
Abstract
Saddle nose deformity is most often the result of intranasal cocaine use, but it may also occur in autoimmune conditions such as granulomatosis with polyangiitis (GPA). Many of these patients are poor candidates for surgical reconstruction because of poor vascularity, ongoing substance use, or large septal perforations, making rib grafting and traditional techniques high risk. In our practice, we have managed this challenging group with injectable filler as a minimally invasive alternative. Between January 2020 and June 2025, 6 patients with cocaine-induced saddle nose deformity were treated in an outpatient setting using Revanesse Sculpt. Outcomes were assessed with standardized pre- and posttreatment photographs and Standardized Cosmesis and Health Nasal Outcomes Survey (SCHNOS) scores obtained at baseline and 3 months. Patients demonstrated visible cosmetic improvement with restored contour and symmetry. All procedures were well tolerated under local anesthesia. To our knowledge, this represents one of the first detailed descriptions of a systematic filler technique for managing saddle nose deformity in this high-risk population. This approach provides a safe, cost-effective, and reproducible method for temporary correction when surgical reconstruction is not feasible.
Introduction
Saddle nose deformity (SND) represents a complex structural and aesthetic challenge, characterized by loss of septal and dorsal support with consequent nasal airflow compromise and esthetic distortion.1,2 Chronic intranasal cocaine is one of the most common etiologies. 1 Through potent vasoconstrictive and ischemic effects, cocaine induces mucosal necrosis and cartilage loss, leading to cocaine-induced midline destructive lesions (CIMDL). 3 Septal perforation occurs in nearly all long-term users, with disease progression extending to the palate, paranasal sinuses, and bony framework. 3 Autoimmune vasculitis, particularly granulomatosis with polyangiitis (GPA), may produce a similar destructive pattern, complicate diagnosis and resulting in severe cosmetic and functional impairment.1,4 Surgical reconstruction with autologous rib, septal, or costal cartilage grafts remains the standard treatment, offering durable structural restoration. 5 However, surgery is not universally feasible. Patients with ongoing cocaine use, impaired vascularity, massive perforations, or significant comorbidities face increased risks of infection, graft failure, and poor healing, while the financial and time burdens of surgery may further limit access. 2 Injectable fillers, widely used in cosmetic rhinoplasty, offer a minimally invasive alternative for selected patients. 6 Hyaluronic acid fillers can temporarily restore nasal contour with relatively low morbidity, minimal downtime, and reduced cost, making them particularly useful for patients unsuitable for formal reconstruction. 6
In this study, we present our nonsurgical technique using Revanesse Sculpt for the correction of cocaine-associated SND. We describe our injection technique, evaluate patient outcomes, including pre- and posttreatment Standardized Cosmesis and Health Nasal Outcomes Survey (SCHNOS) scores, and discuss the role of injectable filler as a practical adjunct or alternative to surgical reconstruction in this challenging patient population.
Methods
Patient Selection
This study was a retrospective, single-center descriptive chart review conducted at a private outpatient Otolaryngology–Head & Neck Surgery clinic between January 2020 and June 2025. Eligible participants were adults (≥18 years) with saddle nose deformity secondary to cocaine use or GPA who underwent filler injection with Revanesse Sculpt (Prollenium Medical Tech, Richmond Hill, Canada). Patients were included if they had standardized pre- and posttreatment photographs, documented procedure details, and SCHNOS scores at baseline and 3 months. Patients were excluded if the deformity was unrelated to cocaine or GPA, if records were incomplete, or if research consent was not obtained.
Preoperative Assessment
All patients underwent standardized clinical photography before the procedure. Standardized Cosmesis and Health Nasal Outcomes Survey questionnaires were completed at baseline.
Procedure
All procedures were performed in the outpatient clinic under local anesthesia. A Doppler ultrasound probe (Huntleigh DMX Digital High Sensitivity Vascular Ultrasound; Huntleigh Healthcare; unit cost $1617 CAD) was used to map out the location of the various facial arteries (labial, facial, supratrochlear, supraorbital, dorsal nasal) to ensure there was no confounding vessel in the surgical field that would risk occlusion. Once this was completed, the location of the saddle nose was drawn out, after which Revanesse Sculpt was injected using the manufacturer kit including 30g needle to augment the depressed segment of the dorsum. In all cases areas of stability were palpated for that would assist in acting as a firm “floor” to place the filler on, in most cases being either residual upper lateral cartilage or residual dorsal septum. Most patients required a full syringe (1-1.2 cc) of filler to complete the augmentation. Representative arterial mapping and the planned safe midline injection plane are shown in Figure 1; handheld Doppler probe positioning with a representative tracing is shown in Figure 2.
