
Abstract
Objective
Patients receiving palliative care are more prone to dermatological disease. The aim of our study was to determine the frequency of dermatological diseases and associated factors in patients receiving palliative care support.
Methods
This prospective observational study included inpatients in the palliative care unit of our university hospital in Erzurum/TURKEY. The patients were evaluated by the same dermatologist within the first 48 h of admission and 3 days a week during follow-up. Demographic data, reasons for admission to the palliative care unit, and skin lesions at the time of admission and during follow-up were recorded.
Results
The median age of the 259 patients included in the study was 77.0 years (min- max, 19-108) and 54.4% were women. Dermatological disease was detected in 246 patients (96.1%) at admission to the palliative care unit and in 185 patients (71.4%) patients during follow-up. The most common dermatological disease at admission was dry skin (n = 175, 67.6%), which was also the most common cause of pruritis (n = 29, 11.2%). The most common skin infection was dermatophytosis (n = 57, 22.0%) and the most common type of dermatitis was contact dermatitis (n = 17, 6.6%). Nearly all tumors were benign (n = 32, 12.4%) and most chronic wounds were pressure ulcers (n = 96, 37.1%). During hospital follow-up, the most frequent dermatitis was contact dermatitis (n = 44, 17.0%), the most frequent skin infection was candidiasis (n = 25, 9.7%), the most common chronic wound was pressure ulcers (n = 25, 9.7%), the most common dermatological disease was urticaria (n = 14, 5.4%), and all cases of pruritus were associated with dry skin (n = 8, 3.1%).
Conclusions
The frequency of dermatological findings is high among patients receiving palliative care. Therefore, dermatologists should be included in multidisciplinary palliative care teams and evaluate palliative care patients early and regularly.
Introduction
Palliative care is a medical specialty that brings together multiple disciplines to increase the quality of life of individuals with serious and terminal diseases. The multidisciplinary palliative care team should include the patient and their relatives, physicians, nurses, physiotherapists, psychiatrists/psychologists, religious officials, social workers, and dieticians. Regardless of the patient's disease, the primary goal of palliative care is to alleviate and control their symptoms and provide psychosocial, social, and spiritual support. 1
Factors such as malnutrition, incontinence, immobility, immunosuppression secondary to the disease or its treatment, pain, and difficulties in the care plan predispose palliative care patients to dermatological diseases such as skin infections, dermatitis, and pressure ulcers. 2 There is also high risk of exacerbating existing skin lesions or developing new treatment-related lesions or malignancy-related dermatosis. 3 The presence of skin lesions reduces quality of life and disrupts social relations because of pain, pruritis, or the emotional impact. 4 However, dermatologists are rarely included in the palliative care team. There are few studies in the literature examining dermatological problems in patients receiving palliative care.3–5 The aim of our study was to determine the frequency of dermatological diseases and associated factors in patients receiving palliative care support.
Methods
Study Design
This prospective observational study was conducted with patients admitted to the palliative care unit of Atatürk University Faculty of Medicine Hospital in Erzurum/TURKEY. Patients are admitted to our palliative care unit with primary and secondary criteria.
Primary Criteria
1. Presence of life-threatening or life-shortening disease 2. If there is an increase in the reasons for admission to the hospital 3. If there are uncontrolled symptoms 4. Having complex care needs 5. Significant decrease in functions 1. Patients with metastatic or locally advanced inoperable malignancy 2. For medical interventions that can only be applied to the patient in the hospital 3. To make discharge plans of the patient who has been hospitalized for a long time
6
Secondary Criteria:
Setting and Participants
Inclusion criteria were: admission between May 1, 2021 and November 1, 2021, being hospitalized in the unit for at least 48 h, and agreeing to participate in the study by signing the informed consent form. Exclusion criteria were: length of stay less than 48 h and repeat admission to the palliative care unit.
