
Abstract
Background
Physiotherapy in Palliative Care (PC) is effective in the management of a series of respiratory, circulatory and motor symptoms, and often has a positive impact on the patient's mood. The Edmonton Functional Assessment Tool (EFAT) is the only existing validated tool specifically designed for functional assessment in PC, and its use has been recommended in clinical practice. To date, no Italian version of the tool has been validated. The aim of this study was to translate, cross-culturally adapt, and evaluate the psychometric properties of the Italian version of the EFAT2.
Method
After receiving formal permission from the author, Beaton guidelines for cross-cultural adaptation were followed, namely: (1) forward translation; (2) a multidisciplinary focus group (including 4 physiotherapists, 1 physician, 3 nurses, 1 occupational therapist, 1 psychologist) to assess semantic, idiomatic, experiential, and conceptual equivalence; (3) backward translation. The Content Validity Index (CVI) was used to assess content validity of the tool. Construct and concurrent validity were also evaluated. To evaluate the reliability of the EFAT2-I, reliability was measured using Cronbach alfa, item-total correlation, and Cohen's Kappa.
Results
119 patients admitted to a Palliative Care Unit (Italy) agreed to participate in the study. The EFAT2-I mean score was 11.3, ranging from 0 to 30. Very good CVI scores were achieved, both in terms of single item validity (I-CVI) and of whole scale validity (S-CVI). Positive results were obtained from construct, concurrent validity assessment and measures of reliability.
Discussion
The EFAT2-I showed good psychometric properties and can be used as a rehabilitation assessment tool in palliative care settings. The validation of the Italian version will allow comparison of different centres and palliative care facilities on national and international levels.
Introduction
In palliative care the goals of rehabilitation are to help patients to reach their maximum functional potential in a realistic timeframe and to maintain it during the final stages of illness. It is made possible by constantly changing treatments and goals, while taking into consideration that abilities decay. 1
In palliative treatment contexts, physiotherapy is increasingly demonstrating its effectiveness in treating lymphedema, dyspnoea, fatigue, pain,2–4 and in improving joint mobility, transfer ability, walking, and mood.5–7
In the context of rehabilitation during palliative treatments, the term “improvement” is explained well by the term “rehabilitation-in-reverse”.8,9 Contrary to traditional rehabilitation, where a path is established to improve or alleviate various dysfunctions, in palliative treatments the physiotherapist leads the patient through each step of the evolution of their illness, starting from an initial functional improvement towards progressive physical deterioration. This path is characterized by constantly changing the treatment goals, introducing aids that are always related to the clinical, functional and emotional condition of the patient. This aspect clearly underlines the extent to which the role of the physiotherapist could be an important beacon for the patient along his path towards the end of life.
Although the literature clearly describes the interventions a physiotherapist can carry out, 10 few tools are available that assess or validate the effects of the proposed treatments.
From the literature, 10 it is clear that the assessment tools employed in rehabilitation during palliative treatments are widely heterogeneous; some of them verify performance in very general terms, others, despite being specific rehabilitation tools, are very difficult to use in a palliative treatment context. The Karnofsky Performance Status (KPS)11–14 and the Eastern Cooperative Oncology Group (ECOG) performance status 15 are examples of general assessment tools. They do not take the evolution of the patient's condition into account, mainly because their scores tend to appear together, towards the final values of the scale, thus offering only a partial view of the problem.16–19 Although the Palliative performance scale 13 might be a valid tool for evaluating the prognosis, it is not considered suitable for highlighting rehabilitation needs. The literature describes various tools, specifically intended for the assessment of a patient in a rehabilitation context.15,20–35 The critical issue with these rehabilitation tools is that they are not able to combine the functional assessment of patients with an assessment of their quality of life, which represents the main goal of palliative treatments. For example, the Functional Independence Measure (FIM) results face the “floor-ceiling effect”, which happens when the level of the task is so difficult that none of the patients can complete it; moreover, it is very difficult to employ the FIM in a palliative context. 36 The Barthel and Katz scales only evaluate the physical aspects of daily activities in patients undergoing palliative treatments. 36
According to the Association of Palliative Medicine of Great Britain and Ireland, 37 the Edmonton Functional Assessment Tool (EFAT) 17 is considered a specific tool to assess functional rehabilitation during palliative treatments. Considering the great developments and changes in approach towards palliative treatments, the original tool later had to be modified. The same authors introduced a second version of the tool (EFAT2) that encompasses pain and fatigue assessment and an extra item (performance status) that aims towards an overall view of the entire scale.
