
Abstract
Background
Parental bereavement after the death of an infant in a neonatal intensive care unit (NICU) is a complex and nuanced experience. Support from healthcare practitioners can have a significant impact on bereavement experiences in the short- and long-term. Although several studies exist exploring parental perceptions of their experience of loss and bereavement, there has not been a recent review of beneficial practices and common themes in the current literature.
Objective
This review synthesizes empirical research to identify considerations that ought to guide the caregiving practices of healthcare professionals to support parental bereavement.
Settings/subjects
Data was collected from studies identified in MEDLINE, Embase, and CINAHL. The search was limited to English-language studies describing parental bereavement in the NICU population from January 1990 to November 2021.
Results
Of 583 studies initially identified, 47 studies of varying geographic locations were included in this review. Various themes surrounding healthcare support in parental bereavement were identified including ensuring the opportunity for parents to spend time caring for their child, understanding their perception of infant suffering, recognizing the impact of communication experiences with healthcare providers, and offering access to alternative means of support, all of which have been described as suboptimal. Parents generally want the opportunity to say goodbye to their infant in a private and safe space, be supported through their decision-making and be offered bereavement follow-up after loss.
Conclusion
This review identifies methods of support in parental bereavement based on first-hand parental experiences and routine implementation of these strategies may be beneficial in supporting parents through their bereavement after the loss of a baby in the NICU.
Introduction
Death is no stranger to the neonatal intensive care unit (NICU). Because of extreme prematurity, congenital anomalies, or other complex medical issues, some babies cannot survive despite medical interventions. Others are anticipated to have persistent health problems that severely impact their quality of life. Most NICU deaths result from withdrawing or withholding medical interventions.1‐4
End-of-life decision-making and subsequent neonatal death can create significant emotional turmoil for parents as they navigate their loss and associated bereavement. 5 These parents need to live with the ethical decisions they make, recognizing that the decisions themselves have moral weight. The occasion of the birth of a child, which typically brings excitement and happiness, can instead be filled with grief, despair, and guilt. 6 Recognizing the importance of, and supporting parents through, this loss is a challenging task for those working in the NICU. Healthcare practitioners need to have insights into parents’ experiences to ensure not only that they support decisions that forefront the interests of NICU infants, but also support the parents’ subsequent bereavement. It is important to understand what considerations ought to guide the caregiving practices of practitioners. Through consistent and compassionate bereavement care, practitioners will ultimately be able to enhance experiences for families as they navigate the complexities of infant loss.5,7,8
There have been no systematic reviews in the past decade exploring parental bereavement support in the NICU; however, there have been several related empirical qualitative studies. These studies provide understandings, reflections, and considerations regarding how healthcare practitioners can support families after a neonatal loss.
This review aimed to synthesize the findings of empirical NICU studies relating to parental bereavement and elaborate on considerations that healthcare practitioners can use to guide their caregiving practices and bereavement support.
Methods
Search Strategy
The search strategy for this review was developed with the assistance of a medical research librarian. A search of 3 electronic databases (MEDLINE, Embase, and CINAHL) was performed using a combination of keywords specific to the population (baby, neonate, newborn), the experience pertaining to loss (bereavement, death, dying, grief), and the type of care (palliative, terminal, end-of-life, comfort care). See Appendix 1 for details of the search terms and strategy used.
Selection of Studies
This review included peer-reviewed articles published from January 1990 to November 2021. This date range was chosen to explore contemporary experiences surrounding parental bereavement in the NICU. After excluding duplicates and non-English studies, articles were eligible if based on the primary analysis of empirical data (such as interviews, surveys, and questionnaires). Systematic reviews, editorials, opinion pieces, conference abstracts, and articles published before 1990 were excluded. Grey literature was not reviewed; however, references from included studies were reviewed to ensure no key literature was missed.
After abstract screening by 2 independent reviewers (JL/MvM), studies that involved general pediatric populations, combined pediatric and neonatal populations, or stillbirths and fetal death were excluded unless there was specific mention of independently analyzed NICU-related results. After screening full texts of the remaining results, 47 articles were included. Figure 1 illustrates the study selection process.
