
Abstract
Introduction
Heart disease, cancer, cerebrovascular accidents, and chronic lower respiratory disease are the four most common causes of death in the US. 1 Many chronic diseases progress to end-stage conditions that cannot be cured and often result in poor quality of life, excessive medical resource use, and ultimately, death. Palliative care (PC) is the provision of care intended to alleviate or control symptoms, provide psychological and spiritual support, relieve physical discomfort, and improve or maintain the quality of life for such patients with chronic end-stage diseases and their families.2,3
While PC has been noted to be essential for all patients with severe advanced illness, traditionally, it has been directed mostly toward patients with cancer.4–7 There are significant differences in access to PC among patients with chronic diseases or those presenting with acute deterioration.8,9 Despite being the leading cause of death in the US, patients with heart disease approaching the end of life remain less likely to receive upstream non-hospice-based PC. 10 Similarly, lower use of PC has been observed for other chronic conditions such as chronic obstructive pulmonary disease (COPD) and dementia.11–13 Patients with chronic diseases are often burdened with complex symptoms, physical and emotional distress, and significantly impaired quality of life. Therefore, integrating PC into disease management is even more crucial.11,14 According to the Center to Advance Palliative Care (CAPC), the prevalence of hospitals with PC service has increased from 658 to 1831 from 2000 to 2016. 15 However, despite this continued growth in the availability of PC services, data about the secular trends and uptake of PC in managing acute exacerbation of common chronic diseases are limited. We utilized the largest all-payer inpatient database in the United States to study the rates and trends of inpatient PC encounters among the top four common causes of mortality in the US. Our second objective was to identify independent predictors of inpatient PC encounters. Finally, we aimed to describe associations between resource utilization and subsequent discharge destination.
Methods
Study Design
This is a retrospective, longitudinal observational cohort study of all patients hospitalized with a diagnosis of heart disease, cerebrovascular accident, cancer, or chronic lower respiratory disease within the National Inpatient Sample (NIS) database.
Study Data
In this study, we analyzed patients from the NIS database admitted with a primary diagnosis of heart disease, cerebrovascular accident, cancer, or chronic lower respiratory disease between January 1, 2004, and December 31, 2017. The NIS is part of the Healthcare Cost and Utilization Project sponsored by the Agency for Healthcare Research and Quality. 16 It is the largest all-payer US inpatient care database, containing more than 100 clinical and non-clinical variables derived from billing data submitted by hospitals to state-wide organizations across the United States.17–19 It includes data from about 8 million hospital stays per year and covers more than 95% of the US population.
Study Population
Adult patients >18 years old who were admitted with a primary diagnosis of heart disease, cerebrovascular accident, cancer, or chronic lower respiratory disease were included. The first discharge diagnosis in the database is referred to as the “principal diagnosis.” These patient records were recognized utilizing International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes up to September 30, 2015, and then ICD-10-CM codes till December 31, 2017. Heart disease, cerebrovascular accident, cancer, and chronic lower respiratory disease were defined as per the Centers for Disease Control and Prevention (CDC) ICD codes classification (Supplementary Table 1). All patients diagnosed with hospitalizations for each of the four chronic diseases were then stratified based on PC encounters using ICD-9-CM code V66.7 and ICD-10-CM Z51.5 codes. These codes have been used in previous studies and were shown to have high specificity and positive predictive value in identifying PC encounters.20–22 We also collected demographic data, including age, sex, race, ethnicity, median home income, and primary expected payer. NIS contains comprehensive information about comorbidity burden in the form of 29 Elixhauser comorbidities, hospital region, teaching status, and bed size, which were also included in this study. Additionally, we used ICD-9-CM and ICD-10-CM codes to extract information about important comorbidities such as previous myocardial infarction, percutaneous coronary intervention, smoking, coronary artery bypass graft surgery, stroke, and family history of coronary artery disease. 18,23 Patient records with missing information for age, sex, in-hospital mortality, and PC were excluded.
Study Outcomes
The primary outcome of interest for this study was the in-hospital PC encounter during hospitalization. Secondary outcomes of interest were (1) to study the independent predictors of PC encounters, (2) to study the association between PC encounters and hospital costs, length of stay, and discharge destination. Costs were calculated by multiplying the charge-to-cost ratio by the total charge representing the bill for the patient stay but did not include professional fees and non-covered charges. All costs were also adjusted for inflation using the federal government's publicly available inflation adjustment calculator (https://data.bls.gov/cgi-bin/cpicalc.pl) using December 2019 as the reference. All outcomes were assessed for the heart disease, cerebrovascular accident, cancer, and chronic lower respiratory disease groups separately, whereas, in the subgroup analyses, cancer was considered as the reference group.
