
Abstract
Objective
Access to palliative and end-of-life (EOL) care might be influenced by knowledge, attitudes, and representations of these practices. Socioeconomic factors might then affect what people know about EOL care practices, and how they perceive them. This study aims to compare knowledge, attitudes, and representations regarding EOL practices including assisted suicide, medical assistance in dying, and continuous palliative sedation of adults, according to socioeconomic variables.
Methods
A cross-sectional community-based questionnaire study featuring two evolving vignettes and five end-of-life practices was conducted in Quebec, Canada. Three sample subgroups were created according to the participants’ perceived financial situation and three according to educational attainment. Descriptive analysis was used to compare levels of knowledge, attitudes, and representations between the subgroups.
Results
Nine hundred sixty-six (966) people completed the questionnaire. Two hundred and seventy participants (28.7%) had a high school diploma or less, and 42 participants (4.4%) were facing financial hardship. The majority of respondents supported all end-of-life options and the loosening of eligibility requirements for medical assistance in dying. Differences between subgroups were minor. While respondents in socioeconomically disadvantaged subgroups had less knowledge about EOL practices, those with lower educational attainment were more likely to be in favor of medical assistance in dying, and less likely to favor continuous palliative sedation.
Conclusions
People living with situational social and economic vulnerabilities face multiple barriers in accessing health care. While they may have poorer knowledge about EOL practices, they have a positive attitude towards medical assistance in dying and assisted suicide, and a negative attitude towards continuous palliative sedation. This highlights the need for future research and interventions aimed at empowering this population and enhancing their access to EOL care.
Keywords
Introduction
According to the WHO, the goal of palliative is to ensure the quality of life and comfort of people with a life-threatening illness through the relief of suffering, as well as other physical, psychosocial, or spiritual problems. 1 EOL care is part of palliative care and is provided when death is imminent. It includes medical assistance in dying (MAID) a and support for the bereaved. 3 Access to quality palliative and EOL care is a right for everyone who needs it, 1 but many studies have shown that people who have multiple social and economic vulnerability factors, such as financial hardship and low levels of education, experience barriers to receiving these services, even in developed countries.4–6 They are more at risk for physical, psychological, and social problems, which are associated with health disparities. 7 In Canada, 10.1% of households face financial hardship, 8 8% of adults aged 25 to 64 years do not hold a high school diploma9 and 48% of adults have literacy skills lower than grade 12, which negatively affects their capacity to function at both personal and professional levels. 10
In the Canadian province of Quebec, MAID was legalized in 2015 through the Act Respecting End-of-Life Care, 11 which also regulates continuous palliative sedation b and advance medical directives. It also reiterates core elements such as the right to palliative care for any person whose condition requires it, the right to withdraw and withhold life-sustaining treatments even if it leads to death, and the obligation for health care professionals to maintain open and frank communication about all EOL options. 11
A Canadian retrospective study comparing the socioeconomic situation of decedents who received MAID, and those who did not, conclude that those with a higher income, who were married, and those who were younger, were more likely to receive MAID. However, according to the researchers, whether this finding reflects a lower desire for MAID or a lack of access to EOL care options in lower socioeconomic groups is not clear. 13 Many factors may influence knowledge about palliative and EOL care options. It has been shown that people with a lower level of education, lower income, perceived poor levels of health, lower levels of social activity, or who are part of a minority group, have less knowledge about palliative care and are less likely to resort to it14–20. Age could also affect one's preferences toward EOL decision-making, as younger adults prefer to be more involved in treatment decisions compared to older adults. 21 Having cancer and being confronted with the possibility of death could also possibly impact preferences for EOL options. 22 Attitudes toward palliative and EOL care could be influenced by knowledge of these practices, which helps form opinions and perceptions about them. 16 Moreover, having better knowledge and a favorable attitude towards palliative and EOL care could be a predictor of the intention to request such care. 23 The many barriers to accessing health care for people facing situational social and economic vulnerability could contribute to their lack of awareness about these services.4,24
This study aims to assess the association between perceived financial situation and level of education with knowledge, attitudes, and representations regarding different EOL practices. The main hypothesis was that persons facing financial hardship or those with a low level of education would have less knowledge about EOL practices, would have more negative attitudes towards them, and would have different perceptions about EOL and MAID.
Conceptual Model and Main Concepts
According to the health literacy model, 25 literacy is influenced by determinants like education and living conditions and impacts one's access to health information and services. Death literacy, which refers to a set of knowledge and skills enabling one to understand, act on, and make informed decisions on EOL options, 26 includes four functionalities: knowledge, skills, experiential knowledge, and social action.