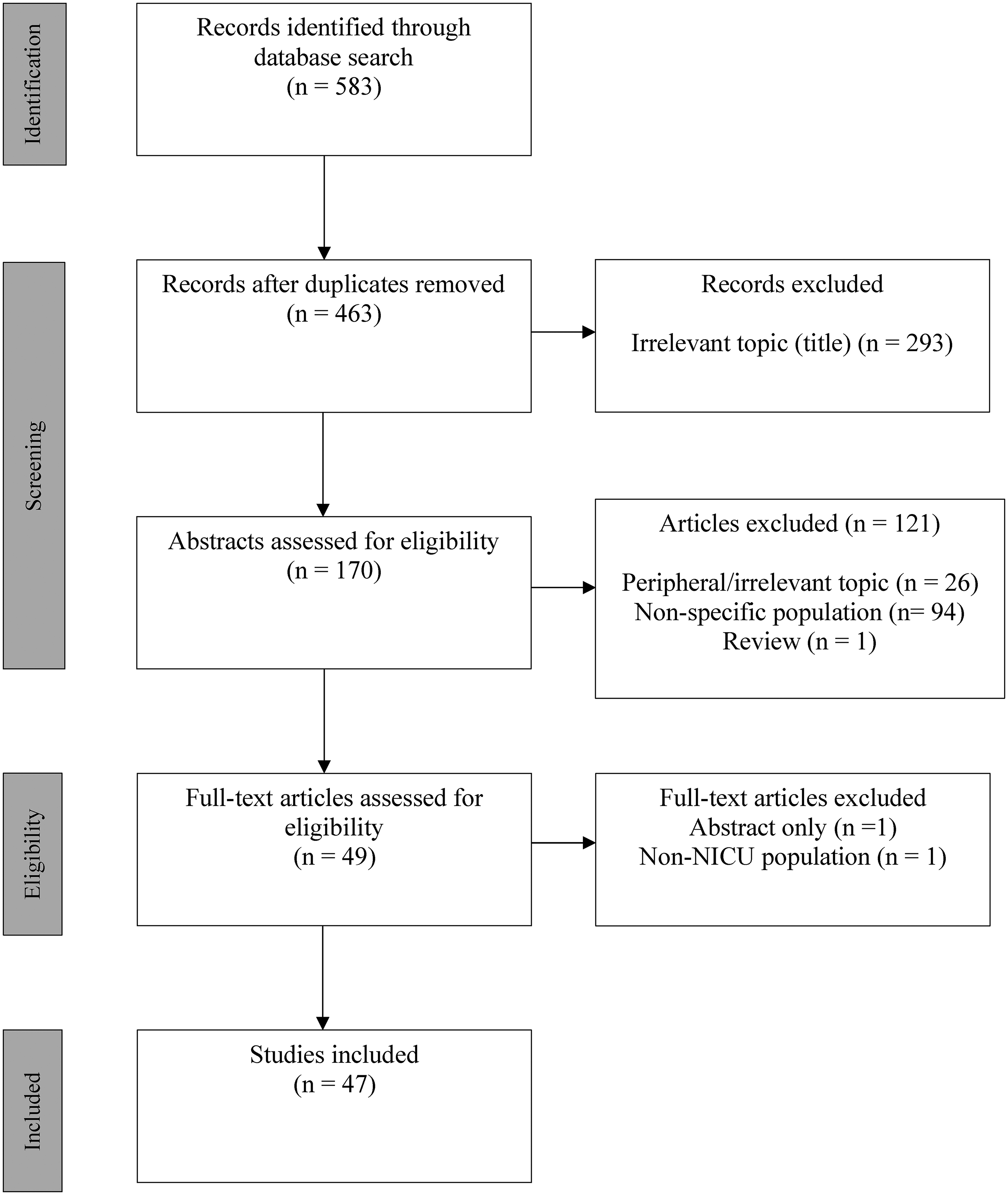
Article Selection Flow Diagram.
Data Analysis
Each study was reviewed by 2 independent reviewers (JL/MvM). Descriptive data on the studies included first author, year of publication, location of study, journal of publication, research design (as described by the author), study purpose, and representative findings. The studies themselves were subjected to a qualitative description analysis, as described by Sandelowski, which seeks to summarize and present information in a coherent manner. 9 ,10 For this study, the aim was to articulate themes that respond directly to the question: For parents experiencing the death of a child in a NICU, what considerations ought to guide the caregiving practices of healthcare professionals to support parental bereavement? In this way, the analysis was oriented specifically to the clinical practices of physicians, nurses, and others working in the NICU. The Mixed Methods Appraisal Tool (MMAT) was used to assess the quality of included studies.1 1 An overall quality score was generated based on the percentage of quality criteria met, ranging from 0% to 100% such that the higher the percentage, the higher the study quality. Two reviewers (JL/MvM) independently assessed the quality of the studies and consensus was reached through discussion for any discrepancies.
Results
A total of 583 studies were identified using the described search strategy. MEDLINE provided 282 studies, Embase provided 102 studies and CINAHL provided 197 studies.
Forty-seven studies (n = 47) were included in this review after assessing relevance. Geographic diversity was identified with the majority of studies being from the United States (N = 22) and others originating from the United Kingdom (N = 7), Australia (N = 5), Canada (N = 3), Jordan (N = 2), Netherlands (N = 2), Switzerland (N = 1), France (N = 1), Norway (N = 1), Ireland (N = 1), Israel (N = 1), and China (N = 1). Demographic information was variably presented in the reviewed papers and the majority did not specify details on participant demographics. However, 18 of the studies reported a participant population that largely included Caucasian mothers who were married at the time of infant death and with some level of higher education. Table 1 describes each study in detail, including the Mixed Methods Appraisal Tool (MMAT) score for each, which was calculated using the detailed MMAT assessment found in Table 2.
