
Abstract
Objective(s)
LGBTQI+ disparities in hospice and palliative care have been vastly underrecognized in medical practice and research. This may result in LGBTQI+ community members distrusting health care professionals, avoiding encounters due to fears of discrimination or mistreatment, and seldom disclosing their identities to health care professionals. LGBTQI+ patients often lack familial emotional and caregiver support, a central theme of hospice and palliative care – for example, older LGBTQI+ people are twice as likely as cisgender heterosexual people to live alone and four times as likely to not have children. LGBTQI+ populations are also highly intersectional; therefore, members may be further stigmatized. Blue Diamond Society is a non-governmental organization in Nepal that specializes in LGBTQI+ advocacy and patient care. Our main objective in this study was to explore Nepali LGBTQI+ patients’ experiences in hospice and palliative care.
Methods
29 interviews were conducted with patients, health care professionals, family members, and administrators involved with Blue Diamond Society (BDS), a Nepali NGO that serves Nepal's LGBTQI+ community. Questions were developed based on open-ended questioning to abstract relevant life and health history information pertaining to experiences with BDS and palliative care. These interviews were translated and transcribed verbatim. Qualitative Content analysis was conducted to identify prevalent themes.
Results
Four themes were identified: Fear of Dying without Family; Understanding Oneself and Sense of Community; Patient as Advocate; and Intersectionality and Eliminating Reductionism.
Conclusions
This study elucidated themes inherent to the experiences of LGBTQI+ Nepali people receiving palliative and hospice care, ultimately describing the unique needs of LGBTQI+ Nepali patients in palliative and hospice care settings. In doing so, this study presents an intersectional focus on palliative and hospice care, elaborating on challenges specific to a deeply marginalized community that remains underrepresented in academia. Findings from this study describe an expanded notion of “palliation” to embody “whole-person care,” that is, the palliation of social and structural pain, in addition to the more traditional conceptions of palliation as purely physical, emotional, and/or spiritual. This study also identified the importance of acknowledging and affirming the intersectional marginalization at which LGBTQI+ Nepalis live, ranging from experiences with socioeconomic status, family and communal conflict, ethnicity, race, sex, gender, sexual orientation, age, and environmental resource scarcity. In further understanding and improving upon intersectional LGBTQI+ cultural humility, this study provides opportunities for further research on cross-cultural LGBTQI+ patient needs in hospice and palliative care in a variety of resource settings.
Introduction
There is growing recognition of LGBTQI+ disparities in hospice and palliative care, including considerations of the impacts of COVID-19 on LGBTQI+ inclusive palliative care.1–5 These disparities are further exacerbated by a historical lack of research in this area.6, 7 These challenges are particularly acute in Asian and African countries, where fewer than six percent of the thousands of overall palliative care initiatives are located. 8
Blue Diamond Society (BDS) is a nonprofit organization in Nepal (with branches in most of Nepal's provinces) that coordinates several advocacy initiatives, health programs, education programs, shelter homes, and community outreach programs for the LGBTQI+ community in Nepal. One of BDS’ central health programs is its LGBTQI+ hospice and palliative care facility, referred to locally as the “BDS care and support center,” located in Lazimpat, Kathmandu. All patients are treated free of charge at the center. The primary aim of the palliative and hospice care facility is to provide support to Nepali LGBTQI+ community members living with chronic or terminal illnesses. 80–85% of health care professionals and administrators working for BDS are members of the Nepali LGBTQI+ community themselves. Approximately 70% of BDS’ palliative and/or hospice care patients have HIV/AIDS, and approximately 40% have opportunistic diseases, tuberculosis, cancer, or kidney disease. Patients at BDS are provided room and board in the palliative and hospice care center, in addition to literacy training, necessary medications (for ex., antiretroviral therapy for LGBTQI+ patients who are diagnosed with HIV/AIDS), and psychosocial support.9, 10
In Nepal, terminology pertaining to LGBTQI+ people are culturally nuanced and thus often distinct from terms in the English language. Many of these terms were created by Indigenous Nepalis in opposition to heteronormativity. 11 Recognizing this diversity in terminology is important. Instead of the acronym “LGBTQ+,” Nepali people predominantly utilize “LGBTI,” where the “I” stands for “Intersex” – the term “Queer” is not as widely utilized as in Western nations. 11 Thus, in this paper, the term “LGBTQI+” has been used to reflect the diversity of self-expression. Members of Nepal's gay community may self-identify as “meti”, “singaru,” or “kothi”. 11 Gay or bisexual men who do not present nor identify with traditional notions of “femininity” may self-identify as “Dohori.” 11 Men with femme gender expression may use “fulumulu” as well. 11 Some trans people may self-identify as “Hijara” or “Hijra.” 11 In Nepal, trans people may also self-identify as “third gender,” or “tesro lingi.” 11 In prior surveys asking an open-ended question about identity and self-identification, participants answered using all the aforementioned terms and further terms including “kinnar,” “nachanib,” “dhurani,” “natuwa,” “maugiya,” and more. 12