In this study, knowledge is defined as an understanding of facts, information, and skills obtained through experience or education. 27 Attitude is defined as a feeling or an opinion about something or someone, or a way of behaving that is caused by it. 28 Representation is conceptualized as an organized and structured set of opinions, attitudes, beliefs, and information. 29
This model guided the study's hypotheses, the choice of variables, the analysis, and data interpretation.
Methods
Design
A community-based cross-sectional questionnaire study was carried out in the province of Quebec, Canada, as part of a larger study.
Population
Participants were part of the general population, 18 years of age or older, and able to read French or English. The recruitment strategy targeted residents of the province of Quebec, but it was not part of the inclusion criteria.
Data Collection
Data was collected between October 24th, 2019, and February 1st, 2020. The recruitment strategy included active (paid-for ads targeting the population of interest 30 ) and passive Facebook advertising, Twitter, posters, and partnerships with regional and provincial not-for-profit organizations tied to the subgroups of interest, as well as community gatekeepers. Participants self-screened their eligibility and then self-administered the questionnaire online.
Questionnaire
The bilingual (French and English) questionnaire was adapted from previous studies 31 and featured three sections. The first section introduced two evolving vignettes (Appendix 1). The first vignette involved a terminal cancer patient who could consent to his health care choices, while the second was about a patient with dementia who had lost her capacity to consent. This first section aimed to assess participants’ knowledge and attitudes concerning five EOL practices: an order protocol for distress c , treatment withholding d , assisted suicide, MAID, and continuous palliative sedation. The two latter practices were introduced in both vignettes. For each vignette, questions about knowledge centered around whether the described practice corresponded with MAID and whether it was legal in the province of Quebec at the time of the study. Then, participants indicated the acceptability of the practice within the described context using 5-point Likert scales (completely acceptable/completely unacceptable). They also indicated whether they would hypothetically request MAID and continuous palliative sedation for themselves in the described scenario using 5-point Likert scales (definitely/definitely not). The second section assessed their representations using 12 statements regarding EOL and current and potential requirements for MAID using 5-point Likert scales (strongly agree/strongly disagree). Finally, the third section was comprised of socio-demographic questions: age, gender, educational attainment, financial situation, importance of religion, and perceived levels of health.
Following best practices in questionnaire validation, 34 the content validity of the questionnaire was assessed by 10 palliative care experts, including doctors, nurses, ethicists, and a social worker. It was then pre-tested for acceptability and usability with a convenience sample of 11 members of the target population, those living in a situation of socioeconomic vulnerability. Iterative phases of modification, simplification, and validation were carried out until a unanimous version was reached.
Data Analysis
Answers to the questions about knowledge were converted into a dichotomous variable (correct answer (1) or incorrect answer (0)), then tallied up for a maximum score of 14. Responses relating to attitudes were clustered into three categories (favorable, unfavorable, or neutral), as were responses relating to representations (agree, disagree, or neutral).
Three subgroups were created according to the participants’ perceived financial situation: 1) poverty (poor or very poor); 2) income sufficient to meet basic needs; 3) financially comfortable (income adequate to meet all their needs).
Three subgroups were created according to educational attainment: 1) high school diploma or less; 2) college degree (pre-university); 3) university degree.
The mean knowledge score was calculated for each subgroup and all participants. Since the data distribution was skewed, a Kruskal-Wallis test was performed to identify differences between subgroups. Chi-square statistics were used to test the relationship between financial situation, attitudes, and representations, and between educational attainment, attitudes, and representations. Missing data was rare (from 0.2% to 5% across questionnaire items) and excluded from all analyses. All results were interpreted at the 0.05 significance level. Analyses were conducted using IBM SPSS v27.
Ethical Considerations
This multicenter project was approved by the Quebec Heart and Lung Research Centre (approval number MP-10-2019-3237), and by the research ethics boards of the partner organizations. Upon submission of the questionnaire, participants authorized the research team to gather their information. Questionnaires were anonymous and were automatically attributed ID numbers. Data was stored in the secure servers of the research center.