Although the EFAT2 is considered an adequate tool for evaluating palliative treatments, an Italian version has not yet been validated. Such validation would help the internationalisation of palliative treatments, allowing comparisons and summarising the results of studies carried out in different cultural contexts.
The goal of this study is to validate the Italian version of the EFAT2 (EFAT2-I), testing its psychometric features.
Methods
To run the psychometric test of the Italian version of the EFAT2-I, the study was divided in two different phases: Phase I focussed on developing the Italian version; Phase II focussed on testing its psychometric properties.
Sample and Setting
This study was carried out on all patients undergoing palliative treatment in a palliative care centre of Rome, Italy. The inclusion criteria were: Karnofsky index score of between 20 and 50; being able to undergo a physiotherapeutic programme; being at least 18 years old; being able to consent to participation in the study; and having received palliative treatment for at least 5 days. All eligible patients were invited to participate in the study, then they were informed about the aims, procedures, and implications of the study, before asking for their written informed consent to participate. The EFAT2-I was administered directly by health care professional (physiotherapist or occupational therapist) during the rehabilitation assessment.
Ethical Considerations
The study was approved by the Ethics reference Committee of the centre (Prot. No. 1066/2017). To ensure personal data confidentiality, all information was treated anonymously.
Tool
The original version of the EFAT 17 was developed to evaluate the performance of terminally ill patients with tumours. It is composed of 10 items that evaluate the status of some main functions, such as: communication, mental health, sensitivity, respiratory condition, balance, mobility, activity level, wheelchair use, and activities of daily living (ADL). Each item has a scoring system ranging from 0 (independent functional performance) to 3 (total loss of performance) The potential score range of the scale is between 0 and 30. Higher scores indicate a poorer condition, and lower scores indicate a better one. Moreover, to summarise the patient's performance status the scale includes a single final item (range 0-3) that is not calculated as part of the total score.
Procedures
First phase: cultural-linguistic adaptation
The EFAT2 cultural-linguistic adaptation followed the guideline proposed by Beaton et al., 38 which mainly evaluated a forward translation (FT1 + FT2) and a backward translation (BT1 + BT2), plus the introduction of an expert committee involving the author, to discuss the different versions. The first translator was a native speaker while the second one was an expert in field.
Following these steps, every discrepancy was resolved until consensus on the final version of the scale was reached. Subsequently, semantic equivalence, idiomatic equivalence, experiential equivalence, and conceptual equivalence of the scale were evaluated. The cultural-linguistic analysis of the tool led to the application of changes in the semantic equivalence of the item “balance”: in the Italian version, it was translated using a concept that better explains the concept of balance in Italian physiotherapy, which is “getting and maintaining the upright position”.
Second phase: testing the psychometric properties
Content validity was tested using the Content Validity Index (CVI) according to Lynn, 39 Polit and Tatano-Beck 40
To determine the CVI, five physiotherapists and two occupational therapists who were highly experienced in palliative care 41 were asked to verify the relevance of each item (I-CVI) and of the entire scale (S-CVI) regarding functional status rehabilitation assessment within palliative care. In this respect, experts were provided with all the necessary information for making their judgement concerning the relevance of the EFAT2 on a 4-point Likert scale (1 = not relevant, 2 = somewhat relevant, 3 = quite relevant, 4 = highly relevant).
Experts’ assessments were then collected and to obtain the I-CVI, the number of those judging the item as “relevant” (rating 3 or 4) was divided by the number of content experts. Similarly, the S-CVI was calculated using the number of items that achieved a rating of “relevant” within a tool. An I-CVI score of 0.78 and an S-CVI of 0.90 were the minimum acceptable indices. 4
Besides content validity, evaluated through CVI computation, we also evaluated construction validity and concurrent validity.
