
Abstract
Introduction
In the context of adult palliative care, cancer and noncancer patients sometimes develop severe physical symptoms and/or psychological, existential, spiritual, or social distress that is unbearable for them and refractory to all standard palliative care measures. In these complex situations, palliative sedation can be considered.1–3
According to the European Association for Palliative Care (EAPC), palliative sedation “is the monitored use of medications intended to induce a state of decreased or absent awareness (unconsciousness) in order to relieve the burden of otherwise intractable suffering.” 1 This therapy of last resort can be used in various settings and, consequently, differs in clinical modalities and ethical reflection. In other words, there is no one “palliative sedation” that is applicable to all patients with intolerable and refractory distress but there are various forms of this treatment, the application of which depends on the clinical and personal situation of the patient.4,5 Conceptually, “palliative sedation” often encompasses all forms of sedation, 1 which has led to criticism and suggestions to abandon the use of the term on the ground that it is too general. 5 However, consistent terminology and definitions are lacking to date, which is a source of much ambiguity, confusion, and controversy in clinical practice and research.4–7 Clinically, regardless of the form of sedation, this therapy always requires multiprofessional discussion, prudent application, broad clinical experience, and good practice. The major ethically contentious form seems to be continuous deep sedation until death,4,5,8,9 which is sometimes considered “an extreme facet of end-of-life sedation.” 8
Over the past 2 decades, many clinical practice guidelines (CPGs) have been published by international medical associations,1,2 national and regional scientific societies,10–12 and local institutions. 13 These guidelines are developed not only to help palliative care professionals to address the clinical challenges related to this practice, but also to close the gap between research and practice and, ultimately, to improve the quality of care provided to patients and their relatives.14,15
To date, some systematic reviews of CPGs have been performed.16–21 However, the information sources and research strategies used appear to be insufficient. The authors of 2 systematic reviews explicitly pointed to the difficulty of searching for current CPGs and the significant variation in the form and content of these texts.20,21 Most of the systematic reviews focus on “palliative sedation” without specifying the form of sedation.16–19 The results of 1 systematic review suggest that the CPGs found were conceptually similar, 16 whereas other studies provided contrary results for other CPGs.20,21 In addition, most of the reviews essentially focus on the clinical aspects of palliative sedation and little is known of the ethical issues involved in the various forms of sedation.16–19
The principal aim of our review was to identify, systematically and transparently, CPGs from around the world. The purpose of the analysis was purely descriptive. The secondary objective was to conduct a comprehensive exploration of the full spectrum of ethical challenges of all the forms of sedation presented in these texts. This study also aimed to determine whether CPGs explicitly specified the ethical challenges of applying this therapy with cancer and noncancer patients and, if so, exactly how they did this. To the best of our knowledge, at the time of performing our review and writing this article, no similar study was available.
Given the breadth and complexity of the results, we decided to present all the steps and outcomes of searching for CPGs in this paper, as well as the results of an analysis regarding the formal characteristics and thematic scope of these texts. The results related to the ethical challenges of palliative sedation will be published in a separate article.
Methods
Study Design
We performed a systematic review between 22 June 2021 and 30 June 2022 of CPGs on the palliative sedation of adults. The systematic review protocol was registered on the International Prospective Register of Systematic Reviews — PROSPERO (registration number: CRD42021262571) 22 — and its integral version was published as a preprint on Research Square 23 and in a peer-reviewed journal. 24 The methods presented in the protocol were enriched as the research progressed, without being fundamentally changed. In this paper, the review is reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) statement 25 (see Supplemental File 1).