Results
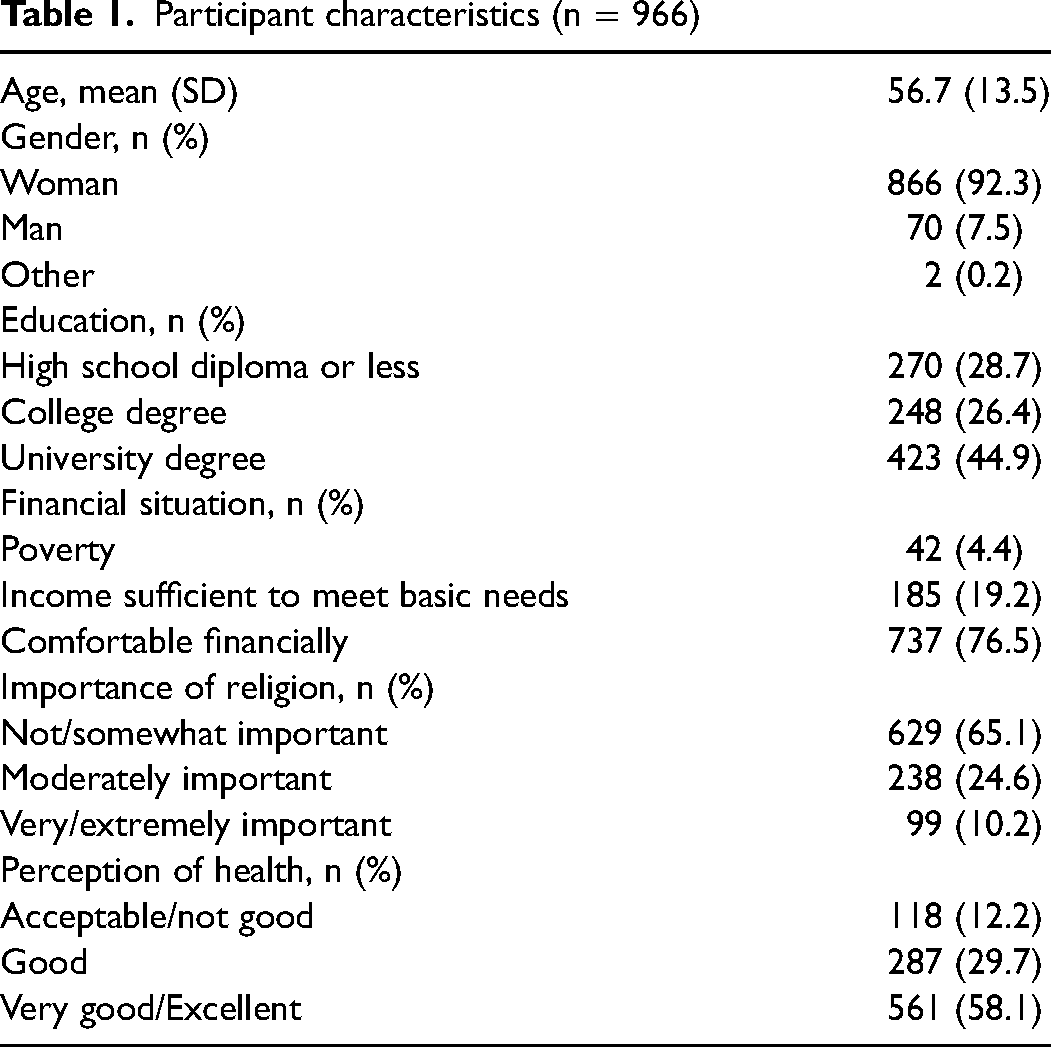
Overall, 966 participants were included in the analyses (80% response rate). Most were women (92.3%) aged between 19 and 90 years. More than a quarter (28.7%) had completed a high school diploma or less. Forty-two (42) participants (4.4%) identified that they faced financial hardship (Table 1). All (100%) were living in the province of Quebec.
