
Abstract
Background:
Continuity of care is important for palliative patients in their end of life. In the Netherlands, after-hours primary care for palliative patients is either provided by large-scale general practitioner (GP) cooperatives or GPs choose to give palliative care by themselves while they are not on duty.
Aim:
To examine the availability of, perceived problems by, and attitude of Dutch GPs regarding providing palliative care for their own patients outside office hours.
Design and Setting:
Cross-sectional observational study among 1772 GPs from 10 Dutch regions.
Method:
Online questionnaire among GPs affiliated with 10 GP cooperatives.
Results:
Five hundred twenty-four (29.6%) eligible questionnaires were returned. Of the GPs, 60.8% were personally available outside office hours for their own palliative patients on their own private cell phone and performed home visits if needed. In 33.0%, GPs were willing to make home visits in private time instigated by the GP cooperative and 26.8% were only accessible for telephone consultation by the GP cooperative. In 12.2%, the GP delegated after-hours palliative care completely to the GP cooperative. The GPs predominantly reported “time pressure” problems (17.3%) as a barrier and 61.7% stated that after-hours palliative care is the responsibility of the own GP.
Conclusion:
The large majority of Dutch GPs is personally available for telephone consultation and/or willing to provide palliative care for their own patients outside office hours. For the future, it is important to maintain the willingness of GPs to remain personally available for their palliative patients.
Introduction
Continuity of care for palliative care patients is very important. In the Netherlands, both doctors and patients prefer that general practitioners (GPs) treat their own palliative patients not only during the day but also outside office hours. 1 –3 The Dutch GP Society (NHG) recommends that for these patients, GPs themselves are accessible and available as much as possible outside office hours. 4
To perform after-hours primary care, Dutch GPs have organized themselves in large-scale GP cooperatives. These GP cooperatives provide primary care from 5
Continuity of care in person is optimally delivered when the own GP also is available for home visits. Home visits can take place at the GP’s own initiative, after a direct request by the patient on the GP’s private cell phone, or at the instigation of the GP cooperative, when the patient initially contacts the GP cooperative for a request for help outside office hours. Previous Dutch studies investigated the availability of GPs for terminally ill patients and found that 75% to 86% of Dutch GPs are personally available for terminal care outside office hours. 8,9
Although an extension of the availability of GPs beyond office hours leads to an increased workload, GPs apparently are willing to do this extra task. However, concerns were made about the future availability of GPs for their own patients outside office hours. It has been found that there are more part-time working domestic physicians and there is an increase in the proportion of female GPs who work part-time more often. 10
We conducted this study to measure the current availability of Dutch GPs for their palliative care patients outside office hours and to monitor whether there is a change in the availability over the passing years. Second, we wanted to know whether there are differences in gender and amount of working days a week. Further, we wanted to determine perceived barriers and GPs attitude toward providing palliative care 24/7.
Methods
Design
We performed a cross-sectional observational study among GPs in the Netherlands. Data were collected by means of an online questionnaire.
Population
All 1772 GPs with an own daytime general practice in 10 regions spread over the Netherlands were invited to participate. The Netherlands consists of 50 regions corresponding to 50 general practitioners (GPCs). Every GPC was invited by e-mail and digital newsletter to participate in our study. From the interested GPCs (15), 10 were selected for their variation in size, location, and degree of urbanization. General practitioners without an own practice were excluded.
Instrument
The questionnaire was developed based on previously validated questionnaires used in similar studies and tested by experienced researchers and health-care professionals. 8,11 Additional questions were formulated by the researchers and then tested by 2 GPs.
The questionnaire focused on accessibility and availability, barriers, and attitude with respect to palliative primary care. Seventeen questions with ordinal answering scales (never/sometimes/regularly/often/always) were used. General practitioners also had the opportunity to explain matters in open questions. Furthermore, there were some topics explored in the same questionnaire which we do not report here but are planned to be published separately. In addition, GPs were asked for background characteristics: gender, age, working experience, type of practice, practice location, and number of working days per week.
Data Collection
The management of the GP cooperative in each participating region announced the study via e-mail, during a GP meeting, and/or via a digital newsletter. Subsequently, the researchers sent an e-mail with a link to the online questionnaire to all GPs with an own daytime practice in the area of the GP cooperative. General practitioners who had not responded after 14 and 28 days received a reminder. The study was performed in May and June 2016.
