
Abstract
Introduction
Clinically significant depressive symptoms are prevalent in people with advanced life-limiting illnesses.1,2 These can exacerbate physical and psycho-existential sufferings, worsen the quality-of-life for families and individuals, and deprive people from having meaningful social interactions for good closures at the end-of-life.2–8 In the general palliative care population, assessment and management of such can be challenging due to co-existing symptom burdens, associated complications from physical illnesses, and often complex psychosocial dynamics.2,9–11 Within this cohort, there is a subgroup with very poor prognoses measured in days-to-weeks. This subgroup may pose extra clinical challenges as they usually have poorer functional status and higher symptom burden than others while the usual interventions for depressive symptoms may not benefit in-time nor be tolerated.1,12–16 For the purpose of this study, the term “depression” will be used to indicate clinically significant depressive symptoms that include various depressive disorders and depressive symptoms that fulfil thresholds of depression-specific assessment tools.1,17–19
There were studies that explored clinicians’ perspectives towards delivering depression care in the general palliative care population, showing varying degrees of clinician confidence.20–23 For people whose prognoses are in the range of days-to-weeks, these studies suggested that clinicians may have a sense of nihilism, and were less likely to assess or treat depression.20–22 While palliative physicians and psychiatrists are integral parts of providing specialist depression care in the palliative care context, 24 no study explored their perceptions and approaches to depression care in people with very poor prognoses.
The authors undertook a survey of Australasian (Australia and New Zealand) palliative care physicians and psychiatrists to address such. 11 The survey identified low rates (40%) of depression screening with all participants having experienced diagnostic uncertainty, reporting assessment and management variations. 11 Less than 25% of participants reported more likely to intervene for major depressive disorder with non-pharmacological and/or typical antidepresants when life-expentancy is short. 11 A sense of “therapeutic nihilism” was described: “Why assess it if there is little I can do about it?”; “Pointless if interventions (including psychosocial) will not be practical/acceptable.” (Supplemental Material 1) 11 A qualitative study was subsequently needed to explore these issues in greater depth.
This study aimed to ascertain the perceptions of Australasian palliative physicians and psychiatrists regarding depression screening, assessment and management in the very poor prognosis setting (defined by an estimated life-expentancy of days-to-weeks), exploring key barriers to care and potential solutions.
Methods
Study Design & Methodology
This study is the second part of a mixed-methods study with a sequential explanatory design, informed by the methodology of pragmatism.25–27 After conducting an initial predominantly quantitative survey that identified clinicians’ practices and perceived barriers, this qualitative study used a focus group method for triangulation to gain insight into the survey findings and generate potential improvement strategies.11,25,28
Population & Recruitment
Eligible participants were palliative physicians and psychiatrists based in Australasia who were members of Australian and New Zealand Society of Palliative Medicine (consisting of general practitioners and specialist physicians with advanced training in palliative medicine) and Royal Australian and New Zealand College of Psychiatrists. Participants were recruited through emailed invitations distributed by both organisations. Initially only those who have completed the preceding survey (n = 9; 60.0%) were eligible. 11 Due to poor recruitment, the invitation was then expanded to include clinicians who were unsure of (n = 4; 26.7%) or denied survey completion (n = 2; 13.3%) by two subsequent email invitations using purposive and snowball sampling. Further email invitations were restricted by the organisations’ dissemination policies.
Data Collection
Three focus groups (palliative care physicians: n = 2; CL psychiatrists: n = 1) each containing four to eight participants were conducted in November and December 2020, arranged according to participants’ medical specialities. The focus groups were of one-hour duration, conducted online using Zoom. Only participants and the facilitators were present in the discussions. Each participant attended the focus group once.
Two facilitators (authors) conducted the focus group discussions. The primary facilitator was a male palliative care specialist and research fellow undertaking clinical care and doctoral studies on this topic. The secondary facilitator was a doctorally-qualified female academic with a background in psychology and experience in qualitative research in people with chronic and life-limiting illnesses. The primary facilitator was known to some palliative care participants as a clinical colleague, but not in a hierarchical relationship. The secondary facilitator was not known to any participants. While the primary facilitator facilitated the group discussion, the secondary facilitator moderated the discussion and recorded relevant field notes to aid data analysis.
Participants were emailed the initial survey results (inclusive of psychiatry results [n = 32] – Supplemental Material 1) and were informed that they would be asked to comment on these when attending the focus groups. 11 To begin each session, participants were asked about their general impression of depression in people with very poor prognoses. The survey results were then presented by the primary facilitator. 11 Following this, participants were prompted to comment on the survey findings, elaborate on the perceived reasons for clinical practices and challenges, and postulate potential improvement strategies using open-ended questions designed a priori (Supplemental Material 2).
