
Abstract
Informed consent is a foundational component of ethical patient care and may be effectively provided when a competent patient is given pertinent information to make well-informed decisions on their health care. Various studies have considered patients’ experiences with surgery for aesthetic reasons, rather than plastic surgery procedures which are medically warranted for reasons such as restoring form and function. Current empirical discourse on the consenting process, and ultimately how informed patients undergoing cosmetic surgical procedures are, is scant, particularly in Australia. The key aim of this review was to synthesize qualitative and quantitative research which considers the consenting process and the factors which impact on the patient’s decision-making process to undergo invasive cosmetic procedures. Eligible studies were identified via systematic searching across the PubMed and Medline databases; and hand searches were conducted of gray literature databases including university databases and Google Scholar. Reference lists of included studies were also examined for relevant studies. Eligible studies had to meet specific participant criteria including an age requirement of 19 to 64 years and discuss factors or present discussion surrounding the “informed consent” process for invasive cosmetic procedures. The characteristics and findings of each study were extracted. The studies were analyzed and presented under question categories. The Mixed Methods Appraisal Tool was used to assess the quality of evidence. Thirty-one studies were eligible for inclusion. Most studies were quantitative (90.3%). The highest proportion of these studies were focused on the United States (51.6%), followed by the United Kingdom (12.9%). The dominant methodology utilized by these studies was questionnaires/surveys (37.5%). The literature identified was classed into one of the 5 groups based on their overall concepts and objective. These 5 categories included (1) articles focusing on the types of information which should be communicated to a patient before they undergo their procedure or provide consent; (2) legal claims and cases based on a lacking informed consent; (3) sources of information patients access to become “informed” on their procedure; (4) studies exploring the readability of online information on certain invasive cosmetic procedures; and (5) studies focusing on the most effective methods of obtaining patient consent for cosmetic surgery procedures. These categories were reformulated into research questions and addressed in the section “Results of the Findings.” Most of the studies included in this review were quantitative (90.3%). Most studies (where gender was mentioned) had a higher population of female participants or respondents. Women have a greater tendency to have cosmetic surgery opposed to men. There are few studies (particularly qualitative studies) exploring the pre-operative patient experience in Australia for those having or seeking cosmetic surgery. A key stage in this process is obtaining and providing informed consent. A “lack of informed consent” is one of the more dominant factors identified consistently throughout these studies which focus on legal case reviews and claims. A significant source of information patients use to become informed of their procedure is through the Internet. This may be problematic as the readability of online materials is most commonly above the recommended reading level in multiple jurisdictions; and some online materials may have questionable accuracy or validity. Whether or not patients verify the information they access through external sources such as this, is of concern. There have been minimal studies identified exploring the patient experience pre-operatively including during their consultations and decision to provide consent.
Keywords
Introduction
Cosmetic surgery often described as “aesthetic surgery” (such as breast augmentation) is on the rise in Australia and overseas. The industry’s popularity and remunerative nature is reflected in its 2015 estimated annual value of $1 billion (AUD). 1 Cosmetic procedures have become widely accepted in Australia, coinciding with the rise of social media and advances in aesthetic centered medicine. 1 Commonly performed elective procedures include face lifts, liposuction, and breast enhancements. Women tend to be the more dominant group opting for elective cosmetic surgery, although the number of men undergoing cosmetic surgery is also increasing. 2
Piras et al 3 identify cosmetic surgery as one of the 2 branches of plastic surgery. Cosmetic surgery is defined as the desire of patients to improve features or parts of their bodies they perceive to be imperfect. The Medical Board of Australia in their “Guidelines for registered medical practitioners who perform cosmetic surgery and procedures” (2023) (“Guidelines by the Medical Board of Australia”) separates medically justified surgery or procedures from cosmetic surgery, which may lead to improvement in appearance. These guidelines also separate reconstructive surgery from cosmetic surgery, as reconstructive surgery restores form and function, as well as normality of appearance. This review excludes medically justified plastic and reconstructive surgeries. The predominant focus of this review is on cosmetic surgical procedures which have the main objective of achieving what the patient views to be a more desirable appearance. 4 Piras et al 3 identify further that one of the most pertinent topics concerning cosmetic surgery includes the receiving of informed consent. Despite the clear demand for cosmetic surgery, there appears to be minimal knowledge about the characteristics of the patients. 2 Furthermore, very little literature has examined women’s motivations for having cosmetic surgery, and the surgery process they undergo including consultations, aftercare, and recovery. 5 The lack of research in this area (particularly in Australia) is problematic due to the scrutiny surrounding the regulation of the industry. The quality of consent provided by patients may be problematic when considering the commercial nature of the industry and the advertising styles of some medical practitioners. 1