Palliative and hospice care in Nepal grew following 2009 with the advent of the Nepalese Association of Palliative Care (NAPCare). 13 Since then, rising awareness about palliative and hospice care has led to a slight increase in palliative care initiatives across academic institutions, cancer hospitals, and other medical institutions. However, just as is the case across much of the world, LGBTQI+ people in Nepal face unique health care disparities; in recorded cases of HIV/AIDS, for example, transgender women account for a higher percentage of all cases, and higher risk, with lower health care utilization and access when compared to the cis-hetero Nepali populace. 14
There is no officially documented national LGBTI movement prior to 2001, when an organization called Neel Heera Samaj, known as “Blue Diamond Society,” was formed. 11 In December 2007, a landmark Supreme Court ruling, Sunil Babu Pant and Others v. Government of Nepal and Others, resulted in a verdict calling for anti-discrimination policies for LGBTQI+ people, same-sex marriage, and the explicit recognition of transgender people and a formal “third gender” category on all legal frameworks and documents. 11 The Supreme Court ruling brought Nepal to the forefront of international LGBTQI+ rights, as more than 80 countries at the time still criminalized LGBTQI+ identity. 15 Furthermore, as of 2021, LGBTQI+ Nepalis will be counted in Nepal's annual census for the first time. 16
However, overall, on-the-ground implementation of the ruling has not translated into proportionate concrete advances in the livelihoods of LGBTQI+ people. There remains significant discrimination, stigma, social exclusion, and health disparities among Nepalese LGBTQI+ people. 17 One study writes, “there is dissonance in Nepal between a progressive legislative environment in respect of gender and sexual minority issues and everyday sociocultural ambivalence toward such sexual and gender minority persons”. 18 Homophobic and transphobic violence exists in pockets of Nepal and social pressures to conform to heteronormative constructs of gender and sexuality govern the lives of LGBTQI+ people. One study of transgender people in Nepal found significant levels of verbal, physical, and/or sexual violence from spouses or sexual partners. 19 In another study, a large percentage of LGBT respondents reported having been raped, sexually abused during childhood, blackmailed, abused by police, or harassed verbally. 20 Furthermore, Nepal lacks employment anti-discrimination laws, housing discrimination laws, marriage discrimination laws, and several health services for LGBTQI+ people. 21
This study explores LGBTQI+ experiences in hospice and palliative care provided by BDS. Our goal was to interview palliative and hospice care patients, professional caregivers, administrators, and community/family members to understand LGBTQI+ patient's experiences of palliative and hospice care.
Methods
Study Design
This study consisted of semi-structured interviews conducted with patients (n = 8), health care professionals [RN, MD and/or nurses’ aides] (n = 5), administrators (n = 14), and community or family members (n = 2) at BDS’ care and support facilities in Lazimpat, Kathmandu, Nepal and central administrative facility in Dhumbarahi Marga, Kathmandu.
Setting and Participants
Most patient interviews (∼66%) and all health care professional interviews (100%) were conducted in private conference rooms located on the upper floors of the BDS care and support facility in Lazimpat. The remainder (∼33%) of patient interviews were conducted in patient homes located across the city of Kathmandu and neighboring villages, with family members absent to ensure and protect patient privacy. Many patients lived in rural, mountainous, village regions that required a combination of taxi or motorcycle transport and walking to access. All administrator interviews were conducted in the central BDS administrative facility in Dhumbarahi Marga, Kathmandu. Family and community member interviews were conducted in Lazimpat, either at the BDS care and support facility or at the community member's home.
Semi-structured interviews were conducted with 29 participants, representing a mix of patients, health care professionals, providers, and community or family members. All patients and health care professionals were recruited purposefully, seeking to represent transgender and/or nonbinary people, intersex people, lesbian people, and gay people, in equal proportions to one another. Our goal was to overrepresent patients, followed by health care professionals and administrators, followed by community and family members.
However, many interviews with patients were unable to be conducted due to patients’ changes in availability as well as geographic barriers to meeting with certain patients located in particularly rural, mountainous, isolated regions of Nepal. Furthermore, upon arrival in Nepal, we learned that several patients the facility was treating with hospice care had recently passed away. Similarly, we also learned that one doctor who we sought to interview had passed away due to the devastating 2015 Nepali earthquakes.