In order to test the validity of the tool it was hypothesised that the patients admitted to a hospice, due to their unstable clinical condition that caused them to require residential care, had a worse score than the sample who remained at home. Specifically, a sample of 119 patients undergoing palliative care from July 2015 to March 2016, both at home and in hospice, were evaluated.
To test concurrent validity, the 119 patients were evaluated at the same time, using both the KPS and the EFAT2-I. Our theory was that we would find negative correlation between the two indexes.
The reliability of the scale was evaluated using inter-rater reliability, Cronbach alpha, and item-total correlation. To determine the size of the sample required for measuring inter-rater reliability using Cohen's K, we considered the power of 0.90 and Alpha error of 0.05. 42 Two physiotherapists used the EFAT2-I to conduct the assessments independently on 119 patients. Cronbach alpha is a measure of internal consistency of a scale and acceptable scores ranges between 0.70 and 0.90. 43 The item-total correlation is a correlation between the single item and the total scale score and values above 0.20 for each item are commonly considered satisfactory. 44
Statistical Analysis
Means and frequency distributions were used to describe the characteristics of the sample.
To determine construct validity, the difference between the averages of the two groups (hospice vs. home) was evaluated. Concurrent validity and inter-rater reliability were evaluated using Pearson's correlation and Cohen's K, respectively.
Validity and reliability were performed with a complete case analysis. As such, we utilised only cases where there were no missing values in any of the variables under analysis.
Results
Sample Characteristics, EFAT2-I Scores and Usability
The sample was composed of 119 patients. The characteristics of the sample are shown in detail in Table 1.
Characteristics of the Sample (n = 119).
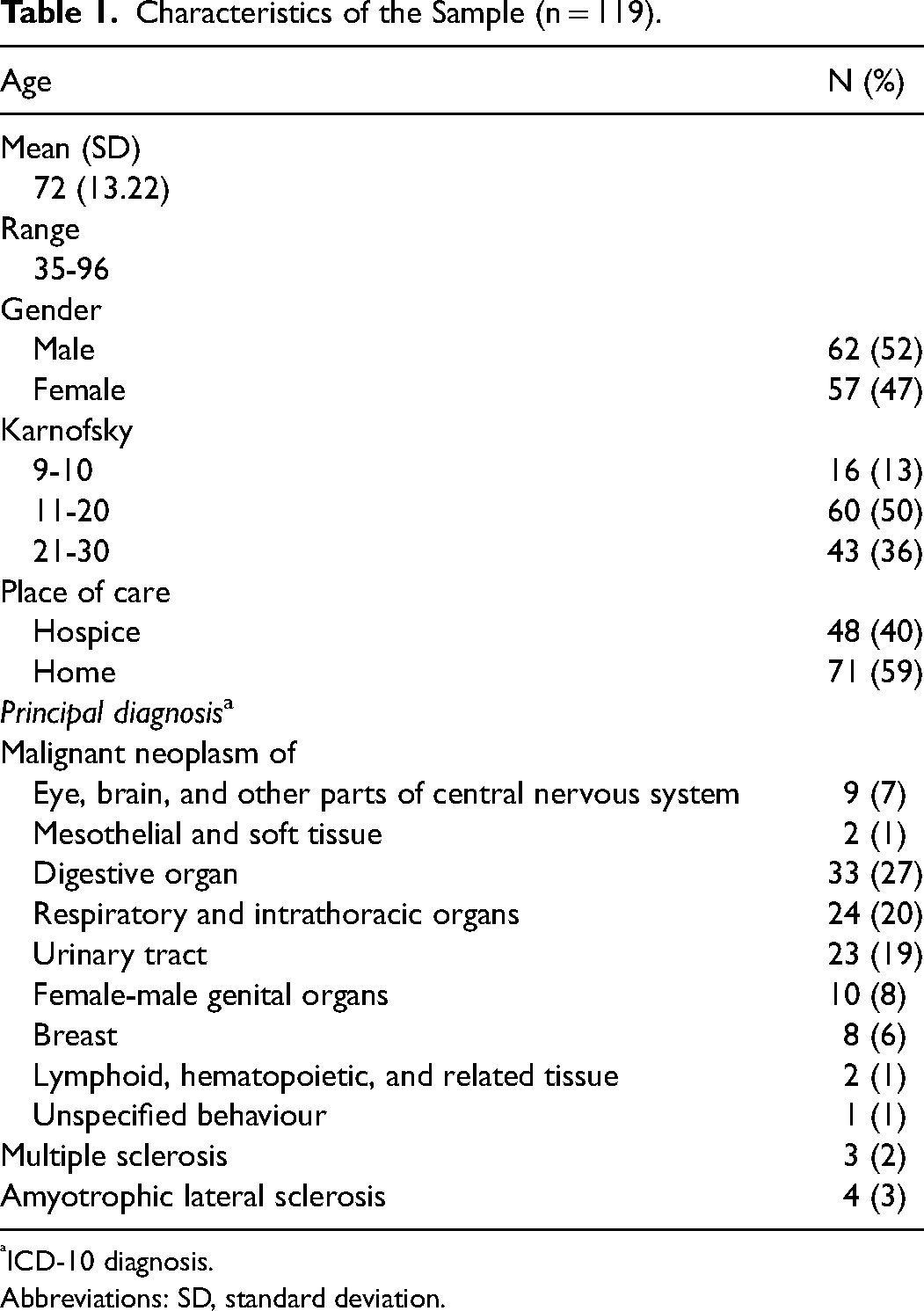
ICD-10 diagnosis.
Abbreviations: SD, standard deviation.
The mean (SD) age of the participants was 72 (13.2). Most of the patients (59.7%) were enrolled at home, while 48 (40.3%) out of 119 were admitted to a hospice. Almost the entire sample (94%) had oncological pathologies and the majority had either digestive tract (27%) or respiratory and intrathoracic organ tumours (20%).
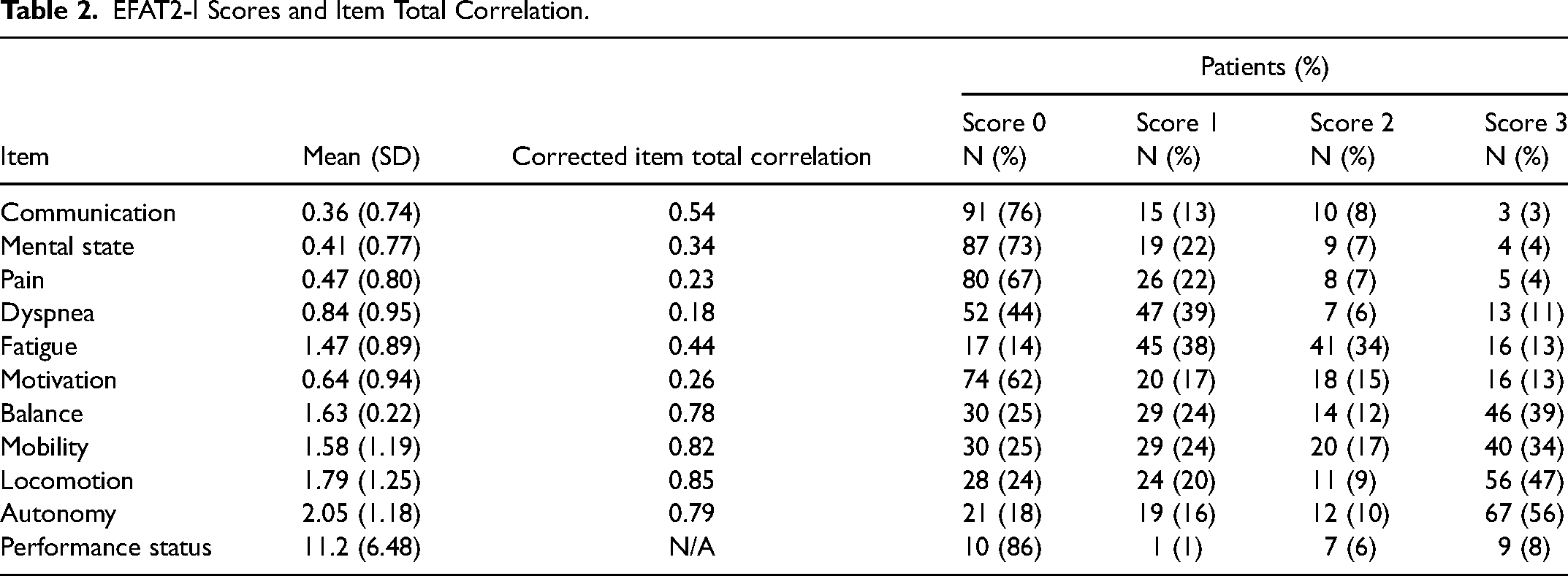
The total mean score of the EFAT2-I was 11.3, while the mean score of each item was 1.12. The worst scores were obtained by autonomy (2.05), locomotion (1.79), balance (1.63) and mobility (1.58), respectively. The majority of patients were able to communicate (76%) and had a clear state of mind (73%) (Table 2).