Information Sources and Research Strategy
The identification of CPGs was conducted in 2 main steps by MT, a postdoctoral researcher in the ethics of palliative care; CJ, a medical librarian; and RJJ, a palliative care physician and bioethicist. The global strategy and information sources are presented in Figure 1. The exact date on which each source was last consulted or searched is specified in the corresponding supplemental file.
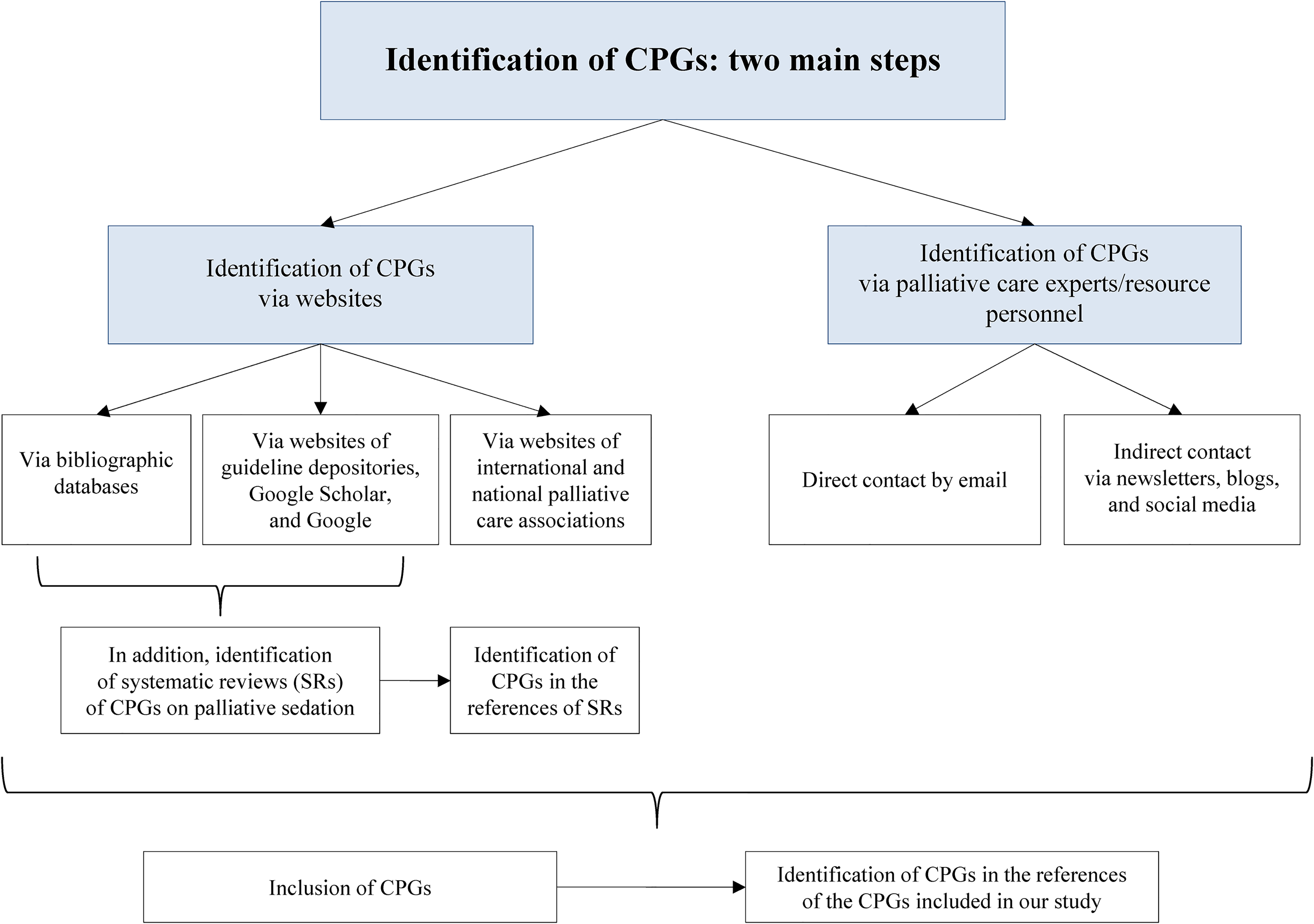
Global Strategy and Information Sources.
In the first step, CPGs were searched for using several websites. More specifically, 5 bibliographic databases were searched first: MEDLINE ALL (Ovid), Embase.com, CINAHL with Full Text, APA PsycInfo (Ovid), and Web of Science (All Databases). Strategies included controlled vocabulary (if available) and free-text terms, and were reviewed by another librarian from the Medical Library of the Lausanne University Hospital and the University of Lausanne using the Peer Review of Electronic Search Strategies checklist 26 (see Supplemental File 2 for the strategies used). Citations were integrated using citation management software (EndNote X9) for deduplication.
The following 13 guideline depository websites were then consulted: Trip Medical Database Pro, ECRI Guidelines Trust, Guidelines International Network (G-I-N), NHS Evidence Search, CISMef Bonnes Pratiques, Society guideline links (UpToDate), LIVIVO, Australia's Clinical Practice Guidelines Portal, Scottish Intercollegiate Guidelines Network, NICE Guidance (UK), and CPG Infobase: Clinical Practice Guidelines/Canadian Medical Association, Registered Nurses Association of Ontario, and Haute Autorité de Santé [French National Authority for Health]. A search was also performed using Google Scholar and Google in English, French, German, Italian, and Polish. This step is detailed in Supplemental File 3.
Although our objective was not to search for texts other than CPGs, some relevant systematic reviews of CPGs on palliative sedation were identified during these 2 substeps and CPGs were sought that appeared in their reference sections.
Finally, we also looked for CPGs on the websites of international and national/regional associations for palliative care (see Supplemental Files 4 and 5). The website addresses of the national/regional associations were found on the EAPC and International Association for Hospice and Palliative Care (IAHPC) websites (for the IAHPC website, only “Hospice/Palliative Care unit IAHPC Institutional Lifetime member” and “Hospice/Palliative Care unit — IAHPC Institutional Member” were consulted; “Hospice/Palliative Care units” were not consulted).
Contrary to our study protocol,22–24 guidelines for palliative sedation were not sought via the websites of societies of medical ethics because a quick search showed that no CPGs were published on these sites. Sometimes, the sites contained ethical positions or ethical reflection on palliative sedation but not CPGs.
In the second step, if no national CPG was found on the internet, the national/regional association for palliative care (identified during the previous step) and/or palliative care experts/resource personnel (identified mostly via these websites) were contacted and asked about CPGs currently used in the country/region. Moreover, 3 international palliative care organizations helped us by publishing a brief announcement of our project and an invitation to participate in it on their websites and in their newsletters.27–29 The President of the International French-speaking Federation for Palliative Care contacted the members of the Committee. In addition, to find as many CPGs as possible from around the world, a call was published on the professional and private social media of the first author, including LinkedIn, Instagram, and Facebook.
Finally, once all the steps were finished and CPGs were included in our study, citation chasing was carried out on all the papers in order to identify guidelines that may not have appeared through the database and complementary searches.