Statistical Analysis
Weighted data were used for all statistical analyses by applying the discharge weight (DISCWT) up to 2012 and “TRENDWT” after that and using Stata's survey estimation (svy) command to account for the change in the sampling strategy by Healthcare Cost and Utilization Project (HCUP) in 2012. 24 As the records are being sampled by hospitals rather than individuals in the NIS, clustering of records within hospitals was considered in the survey estimation. 24 For descriptive statistics, categorical variables were presented as percentages, while continuous variables were presented as median (interquartile ranges). The baseline variables of PC patients compared to non-PC patients across the four groups were compared using descriptive statistics. We constructed Poisson regression models, including PC encounter count as an outcome variable and disease group, age, and year as covariates to calculate incidence rate ratios (IRRs) of PC utilization with 95% confidence intervals (95% CI). Post-estimation commands were used to estimate absolute rates. We used an interaction term between the calendar year (as an ordinal variable) and disease group to estimate absolute rates of PC encounters per 100,000 hospitalizations per year for each disease group and calendar year, adjusting for age. We also performed the same models using the calendar year as a continuous variable to estimate the average absolute change in rates per calendar year for each disease group. A statistically significant difference in trends over time between each disease group compared to the cancer group was identified using the interaction term's P-value in the primary model. Joinpoint regression analyses were undertaken to estimate the average annual percentage change (AAPC) in PC encounters for each population group by using statistical software that calculates AAPC in rate and tests whether any apparent change in trend is significant. 25 Adjusted Poisson models were also constructed for overall rate differences, including demographics, important comorbidities, hospital characteristics, and 29 Elixhauser comorbidities in the model (Supplementary Table 2). Finally, multivariable logistic regression analyses were performed to study the independent predictors of PC encounters for each population group using the same variables provided in Supplementary Table 2. Collinearity diagnostics were performed by measuring the tolerance and variance inflation factors. 26 To further study the association between disease severity and PC encounters, subgroup analyses were undertaken for patients who died in hospital, patients discharged alive, and subgroups of patients hospitalized with heart failure, acute myocardial infarction, chronic lower respiratory disease, CVA, and cancer. Stata v14.2 MP (Stata Corp, College Station, Texas) was used to perform all statistical analyses, and α was set at .01 for any statistically significant result.
Ethical Consideration
An institutional review board was not required for this study as NIS is publicly available anonymized data and does not contain any patient-identifiable information.
Results
Study Population
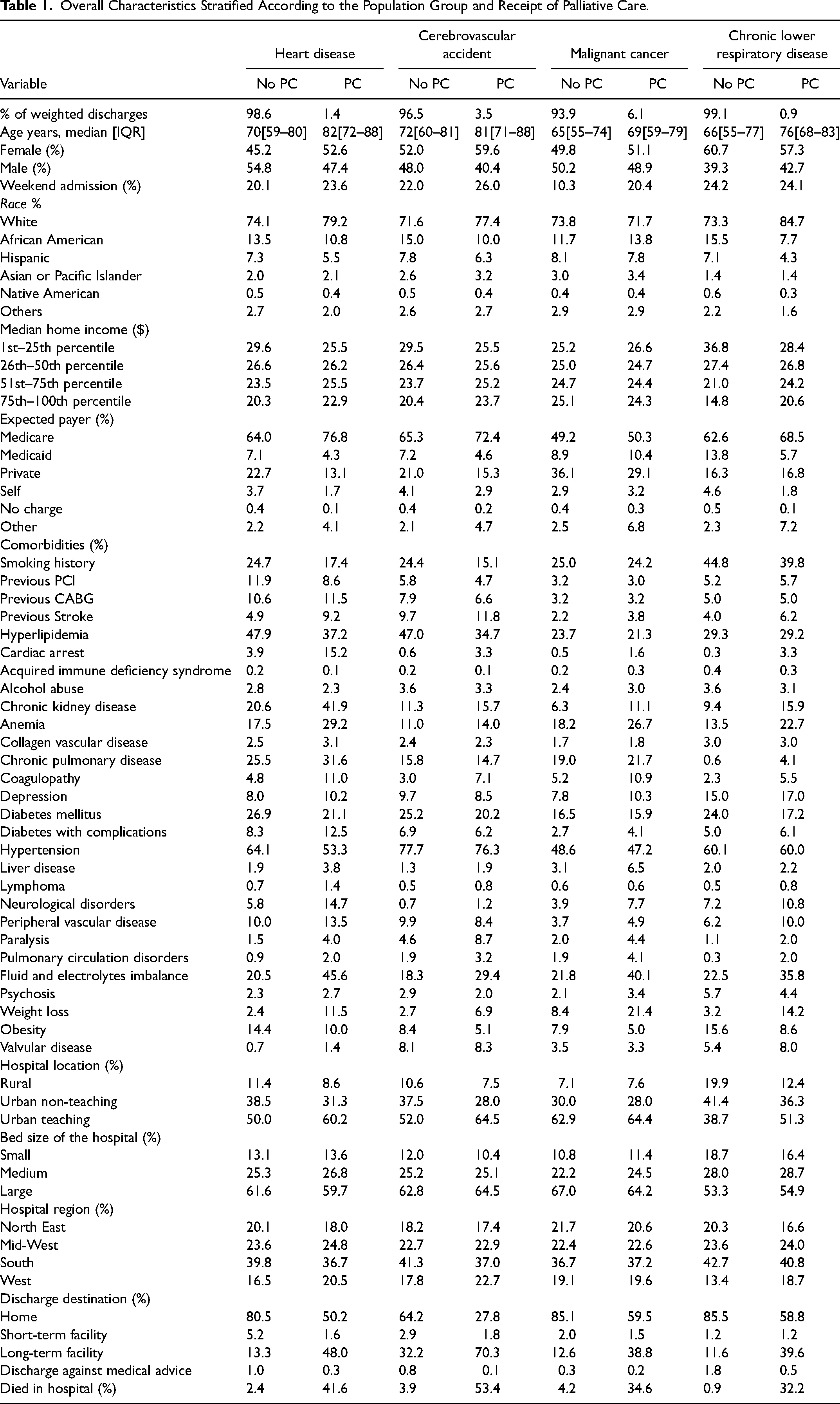
Out of 91,877,531 total hospitalizations between 2004 and 2017, 50,667,180 (55.2%), 12,758,741 (13.9%), 15,843,276 (17.2%), and 12,608,335 (13.8%) were related to heart disease, cerebrovascular accident, cancer, and chronic lower respiratory disease, respectively. Overall proportions of PC encounters were 1.4% in heart disease, 3.5% in cerebrovascular accidents, 6.1% in cancer, and 0.9% in chronic lower respiratory disease cohorts (Supplementary Figure 1). Patients receiving PC were generally older and more likely to be females, Caucasian, and Medicare beneficiaries across all four cohorts. Receipt of PC was significantly higher in patients with comorbidities such as co-existing chronic kidney disease, previous stroke, previous coronary artery bypass graft, COPD, complicated diabetes, neurological disorders, and peripheral vascular disease. Patients admitted with high-risk features such as cardiac arrest were also more likely to receive PC, particularly in the heart disease cohort. A higher proportion of patients referred to PC in the heart disease (41.6%) and cerebrovascular accident cohort (53.4%) died in the hospital compared to cancer (34.6%) and chronic lower respiratory disease (32.2%) cohorts (Table 1).
