
Abstract
Introduction
Management of cancer-related pain has been historically difficult and remains a significant issue in the overall care of patients with active cancer. Cleeland et al identified that two-thirds of patients with advanced cancer required analgesic use to manage pain; however, pain management was found to be inadequate for approximately 40% of these patients. 1 Several initiatives were instituted to improve analgesia in patients with cancer, yet investigators found that pain management remained inadequate in 33% of patients with cancer despite these targeted interventions. 2 In attempts to explain this marginal improvement in cancer pain prevalence, previous investigators have attempted to explain barriers to improved pain control, including poor pain assessments by healthcare workers, patients' fear of complications relating to opioid use, and patients' reluctance to report pain.2,5 Much of the existing literature focuses on the outpatient setting, but it remains unclear whether these outpatient studies can be applied to acute care settings, namely the Emergency Department (ED). Cancer-related problems account for greater than 4.5 million ED visits in the United States annually, and this number continues to rise.6,7 A 2019 multicenter cohort study reported that the majority of patients with active cancer visiting the ED presented with pain as their chief complaint, and over half of these ED visits resulted in admission. 8
Despite pain being one of the most common chief complaints in the ED, analgesics may be underutilized and delays in treatment are common. 9 The effects of insufficient analgesic use are likely amplified in patients with active cancer, who are already at high-risk for poor pain control. A recent study demonstrated that patients who suffer from moderate-to-severe cancer-related pain often receive inadequate doses of pain medication while in the ED. 10 Given the large proportion of cancer patients who present to the ED for pain, effective pain management for this vulnerable population presents a serious challenge. Our objective is to evaluate how certain variables including patient demographics, cancer characteristics, functional status, and ED treatment factors may affect patient outcomes. We hypothesize that there is a need for improvement in the emergency care of cancer pain and that a detailed analysis may provide future targets for quality improvement measures.
Methods
Study Design and Selection of Participants
We conducted a retrospective cohort study to evaluate patients presenting with cancer-related pain to two academic EDs that are affiliated with a National Comprehensive Cancer Network (NCCN) designated cancer center from June first, 2012 to January first, 2016. Each of the study hospitals are located in the Southern California region of the United States. We included all patients who were 18 years of age and older with active cancer who presented to the study EDs during our enrollment period with a chief complaint of pain. Active cancer was defined as a diagnosis of cancer with ongoing treatment (within the past month), ongoing symptoms relating to cancer, or a known recurrence of a previous cancer. Patients excluded were those who were in remission, had non-melanomatous skin cancer (ie, basal cell carcinoma, squamous cell carcinoma), benign tumors, or carcinoma in-situ. At the time of this study, neither of the affiliated EDs utilized treatment protocols for cancer pain.
Methods of Measurement
Data were collected through an electronic medical records system and entered into a REDCap database by trained research associates (AK, VR). Each data abstractor underwent dedicated training to assure validity in data collection. Monthly meetings were conducted to ensure adherence to study protocols and review inconsistencies or questions throughout the data collection period. All research associates were blinded to the study hypotheses. Variables were defined a priori, and a measurement of inter-rater reliability was performed on 5% of patient charts, utilizing ECOG status as our variable of interest. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) methods were utilized when conducting and reporting this study. 11 ICD codes that were used for the abstraction of patient records are included in the Supplemental materials.
We collected and analyzed demographics, cancer type, Eastern Cooperative Oncology Group (ECOG) performance status, primary pain site, pain scores, type of pain medications administered, and time-to-analgesia. Outcome variables included initial pain score, final pain score, delta pain (final pain score minus initial pain score), ED diagnosis, ED disposition, admission level of care, and return ED visit within 72 h. The ECOG score, which is a measurement of the performance status and disease progression of patients with cancer, was determined based on documentation from oncology visits that preceded the index emergency visit (within 90 days) in addition to ED provider notes 12 (Supplemental material). We defined a high ECOG as those with a score of 3 or 4, representing those with very limited functional status. We categorized pain based on the numerical scale as: none (0), mild (1-4), moderate (5-6), and severe (7-10). 13 Cancer type and pain were both grouped according to primary organ system involvement. Elderly patients were categorized as those who were ≥ 65 years of age, and patients under the age of 65 were categorized into the adult group.