Consent involves the voluntary and active permission of the patient to have a particular treatment based on sufficient knowledge of the purpose, nature, and risks of the treatment. This includes the prospects of the treatments “success” and any alternatives to it. 6 Consent is a process rather than a single event. Consent can be withdrawn at any point and should be given by an individual who is adequately informed and capable of making this decision. 6 Informed consent is consent which is obtained from a patient following the discussion of the risks and benefits of the procedure, compared to alternative procedures or the absence of any treatment. 6 Based on these definitions, it appears that the process of providing “informed consent” is 2-fold. This involves the patient’s decision to consent, and the practitioner’s ability to identify whether valid and informed consent has been given, by ultimately accepting that decision and proceeding to conduct or prepare for the surgery.
Guideline of Patient’s Decision-Making for Cosmetic Surgery
The Guidelines by the Medical Board of Australia (2023) state that informed consent is an individual’s voluntary decision made in consideration with the comprehension and knowledge of the benefits and risks of their medical treatment. According to these guidelines, effective medical practice involves providing information to patients in a manner they can comprehend prior to obtaining their consent. Consent cannot be requested from the patient at their initial consultation and must be provided by the patient at the consultation with the medical practitioner who will perform their surgery. Following the patient’s 2 consultations and informed consent, they are required to have a “cooling-off period” of at least 7 days before they may book their surgery or pay a deposit. 4
The guidelines state that the information provided by the medical practitioner who will perform the surgery must not glamorize the surgery, underplay the complexity of the surgery, overstate the outcomes of the surgery, or insinuate that the patient may achieve unrealistic expectations from the surgery. The information provided to the patient should include information about the cosmetic surgery; the logistics around the surgery (including pain management and anesthesia); the location where the surgery will be conducted; the nature of the surgery (new or experimental); the different possible outcomes of the surgery (both short and long term); the risks, including the possible complications associated with the surgery (both short and long term); patient-specific risks; the likelihood of revision surgery or more treatment (both in short and long term); details about the recovery period including recovery time and care requirements; the registration of the medical practitioner (including whether the medical practitioner has an endorsement for cosmetic surgery on their registration [if applicable]); the qualifications, training, and experience of the medical practitioner; and the other practitioners who will be involved in the surgery (if applicable). Patients will need to be made aware of fees and charges within an appropriate timeframe, to make an informed choice to proceed with consultations and the procedure. Additional costs will need to be disclosed to the patient. 4
Factors Contributing to Patient’s Decision-Making
Various factors may impact a patient’s decision-making process when they provide consent. This may include psychological conditions such as body-dysmorphic disorder (BDD). Body-dysmorphic disorder may be defined as an obsessive-compulsive disorder centered around an obsession with perceived impairments in physical appearance which are unnoticeable or appear to be minor to others. This obsession may cause great distress or impairment in different areas of functioning, including social or occupational. 7 In the Guidelines by the Medical Board of Australia (2023), practitioners are required to assess the patient for underlying psychological conditions (such as BDD), which may make them an unsuitable candidate for their surgery through a validated psychological screening tool. 4 This review seeks to extend the current discourse by (1) summarizing the extent of “informed consent” as a basis for claims against medical practitioners or surgeons providing aesthetic, invasive procedures; (2) highlighting the need for further research and collection of Australian data on patient experiences of the consent process including engagement with information materials and sources on their respective procedures, ultimately affecting the “informed consent” process; and (3) the most effective methods in ensuring patient consent.