Data Analysis and Reporting
The focus group discussions were video-recorded with participants’ permissions. The audio recordings were transcribed using a professional transcription service. Primary facilitator checked transcripts for accuracy. The primary and secondary facilitators undertook conventional qualitative content analysis.29,30 They independently read and re-read transcripts, coded text inductively, and created coding trees using NVivo 12. They met to rectify differences and consolidate codes into agreed categories through multiple discussions among them and the rest of the authorship team (consisting of researchers and clinicians with backgrounds of palliative medicine or psychiatry) until 100% consensus was reached. Aligning with the aim of this study, data are reported according to general perceptions, challenges, and solutions. Following inductive analysis, categories of challenges and solutions, broadly influenced by McLeroy's ecological framework, were applied post-hoc to organise data for reporting, as they reflect various levels of influence required to drive changes. 31 This article was written using the Consolidated Criteria for Reporting Qualitative Research (COREQ) framework. 32
Results
Overall, fifteen clinicians participated (Table 1) - 11 palliative physicians and four consultation-liasion (CL) psychiatrists, predominantly (> 90%) based in Australia with mean years of specialty experience of 10.7 (SD: 6.4) and 15.5 (SD: 5.1) respectively.
Participant Characteristics.
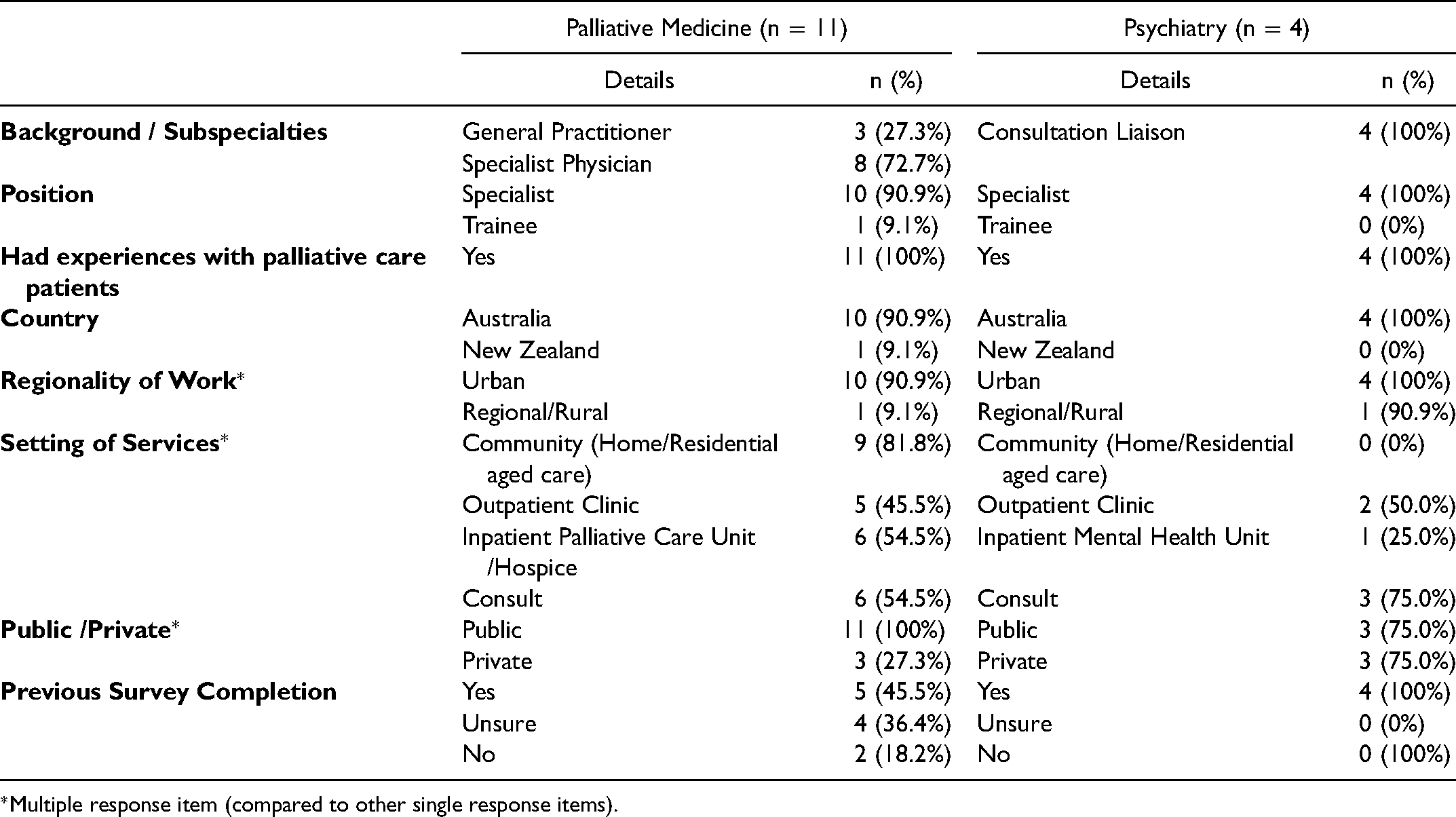
*Multiple response item (compared to other single response items).