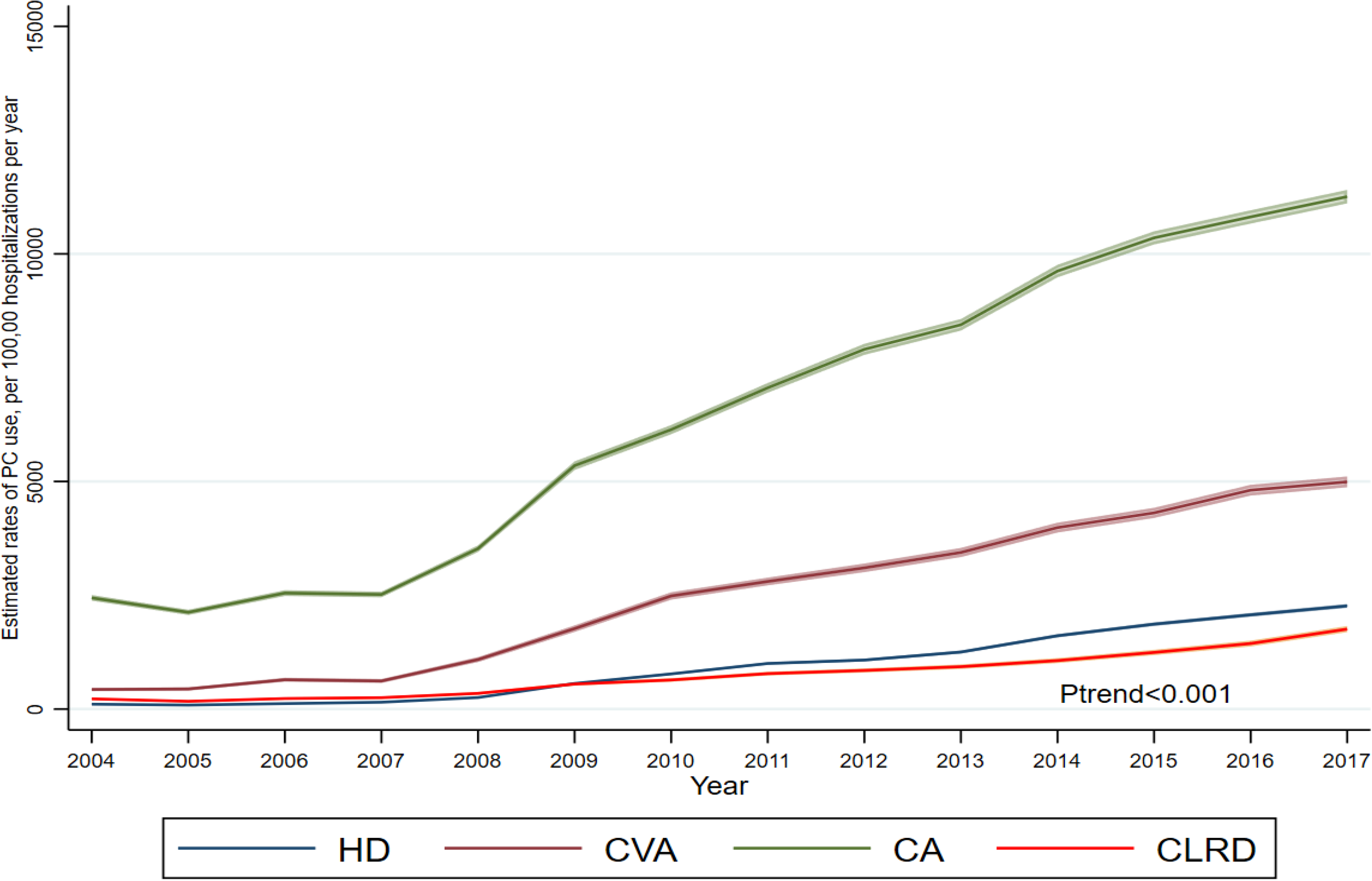
Temporal trends in receipt of palliative care stratified according to population group and year. HD, heart disease; CVA, cerebrovascular accident; CA, cancer; CLRD, chronic lower respiratory disease; PC, palliative care.
