
Abstract
Objective
People living with dementia often have high care needs at the end-of-life. We compared care delivery in the last year of life for people living with dementia in the community (home or assisted living facilities [ALFs]) versus those in skilled nursing facilities (SNFs).
Methods
A retrospective study was performed of older adults with a dementia diagnosis who died in the community or SNFs from 2013 through 2018. Primary outcomes were numbers of hospitalizations and emergency department visits in the last year of life. Secondary outcomes were completed advance care plans, hospice enrollment, time in hospice, practitioner visits, and intensive care unit admissions.
Results
Of 1203 older adults with dementia, 622 (51.7%) lived at home/ALFs; 581 (48.3%) lived in SNFs. At least 1 hospitalization was recorded for 70.7% living at home/ALFs versus 50.8% in SNFs (P < .001), similar to percentages of emergency department visits (80.2% vs 58.0% of the home/ALF and SNF groups, P < .001). SNF residents had more practitioner visits than home/ALF residents: median (IQR), 9.0 (6.0-12.0) versus 5.0 (3.0-9.0; P < .001). No advance care plan was documented for 12.2% (n = 76) of the home/ALF group versus 4.6% (n = 27) of the SNF group (P < .001). Nearly 57% of SNF residents were enrolled in hospice versus 68.3% at home/ALFs (P < .001). The median time in hospice was 26.5 days in SNFs versus 30.0 days at home/ALFs (P = .67).
Conclusions
Older adults with dementia frequently receive acute care in their last year of life. Hospice care was more common for home/ALF residents. Time in hospice was short.
Introduction
Dementia is a life-limiting illness, and 1 in 3 older adults in the US die with a diagnosis of Alzheimer disease or other dementia. 1 The course of advanced dementia often is marked by severe disability, especially in the last year of life.2,3 Because of functional decline, the last year frequently is spent in a skilled nursing facility (SNF), and approximately two-thirds of dementia-related deaths occur in nursing homes. 4 Many older adults living with dementia have burdensome interventions and care transitions as they approach the end of life. 5 Many do not receive adequate relief of their symptoms, such as pain and neuropsychiatric symptoms.6–11Palliative care is an important part of care delivery for people with life-limiting illness including dementia because it offers opportunities for symptom control, advance care planning (ACP), and psychosocial support. However, people living with dementia have less access to palliative care than patients with other conditions.12,13
Previous study findings have described areas needing improvement; therefore, it is important to explore care at the end of life for people living with dementia. ACP has been identified as a priority in dementia care to help communicate individual goals and preferences for medical treatments and identify surrogate decision-makers. 14 For older adults living with dementia, ACP rates vary widely, and ACP often is addressed only at times of crisis and is poorly communicated.15–18 Ensuring access to hospice care for persons who qualify for and will benefit most from hospice is another important part of end-of-life care. 19 Although strides forward have been made in this area of dementia care, room for improvement still exists. Of Medicare beneficiaries receiving hospice care in 2017 through 2018, approximately 15% had a principal diagnosis of dementia, increased from 9% in 2005. 20 For nursing home residents living with advanced dementia, hospice access tripled between 1999 and 2006, such that 42% had access to hospice in 2006. 21 Dementia is the condition associated with the longest time spent in hospice (median, 55 days), 20 although this period still falls below the 6-month eligibility benefit for hospice.
An understanding of care delivery for people living with dementia as they approach the end of life is needed to direct palliative care delivery and health system planning across our practice, which covers community and skilled nursing settings. In this study, we aimed to describe acute care utilization, ACP completion, and hospice access for people living with dementia over the last year of life and to compare care received in the community (home or assisted living facilities [ALFs]) with that in SNFs, which has not been evaluated in this community. We plan to use the information gained to identify areas of need and guide palliative care practice change within our primary care practice to ultimately improve care for people living with dementia in all settings.
Methods
Study Design and Population
A retrospective cohort study was conducted of decedents with a dementia diagnosis who were followed up in our primary care practice before they died. Our practice involves primary care practitioners in family medicine and community internal medicine who provide longitudinal care to patients in the community and in 11 SNFs in the Rochester, Minnesota, area. Patients were eligible for inclusion in the study if they had a dementia diagnosis, were 65 years or older at diagnosis, were empaneled in our health care network, and died during the study period from December 31, 2013, through December 31, 2018. Patients living in the community (home/ALF) had an assigned primary care practitioner in the ambulatory care practice and had visited a practitioner within the past 3 years. SNF residents were empaneled to clinicians in our practice, who provided regulatory and acute care visits as needed. We excluded anyone who did not give electronic health record (EHR) research authorization.
