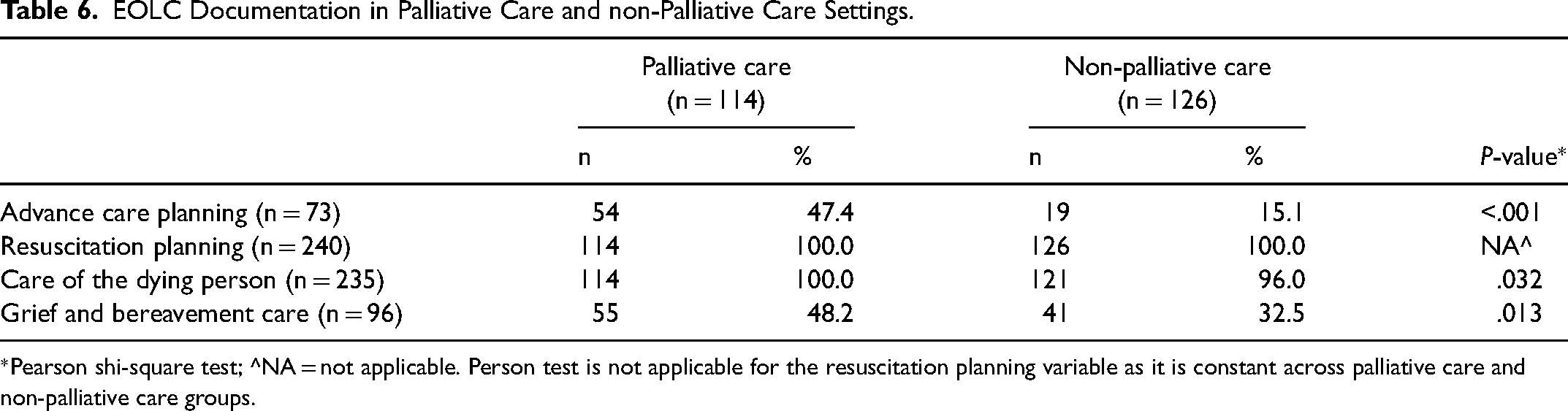
*Pearson shi-square test; ^NA = not applicable. Person test is not applicable for the resuscitation planning variable as it is constant across palliative care and non-palliative care groups.
The post hoc analysis showed no significant association between referral to the hospital-based Palliative Care Consultation Team in nonpalliative care settings and EOLC documentation (Table 7).
Association between Hospital-based Palliative Care Consult Team and EOLC Documentation in non-Palliative Care Settings.
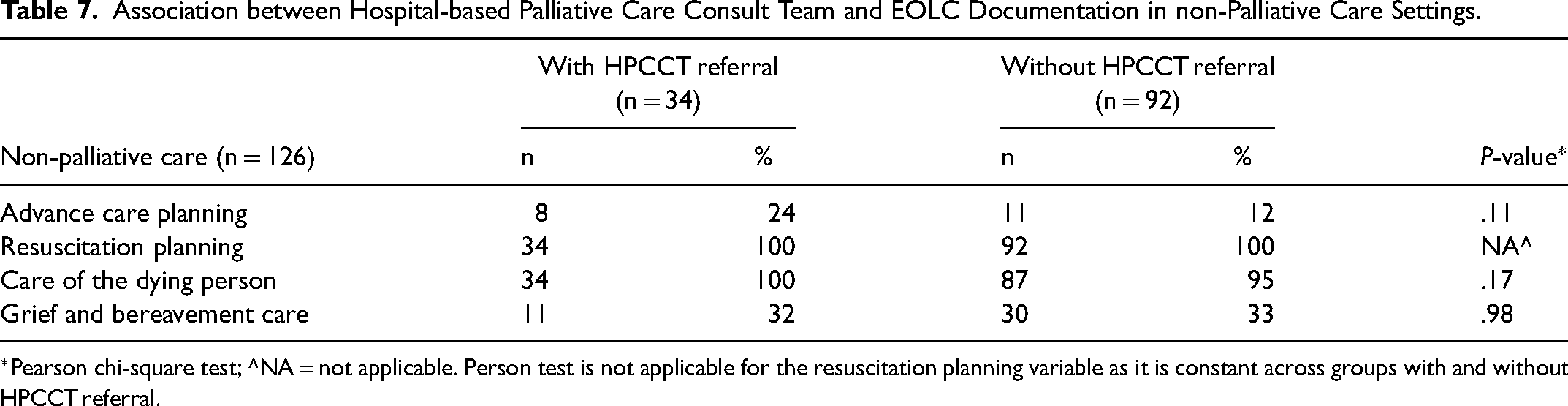
*Pearson chi-square test; ^NA = not applicable. Person test is not applicable for the resuscitation planning variable as it is constant across groups with and without HPCCT referral.