Statistical Methods
We utilized descriptive statistics to characterize patient demographics, ECOG score, and outcome frequencies. We reported medians for non-normally distributed data and means for normally distributed data. We compared medians for non-normally distributed continuous variables using the Kruskal Wallis test and utilized multivariable logistic regression to evaluate the association of our exposure variables on hospital admission/discharge. An alpha less than 0.05 was significant.
Results
Cohort Characteristics
We identified 553 patients during our study period who were over the age of 18, had a past medical history of cancer, and presented to the ED with a pain-related chief complaint. Of these patients, 38 were excluded because their condition was not considered a true malignancy (eg, colon polyp, non-melanomatous skin cancer, carcinoma in situ), and 32 additional patients were excluded for having a non-active cancer. The remaining 483 patients were included in the final analysis (Figure 1). Our test of inter-rater reliability resulted in a kappa score of 0.78, which represents substantial agreement. Our cohort had a median age of 59, was predominantly non-Hispanic white (60%, 290/483), and was 53.80% (260/483) female (Table 1). The most common cancer types were colorectal, gastrointestinal, leukemia/lymphoma, and female reproductive malignancies in descending order (Table 2). Our cohort had a median ECOG score of 1. 39.3% (190/483) our patients were admitted to the hospital and 7.7% (37/483) revisited the ED within 72 h.

Flowsheet of Study Design. 483 out of 553 patient charts were retrospectively reviewed and included in the study. Inclusion criteria included patients over the age of 18 with past medical history of cancer who presented to the ED with active cancer and a chief complaint of pain. Active cancer was defined as a diagnosis of cancer with ongoing treatment, ongoing symptoms relating to cancer, or a known recurrence of a previous cancer.
Demographics of Study Population. Quantified Metrics of Patients” age, sex, Race/Ethnicity, and ECOG status are Depicted in the Following Tables.

Pain Scores Stratified by Cancer Type. Initial, Final, and delta Pain Scores Stratified by Different Cancer Types.

Cancer Types and Primary Pain Site
Breast, CNS, colorectal, ENT, gastrointestinal, leukemia/lymphoma, lung, female reproductive, and male reproductive cancers had strata that consisted of at least 20 patients with greater than 50% reporting initial severe pain (Table 2). Of these, reproductive female cancers had the greatest percentage of patients presenting with severe pain (81.8%, 45/55). The cancer types with the least improvement in pain (delta pain <2.5) upon ED disposition were breast, colorectal, ENT, and lung. When investigating the responses to analgesia among patients who had a primary diagnosis of pain upon ED disposition (n = 233, eg abdominal pain, musculoskeletal pain, pelvic pain), patients with musculoskeletal pain had significantly less improvement in reported pain than all other pain types (delta pain −2.1 vs −3.4, OR 2.3, p = 0.025) [ Table 3]. After adjusting for age, sex, and race/ethnicity, there was no statistical difference in initial, final, or delta pain based on cancer type as well as no statistical difference between solid and hematologic malignancies for delta pain.
Pain Scores Stratified by Pain Character. This Table Represents the Statistics of Initial Pain, Final Pain,and delta Pain Stratified by the Different Pain Characters in Those That had a Pain-Related Diagnosis on ED Disposition (n = 232).

Age
Patients who presented to the ED with severe pain tended to be younger than patients who did not present with severe pain (median: 58 vs 62 respectively, OR 8.0, p < 0.01). However, among those that had severe pain on ED disposition, there were no significant differences in delta pain with respect to age.
ECOG
Among patients with a high ECOG score, 51.5% (50/97) were admitted, which is significantly greater than those who presented with lower ECOG statuses after adjusting for age, sex and race/ethnicity (n = 386, 37.8% admitted) (AOR 1.6, p = 0.034). Furthermore, 94% (30/32) of patients with both high ECOG scores and severe initial pain continued to have severe pain on ED disposition. In comparison, only 25% (16/65) of patients with a high ECOG but without severe pain on presentation had severe pain on ED disposition. The median delta pain for patients with high ECOG scores and severe initial pain was −1, while the median delta pain for all other patients was −3. Patients with high ECOG scores and moderate/severe initial pain saw significantly less improvement in their pain than others in the cohort (OR 8.4, p < 0.01).