Outcome Measures
The primary outcomes were the number of hospitalizations and the number of emergency department (ED) visits in the last year of life. Secondary outcomes were ACP documentation, hospice enrollment, time spent in hospice care, the number of practitioner visits, and the number of intensive care unit (ICU) admissions in the final year. We recorded ACP as the last advance directive or provider orders for life-sustaining treatment (POLST), if any, on record and the last ACP note, if any, in the EHR. For each person, we recorded if there was a POLST filed in the EHR, an advance directive in the EHR, and a separate ACP clinical note. Our EHR has an option to create a distinct ACP note, which allows a provider to document ACP discussions and to fill in the designated decision-maker and preferences for end-of-life care, which are then easily accessed by treating providers later.
Data Collection
Data were abstracted from the EHR by a certified clinical research coordinator, who documented ACP, practitioner visits, ICU admission, and hospice enrollment. Demographic data were abstracted from administrative data using Advanced Cohort Explorer, an institutional web-based software tool, and from the EHR; data included the age at death, sex, race (self-report), and marital status (divorced, legally separated, married, single, widowed, or missing/unknown). The burden of comorbid health conditions was quantified with the Charlson Comorbidity Index calculated 1 year before death. Data on comorbid conditions were obtained by using diagnosis codes obtained from 5 years earlier (International Classification of Diseases, Ninth Revision [ICD-9] and International Classification of Diseases, Tenth Revision [ICD-10] codes). 22 Dementia was classified using 30 ICD-9 and 14 ICD-10 diagnosis codes. We recorded the dementia subtypes of Alzheimer disease; Lewy body disease; vascular; mixed Alzheimer and Lewy body, mixed Alzheimer and vascular; mixed Alzheimer, Lewy body, and vascular; and dementia type not specified clinically.
SNFs were defined as licensed nursing homes receiving federal funding as SNFs. Practitioners in our health care system cover 11 area SNFs. We defined ALF according to the Minnesota state statutes' 23 definition of a facility that provides accommodation and assisted living services to 1 or more older adults and identified ALF residence by using known addresses of area ALFs. The cohort living at home was identified by residential address.
Statistical Analysis
Demographic and clinical variables were compared between groups using t tests or χ2 tests as appropriate. Kruskal-Wallis tests were used to compare medians. Univariate and multivariate Poisson regression were used to evaluate associations between variables of interest and hospitalization in the last year of life. The regression models were subset by residential location: home/ALF or SNF. Covariates included in the models were age at diagnosis, sex, marital status (married vs unmarried), race (other and unknown vs White), Charlson Comorbidity Index score, presence of a POLST, completion of ACP, and hospice status. The results from the Poisson regression models were reported using incidence rate ratios and 95% CIs, and both univariable (unadjusted) and fully adjusted results were reported. P values less than.05 were considered significant. Analyses were performed in SAS version 9.4 (SAS Institute Inc).
Ethical Considerations
This study was deemed exempt by the Mayo Clinic Institutional Review Board because it contained data from decedents only. We conducted the research within the ethical framework of the Declaration of Helsinki. 24 The relevant EQUATOR (Enhancing the Quality and Transparency of Health Research) Network reporting guidelines were followed.