EFAT2-I Scores and Item Total Correlation.
The physiotherapists who administered the tool concluded that the average time required to complete the EFAT2-I was approximately 15 min and that the format was easy to complete without tiring patients. Thus, the EFAT2-I was proved to be a suitable tool for measuring functional outcome in palliative care setting.
EFAT2-I Psychometric Properties
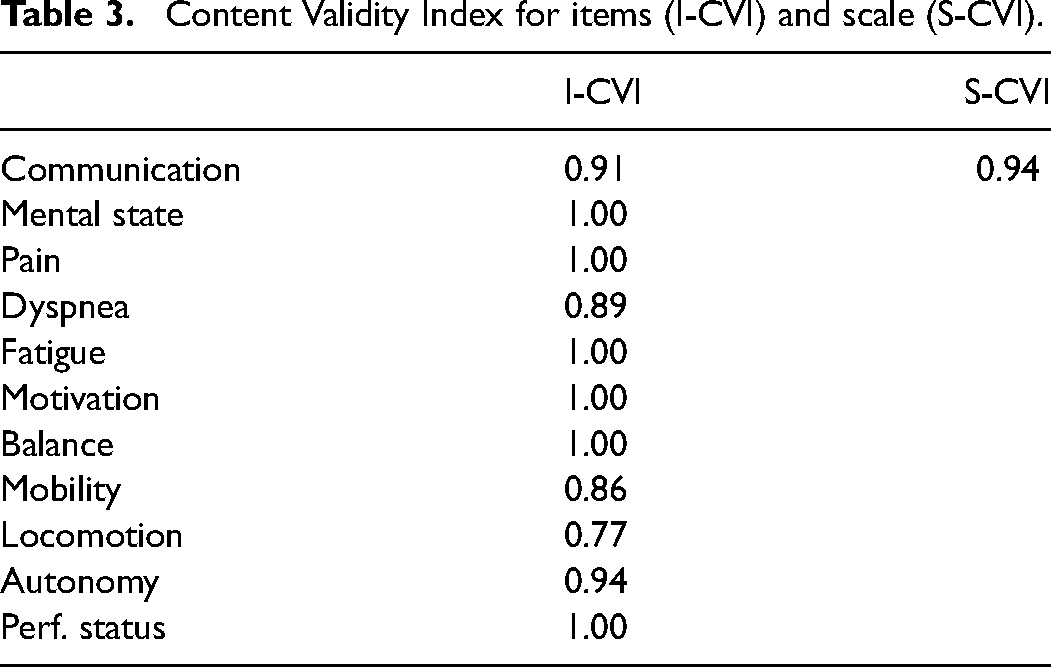
Content validity (CVI) was very good both in terms of validity the items (range 0.77-1), and in terms of the whole scale (0.94). The most problematic item was locomotion (I-CVI = 0.77) (Table 3). Construct validity was confirmed by the significant differences between the average score of the patients admitted to a hospice and the patients who remained at home (13.4 vs. 9.9), thus showing that the EFAT-2I was able to discriminate between the different conditions of the two samples under study (Table 4). The sample of patients admitted to a hospice, due to their unstable clinical condition that caused them to require residential care, had a worse score than the sample who remained at home.