Included Articles Describing Support of Parental Bereavement in the NICU.

Abbreviations: NICU, neonatal intensive care unit; TEARDROP, Teaching, Excellent, pArent, peRinatal, Death-related inteRactions, tO, Professionals.
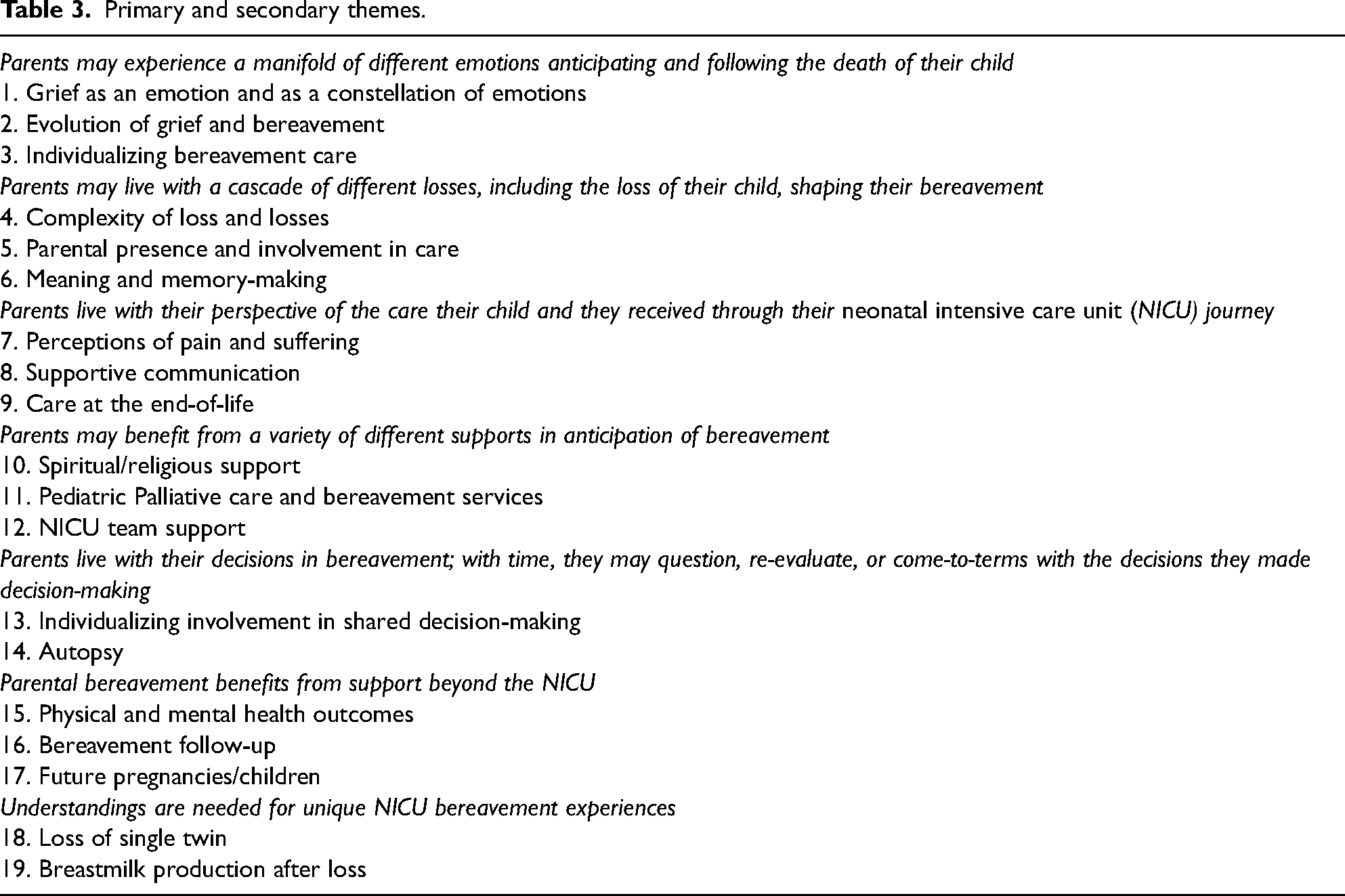
Seven thematic considerations with relevant subthemes were derived from the analysis of included studies (see Table 2).
Mixed Methods Appraisal Tool (MMAT).