General Perceptions
When asked about their overall perceptions, the participants from each focus group described the topic of depression care in people with very poor prognoses to be “complex”. A sense of disempowerment was expressed among the palliative physicians: “uncertainty”, “…it just makes me a bit depressed”, and “[I feel] helpless”. “I think…there was the lack of skills [in depression screening, assessment and management] and we don't really know… We can't do anything, so then we're less likely to want to assess it.” (Pallliative Physician 2)
In contrast, while still reflecting a sense of complexity towards the topic, CL psychiatrists conveyed a sense of empowerment and optimism that depression in this context is still “worth treating” and “not necessarily inevitable”.
“I think people are more treatable than a lot of people think. People think there's an inevitability of depression and an understandability about it, but that's not always the case.” (Psychiatrist 3)
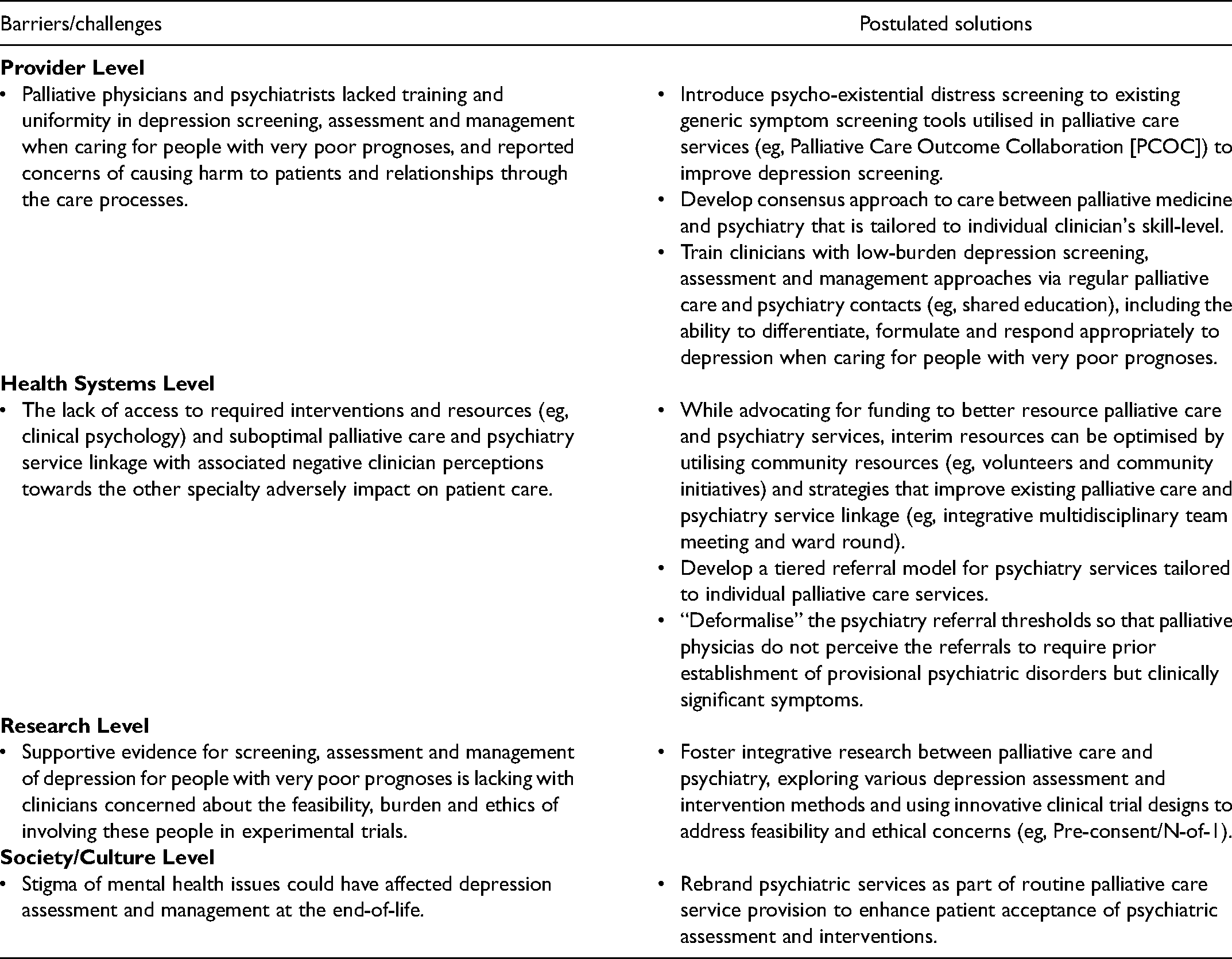
Comparisons of perspectives of palliative physicians and psychiatrists revealed differences in the perceived roles and needs of the two specialities, with palliative physicians describing the need for guided first-line depression care delivery while psychiatrists reporting inadequate resources to deliver second-line care (Table 2). Perceived key challenges and postulated potential solutions were described, synthesised post hoc into levels of influences informed by McLeroy's ecological framework (Table 3). 31
Barriers & Challenges
Provider-level
Overall, participants described that clinicians lacked the required training and intra- and inter-disciplinary uniformity in approaches to depression care in people with very poor prognoses. Palliative physicians were perceived to lack the necessary psychiatric skills with poor knowledge of therepuetic options while psychiatrists were perceived to lack the required palliative medicine training to deliver optimal depression care at the end-of-life. “I think it's skills [identifying and responding to depression] that palliative care physician should have, but the simple fact is they don't, some of them.” (Psychiatrist 3)
Comparison of Palliative Medicine and Psychiatry Cohorts.