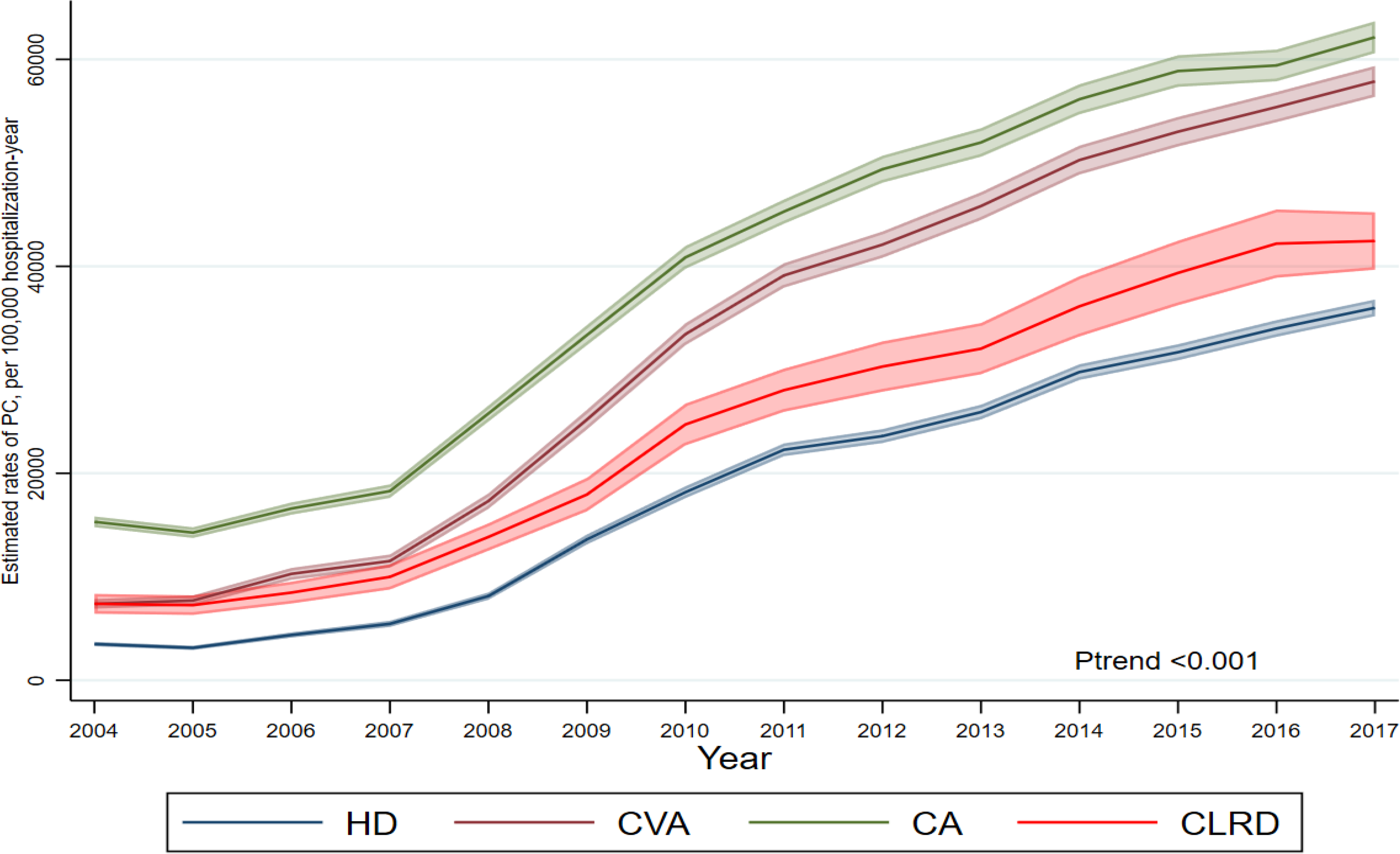
Temporal trends in receipt of palliative care in patients died during admissions stratified according to population group and year. HD, heart disease; CVA, cerebrovascular accident; CA, cancer; CLRD, chronic lower respiratory disease; PC, palliative care.
Overall Characteristics Stratified According to the Population Group and Receipt of Palliative Care.
Rates of Palliative Care
Age-adjusted estimated rates of PC encounters were highest for the cancer group throughout the study period, increasing from 2308 (95% CI 2249–2366) in 2004 to 10,794 (95% CI 10,652–10,936) in 2017. Chronic lower respiratory disease cohort had the lowest rates of PC encounters; 255 (95% CI 231–278), rising to 1882 (95% CI 1821–1943) per 100,000 hospitalizations, respectively (Table 2, Figure 1). The average absolute increases in rates per calendar year were also highest for the cancer group, followed by the cerebrovascular accident, heart disease, and chronic lower respiratory disease groups, respectively (Table 2). Joinpoint regression analysis showed the highest AAPC in PC encounters in heart disease (31.4% 95% CI 22.6%–40.8%) and the lowest in cancer (14.9% 95% CI 10.1%–20.0%) group (Supplementary Figure 2). Temporal analysis of AAPC in each population group showed a higher rise in AAPC in each population group until 2011 and a constant steady rise afterward except for the cancer cohort, which had a statistically insignificant increase after 2012 (AAPC 7.49, P = .1) (Supplementary Figure 2). In the subgroup analysis of patients who died in the hospital, the chronic lower respiratory and heart disease groups had the lowest absolute rates of increase over time. Notably, the absolute rate change was highest for the cerebrovascular accident group dying in hospital (4979 95% CI 4918–5040) per 100,000 hospitalizations per calendar year (Table 2, Figure 2). Similar trends were observed for subgroup analysis of admissions discharged alive (Table 2). PC encounter rates also increased in patients hospitalized with heart failure from 290 (95% CI 270–310) to 4193 (95% CI 4016–4369) and acute myocardial infarction from 266 (95% CI 241–292) to 5456 (95% CI 3138–3559) between 2004 to 2017 (Table 3). Finally, heart failure patients who died in the hospital had a lower absolute rate increase per year 3679 (95% CI 3578–3780) than cancer group 4241 (95% CI 4189–4292) in PC encounters.
Age-Adjusted Estimated Rates of Palliative Care Referrals per 100,000 Hospitalizations per Year by Population Groups and Calendar Year.