Results
Demographic and Clinical Characteristics
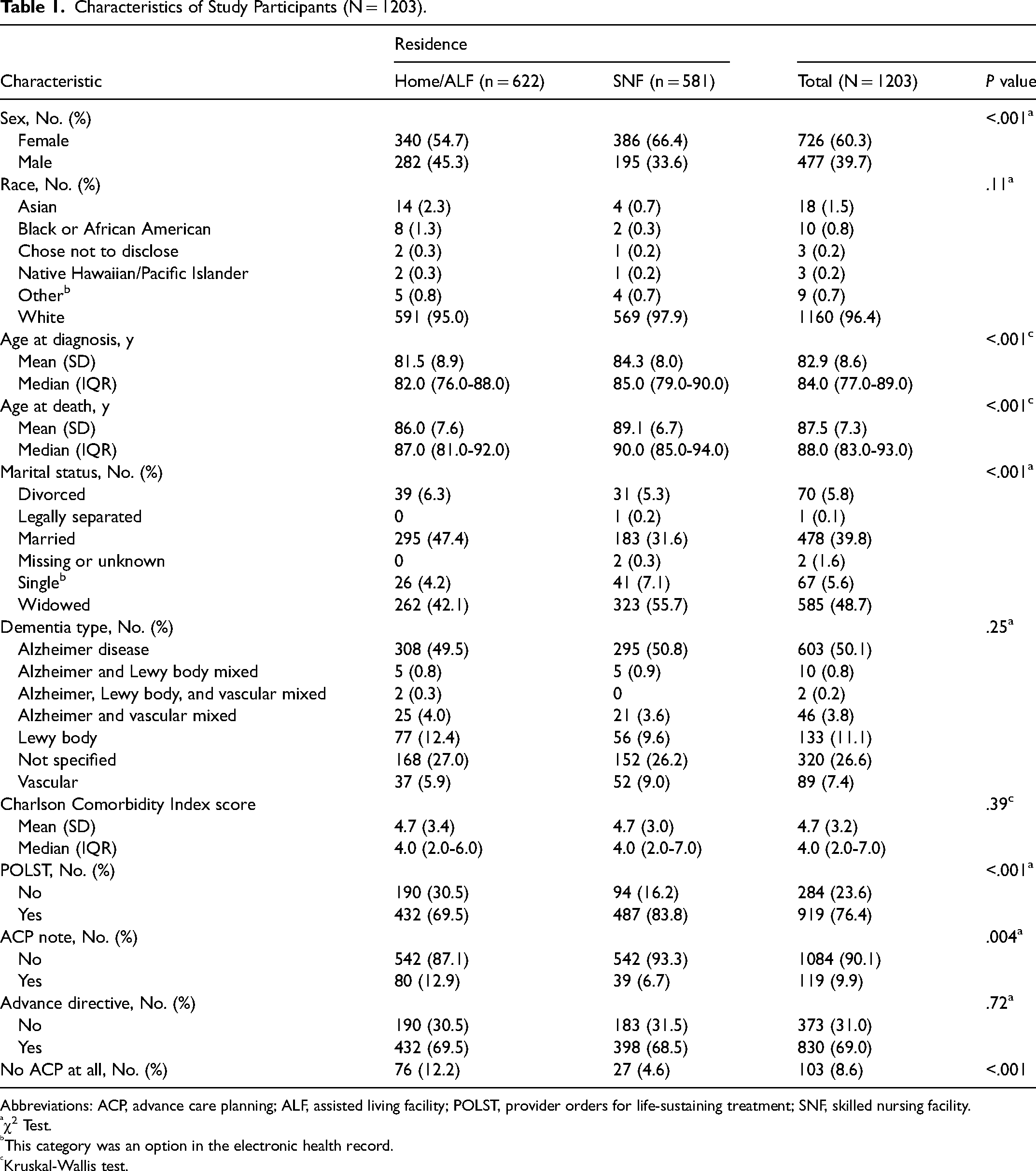
Initially, 1978 decedents were identified who had an ICD diagnosis code for dementia. Of the 1978 older adults whose records were reviewed, 775 did not meet study criteria (had a primary care practitioner elsewhere or an alternate diagnosis code) and were excluded, leaving 1203 study participants. Among the 1203 remaining, 726 were women (60.3%). In total, 581 participants (48.3%) were living in SNFs; in the community (n = 622), 382 participants (31.8%) lived in an ALF, 238 (19.8%) lived at home, and 2 (0.002) lived in a group home. Residents of SNFs were older at death, with a median age of 90 (IQR, 85.0-94.0) years versus a median of 87 (IQR, 81.0-92.0) years for the home/ALF group. Older adults living at home/ALFs were more likely to be married (47.4%; n = 295) than those in SNFs (31.6%; n = 183). In the entire cohort, the most common dementia subtype was Alzheimer disease (50.1%; n = 603). No significant difference was found between groups in Charlson Comorbidity Index scores. Patient characteristics are shown in Table 1.
Characteristics of Study Participants (N = 1203).
Abbreviations: ACP, advance care planning; ALF, assisted living facility; POLST, provider orders for life-sustaining treatment; SNF, skilled nursing facility.
χ2 Test.
This category was an option in the electronic health record.
Kruskal-Wallis test.
