
Abstract
Introduction
In parallel to changing demographics across the country, (hospice) palliative care plays an increasing role in Canada's healthcare systems, as the burden of terminal illness increases. 1 Palliative care is a person-centred approach that works with patients and their family members or friends to provide physical, spiritual, and psychosocial support. 2 Oftentimes, friends and/or family members also play an important role as informal caregivers, providing physical and/or psychosocial support to the person receiving (hospice) palliative/end-of-life care. 3 In 2018, approximately 25% of Canadians, aged 15 and older, reported to have provided informal caregiving to a family member or friend. 4
The term “(hospice) palliative care” in Canada refers to an approach that aims to reduce suffering and to improve the quality of life for people who are living with life-limiting illness. This includes pain and symptom management, psychological, social, emotional, spiritual and practical support, and support for caregivers during the illness and after the death of the person they cared for. 5
In Canada, health care is a provincial and territorial responsibility and thus funding and organization of (hospice) palliative care programs vary between the ten provinces and three territories. Most provinces/territories have released individual strategic priorities for the improvement of palliative care based on the unique characteristics, resources, and needs of their populations. 5 At the federal level, various policy and funding initiatives have been rolled out in recent years to support the actions of provinces, territories, and several non-governmental organizations to improve palliative care in Canada. 5 This includes the creation of the Compassionate Care Benefits and the Caregiver Benefit, which support caregivers to take leave from work to care for their family members. 5
Patients can receive (hospice) palliative care across all settings, for example through home care, in long-term care homes, residential hospices, and in hospitals. How (hospice) palliative care is funded varies from province/territory to province/territory, and between care settings. (Hospice) palliative care provided in hospital, for example, is typically covered by the provincial/territorial health care plan. (Hospice) palliative care in the home, however, is not always (fully) covered, resulting in barriers to access. 5 Furthermore, family and friends play an essential role in service provision, with a majority of (hospice) palliative home care clients reporting they had family or friends helping to care for them. 6
The number of informal caregivers in Canada is projected to increase as the population ages, indicating a heightened need for supportive interventions. Canada's senior population is projected to be 10.4 million in 2037, a 68% increase from 2017. 7 The COVID-19 pandemic has increased the mortality of Canadians, particularly among older adults. 4 This has resulted in an “unprecedented reliance” on informal caregivers to support the healthcare systems, as well as increased caregiver stress and pain.8,9
The World Health Organization (WHO) advocates for supporting not only patients, but also their caregivers. 10 This includes grief and bereavement supports, which are essential to high quality end-of-life care. 11 During the end-of-life process, informal caregivers experience grief and bereavement, and a recent Canadian study showed that 42% of bereaved individuals obtained some type of bereavement support. 12 It is evident that effective and accessible bereavement services are essential for informal caregivers.
This scoping review builds on previous work exploring the grief and bereavement experiences of informal caregivers in the North American context. 13 Findings pointed to various mediators which affect the grief and bereavement experience, including the patient's disease type, demographic factors of the caregiver, and the care setting. These mediators were found to contribute to the types of grief experienced, including anticipatory and complicated grief. Grief was also associated with other psychosocial outcomes such as hope, relief, guilt, and distress. The complexity of informal caregivers’ grief highlights the need for effective interventions. Thus, the aim of this scoping review was to identify current interventions which address the grief and bereavement experiences of informal caregivers of geriatric patients in the Canadian (hospice) palliative/end-of-life care realm.
Methods
This scoping review was conducted from October 2020 to February 2021 in adherence to the five-stage framework outlined by Arksey and O’Malley, 14 and further supported by guidance taken from Levac, Colquhoun, and O’Brien. 15 The five-stage framework is made up of the following steps: (1) Identifying the research question, (2) Identifying relevant studies, (3) Study selection, (4) Charting the data, and (5) Collating, summarizing, and reporting the results. This review further adheres to PRISMA Scoping Review Extension (PRISMA-ScR) guidelines. 16
Identifying the Research Question
Informed by a previous scoping review exploring the grief experiences of informal caregivers in North America,
13
the objective of this work was to answer the question: What interventions exist in Canada to support grieving and bereaved caregivers of older adults/geriatric patients in (hospice) palliative care? After forming a scoping review team in the fall of 2020, the target population was defined as informal caregivers of older adults in a (hospice) palliative/end-of-life care setting who have experienced grief and bereavement. Any interventions available for grief and bereavement in the Canadian context were explored. Secondary questions of interest were:
Who can benefit from formal grief and bereavement care? What is the efficacy of these interventions? Are there differences in the effect of interventions for those with ‘normal’ grief, those at risk for complications, and those with complicated grief? When should bereavement care be offered? Who should provide grief and bereavement services/interventions? What services should be offered for grief and bereavement? What do bereaved persons find useful/helpful?