Inclusion and Exclusion Criteria
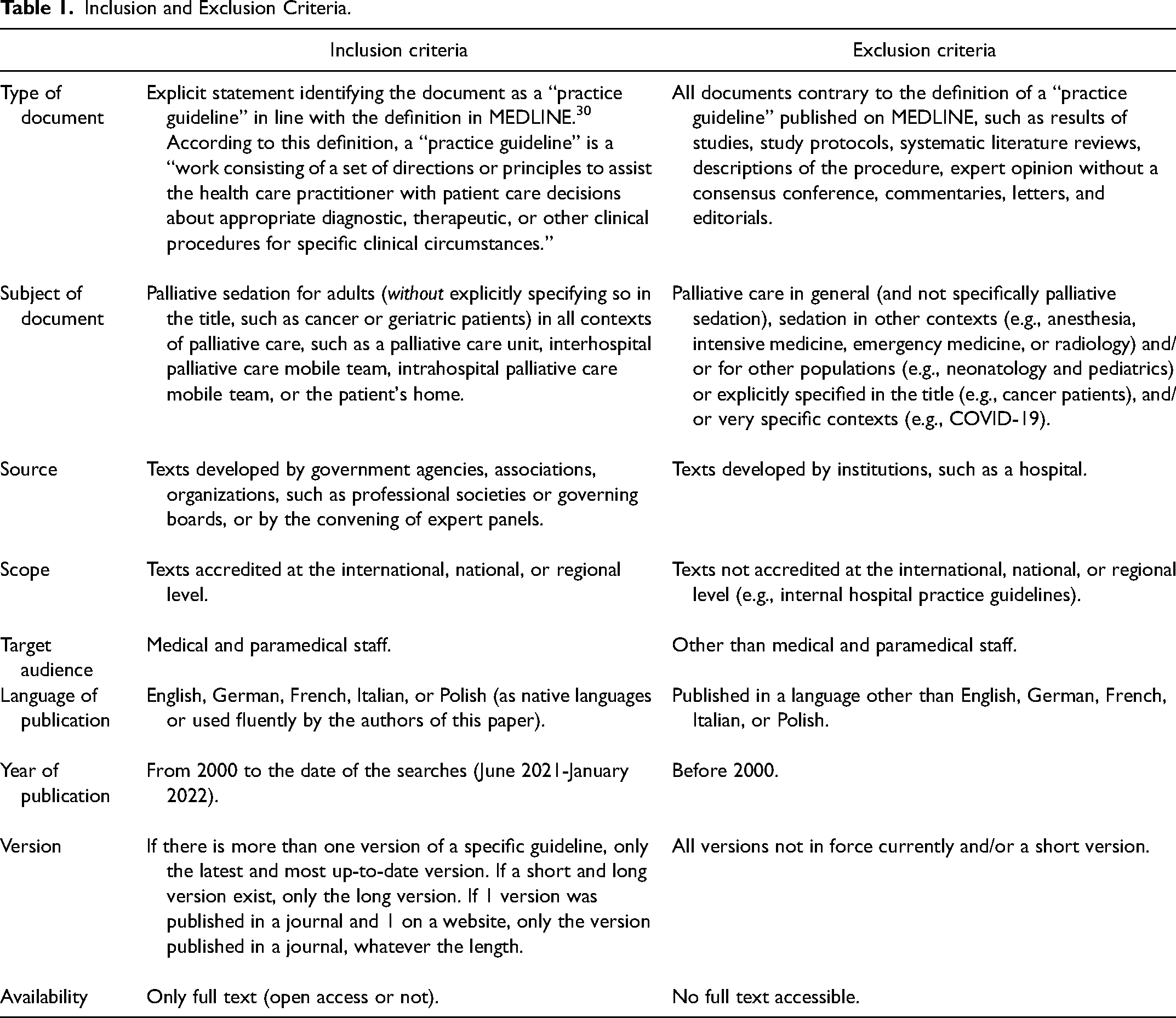
The inclusion and exclusion criteria are presented in Table 1.
Inclusion and Exclusion Criteria.
Selection Process
The selection of CPGs was manually performed by MT and RJJ. No automation tools were used in the process. In the first step, the titles and abstracts of all CPGs identified via bibliographic databases, websites of guideline depositories, Google Scholar, and Google were screened by MT. Relevant CPGs were retrieved and assessed for potential inclusion in accordance with the inclusion and exclusion criteria presented in Table 1. Where it was unclear how to apply the inclusion/exclusion criteria, discussions between the 2 researchers involved in this stage (MT and RJJ) were held and a consensus procedure applied.
In the second step, the eligibility of each full text was assessed and a final decision made regarding whether it would be included in our initial corpus. Any disagreements were resolved by discussion between the 2 researchers. All CPGs initially included in our corpus were sent to the respective resource personnel from national/regional associations for palliative care or to palliative care experts in order to obtain more detailed information. Our objective was to establish whether the version of the CPGs previously identified on the internet was the most recent. All CPGs confirmed were included in our study. If there was no response from the associations or experts, the CPGs were also included in our study.
Data Extraction, Analysis, and Synthesis
In the first main step, vertical analysis (text by text) was carried out in accordance with the analysis grid (see Supplemental File 6). The formal characteristics and thematic scope of each set of CPGs were analyzed. By the “explicit thematic scope of the CPGs,” we understand this as an explicit definition of the form of palliative sedation, based on duration and depth of sedation, clearly mentioned in the text. Our analysis focused on the definitions of palliative sedation and did not concern the terms used to name this practice.
In the second main step, transversal analysis of all CPGs was undertaken in accordance with 2 analysis grids (see Supplemental File 7). All the results were synthesized and, as the purpose of the analysis was purely descriptive, we did not carry out theory development.
Results
Sample Size
Figure 2 presents a PRISMA flow diagram that summarizes the results of the search and selection process. Some items were added to this diagram following our original supplementary searches. The CPGs identified via the 5 databases referred to earlier are presented in Figure 2. Detailed results of the identification of the CPGs via all other sources are presented in Supplemental files (see Supplemental Files 8-14).