Data Collection
All patients were evaluated within the first 48 h of admission by the same dermatologist. Demographic data (age, gender, chronic diseases, number of medications, habits), reasons for admission to the palliative care unit, and skin lesions at the time of admission and during follow-up in the unit were recorded. The dermatological findings observed during follow-up were all observed in the hospital and were evaluated independently of baseline. Skin lesions, infection, skin tumors, dermatitis, chronic wounds, nail and hair diseases, pruritis, and associated local or systemic treatment methods were noted. The patients were re-evaluated by the same dermatologist three days a week during follow-up, which continued until discharge, transfer to another clinic or hospital, or death.
Statistical Analysis
The data were recorded and analyzed using the package program SPSS version 21 (IBM Corp, Armonk, NY). Using descriptive statistics, continuous variables were presented as median, minimum, maximum, and interquartile range (IQR), categorical variables as frequency and percentage. Chi-square test was used to test the relationship between two categorical variables. Fisher's Exact test was used in the presence of less than five patients in one cell. A p value less than 0.05 was considered statistically significant.
Ethical Considerations
The study was conducted after obtaining approval from the Atatürk University Faculty of Medicine Ethics Committee (dated 15.04.2021, meeting/decision number: 03/11).
Results
Demographic and Basic Characteristics of the Patients
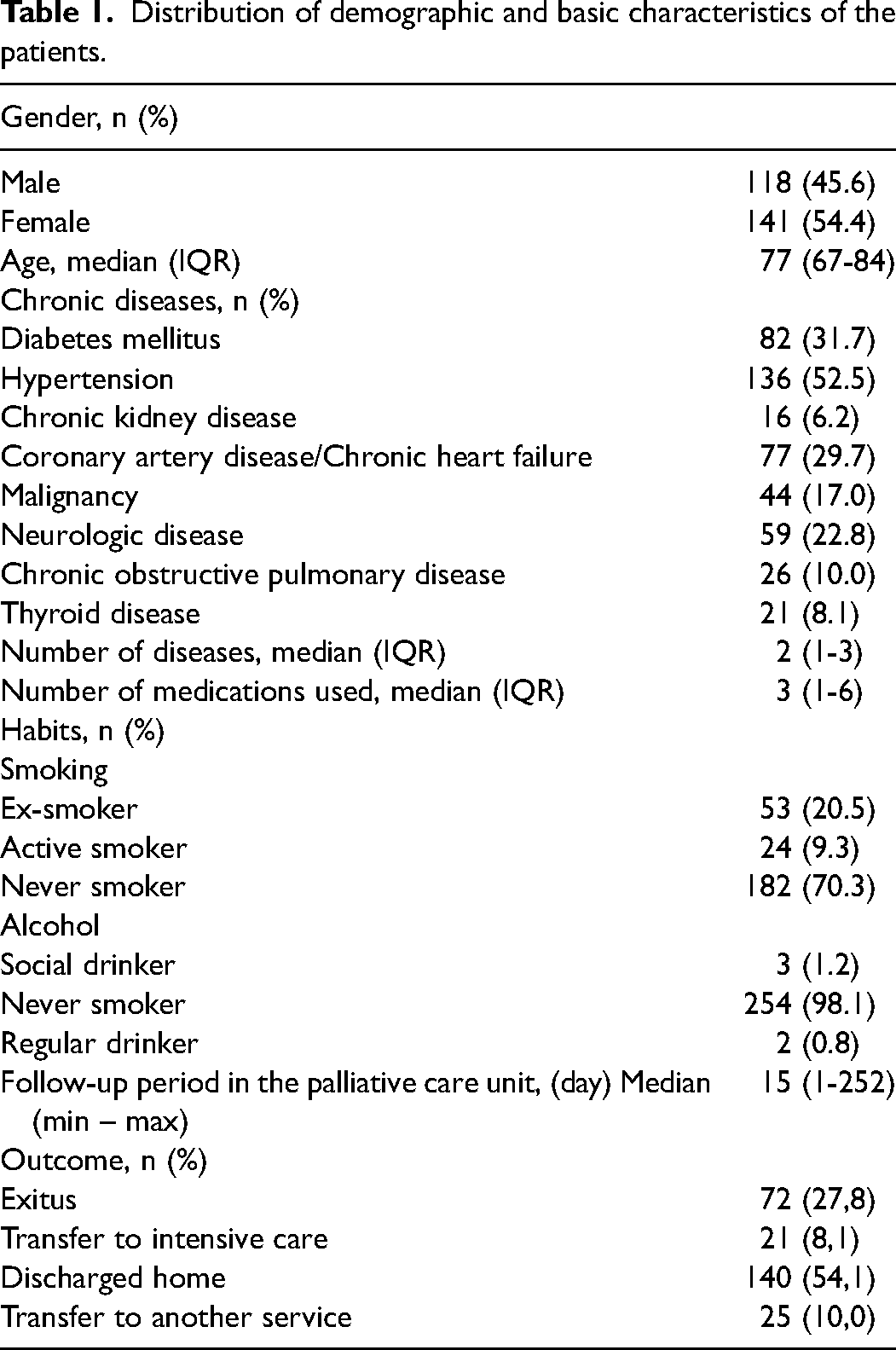