Participant characteristics (n = 966)
Knowledge
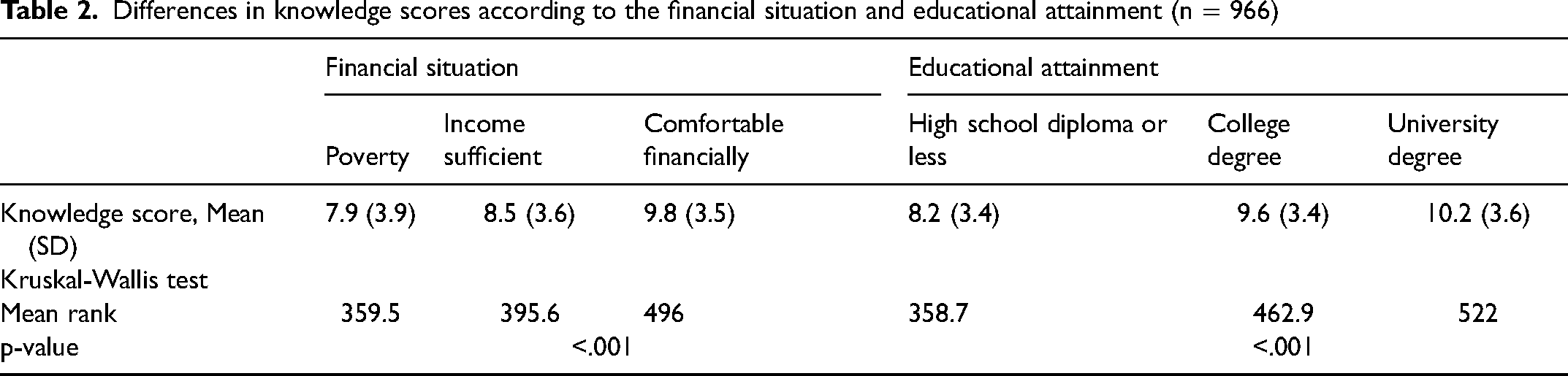
The mean overall knowledge score was 9.5 out of 14 (SD = 3.6). The Kruskal-Wallis test showed significant differences in knowledge between financial situation and educational attainment subgroups. Participants facing financial hardship and those who had completed high school or less had, on average, lower knowledge scores (Table 2).
Differences in knowledge scores according to the financial situation and educational attainment (n = 966)
Attitudes
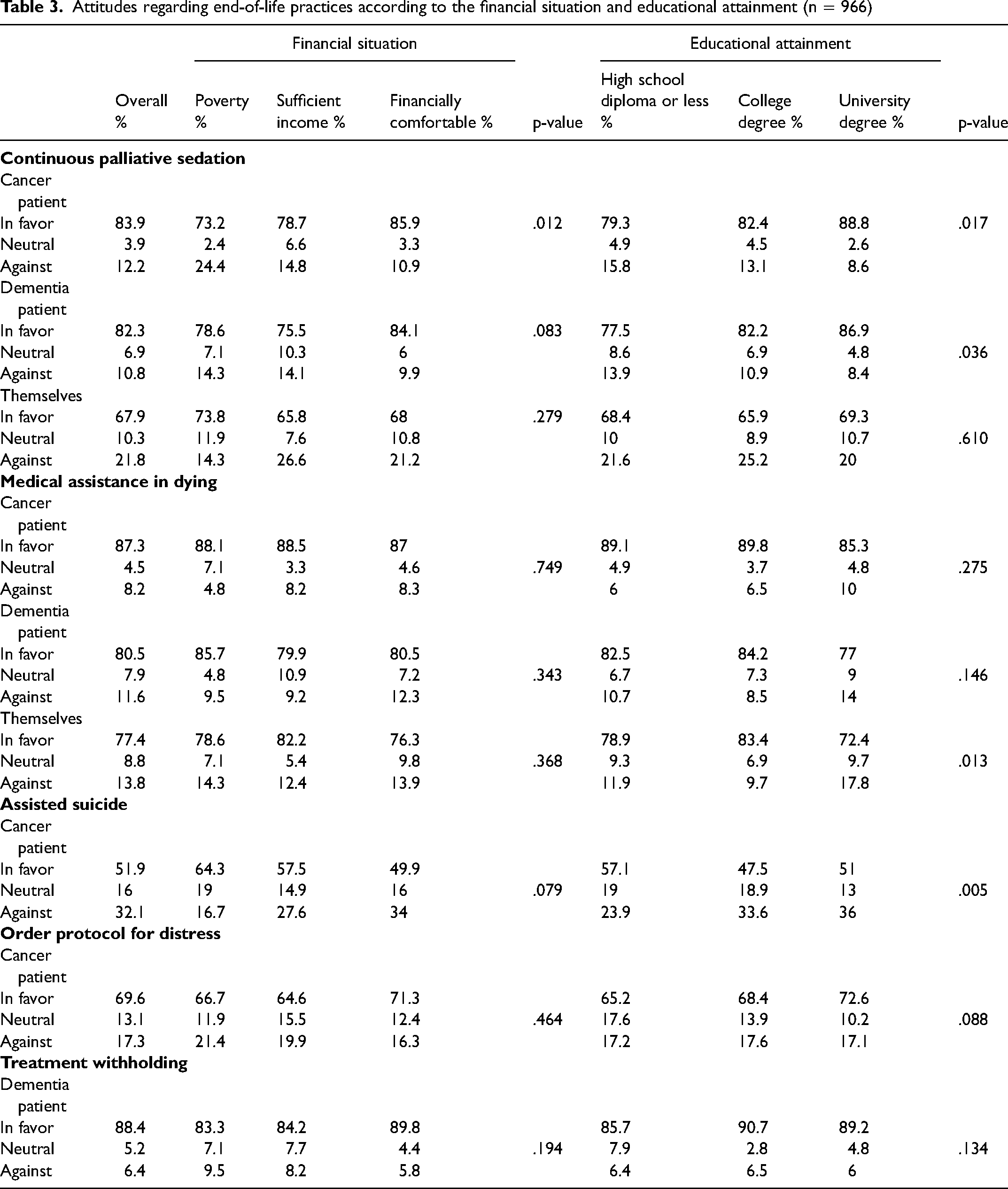
Overall, a large majority of respondents had favorable attitudes towards continuous palliative sedation and MAID for both vignettes. In the vignette about the cancer patient, more participants facing financial hardship were against continuous palliative sedation (p = .012). In the same vignette, people with lower educational attainment were less favorable to continuous palliative sedation (p = .017), and more favorable to assisted suicide (p = .005). Participants with a college degree considered it more likely to seek MAID for themselves (p = .013). People with lower educational attainment were also less favorable to continuous palliative sedation in the vignette about the dementia patient (p = .036) (Table 3).