Content Validity Index for items (I-CVI) and scale (S-CVI).
ANOVA (EFAT Score by Care Setting).

Concurrent validity was confirmed by Pearson's linear correlations, which turned out to be very high considering the KPS score and EFAT2-I score (r = −0.695), and the KPS and EFAT2-I descriptor “performance status” (r = −0.612). It is interesting to note that correlations between the 10 items of the EFAT2-I and the score of the descriptor “performances status” were significant (Table 5).
Correlations between KPS Score and EFAT2-I Score, and the KPS and EFAT2-I Descriptor “Performance Status”.
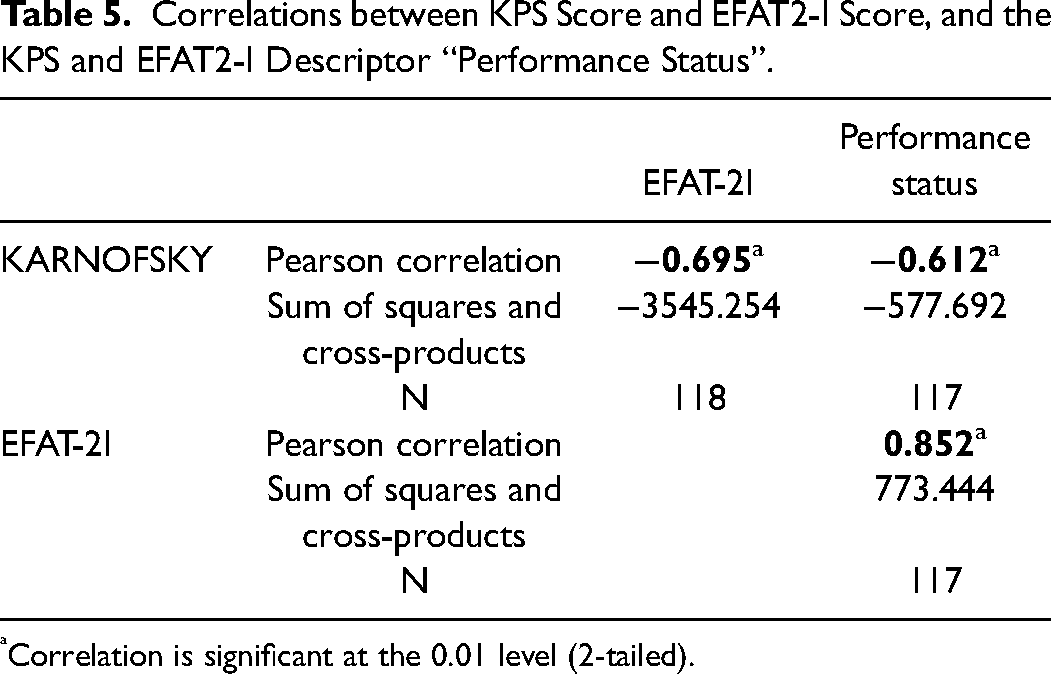
Correlation is significant at the 0.01 level (2-tailed).
The inter-rater reliability and Cronbach alpha (internal consistency) were 0.95, and 0.84 respectively. Corrected item total correlation ranged between 0.18 and 0.85. The only item that obtained a score <0.20 was dyspnoea (0.18) (Table 2). These results confirmed the good reliability of the EFAT2-I.
Discussion
The present study was performed for translating, culturally adapting, and testing the Italian version of the Edmonton Functional Assessment Tool-2 (EFAT2-I). Our results showed that the majority of the sample had an oncological diagnosis (94%), confirming the difficulties in enrolling non-oncological patients in palliative care centres. Furthermore, in accordance with other research, 45 our sample had an average age of over 70 years. As reported in Table 2, the item that obtained the worst score was “autonomy”, which underlines the fact that palliative care patients often need the help of others for their activities of daily living (ADL). The other items that received poorer scores were “balance”, “mobility”, and “locomotion”. These items show how palliative care patients were in need of physiotherapeutic intervention aimed specifically at recovering or maintaining their autonomy. On the other hand, “motivation” fortunately reported a high score, as, together with communicative and cognitive conditions, it is one of the key elements that deserves great attention when planning rehabilitation. The EFAT2-I focussed both on specific rehabilitation items and on indirect items that enable healthcare professionals to see whether it is possible to start a rehabilitation programme.