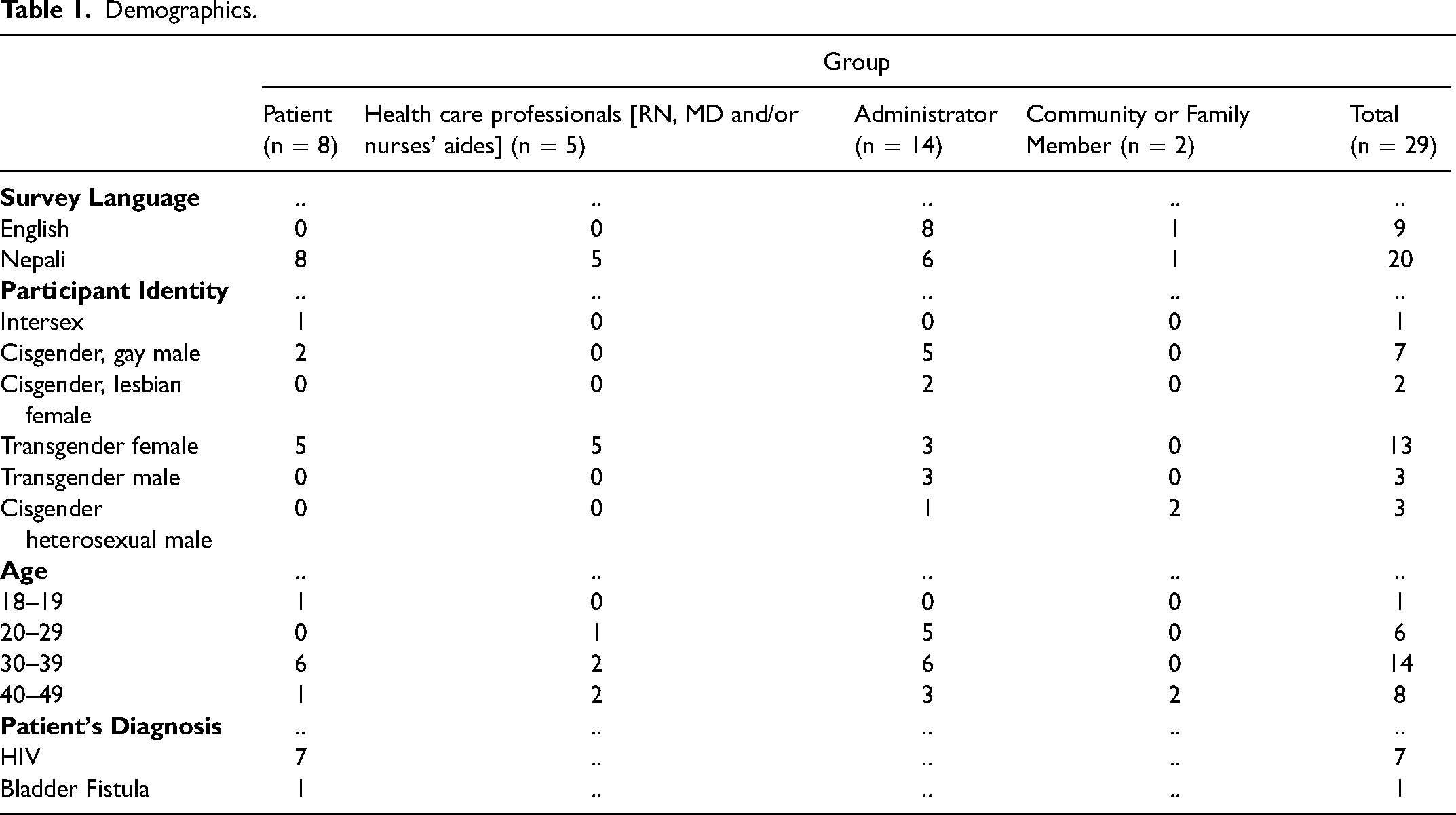
Seven administrators were chosen directly by the investigators for their involvement in both the BDS palliative and hospice care and support center as well as the BDS executive board. The remaining seven administrators were recruited by the investigators following referral from BDS administrators working on the organization's palliative and hospice care and support program (Table 1). These administrators had worked with the hospice and palliative care and support center at some point in time in varying capacities. All participants were at least 18 years old and spoke primarily Nepali, English, Hindi, or other regional languages.
Demographics.