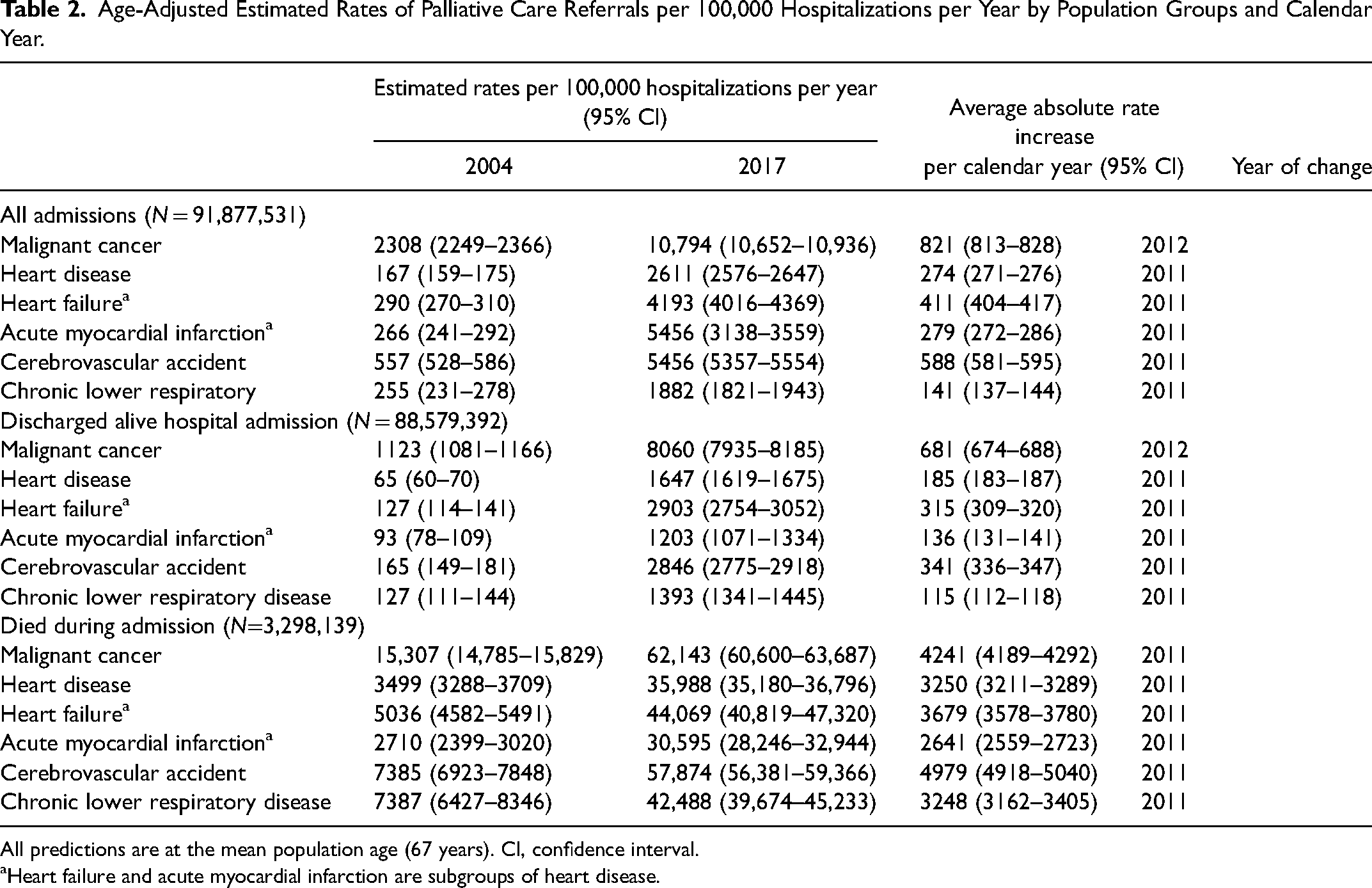
All predictions are at the mean population age (67 years). CI, confidence interval.
Heart failure and acute myocardial infarction are subgroups of heart disease.
Adjusted Relative Rates of Palliative Care Referrals Stratified According to Population Group and Calendar Year.
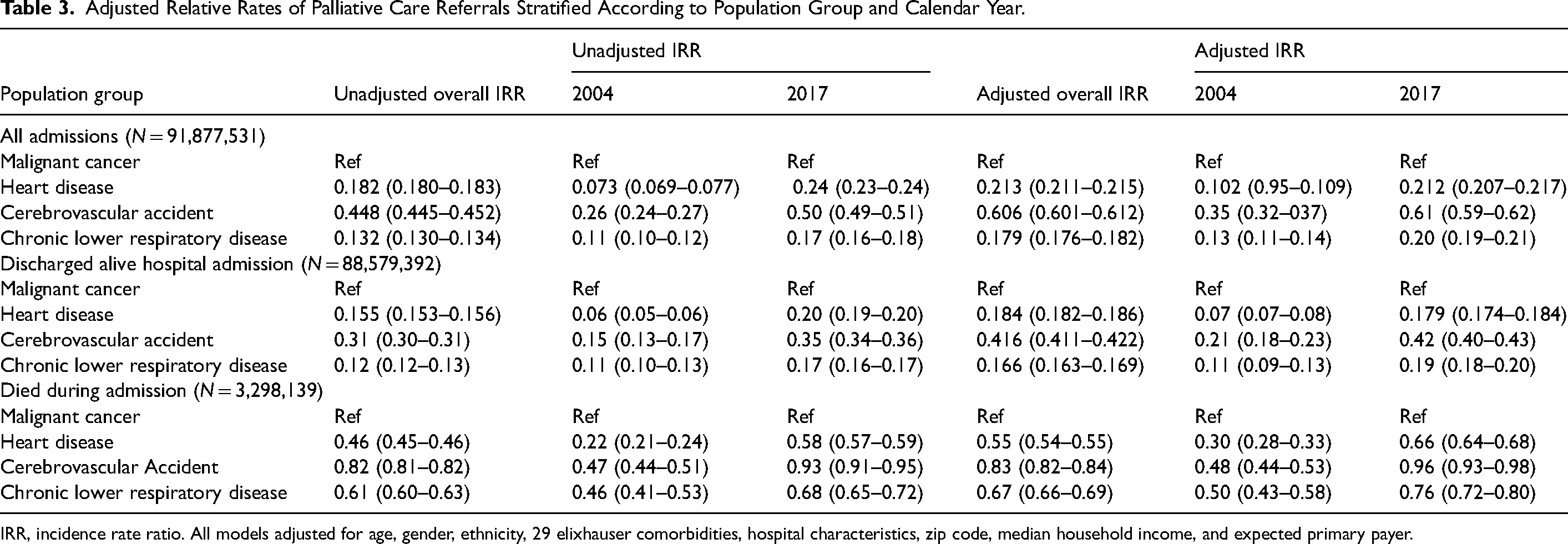
IRR, incidence rate ratio. All models adjusted for age, gender, ethnicity, 29 elixhauser comorbidities, hospital characteristics, zip code, median household income, and expected primary payer.