The median age of the 259 patients included in the study was 77.0 years (min-max, 19-108) and 141 (54.4%) were women. The three most common indications for admission to the palliative care unit were malnutrition (n = 140, 54.1%), decubitus ulcer (n = 90, 34.7%), and pain palliation (n = 30, 11.6%). The distribution of the patients’ demographic and basic characteristics is presented in Table 1. The patients had a median of 2 (IQR, 1-3) chronic diseases, the most common of which was hypertension (52.5%).
Distribution of demographic and basic characteristics of the patients.
Dermatological disease was present in 246 (96.1%) of the patients at admission to the palliative care unit and was detected in 185 (71.4%) of the patients during follow-up. The dermatological findings observed during follow-up were independent of baseline. All dermatological findings observed during follow-up were observed in the hospital and during follow-up. Patients in whom dermatological disease was observed at admission to palliative care had between 1 (n = 42, 16.2%) and 10 (n = 1, 0.4%) dermatological diseases. During follow-up, at least 1 (n = 98, 37.8%) and at most 5 (n = 2, 0.8%) dermatological diseases were detected together. The frequency of dermatological diseases at admission and during follow-up is shown in Figure 1. The most common dermatological disease at admission was dry skin (n = 175, 67.6%), which was also the most common cause of pruritis (n = 29, 11.2%). The most common skin infection was dermatophytosis (n = 57, 22.0%) and the most common type of dermatitis was contact dermatitis (n = 17, 6.6%). Nearly all tumors were benign (n = 32, 12.4%) and most chronic wounds were pressure ulcers (n = 96, 37.1%). During