Identifying Relevant Studies
The following electronic health and social science databases were searched: Ageline, Applied Social Science Index and Abstracts (ASSIA), Cumulated Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library, OVID Embase, OVID Medline, OVID PsycInfo, Proquest Sociological Abstracts, and Scopus. Key words/Medical Subject Headings (MeSH) such as “caregivers”, “grief”, and “interventions” were used in various combinations with Boolean operators (eg, AND, OR, NOT) when searching for relevant peer-reviewed scholarly articles and grey literature sources (see Supplemental Materials). The search strategy was refined with the help of a librarian and enhanced by conducting a trial search.
The grey literature search included the Proquest Dissertations & Theses GlobalTM database and stakeholder websites such as Canadian Hospice Palliative Care Association (CHPCA) and Canadian Virtual Hospice (CVH), alongside government websites. The selected resources were searched using Advanced Google, the website search engine, and hand searching where necessary.
Study Selection
Six independent reviewers [AA, AH, CT, MCB, NS, SL] initially screened the scholarly articles for the review, based on their titles and abstracts. The criteria for inclusion were: English language, conducted in Canada, and focused on interventions, strategies, or services offered in geriatric (hospice) palliative/end-of-life care settings to support informal caregivers through grief and bereavement. Two reviewers screened each article.
Three independent reviewers conducted a review of the grey literature [AM, IM, MB]. Articles identified as relevant were then included for full text screening along with the scholarly literature.
Both scholarly and non-scholarly articles that were selected after the initial screening process were subsequently evaluated by eight independent reviewers [AB, AW, CT, IM, MCB, MB, NS, SL], based on the complete text of the article. As in the previous stage, two reviewers screened each article. Throughout the entire screening process discrepancies were resolved through discussion with the full team.
As per Arksey and O’Malley's framework, 14 study design was excluded as a criterion for inclusion to capture the breadth of the field. The period for inclusion was from January 2000 to October 2020 to stay as current as possible.
Charting the Data
Two independent reviewers [MB, MCB] completed the data extraction and input. The extraction table identified the following areas of study: Purpose, sample and setting of care, study design, outcome measures, findings, themes, and practice/policy/research implications (see Supplemental Materials). The themes and subthemes identified were iterated upon before, during, and after the charting process by the whole team to ensure applicability and adherence to the interventions and intervention outcomes.
Collating, Summarizing, and Reporting the Results
Since the aim was to compile all existing literature related to the topic, no appraisal of the quality of the evidence was conducted. 14 Final themes were determined by the team after review of the scholarly and grey literature in the extraction table. Themes that occurred frequently and/or were highly relevant to the overall scoping review were identified via thematic content analysis 17 and cross-referenced with the research questions.
Results
Initial selection results from searching the academic and grey literature yielded 33,006 results (Figure 1). After deduplication, articles were filtered out by eliminating those published before the year 2000. Proceeding this filtering, the titles and abstracts of the remaining studies were reviewed against the selection criteria. In total, 358 articles were selected for full text review. During the full-text stage, 13 reviews were manually searched for references, however no additional articles were identified. Following full text review, 18 articles were selected for inclusion.18-35 Figure 2 displays the organization of themes and subthemes which were finalized after completion of the extraction table. The three main themes that emerged from this process were: (I) Classification of the intervention, (II) Format of the intervention, and (III) Intervention target.