Data Collection
The survey included 17 questions for patients, 13 questions for health care professionals, eight questions for community or family members, and nine questions for administrators on the following topics: life history, personal and professional relationships, stigma and discrimination, wishes and desires in old age and end-of-life, work experiences, health care experiences, and perspectives on BDS. All questions were developed by study authors in consultation with a Northwestern University anthropology and global health studies professor, BDS Executive Board members, and Nepali translators.
In July and August 2016, 29 interviews were conducted, lasting between 35 and 120 minutes. Interviews were conducted in a private room with a translator. Interviews were conducted in English or Nepali, with the Nepali translator providing simultaneous verbal translations. All conversations were audio-recorded. Audio files were deleted upon transcription. The translator transcribed Nepali audio recordings into English. All participants provided written consent. To ensure that oral and written information was in their language of choice, translators from a facility based in Kathmandu or from BDS translated all consent documents and questions.
Qualitative Content Analysis
Qualitative content analysis was performed to identify prevalent themes.22, 23 First, each author independently read transcripts. Second, the authors met and determined the analysis to begin at the level of sentences. The interview content was the level of analysis. Authors decided upon an inductive coding approach, adding themes throughout the process of coding as themes emerged. The authors reviewed each transcript together and coded them sentence-by-sentence for existence and frequency of topics. A coding schema was established through constant comparison of sentences, to further develop codes throughout the analysis process. All coding was done by hand. Third, from the over 15–20 themes that emerged from this initial round of analysis, themes were subsequently discussed and merged into a common set of overarching themes. Finally, authors met once last time to resolve any discrepancies from independent verification of themes.
Ethical Considerations
Institutional Review Board (IRB) approval was obtained from the Northwestern University Institutional Review Board, which reviewed and provided ethical oversight over the study procedures. All materials utilized in the study, including semi-structured interview instrument tools and consent forms, were approved by the Northwestern IRB. Further approval was obtained from the Blue Diamond Society Executive Board. Prior to the study, the lead investigator received formal training in qualitative and social science research methods through an approved course administered by the Northwestern University Department of Global Health Studies. Participants were not compensated for their participation, and participants were made aware that their participation was completely voluntary with formal paperwork signed as part of the consent process. The Nepali translator for this study was compensated for their participation during interviews with all Nepali-speaking participants and for written/verbal translation of all interview materials.
Results
A total of 8 patients, 5 health care professionals (RN, MD and/or nurses’ aides), 14 administrators, and 2 community or family members were interviewed. Out of all 29 interviewees, 1 patient identified as intersex; 2 patients and 5 administrators identified as cisgender, gay men; 2 administrators identified as cisgender, lesbian women; 5 patients, 5 health care professionals (RN, MD and/or nurses’ aides), and 3 administrators identified as transgender women; 3 administrators identified as transgender men; and 1 administrator and 2 community/family members identified as cisgender, heterosexual men. 1 participant was between 18–19 years old; 6 participants were between 20–29 years old; 14 participants were between 30–39 years old; and 8 participants were between 40–49 years old. Patients identified among several faith backgrounds, including Christianity, Hinduism, and Buddhism. Most lived alone and the most frequent occupations were administrative work and sex work. Four overarching themes from the interview data are discussed below:
Fear of Dying Without Family
Patients described a common theme of their fears growing old without any form of support. For them, the aging process conveyed a sense of meaninglessness, fear, and isolation; and more so than preoccupation with the quality of or access to services they would receive for their health in old age, their chief concerns were instead centered around who they could obtain social support from as they faced their own mortality.
One patient described, “I am scared of growing old. If I grow old then whether my son will look after me or not, I wonder how they will react after they find out about my status. I am afraid to tell my sons about my condition. Will they help me get medications or not, I fear.”
Similarly, another person commented on the fears associated with not only having no support, but fear of family members seeking dispute or legal trouble following death: “Due to discrimination towards transgender, family members do not care about them during old age. In addition, there are many cases that family members leave their members… after that they become out of contact. Even if they expire, family members come and create disputes and file cases.”
Several participants endorsed similar concerns about being alone while aging and dying. Their disparities throughout life were themselves sources of depression and loneliness; these same disparities exacerbated toward the end of life when participants described being most vulnerable.
For example, one participant exclaimed, “And me, who is all alone, I am pretty sure my situation will be more worst. Therefore, I wish some people voluntarily look after me in my old age.”
In this setting, the health care professionals described how patients often miss their loved ones at the end of their lives. Many times, loved ones are absent during patients’ final moments, necessitating the health care professional to step in.