Analysis
The data were analyzed with the Statistical Package of the Social Sciences (SPSS) 22.0. Questionnaires with missing data were excluded. Results are expressed in percentages and means. To improve the clarity of the tables, we reduced the 5-point scales to 3 categories (see head of the tables). To examine whether GPs’ background characteristics were related to GPs’ personal availability, we performed a multiple regression analysis using gender, age, working experience, working days a week, practice location, and practice type as independent variables. All characteristics were simultaneously entered into the model to calculate independent effects. Results were considered statistically significant at P < .05. We compared our data with previous studies conducted in 2008 8 and 2011. 9
Results
Characteristics of the Respondents
The response rate was 29.9% (N = 530). Six questionnaires were excluded because of missing values, so 524 (29.6%) eligible questionnaires were included. Table 1 shows the characteristics of the respondents. About half of the GPs was female (50.3%) and the average age was 49.5 years. The practices of the GPs were mainly located in the city (43.3%) or the urbanized countryside (41.2%). Most GPs worked in a group practice (57.8%).
Characteristics of the Respondents.
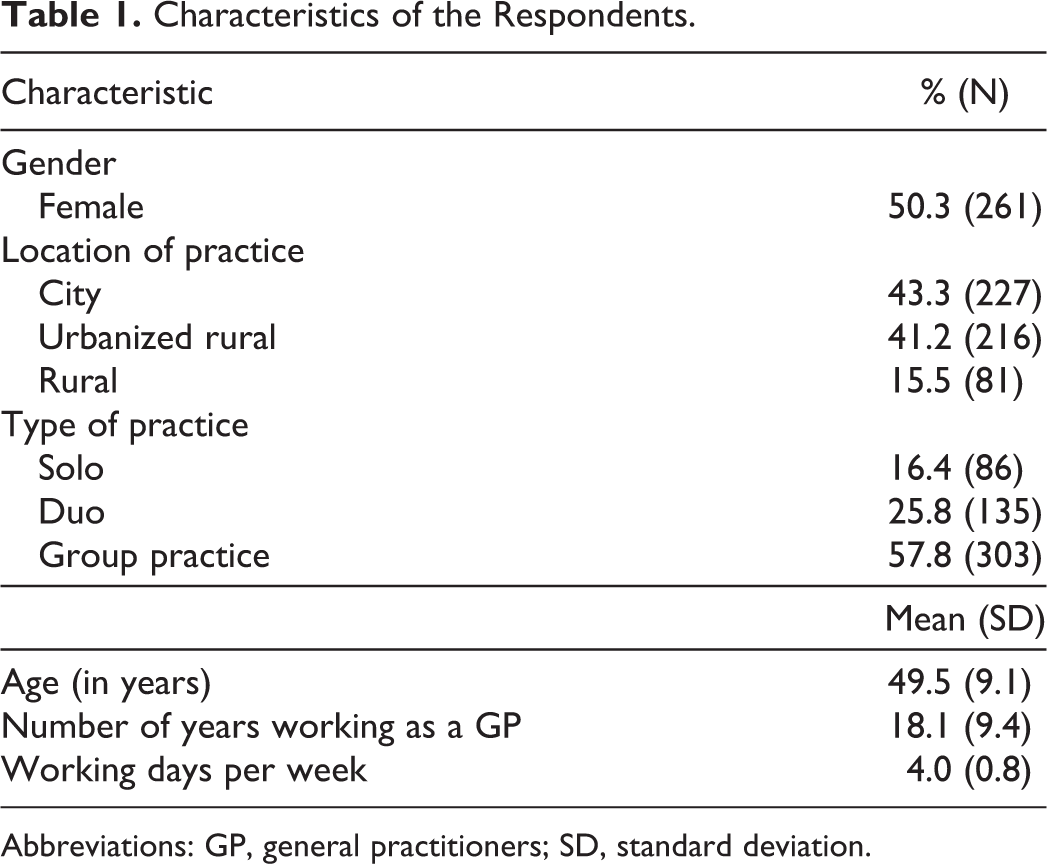
Abbreviations: GP, general practitioners; SD, standard deviation.
After-Hours Availability
General practitioners reported having an average of 5.8 (standard deviation: 4.1) palliative patients per 1000 patients per year (not in table). The majority of GPs (60.8%) reported to be available outside office hours on their private cell phone and for home visits for their own patients in the last stage of life. One-third (33.0%) was willing to make a home visit at the instigation of the GP cooperative and a quarter (26.8%) was only accessible for telephone consultation with the GP cooperative. Approximately 12% delegated palliative care completely to the GP cooperative and 8.0% delegated palliative care to a fellow doctor from their own practice. Of the GPs who were personally available, 54.8% reported to make home visits on their own initiative (Table 2).
Availability of GPs Outside Office Hours for Their Own Patients at the End of Life.