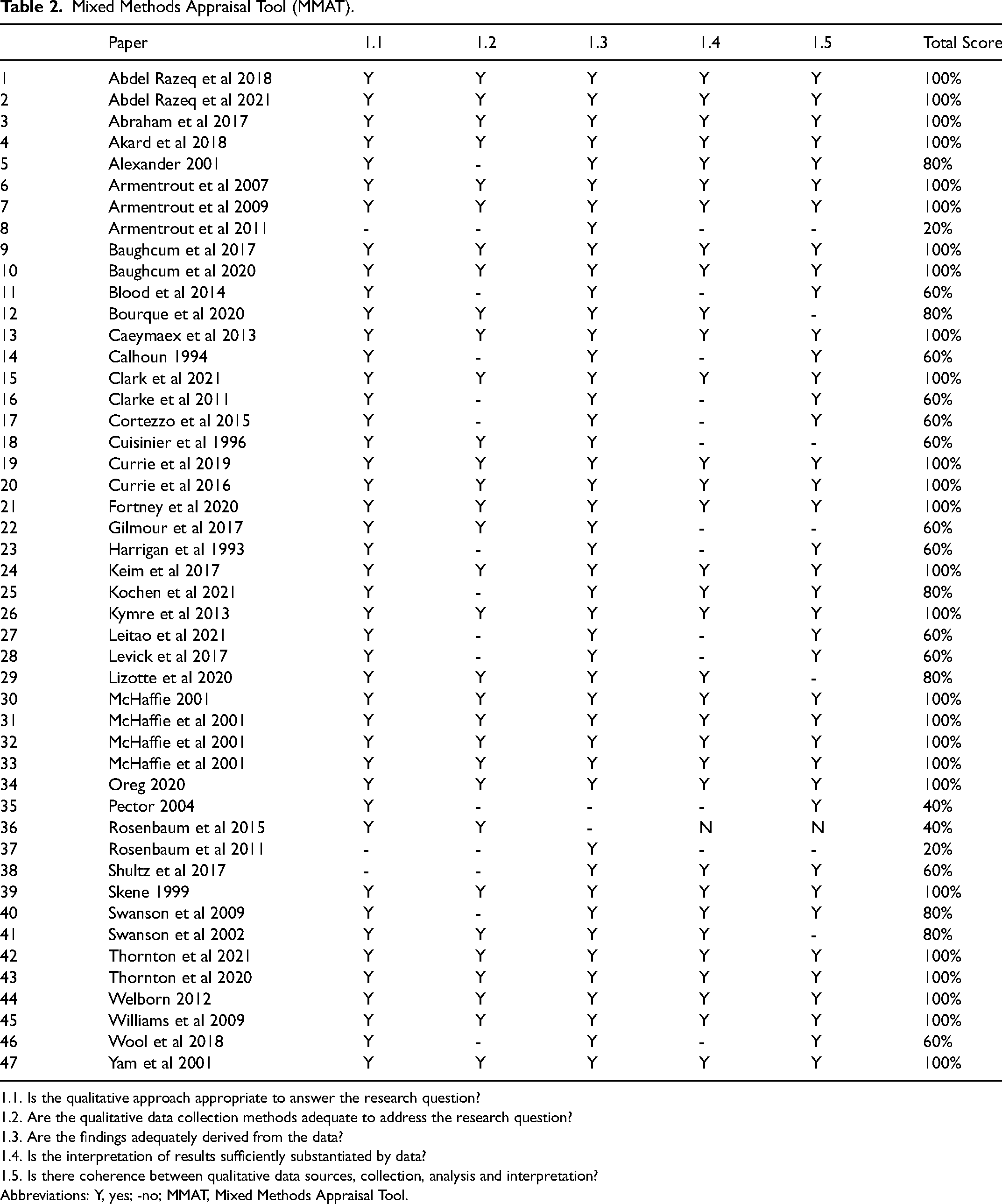
1.1. Is the qualitative approach appropriate to answer the research question?
1.2. Are the qualitative data collection methods adequate to address the research question?
1.3. Are the findings adequately derived from the data?
1.4. Is the interpretation of results sufficiently substantiated by data?
1.5. Is there coherence between qualitative data sources, collection, analysis and interpretation?
Abbreviations: Y, yes; -no; MMAT, Mixed Methods Appraisal Tool.
Primary and secondary themes.
Parents may Experience a Manifold of Different Emotions Anticipating and Following the Death of Their Child
Shared between the included studies is the consideration that parents vary in how they identify and resolve their emotional reactions to the loss of their baby. Grief was described as a predominant constellation of emotions experienced by parents in coping with the acute loss of their baby. From a psychological perspective, grief may be specified as those emotions associated with loss (compared to mourning as those actions resulting from grief). 12 Encircling grief is uncertainty, disappointment, shame, guilt, suffering, and helplessness.13‐17 During an infant's end-of-life, parents often need to balance attachment to their infant with the impending separation. 17 Following, grief may be described as a social phenomenon that is resolved through interactions with various support systems. 18 Severity of grief can be linked to the baby being acknowledged as a separate entity and the duration of postnatal bonding time.19‐21 Finally, grief may be conceptualized as evolving through stages: denial, anger, bargaining, depression, and acceptance. 22 With a neonatal loss, parents may experience these stages partially or fully, in a variety of sequences, and acceptance may never fully transpire.