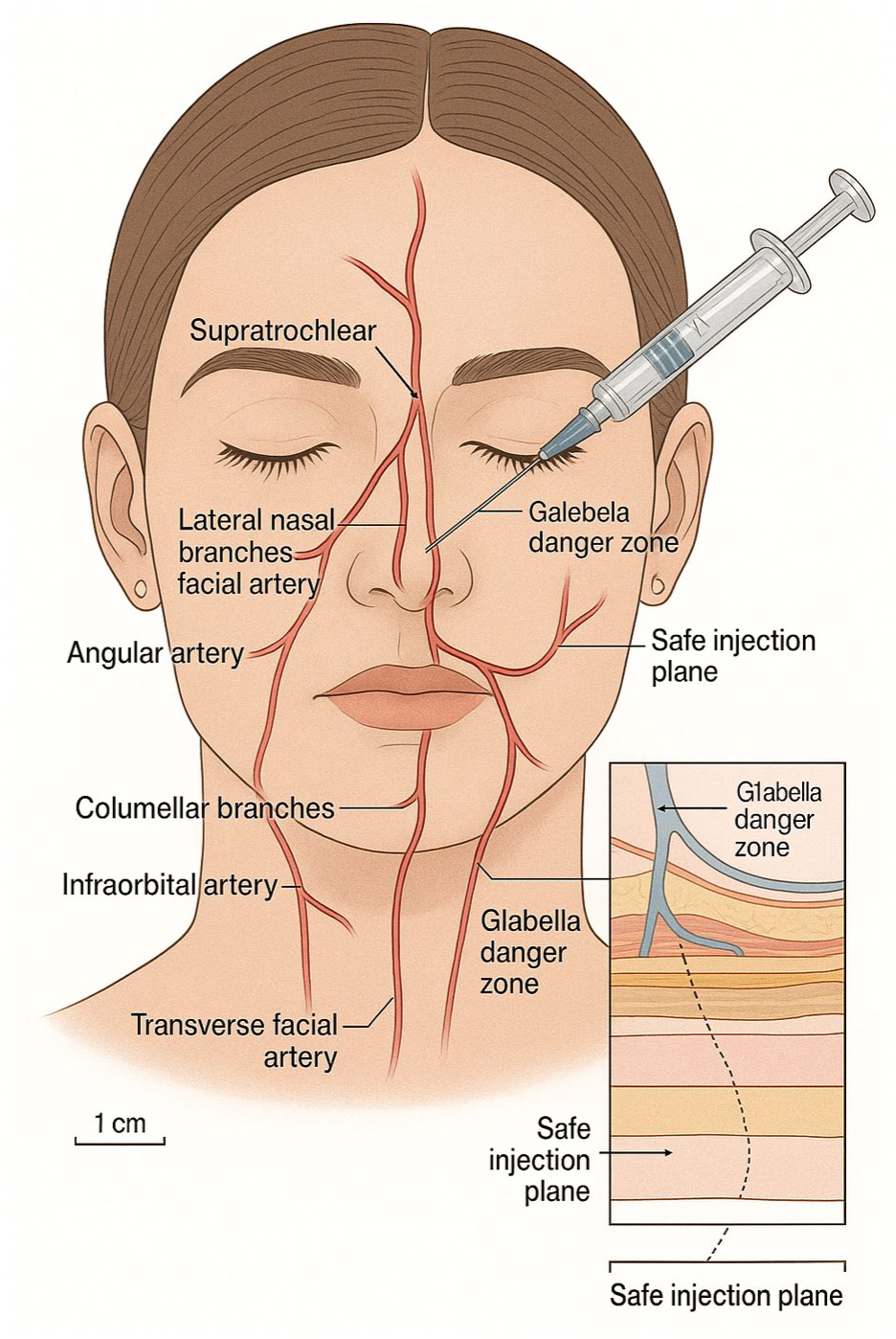
AI-generated medical illustration of frontal arterial anatomy and Doppler-informed injection plan for correction of saddle-nose deformity.