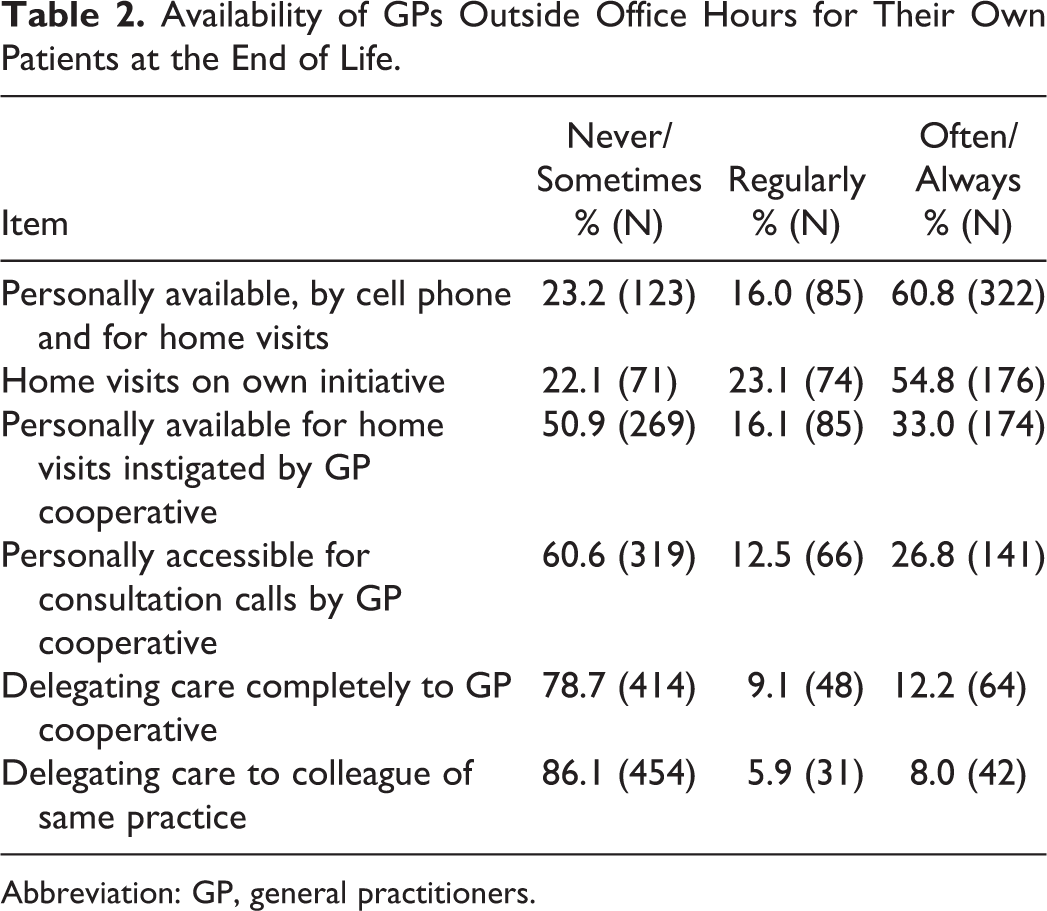
Abbreviation: GP, general practitioners.
There were significant differences between GPs’ personal availability regarding gender (B = −0.97; 95% confidence interval [CI]: −1.23, −0.71), the number of working days per week (B = −1.39; 95% CI: −1.62, −1.15), and location of practice (B = −2.08; 95% CI: −2.62, −1.54): female GPs, GPs working less than 3 days a week, and GPs having a practice in the city or urbanized countryside were less available for palliative patients in their end of life. Personal availability for palliative care was not related to age, type of practice, and working experience.