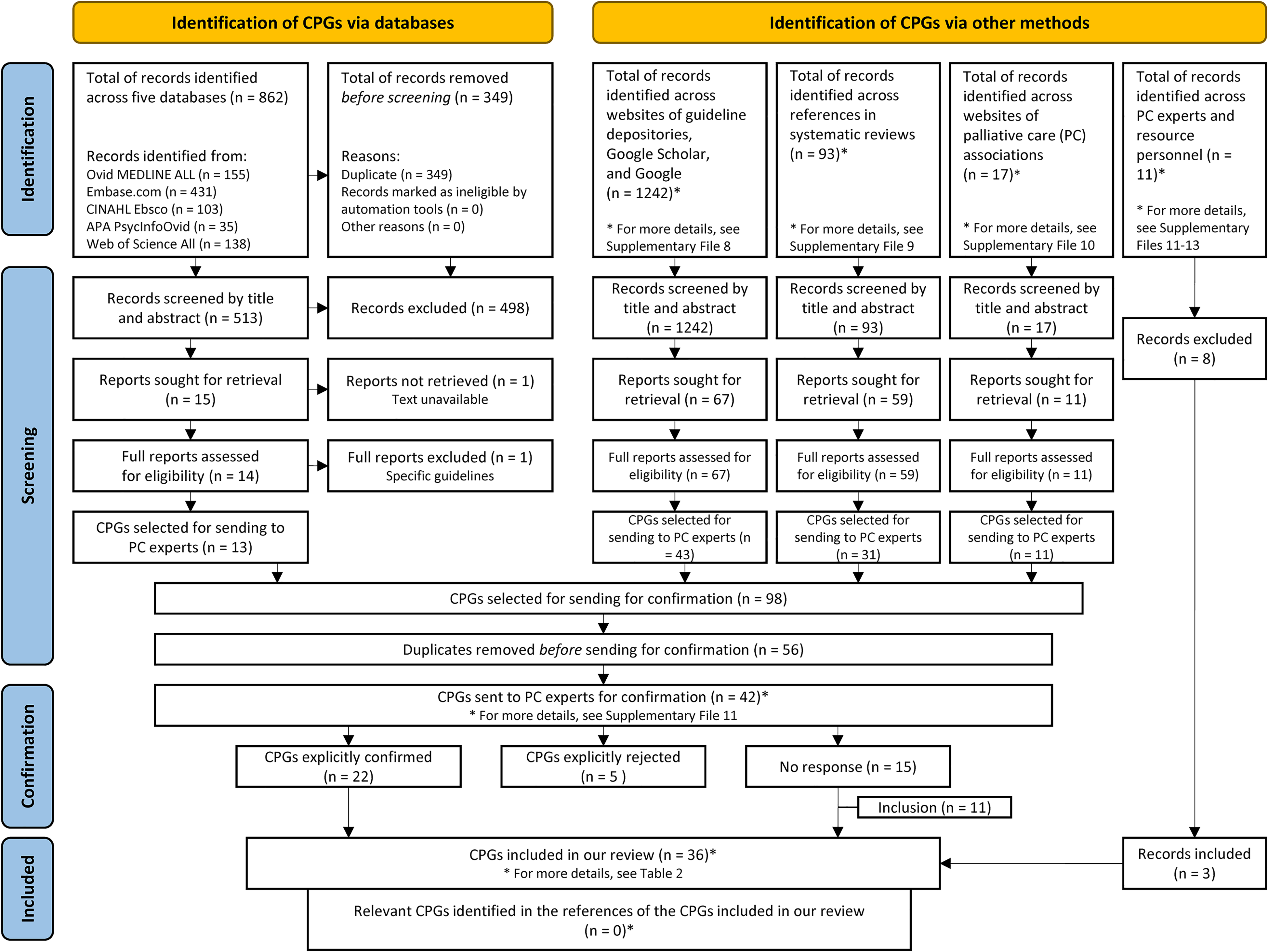
Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) flow diagram.
In total, 36 CPGs were included in the analysis, of which 25 (25/36) were explicitly confirmed by palliative care experts/resource personnel. Most of the CPGs originated in Canada (10),31–40 France (6),42–47 or the USA (5).12,48–51 All the CPGs included in this study are listed in Table 2.
CPGs Included in the Analysis.