Bereavement, like grief, is highly individual, yet also a recognizable human experience, as parents live with the loss of their child over time.12‐15 Living with loss is a sense-making experience as parents come to terms with what their child's life was like their presence for their child as parents, and other value-judgments. 15 Healthcare professionals may anticipate, recognize, and respond to parental grief to support evolving and delayed emotional reactions that accompany bereavement.12,14 Focusing on attaching positive meaning to the life lost and maintaining hope—that suffering has ended or that the infant's life had purpose—can support parental bereavement.12,14,22 However, this consideration cannot be generalized because parents’ wishes, values, and other moral beliefs may vary.13,14 Generalizations can lead to a disconnect between healthcare professionals and parents by influencing opinions on what the perceived right action may be in a difficult scenario. 23
Parents may Experience a Cascade of Different Losses Shaping Their Bereavement and Healthcare Professionals can Affect This Burden of Loss
The reviewed studies reflect the broader NICU literature describing the complexity of losses parents may experience when their child requires hospitalization in a NICU: physical separation in the first days of life, parental role interruptions, and so forth.14,24‐27 Parental bereavement unfolds against the backdrop of parents’ NICU experiences, which can include loss experiences before, and in addition to, the death of their child.13,14,26 Activities of healthcare professionals that support parental involvement may potentially alleviate some of what is lost in these situations.13,14,26‐28 From the void of loss, healthcare professionals can support meaningful moments and memory-making, which is highly valued as part of bereavement.13‐15,23,27,29,30‐35 Parents seemingly appreciate any opportunity to be involved in their infant's care including bathing, dressing, diapering, and taking on other parental responsibilities.13,14,26,27,35 Photographs and other media provide parents with tangible objects to relieve their worry about their baby's memory fading over time. 36 It also allows them to share memories and experiences with others who may not have been present for this difficult journey.13,29,34 Other objects include hand/foot molds, clothing, identification bands, or blankets. 34 Photographs taken after death can depict loss and provide meaning to the experience as one of the most common forms of memory-making at neonatal end-of-life. 36 Individualizing the extent of bereavement care is essential as some parents may not be comfortable with these opportunities and can feel pressure if nurses elude to any associated regrets that may arise in the future.23,32,34,35
Parents Live With Their Perspectives of the Suffering Their Child Experienced and Their Communication Experiences With Healthcare Professionals
Families carry with them what happened in the NICU.14,26 In several studies, associations between the perception of infant suffering and the degree of parental grief, adjustment difficulty, and posttraumatic stress symptoms were clearly illustrated.16,25,37‐39 Parents perceive suffering through their infants’ symptoms and based on information received from healthcare providers.16,25,26 Distressing symptoms include skin breakdown, respiratory distress, pain, agitation, lethargy, feeding difficulties, and edema.16,26,39‐41 A common finding illustrated that parents more often perceived suffering in their baby compared to healthcare professionals.30,39
How healthcare providers communicate with parents is highly consequential: the language used needs to be sensitive yet appropriate to the situation.13,15,24,41,42 Statements that presume understanding such as “I know how you feel” can be distressing. 15,24,42,43 Though parents often want to be told medical information in a sensitive, yet straightforward manner, ambiguity may be the reality regarding the timing of death and other less predictable events.41‐43 A lingering prolonged death may undermine parents’ confidence in their decisions. 41 Multiple studies portray the difficulties that arise for parents at the last moments of a baby's life in the NICU. Ensuring privacy, comfort, and security are generally valued.13,18,28,31,36 Healthcare professionals can support families by being deliberate yet flexible in end-of-life care practices.15,36,43 Some parents may not be comfortable being present for the final moments of their child's life. In these cases, parents may still find comfort in speaking to their baby before death, holding their baby while still warm, or entrusting the care of their child to a friend or healthcare provider.27,36,43 For others, holding their child is deeply meaningful.14,27,31 Removing monitoring and medical devices may support a family to focus on their baby.14,27,31 Managing end-of-life symptoms can help parents achieve a “good death” for their child. 39 Providers should be aware that the suffering perceived by parents can contribute not only to their end-of-life decision-making, but also to how they ultimately live with their decisions in bereavement. 16
Parents may Benefit From a Variety of Different Supports in the NICU in Anticipation of Bereavement
Several studies explored the support parents value when navigating the emotional complexities of neonatal end-of-life. The benefits of spiritual care, including prayer, rituals, clergy, and belief in the transcendent quality of the parent-infant relationship are well established; however, healthcare professionals may feel uncomfortable broaching such subjects. 12,14,22,32‐34,44 Education in spiritual and religious concepts can help diminish the disconnect between parental values and provider discomfort. 22 In comparison, palliative care consultation can offer expertise in psychosocial support, symptom management, and coordination of care. 25 Neonatal practitioners find benefit in palliative care team members’ ability to learn about each family's individualized priorities, circumstances, and wishes. 30 Palliative care involvement is associated with an increase in the number of family meetings, the identification of more symptoms, and creating symptom management plans. 40