Research Questions
“Cosmetic surgery,” “aesthetic surgery,” and “plastic surgery” may be used interchangeably throughout this review to mean invasive (surgical as opposed to non-surgical) procedures associated with aesthetic purposes or to achieve what is perceived to be a more desirable appearance.
Methods
Search Strategy and Selection Criteria
Peer-reviewed articles were searched across the PubMed and Medline databases from June to July 2022. Search terms were created by centering our primary search around materials combining search terms such as “consent” OR “informed consent” AND “plastic surgery” OR “cosmetic surgery.” All search terms and variations of search terms were searched for in all titles, abstracts, and keywords. A preliminary search indicated that there were minimal Australian studies collecting data from Australian participants. Therefore, it was decided that international studies would also be included. Filters were applied on both PubMed and Medline databases to limit the scope of the articles obtained. These filters included articles only considering participants aged 19 to 64 years; were in English; and published between 2012 and 2022.
A much broader search without filters was conducted and manually reviewed in addition to the main search to identify relevant studies potentially missed in PubMed and Medline. The following search terms were used in both Medline and PubMed (Informed consent OR Consent, Informed OR patient understanding OR comprehension OR readability OR understanding OR literacy OR health literacy OR consent forms OR consent documents) AND (Plastic Surgery OR Esthetic Surgery OR Esthetic Surgeries OR Surgeries, Esthetic OR Surgery, Esthetic OR Surgery, Cosmetic OR Cosmetic Surgery OR Aesthetic Surgery). The results on both databases were then filtered to show articles between 2012 and 2022. This set of articles were also uploaded into Covidence but reviewed by a single author (JM). Furthermore, a hand search was conducted across university library systems and databases such as Google Scholar for any additional studies which may also be relevant. A further search was conducted in May 2023 to seek out any relevant studies which may have been overlooked.
Participants
The target participant population were those who sought or were seeking cosmetic surgery procedures which were surgical or invasive (eg, breast augmentation), opposed to minimally invasive or non-surgical (eg, cosmetic injectables). The data collected from the participants, or the research conducted must have related to the decision-making process or overall decision of the patient to have their procedure.
Inclusion criteria
Studies must have centered around the informed consent process for invasive cosmetic surgery procedures. The articles were screened to ascertain if they centered on the patient’s decision-making process. The focus was primarily on surgical cosmetic procedures such as rhinoplasty, liposuction and breast augmentation. Filters were applied in PubMed and Medline to only include studies within the last 10 years (2012-2022). Additional filters were applied to focus on those articles which considered the experiences of participants aged between 19 and 64 years. This age range was selected as most individuals undertaking certain cosmetic procedures appear to be majorly dispersed within this age bracket (ISAPS, 2021). 8 The studies were further filtered to only include articles in English.
Exclusion criteria
Reviews (including literature reviews) and clinical trials were excluded; however, the reference lists of these reviews were screened to determine if any met the inclusion criteria for this review. Articles including non-invasive cosmetic procedures which did not involve cutting beneath the skin, such as botox, cosmetic dentistry, or dermatology were excluded. Studies involving patients having reconstructive, burns, or hand surgery were also excluded.
Study Selection
Results from the searches were exported into Covidence (https://www.covidence.org), which is software to assist in managing the systematic review process. Two reviewers individually screened titles and abstracts for eligibility and retained any articles which centered on the decision-making process or final decision to consent to invasive cosmetic surgery procedures. The full text of the articles was then screened by an additional 2 reviewers (JM and LM) for the inclusion and exclusion criteria. The 2 reviewers (JM and LM) then met to resolve any conflicts through a discussion of the article in question, and how it applied to the inclusion and exclusion criteria. All conflicts were resolved through this process.