Outcomes
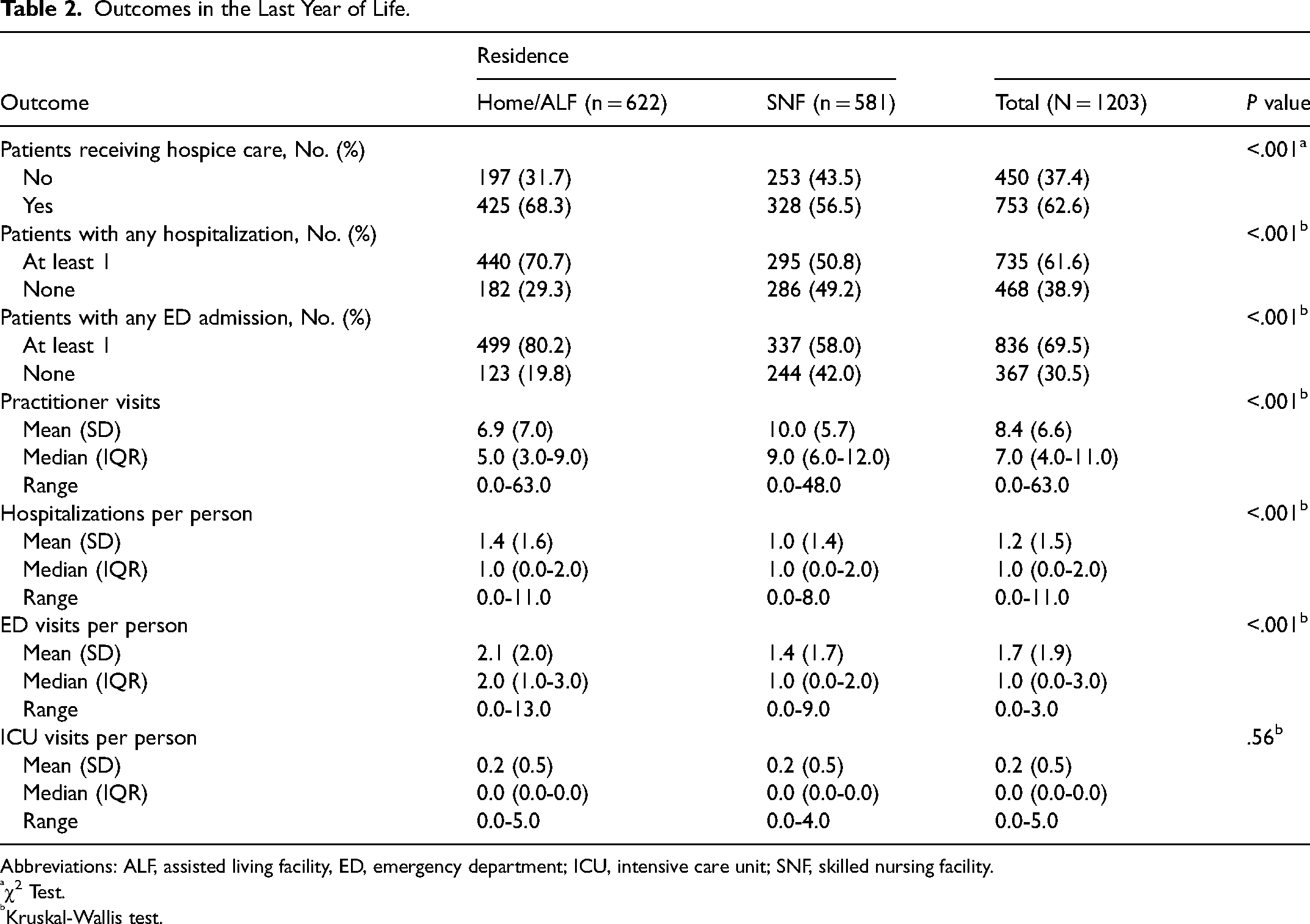
Home/ALF residents had significantly more hospitalizations and ED visits in the last year of life: 70.7% had at least 1 hospitalization versus 50.8% of the SNF group (P < .001), and 80.2% had at least 1 ED visit versus 58% of the SNF group (P < .001). In both groups, the number of hospitalizations and ICU and ED visits per person was low (Table 2).
Outcomes in the Last Year of Life.
Abbreviations: ALF, assisted living facility, ED, emergency department; ICU, intensive care unit; SNF, skilled nursing facility.
χ2 Test.