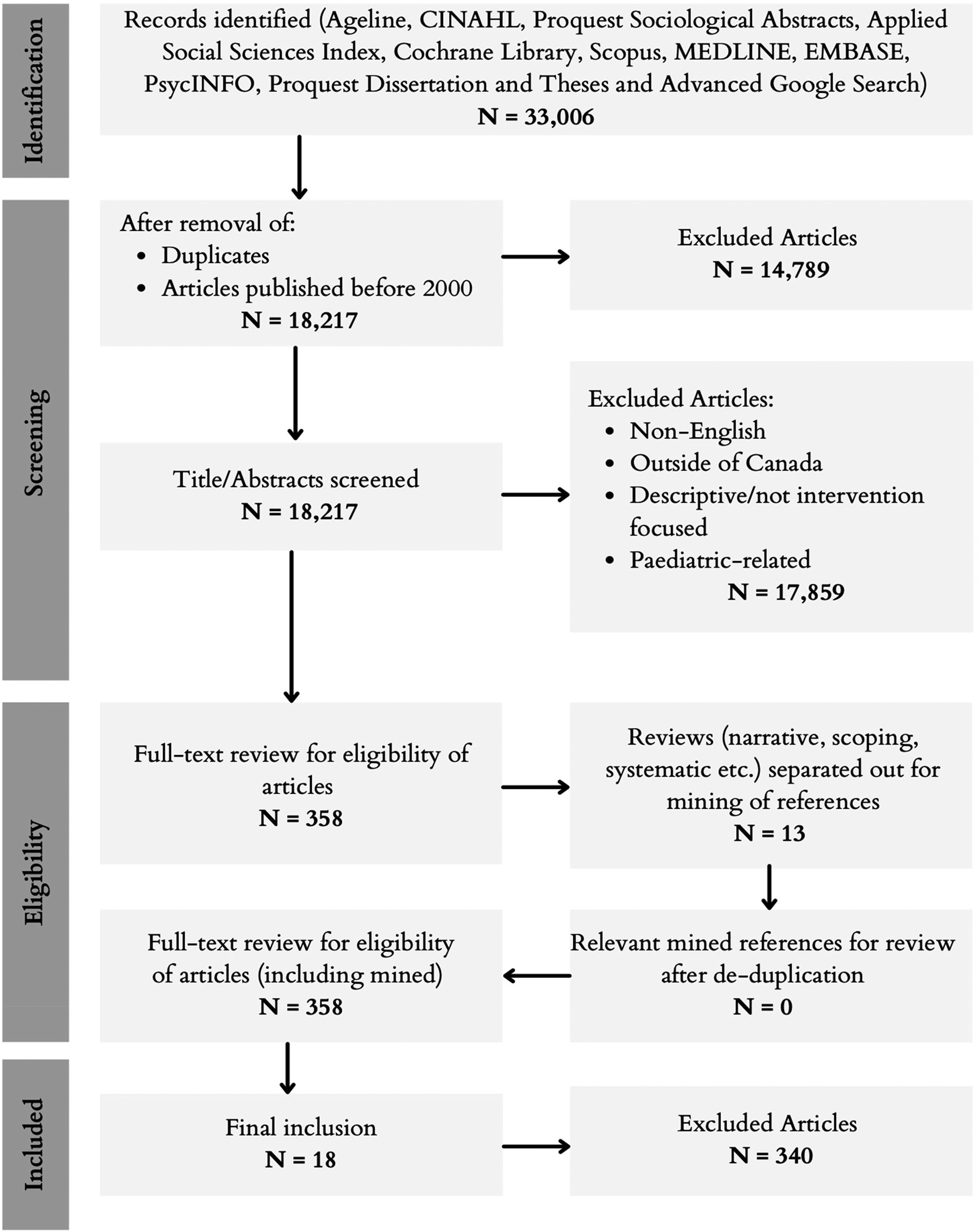
PRISMA flow chart.