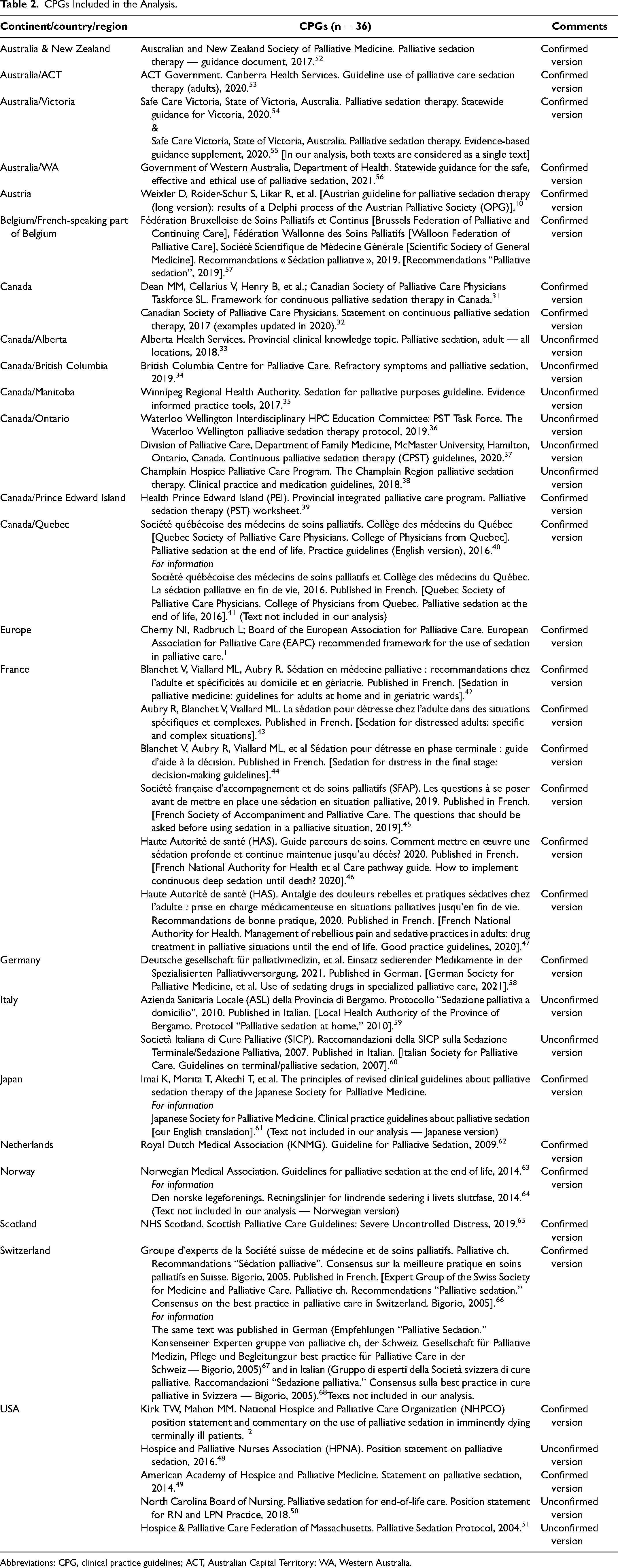
Abbreviations: CPG, clinical practice guidelines; ACT, Australian Capital Territory; WA, Western Australia.
Formal Characteristics of the CPGs
Type of Document
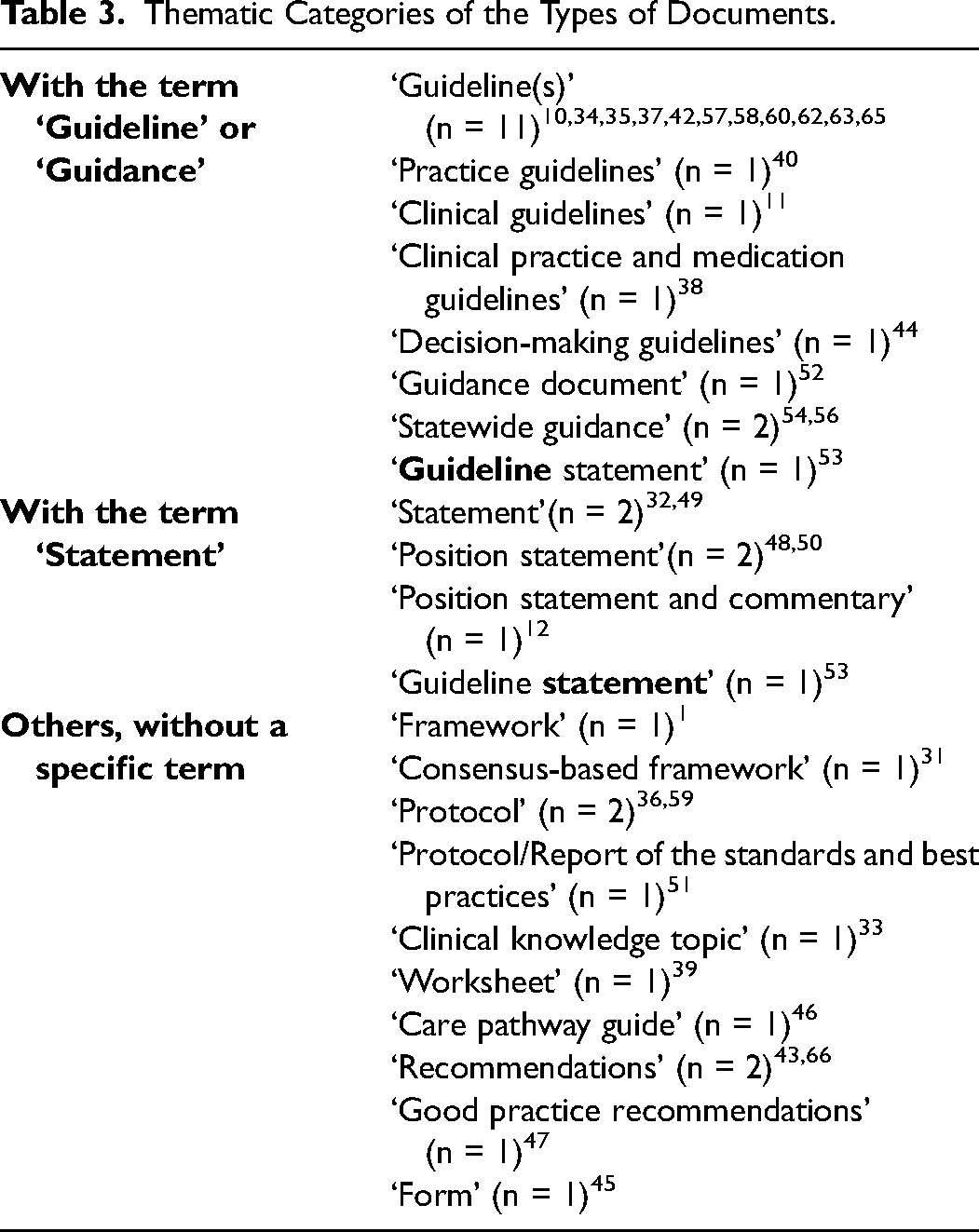
In all cases, CPGs were included in the study according to the inclusion criteria. However, the texts were named in diverse ways. All the nomenclature given can be grouped into 3 main thematic categories. These results are presented in Table 3. No correlation between the type of text and other formal characteristics or the thematic scope of the CPGs was observed.
