
Abstract
Introduction
Maslach and Leiter defined burnout as, “…a psychological syndrome emerging as a prolonged response to chronic interpersonal stressors on the job. The three key dimensions of this response are an overwhelming exhaustion, feelings of cynicism and detachment from the job, and a sense of ineffectiveness and lack of accomplishment.” 1
Burnout is a well-known feature of healthcare work, co-occurring with long hours, verbal and physical workplace harassment, anxiety and depression and compassion fatigue.2,4 However, end-of-life (EOL) work challenges staff members with the additional and unique stress burden of caring for people who are dying, adding to the usual stressors of patient care the constant contact with death; 5 interactions with grieving and distraught family members; and, the difficult process of supporting individuals, sometimes frightened, in great physical or emotional pain, through the dying process.6,7 Stressors that may be encountered by any healthcare professional on occasion are omnipresent in EOL care; specifically, those to do with the dying process and the emotional experiences common to those who attend at death.
Discussing burnout in critical care professionals, Moss et al. 8 listed four categories of risk factors for Burnout Syndrome 1) personal characteristics, 2) organisational factors, 3) quality of working relationships, and 4) exposure to EOL issues. Another study found that EOL professionals experience an average of seven patient deaths per month. 9 Repeatedly experiencing patients’ deaths has been shown to affect healthcare providers in particular ways with increased mortality salience affecting death anxiety, 10 with occasions of moral distress, vicarious traumatisation 11 or secondary traumatic stress (STS), grief and bereavement, and post-traumatic stress. 12
While some EOL professionals have experienced great emotional and spiritual rewards in EOL care, 13 there are also perpetual experiences of grief, alienation, frustration, moral distress and helplessness, which, too often unchecked and unacknowledged, lead healthcare professionals to states of burnout, to compassion fatigue and to abandoning their work for less demanding employment.8,11,14,15 A recent survey of the American Academy of Hospice and Palliative Medicine 14 calculated the prevalence of clinicians’ burnout at 38.7%. A global review of palliative care surveys 16 reported burnout rates (by country) at 24% - 50%.
Researchers have discovered connections between trauma and death anxiety, and secondary traumatic stress and burnout.17,18 Trauma has been linked to increased death anxiety 12 and death anxiety has been shown to negatively impact EOL staff's interactions with and care for, dying patients and their families. 10 A descriptive study 9 of 216 nurses found 78% of them at moderate to high risk of compassion fatigue. Regression analysis showed that 91% of the variance of the risk of compassion fatigue was due to trauma, anxiety, life demands, and excessive empathy that blurred professional boundaries.
Researchers agree on the pressing need to investigate methods for reducing stress and burnout in EOL care staff members.2,14,19 Hospice UK reports, “Patient care will suffer if staff are not cared for.” 20 EOL staff experience conditions similar to other health care professionals, but research demonstrates that EOL staff members are additionally challenged by a work life that elicits the continuous psychological discomfort of facing death while witnessing intractable conditions of suffering—all this in a medical tradition that posits death as the ultimate enemy and makes little provision for coping with it. 21 Some hospices are turning to mindfulness practices to help staff members find healthier ways of dealing with the many challenges—professional, ethical, interpersonal and intrapsychic—of working in the presence of death.13,22,23 While general health care settings have used mindfulness teaching to help staff members avoid burnout and increase compassion,24,26 EOL interventions need also to address the unique suffering of those working with people who are dying.2,6,9 Mindfulness, with its focus on the present, on teaching how to experience strong emotions and difficult situations without being overwhelmed by them, may be able to provide this important additional support.7,27,28
Mindfulness is, “the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally to the unfolding of experience moment by moment.” 29 Mindfulness-based stress reduction techniques are increasingly used to alleviate stress and reduce burnout, for staff members as well as patients.25,26,30 Mindfulness, focusing on the present moment rather than ruminating on the past or anticipating the future, has been shown to reduce stress, anxiety and burnout in clinical and non-clinical populations.22,27,31
MBSR and MBCT are being used to reduce EOL workplace stress and anxiety.15,25,32 Decentering has been called an insight; an outcome of shifting perspective. 33 Lebois et al describe decentering as a way to escape perseveration that plunges the mind into imagining not only the worst outcome, but to feeling that it's happening in the present moment. They define it as, “The realization that thoughts, feelings, and reactions are transitory patterns of mental activity, that they are not necessarily true representations of the self and events, and that they are not actually happening…”. 33 MBIs can help employees “de-center” from unhealthy emotional perspectives as they learn to encounter stressful work-related events with less reactivity.33,34 MBIs may provide accessible means of reducing stress and burnout as well as increasing wellbeing in EOL professionals.
MBIs tailored to EOL professionals are attempting to help them respond healthily to EOL workplace stressors. 35 Depner et al. 28 identified Mindful Self Care and meaning-making as the most important factors in the quality of life of palliative care workers. EOL workers need support processing and integrating their experiences of patients’ deaths. 36
A recent systematic review of the effect of mindfulness interventions on burnout in (general) healthcare professionals contrasted the promising results of studies in the area, with the lack of useful evidence in the literature, calling for more precise methodology and reporting. 26 A systematic review on the impact of mindfulness on death anxiety in EOL professionals, after applying reasonable search standards, found not a single study met the inclusion criteria. 37 Mindfulness-based studies in EOL workplaces to date have been largely uncontrolled, qualitative, and anecdotal, with small numbers of participants and interventions widely varied in methodology. 38 MBI's for EOL professionals are not yet being planned, documented and reported sufficiently to create a useful body of research, to forward the work of promoting the wellbeing of this unique population.