Developing bereavement expertise among a subset of NICU team members can support the provision of palliative care.32,42 Parents often look to nurses for support as the time spent at the bedside helps build trust and effective communication.7,14,19,26,35 Tailored education with a focus on communication, coping strategies, and enhanced exposure may help providers develop skills in enabling quality of care and supporting grief, navigating anxiety, and overcoming inexperience in end-of-life scenarios.12,13,24,28,42,45,46 Workshop initiatives have been piloted including the Teaching, Excellent, pArent, peRinatal, Death-related inteRactions, tO, Professionals (TEARDROP) program, which uses a Structured, Clinical, Objective, Referenced, Problem-oriented, Integrated and Organized (SCORPIO) approach to teach providers bereavement care strategies. 45
Parents Live with Their Decisions in Bereavement — with Time, They may Question, re-Evaluate, or come to Terms with the Decisions They Made
In bereavement, parents live with their decisions from the NICU.14,26 As such, it is important to consider how parents are supported in their decision-making. Studies describe various models of decision-making including shared decision-making (parents and providers approach a decision together), medical/paternalistic decision-making (a decision made exclusively by healthcare providers), and informed parental/autonomous decision-making (parents make a decision after a provider explains the medical information).37,43 Shared decision-making is generally recognized as the most appropriate approach as it benefits from healthcare providers’ medical expertise and family members’ values and beliefs. 37 These conversations provide opportunities to clarify understanding, align clinical care with care goals, and express compassion to families.7,8,43,47 Parents should have the opportunity to express their preferences for their role in decision-making. 37 Continuity of care and relationships, veracity in communication, expressions of empathy, expertise, and use of evidence, and clear documentation have all been identified as beneficial.7,8,24‐26,39,43,46 Parents who experience shared decision-making seem to have less grief than those who experience medical or parental decision-making. 37
Included studies also highlighted how parents not only live with their decisions regarding goals of care and medical interventions, but also those decisions impacting how present they were for their child engaging in parenting actions, memory-making, and involving others in the lives of their child.14,15,26,27,34,47 There are also those decisions specific to end-of-life that parents live within their bereavement. For example, whether to pursue an autopsy can be a challenging decision. Often the infant's cause of death is known; however, errors in diagnoses may be found in postmortem evaluations. 48 Parents may find benefit in an autopsy's ability to assess obstetrical and genetic risks for future pregnancies. 48 Information may also be found that validates end-of-life decisions. These benefits are not always encountered as providers may be hesitant to offer an autopsy. 48
Parental Bereavement may Benefit From Support Beyond the NICU
It is well recognized that parents whose children died in the NICU have increased risks for physical health concerns, including hospitalizations and higher mortality.15,18 Bereaved parents also experience higher rates of clinical depression, anxiety, and post-traumatic stress.38,49 Screening for pre-existing mental health concerns and developing support strategies before an anticipated death can be beneficial. 25
To support mental health, professional counselling, support groups, peer counselling, and community physicians have all been described as potentially helpful to support acceptance and adaptation to loss.15,33,40,50 For some families, spiritual or religious supports are significant; however, finding adequate support can be challenging.14,15,27,49 Additionally, there is a timeliness to the extent, interval, and duration of support. 51 Parents may experience an abrupt loss of support following the death of their child as they lose the support of the NICU. 30 Initiation of timely supportive care to where parents are in their grieving beyond the NICU is needed.17,30
Most parents will attend a follow-up appointment with the healthcare team if offered. 52 It would seem that these follow-ups should be scheduled 6 to 8 weeks after the death and in a location outside of the NICU. 52 These follow-up visits can help provide answers to parents’ questions and reassurance about end-of-life decision-making. 52 Other options for bereavement follow-up involve familiar staff individualizing follow-up contact over time, sending a card on the first anniversary of the infant's death, and telephone calls by the involved neonatologist. 32 Parents described the benefit from being copied on the written summary from the NICU. 51 Neonatologists should ensure that these summaries maintain sensitivity, use the baby's chosen name if available, and simplify terms to ease parental understanding. 51 Deficiencies in bereavement support include medical follow-up, autopsy discussion, sibling grief management, marital concerns, and expectations surrounding return to normalcy.48,49
Understandings are Needed for Unique NICU Bereavement Experiences
Bereavement following the loss of 1 infant from a multiple gestation pregnancy is a unique phenomenon that may be encountered in the NICU. Losses may occur before or following birth leading to varied bereavement experiences.14,44,53,54 At times, NICU healthcare providers may fail to acknowledge pregnancy loss as the focus is diverted to the surviving infant receiving care. 14 It is essential to document and communicate pregnancy loss to NICU team members to acknowledge this grief potential. 53 It can be challenging for parents to balance grieving the deceased while maintaining attachment to the living. 53 Grief may be compounded by a failure to acknowledge the loss and/or by associated challenges of the surviving sibling.14,20,54 Some families will request aggressive treatment for the surviving child despite poor prognosis, while others are willing to stop when treatment is considered futile. 43 The complexities of loss and survival of siblings may be challenging for families to navigate, recognizing mothers and fathers may vary in their bereavement. 44