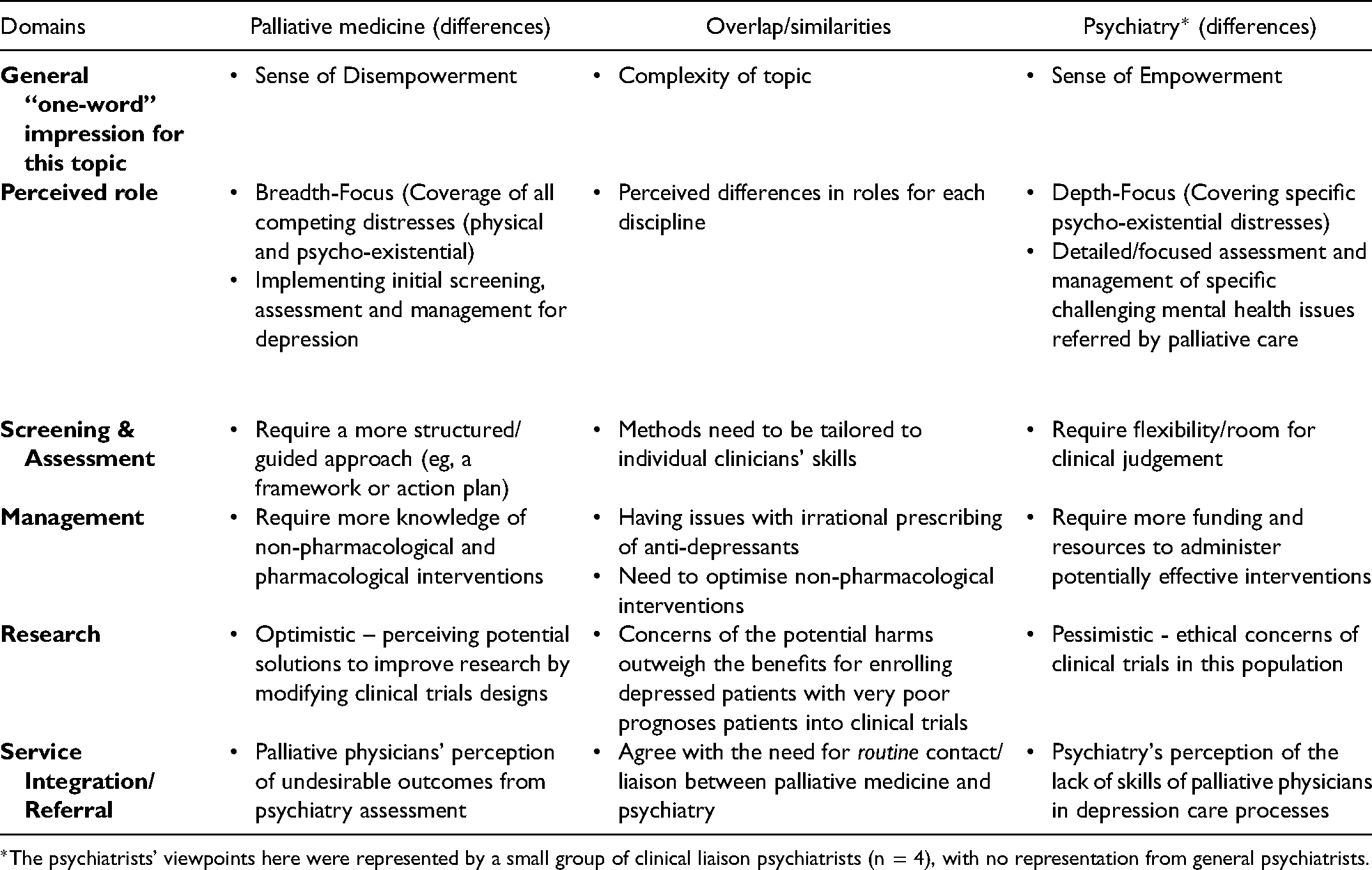
*The psychiatrists’ viewpoints here were represented by a small group of clinical liaison psychiatrists (n = 4), with no representation from general psychiatrists.