Thematic Categories of the Types of Documents.
Geographic Scope (International/National/Regional)
The geographic scope of the CPGs varied and was most often national (18/36) or regional (15/36). The national CPGs were from Austria (n = 1), 10 Canada (n = 2),31,32 France (n = 6),42–47 Germany (n = 1), 58 Italy (n = 1), 60 Japan (n = 1), 11 Netherlands (n = 1), 62 Norway (n = 1), 63 Scotland (n = 1), 65 Switzerland (n = 1), 66 and the USA (n = 2).12,49 The regional CPGs originated from Australia (n = 3),53,54,56 Belgium (n = 1), 57 Canada (n = 8),33–40 Italy (n = 1), 59 and the USA (n = 2).50,51 It should be noted that Belgium was unique in terms of operating only regional (but no national) CPG. Australia and Canada had national and several regional CPGs, and Italy had 1 national and 1 regional text. Only 1 of the 36 texts was international (Europe) 1 and 1 other was bi-national (Australia and New Zealand). 52 Finally, the geographic scope of 1 text was not explicitly mentioned. 48
Language of Publication
Most of the CPGs were published only in English (n = 21).1,12,31–39,48–54,56,62,65 Three texts were published in the national language (French, 41 Norwegian, 64 and Japanese 61 ) as well as being fully translated into English40,63 or summarized in English. 11 The other CPGs were published solely in French (n = 7),42–47,57 German (n = 2),10,58 or Italian (n = 2).59,60 Swiss CPG were published in 3 of the 4 official languages of the country — in French, 66 German, 67 and Italian. 68
Source of Publication
Just over half of the CPGs were published by a single palliative care association (n = 12)1,10–12,31,32,45,49,51,52,60,66 or in collaboration with another medical/scientific society (n = 3)40,57,58 or a health authority (n = 4).42–44,65 Other CPGs were published by a single health authority (n = 8), 33,35,39,47,53,54,56,59 medical association (n = 2),62,63 nursing association (n = 2),48,50 or academic institution (n = 1). 37 One text was published by a health authority in collaboration with several associations, not only those connected with palliative care. 46 The source of the publication of 3 texts was not fully clear.34,36,38
Year of Publication
Most of the CPGs were published in the previous 5 years (2016-2021, n = 22).10,11,32–38,40,45–48,50,52–54,56–58,65 Other CPGs were less recent (2010-2015, n = 8)12,31,42–44,49,59,63; (2004-2009, n = 5).1,51,60,62,66 In 1 text, the year of publication was not mentioned. 39
Availability
Most of the CPGs were published on a website with open access (n = 28).10,32–38,40,45–54,56–60,62,63,65,66 Only 7 CPGs were published in a journal.1,11,12,31,42–44 One text was not published anywhere (it was sent to us by a palliative care expert). 39
Length of Document
All the CPGs included in the analysis contained a total of 690 pages. Separately, the number of pages of each text varied. Most of the CPGs were rather short and contained 1 to 10 pages (n = 14).11,12,32,39,43–45,48,50,52,59,63,65,66 Nine CPGs contained 11 to 20 pages,1,10,31,38,42,51,54,56,57 and 7 CPGs had 21 to 40 pages.33–37,47,53 Five texts were rather long, containing 41 to 78 pages.40,46,58,60,62 The number of pages of 1 text was not mentioned (the text was published directly on a website and not as a PDF). 49
Targeted Users
In half of the CPGs, the targeted users were not explicitly mentioned (n = 18).1,12,31–33,36,38,39,42–45,49,51,59,63,65,66 In other CPGs, even if this aspect was clearly mentioned, it was difficult to summarize exactly. Indeed, there were various denominations and functions of profession (reflecting legal and cultural differences) in the countries included and, for example, the term “palliative care clinician” did not have the same meaning in all the countries. Moreover, the scope of the target users, when mentioned, was highly diversified. Generally, the CPGs addressed to all members of an interprofessional palliative care team, but sometimes the scope of the targeted users was extremely large or, in contrast, very narrow. For instance, there was CPG that was addressed to “everyone,” including civil society and all medical professionals (not only palliative care specialists), etc. 40 In contrast, there was also CPG that was only intended for “various medical specialists who may have to administer palliative sedation.” 62 In addition, in some cases, the targeted users were contradictory from one text to another. For example, the Victoria CPG explicitly stated that the “guidance is not intended for use by generalist clinicians,” 54 whereas the Belgian CPG was addressed to a “generalist or specialist physician [and] nurses […].” 57
Number and Affiliation of Individual Authors
The individual authors were not mentioned in 14 of the CPGs.32,34,36,39,45,48–50,52,53,56,57,63,65 In other CPGs, because of the heterogeneity of the working and publication methods, as well as the designations of the professions (due to legal differences from one country to another), it was difficult to synthesize the data. Nonetheless, the analysis showed that an interprofessional group was always involved in the elaboration of the CPGs. In all cases, there was a group of palliative care clinicians (physicians, nurses, psychologists, etc.) alone or working with clinicians from other medical specialities (e.g., oncologists and psychiatrists). Other specialists, such as ethicists, philosophers, lawyers, theologians, specialists in spiritual care, chaplains and/or palliative cadre volunteers, sometimes participated in the elaboration of the CPGs.