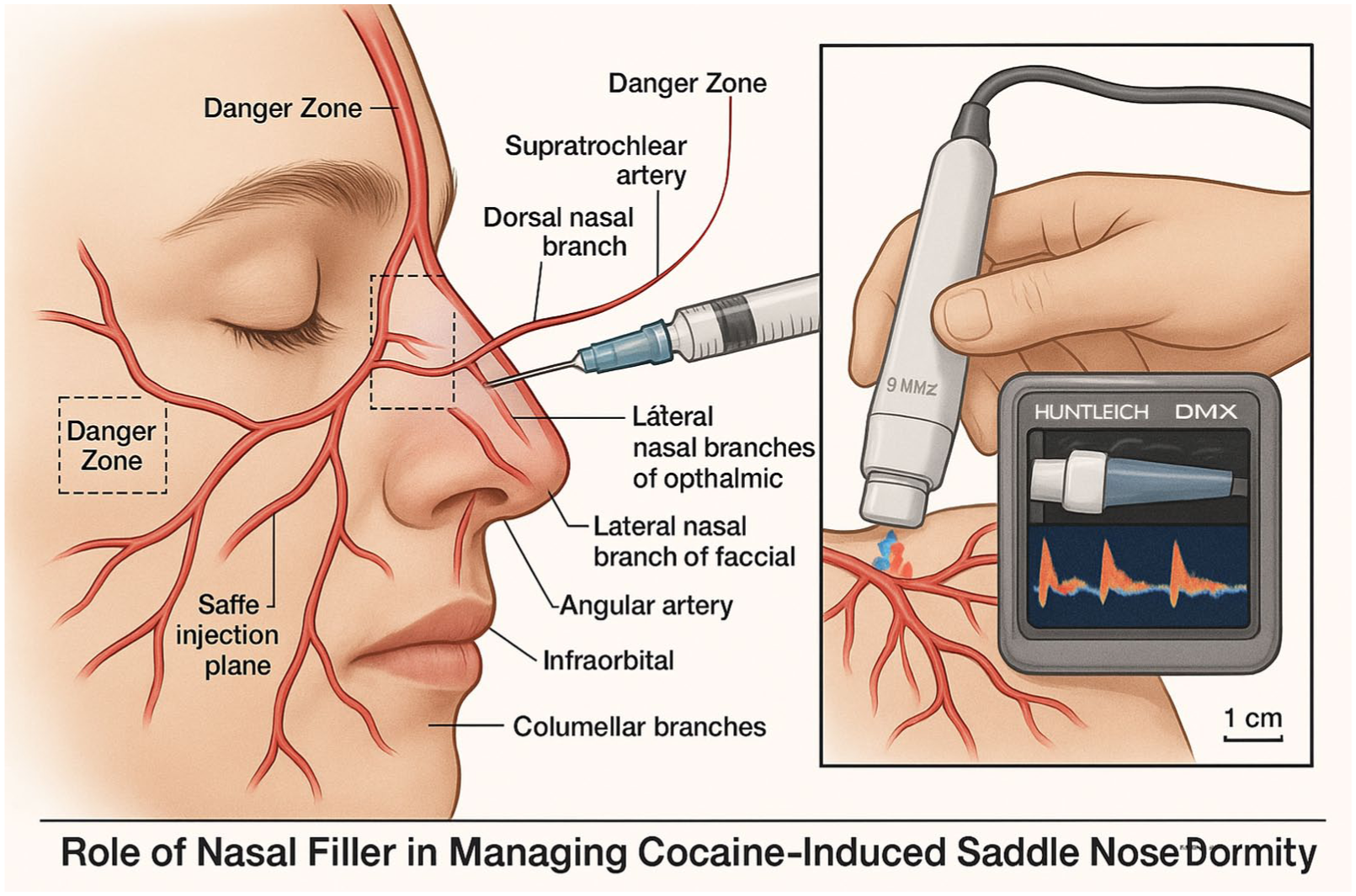
AI-generated medical illustration of handheld Doppler (Huntleigh) mapping of perinasal vessels prior to nasal dorsum injection.