One health care professional described a patient who recently passed away: “We gave full assistance as a caregiver to her and during the process of treatment she passed away. During her last days, she was expecting her kids to visit her, but they did not come to see her.…. her son and daughter had already answered us, that they don’t care about her, for them she is equal to die. But she always expecting her kids to visit her. That used to make her upset.”
Participants endorsed extensive discrimination from their families and communities. They spoke about a crisis of acceptance disproportionately affecting older LGBTQI+ people. Many members spoke about their experiences with humiliation from family and exclusion from family events. They often remarked on their loneliness and sense of abandonment from everyone close to them.
One person remarked, “When I confessed about my identity neither the society nor my family supported me. My own family member discriminated me, humiliate me. That made me to leave my family and society. They don’t invite me to join them during special festival and other religious ceremony. I am alone.”
Participants shared a sense of shame and sorrow in feeling not only alone, but ostracization. The notion of community and friendship was a central theme of their expressions of grief; not only did they receive hate and discrimination from their family, but equally from their friends and neighbors. The notion of loneliness extended to tertiary support networks. Participants often utilized animalistic or sub-human descriptors to describe their feeling toward their circumstances.
Another person similarly commented, “The local people even didn’t allow me to take water from public well. Those friends of mine, who were straight used to ignore me, even refused me to be my friend. Even in the case of security persons used to treat us as if we are not a human. They used to use offensive words.”
Another person commented, ““My father told me we know you are not a lesbian because we gave you birth, you grew up in front of us. They had some understanding that lesbians are insects…I just told him this is what I am and if you don’t want to accept me don’t accept me.”
The centrality of marriage and divorce in participants’ lives was called into question with several relationships participants described. Some participants described their spouses receiving abortions following disclosure of identity. The implication of this on notions of stability and family are important, for the sense of loss and powerlessness that participants described stemming from the loss of kin, loss of love and marriage, and loss of family and extended family, all were amplified in the setting of divorce and abortion. Accordingly, many participants saw their only solution as running away from home and living without support.
A participant commented on the impact discrimination had on his marriage: “The first three years of my marriage was good. After that my wife got to know about my feeling and identity. I never tried to tell her before. When she got to know, she moved to her father house and get divorce… At that time, she was pregnant but immediately after she got to know about my identity, she did abortion.”
Participants’ experiences of discrimination and hate from family members, friends, and tertiary support networks are exacerbating factors in their sense of loneliness and estrangement. Discrimination and hate toward LGBTQI+ community members sometimes lead to outright social exclusion, ejection from the home, and vicious cycles of being undomiciled and alone without sources of income or support. Without any help or support, community members describe the fear of family and friends, and the resulting need for support when dying.
One participant explained this cycle of discrimination toward trans people leading to social exclusion and ultimately estrangement at the end-of-life: “Among [LGBTI community members], only 5% get supported by their family members in hospice. Around 95% do not get support. Trans gender people do not behave as per the expectation of the family members and society due to the same they need face discrimination from them… the discrimination goes double to them regardless of their economic status. Most of the family members don’t want them to stay in home due to their trans identity… Mostly at that time when their family members kicked them out from home. There is not any space to stay in head office so till the time to find any alternative way for their livelihood they get support for food and shelter from hospice.
Understanding Oneself and Sense of Community
Multiple participants described a process of coming to terms with their own identity, namely through learning about their feelings as well as in finding other people like them. The solidarity they reference was instrumental in enabling them to feel happy, through a sense of shared comraderie and solidarity. Many participants described the significance of this during old age, during which finding a community to help look after oneself was expressed to be an important factor in finding happiness. Participants often described the importance of learning about their identity as a source of healing.
One person explained, “During my early age, I used to feel that I am the only one who has this kind of feeling. I hadn't had any attraction or feelings towards girls. However, I got in touch with other [LGBTI] friends. I felt so happy to be their friends. The time was passing on its pace.”
Another person explained, “I thought I am the only one…When I came here, I met with other friends, and then, I understood I wasn’t the only one. There are many other people like me.”
Several participants described the centrality of meeting community members with a similar sexual orientation. Meeting with community members who had similar attraction to other community members was often perceived as extremely important, since many participants lacked that fundamental communal support throughout their lives.
For example, a participant commented, “When I came to BDS and met with other sexual and gender minorities during that time, I felt a little happy in my life thinking that ‘oh I am not the only person who has attraction towards male’ – there are other people as well.”
Coming to terms with one's own identity and thereafter finding a community of similar people to embrace one's identity was a recurring theme participants described which helped them feel open and comfortable discussing their needs.
One person explained, “For the people like us, we do feel comfortable to share our feeling with the person who has similar kind of feelings rather than our family members. So, I want to be with my friends with whom I could share my feeling at the end of life.”