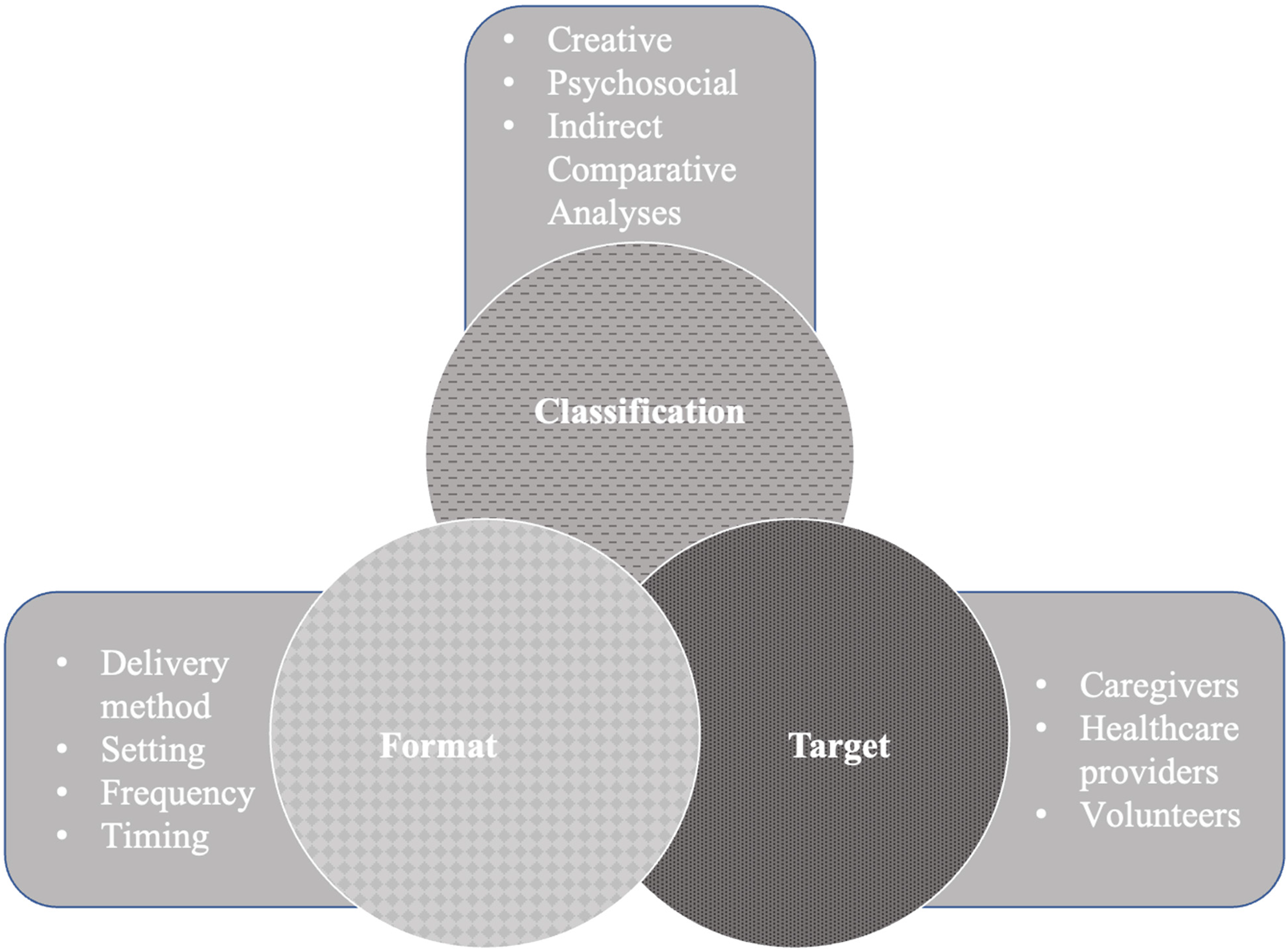
Themes and subthemes.
I. Classification of Intervention
Classification of intervention refers to the content of which the intervention consists. This section will describe interventions based in creativity, grief and bereavment education, the provision of psychosocial support, and comparative analyses of bereavement programs.
Creative interventions
This section speaks to the use of interventions based in creative activities to support grieving caregivers. In total, thirty-nine percent (7/18) of articles described creative interventions.19,21,23-25,29,35 This included art therapy,19,25,29 music therapy,23,24,35 and written interventions. 21
Art Therapy
Seventeen percent (3/18) of articles reported the use of art therapy in helping caregivers during periods of grief.19,25,29 The incorporation of art into caregivers’ bereavement experiences was reported to exemplify the legacy of the deceased.19,29 This supported caregivers throughout their grief, as it provided a positive attachment to the specific artifact, as well as acted as an immortal keepsake through which their loved one's memory could live on. 25 In one study, the use of personalized casting of the patient's hands was used as a tool to help guide caregivers in a future without the deceased. 29
Music Therapy
Seventeen percent (3/18) of articles discussed the use of music therapy interventions to support caregivers in their bereavement experience.23,24,35 One study examined ‘The Singing Well Group’, a form of music therapy that engaged grieving individuals in a therapeutic vocal experience, in hopes of fulfilling their unique and changing needs throughout their bereavement process. 35 Participants reported feelings of joy and renewed self-awareness that enabled the continuation of their grieving process and helped them move on after the death of their loved ones.23,35
Written Interventions
One article (6%, 1/18) examined a written intervention. 21 This written intervention enabled participants to focus on their thoughts, emotions, and daily activities. The intervention group in this study showed a statistically significant increase in restoration-oriented coping. This suggests the intervention may be effective in supporting grieving caregivers to find balance between grieving and moving forward in their lives. 21
Educational interventions
In total, twenty-two percent (4/18) of articles described educational interventions used to understand how to most effectively support caregivers during bereavement.26-28,33 These educational interventions, such as handbooks and learning modules, provided information on the different states of grief, and techniques to best support an individual during the bereavement process.26-28,33
Psychosocial interventions
In total, seventeen percent (3/18) of articles discussed caregiver bereavement support tools classified as psychosocial interventions.22,31,32 This included both spiritual care interventions 32 and support groups22,31 to address the needs of grieving caregivers.