Perceived Key Barriers and Challenges to Depression Care for People with Very Poor Prognoses and Postulated Solutions by Australasian Palliative Physicians and Psychiatrists.
“[psychiatrists] who aren't experienced in the area [palliative medicine], as soon as a patient expresses “I wish it was just all over,” which is a pretty normal thing to say, they suddenly think they're suicidal…” (Palliative Physician 6)
Clinicians reported concerns of causing harm to patients and relationships through depression care processes: depression screening using lengthy questionnaires might “fracture” the therapeutic relationship; interventions may cause adverse effects while not producing timely benefits; and peer pressure against administering potentially helpful interventions that have little supportive evidence. In separate focus groups, two participants voiced depression can be perceived as a “driver” for people to make meaningful social interactions, and treating it might cause harm.
“I wouldn’t want to be robbing people of appropriate drivers to help people at the end-of-life (by treating their depression). The stress (depression) can be a driver to bring people together in a way if you do it right.” (Palliative Physician 7)
“Are we robbing people of appropriate sorrow by diagnosing them with depression and treating them?” (Palliative Physician 2)
Health system-level
Clinicians perceived a general lack of access to required liaison psychiatry and psychology services, especially those with palliative care expertise, even in urban settings where resources and skilled personnels tend to be more readily available. “It goes back to resources. It just keeps going back to it. You [palliative physicians] can screen all you want, but if there’s nobody [liaison psychiatry and psychology services with palliative care expertise] there to help you as a palliative care physician, you might do a good job of it, but you might feel under-supported…” (Psychiatrist 4)
Access to potentially effective interventions was impacted by regulatory issues, contributed by the limited evidence-base in the literature.
“The other issue that comes up with novel treatments [in context of ketamine] or non-standard treatments are the limitations of the evidence-base and regulatory issues, which vary from state to state.” (Palliative Physician 1)
Participants noted that linkage and collaboration between existing palliative care and psychiatry services were often suboptimal. Negative clinician perceptions towards the other discipline were described to have contributed to the infrequent contact and late referrals. For example, some palliative physicians perceived undesirable assessment outcomes from psychiatry referrals.
“My CL [Consultation Liaison] service at one site, definitely, everybody seemed to have ‘adjustment disorder’…But I think sometimes it gets a bit tiring to see ‘adjustment disorder’…it just affects how often I want to ask them to come and give help really…” (Palliative Physician 8)
Research-level
A lack of research with evidence to support various assessment methods and interventions in people with very poor prognoses was a key challenge, as there was reluctance to enrol these individuals into clinical trials. While palliative physicians reported concerns around feasibility and burden of clinical trials on participants, CL psychiatrists voiced ethical concerns of patients possibly receiving ineffective interventions during randomisation. “…there is a lot of barriers with researching in this patient group because we don’t have a lot of time to get to them, and also the burdens often catch up and you have to weigh up…often research has a lot of questionnaires…that can be very challenging in such a difficult time” (Palliative Physician 11)
“I did a small pilot trial looking at ICBT [Internet-based Cognitive Behavioural Therapy] in people with advanced cancer, but you can't randomize them, you know…very ethically problematic thing to do. Like you can, but it would be really hard to go through the ethics board. And also personally I would find that hard!” (Psychiatrist 4)
Society-level
Stigma of mental health issues was reported as a barrier to care. Initiating patient discussion around psychological needs and having liaison psychiatry or psychology input was not observed by patients to be the norm, contributing to patients’ resistance in depression care. “…a lot of patients, particularly in certain age groups where you never talked about psychiatric issues, and then when they’re at the end of life and you start to bring that up, they get quite ‘What do you mean?’” (Palliative Physician 2)
Potential Solutions
Overall, the potential solutions postulated by participants involved an integrative approach established upon the foundation of a better collaboration between both palliative care and psychiatry disciplines (Figure 1 & Table 3).