Results
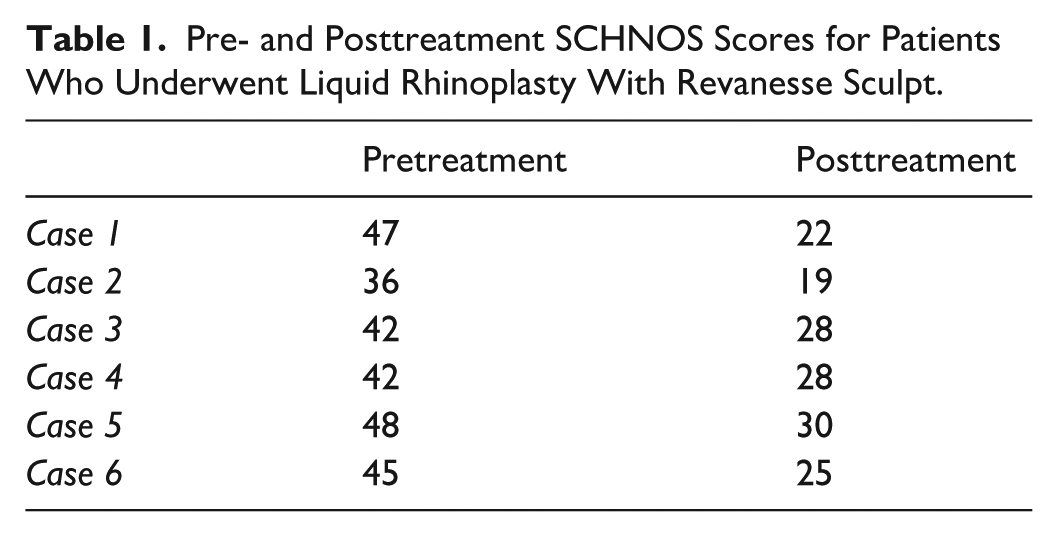
A total of 6 patients were treated with cocaine-induced saddle nose deformity. All patients demonstrated visible improvement in dorsal contour, height, and midline projection. Standardized photographs confirmed cosmetic changes. Standardized Cosmesis and Health Nasal Outcomes Survey scores improved from baseline to 3 months (mean pretreatment 43.3 vs posttreatment 25.3). Illustrative AI-images of the pre-injection mapping and Doppler used to avoid at-risk vessels are