Kruskal-Wallis test.
The SNF group had significantly more practitioner visits in the last year of life than the home/ALF group (median [IQR], 9.0 [6.0-12.0] vs 5.0 [3.0-9.0], respectively; P < .001). Home/ALF residents were more likely to be enrolled in hospice than those living in SNFs (68.3% vs 56.5%, P < .001; Table 2). The median time in hospice care was 30.0 days for those living at home/ALFs and 26.5 days for those living in SNFs (P = .67).
Results of ACP documentation are shown in Table 1. Residents of SNFs were significantly more likely to have a POLST (83.8% vs 69.5% of the home/ALF group, P < .001). No significant difference was found between groups in the percentage who had completed advance directives on record (69.5% of the home/ALF group, 68.5% of the SNF group; P = .72). When we studied how many participants had no ACP documentation of any kind (no advance directive, POLST, and ACP note in the EHR), 27 (4.6%) were SNF residents and 76 (12.2%) were home/ALF residents (P < .001).
In adjusted Poisson regression models to assess predictors of hospitalization (Table 3), male sex, having no ACP documentation at all, or having a higher Charlson Comorbidity Index score increased the likelihood of SNF residents being hospitalized in the year before death. For older adults living at home/ALFs, having a higher Charlson Comorbidity Index score and not being in hospice care were associated with a greater likelihood of hospitalization (Table 3).
Predictors of Hospitalization in the Last Year of Life a .
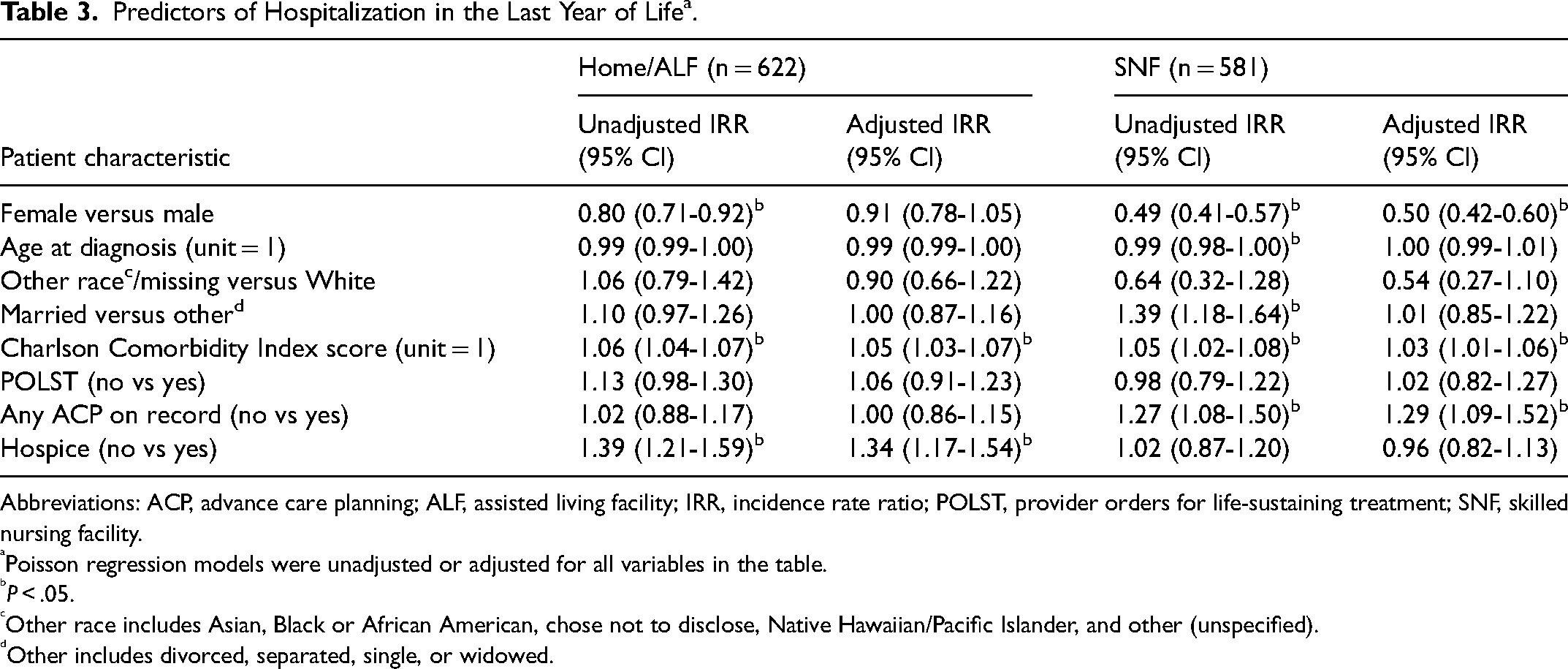
Abbreviations: ACP, advance care planning; ALF, assisted living facility; IRR, incidence rate ratio; POLST, provider orders for life-sustaining treatment; SNF, skilled nursing facility.