Quality Assessment
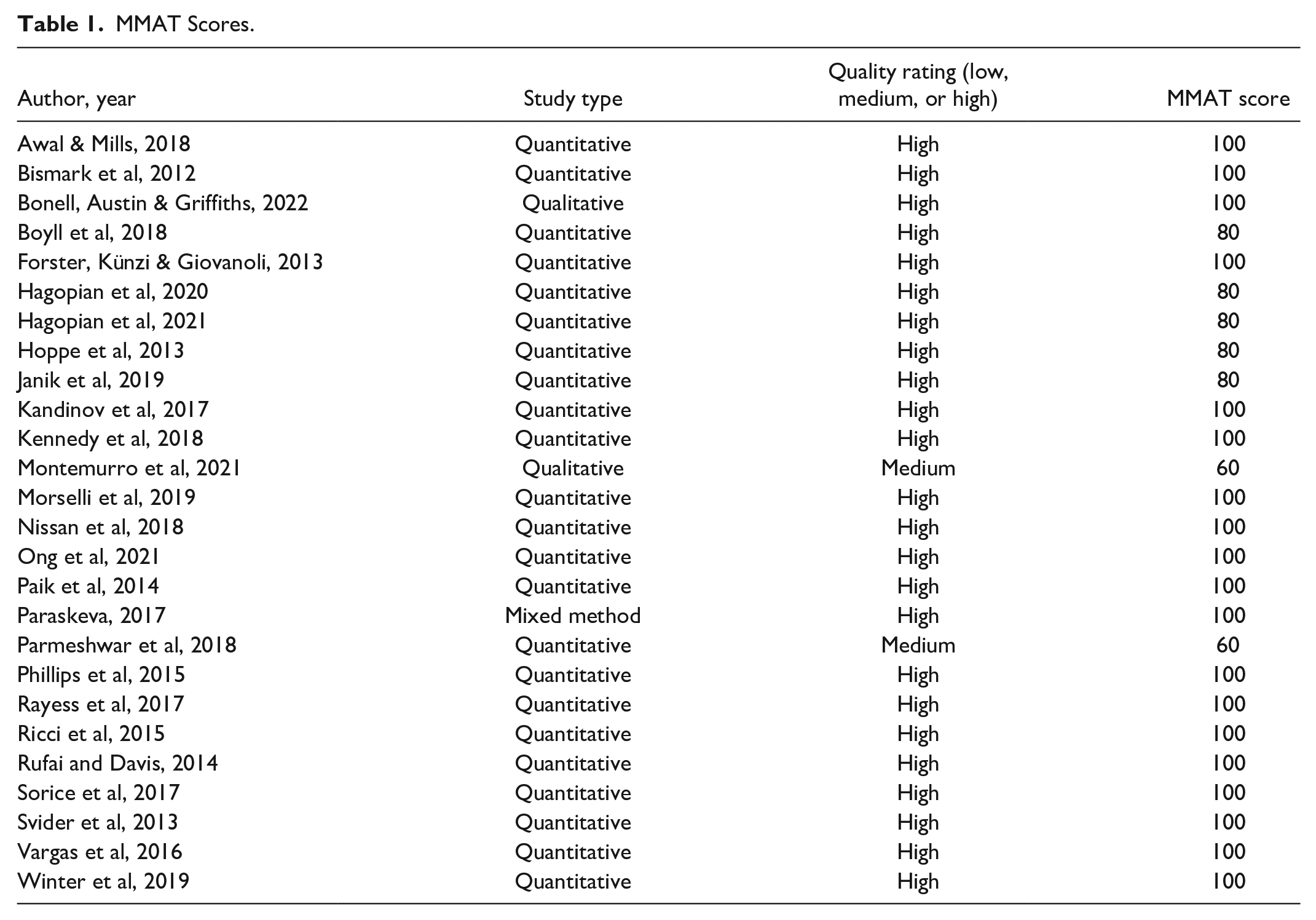
Eligible studies were appraised for quality using the Mixed Methods Appraisal Tool (MMAT). Two authors (JM and SZH) co-rated all studies to ensure consistency. A single author (JM) appraised all studies. The co-rated/assessed articles had 100% consensus between both authors without the need for conflict resolution. No studies were excluded based on the quality assessment. All studies included in the quality assessment had a score of 60% or higher (medium to high quality) (see Table 1).