provided in Figures 1 and 2, and Table 1 reviews the SCHNOS scale changes. Figures 3 and 4 provide reprensative results of this technique.
Pre- and Posttreatment SCHNOS Scores for Patients Who Underwent Liquid Rhinoplasty With Revanesse Sculpt.
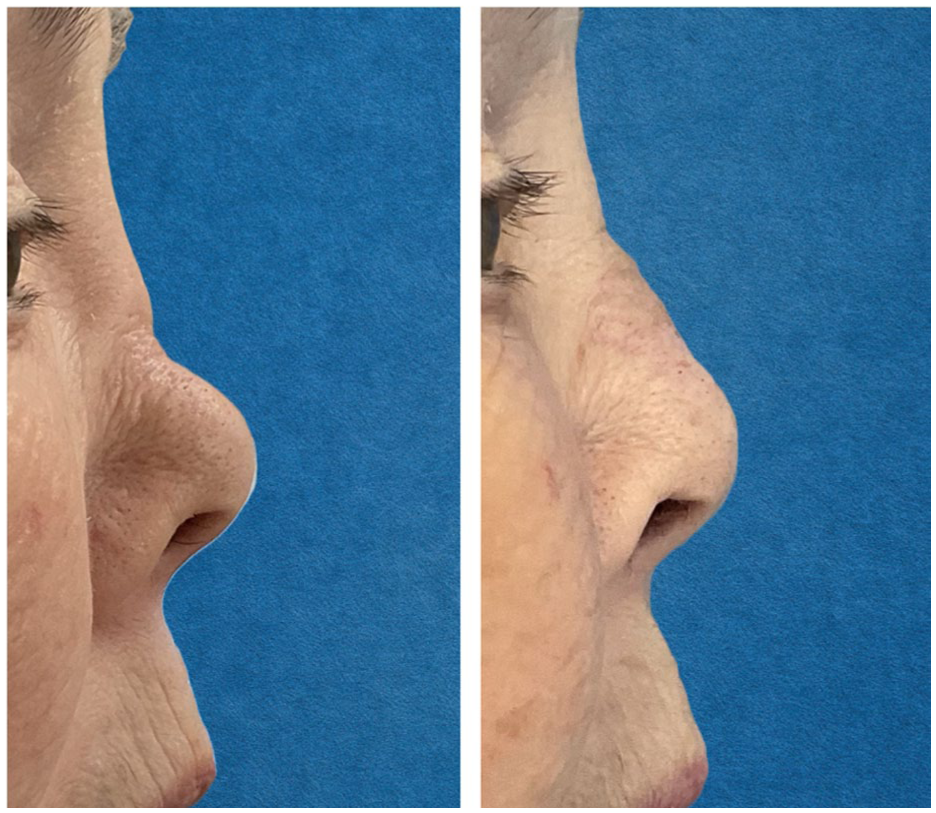
Patient 1 at baseline (left) and 12 months posttreatment with 2 injections (1.0 and 1.1 cc, right).
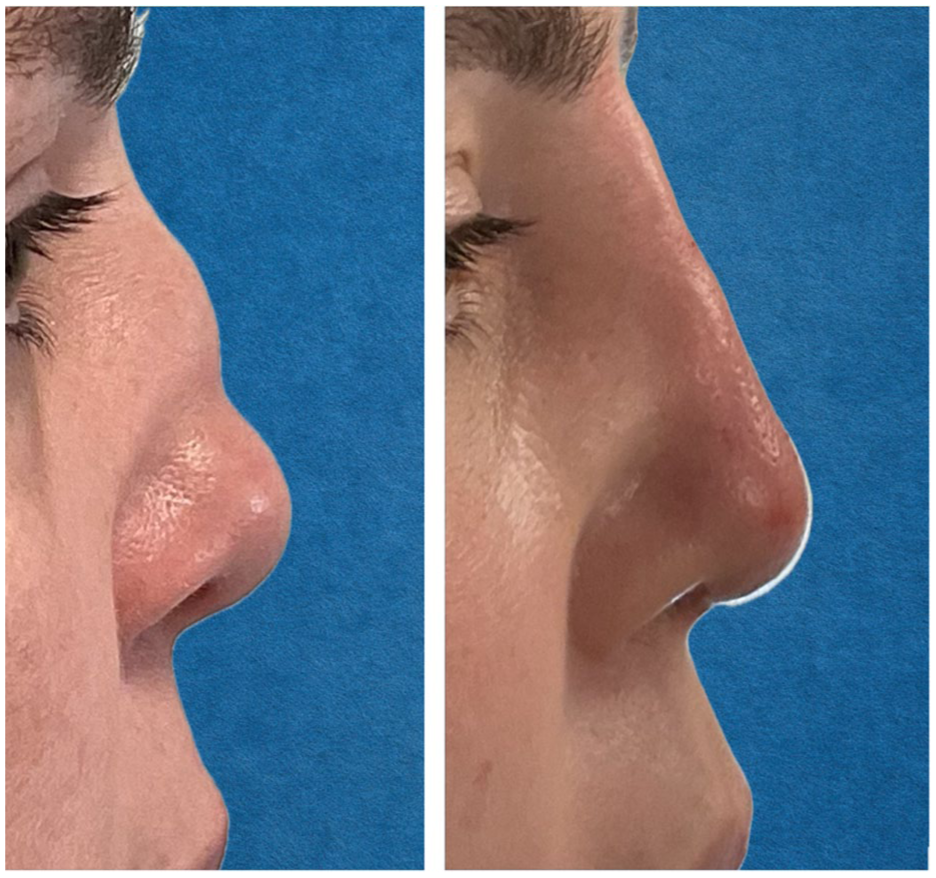
Patient 2 at baseline (left) and 14 months posttreatment with 2 injections (0.9 and 1.2 cc, right).