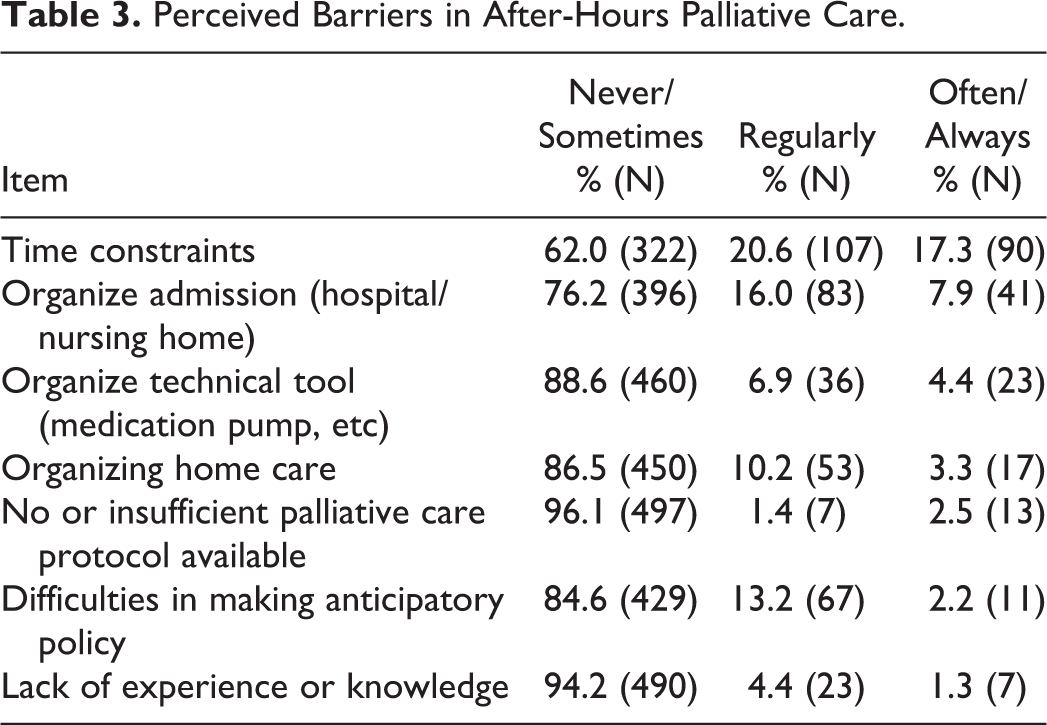
A number of possible problems was presented to the GPs for the situation if they were personally available outside office hours for their own palliative patients (Table 3). Problems with “time pressure” (17.3%) and “organizing a hospital or nursing home admission” (7.9%) were experienced most frequently. Besides the presented potential problems, several GPs (N = 44) mentioned in the free text that being personally available 24/7 conflicts with private life.
Perceived Barriers in After-Hours Palliative Care.
Almost every GP perceived palliative care as a beautiful part of the profession (94.0%). Most GPs indicated that their accessibility and availability outside office hours increases when the patient’s life expectancy decreases (86.7%). A large part of the GPs felt that personal availability gives better quality of care (76.6%) and that after-hours palliative care is the responsibility of the own GP (61.7%; Table 4).
Attitudes of GPs Concerning After-Hours Palliative Care.
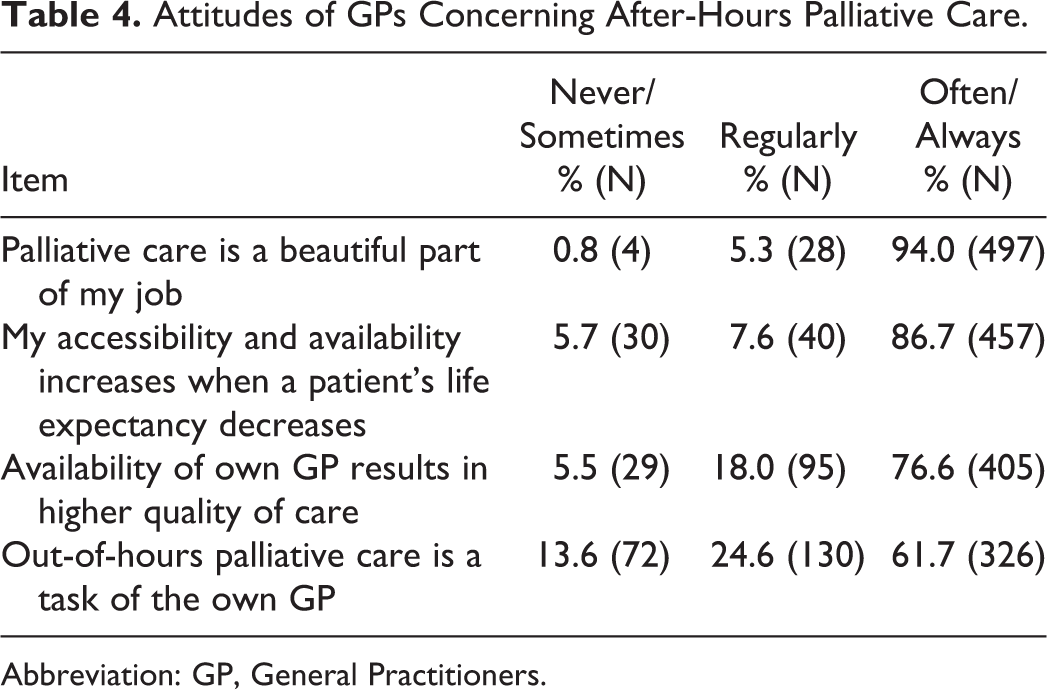
Abbreviation: GP, General Practitioners.