Overall unadjusted and adjusted rates of PC encounters stratified by population group showed that all groups had a significantly lower uptake of PC compared with the cancer group. The heart disease cohort was least likely to receive PC (adjusted IRR 0.213 95% CI 0.211–0.215). Similar differences were observed in the study cohort who died in the hospital, where heart disease (adjusted IRR 0.55 95% CI 0.54–0.55), cerebrovascular accident (adjusted IRR 0.83 95% CI 0.82–0.84), and chronic lower respiratory disease (IRR 0.67 95% CI 0.66–0.69) groups had significantly lower PC encounters compared with the cancer group (Table 3).
Independent Predictors of Palliative Care Encounters
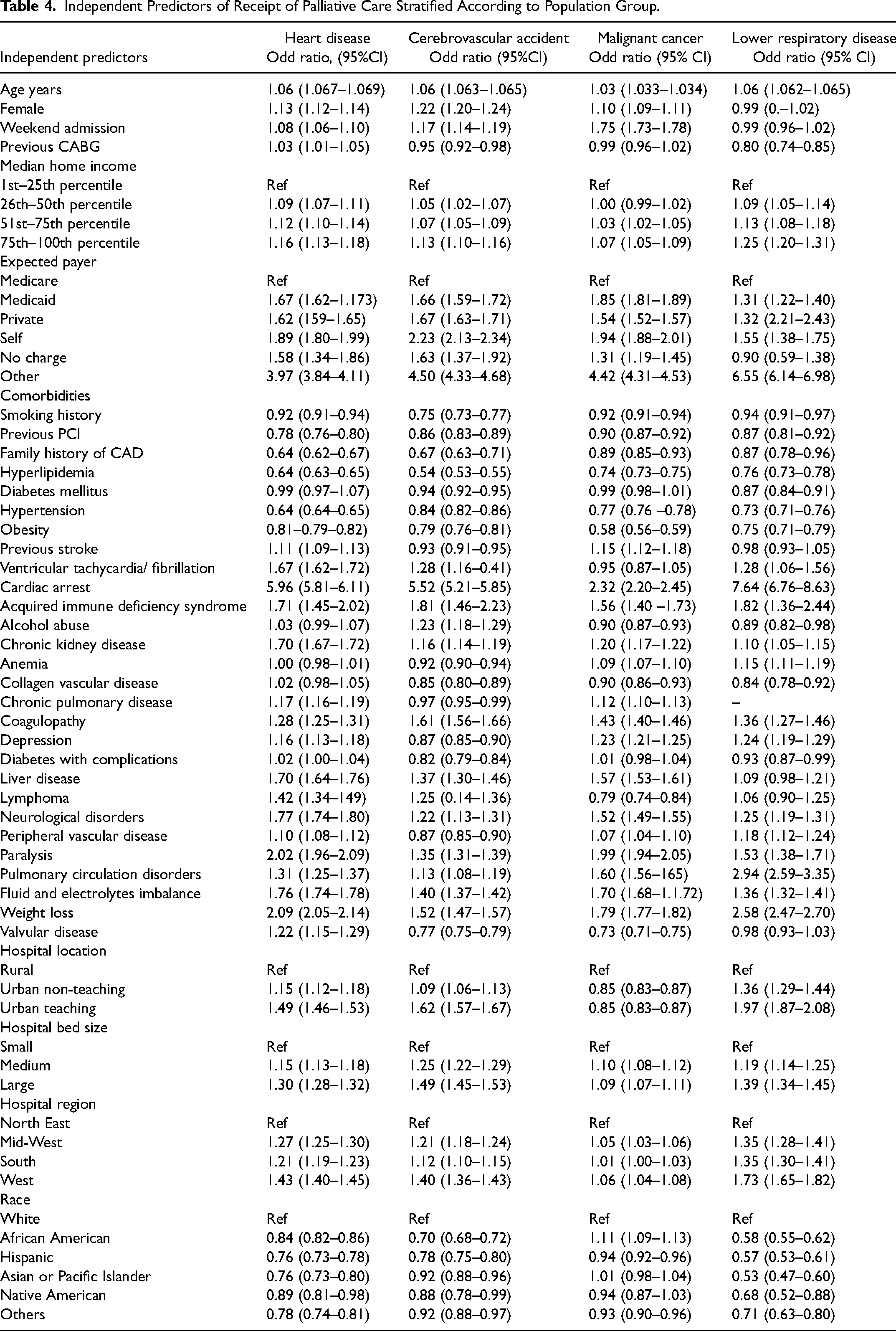
The independent predictors for PC encounters for each cohort are reported in Table 4. Female sex had the strongest association with receipt of PC in the cerebrovascular accident cohort (OR 1.22 95% CI 1.20–1.24). High-risk features such as cardiac arrest, ventricular arrhythmias, neurological disorder, metastatic cancer, weight loss, and solid tumors were strong independent predictors of PC across all four groups. Urban teaching hospital status was associated with increased PC encounters in heart disease, cerebrovascular accident, and chronic lower respiratory disease cohort but not in the cancer group. All racial and ethnic minorities were less likely to receive PC compared with white Americans, except for African Americans with cancer, who had higher odds of receiving PC (OR 1.11 95% CI 1.09–1.13). Finally, there were significant regional variations across all four population groups in receipt of PC, where the West region had the highest odds of PC use compared with the North East region. In the subgroup analysis of patients who died in the hospital, ethnicity, male sex, and cardiovascular risk factors such as hypertension, hyperlipidemia, and family history of coronary heart disease were negative predictors of PC encounters (Supplementary Table 3).