Admitted Versus Discharged Patient Groups
We compared initial pain, final pain, and delta pain between admitted and discharged groups (Table 4). Although initial pain levels were found to be similar between both groups, discharged patients tended to have lower final pain scores than admitted patients (median 3 vs 5). Discharged patients had greater improvement in their pain, as indicated by significantly lower median delta pain than admitted patients (−3 versus −2 respectively) [OR 1.101, p = 0.001]. Patients who experienced a delay of greater than 180 min from being placed in their ED room to first analgesic administration were more likely to be admitted to the hospital after adjusting for age, sex, race/ethnicity and ECOG status (AOR 3.4, p = 0.014).
Pain Scores of Admitted and Discharged Cohorts. Initial Pain, Final Pain, and delta Pain Scores Stratified by Admitted, Discharged, and Total Cohorts.

Medications
A description of medication frequencies can be found in figure 2. When comparing analgesic responses, patients who did not receive opioids had a median decrease in pain of 2, whereas patients who received opioids had a median decrease of 3 (OR 0.921, p = 0.005). Patients who received opioids, however, were admitted more frequently than those who did not receive opioids (43.2% (144/333) versus 34% (51/150) after adjusting for demographic factors (AOR 1.51, p = 0.048)).
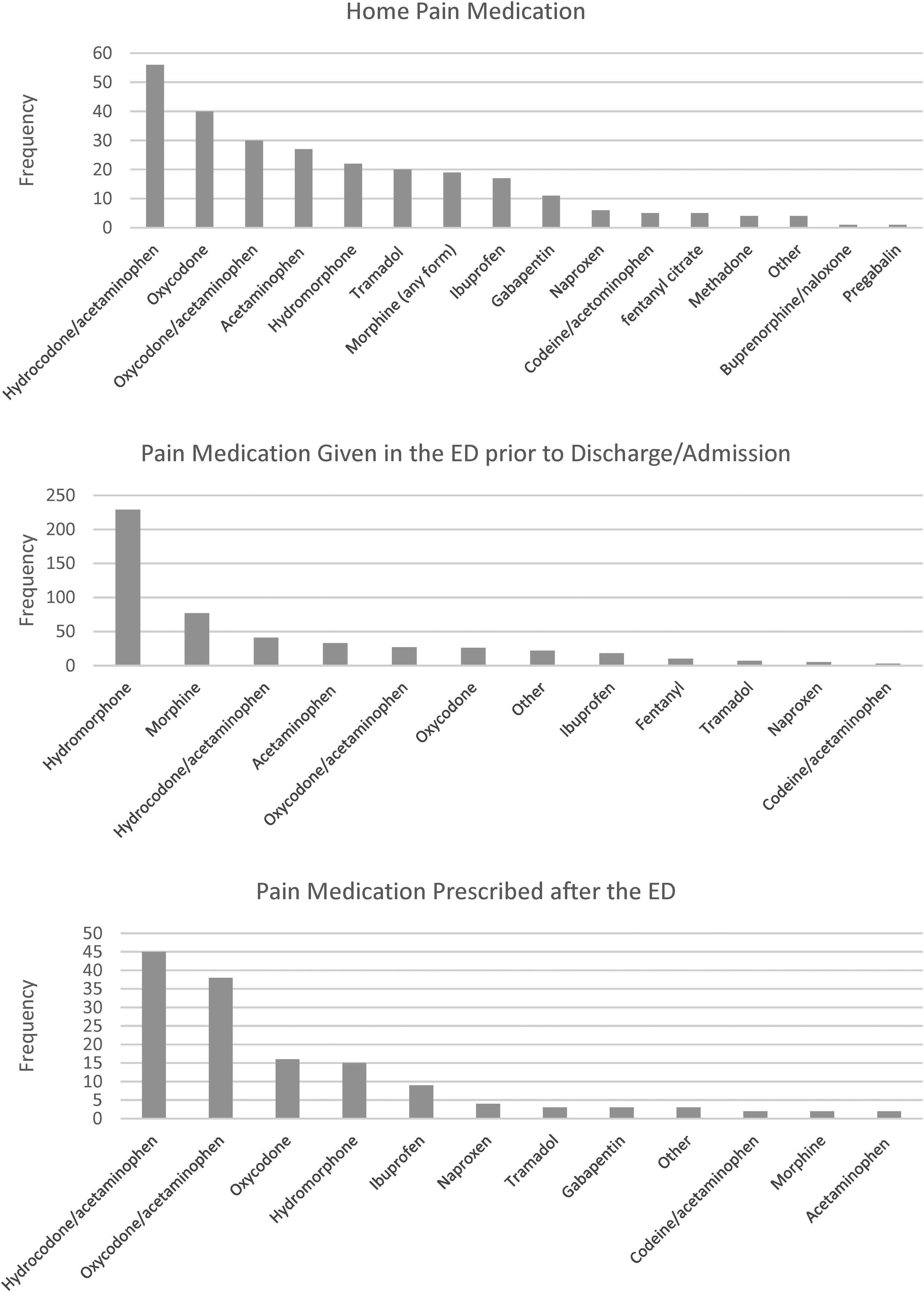
Medications. Distributions of medications stratified by home pain medication, pain medication given in the ED prior to discharge/admission, and pain medication prescribed upon ED disposition.