hospital follow-up, contact dermatitis was the most frequent finding overall (n = 44, 17.0%), while candidiasis was the most common skin infection (n = 25, 9.7%). Pressure ulcers were also the most common chronic wounds observed during follow-up (n = 25, 9.7%), and the most common dermatological disease during follow-up was urticaria (n = 14, 5.4%). All cases of pruritus were caused by dry skin (n = 8, 3.1%).
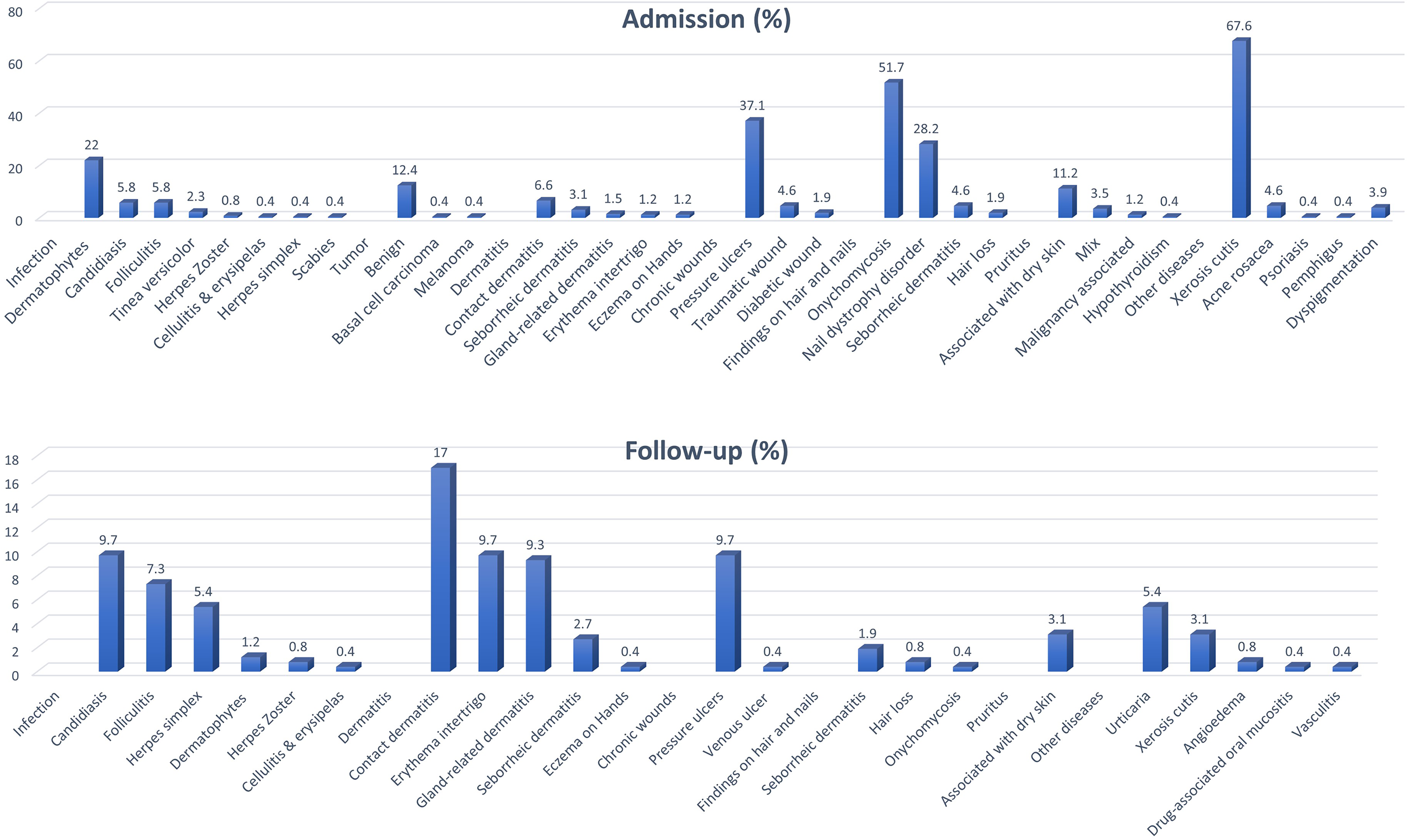
Frequency of dermatological diseases observed in palliative care patients during admission and follow-up
Distribution of Dermatological Diseases According to Chronic Disease
The relationships between the patients’ chronic diseases and their dermatological diseases at admission and follow-up in the palliative care unit were evaluated in supplement Tables 1 and 2, respectively. Naturally, patients with diabetes mellitus had a significantly higher prevalence of diabetic wounds (p = 0.036). They also had a higher rate of onychomycosis (p = 0.010). None of the patients with DM had dyspigmentation, which was statistically significant (p = 0.020). Traumatic wounds were significantly less frequent (p = 0.011) and onychomycosis was significantly more frequent in patients with HT (p = 0.038). Chronic pressure ulcer was significantly more common among patients with malignancy and neurological disease (p = 0.031 and p = 0.029, respectively). During follow-up, patients with malignancy had a significantly higher frequency of pressure ulcer (p = 0.001), whereas those with thyroid disease developed seborrheic dermatitis significantly more (p = 0.013).
Distribution of dermatological diseases present at admission by gender.