Attitudes regarding end-of-life practices according to the financial situation and educational attainment (n = 966)
Representations Regarding End-of-Life
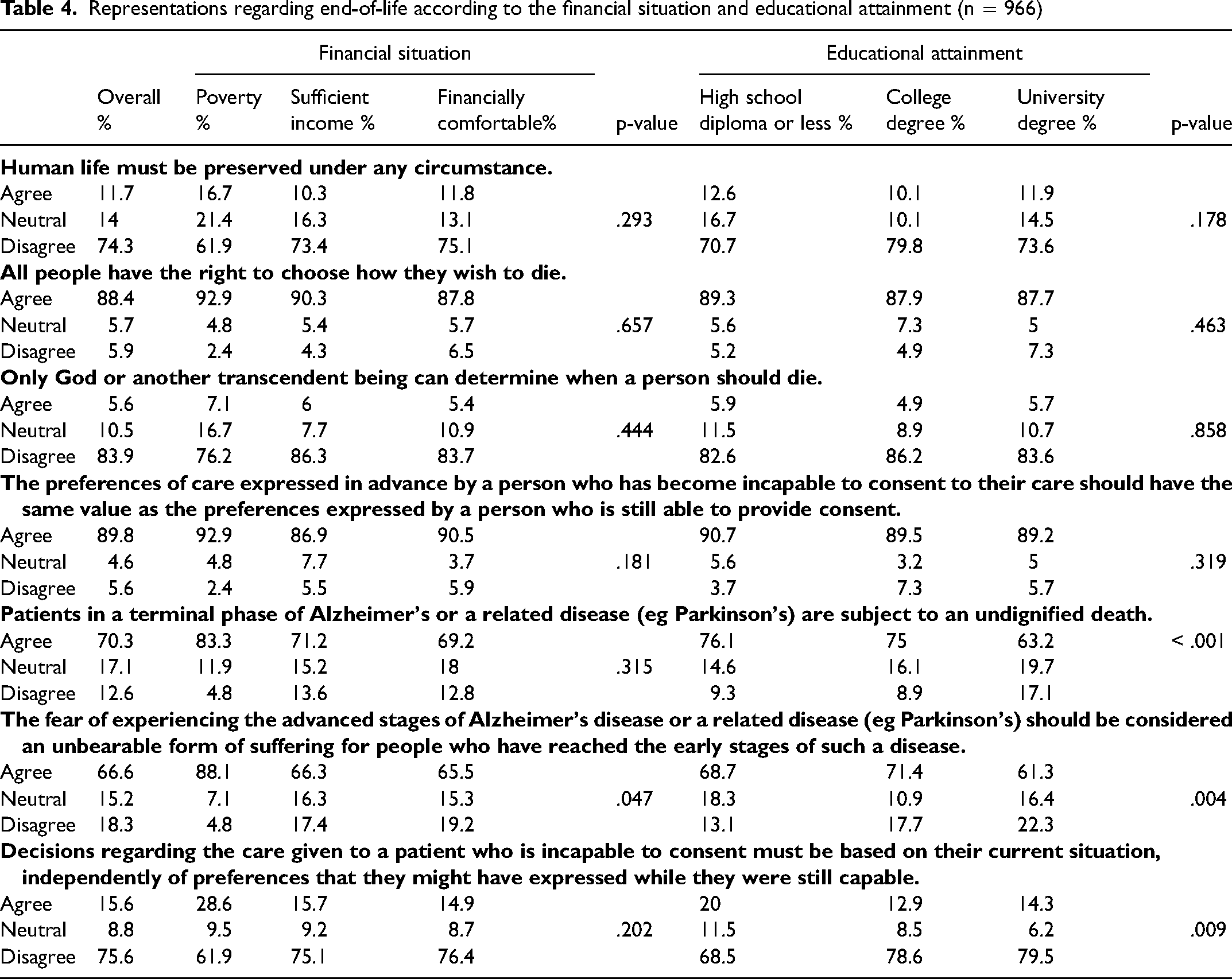
Most participants agreed with statements featuring a positive representation of MAID, such as “All people have the right to choose how they wish to die” (88.5%), and only a very small minority agreed with the statements against the principles guiding MAID, such as “Only God or another transcendent being can determine when a person should die” (5.6%).