This process of coming to terms with oneself and feeling safe and secure is made possible through participants’ journeys in finding other LGBTQI+ community members. Multiple members described the importance of meeting other community members along their journey of obtaining care and support.
One person explained, “Even I don’t have single relative who accept me and close to me. So, for me BDS and the community members are everything.”
A few other members explained: “On that day I saw Metis from mountain region as well. I was really very happy to see all of them on drag.” “I used to stay at home alone because I used to enjoy staying alone. I didn’t have that kind of friends before joining BDS.”
Just as participants described their loneliness from lacking friendship and family support, so too did several participants describe the profound impact of friendship with fellow community members. Notably, participants often described this support as a type of indirect therapeutic alliance; that is, participants described a sense of resolution of their various confusions directed primarily at the self and the community. Questions of how they felt, questions of how fellow community members felt – it all began to make sense as participants described their process of finding friendship and resulting hope and meaning.
“After joining BDS, it took me almost 4 month to understand all behavior of community member. At that time, [fellow community member] was the one who helped me a lot to understand the community's behavior. Slowly, I started to introduce to other members. I was happy to be with most of the members.”
Another person commented “I got lots of information, booklets, and posters about the LGBTQI+ people and their problems, who had similar kind of sexual problems like mine. This was the first time that I got chance to meet with other intersex people… I was in a hard time/situation before, but now I do not have any pain and difficulty – that’s why I am very happy.”
One consistent pattern in participants’ characterization of their past prior to finding commonality through community was their use of metaphor. Notions of being “caged” or “subdued” were common, versus the contrasting “freedom” that resulted from their feeling of being understood finally.
One patient, for example, shared poignant and poetic words about the hope and meaning they found through their time finding community at the palliative and hospice care facility: “At the beginning I was feeling that I was in cage but… currently I am feeling that I am living under the open sky.”
Patient as Advocate
A central theme in many participants’ interviews was the importance of feeling empowered as a modality of healing and recovery. Participants often discussed work-related projects centered around LGBTQI+ community organizing, education, and advocacy they were participating in while receiving care. Participants described how healing for LGBTQI+ community members entailed providing them with toolkits to combat societal root causes of their disparities in prosperity and happiness.
One person said, “I raise my voice for equal opportunity to LGBTI people… To change society at first, we have to change the rules and laws, each and every person should know about LGBTI issues… I don’t know whether it is my goal or dream, but I wish I could built care home for LGBTI people, where all community members could live happily and can share their feeling with each other.”
Other participants similarly endorsed the importance of empowerment and advocacy as instruments of change and healing. Particularly for Nepali LGBTQI+ patients receiving palliative and hospice care services, the theme of helping other LGBTQI+ community members was important as a coping mechanism.
Members explained, “I wish for the good livelihood of community people. I want the welfare of community members and want to be a cook.” “I got to know that for my right and for the right of community, I have to do advocacy… Now, I can raise voices for the rights and the needs of community members with coalition group and do advocacy for equal treatment like other population to sexual and gender minorities.”
One person described how helping other LGBTQI+ community members is tantamount to helping oneself: “I believe faith in action is love and love in action is service… So many people come here with the same pain and story [as me], so I help them by thinking my own problem and by seeing me in that problem. I feel so happy to help them.”
Patients described the numerous ways by which they involve themselves in advocacy for fellow community members, namely through peer-to-peer patient support and community education. Nepali LGBTQI+ patients and health care professionals often described their roles in staffing hotline services to help educate LGBTQI+ people from rural Nepal who call in with questions about their gender or sex identity.
One participant described, “…Hotline occupation is one example and people call here and its toll-free number. And they call and if they confusing about their sexuality our hotline operator counsels them, and it will be easy to calm them and understand about their sexuality.”
Patients often spoke to their wishes and dreams as they grew old and faced mortality. Most described, in some form, helping their fellow LGBTQI+ community members through the transformation of public policy and law. Equality was described as inherent to healing and finding peace at the end-of-life.
One person described, “In my end of my life, I want to see the equality of all the people. No discrimination for LGBTQI+, disabled people, and lower caste people. I want to see all our equal and equality for all persons.”
Intersectionality and Eliminating Reductionism
Participants discussed an inability to enjoy freedom from persecution without redress of additional marginalization presented by their intersecting identities. Many of these identities were described by participants as simultaneously oppressive, giving rise to a combined oppression represented by the amalgam of their various marginalized identities. This notion of “intersectionality” draws from prior work by Dr Kimberle Crenshaw in her seminal 1989 paper. 24
One participant described the intersectionality she navigated as a closeted trans woman in a misogynistic household. “Nepal is male-dominated society and still women are taken as second-class citizen – that’s why we are facing double discrimination than other LGBTI people. We are lots of problem to come out being a lesbian because I already told you that if you are woman you can’t tell you’re openly to them because people say that you are woman you don’t have any you can’t speak more.”