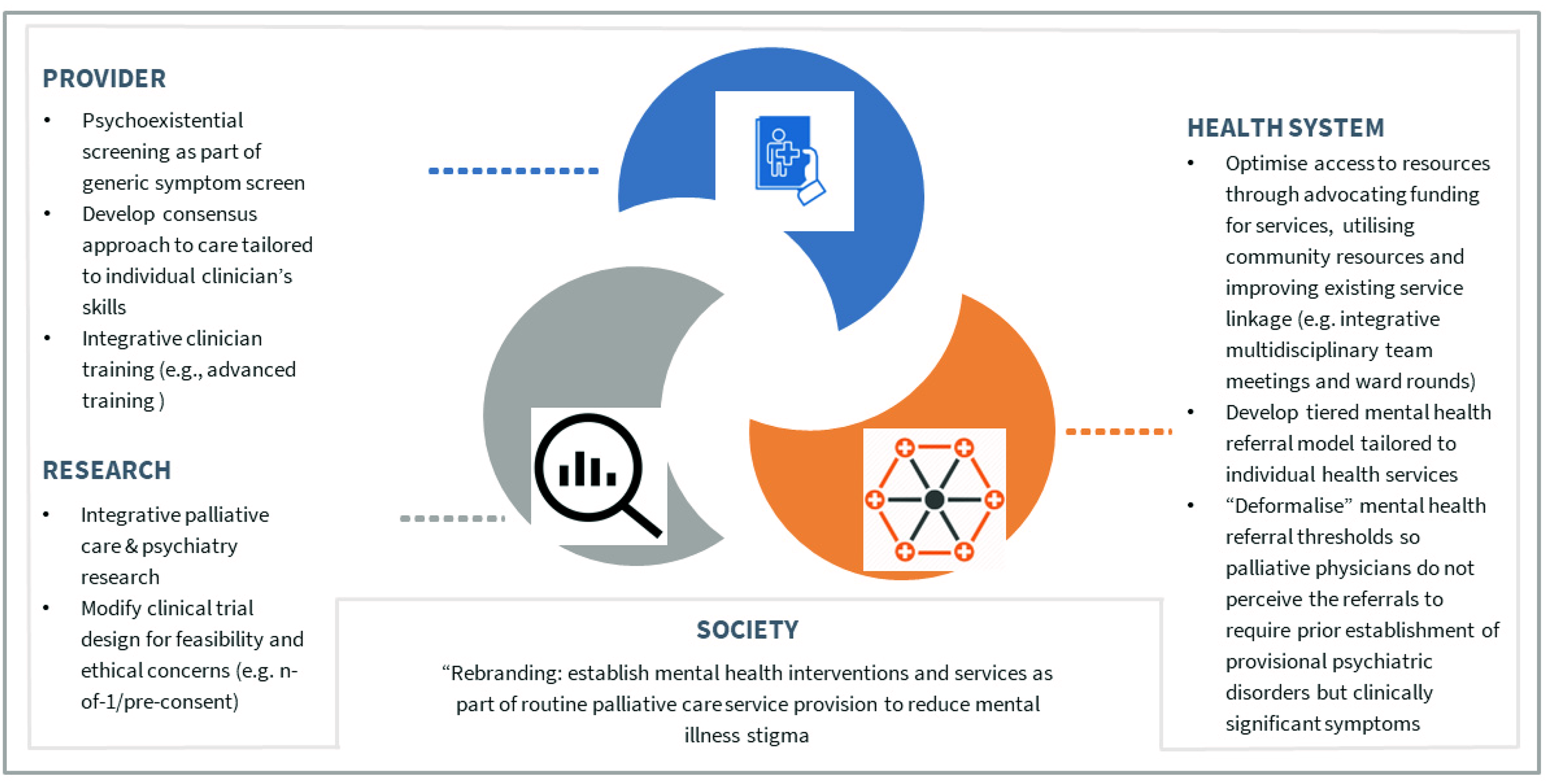
Care Process Integration of Palliative Medicine and Psychiatry – Postulated Solutions by Participants.
Provider-level
Screening
For better depression recognition, participants postulated that low-burden depression screening as part of a general screening for psycho-existential distress be added to the current generic symptom screening tool (eg, Palliative Care Outcome Collaboration Symptom Assessment Scale [PCOC SAS]) used in palliative care services. “..[Depression screening] being part of the PCOC [Palliative Care Outcomes Collaboration] scoring might be helpful, part of the standard scoring that we do before we see the patient…That might just help alert us there's something else that we need to screen for.” (Palliative Physician 11)
Development of Consensus Approach
Participants perceived the need for palliative care and psychiatry to develop a consensus approach to care using best available evidence. The approach needs to be tailored to the skill-level of individual clinicians - a structured approach to guide less experienced clinicians, and a flexible approach relying more on clinical judgment for the more experienced. “I felt like maybe we, as two groups, need to get together and talk about what is actually the best way to manage these patients’ depression - because I think there are two very different disciplines, and two very different skill sets that we need to marry to come up with a best way to approach this treatment.” (Palliative Physician 11)
Improve Clinician Training
Participants described that palliative physicians can be trained with low-burden approaches to depression care. Specifically,the training content may include: the use of ultra-short screening methods such as one- or two-item depression screening tools; the skills to differentiate and formulate the complex interplay of biopsychosocial aetiology during depression assessment
33
; and the ability to respond appropriately to depressed patients with the knowledge of potentially rapid-onset therapeutic options (ie methylphenidate and ketamine). Meanwhile, psychiatrists need the foundational knowledge of general management of symptoms and end-of-life issues. Clinician training can occur through establishing: regular interdisciplinary contacts; shared education; integrative advanced training; and formal education. “…increasing exposure to junior medical staff [including palliative care trainees] to psychiatry rotations, so that there's capacity building and so that people have a basic building block of how to actually do psychiatrist assessments and start treatment…That [integrative training between palliative care and psychiatry] would be excellent.” (Psychiatrist 3)
Health system & service-level
Optimising Resources
While participants reported a need for more funding to better resource the palliative care and liaison psychiatry services, participants also postulated strategies to optimise interim resources. Community resources such as volunteers and community initiatives may be utilised to deliver necessary non-pharmacological interventions that do not necessitate psychiatry or psychology services. Strategies to improve current linkage between existing psychiatry and palliative care services may optimise resource access. This can include establishing routine palliative care–CL psychiatry multi-disciplinary team (MDT) meetings, ward rounds, and informal gatherings. “…that weekly [palliative care psychiatry multidisciplinary] meeting, like tomorrow I [psychiatrist] will discuss two new patients at that meeting with the broader team, and they [palliative care clinicians] just find that invaluable…it really up-skills them over time.” (Psychiatrist 4)
Optimising Referrals
Participants postulated a tiered approach for psychiatry referral, involving palliative physicians performing first-line depression care using low-burden structured methods or guidance from psychiatry, followed by psychiatry input if further assessment and management are needed. Participants voiced that the referral criteria for each discipline need to be tailored to clinicians’ skills in individual local health services, including “deformalising” the referral processes to encourage earlier referrals. “…to de-formalise [psychiatry referral criteria] and allow [palliative] clinicians to simply flag potential ‘mood problems’. We found similar with delirium, many of our multi-D[isciplinary] team were reluctant to use the word ‘delirium’ verbally or in the case notes as they felt they hadn’t ‘diagnosed’ it properly. However when we encouraged them to just flag ‘confusion’ or ‘altered behaviour’, [clinical service provision improved]… Perhaps a similar approach could work for depression.” (Palliative Physician 4)