Among participants facing financial hardship, 88.1% (n = 37) agreed with the statement “The fear of experiencing the advanced stages of Alzheimer's disease or a related disease (eg Parkinson's) should be considered an unbearable form of suffering for people who have reached the early stages of such a disease”, compared to 66.3% for people with a sufficient income and 65.5% for financially comfortable participants (p = . 047). More participants with a high school diploma or less agreed with the same previous statement (p = .004) but agreed less with the statement “Patients in a terminal phase of Alzheimer's or a related disease (eg, Parkinson's) are subject to an undignified death” (p < .001). However, more participants with a high school diploma or less (20%) agreed with the statement “Decisions regarding the care given to a patient who is incapable to consent must be based on their current situation, independently of preferences that they might have expressed while they were still capable” than participants with a university degree (14.3%) (p = .009) (Table 4).
Representations regarding end-of-life according to the financial situation and educational attainment (n = 966)
Representations Regarding Requirements for MAID
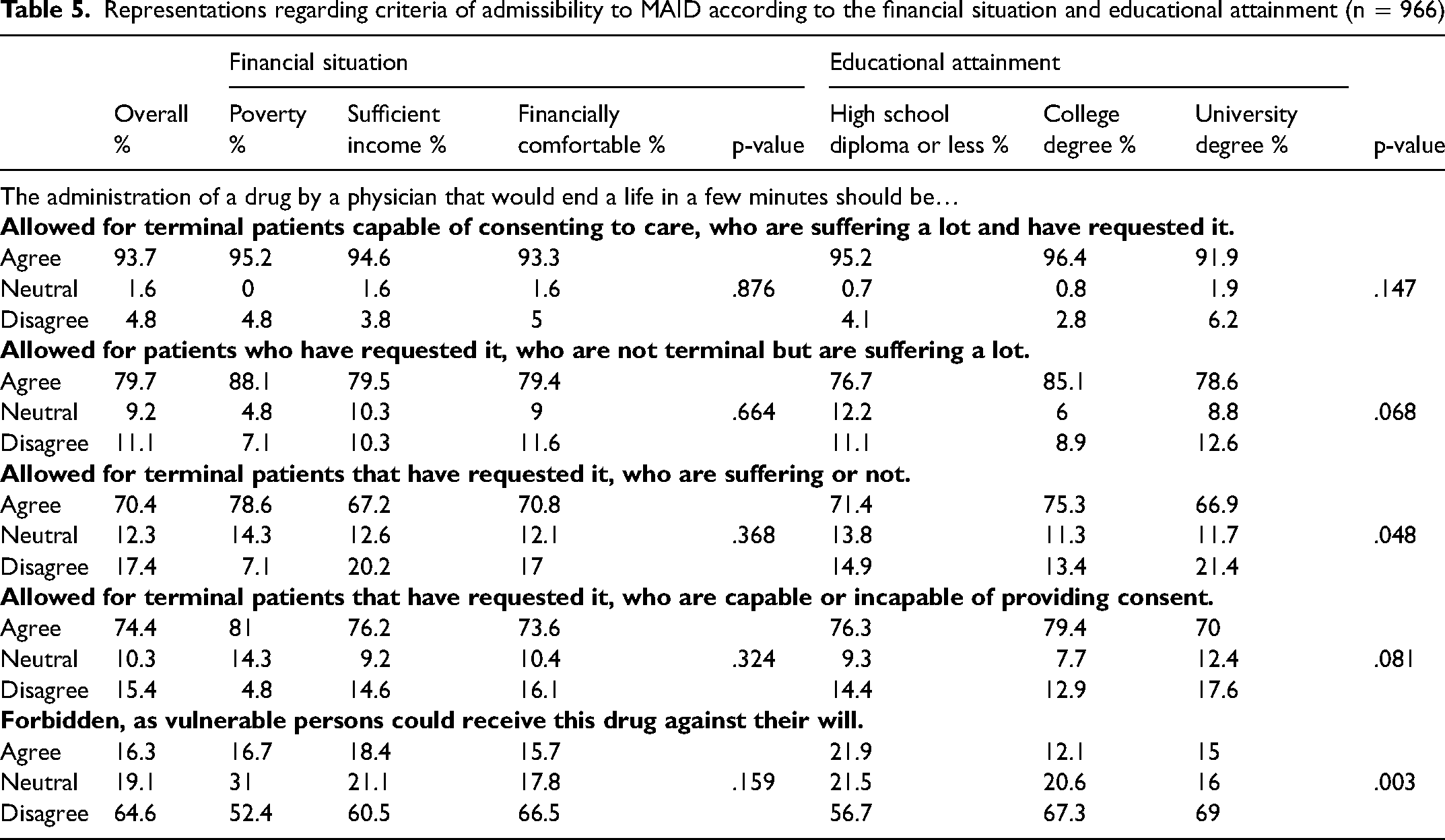
Most participants agreed with statements in support of more flexible requirements for MAID. Participants with a high school diploma or less education (71.4%) and with a college degree (75.3%) were more likely to agreed that MAID should be allowed for all EOL patients who request it, independently of their suffering (p = .048), than those with a university degree (66.9%). Of those with a lower level of education, more were in favor of prohibiting this treatment option because of the perceived risk that vulnerable people would receive it against their will (p = .003) (Table 5).
Representations regarding criteria of admissibility to MAID according to the financial situation and educational attainment (n = 966)
Discussion
This community-based cross-sectional questionnaire study aimed to assess the influence of perceived financial situation and level of education on knowledge, attitudes, and representations of different EOL practices using evolving vignettes.
Main Findings
Consistent with the initial hypothesis and the literacy conceptual framework, there was a relationship between financial situation and level of education, and participants’ knowledge of different EOL practices. Indeed, people facing financial hardship had less knowledge about the legality of these practices and what constitutes MAID, which is consistent with previous studies.15,18,35,36 A lower level of education has also been associated with less knowledge about EOL practices in a few studies.35,37–39 This lack of awareness of EOL options constitutes one of many barriers to accessing these services. 36 Paradoxically, it could also be a result of these barriers since people facing situational social and economic vulnerability have less access to a family doctor and more generally to primary care. 40