Spiritual Care
Six percent (1/18) of articles explored the effect of a spiritual intervention on the bereavement experience of grieving caregivers. 32 A spiritual care provider was integrated with the palliative care team to provide standardized routine care, with an additional layer of compassionate support for the caregivers as they experienced the process of bereavement. Participants utilized the spiritual care practitioners as an additional source of grief-related materials, and reported the practitioner to be an individual with whom they felt they could openly speak with about their loved ones and their end-of-life experiences. 32
Support Groups
Eleven percent (2/18) of articles examined the use of support groups for bereaved caregivers.22,31 One study examined the impact of meaning-based group counselling on the bereavement experience of grieving caregivers. 22 Consistent attendance to this type of support group was seen to strengthen participants’ abilities to not only re-establish their psychological well-being during bereavement, but to also find benefits in reconstructing the identity of the deceased. 22 In another study, participants revealed that within therapeutic support group settings, they felt safe enough to share their feelings and to discuss some of their most pressing concerns. 31
Indirect comparative analyses
In total, eleven percent (2/18) of articles were indirect comparative analyses to support bereaved caregivers.18,34 The result of one study's creation of a bereavement program and service map enabled the comparison of existing services over four years. 34 Using publicly available information, this study demonstrated the considerable growth in the number of bereavement programs and services across Alberta. 34 In another study, a comparative analysis of caregiver trends shed light on the current climate of social, cultural, and political perspectives surrounding death and dying in Canada. 18
II. Intervention Format
Intervention format consists of the logistical aspects of the intervention, including the delivery channel, setting, frequency, and stage.
Delivery
This section speaks to the various delivery channels used to provide grief and bereavement support. Seventy-seven percent (14/18) of articles specified a particular delivery channel for the intervention described.18,19,21-29,31,32,35 This included interventions that were delivered over the phone, the Internet, and in-person.
In-Person
Fifty percent (9/18) of articles described interventions to be delivered in-person.19,21-26,29,35 This included many creative interventions, that might not conveniently lend themselves to remote delivery (eg, music or art therapy).21,23,24,29,35
Online
Eleven percent (2/18) of articles described interventions that were delivered over the Internet.28,31 Both of the interventions described were offered by CVH. The first was a synchronous support group facilitated by a counsellor, offered to eligible caregivers in both rural and metropolitan areas. Participants in this support group reported that the anonymity and privacy of an online intervention were of great value, and provided them with a sense of emotional safety. 31 The second article described the various informational resources available through the CVH website. 28
Telephone
Eleven percent (2/18) of articles described interventions that were delivered over the phone.27,32 One of these was a phone call from a spiritual care provider after the patient's death. This call provided the opportunity for the spiritual care provider to offer bereavement support in the form of compassionate enquiry and listening. 32 The other article described telephone check-ins offered by volunteers at a palliative care organization. The article was a training manual for these volunteers, that advised them on how to best offer support for grieving caregivers over the phone. 27
Setting
Sixty-one percent (11/18) specified a particular setting for delivery of the intervention.19,21-27,29,32,35 These were divided somewhat evenly between the care setting and the home.
Care Setting
Thirty-three percent (6/18)19,22,25,26,29,35 of interventions described were based in a specific care setting. This included hospitals, long-term care homes, and hospices. Twenty-two percent (4/18) were delivered in the hospital.19,22,25,29 One was delivered in a long-term care home, 26 and the last was delivered in a hospice. 35
Home
Twenty-eight percent (5/18) of interventions described were delivered in the home.21,23,24,27,32 This included interventions that were delivered over the phone,27,32 as well as music therapy delivered by a home hospice program.23,24 One of these interventions was writing-based, and self-administered. 24
Frequency
Sixty-seven percent (12/18) of the articles described a specific frequency at which the intervention should be administered.19,21-27,29,31,32,35 Interventions were either delivered at a single point in time, or on an ongoing basis.