Participants also discussed the intersections between poverty and LGBTQI+ identity – low-income LGBTQI+ Nepalis are predisposed to join the sex worker industry, often without other employment options, potentially living in further silence while experiencing higher rates of sexual violence. 25
“Many community members are forced to leave their home; reasons might be different of being homeless but after being homeless as well they have to gone through different kind of struggle to live their life. People don't give job opportunity, fortunately if they succeed, they need to go [to] their different kind of hassle. Some are raped by their senior in the officer those who are involved in sex work as well, infected by HIV in addition they have been raped by police denied treatment.”
Another participant described the influence of religion in their life and the intersections between their married life, their gender identity, and their religious practice: “ I changed my religion in 2060 BS (2002). Before that I was living my life in depression. I wanted to get rid of all frustration and depression. My family members used to force me for heterosexual marriage, but I had not had any feeling towards any female. I was living in depression due to all those situations in my village… When I changed my religion into Christianity there, I got to understand that this is me, whatever I am. I [was] happy and thankful to God for this beautiful life. Since then, I got to accept my own feelings. That was the first happiest moment in my life.”
A select group of participants – primarily those from rural areas – additionally discussed a cultural mismatch between larger cities in Nepal and surrounding rural areas, in which a culture of silence pervades daily life around gender and sexuality. The notable intersectionality between environment, culture, and gender/sexuality seemingly pervaded many narratives in our study: “Most of the local people—don’t talk about sex, gender, and sexuality in front of their parents, in front of their children, even in front of their wives and mothers… There is some kind of awareness, institutional awareness, but in local village and local community, still people don’t want to talk.”
Several participants accordingly described the importance of acknowledging and affirming their unique identities without treating them as, generally speaking, “an LGBTI person.” Patients often wished for health care professionals to treat them s who they are, rather than who they perceive them to be.
One health care professional further described how they meet this need from patients: “I treat all the people according to their nature and make sure they are not feeling awkward. Like if the service holder is trans-gender, then I talk very fluently and freely with them. Since there are certain things that trans feel happy talking in between transgenders. But if there is lesbian women, I will talk normally restricting myself sharing certain things that only comfortable to share within trans community. So, it depends upon their identity and sexuality.”
Another health care professional elaborated on this further: “How do you treat gay man differently? I always try to make the patient happy by talking about the things they enjoy talking in order to divert their mind and to be free from any kind of tension and stress. How about the lesbian women? I mostly talk with them normally by putting myself in the position of lesbian. I generally say if I would be a lesbian I would do this and that. Always try to find a topic to talk to become more familiar with them and make them happy… But I always be careful not to hurt them.”
An important interview finding from participants’ reports was that investigations surrounding palliative and hospice care interventions for LGBTQIA+ populations required nuanced and specific development. LGBTQIA+ community members described how they are not monolithic; therefore, reductionist interventions and survey development would not do justice to both validating and better understanding the needs of their various communities with all their complex intersectionality. This finding is further elaborated upon in the subsequent analysis.
Discussion
Our study's objective was to explore Nepali LGBTQI+ patients’ experiences in hospice and palliative care. We found that patients find peace and meaning through achieving a sense of community previously absent in their lives. This occurs due to holistic care involving both medical and non-medical components of safe space building – from meeting people from patients’ own identity groups; meeting health care professionals who come from patients’ own communities; being invited to share stories, provide peer-to-peer patient support, community education, and LGBTQI+ advocacy; and more. In Western countries, palliative care is interdisciplinary and aimed at preventing or palliating symptoms, relieving of suffering, and improving quality of life. 26 This often occurs through a combination of modalities, ranging from analgesia for physical symptom control; chaplains for spiritual support; and a variety of other providers for emotional support. But in Nepal, LGBTQI+ participants in our study additionally described how they required not only “palliation” of their physical, emotional, and spiritual pain, but also their social and structural causes of pain, emerging from the various experiences of systemic discrimination and marginalization they faced throughout their lives. In bolstering LGBTQI+ Nepali community members’ abilities to share their stories, meet other community members, and organize and advocate for their rights while simultaneously tending to patients’ health care needs, health care professionals at BDS explore discrimination and inequity as symptoms, thereby embodying “whole person” care in which palliative and hospice care is seen as a palliation of inequity.