Independent Predictors of Receipt of Palliative Care Stratified According to Population Group.
Trends in Resource Utilization and Discharge Destination
Patients with a longer length of stay received PC more frequently across all disease groups and the overall trend throughout the study period remained stable (Supplementary Table 4). Compared to the cancer group, heart disease, cerebrovascular accident, and chronic lower respiratory disease cohort receiving PC had shorter hospital stays. There was a significant cost rise for PC cohorts across all four groups. However, the differences in the cost of care between PC and non-PC groups for heart disease, cerebrovascular accident, and chronic lower respiratory disease narrowed down over time to almost similar costs by the end of the study period. In contrast, there remained a significant difference in the cost of care between PC and non-PC groups for the cancer cohort throughout the study period (Supplementary Table 5). Finally, patients discharged to long-term care facilities were more likely to receive PC across all four groups whereas home destination had lower PC uptake (Table 1).
Discussion
These nationally representative data of over 90 million hospitalizations provide an important overview of trends, characteristics, and cost of care for patients referred to inpatient PC services after admission with one of the four most common causes of death in the US. Between 2004 and 2017, there was a temporal increase in the use of in-hospital PC encounters across all patients admitted with primary diagnosis of cancer, heart disease, cerebrovascular accident, and chronic lower respiratory disease. The growth of PC encounters was significantly higher in earlier years until 2011, after which it increased at a slower rate until 2017. Despite these encouraging trends, heart disease patients, including those with heart failure and acute myocardial infarction, remained least likely to be referred for inpatient PC consultation. Similar lags in PC encounters were observed in patients who died in the hospital, with heart disease patients almost twice as less likely to receive PC compared with the cancer cohort. Our study provides important information on temporal changes of PC encounters and factors associated with differential use of PC among the four most common causes of death in the US.
Despite a consensus regarding the early integration of PC services into the management of chronic diseases, there remain significant disparities in the use of PC services.27–30 Previous studies have reported that patients with chronic illnesses such as COPD, heart failure, and cerebrovascular accident suffer from poor quality of life, increased psychological, social, and emotional discomfort in addition to chronic symptoms of the disease and are likely to benefit from early access to PC specialist services compared to patients with cancer.13,31–33 Our study shows that despite a significant increase in access to PC services, patients with non-malignant illnesses have lower rates of access to PC. This was particularly evident in later study years, where uptake of PC services utilization was even slower. Prior studies have shown a modest rise in referral to PC services, particularly in the terminal manifestation of cerebrovascular disease (CVD).9,10,20,34 Our study highlights significant differences in the trajectory of inpatient PC use among the common cause of death in the US. These differences were also evident in patients dying in hospitals from heart disease and chronic lower respiratory disease. Heart disease remains the most common cause of death in the US, and its prognosis is worse in patients with heart failure, acute myocardial infarction complicated by cardiogenic shock, cardiac arrest, or those with co-existing malignancy. 35 Cardiologists are also known to have a lower tendency to refer patients to PC services.10,36 We also noted significant differences in the use of PC based on the admitting hospital location, where urban teaching hospitals had the highest uptake of PC compared to the rural hospital. These differences may be related to the lack of local specialist PC service at the admitting hospital. A multidisciplinary team approach with the early involvement of PC specialists, family caregivers, patients, and relatives is required to improve access to PC in this cohort. 37
Our study also identifies various patient and hospital characteristics which were independently associated with PC referrals. We found that African American ethnicity, male sex, and home discharge destination had significantly lower odds of PC referrals. There are various barriers for early access to PC services in patients with heart disease, CVA, and chronic lower respiratory disease, such as lack of awareness among treating physicians, unrealistic expectations from family or patients, local availability of specialist services, uncertainties regarding patient goal and prognosis, and lack of funding for specialist PC services.32,38–40 Our results show that the characteristics of patients with chronic illness receiving PC are significantly different compared to cancer. Furthermore, uncertainties regarding their prognosis may require a different model of care compared to cancer patients involving a multidisciplinary team with a dual focus on active disease management and providing psychological, social, and symptom control from the PC services. 33
These data illustrate temporal differences in length of stay and cost of care in all four population groups. Patients with cancer had more extended hospital stays and increased healthcare costs compared with heart disease, cerebrovascular accident, and chronic lower respiratory disease. However, it appears that the total and inflation-adjusted cost of care difference between the PC and non-PC groups has narrowed down over the study period. Finally, we also observed that discharge to a home or a short-term facility was associated with significantly lower PC use than a long-term facility. Recent data show that home has become the most common place of death for patients with CVD, COPD, and other chronic illnesses.41–44 Our results highlight the need to develop pathways to ensure individualized, uniform access to PC in patients discharged home.