Poisson regression models were unadjusted or adjusted for all variables in the table.
P < .05.
Other race includes Asian, Black or African American, chose not to disclose, Native Hawaiian/Pacific Islander, and other (unspecified).
Other includes divorced, separated, single, or widowed.
Discussion
This study of decedents with a dementia diagnosis showed frequent health care contacts in their last year of life. More than 70% of our cohort living at home/ALFs had at least 1 hospitalization and 1 ED visit in their final year. Acute care utilization differed depending on study participants' residential location; the SNF group had more frequent primary care practitioner visits, which included SNF regulatory recertification visits. In conjunction with the frequent health care contact, we did see high rates of ACP documentation overall. However, some room for improvement was still noted, especially for home/ALF residents, 12.2% of whom had no ACP of any kind on record compared with 4.6% of the SNF group. Although the ACP documentation rate was better in the SNF group, the absence of ACP in that group showed an association with hospitalization rate. Furthermore, the time in hospice care was lower than the national figure (median, 55 days) 20 : 30 days for the home/ALF group and 26.5 days for the SNF group. Finally, the Charlson Comorbidity Index score influenced hospitalization rates in both groups.
Previous study results have shown that hospitalization is common in later stages of dementia. In the landmark Choices, Attitudes, and Strategies for Care of Advanced Dementia at the End-of-Life (CASCADE) study of nursing home residents living with advanced dementia, 16% of the cohort was hospitalized. 11 Rehospitalization rates are high for people living with dementia, with one cohort study showing a 30-day rehospitalization rate for people living with dementia of 23%. 25 Among all hospitalized patients discharged to SNFs, a 30-day rehospitalization rate of 18% was found, 26 which highlights the added complexity of caring for patients living with dementia. In our study, home/ALF residents were more likely to have had a hospitalization or ED visit than SNF residents, a finding that may have been influenced by the frequent practitioner visits, high ACP rates for the SNF residents, and potential differences in disease trajectory of older adults living in the community versus in SNFs. We recognize that some of the SNF visits were recertification visits, which are mandated and do inflate the number of practitioner visits. Overall, the number of hospitalizations per resident was low, which in the home/ACP group may have been influenced by participating in our division's homebound programs that target high-risk frail older adults still living in the community. 27 The burden of comorbid conditions was a predictor of hospitalization, as in other studies.28,29
Similar to some previous studies,30,31 our results showed that ACP could have an influence on hospitalization from SNFs; SNF residents who had no ACP documentation were more likely to be hospitalized. Although the evidence of ACP for people living with dementia is limited in the community setting, some positive outcomes were described that support ACP for people living with dementia, primarily those in care homes, notably the resident's improved satisfaction scores with care, improved markers of distress, and reduced acute care utilization.30–33 Data from the Health and Retirement Study showed that advance directives affected care more for patients with advanced dementia in the community than for those in SNFs. 34 In the community, patients with advanced dementia who did not have an advance directive received end-of-life care that was as aggressive as care provided to persons with normal cognition, whereas those with advanced dementia who had an advance directive received much less aggressive care. 34 This difference was not found for persons at early stages of dementia, suggesting the potential impact of timely care discussions on end-of-life care in the community. In the same study, care for nursing home residents living with advanced dementia tended to be less aggressive at the end-of-life regardless of the presence of an advance directive. 34 In a study of practitioners caring for nursing home residents living with advanced dementia, the decision to hospitalize a resident was based on the groundwork laid by ACP but ultimately depended on the resources and comfort levels of the facility staff and the family to respond to the acute event. 35 These findings show the need for adequate resource planning and effective communication.