Regarding attitudes and representations, a large majority of respondents supported the availability of all EOL options mentioned, in both scenarios. There was also overwhelming support for loosening of eligibility requirements for MAID, which was also observed in the qualitative interviews conducted as part of the larger study of which this sub-study is part, 41 and in a recent Canadian qualitative study. 36 In three-quarters of the comparisons, responses did not vary significantly by educational or financial status. Where levels of support did vary according to these factors, the differences between groups were numerically small (usually <15%) and the prevailing opinion was the same in each group. Nevertheless, participants with a lower level of education had a more positive attitude towards MAID and assisted suicide, and a more negative attitude towards continuous palliative sedation, which partly invalidates our hypothesis that they would have a negative attitude towards EOL practices in general. They were also more likely to believe MAID should be allowed independently of the patient's suffering or ability to consent. Paradoxically, they were also more prone to agree that it should be banned, as vulnerable persons could receive it against their will. According to an American qualitative study, homeless adults fear becoming a burden on others and losing their independence, and consider that living a life without quality is considered meaningless, 42 which could partly explain their positive attitude toward MAID. However, a Canadian retrospective study comparing the socioeconomic situation of decedents who received it, and those who did not, found that having a high income was associated with higher use of MAID. 13 Another Canadian study found that more people with low socioeconomic status requested it, however, more than half of participants who requested MAID did not receive it. 43 Therefore, it raises the question of whether there is truly equal access to all palliative and end-of-life options, as promoted by the Quebec Act Respecting End-of-Life Care. 11 The hypothesis that people facing socioeconomic vulnerability would resort to MAID or assisted suicide because of reduced access to palliative care or a generalized ignorance of EOL options has been raised previously. 44 Our findings suggest that these individuals may have nuanced opinions, as they are less favorable towards palliative care practices and more favorable towards MAID.