No complications were reported beyond mild skin redness at the injection sites that self-resolved. There was no vascular occlusion. Four patients required 2 sessions 6-months apart to achieve long-lasting results; 1 patient required a third session. This pattern highlights the short-term nature of filler efficacy and underscores the need for further study of durability and maintenance strategies.
Discussion
Cocaine-induced SND remains a reconstructive challenge, as ischemic tissue damage results in septal perforation and midline collapse. 3 Although autologous grafting with rib or bone provides durable structural restoration, many patients with cocaine-associated deformity are unsuitable for major surgery. 7 Poor vascularity increases the risk of graft necrosis and infection; ongoing cocaine use further compromises healing; massive septal perforations limit the feasibility of rib or septal grafting; and for many, the financial and time burdens of open reconstruction are prohibitive.4,7,8
In this context, injectable filler represents a practical and accessible alternative. In our series, Revanesse Sculpt produced meaningful improvements in nasal contour and SCHNOS scores. These results mirror broader nonsurgical rhinoplasty data for other indications showing high efficacy with low complication rates. 9 Importantly, no major complications occurred in our study, consistent with large, published cohorts of nonsurgical rhinoplasty in which serious adverse events such as vascular compromise or necrosis were rare.8,10
Our findings align with recent literature. Ossanna et al 11 demonstrated sustained satisfaction in 97 patients undergoing nonsurgical correction of SND with hyaluronic acid filler and adipose-derived products. Jalali reported durable correction of cocaine-related SND, maintaining results at 18 months with only transient side effects. 8 Harb and Abdul-Razzak described over 2000 cases where fillers successfully addressed post-surgical deformities, again with high satisfaction and minimal complications. 10 Together, these studies support injectable fillers as a safe, reproducible, and minimally invasive adjunct or alternative to structural reconstruction, particularly in high-risk patients. Our study differs from those in that in the aforementioned citations many patients with CIMDL were excluded from the data pool, whereas in our group these were the patients specifically treated. Since CIMDL lesions represent a large number of the patients who present with SND, but their needs are complex but reconstructive options are limited, the data from our study presents a new safe and effective method of treating these patients who are otherwise limited by both finance and reconstructive options.
It is important to emphasize that filler injections are inherently temporary. While our study demonstrates cosmetic benefit, durability remains limited. Filler may represent a particularly reasonable option for patients with unstable disease status, such as those with GPA or ongoing cocaine use, where reconstructive surgery may not be feasible due to healing concerns or disease progression. This study is limited by its small sample size and short follow-up, but it represents the first systemic techniques for filler use in the CIMDL group. We plan to initiate a prospective extension of this cohort and subsequent patients with planned longitudinal follow-up, including standardized photography and SCHNOS assessments, that will report durability and maintenance intervals. Future prospective studies should evaluate long-term durability, evaluate the role of repeat treatments in enhancing durability, compare filler rheology in structurally deficient noses, and further define patient-reported outcomes.
Conclusion
Patients with cocaine-induced saddle nose deformity are frequently poor candidates for major reconstructive surgery due to compromised vascularity, ongoing cocaine use, massive septal perforations that preclude grafting, and prohibitive cost. In this high-risk population, injectable filler with Revanesse Sculpt provides a simple, safe, and cost-effective option for temporary correction. Although not permanent, filler offers immediate restoration of contour with minimal morbidity, serving as a practical bridge or alternative when traditional graft-based reconstruction is not feasible.
Footnotes
Acknowledgements
The authors thank the participating patients for their consent to use anonymized photographs and clinical data for research and teaching purposes. AI-generated educational illustrations (non-clinical) were created using a generative image tool to depict generic nasal arterial anatomy and probe positioning. Prompts and edits were provided by the authors; outputs were reviewed and verified for anatomical accuracy. No patient images or protected health information were used.
Ethical Considerations
Ethics approval was obtained. All participants had previously provided written informed consent for research use of medical data and photographs.
Consent to Participate
Written informed consent to participate in research was obtained from all included patients.
Consent for Publication
Written informed consent for publication of anonymized clinical images was obtained from all patients.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study are securely stored on encrypted Western University servers. Anonymized data may be available upon reasonable request from the corresponding author, subject to ethical approval.