Discussion
This retrospective study of 240 cancer decedents found that a half of the study population was receiving care on acute wards or in the intensive care unit at the time of death. Care needs for the dying person were reported in nearly all patients and documentation of the care plan for the dying person was initiated for most patients within 48 h of their death. Specialist palliative care interventions were referenced in 95% of patients’ medical records, but less than a half had grief and bereavement care documented. An even lower number had an ACP documented. EOLC documentation was significantly greater in the specialist palliative care unit settings than that in other hospital settings.
While an ACP was more likely to be documented in palliative care settings than that in other hospital settings, it occurred for less than a half of the patients. Our findings correlate with previous research conducted in Australian acute care settings, where the presence of an ACP was documented in 12% of patients before admission. 19 Despite the national guidance, the prevalence of ACP remains low in acute care settings. 20 Some have questioned the practicality of completing and maintaining an ACP, 21 especially in acute settings when patients are actively dying. It is worth highlighting that advance care planning is a voluntary process that should start before admission to acute care when a person is in stable health, and can reflect on and communicate their healthcare preferences. A study of over 15 000 cancer decedents diagnosed with multimorbidity found that patients who had an ACP documented at least 30 days before their death were less likely to receive high-quality EOLC. 6 It is possible that conversations about advance care planning have taken place outside hospital settings between patients and family members or carers. The presence or absence of a formal ACP may not be an appropriate indicator of patient centered EOLC, but does provide a clear and accessible documentation of the person's wishes, values, and treatment preferences at a point in time. There needs to be a process that regularly triggers the review of a formal ACP to ensure that it aligns with the patient's progress notes. Consolidating progress notes with ACDs will require continued organizational endorsement of clear practice frameworks and staff training as demonstrated in the standardization of resuscitation planning over the past six decades. 22
In contrast to ACP, resuscitation planning and CPDP were well documented in our study cohort. Resuscitation planning and CPDP are medically oriented processes; the former was completed on patient admission to manage clinical deterioration 23 and the latter was started for all dying patients. 16 Both processes may be more aligned with the existing clinical practices, and therefore more amenable to apply in hospital settings than current ACP guidelines.
Grief and bereavement care was documented for less than a half of the patients in our study. It is possible that informal discussions related to bereavement care occurred but were not documented. However, barriers to bereavement support may include resource limitations, 24 clinicians’ perceived lack of time and organizational support, insufficient training, or clinicians appraising bereavement care as beyond their role. 25 With increased funding constraints across the healthcare sector, the question of whose role it is to provide this support in hospital setting remains unanswered. Current gaps in the mental health care provision in the Australian health system 26 may also account for the absence of referrals to clinical psychologists in our study, and potentially a lack of skilled psychologists in EOLC.27,28 Because of gaps in funding and skilled staff, some hospitals offer mental health support on an ad hoc basis to ensure a sustainable and cost-effective service.29,30
Our post hoc analysis did not show a statistically significant association between the HPCCT and EOLC documentation in nonpalliative care settings. Patients with cancer tend to have higher referral rates to palliative care services compared to noncancer patients. 31 A Canadian study of more than 145 000 people who died of cancer and noncancer illnesses found that palliative care was more likely to be initiated earlier, in the hospital setting, and delivered across multiple care settings in patients with cancer than in those with terminal noncancer illnesses. 32 These findings suggest that medical oncology may be more familiar with the EOLC process and documentation than other specialties.
It is worth highlighting that understanding of the process of EOLC provision in this study is limited to what is documented. While medical records are legal documents which require all relevant care to be documented, the presence or absence of EOLC documentation does not necessarily imply quality or appropriateness of care. Furthermore, data collection in our study was limited to the final admission and may have missed documentation of ACP or grief and bereavement support in previous admissions. For bereavement support, for example, patients and their families may access external support through their own faith or religious practice or other spiritual care where hospital referral would not be required. Another limitation of this study is that grief and bereavement indicators could not be separated into anticipatory and postmortem grief and bereavement care. Additionally, our findings may not be generalizable to noncancer cohorts.
Conclusion
Our study found that the process of dying was well documented among inpatients with a cancer diagnosis. While ACP documentation was low, evidence of related discussions was present in all patient records, indicating a high frequency of EOLC discussions. Consolidation of these discussions with EOLC documentation and embedding grief and bereavement support documentation in a clear practice framework will greatly improve the quality of EOLC documentation in hospital settings. The proposed changes are an essential step towards further improving the quality of EOLC.
Supplemental Material
sj-docx-1-pal-10.1177_08258597231170836 - Supplemental material for Cancer Decedents’ Hospital End-of-Life Care Documentation: A Retrospective Review of Patient Records
Supplemental material, sj-docx-1-pal-10.1177_08258597231170836 for Cancer Decedents’ Hospital End-of-Life Care Documentation: A Retrospective Review of Patient Records by L. Russell, R. Howard, M. Street, C. E. Johnson, D. Berry, E. Flemming-Judge, S. Brean, L. William and J. Considine in Journal of Palliative Care
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.