Discussion
Summary
Most GPs (61%) are personally available by phone for their own palliative care patients outside office hours and make home visits if necessary. One-third was willing to make a home visit at the instigation of the GP cooperative and a quarter was only accessible for telephone consultation with the GP cooperative. A small group of GPs delegates care to a colleague of the same practice, which most of the times is also familiar with the patient. Another small minority of GPs fully delegates palliative care to the GP cooperative. General practitioners sometimes find it hard to be personally available outside office hours because of a conflict with their private life. This corresponds with our finding that part-time working GPs were less available for patients in the final stage of life. We also found that female GPs and GPs having a practice in the city or urbanized countryside were less available for palliative patients. These findings support our concerns about the availability of GPs in the future as the proportion of female, part-time working GPs increases. 10
When GPs do provide palliative care outside office hours, they most frequently experience time constraints and problems in organizing admissions. Almost each GP believes that palliative care is a beautiful part of the job and that accessibility and availability should increase with decreasing life expectancy of the patient. However, only slightly more than 60% believes that the own GP should do all palliative primary care.
Strengths and Limitations
A large number (N = 524) of GPs in 10 regions located across the country participated in our study, although the response rate is rather low (29.6%). Furthermore, all kinds of practices in terms of size and location (rural to city) were represented. We were not able to perform a nonresponse analysis, but the GPs who responded were representative for the total population of Dutch GPs in terms of age, sex, and working experience. 10 A limitation is that we asked the GPs about their own accessibility and availability. This could have led to socially desirable answers, although the survey was anonymous. A selection bias may have taken place since GPs with an interest in palliative care could have been overrepresented. This could have resulted in an overestimation of GPs being personally accessible and available for palliative care.
Comparison With Existing Literature
Few studies have been performed on this topic. In 2008, Giesen et al showed that 75% of Dutch GPs, in principle, was personally available for their own terminal patients, of which 65% directly on their own cell phone and 45% (also) by the GP cooperative. 8 Hoexum et al found a higher percentage: 86% of the GPs was willing to provide after-hours care for their own terminally ill patients. 9 Similar to our findings, they found a higher availability for male GPs and no differences in availability related to the age or working experience of the GP. Similar to our findings, they found that GPs working in rural areas were more available for palliative care. Our study showed that GPs having a practice in the city or urbanized countryside were less available for patients in the final stage of life. It should be noted that the comparability of these studies with our study is limited, as the included period of delivered care differs: Giesen et al studied the “terminal phase” of disease and Hoexum et al specified that this terminal phase lasts “a few days to a few weeks.” Further, we asked respondents to judge their palliative care in general, not specifically the terminal phase. This can explain why we, in general, found a lower accessibility and availability.
A study among Canadian family physicians (FPs) and GPs revealed that almost every FP/GP (95%) provided home visits after hours. 12 However, it is not mentioned in which capacity they performed this palliative care: Are they making home visits in their own private time (the main focus of our study) or on duty for a larger organization (eg, group practice, general home visit service). So these numbers are not comparable with ours.
Implications for Research and/or Practice
Palliative care is a field with increasing size. This growth is accompanied by an increasing interest among professionals. The professionals are also under pressure, however, when palliative care is provided outside office hours and the balance between private time and work is under pressure. First, it would be interesting to study the strategies that GPs have to monitor this balance, while at the same time being available as much as possible and providing good quality of care. General practitioners, for example, can more often hire an observing GP for their daily work, so that they have more time—both during the day and outside office hours—for palliative patients when their request for help increases in (pre)terminal phase of disease. Another possible reduction in work pressure can be obtained by sharing this care with a colleague from the same GP practice. Second, we advise to measure and publish the availability of GPs periodically as one of the indicators to monitor the quality of palliative care outside office hours. This information can also stimulate GPs to increase their participation in palliative care. And finally, it would be interesting to explore how the participation of female GPs can be improved.
Conclusion
The majority of Dutch GPs is personally available for telephone consultation (by patient or by GP cooperative) or willing to deliver palliative care during home visits for their own patients outside office hours in their own private time. General practitioners experience palliative care as a beautiful part of their profession and state that personal availability outside office hours gives better palliative care. For the future, it is important to maintain the willingness of GPs to make extra efforts for their own patients, while they are not on duty for the GP cooperative, and to examine barriers and facilitators.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by ZonMW (projectnumber R0003118); ZonMW, PO Box 93245, 2509 AE The Hague.