Thematic Scope
The thematic scope of the CPGs was difficult to analyze rigorously because of significant variation in the terms and definitions of palliative sedation used and the editing of the texts. We identified 3 main sets of circumstances: (1) CPGs with a fully explicit thematic scope; (2) CPGs with a partially explicit thematic scope; and (3) CPGs without an explicit thematic scope.
In total, we identified 22 CPGs (22/36) with a fully explicit thematic scope.10,11,33–38,40,42,43,46,47,50,53,54,56–59,62,66 Twelve of those CPGs were general and covered a range of types of palliative sedation,10,11,40,42,43,47,50,53,57–59,62 6 concerned “proportionate continuous sedation,”34–36,38,54,56 and 1 was on “proportionate sedation with all types of the duration of this therapy.” 66 Two texts related to “continuous deep sedation until death”33,46 and 1 text concerned this form of sedation and specified that “deep sedation” is not necessary in all cases. 37
In contrast, the thematic scope of 9 of the CPGs (9/36) was partially explicit.1,12,31,39,49,51,52,60,63 Eight texts did not specify the duration of palliative sedation, only the depth1,12,39,49,51,52,60,63: 7 of them referred to “proportionate sedation”1,12,39,49,51,60,63 and 1 concerned “deep sedation.” 52 One text related to “continuous sedation” without specifying the depth of this sedation. 31 The thematic scope of the other 5 CPGs was unclear.32,44,45,48,65
Several CPGs explicitly stated what forms of sedation were excluded from the text. However, this presentation was often confusing. For example, most of them confused differences between palliative sedation and other practices (e.g., palliative sedation is not a side effect of symptom control measures) and the thematic scope of the text (e.g., palliative sedation as a side effect of symptom control measures is not included in the guidance). This made our analysis very difficult and, consequently, our results are not exhaustive. In this section, we only present summary results in order to outline the variety and complexity of the thematic scope. The most important differences between the CPGs concerned emergency sedation in catastrophic events and sedation used at end of life in weaning the patient off life-sustaining treatment (e.g., ventilator support). For instance, whereas Canadian (Champlain Region) CPG excluded emergency sedation in catastrophic events from their texts, 38 Belgian CPG developed recommendations for using sedation in this context. 57 In Australian CPG, sedation at end of life in weaning patients off life-sustaining treatment was clearly included in the thematic scope. 53 In contrast, this context was explicitly excluded from the EAPC guidelines. 1
Discussion
To the best of our knowledge, our systematic review of CPGs on palliative sedation from around the world is the first in the international context of palliative care. As no similar study exists, direct comparison is not possible. Nevertheless, some results, as well as methodological aspects, should be discussed in order to enrich reflection related to this study and, consequently, improve the quality of CPGs when updating or editing these texts.
First, in comparison with the information sources and research strategies used in other systematic reviews, our search methods were more developed and complex in order to find as many CPGs as possible from around the world, but without claiming to be exhaustive. For this reason, we searched not only several bibliographic databases, websites of guideline depositories, Google Scholar, and Google, but also the websites of international and national/regional associations for palliative care, and were in contact with palliative care experts/resource personnel across the world. In addition, a brief announcement of our project and an invitation to participate were published in the newsletters and on the websites of international palliative care organizations,27–29 as well as in accounts on professional and private social media. As most of the CPGs, especially those published in languages other than English, are part of the grey literature (i.e., they are not published in a scientific journal), our methods could be useful or even exemplary for future research. Moreover, sending the CPGs identified on websites to palliative care experts/resource personnel for confirmation seems an optimal method. Indeed, we found several versions of CPGs on the internet that had not been updated. However, it should be noted that this step is time-consuming and this aspect should be considered when planning research and interpreting the results. Furthermore, although we contacted several palliative care experts/resource personnel in each country in order to confirm the version of a CPG, we did not receive a response in all cases; in our study, 11 CPGs (11/36) were not confirmed. On the one hand, this is one of the limitations of our review. On the other hand, the confirmation of texts found on the Internet is not a standard methodological rule; the authors of previously published systematic reviews of CPGs did not commonly use this method.16–21
As earlier mentioned, our systematic review was performed between June 2021 and June 2022. The review required 12 months because of the complexity of the research strategy, the Covid-19 situation, the unavailability of many palliative care experts, and the deadlines for publication of our announcements and study protocol. The results presented in this article must, therefore, be interpreted only with respect to the period of our research.
However, this generates an important limitation of the inclusion criteria concerning the most recent versions of CPGs. Some of the CPGs selected were being updated when we were conducting our study. For instance, the review date of the Canberra CPG, published by the ACT Government, was 1 October 2021, 53 which was when we were carrying out our research. In addition, some palliative care experts informed us of works related to the update of current versions of CPGs (e.g., Dutch, Swiss, and Quebec CPGs). Finally, when we were performing the systematic review, the most recent EAPC framework was from 2009, 1 but we knew that an international expert group was working on an update of these guidelines. It is possible that by the time this article is published, an updated version of the EAPC guidelines will be available. Moreover, at the time this manuscript was being reviewed, a systematic review of European CPGs was published. 69 However, only 9 CPGs were included in this study.