Another unique phenomenon surrounding neonatal loss involves lactation. Studies reflect a movement to advocate for a holistic approach to supporting mothers with lactation through their bereavement. 55 Pumping milk has been an outlet for grief and milk donations have been associated with acceptance and healing.42,53 Mothers may experience several emotions when pumping after neonatal death including sadness, emptiness, anxiety, and relief. 53 They may find strength in believing that donating milk will help sustain their child's legacy, maintain their parental identity, and keep the memory of their infant alive through helping others.33,55
Bereavement experiences can continue into future pregnancies. 12 The decision to have another child after a neonatal loss may be very difficult.21,49 However, it would seem most parents have additional children following their loss and this is associated with fewer symptoms of prolonged grief, and posttraumatic stress.12,21 It is suggested that healthcare providers should not discourage or provide recommendations for the timing of future pregnancies. 21 Instead, they should approach such discussions nonjudgmentally with compassion and sensitivity.
Discussion
Key Concepts of Supporting Parental Bereavement in the NICU
Through conducting this review, several themes exploring parental bereavement after the death of an infant in the NICU were identified based on primary data gathered from direct communication with bereaved parents. Although the burden of neonatal death and the impact of provider support is well-established in the literature, this review revealed that the ability of parents to spend time caring for their child, their perception of infant suffering, their communication experiences with healthcare providers, and the access to alternative means of support is often suboptimal. These themes can be a starting point in enhancing the support healthcare providers deliver to parents experiencing the loss of an infant and their subsequent bereavement. Based on the reviewed studies, implementing additional methods of support including access to spiritual and palliative care, shared decision-making, lactation support, and ensuring ongoing bereavement support may have significant benefits. Although general themes have been identified, it is important to appreciate that bereavement care both during and after an infant's death should be individualized. Different values, cultural backgrounds and family circumstances can contribute to different wishes and coping mechanisms for a family during their bereavement. Recognizing these nuances, healthcare providers need to customize their approaches to ensure optimal outcomes.
Gaps in the Literature
There is an abundance of literature surrounding bereavement care after pregnancy loss, stillbirth, and perinatal death, including the death of a fetus between the 22nd full week gestation (or 500 g estimated weight) and 7 days after birth. 57 While some of this literature appeared to include parental perspectives of those whose child died in the NICU, issues unique to perinatal bereavement for such families were left unarticulated. There is a clear need for literature that focuses exclusively, or at least forefronts some of the perspectives of parents whose child received medical interventions and admission to a NICU. The notion of perinatal death includes experiences that may resemble yet also differ from those occurring in the NICU.
Given that the studies reviewed reported specific demographic information on participants being Caucasian, educated, English-speaking and married, uncertainty remains in the influence of familial and cultural diversity in contributing to parental bereavement after a neonatal loss. Broader populations including those who are geographically distanced, recent immigrants, or less educated may have different values in bereavement practices, satisfaction, access to care and involvement in decision-making. An attempt to close this research gap by diversifying inclusion in related research studies could impactfully contribute to the current literature.
Unresolved Tensions in the Literature
Although several conclusions can be formed through similarities found in the reviewed articles, some discrepancies remain. Cultural differences when providing bereavement care are a complex area to navigate. In some cultures, burial and body preparation as well as seeing the body after death is not considered appropriate; however, mothers often find it difficult not to have this opportunity and the literature strongly supports inviting parents to participate. 12 Additionally, in similar cultures, the delivery of news about prognosis and goals of care are often relayed through family members and not the mother directly—which is contradictory to what is considered beneficial to parents as described in most papers. 12 Mothers often find lactation difficult when their neonate is critically ill and despite several papers focusing on pumping and donating milk as an emotional release, some mothers find the pressure to pump and produce milk adds to their burden of stress. 13 Despite education surrounding communication in goals of care and end-of-life being described as rare and suboptimal, 1 paper explores how practitioners feel confident in end-of-life care. 15 Majority of other papers describe practitioners’ desire for further education and training in this area of neonatology.16,30 Moreover, despite the abundance of literature describing the benefit of pediatric palliative care consultations in the NICU, 1 paper illustrated palliative care as being nonsignificant when reporting parental satisfaction. 40 These specific controversies remain unresolved but are crucial to consider when establishing bereavement practices and further emphasize the importance of individualizing care based on each family's beliefs and values.