Research-level
Despite participants voicing mixed feelings towards research in those with very poor prognoses, participants all agreed that collaborative research between palliative medicine and psychiatry in studying various assessment and management options is pivotal. “I think research are very important in our patient group and with the research then we'll be better guided on how we can manage these patients.” (Palliative Physician 11)
To address the feasibility and ethical concerns of enrolling patients with very poor prognoses into experimental trials, modification of clinical trial designs was suggested (e.g., utilising pre-consenting method of consent or n-of-1 design).
“I'm interested in n-of-1 trials. I've seen them used for other medications. I think that could be something that could be applied to palliative care” (Palliative Physician 7)
Society-level
At the societal level, clinicians thought “rebranding” psychiatric interventions and services by making them part of the routine palliative care service provision might reduce stigma of mental illness and enhance patient acceptance of psychiatric assessments and interventions. “…’rebrand’ psychiatry in oncology and palliative medicine, so that like in chronic pain, psychology is just part of your assessment, because it's normal to need a psychologist or psychiatrist as part of your team to help manage and get your optimal outcome in a very difficult situation” (Palliative Physician 2)
Discussion
This study provides insights into the previous survey findings of perceived complexities of palliative physicians and psychiatrists when providing depression care for those with very poor prognoses. 11 It expounded upon the sense of nihilism reported in the survey, detailed the contributing challenges, and postulated solutions (Table 3). 11
While patients might be fearful in eliciting their depression with treating clinicians, this study findings support that palliative physicians may also feel inadequately trained to initiate and effectively perform depression screening and assessment, perceiving these processes as time-consuming and burdensome for patients and themselves.2,8,11,34–36 The concern of “robbing people of appropriate drivers” for good closure with important persons at the end-of-life by treating depression highlights the challenges for palliative physicians in differentiating pathological depressive syndromes (for which interventions may improve social engagement) from appropriate reactive sadness, where offering interventions beyond psychosocial support may cause harm.2,16 The reported observation that inexperienced clincians may consider more typical antidepressants instead of non-pharmacological interventions (eg, dignity therapy) as foundation and adding rapid-onset pharmacological agents with psychiatry inputs (eg, methylphenidate or ketamine) if indicated also highlight the need for better education and supportive infrastructure (eg, regulations towards methylphenidate prescribing).2,35,37–39
Meanwhile, the participating CL psychiatry cohort were skilled and experienced in treating patients with depression in this setting. Consistent with the literature, they perceived depression in advanced life-limiting illnesses to be potentially treatable, even in those nearing death.2,10,16,39 However, they acknowledged that they were a minority and felt under-resourced. This is echoed by the perception that psychiatrists who are skilled and experienced in palliative care are lacking, with some avoiding this field.2,23,35 In fact, one previous psychiatry survey respondent reported “Very few psychiatrist are comfortable working in the clinical space” (Supplemental Material 1). To improve care, there needs to be an increased awareness of the importance of palliative care psychiatry with funding prioritised.2,24
The postulated solutions by participants, as discussed below, centered around care process integration between palliative care and psychiatry, consistent with strategies suggested for improving palliative care and psychiatry collaboration in the general palliative care population.24,40,41 While these strategies were postulated to facilitate consensus in approaches and amalgamate the forte of both specialties, their effectiveness to improve patient outcomes for people with very poor prognoses and the associated implementation barriers warrant future studies.