Second, the type of text was 1 of our 10 inclusion/exclusion criteria. We intended to include all documents considered a “practice guideline” in line with the definition in MEDLINE. 30 According to this definition, a “practice guideline” is a “work consisting of a set of directions or principles to assist the health care practitioner with patient care decisions about appropriate diagnostic, therapeutic, or other clinical procedures for specific clinical circumstances.” 30 However, this definition is very general and does not make a distinction between, for example, “clinical practice guidelines”, “position papers,” and “consensus statements.” Consequently, our systematic review included texts that were in accordance with this general definition. Surprisingly, although the texts were variously named, no correlation between the name given to the type of document and other formal characteristics or the thematic scope of the text was observed. However, from a methodological perspective, CPG is generally distinct from a “statement.” CPG must be developed systematically and in a fully transparent way and report the quality of the evidence and the strength of the recommendations. A “statement” is only used when, for example, evidence is lacking or is of poor quality. 70
In general, an assessment of the quality of the selected CPGs is part of a systematic review and is usually performed using the Appraisal of Guidelines Research and Evaluation instrument (AGREE II).71–73 However, this tool only permits an evaluation of the overall methodological quality of CPGs, especially their development process. As a complement to AGREE II, the Appraisal of Guidelines Research and Evaluation Recommendation EXcellence 74 was recently developed to evaluate the clinical applicability, values and preferences, and implementability of CPGs. 75 As our systematic review focuses solely on the ethical challenges of palliative sedation (i.e., the nonclinical aspect of this practice) as presented in the CPGs, we decided, from the beginning of our study protocol, not to appraise the quality of these texts. It should be noted that there is a specific tool for evaluating guidelines and guidance documents on palliative sedation.16,76 However, it was not applicable to our study for 2 principal reasons. First, the objective of our study was not to compare national CPGs with the EAPC framework published in 2009, but to identify, systematically and transparently, CPGs on palliative sedation for adults from around the world and to explore and describe the full spectrum of ethical challenges of all forms of palliative sedation as presented in these documents, including the EAPC framework. Moreover, as already mentioned, this European framework is in the process of being updated.
Finally, contrary to the study performed by Abarshi et al, 16 our systematic review shows that the thematic scope of CPGs is very difficult to analyze rigorously because of significant variation in the terms and definitions of palliative sedation used and the editing of the texts. Regarding the terms used to refer to palliative sedation, these are multiple and various and, in order not to make our analysis even more complex, we chose to focus our investigation on explicit definitions of sedation. The problem of the inconsistent terminology related to palliative sedation has frequently been addressed in the literature for many years, without finding an optimal solution.6,7,77–79 The results of our analysis reveal that several CPGs cover a range of types of palliative sedation or concern only 1 form of sedation. Other CPGs (less than half) are partially clear or unclear. On the one hand, in the absence of thematic consistency, it is impossible to compare these texts and, on the other, in retrospect, this demonstrates that our initial decision not to assess the quality of the CPGs was appropriate. It should be noted that our analysis related to thematic scope focused only on the forms of palliative sedation, and other aspects, such as setting, indications or target population, could potentially be explored.
Methodological Limitations
We decided to include only CPGs on palliative sedation in general, without explicitly specifying, for example cancer or geriatric patients. Firstly, as mentioned in our study protocol,22–24 one of the objectives of our systematic review was to determine whether the CPGs explicitly specify the ethical challenges of the use of this therapy for cancer and noncancer patients and, if so, exactly how they did this. If we had included specific CPGs on palliative sedation for cancer patients, we would not have been able to achieve this objective. Secondly, a particular context, such as geriatric or neurological patients, could potentially raise specific ethical challenges. It was thus important that the thematic scope be more or less homogeneous, and without specific contexts. However, in practice, this was very difficult and biased because of the inaccuracy of the texts. For example, despite the specific title of the French CPG (Sedation in palliative medicine: guidelines for adults at home and in geriatric wards), 42 the text was general and did not give any information about these particular contexts. In contrast, the title of the Japanese CPG was general (The principles of revised clinical guidelines about palliative sedation therapy of the Japanese Society for Palliative Medicine), 11 but the text referred to the oncology context: “The target population [was] adult patients with incurable cancer.” 11 Consequently, this may bias the results of our systematic review.
Conclusion
At the time of writing this article, our study is the first to present an overview of CPGs from around the world. It provides several pieces of information that could guide reflection in this field and that could be used to develop or update CPGs at the international, national, or regional level. Efforts should be made to clarify the thematic scope of CPGs on palliative sedation, in order to generate an understanding of the forms of this therapy addressed in the texts.
Supplemental Material
sj-pdf-1-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-1-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-2-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-2-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-3-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-3-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-4-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-4-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-5-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-5-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-6-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-6-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-7-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-7-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-8-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-8-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-9-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-9-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-10-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-10-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-11-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-11-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-12-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-12-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-13-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-13-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-14-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-14-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Supplemental Material
sj-pdf-15-pal-10.1177_08258597221138674 - Supplemental material for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review
Supplemental material, sj-pdf-15-pal-10.1177_08258597221138674 for Clinical Practice Guidelines on Palliative Sedation Around the World: A Systematic Review by Martyna Tomczyk, Cécile Jaques and Ralf J. Jox in Journal of Palliative Care
Footnotes
Authors’ Contribution
MT and RJJ conceived and designed the study; they are the guarantors. MT, CJ, and RJJ contributed substantially to the development of the methodological section. MT performed all the searches for and analyzed all the CPGs, with help from CJ and RJJ. All authors participated in the interpretation and discussion of the results. MT wrote the manuscript with input from both the other co-authors. All authors read, provided feedback, and approved the final version of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This systematic review is funded by a grant (grant number: not applicable) from the Pallium Foundation (Canton of Vaud, Switzerland). The research is independent of any involvement from this sponsor.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.