One-time
Twenty-eight percent (5/18) of articles described interventions that were administered on a single occasion.19,25,26,29,32 Three of these were interventions with a tangible component, including the casting of hands, provision of keepsakes, and gifting of commemorative paintings.19,25,29 The other two were interventions introduced by the hospital or long-term care home to facilitate connection with the bereaved caregiver.26,32
Ongoing
Thirty-nine percent (7/18) of articles described interventions that were administered on an ongoing basis.21-24,27,31,35 These included music therapy, a writing intervention, ongoing check-ins from hospice volunteers, and both in-person and online support groups. Several of these reported promising efficacy results, demonstrating the value of providing support throughout the grieving period.21-24,31,35 Support groups reported high levels of continued attendance, demonstrating that ongoing support was desired and valued by caregivers.22,31
Timing
Seventy-two percent (13/18) of articles described a specific time at which the intervention be administered, relative to the death of the patient.19,21-27,29-32,35 One intervention was provided throughout the process, both before and after the death of the patient. This was an intervention to provide the caregiver with a keepsake at the end of the patient's life. 25
Pre-Death
Thirty-three percent (6/18) of the articles described interventions that were provided before the death of the patient.23-25,29-31 This included music therapy, the provision of physical artefacts, online support groups, and grief screening tools. The provision of physical artefacts involved the patient, providing an opportunity for legacy-building.25,29 These pre-death interventions provided a valuable opportunity for relationship building with the patient and caregiver.23-25,29
Post-Death
Forty-four percent (8/18) of the articles described interventions that were provided following the death of the patient.19,21,22,25-27,32,35 This included both creative and psychosocial interventions, such as art therapy, music therapy, writing, support groups, and check-in phone calls. In some cases, these interventions provided an opportunity for remembrance of the patient, validated caregiver emotions, and provided a way of moving forward.19,21,22,25,35 These interventions also acted as opportunities to refer the caregiver to further resources if necessary.27,32
III. Intervention Target
It was noticed that articles on grief and bereavement interventions targeted three major stakeholders in palliative care. The studies and reports not only described interventions to directly support caregivers during bereavement, but also interventions to inform healthcare professionals and volunteers.
Caregivers
Seventy-eight percent (14/18) of articles described interventions to be delivered directly to informal caregivers.18,19,21-25,28,29,31-35 These caregiver-focused articles ranged from studies assessing effectiveness and/or caregiver satisfaction with a given intervention,19,21-25,31,32,35 to more descriptive articles that provided an overview of one or more interventions.18,22,28,30,35 These descriptive articles included a review of online resources, 28 an overview of a hand casting intervention, 29 and a description of the role of death doulas in Canada. 18
Healthcare professionals
Twenty-eight percent (5/18) of the articles described interventions designed to educate and inform healthcare professionals, such as physicians, nurses, long-term care staff, and social workers.20,26,28,30,33 Two of these overlapped with articles that also focused on interventions that targeted informal caregivers.28,33 These articles described interventions that would improve the knowledge and skills of professionals to handle the grief of their patient's caregivers. One article focused specifically on providing a tool for social workers to evaluate and engage the caregiver in discussions about grief. 30 Another focused on effective interventions available for healthcare professionals in long term-care homes to develop open lines of communication with grieving caregivers. 26 The final article described how healthcare professionals could contribute to an improved experience of grieving by working alongside communities to develop grief literacy initiatives. 20
Volunteers
One article (5%, 1/18) was an intervention itself to educate and inform volunteers that were providing supportive phone calls to recently bereaved caregivers. 27 This article served as a handbook that volunteers could refer to when providing support. The handbook outlined definitions, common reactions associated with grief, and how a volunteer should handle different situations that may arise. This included the protocol that volunteers should follow, and other bereavement resources that volunteers could direct caregivers towards. 27
Discussion
The common themes that emerged in studying interventions for grieving caregivers were: (I) the classification, (II) format, and (III) target of the intervention.
The classification of the intervention referred to the actual content of which the intervention was composed. The format of the intervention described logistical aspects, such as how and where it was delivered, who was delivering it, how often, and at what time. The intervention target referred to who would use and benefit from the intervention. This included caregivers, healthcare providers, and volunteers.