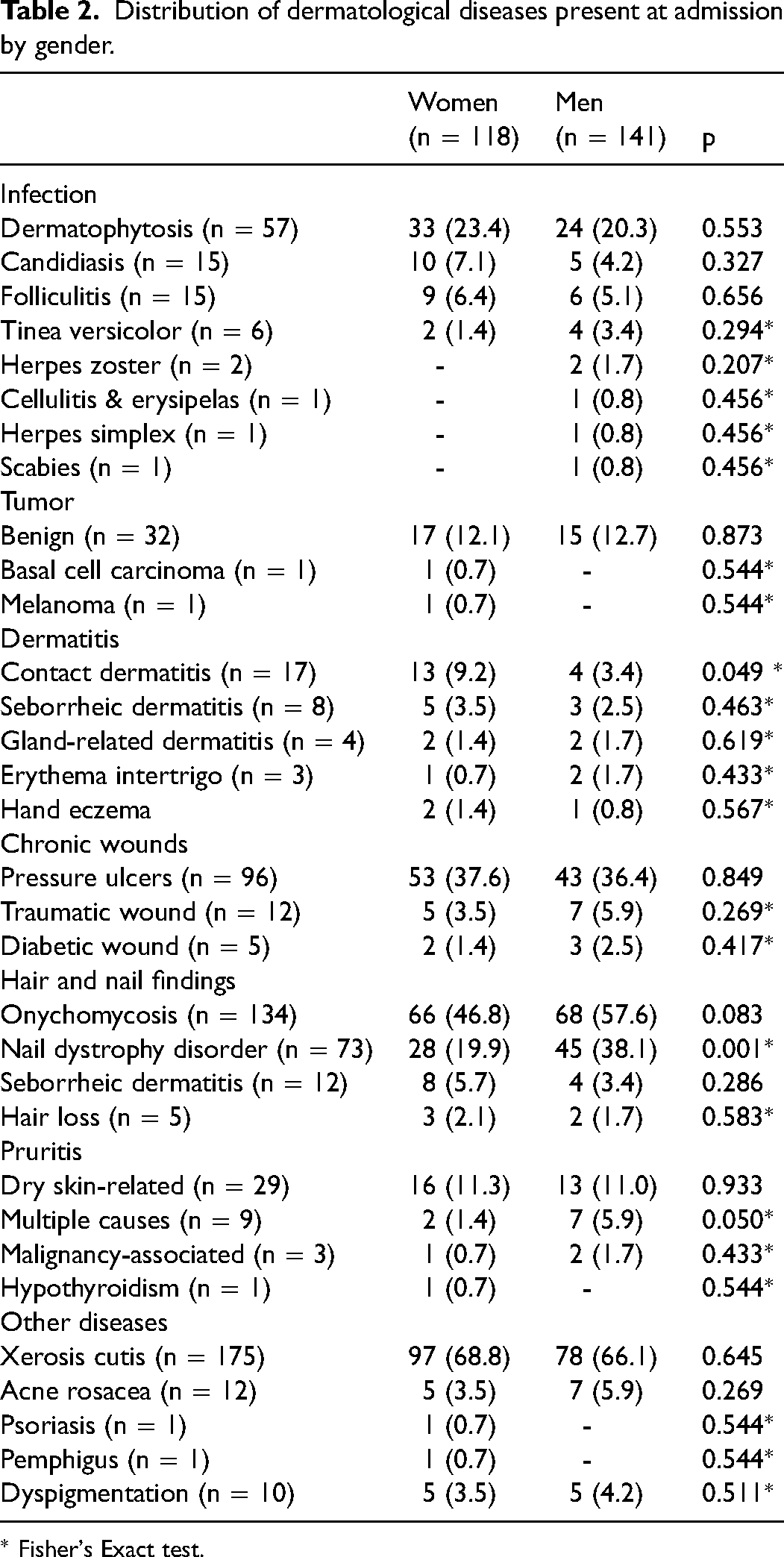
* Fisher's Exact test.
The relationship between age group and dermatological diseases at admission to the palliative unit and during hospital follow-up were evaluated in supplement Tables 3 and 4, respectively. There was a significant difference in pressure ulcer among the age groups (p = 0.039). This difference was associated with a higher incidence of pressure ulcer in patients under 65 years of age compared to those aged 65–74 and 75–84 (p = 0.018 and p = 0.017, respectively). Nail dystrophies were more common in patients in the 75–84 and over 84 age groups compared to those under 65 years of age (p = 0.012 and p = 0.009, respectively). Dry skin was also more frequent in the 75–84 and over 84 age groups than in the under 65 group (p = 0.010 and p = 0.012, respectively). No significant correlation was observed between age group and dermatological diseases developed during follow-up.