Indeed, communication, mental state, pain, fatigue and motivation are very subjective items and they make us aware of patient experiences that are otherwise not easily observable. Moreover, analysis of the above-mentioned items may mean a physiotherapist can request a timely intervention by other members of the team, such as psychologists, nurses, doctors, etc. To use the scale in order to gain a general view of the patient's condition, attention must be paid to the overall score. Nevertheless, when planning an individual therapeutic programme, it is essential to focus on each single item to understand which functions are compromised.
The results show also that the EFAT2-I has good psychometric properties, both in terms of validity and reliability. Regarding content validity specifically, experts agree that the EFAT2-I items are essential for evaluating rehabilitative functional assessment on patients undergoing palliative care. “Locomotion” obtained a CVI score of 0.77, probably because it is considered a sub-specification of the “mobility” item by the experts. According to Lynn's formula, 39 items that obtained a CVI score below 0.78 should be removed from the scale during the validation phase. In this case, however, the research team decided to keep the “locomotion” item, as it was considered substantially different from the “mobility” item. In fact, “locomotion” refers to the patient's ability to move around in a space, while “mobility” is the ability to carry out movements within the peripersonal space.
Consistently with the original study, 17 data related to construct validity confirmed that patients who remained at home and those admitted to a hospice had different functional conditions. Specifically, patients at home showed a better performance status than patients admitted to a hospice. These data confirmed the ability of the EFAT2-I to underline the differences between the two groups. The latter aspect showed that the admission criteria for home or hospice are influenced by patients’ critical clinical conditions rather than contextual factors such as not having an individual room or not having family members close by to assist them. Concurrent validity was demonstrated by the high negative correlation between the KPS correlations and those of the EFAT2-I, thus confirming the inverted scores of the two scales. There is no doubt that the EFAT2-I has the specific ability to evaluate physiotherapeutic aspects that a non-specific scale such as the KPS index is unable to identify.
Agreement among the independent assessments by physiotherapists and Cronbach alpha demonstrate the good reliability of the scale. Notably, the interrater reliability of the total EFAT2-I score resulted even better than the original version (0.95 vs. 0.88). Regarding item-total correlation, the only item that obtained a score <0.20 was that on dyspnoea (0.18). Nevertheless, by deleting it the Cronbach alpha would be only slightly improved, and as the dyspnoea represents an important parameter, the deletion was considered inappropriate.
It proved to be quick and easy to fill in the scale on a daily basis and, most importantly, it was not tiring for the patient. A minimum number of functions to evaluate, together with the option of not evaluating those items that are considered totally compromised or not suitable for assessment, means the patient is not subjected to demanding and difficult activities.
Limitations and Future Developments
This study has some limitations that must be taken into consideration.
First of all, the study was conducted in one centre only, whose organisational and clinical procedures may have had an important impact on the validity and reliability of our results. More studies need to be conducted in more centres in order to verify the psychometric features of the scale.
Secondly, the analysed sample has not been followed up over time; assessments were made at the time of admission. It would be optimal to plan studies that investigate the ability of this tool to distinguish the conditions of the sampled patients over time (responsiveness to change).
It would be interesting to investigate how the different items on the scale are aggregated, considering that some of them (pain, motivation, dyspnea, mental health) may be factors in a physiotherapeutic plan, while others are much more specific (mobility, balance, locomotion).
Conclusions
The EFAT2-I proved to have good psychometric features for evaluating physiotherapeutic elements in a palliative treatment context.
Employing the EFAT2-I in Italian would allow the comparison of results in various situations, both national and international. It would also allow for planning and would therefore join different international studies in defining and assessing the outcomes of physiotherapy during palliative treatments, giving us the chance to document the entire process.
We hope that through the daily employment of the EFAT2-I, we can highlight potentially critical issues in physiotherapeutic contexts, in order to offer new and better developments.
Footnotes
Declaration of Conflicting Interests
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.