MMAT Scores.
Data Extraction and Synthesis
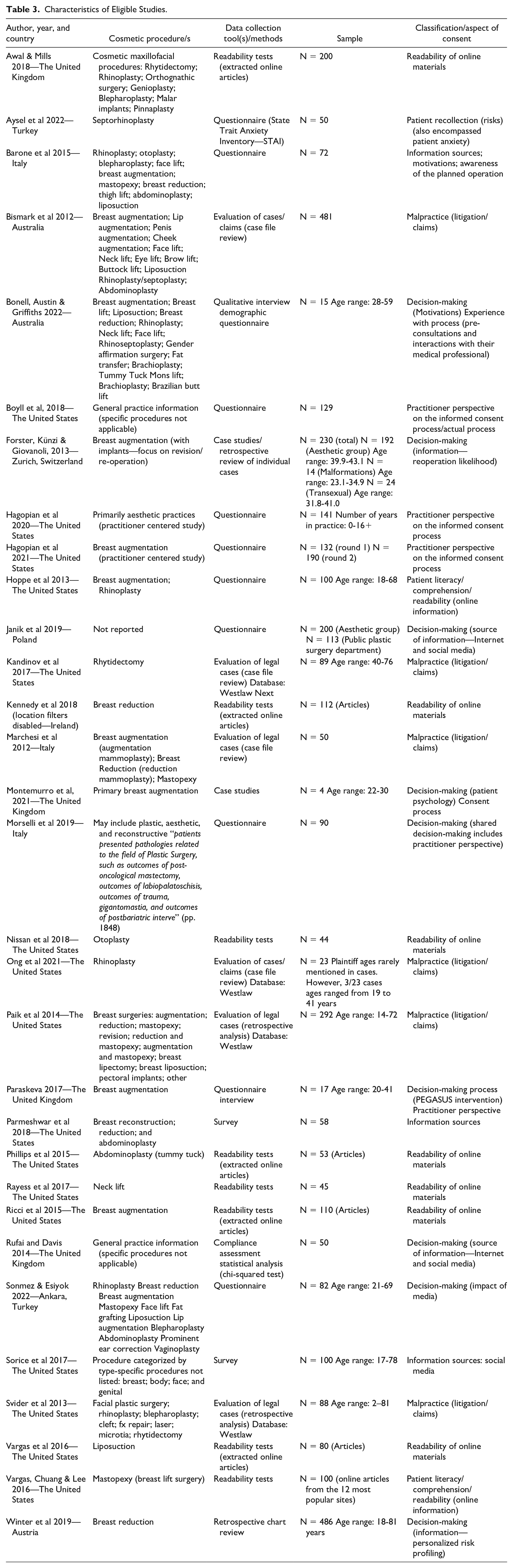
A data extraction spreadsheet was designed identifying key characteristics associated with each study including the author, study objective, methods, and sample (see Table 3). The studies were then grouped by similarity, primarily based on how they fit into the research questions which are the subject of this review.
The progression of the review is shown in Figure 1. Database searches on PubMed and Medline rendered 1672 results. Reference lists of some studies were reviewed for further eligible studies; however, most were not eligible as they were not published between 2012 and 2022. A total of 20 additional studies were identified through a hand search on university databases and Google Scholar.