This review is an attempt to identify and evaluate the empirical evidence so far accumulated as to the effects of mindfulness-based interventions on the wellbeing of EOL professionals.
The specific aims of this systematic review are to: 1) identify and describe published research of projects using MBIs for EOL professionals; and, 2) to evaluate the effectiveness of MBIs on EOL professionals’ levels of well-being and stress.
Method
A systematic search of literature was undertaken to identify MBIs for staff members in EOL care settings. The following electronic databases were searched: EBSCO, ERIC, PubMed Central (PMC), PsycInfo, Web of Science, from the inception of each database until February, 2022.
The following search terms were used: (mindful OR mindfulness) AND (hospice or palliative care or EOL care or terminal care) AND (staff or nurses or healthcare professionals or professionals). While there is an increasing body of research on interventions for patients in palliative care and hospices, and numbers of articles on family caregivers for such patients, the literature on interventions for staff members are relatively rare. Adding the keywords related to the healthcare occupations helped us target the population of interest. (That said, a large number of the articles focussed on patients and caregivers appeared in searches and were excluded from the review.
Only peer-reviewed journal articles were included. Articles written in languages other than English were not excluded as long as it was possible to obtain an English translation.
Criteria for Inclusion / Exclusion
Population
We included studies carried out with any type of healthcare professionals (nurse, physicians, respiratory therapists, social workers, care workers, etc) working primarily or exclusively in dedicated EOL settings—hospice or palliative care units. We narrowed down the universe of searchable articles on healthcare providers by limiting search terms to those in hospice, palliative care and end-of-life care, and then expanded the search within that realm by capturing as much as possible the wide range of occupations within end-of-life milieus. We did so by purposely using broad occupational categories rather than attempting to itemise particular occupations. In this way, we located occupations we might not have otherwise thought of (e.g., chaplains).
Excluded were settings where EOL care is not the primary function of the setting—the usual expectation is that most patients are not admitted to die—A&Es, ICUs, critical care wards, old age homes and emergency services, such as policing or fire services. As the focus of this review was on those employed (doing paid work) in EOL careers, volunteers, caregivers, family members, students and patients were excluded. A lack of pertinent research means we cannot definitely assert that there are known differences in the stressors of volunteers versus family caregivers versus paid employees: however, this review is focussed on those making their professional careers in end-of-life care.
Type of intervention
Any intervention denoting mindfulness as a primary component of at least one experimental group was included; therapeutic modalities containing a mindfulness component along with other, equally-or-greater-weighted components (e.g., Dialectical Behaviour Therapy (DBT) and Acceptance and Commitment Therapy (ACT) were excluded, as mindfulness was merely a portion of multi-modal therapies focussed on behavioural change.)
All delivery systems were included—face-to-face, self-help, online, video trainings, conducted in or outside of working hours. Interventions could be of any length and any duration.
Comparator(s) / Control
As long as the study was an empirical one, with quantifiable results, any type of comparison group would be acceptable.
Outcomes
Any outcomes, physical or mental, were considered, as long as they related to aspects of mindfulness, burnout or professional quality of life.
Study Design
This review only considered empirical studies, reporting quantitative results, although it should be mentioned that some of the studies reviewed contained qualitative analyses of journals, interview questions and other written forms of participant feedback.
Study selection
Titles and citation information were downloaded to Mendeley referencing software, after which, Mendeley was run to check for duplicates. Afterwards, titles and citation information were placed into an Excel spreadsheet, annotated with the database where each article was located. It became apparent that Mendeley had not found all the duplicates: the articles were sorted by title and further duplicates, along with artefacts from the searches (e.g., search terms and dates of searches), removed by hand.
Articles were first reviewed by titles. When the title did not clearly exclude the article, abstracts were read, and finally, the researcher obtained and read the full text of the articles whose abstracts left open the question of inclusion. Reasons for exclusion were marked as “Book Review, Report, Systematic Review, Not Hospice, No RCT, Wrong Topic. Potential inclusions were marked HOSPICE WORKERS and RCT: to be included, a study had to be an intervention targeting paid hospice/palliative care professionals, with quantifiable results. If randomised control trials formed part of the literature, we planned to conduct a meta-analysis with the data from those studies.