This analysis has certain limitations. Although NIS collects comprehensive information regarding comorbidities, length of stay, and care costs, we did not have information regarding the degree of symptoms or disease severity. Differences in the rates of PC utilization between the different conditions studied may relate to differences in the proportion of end-stage patients in each group. Nevertheless, we recorded similar observations in sensitivity analyses undertaken to analyze hospital episodes where the patients had died. NIS also lacks information around other important, relevant predictors and quality indicators of PC utilization, such as the presence of family care providers at the time of referrals, appropriate medical therapies for chronic disease management, quality of PC being offered such as psychological support and timing of PC referrals. It is possible that a small proportion of patients with heart disease or chronic lower respiratory disease suffered from acute deterioration or a terminal event such as cardiac or respiratory arrest with unsuccessful resuscitation. Consequently, these patients may have died before being referred to PC services. As the PC encounter in NIS was derived using the ICD codes ICD-9-CM V66.7 and ICD-10-CM Z51.5, which are specific for specialist PC services input, PC rates may be underestimated in our study, particularly when other physicians or providers provide PC. Finally, although we used the primary diagnosis to categorize patients into four mutually exclusive groups, diagnosis code misclassification or error cannot be ruled out. The costs charged in the NIS represent the actual amount billed by the hospitals and do not account for physician fees and non-covered charges, which may have resulted in an underestimation of the actual costs.
Conclusion
In this most contemporary analysis of patients admitted with acute exacerbation of common chronic conditions from the US, we found significant differences in upstream non-hospice in-hospital PC utilization. Despite increasing trends, the uptake of PC referrals in patients hospitalized with heart disease, cerebrovascular accident, and chronic lower respiratory disease still lags behind cancer, particularly in patients dying during hospitalization. Heart disease patients, especially those hospitalized with heart failure and acute myocardial infarction, are least likely to receive PC despite it being the most common cause of death in the US. Our results show that PC utilization is not associated with increased costs or length of stay. Further research is needed to identify potential barriers, develop tailored pathways, and raise awareness among the non-PC specialist to involve PC services as soon as physical or psychological distress is identified in patients with non-malignant conditions.
Supplemental Material
sj-docx-1-pal-10.1177_08258597221136733 - Supplemental material for Palliative Care Utilization Among Hospitalized Patients With Common Chronic Conditions in the United States
Supplemental material, sj-docx-1-pal-10.1177_08258597221136733 for Palliative Care Utilization Among Hospitalized Patients With Common Chronic Conditions in the United States by Muhammad Rashid, Haider J Warriach, Claire Lawson, Mohamad Alkhouli, Harriette G. C. Van Spall, Safi U Khan, M Shahzab Khan, Mohamed O Mohamed, Muhammad Zia Khan, Ahmad Shoaib, Masroor Diwan, Raktim Gosh, Deepak L. Bhatt and Mamas A. Mamas in Journal of Palliative Care
Footnotes
Abbreviations and Acronyms
Author's Contributions
MAM and MR designed the study; acquired, analyzed, and interpreted data; revised the report; and agreed to be the guarantors who are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. CL provided the statistical support for the analysis. HJW, MA, HV, SUK, MSK, MOM, MZK, AS, MD, RK, and DLB made substantial contributions to the design of the work, revised the report; and agreed to be accountable for all aspects of the work. All authors have read and approved the manuscript for submission.
Declaration of Conflicting Interests
Dr. Deepak L. Bhatt discloses the following relationships—Advisory Board: Cardax, CellProthera, Cereno Scientific, Elsevier Practice Update Cardiology, Level Ex, Medscape Cardiology, PhaseBio, PLx Pharma, Regado Biosciences; Board of Directors: Boston VA Research Institute, Society of Cardiovascular Patient Care, TobeSoft; Chair: American Heart Association Quality Oversight Committee; Data Monitoring Committees: Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Cleveland Clinic (including for the ExCEED trial, funded by Edwards), Contego Medical (Chair, PERFORMANCE 2), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo), Population Health Research Institute; Honoraria: American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ACC.org; Vice-Chair, ACC Accreditation Committee), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee funded by Boehringer Ingelheim; AEGIS-II executive committee funded by CSL Behring), Belvoir Publications (Editor in Chief, Harvard Heart Letter), Duke Clinical Research Institute (clinical trial steering committees, including for the PRONOUNCE trial, funded by Ferring Pharmaceuticals), HMP Global (Editor in Chief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (Guest Editor; Associate Editor), K2P (Co-Chair, interdisciplinary curriculum), Level Ex, Medtelligence/ReachMD (CME steering committees), MJH Life Sciences, Population Health Research Institute (for the COMPASS operations committee, publications committee, steering committee, and USA national co-leader, funded by Bayer), Slack Publications (Chief Medical Editor, Cardiology Today's Intervention), Society of Cardiovascular Patient Care (Secretary/Treasurer), WebMD (CME steering committees); Other: Clinical Cardiology (Deputy Editor), NCDR-ACTION Registry Steering Committee (Chair), VA CART Research and Publications Committee (Chair); Research Funding: Abbott, Afimmune, Amarin, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Cardax, Chiesi, CSL Behring, Eisai, Ethicon, Ferring Pharmaceuticals, Forest Laboratories, Fractyl, Idorsia, Ironwood, Ischemix, Lexicon, Lilly, Medtronic, Pfizer, PhaseBio, PLx Pharma, Regeneron, Roche, Sanofi Aventis, Synaptic, The Medicines Company; Royalties: Elsevier (Editor, Cardiovascular Intervention: A Companion to Braunwald's Heart Disease); Site Co-Investigator: Biotronik, Boston Scientific, CSI, St. Jude Medical (now Abbott), Svelte; Trustee: American College of Cardiology; Unfunded Research: FlowCo, Merck, Novo Nordisk, Takeda. All other authors confirm that they have no relevant conflict of interest. MR conceived the idea and designed the study. MR had full access to the data and performed all the statistical analyses with support from CL and HJW. MAM supervised the study and all other authors provided intellectual input in the manuscript writing and revision. HJW and CL contributed equally to the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for Publication
Not applicable.
Availability of Data and Materials
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.