We also found that among patients who did not already have a home opioid prescription, the majority received a prescription for opioids upon discharge from the ED if they required any opioid (PO or IV) while in the ED for pain control (36% (120/333) versus 7.3% (11/150). We found that patients without a home opioid prescription who received an opioid for pain control in the ED were less likely to return to the ED within 72 h if they also received an opioid prescription upon ED discharge (11.6% vs 14.5%), however, this result was non-significant.
Discussion
Management of cancer pain is challenging, especially during periods of acute exacerbation that require a visit to the ED. Previous literature has helped elucidate the scope of the problem,1,4 though few have focused specifically on cancer pain in the ED. We performed this study to better define the population at risk, the current status of pain management in the ED, and the associated outcomes, in an effort to identify future targets for intervention.
Cancer Types and Primary Pain Site
After stratifying pain scores by cancer type, we noticed that breast, colorectal, ENT and lung cancers had both a high frequency of initial severe pain presentations and a low median delta pain. As a result, these cancers were of particular interest because they seemed to be the least responsive to pain management in our cohort. When comparing differences in delta pain between admitted and discharged patients, we found that discharged patients tended to experience a greater improvement in their pain during their index visits. Given that admitted and discharged patients had similar initial pain scores at presentation, it appears that patients who have more refractory pain are more likely to be admitted to the hospital. Our analysis revealed that patients with musculoskeletal pain encountered a significantly greater resistance to pain management than other pain types. Treatment of bone metastases-related pain remains palliative at present, and typically involves a combination of systemic analgesics, anti-tumor agents, hormones, chemotherapy, steroids, local surgery, anesthesia, and/or external beam radiation. 14 To our knowledge, there is no established protocol for the ED management of acute pain crises for cancer-related musculoskeletal pain, which therefore serves as a potential target for future intervention.
Age and Severe Pain
We found that patients with severe pain on arrival to the ED tended to be younger than those who presented without severe pain. Though no causative explanation can be drawn, we suspect that possible explanations for this finding include: generational differences in experiencing and reporting pain, different age groups being more susceptible to certain cancer types, or other potential differences. For instance, previous investigators have suggested that aging may decrease sensitivity to low intensity pain and increases pain thresholds. 15 One study specifically reported a correlation between decreasing cancer pain severity and increasing age. 16 Additionally, elderly patients may be less likely to report pain because of attitudes of stoicism, fatalism, and resignation. 17 Furthermore, younger patients may be less likely to visit the ED unless their pain escalates to a severe state, thereby reinforcing the trend of higher initial pain scores in this population. We encourage oncology and emergency teams to be acutely aware of how cancer-pain may be experienced and consequently reported incongruously between different age groups.
Using ECOG with Initial Pain Levels to Guide Patient Care
By analyzing patients” functional status in conjunction with their pain scores, we found that patients who presented with a high ECOG scores and severe initial pain had significantly less improvement in their pain than all other patient groups. This vulnerable patient group may experience little improvement in pain not because of poor ED management but rather due to inherent qualities of their illness and physical disability. We encourage ED physicians to recognize this phenomenon, and perhaps explore alternative analgesics (eg ketamine), ultrasound-guided nerve blocks, or anxiolytics. We suggest that patients with a high ECOG scores and severe initial pain could be flagged to alert the care team regarding the increased odds of refractory pain and hospital admission.