Distribution of dermatological diseases during follow-up in the palliative care unit according to gender.

* Fisher's Exact test.
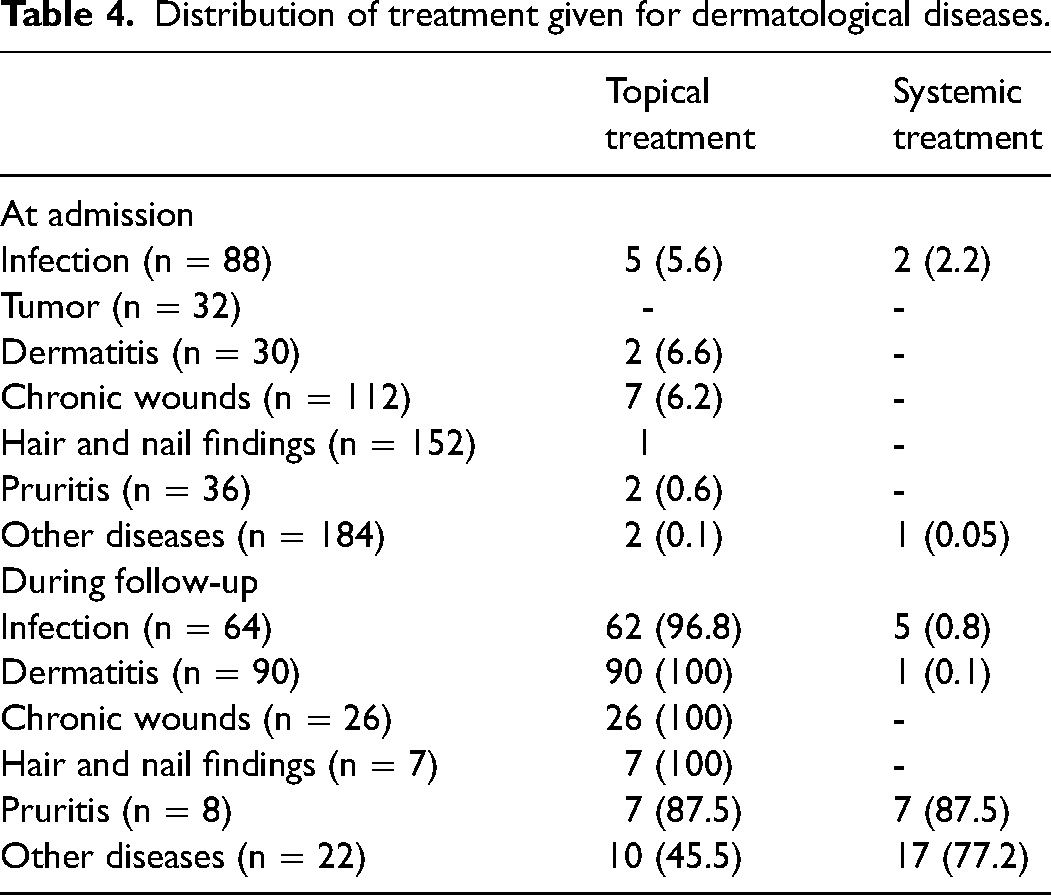
Distribution of treatment given for dermatological diseases.
The relationship between gender and dermatological diseases present at admission to the palliative unit was evaluated in Table 2. Contact dermatitis was more common in women (p = 0.049), while dystrophic nails were more common in men (p = 0.001).
The distribution of dermatological diseases developed during follow-up in the palliative care unit by gender is presented in Table 3. No significant relationship was observed between gender and dermatological disease development during hospital follow-up.
Treatment of Dermatological Diseases
The frequency and type of treatment for dermatological findings detected at admission to the palliative unit and during follow-up are presented in Table 4. Dermatological findings observed during hospital follow-up were more frequently treated as soon as they were detected.