We also found that many patients live at the intersections of multiple identities, including poverty, caste, disability, religion, and rural/city cultural differences. Thus, their needs in palliative and hospice care are multi-faceted, requiring recognition and affirmation of the various factors that cause them hardship or harm throughout their lives. In the same vein, LGBTQI+ community members’ needs are unique based on the individual community with which they most identify and not to be collapsed into a monolithic, general definition of “LGBTQI+.”
Our study also revealed the centrality of a supportive LGBTQI+ Nepali community for members of the population experiencing severe illness. The notion of a health care professional as a family member, and not simply a traditional professional, is crucial: patients expressed how, in a time of having no children and isolation from family and friends, patients felt their health care professionals assume such familial roles. This builds on previous research, particularly for LGBTQI+ elders, or intersectionally marginalized LGBTQI+ individuals, such as those living in poverty, who tend to live alone, without family members.27–31 This finding differs from more traditional Western notions of palliative care, in which health care professionals administer care for patients and their families, rather than assume familial roles themselves. 32
The multiple roles assumed by staff and patients may stem partly from resource scarcity. Due to resource constraints, roles are fluid: a driver may help with cooking, cleaning, bathing the patient; a nurse may also assume roles of counselor, social worker, or bereavement support staff; an administrator may serve the role of social volunteer. This expands the traditional mold of what it means to be a hospice and palliative care health care professional or administrator.
Limitations of this study include a small sample size, meaning that we are unable to differentiate impacts of varying socioeconomic status or caste on interview responses. Despite the diversity of our sample in terms of gender identities, our sample was isolated to one hospice and two languages (English and a mainstream Nepali dialect), a small fraction of the over 123 languages spoken across Nepal. 33 Most of our interviews were conducted in Kathmandu or nearby cities in Bagmati Province, where BDS is located, thus under-representing the experiences of people in Nepal's other provinces. 34 Given that most of our patients were receiving palliative care services for HIV, our study also underrepresented individuals receiving treatment for other illnesses, including cancer.
Potential future studies of interest on Nepali LGBTQI+ palliative and hospice care disparities include, but are not limited to: a repeat study on Nepali LGBTQI+ patient experiences in palliative and hospice care post-COVID; a study specifically on asexual, agender, intersex, non-binary, gender-fluid, and other marginalized sexual or gender identity patient disparities in Nepali palliative and hospice care (given the relative under-representation in both our study and the general literature); and a study comparing and contrasting LGBTQI+ health care services provided directly by BDS versus those provided by the local hospitals in Kathmandu and other major nearby cities.
Conclusions
Too often, health, healing, and dying are primarily viewed using a biomedical paradigm, missing the importance of social context and relationships—and the power of narrative and interpretive social science to consider these dynamics. This study utilized 29 semi-structured interviews with Nepali patients, health care professionals, administrators, and community/family members to shed light on ways that LGBTQI+ Nepali patients experience culturally humble and affirming palliative and hospice care.
Understanding the inherence of community in cushioning the harmful impacts of discrimination LGBTQI+ Nepalis experience throughout their lives is crucial to improving LGBTQI+ patients’ experiences in palliative and hospice care. Components of this community include the opportunity to meet fellow community members in a safe, affirming space; the emphasis on family over role-based hierarchies in professional care settings; and the acknowledgement and affirmation of patients’ lived experiences of intersectionality. These values expand on more traditional palliative care frameworks to deepen attention to social suffering.
Findings from this paper may inform further research, policy, and practice guidelines on palliative and hospice care for LGBTQI+ Nepalis, further embodying “whole person” care that centers the needs of structurally marginalized patients. Next steps include translation of interview materials and consent forms into multiple Nepali languages/dialects, performing further studies in other provinces of Nepal, greater representation of asexual, agender, intersex, non-binary, and gender-fluid Nepali patients, and greater representation of Nepali LGBTQI+ patients with a more varied set of medical diagnoses than those available in our sample.
Footnotes
Acknowledgments
We would like to acknowledge the Northwestern University Department of Global Health John and Martha Mabie Fellowship for Public Health for grant funding to support this study. We would also like to thank Professor Peter Locke, a medical anthropologist at Northwestern University, whose mentorship helped secure funding and develop the knowledge required to carry out the qualitative methodologies used in this paper. Finally, we would like to thank the patients, families and staff of Blue Diamond Society who participated in this project.
Declaration of Conflicting Interests
No competing financial interests exist.
Funding
The Northwestern University Department of Global Health John and Martha Mabie Fellowship for Public Health administered grant funding for this study.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.