Published ACP rates for people living with dementia vary widely, with rates ranging from 9% to 71% in memory clinic and primary care cohorts.16,36,37 A national cohort study of Medicare diagnosis codes for ACP for patients with Alzheimer disease and related dementias undergoing surgical procedures showed that just 7.5% (21,754) of 289,428 patients had codes used in billing for ACP, most commonly done postoperatively. 38 Time spent on ACP may be short. Data from the CASCADE study showed that only 50% of health care proxies had spent more than 15 min discussing advance directives on the person's admission to the SNF. 15 Our rates for ACP and for hospice referral are higher than those in many previous studies, which is encouraging. We recognize that at SNF admission in our state, staff members are required to document code status preferences, which may have prompted them to obtain a POLST and so contribute to higher rates in this cohort. However, even with high rates of ACP completion overall, we highlighted some potential areas for improved care: the need to discuss ACP, especially with those who have no ACP documentation on record, and to offer hospice care where appropriate. Primary care and family medicine practitioners provide longitudinal care to their patients and, as such, can establish trust and initiate thoughtful conversations regarding goals of care. Although it is recognized that ACP is important in dementia care, it is not always reflected in completion rates. 39 Currently, limited guidance exists for practitioners on conducting ACP discussions with patients living with dementia. A consensus group in 2018 proposed criteria for these conversations, including starting ACP discussions early and integrating these discussions into daily care. 40
Evidence suggests that barriers to ACP exist at all levels (patient and family, practitioner, health care system); some barriers are time constraints, training, personal beliefs, diagnostic unawareness or uncertainty, and difficulties with prognostication.41–43 Prognostication can prove challenging in dementia care more than for other illnesses because many older adults living with dementia live with substantial debility for years. Commonly, clinicians will use tools such as the Functional Assessment Staging instrument as a prognostic guide. 44 To qualify for hospice, for example, for which practitioners have to estimate a life expectancy of 6 months or less, a person with dementia must be at stage 7 on the Functional Assessment Staging with substantial motor and verbal impairments and have other qualifying conditions in the past year. 45 Although hospice referral rates have increased for patients living with dementia, they remain low. 21 Rates of referral vary widely, with one study showing hospice referral rates for older adults with advanced dementia living in SNFs and at home as low as 5.7% and 10.7%, respectively, 46 and others showing rates in SNF residents and in the community closer to 30%.47,48 Hospice referral rates were higher in our study, but the time spent in hospice was short, a finding that suggests possible missed opportunities for earlier discussions about eligibility or appropriateness.
Our study has strengths and limitations. Strengths included the large sample and the clinical data from a wide range of skilled care facilities and the community setting. Our study had several limitations, however. First, this retrospective study relied on practitioners who recorded cognitive diagnoses in the EHR during the visit. Because dementia diagnosis records in primary care do not reflect the true prevalence of dementia, 49 it is likely that we did not get the full picture of dementia in our practice. Second, because we relied on data already collected, we did not have a reliable measure of functional status or standardized cognitive assessment, so we likely included persons at different stages of their cognitive trajectory, which would influence outcomes such as ACP discussions. Third, we do not have data on the cause of death or the burden of dementia symptoms, which would affect the timing and appropriateness of a symptom-focused and hospice-focused approach to care. Fourth, our cohort was predominantly white, and our findings may not generalize to more racially and ethnically diverse populations beyond the US upper Midwest. 50 Our study findings, however, add important insights into the health care experiences of people living with dementia as they approach the end of life, data that may be used to highlight areas of priority for palliative care practice change within primary care. Among the lessons learned is the need for practitioners to provide patients who have dementia with more and earlier opportunities for ACP discussions. As health care practitioners caring for people living with dementia, we have learned that traditional models of primary care need to be adapted or replaced by more innovative models of care, with involvement of the patient, caregiver, and facility staff (where applicable).
Conclusion
People living with dementia in our study had regular contact with health care professionals in the last year of life, especially those in SNFs. Acute care visits were more common in those living at home/ALFs. The burden of comorbid conditions influenced hospitalization in both the community and SNFs. Lack of documented ACP in the SNF group, although uncommon, was associated with increased hospitalization. The SNF group, however, had frequent practitioner visits offering multiple opportunities for ACP so that patient goal-directed care could be provided at the end of life.
Footnotes
Acknowledgment
Kathleen Louden, ELS, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading, administrative, and clerical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Population Health Science Scholars Program of the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, from Mayo Clinic benefactor support, and by the National Center for Advancing Translational Sciences, (grant number UL1TR002377). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.