Improving Analgesic Utilization
Our analysis identified that patients who experienced a significant delay in analgesic administration were more likely to be admitted to the hospital. Given the often busy and chaotic environment of the ED, delays in treatment are common. 18 This finding, however, suggests that protocols and other systemic changes to improve the timely administration of analgesia may decrease overall admissions. Physician-driven changes to electronic medical record (EMR) systems have greatly streamlined patient care with studies showing improved patient outcomes as well as decreased physician burnout and increased physician job satisfaction.19,20 A best practice, EMR alert could inform physicians when a cancer patient with documented pain has waited longer than 1.5 h for analgesia administration and thus prompt immediate attention. Similar interventions could be utilized to improve documentation of pain scores as well as medication dosing.
Opioid Analgesics
Though several non-opioid treatment modalities are available, opioid analgesics have been the mainstay for treating patients with moderate-to-severe cancer-related pain. 5 Consistent with the literature, we identified that patients who received opioids had statistically more significant changes in pain levels than those that did not receive opioids. Interestingly, however, we found that patients who received IV opioids for pain management in the ED were more likely to be admitted than those who did not. There are several factors that may contribute to this phenomenon. First, patients that require stronger pain medication may be more ill at baseline and are therefore more likely to be admitted. Secondly, once IV opioids are initiated, it may be difficult for clinicians to transition these patients to oral regimens in a timely manner, thus requiring admission for observation.
Beyond the administration of IV opioids, we were also interested in the patient cohort that received a home opioid prescription upon ED disposition. By analyzing this subgroup of patients who were not already taking opioids at home, we found that these patients were more likely to receive a home opioid prescription if they were given an opioid analgesic during their ED visit. In the literature, there has been discussion regarding the use of step 2 “weak opioids” and step 3 “strong opioids”, in which studies have indicated that opioid-naïve cancer patients with moderate pain are more likely to respond to low-dose morphine, a strong opioid, than to weak opioids.5,21,23 This poses an interesting point for emergency physicians to consider when deciding on the strength and dosing of analgesic agents for patients with active cancer-related pain.
Limitations and Future Areas of Study
Due to the nature of retrospective studies, an inherent limitation is the inability to assume causation. This study was also performed at a specific region in the United States and therefore may not be generalizable to other populations. Although we assessed a surrogate maker of disease progression (ECOG), we did not address stage or extent of metastases in this study, which may influence pain management and associated outcomes. Additionally, although all patients had a component of acute pain, we did not assess the degree to which these painful episodes were chronic. As ICD-10 codes were used to abstract data for this study, it is also possible that patients with pain were excluded from analysis if there was no documentation of pain. This may have skewed the results to include patients with more severe pain episodes. We believe that a more detailed survey of cancer types can help identify features that catalyze exacerbations of cancer-related pain. Another realm of further study should focus on visits involving severe initial pain at presentation to assess potential risk factors. Lastly, a better understanding of differing cancer pain experiences between young and elderly patients may help formulate more tailored protocols for pain management and ideally decrease the number of preventable ED admissions and revisits for cancer-related pain.
Conclusion
Through this investigation of patients with active cancer presenting to the ED with pain, we were able to identify several factors that were associated with adverse outcomes. Notably, delayed administration of pain medication as well as high ECOG scores were associated with an increased likelihood of admission. Patients who presented with severe pain and high ECOG scores were highly refractory to treatment in the ED. Overall, we suspect that one can improve the care of cancer pain in the acute setting by accurately identifying vulnerable patients, developing tailored cancer pain management protocols, and implementing targeted patient-centered interventions.
Supplemental Material
sj-docx-1-pal-10.1177_08258597221121316 - Supplemental material for Evaluating Cancer Pain Characteristics and Treatment Factors in the Emergency Department: A Retrospective Cohort Study
Supplemental material, sj-docx-1-pal-10.1177_08258597221121316 for Evaluating Cancer Pain Characteristics and Treatment Factors in the Emergency Department: A Retrospective Cohort Study by Rishi Gupta, Lucia Lin, Vanessa Resley and Ayesha Khan, David R. Li, Rebecca A. Shatsky, Christopher J. Coyne in Journal of Palliative Care
Footnotes
Author Contributions
RG and LL were the primary authors of the manuscript and assisted with editing. VR and AK were the primary data abstractors and assisted with writing and editing. RS assisted in study design and was heavily involved in editing. CC conceived of the study, assisted in writing, performed data analysis, and edited the manuscript. CC takes responsibility for the manuscript as a whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the study site institutional review board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.