Implications
According to the Quebec Act Respecting End-of-Life Care, health care providers must ensure open and frank communication with patients while respecting their autonomy of choice. 11 Our study suggests that persons facing situational social and economic vulnerabilities could have less knowledge about palliative and EOL care, and consequently lower death literacy, at least regarding the knowledge component. This could be a obstacle to understanding EOL options and making informed decisions. 26 It highlights the importance of adapting information, forms, and educational tools to a lower level of literacy, which is consistent with results from a previous study. 39
However, several barriers to accessing health care coexist for persons facing situational social and economic vulnerabilities, such as a reluctance to seek medical care following negative experiences with providers 45 and prioritization of daily survival over access to healthcare. 4 Health care providers may also have difficulty identifying vulnerable persons who could benefit from palliative care 4 and can stigmatize them, especially those using substances.45,46 Navigating the health and social services system is also complex, and vulnerable people can slip into “service cracks”. 4 Health care and social services providers should advocate for better access to all palliative and EOL care options for vulnerable populations, 47 considering that barriers to accessing health care may contribute to reduced access to health care information. Future research concerning death literacy could focus on the potential of compassionate communities to empower people with terminal diseases at the EOL. 48
Strengths and Limitations
This is the first study conducted specifically on this topic in Canada. Its main strength is its simultaneous interest in the knowledge, attitudes, and representations of the adult population in the face of EOL practices and death. Rigorous pre-testing of the questionnaire among experts and the targeted population also contributed to the study's internal validity.
However, due to the univariate analyses, the significance of some results may be due to relationships between variables. This will be explored in an upcoming article using the same dataset. Confounding factors such as being older, having cancer, being a social media user, or being part of not-for-profit organizations could also have influenced the results.21,22,49 Also, the sample was not representative of the general population, since participants recruited from social media are often younger women, more educated, and with a higher income. 49 Moreover, women are the predominant formal and informal caregivers for seriously ill and dying persons,50,51 and are more likely to be aware of palliative options and more likely to choose palliative care over curative treatments at the EOL. 52 Only 4.4% of participants were experiencing poverty, which may have affected the generalizability of the results in this demographic group. Socioeconomic vulnerability can limit potential participants’ ability to be aware of opportunities to participate in research projects, and can reduce their ability to be meaningfully involved in the research process.53,54 Difficulty in accessing and using technology for people in situational social and economic vulnerability may also limit their access to online surveys. 55 Finally, financial situation and educational attainment were self-proclaimed, which could bias the results.
Conclusion
We found that a large majority of respondents supported the availability of all palliative care options in a variety of EOL scenarios. In some situations, small differences in attitudes and knowledge were found among socioeconomic groups. The results of this study suggest that persons facing situational social and economic vulnerabilities have different levels of knowledge, and different attitudes towards palliative and EOL care, when compared to the rest of the population. This highlights the need for future research to investigate the causes of these disparities in knowledge, attitudes and representations regarding EOL practices, and to propose ways to reduce this knowledge gap. To better understand these variables, a study involving a larger representative sample of the population of interest or using a qualitative approach could be helpful.
Supplemental Material
sj-docx-1-pal-10.1177_08258597221131658 - Supplemental material for Do Socioeconomic Factors Influence Knowledge, Attitudes, and Representations of End-of-Life Practices? A Cross-Sectional Study
Supplemental material, sj-docx-1-pal-10.1177_08258597221131658 for Do Socioeconomic Factors Influence Knowledge, Attitudes, and Representations of End-of-Life Practices? A Cross-Sectional Study by A. Bérubé, D. Tapp, S. Dupéré, A. Plaisance, G. Bravo, J. Downar and V. Couture in Journal of Palliative Care
Footnotes
Acknowledgment
We want to thank all participants who took the time to fill out the survey questionnaire, as well as the participants and experts who took part in the validation and translation of the questionnaire. A sincere thanks to Sandra Lynn Hopps and Annie-Claude Laurin for their diligent proofreading of this paper.
Author Contributions
DT, GB, AP, JD, SD, and VC participated in the design and validation of the questionnaire. AP and DT collected the data. AB and DT analyzed the data and interpreted the results. AB drafted the paper. DT, SD, AP, JD, and VC revised the article critically for important intellectual content. All authors approved the final version of the article to be published and take public responsibility for appropriate portions of the content.
Data Availability Statement
The study data is available from the main researcher upon request:
Diane Tapp, Professor, Faculty of Nursing, Laval University, Qc. Canada.
418 656-2131 (407930), diane.tapp@fsi.ulaval.ca
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Réseau québécois de recherche en soins palliatifs et de fin de vie (RQSPAL). The funding had no influence on the design, data collection, analysis, and interpretation, nor the dissemination of the results of this study.
Supplemental material
Supplemental material for this article is available online.
Notes
Appendix 1. Vignettes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.