Results
The initial database searches yielded 11,812 results: after duplicates were removed, 8701 remained. Records failing to fit the eligibility criteria numbered 8678. Twenty-three articles were screened in full-text: twelve were identified as involving MBIs for EOL professionals. Of these twelve studies, six provided quantitative results, and were included in this review. One piloted a randomised control trial; 4 others were non-randomised pilots and one was called a feasibility study. All attempted to address burnout (and related conditions) in EOL professionals, and all included participants in a variety of occupations (physicians, nurses, social workers, psychologists, etc) One study 39 required participants to have some medical background, and to be able to work in a group process (the authors did not specify how that was determined.) (Table 1)
Prisma Flow Diagram. 40
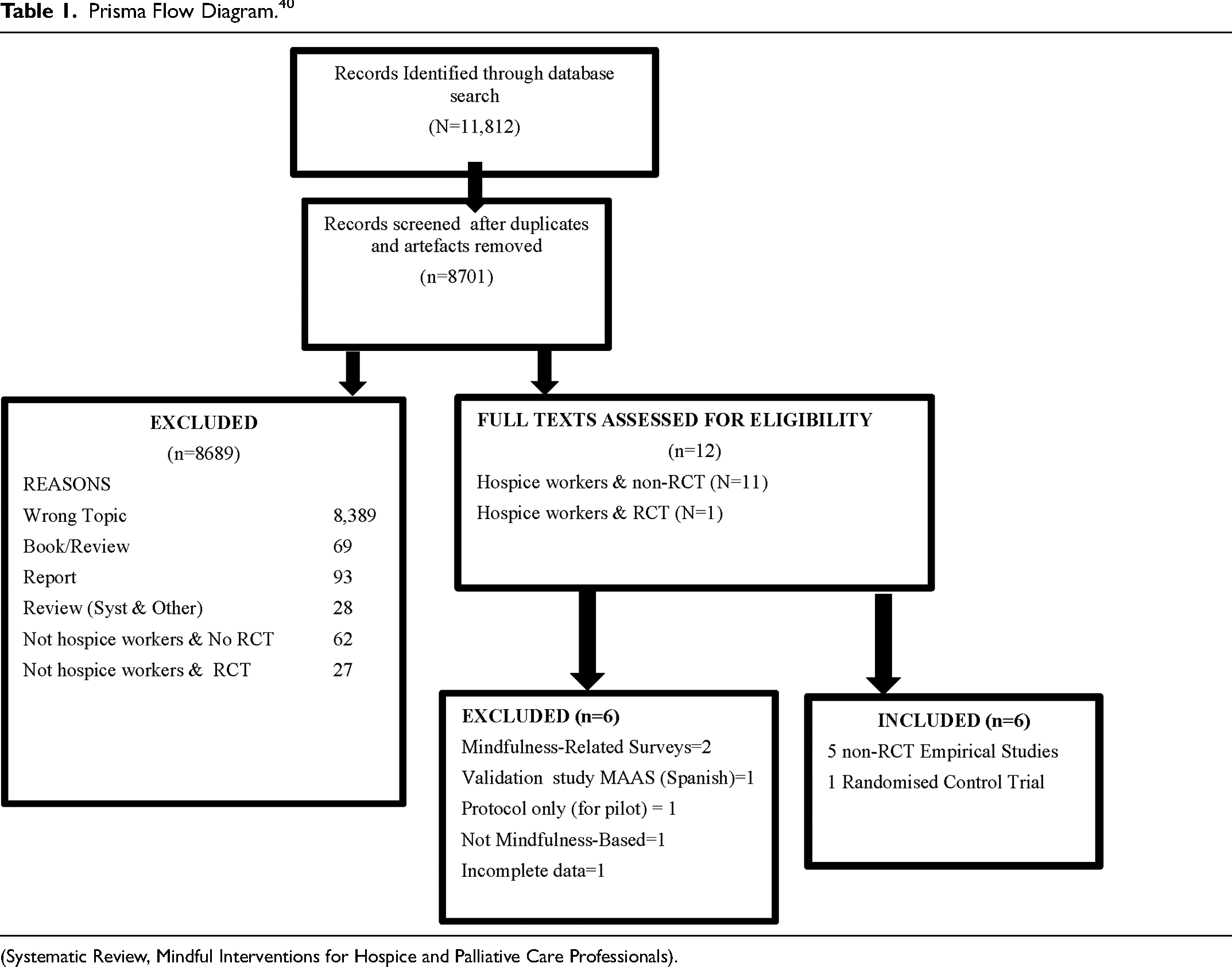
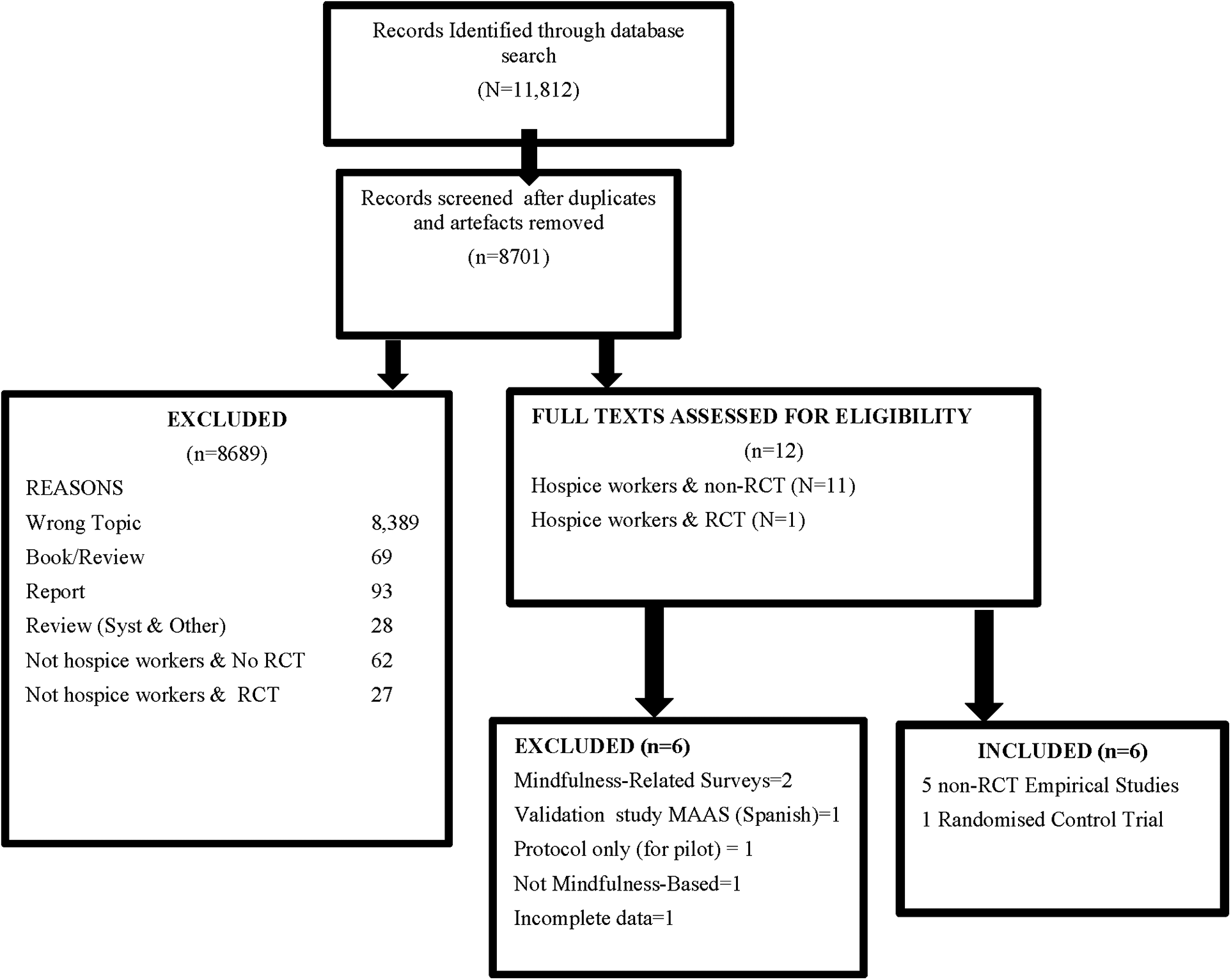
(Systematic Review, Mindful Interventions for Hospice and Palliative Care Professionals).
Studies evaluated interventions’ effects on mental health symptoms and signs of wellbeing (1), self-care and self-compassion (3), resilience (1), stress reduction (1), mindfulness (1), professional quality of life (1), burnout and risk of burnout (2), and empathy (1). Five of the six interventions were mixed-methods, incorporating psychoeducation, meditation, group discussion, journaling, communication, and mindfulness skills. One study, 41 the only RCT, used an unspecified mindfulness intervention and a comparison group of a narrative intervention (poetry reading).
Four studies were conducted in the USA; one in Germany and one in Spain. Studies reported low participant numbers, ranging from n = 13 to n = 43. Most participants were women (69% - 95%), and in the four studies that reported average age, participants were between 40.9 years and 53 years of age. Of 168 participants across all studies, 157 (93.4%) were reported by occupation. Nurses (41.7%), physicians (17.9%) and social workers (16.1%) accounted for 75.6% of participant occupations, with other reported occupations each accounting for less than 5% of the total.
All studies were pre-post designs, with two35,39 also using assessments at intervention midpoint. Only one study used the recruitment process to ask participants to commit to attend at least 4 of 5 sessions. Three studies22,23,41 included some type of qualitative data (interviews, journals), used to track time spent in mindfulness activities away from work, reactions to the intervention, and satisfaction ratings.
Two studies were grounded in Psychological Flexibility Theory.35,39 No other studies mentioned a theoretical base other than mindfulness. One study used the traditional Buddhist terms for different types of meditation taught (“metta” and “tonglen”). 22 The others used secular language (eg, loving-kindness, compassion). Only one study 22 included a physiological outcome measure (cortisol).