International perspective
The themes identified in this scoping review align with the international literature. Several American studies reported on the medium of delivery, with a particular focus on online and telehealth delivery.36-38 One study examined the potential of a Facebook group for bereaved informal caregivers. 36 The intervention allowed caregivers to interact with one another and share advice, and involvement in the group was found to correlate with lowered anxiety and depression. This demonstrated the potential for online delivery, an increasingly common delivery channel 36 that is particularly relevant within the context of the COVID-19 pandemic.
Outside of North America, additional articles supported the theme of “types of interventions” identified in this scoping review. A German study described the effectiveness of bereavement anniversary cards, used to provide follow-up support to bereaved caregivers and family members. 39 Overall, the study found that caregivers reacted positively to the cards, and that there was potential for similar interventions. An Australian study provided evidence for compassionate communities, suggesting that environmental modifications might be an effective way to support caregivers dealing with grief and bereavement. 40 The wide array of international research on grief and bereavement interventions provides an avenue for further investigation into which resources might be beneficial in the Canadian context.
Practice implications
Overall, there was a call for increased clinical attention to the grief issues faced by caregivers. 30 Specific suggestions included education and training for social workers so that they can provide grieving caregivers with appropriate support. 30 Caregiver grief may be challenging to recognize in clinical practice, and may not be frequently recognized by typical burden scales. 41 Previous work has identified difficulties in differentiating depressive symptoms from grief. 42 This highlights the importance of accurately diagnosing grief in informal caregivers, so that healthcare professionals are able to prescribe the appropriate interventions. The development of accurate screening tools to predict grief in informal caregivers will be required to achieve this goal.30,41 It is evident, based on the variety of interventions explored in this scoping review, that there are several diverse avenues to address caregivers’ needs for support. This includes music therapy, spiritual care practices, and the use of keepsakes.23,25,32,35 Interestingly, some articles suggested that collaboration between specialized providers such as social workers and spiritual care practitioners, might have beneficial effects on the experience of caregivers receiving the intervention.32,35 Individuals and organizations involved in the creation of programming should consider potential accessibility issues, as one study found that high quality support groups were not widely available. 31
Policy implications
A societal paradigm shift is needed in the way that grief and bereavement are perceived and addressed. 43 Caregivers have taken on increasing responsibilities, and need to be recognized as a vital link between settings. Programs that support grieving individuals should be considered an important health promotion effort as they help to prevent illness. 34 There is a need for inclusion of grief and bereavement services into hospice and palliative care service provision to increase the support available to grieving individuals in institutional and community settings. The Canadian Grief Alliance has focused on addressing this issue through the call for a National Grief and Bereavement Strategy which aims to identify opportunities for improvement, increase grief services, raise awareness, and provide funding for more research in this space. 44 At the policy level, there is a need for increased funding to bereavement programming as they provide support for one of the most vulnerable groups in society. 34 It must also be determined whether funding is the responsibility of the individual, private organizations, or the governments. 18 Funding and financial support is not an isolated issue within the context of grief and bereavement but is common throughout the experience of caregiving. This need is even more prevalent for low-income individuals. 18
Research implications
Several studies examined future implications for research, and there were several areas of interest identified. A key implication among articles was the need for large-scale studies to investigate the effectiveness of interventions.19,21-25,28,32,35 The studies described in the included articles were mainly feasibility tests, and there overall is a limited understanding of the impact of these interventions. While the authors were able to gain some understanding of the potential benefits of each tool or intervention, there is clearly a need for rigorous, controlled studies to assess effectiveness 22 – including return on investment (RoI). This research would ideally facilitate the development of a defined set of evidence-based bereavement interventions. In addition to evaluating effectiveness, research towards the development of accurate screening tools is required to ensure that healthcare providers are able to prescribe the appropriate intervention. 41
This scoping review also demonstrated how ongoing intervention research has engaged many groups of people connected to caregivers, including healthcare professionals. These interactions often occur when attempting to evaluate a certain intervention, as has been seen throughout the selected articles. However, there are further benefits to engaging caregivers extensively throughout all stages of research, including during the development of interventions. Informal caregivers hold the unique position in their role as care provider and family member/friend, and frequently have differing opinions than healthcare professionals on the usefulness of resources. 45 There is immense potential and importance for future research to continue to engage caregivers in order to develop the most effective grief and bereavement interventions.