Discussion
In our study evaluating dermatological diseases in palliative care patients, we determined that dermatological diseases were detected in 96.1% of the patients at admission to the palliative care unit and in 71.4% of the patients during their follow-up in the hospital. In recent years, the need for palliative care centers has increased because of the growing burden of chronic disease, rising incidence of dementia and cancer, and longer expected life expectancy of cancer patients.7,8
Barnabe et al reported that one-third of 16 patients who received palliative care support had skin lesions that required medical treatment or nursing care support. 5 Neloska et al reported that 271 patients (most with malignancy) had at least one and in total more than 50 dermatological diseases at admission to the palliative care unit. In their study, the most common dermatological diseases were dermatitis (18.3%) and hair and nail diseases (17.5%), and the most common skin finding was dryness (77.8%). 3 Hansra et al evaluated 20 palliative care patients over 2 months and determined that the most common conditions were skin abrasions (37%), infections (26%), and inflammatory dermatosis (17%). 4 In our study, the most common skin finding was dryness (67.6%), and the most common dermatological diseases were onychomycosis (51.7%) and pressure ulcers (37.1%). The main reason for the discrepancy between our results and previous reports is that the study sample consisted of mostly geriatric patients and the majority of chronic illnesses were nonmalignant diseases.
The pathogenesis of pruritis is complex, and a cause is often difficult to determine. 9 It may be secondary to dry skin 10 or paraneoplastic syndrome, indirectly related to treatment, 11 or associated with cholestasis, opioid use, uremia, or hematological diseases. 12 In a study conducted by Neloska et al, the frequency of pruritis among patients receiving palliative care was found to be 35.1%. 3 In our study, the frequency of pruritus was 16.3%, and the most common cause was dry skin (11.2%). In our patients, dry skin frequently accompanied diabetes mellitus. Generalized or localized pruritus may occur in patients with diabetes. Although the cause of pruritus in diabetic patients is not fully understood, it is thought to be due to dry skin, diabetic neuropathy, renal failure, and medicines used. 13
Pressure ulcers are a geriatric syndrome that frequently occurs in palliative care patients and increases health care costs. 3 The prevalence of pressure ulcers in palliative care centers varies between 10.5% and 26% in various countries.14–17 It has been shown that pressure ulcers are particularly common at the end of life. 16 In our study, 37.1% of the patients were found to have pressure ulcers at admission. This high rate is associated with the fact that prolonged hospitalization is the most common indication for admission to our palliative care unit. Only 9.7% of our patients developed decubitus ulcers during follow-up in the palliative care unit. This is the result of preventive care for decubitus ulcer development in our unit and cooperation with the dermatology clinic, and demonstrates the importance of the multidisciplinary approach in palliative care. Lyder et al observed that pressure ulcers were more frequent in patients aged 65 years and older with more than one disease. 18 Consistent with the literature, in our study the prevalence of pressure ulcer was higher among patients with malignancy and neurological disease. In addition, pressure ulcers developed more frequently during follow-up in patients with malignancy, consistent with the literature. Also consistent with the literature, we observed in our study that the prevalence of pressure ulcer increased with age and was higher in men.19–21
Although nail changes seen in palliative care patients do not affect life expectancy, they may impact quality of life in older patients. Some nail disorders are important indicators of underlying systemic disease. Patients with peripheral artery disease and congestive heart failure may exhibit dystrophic nail changes. 22 Nail-related diseases are more common in men due to their exposure to trauma. 23 Similarly, nail lesions were more common among the men in our study. In a study conducted by Neloska et al, the prevalence of onychomycosis at admission to palliative care was 21% and the prevalence of nail-related dystrophic disorders was 22.5%. 3 In our study, these rates were 51.7% and 28.2%, respectively. We attribute the differences between these findings to the large number of geriatric patients with diabetes in our study.
Eczema is common in palliative care patients. Older adults become more sensitive to irritants and allergens due to epidermal barrier dysfunction. Contact dermatitis is an important problem in palliative care patients. Neloska et al reported contact dermatitis in 2.2% of patients at admission to palliative care, 3 whereas this rate was 6.6% in our study and increased to 17% during follow-up in our palliative care unit. The fact that our rate is lower at admission can be explained by the fact that patients who are dependent in functional and daily life activities are exposed to fewer environmental and physical factors than those who are physically active. The increase in contact dermatitis can be explained by the patients’ exposure to allergens such as diapers.