Limitations of Research
The majority of included studies were small-scale studies identifying themes and conclusions based on local trends. A narrative approach was chosen for this review to capture the diversity of research methods employed. The analysis also included the use of the MMAT demonstrating the findings of the study as credible, meaningful, and relevant to neonatal practice. Given the small-scale studies and results from predominantly developed English-speaking countries, caution should be exercised regarding generalizations. However, appreciating that several studies identified similar conclusions, despite the results of each being subjective and individualized, the commonality of these opinions strengthens the review's findings.
Opportunities for Future Research, Medical Education, and Practice Change
Future research into parental bereavement for those who have lost an infant in the NICU should include exploring the contribution of culture on optimal bereavement support. The geographic diversity of studies in this review alludes to the individualization of care for each family, but also for each culture—and investigating these nuances may be beneficial in further tailoring neonatal bereavement care.
Other areas for research involve expanding on education initiatives in equipping healthcare practitioners with communication and support skills to assist families in their bereavement as well as ensure they are getting the support they need, especially if there is a history of pre-existing mental health concerns. Additionally, understanding the influence of autopsy on grief, closure, and future pregnancies could indicate the importance of offering postmortem examination in both confirming diagnoses as well as providing closure. Obtaining longitudinal follow-up data would also be a useful contribution to the literature as understanding how bereavement experiences impact families long-term can help prioritize areas for improvement.
Conclusion
This review is the first of its kind in the past decade to explore current perspectives on parental bereavement and what considerations ought to guide the caregiving practices of healthcare professionals. Various methods of support have been identified based on first-hand parental experiences and routine implementation of these strategies may be beneficial in supporting parental bereavement. Future studies exploring the success of implementing these recommendations from parents’ experiences can help determine the usefulness of these strategies and provide the next steps to further enhance parental bereavement support in the NICU.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix 1: Search Strategy Outline
1.
a. Exp infant, premature/ OR exp infant, newborn/ OR neonat* OR perinat* OR baby OR exp premature birth/ OR babies OR exp infant, diseases/ OR newborn* OR exp intensive care, neonatal/ OR NICU or exp intensive care units, neonatal AND
b. (Bereave* OR grief OR grieving OR loss) adj3 (Parent* OR caregiver* OR mother* OR father*) AND
c. Exp palliative care/ OR palliative OR exp palliative medicine/ OR comfort care OR exp patient comfort/ OR terminal* OR exp terminal care/ OR “end of life” OR exp death/
*1990-current, English language, excluding comments, editorials, reviews or systematic reviews
= 282 results
1. 2.
a. Exp neonatal intensive care unit/ OR exp prematurity/ OR neonat* OR perinat* OR exp newborn/ OR baby or exp baby/ OR babies OR exp newborn period/ OR newborn OR exp newborn death/ OR exp newborn/ OR exp newborn mortality/ OR newborn intensive care or NICU AND
b. (Bereave* OR grief OR grieving OR loss) adj3 (Parent* OR caregiver* OR mother* OR father*) AND
c. Palliative OR exp terminal care/ OR exp patient comfort/ OR comfort care OR terminal* OR “end of life”
*1990-current, English language, excluding editorials, reviews or systematic reviews
= 102 results
3.
a. (MH “Intensive Care Units, Neonatal”) OR (MH “Neonatal Intensive Care Nursing”) OR (MH “Intensive Care, Neonatal+”) OR (MH “Infant, Newborn, Diseases+”) OR (MH “Perinatal Death”) OR (MH “Infant, Newborn+”) OR (MH “Infant, High Risk”) OR (MH “Infant Mortality”) OR “neonat*” OR “perinat*” OR (MH “Infant, Newborn, Diseases+”) OR “baby” OR (MH “Infant, Premature”) OR (MH “Infant, Postmature”) OR (MH “Infant, Premature, Diseases+”) OR (MH “Infant Death+”) OR “babies” OR “newborn*” OR “NICU” AND
b. (Bereave* OR grief OR grieving OR loss) N3 (Parent* OR caregiver* OR mother* OR father*) AND
c. (MH “Palliative Medicine”) OR (MH “Palliative Care”) OR (MH “Terminal Care+”) OR “palliative” OR (MH “Comfort Care (Saba CCC)”) OR “comfort care” OR “terminal*” OR “"end of life"”
*English language, peer reviewed journal, 1990-present, abstract available
= 197 results