Intervention training times ranged from 90 minutes 41 total to around 25 hours. 22 The time period of the studies ranged from 1.5 42 to 5 months. 23
Outcomes
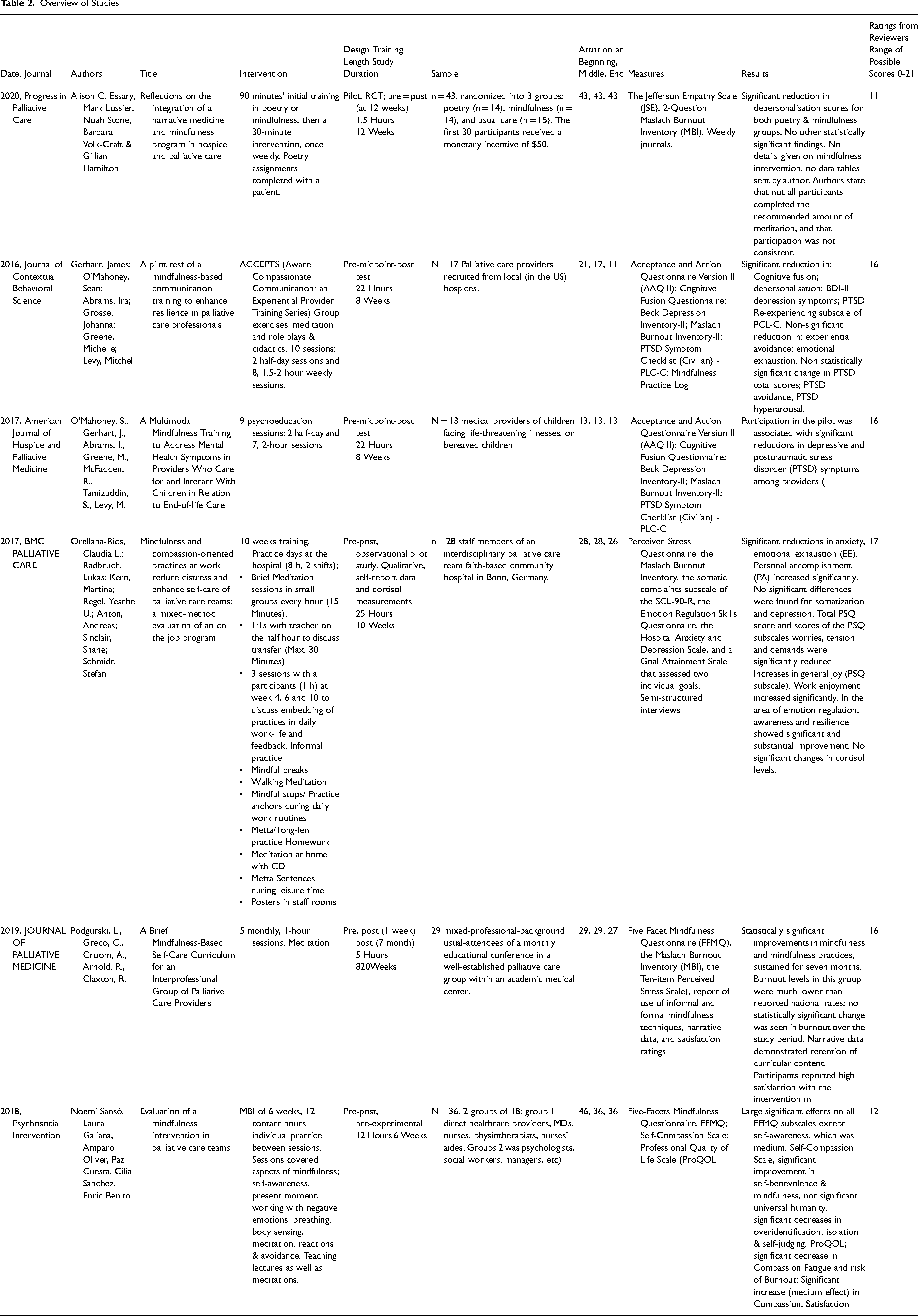
Outcome measures assessed depression, anxiety, stress, PTSD, burnout, quality of life, cognitive fusion and experiential avoidance. In all, researchers used 17 different measures. Five researchers used one of two versions of the Maslach Burnout Inventory, and two researchers used the Five Factor Mindfulness Questionnaire (FFMQ). The two researchers basing their work on Psychological Flexibility Theory used four of the same measures—the Beck Depression Inventory (BDI), the Cognitive Fusion Questionnaire (CFQ), the Acceptance and Action Questionnaire (AAQII) and the PTSD (Post Traumatic Stress Disorder) Symptom Checklist. The measures are itemised in Table 2.
Overview of Studies
Attrition
Some participants left the studies prematurely on learning the aim of the study, 35 or feeling they did not have the time to participate. 22 Two of the 6 studies35,42 reported losing participants in the early stages of the study; one just after recruitment because 4 participants had expected a traditional course in MBSR, and one 23 for various reasons such as perceived time constraints and maternity leave, resulting in a loss of 10 potential participants. Of all 192 of those initially recruited, 160 completed the post-intervention assessments, an 83% completion rate. Attrition rates are itemised in Table 2.
Comparing Results
All six studies found some positive results, reporting statistically significant results in 34 of the 69 variables totalled in 17 outcome measures. Five studies reported significant results in 29%–44% of measured variables. All effect sizes reported in this study were calculated by the original authors. Statistical significance and all reported p-values and effect sizes for scales and subscales are itemised in Table 3.
Scales & Subscales ; Statistical Significance ; P-Values; Effect Sizes.

Sanso's study used Pillai's Trace (n2 rather than Cohen's d).
Cutoffs for Pillai's Trace are .01 (small); 0.6 (medium) .14 (large).
Cohen's d cutoffs: .2 (small); .5 (medium); .8 (large).
One study 42 reported statistically significant results in 13 of 14 dependent variables. However, participants were divided into two occupational groups: “health” (eg, physicians, nurses, nurses’ aides) and “non-health” (e.g., social workers, occupational therapists, psychologists). No particular reason or theoretical base was given for the decision, and no significant differences were found between the two groups on any measure, suggesting homogeneity among participants.