Diaper dermatitis is a form of irritant contact dermatitis that develops in and around the perineum in response to moisture, friction, urea, feces, and the plastic content of the diaper. 24 The condition is common in palliative care units but was less frequent in our unit than in the literature. 3 We attribute this to the use of barrier creams and frequent ventilation and changes.
With aging, the frequency of infections increases due to reasons such as poorer personal hygiene, decreased epidermal turnover, and immune aging. 25 In the study conducted by Neloska et al, the most common infection seen in patients at admission to palliative care was candidiasis (19.2%), 3 while in our study, the most common skin infection was found to be dermatophytosis (22%). Our patients were diagnosed using potassium hydroxide by making a native preparation. All of our patients were treated with topical antifungals. Candidal infections are a fungal infection that occurs in the intertriginous areas, where there is intense friction and moisture. The presence of chronic diseases such as diabetes and frequent antibiotherapy use predispose to candidal infections in palliative care patients. 26 Candidiasis was present in 5.8% of our patients at admission to palliative care, while 9.7% of the patients developed candidal infections in different parts of the body during follow-up. All cases were controlled with topical treatment.
In this study, folliculitis was detected in 7.3% of the patients during follow-up. Because of the presence of risk factors such as long-term antibiotic use, hot and humid weather conditions, and diabetes mellitus in palliative care units and the possibility of serious complications, folliculitis is an important dermatological disease that should not be overlooked. 27 Other dermatological diseases that should be considered in palliative care units include herpes simplex infection and especially herpes zoster due to potentially serious complications that impair quality of life, such as postherpetic neuralgia. 3
In palliative care patients, drug-induced skin rashes to occur more frequently because of polypharmacy, concomitant diseases, delayed drug elimination due to impaired metabolism, and changes in protein binding reactions. In our study, drug-induced urticaria was observed during follow-up and was accompanied by angioedema in two patients.
The strength of our study is that it is one of the few studies to examine dermatological findings in palliative care patients and was designed prospectively. In addition, dermatological diseases are ignored in patients receiving palliative care. This study not only shows how common these diseases are but also reports their frequency with patient-based features. The most important limitation is that the study was conducted in a single center. Moreover, dermatological lesions such as skin cancer were only diagnosed by the clinician, with no pathological diagnosis. Finally, although it is known that corticosteroids often cause dermatological problems in patients receiving palliative care support, this relationship was not analyzed.
Conclusion
Dermatological findings are common among patients receiving palliative care. There are very few studies in the literature about the dermatological care of palliative care patients. Many studies have focused more on decubitus ulcers in palliative patients. However, patients in palliative care are at high risk of dermatological pathologies because of malnutrition, immobilization, incontinence, anemia, metabolic changes, and immunosuppression. Therefore, dermatologists should be included in multidisciplinary palliative care teams and evaluate palliative care patients early and regularly.
Supplemental Material
sj-docx-1-pal-10.1177_08258597221119063 - Supplemental material for Dermatological Diseases in Palliative Care Patients in a University Hospital: A Prospective Study
Supplemental material, sj-docx-1-pal-10.1177_08258597221119063 for Dermatological Diseases in Palliative Care Patients in a University Hospital: A Prospective Study by Erdal Pala, Pınar Tosun Tasar, Ahmet Onur Soguksu, Omer Karasahin and Can Sevinc in Journal of Palliative Care
Footnotes
Author Contributions
Concept and Design: PTT, EP; Data Collection or Processing: AOS, EP; Analysis/Interpretation: OK, CS; Literature Search: PTT, EP, OK, CS; Writing: PTT, EP, OK; Final Approval: PTT, EP, AOS, CS.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Atatürk University Faculty of Medicine Ethics Committee (dated 15.04.2021, meeting/decision number: 03/11).
Informed Consent
Written informed consent was obtained from the patient who participated in this study.
Trial Registration
None
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.