Strategies and Implications
Provider level
The suggested routine depression screening added to an established generic symptom screen in palliative care services such as the PCOC SAS may be helpful, though the optimal depression screening method in this very poor prognosis subpopulation is contentious and requires further studies.40,42,43 Palliative physicians and psychiatrists should learn both psychiatric and palliative care skills relevant to this field.11,23 While evidence informing effectiveness of specific training strategies is scant in this setting, the postulated strategies reinforced by the literature include: informal education through integrative MDT meetings, clinics and ward rounds; and building formal integrative training opportunities such as joint educational seminars, clinical placement of trainees in the other specialty, and mandatory teaching in college training curricula.22,24,40,44–46 As postulated, training content may include skills for both disciplines to work collaboratively to deliver depression screening, assessment and management in low-burden manners, facilitating potentially effective psychotherapies as foundation (eg, dignity and meaning-centered therapies), complemented by rapid-onset pharmacological agents (eg, methylphenidate, and esketamine) as required.16,22–24,35,37–41,47–50
Health system & policy level
Pervious survey identified that palliative physicians perceived a lack of access to required psychiatric resources despite Australasia having some of the most well-resourced health system per capita internationally.11,51 As found in the focus group discussions, a key contributor may be the lack of supportive infrastructure with inadequate liaisons between existing palliative and psychiatric services.2,46 Health services need to prioritise efforts and fundings that promotes palliative care and psychiatry service integration and timely depression interventions (eg, funding for psychiatry presence and exemptions to regulatory restrictions for psychostimulants).2,24 As suggested by participants, community volunteers can be trained to provide general emotional support or counselling to relieve the system burden.52,53 Furthermore, nurses and social workers from both disciplines may be trained to perform first-line depression assessment and interventions for palliative care patients.40,54–56 In line with the postulated solutions, most depression cases may be adequately managed by the treating palliative care team provided there is appropriate training, and a referral to psychiatry can be initiated when escalation of care is required. 16 The pespectives of various MDT members (eg, nurses, pastoral care workers, and psychologists) and ways to leverage their strengths to deliver care warrants future exploration.
Research level
While there is a paucity of palliative care psychiatry implementation studies to guide changes in this field, as perceived by participants, there lacks high-quality evidence of effective interventions when prognoses are poor.11,13,15 Integrative palliative care and psychiatry research is needed. Randomisation, arguably, can be ethical if there is clinical equipoise (eg, dignity therapy and methylphenidate trials).15,37,39,57,58 Researchers need to consider innovative strategies to minimise burden and maximise potential benefits for participants. Feasibility studies prior to phase III trials and the use of alternative inclusive and supportive designs (eg, pre-consent, n-of-1, and Bayesian response adaptive randomisation) warrant considerations.59,60 Using high-quality prospective case-control studies or modifying Naranjo criteria in phase IV pharmacovigilance study settings to imply causal relationship for interventions may also be possible. 61
Limitations
The study's key limitation is the small number of focus groups conducted. As suggested by participants, the poor recruitment might resulted from clinicians prioritising COVID-19 related clinical activities over non-COVID-19 research, potential avoidance by general (non-CL) psychiatrists from perceived lack of relevance or interests, and the limited capacity of participating organisations in disseminating study invitations.24,35 Subsequently, recruitment expanded to include non-survey respondents. Meanwhile, maximum variation and data saturation may not have been reached, especially in the psychiatry cohort, and the comparison between palliative care and psychiatry cohorts is hypothesis-generating in nature.
Conclusion
Palliative physicians and psychiatrists perceived depression care in people with very poor prognoses to be complex and challenging, contributed by the lack of clinician training, interdisciplinary collaboration, research, and supportive societal attitudes. Developing clinician training, supportive health infrastructures and innovative research strategies centering on integrating palliative care and psychiatry care processes may be helpful.
Footnotes
Acknowledgements
We would like to acknowledge Clinical Prof Richard Chye, Sacred Heart Supportive & Palliative Care, St Vincent's Hospital, Darlinghurst, NSW, Australia and University of Notre Dame, Australia for his support of this project.
Author Contributions
Under the supervision of DC, MA, and BD, WL and MD designed the focus group study protocol and collected the data. WL and MD analysed the data. WL drafted the manuscript and DC, MA, BD, and MD provided critical revisions throughout.
Funding
The survey was funded by the Translational Cancer Research Network (Clinical PhD Scholarship Top-up award: 13114323), supported by the Cancer Institute New South Wales, Australia.
Research Ethics and Patient Consent
This project has been approved by the Human Research Ethics Committee of the University Technology Sydney (approval number: ETH19-4071). All participants provided written informed consent.
Data Management and Sharing
Anonymous focus group data can be requested from the corresponding author if required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.