Time/energy commitment
Interventions ranged from very low impact, with a brief, at-work training and an expectation of one, 30-minute workplace activity per week (not enforced and also not necessarily provided-for in the schedule), 41 to a commitment to practice, study and journal outside of work as well as attending on-site training.22,23,35,39
Self-Report Measures
Of the 17 measures used by the studies in this review, 6 were used by more than one. Five measures (Beck Depression Inventory-II (BDI), Cognitive Fusion Questionnaire (CFQ), Acceptance and Action Questionnaire (AAQII), Post-traumatic Symptoms Checklist (PCL), Five Factor Mindfulness Questionnaire (FFMQ) were used by two studies35,39 and 1 (the Maslach Burnout Inventory (MBI)) was used by five.22,23,35,39,41
The two studies which used the BDI, CFQ, AAQII and PCL both found statistically significant improvements in the score of the BDI, with medium effect sizes.35,39 One found statistically significant improvement in the CFQ total, also with a medium effect size.
On the PTSD Symptom Checklist (PCL), one 35 found a significant difference only in the PTSD Re-experiencing subscale. The other 39 reported only the PTSD total score as statistically significant with a small effect size (d = -.27).
Maslach burnout inventory (MBI)
Of the five studies which used the MBI or 2-Question MBI, 2 found statistically significant improvement in the depersonalisation (DP) subscale,35,41 with one 35 reporting a large effect size; the other 41 did not report the effect size. One study 22 reported significant improvements for Emotional Exhaustion (EE) and Personal Accomplishment (PA), with small effect sizes. To sum up, of the 15 burnout subscale scores reported across 5 studies, 4 subscales (26.7%) reached statistical significance.
Five Factor Mindfulness Questionnaire (FFMQ)
Two studies23,42 used the FFMQ to measure the results of the mindfulness-based intervention on factors of mindfulness. One 42 found statistically significant improvements in all five factors (observing, reacting, acting with self-awareness, nonjudging and non-reacting), with a medium effect size for acting with self-awareness, and large effect sizes for the rest. The other 23 found statistically significant improvements in observing, reacting and non-reacting at the post-test conducted 7 months after the study ended. (There were two post-tests in this study, conducted at one week and 7 months after the intervention). The authors of this study did not report effect sizes.
Cortisol
Only one study 22 included an objective physiological measure—cortisol tests. No significant differences were found.
Qualitative results
Three studies22,23,41 used qualitative information, in the form of interviews and journals. Two studies reported post-intervention satisfaction ratings of 93% 23 (obtained by a Likert-type scale of 1-5, with 4 and 5 being considered high satisfaction) and 76% 22 (obtained by post-intervention questions in interviews). Ninety-three percent 23 and 88% 22 expressed willingness to recommend the programme to a colleague. Ninety-six percent of participants in one study 22 said they would continue to incorporate mindfulness strategies into their workday, and 86% 23 indicated an interest in continuing to participate in regular, group-based brief guided meditations.
Two of the three studies using qualitative data found themes of increased connection with others, (patients, family members and colleagues), and all three mentioned the value of mindful pausing and self-awareness. Empowerment of self-care was a primary theme arising in one study, as well as reduced empathic distress. 22
Of the studies that asked participants to discuss or write about their reactions to the intervention, one listed general ideas 23 (called “lessons learned”), and one 22 reported a few (very moving) verbatim accounts of instances where mindfulness training helped them in the room when someone was dying.
Limitations of the observed studies—RCT
The single RCT in this review
41
obtained 1 of a possible 5 points on the 3-item Jadad scale. Participants were randomised into one of three conditions; there was no reference to double blinding of researchers and no mention of withdrawals or dropouts. It was reported (with no added detail) that some participants did not complete their assigned tasks. The study contained low numbers of participants and important design flaws. Some participants were paid; others were not. The poetry intervention required involving patients; the mindfulness intervention did not. Specifics of the interventions were not covered in the article, beyond the fact that both sets of participants were given 90 minutes’ training specific to the intervention. The author noted limitations including:
Self-selected participants Inconsistent and incomplete participation Confusion over how to complete the web surveys Holidays during the intervention period Discomfort with the poetry intervention.
Non RCTs
The remaining five studies’ limitations included, lack of comparison interventions, low participant numbers, varied interventions, and very little overlap in measures used.
All measures but one (cortisol) were self-report.
None of the studies investigated addressed issues related to death and dying such as grief, bereavement, secondary traumatic stress, death anxiety, mortality salience, or moral distress. Only two of the studies35,39 used a PTSD scale. No study investigated the concept of (and frequency of) a “good death”, and how the quality of each individual death experience affects the life and work experience of EOL professionals.