Grief interventions during COVID-19
Measures taken to reduce the spread of COVID-19 have had tremendous impacts on the ability to provide grief support to caregivers. For example, hospice providers have had to transition their programming online. Many programs have been successful in providing online support, but the potential for long-term changes to delivery methods must be considered to increase accessibility and reach.46,47 Notably, the pandemic has shed light on the need for accessible services, even outside of the pandemic context. 47 While the COVID-19 pandemic may have increased the number of individuals seeking bereavement support, it also presents program providers with an opportunity to create and improve upon services that address the needs of bereaved caregivers.43,47 Those seeking to provide support to grieving individuals must consider the unique impacts of the pandemic on the grief experience. Research suggests that the pandemic may result in rising complicated grief as the measures put in place in response to COVID-19 often leave dying individuals and their families separated during their final moments. 48 The pandemic has also stripped individuals’ ability to experience meaningful goodbyes by preventing cultural and social rituals associated with grief. 49 These are some of the many changes that will need to be considered when providing grief support to informal caregivers in the post-pandemic world.
Strengths and Limitations
Strengths of this study include the exploration of grief and bereavement interventions for informal caregivers offered in (hospice) palliative and end-of-life care settings in the Canadian context. Moreover, the use of the Arksey and O’Malley framework 14 allowed for a broad review and synthesis of the literature. Furthermore, the use of both academic and grey literature enabled the capture of a variety of data sources.
There are several limitations for this scoping review. It is noted that the lack of quality assessment of the included articles can be a limitation. However, in keeping with the recommendations from the Arksey and O’Malley framework, 14 this was omitted due to an effort to ascertain a wide breadth of articles, to better understand the full landscape of grief and bereavement interventions for informal caregivers in Canada. A second limitation is the inclusion of only English literature despite Canada being a bilingual country. This was due to the limited French capacity within the research team and a lack of funding to engage translators. Another limitation is the inclusion of articles that were only published in the 2000s in order to gather the most recent articles regarding the topic. Finally, this review is limited in its ability to provide an understanding of the impact of the interventions described because few articles report the direct impact of the intervention.
Conclusions
This scoping review provided an overview of the interventions that have been used or studied to support informal caregivers of palliative patients in navigating grief and bereavement. As the need for informal caregivers increases and their numbers rise, it is important to better understand their needs. The results described here show that although there are a diverse set of interventions that have been studied, there is a need for further evidence and more robust studies to evaluate effectiveness. It is necessary for healthcare providers, policy makers, and researchers to acknowledge the importance of providing evidence-based interventions for informal caregivers facing grief and bereavement. Interdisciplinary collaborations between these individuals will be required to further develop, evaluate, and scale these interventions.
Supplemental Material
sj-docx-1-pal-10.1177_08258597221101826 - Supplemental material for Interventions for Grieving and Bereaved Informal Caregivers: A Scoping Review of the Canadian Literature
Supplemental material, sj-docx-1-pal-10.1177_08258597221101826 for Interventions for Grieving and Bereaved Informal Caregivers: A Scoping Review of the Canadian Literature by Carly Thrower, MHSc(c), Carol Barrie, CPA, Sharon Baxter, MSW, Meryl Bloom, MSc, Maria Carolina Borja, HBA(c), Anica Butters, HBSc(c), Deborah Dudgeon, MD, Ayeshah Haque, MHSc(c), Suzanna Lee, HBSc, Iqra Mahmood, HBSc(c), Mehrnoush Mirhosseini, MD, Raza M. Mirza, PhD, Kate Murzin, MPH, Ankita Ankita, MD, Neerjah Skantharajah, MHSc(c), Christina Vadeboncoeur, MD, Andrew Wan, MHSc, and Christopher A. Klinger, PhD in Journal of Palliative Care
Footnotes
Acknowledgments
The authors would like to thank Kaitlin Fuller, MLIS from the Gerstein Science Information Centre, University of Toronto for lending her expertise towards the refinement of the search strategies used in this review. The authors would also like to extend thanks to Elaine Lung, HBA for her assistance with logistical aspects of the scoping review.
Author Contributions
Conception of the work: AW, CAK, CT, CV, DD, KM, MM, NS, RMM, SB. Initial data acquisition: AA, AB, AH, AW, CAK, CT, IM, MB, MCB, NS, SL. Data analysis: AA, AB, AH, CAK, CT, IM, MB, MCB, NS, SL. Datainterpretation: All. Drafting of the initial manuscript: AA, AB, AH, CAK, CT, IM, MB, MCB, SL. Revisions for critical content: AW, CB, CV, DD, KM, MM, NS, RMM, SB. All authors have seen and approved the final version of thismanuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.