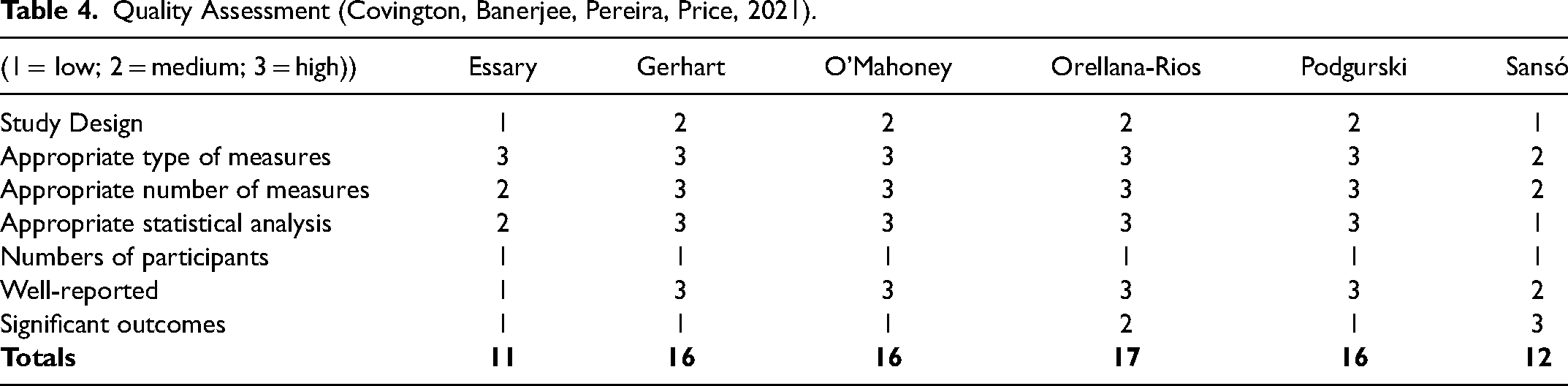
Given the variety of methods, measures and outcomes exhibited in the studies covered in this review, the authors felt it would be helpful to get a sense of the overall strength of each by comparing them on the quality of design, measures, statistics, outcomes and reporting. We created an assessment and rated each study by consensus on a 1–3 scale. We include the assessment as Table 4.
Quality Assessment (Covington, Banerjee, Pereira, Price, 2021).
We also conducted a Cochrane Risk of Bias Assessment, included here as Table 5.
Cochrane Risk of Bias Assessment. 43
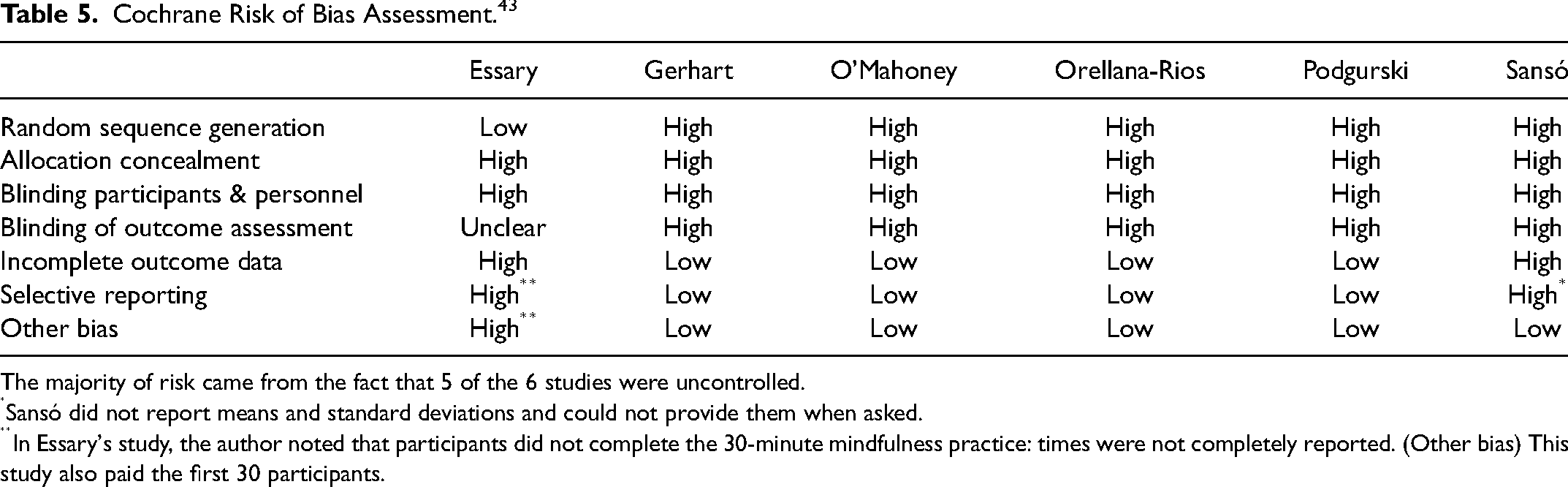
The majority of risk came from the fact that 5 of the 6 studies were uncontrolled.
Sansó did not report means and standard deviations and could not provide them when asked.
In Essary's study, the author noted that participants did not complete the 30-minute mindfulness practice: times were not completely reported. (Other bias) This study also paid the first 30 participants.
In sum, the scarcity of empirical studies on MBIs for burnout and related issues of EOL professionals indicates an important gap in the research. Research indicates there may be challenges particular to EOL professionals, and professional organisations and individuals are stating the need for effective interventions.21,24 While studies showed some positive results, to date, there is little useful empirical evidence regarding the effectiveness of MBIs for addressing burnout and associated stressors of EOL professionals.
Discussion
This review explored the literature concerned with the effects of mindfulness-based interventions (MBIs) on end-of-life (EOL) professionals. The original plan, to identify relevant randomised control trials and conduct a meta-analysis, was revised when only a single study was found to be a randomised control trial (RCT). Expanding the criteria to include studies that were not RCTs, we located five additional articles reporting quantitative results on MBIs for EOL professionals.
Results overall were generally positive, although small participant numbers and lack of comparison groups make it difficult to draw any strong conclusions. The one study showing statistically significant results in nearly every measure subscale 42 used a questionable design.
The Maslach Burnout Inventory was used by five of the six studies in this review22,23,35,39,41 one study 42 used the burnout subscale of the Professional Quality of Life scale (ProQOL). However, important stressors particular to EOL work—moral distress, mortality salience and death anxiety, for example, may be addressed by an intervention, but not captured by the burnout inventory. Future research would benefit from a burnout measure tailored to the needs of EOL staff.
Five of the six studies used multiple techniques to inculcate mindfulness in staff members—teaching, various meditations, group discussion, individual practice, reading, videos, reflective journaling, body scanning and 1:1 tutorials. One added reminder posters in the workplace. 22 Traditional MBSR and MBCT use several practices, but as individual components have yet to be thoroughly validated, it's impossible to say which components of the interventions are more or less effective, and where interactions may occur. Teasing apart the components of mindfulness practices will likely challenge researchers for years to come.
Limitations of this study
Although we followed the PRISMA guidelines in our protocol, we did not register this review with PROSPERO, having learnt after having extracted the data that PROSPERO's guidelines now require registration before data extraction.
This study was limited by the impossibility of conducting a meta-analysis: reliable data are too limited for meta-analysis. The reviewed studies indicate that MBIs may have a positive, moderating effect on burnout in EOL professionals; however, the evidence is too scant to draw strong conclusions.
Future directions
Much of the research on end-of-life professionals has been conducted on nursing staff, and a preponderance of the professionals in the studies included in this paper were nurses. This may indicate a research gap, as physicians, social workers, psychologists, chaplains and care workers (among others) are also involved in EOL care and may experience stressors different from those of nursing staff.
Future research could include the clearer definition and exploration of constructs, exploration of the lived experience of EOL professionals, awareness of organisational factors in employee support, and improved methodologies of study design and reporting. An integrative review of existing qualitative studies would be useful in capturing the richness and depth of experience reported by diverse EOL professionals—physicians, nurses, social workers, chaplains and others working with dying patients.
Research shows that the time required for MBIs, as well as negative thoughts and self-criticism arising during meditation can be barriers to engagement. 44 If employers institute mindfulness training, is it perceived as valuable workplace assistance, as criticism, as another burden on employees’ time and energy? Research should address these questions.
Mindfulness teacher Thich Nhất Hanh 45 taught that group practice and community building are integral supports for mindfulness practice, which is very difficult to sustain alone. More studies are needed to determine the effects of community building on burnout in EOL professionals.
Mindfulness itself requires more exploration, particularly of interrelated constructs and factors which may have not been included in earlier mindfulness research (e.g., self-compassion, empathy, gratitude), but which are now appearing in the lay literature and in mindfulness practices.
There is also further space for exploration of illness. Research on EOL professionals has yet to explore attrition, stress-related leave, physical illness, auto-immune disorders, mental illness, addiction and suicidality. Mindfulness practice may also reduce physiological signs of stress. 29 MBIs may be able to mitigate the detrimental effects of stress in end-of-life care, where staff stress is often associated with attrition, absenteeism 46 and medical errors. Future studies should explore whether MBIs have a tangible impact on physiological stress reactions. Moral distress, mortality salience, death anxiety and trauma/vicarious trauma are hinted at in the research, but very little has been documented, much less adequately explored. There are some indications that these existential issues, specific to EOL professionals, may contribute to burnout and attrition in the field. 28 Much could be learned from research exploring these issues, not only in working EOL care professionals, but those who have left the profession.
On the other hand, there is anecdotal evidence, so far relatively unexplored, that witnessing some dying experiences become sources of joy and positivity for staff members, who find wider meaning in their own lives after being present at and facilitating a “good death”. 28 Future research considering the barriers, causes and conditions of “good death” could greatly benefit the experiences of patients and their families as well as EOL staff.
Abbreviations
End-of-life; EOL: Mindfulness-based intervention; MBI: MBCT; Mindfulness-based Cognitive Therapy; MBCT: Maslach Burnout Inventory: Mindfulness-based Stress Reduction; MBSR: Post-traumatic Stress Disorder; PTSD: Compassion fatigue; CF: Compassion satisfaction; CS: Secondary traumatic stress; STS:
Footnotes
Acknowledgements
LC would like to express her deep appreciation to the other authors for their knowledgeable contributions and patient support.
Author Contributions
LC designed the review, collected and analysed the data and drafted the manuscript. MB contributed to the design of the review and critical revision of the manuscript. AP contributed to the critical revision of the manuscript. MP provided helpful feedback on the manuscript with the additional prospective of a palliative care professional.
Availability of data and materials
No primary data was collected in this study. Detailed search strategy and further information on included studies available on request from Lorena Covington.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.