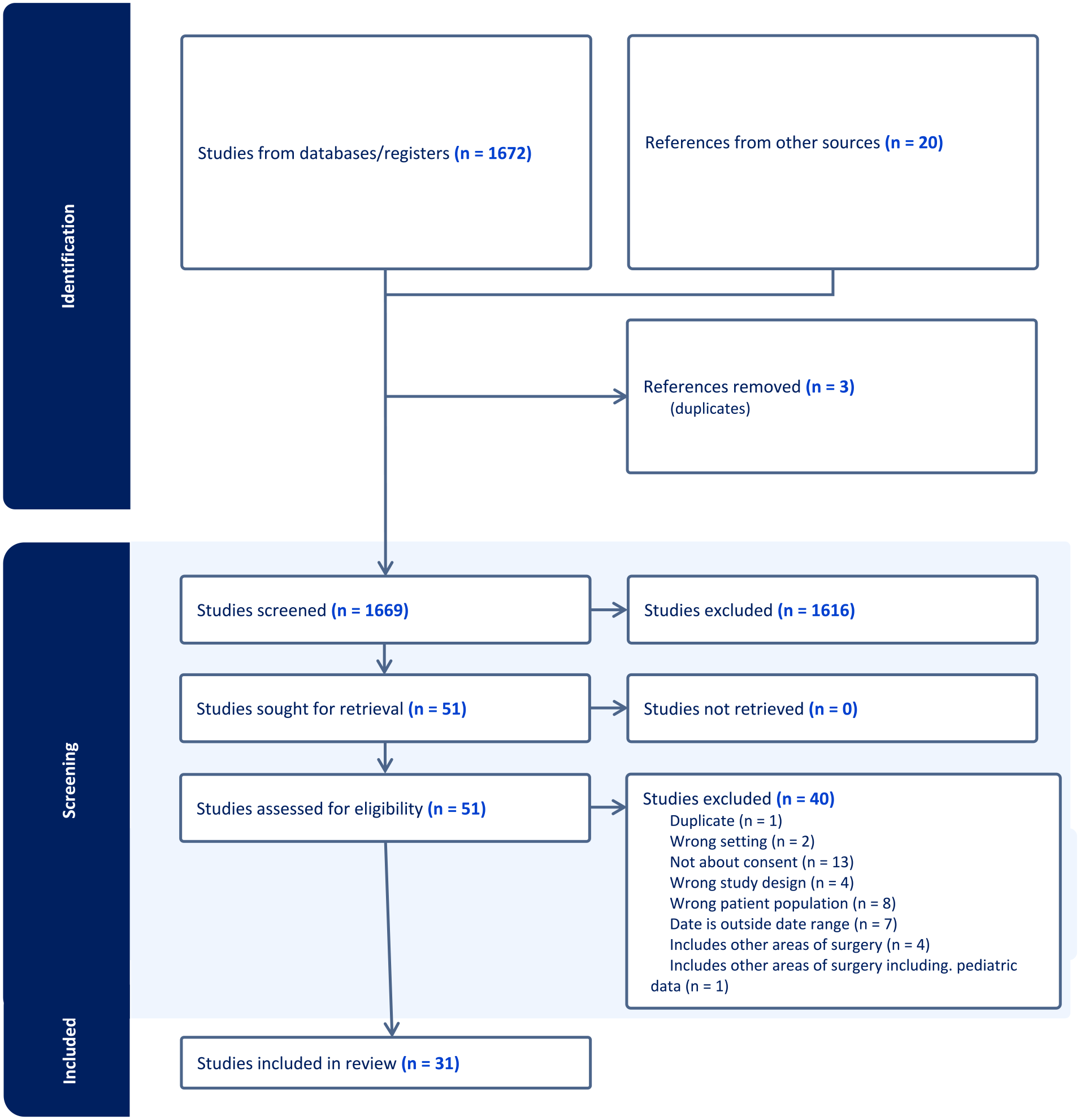
PRISMA table extracted from Covidence. Shows the number of articles identified, screened, assessed for eligibility, and included in this review.
Results
Results from Search Strategies—Preferred Reporting Items for Systematic reviews and Meta-Analyses Table
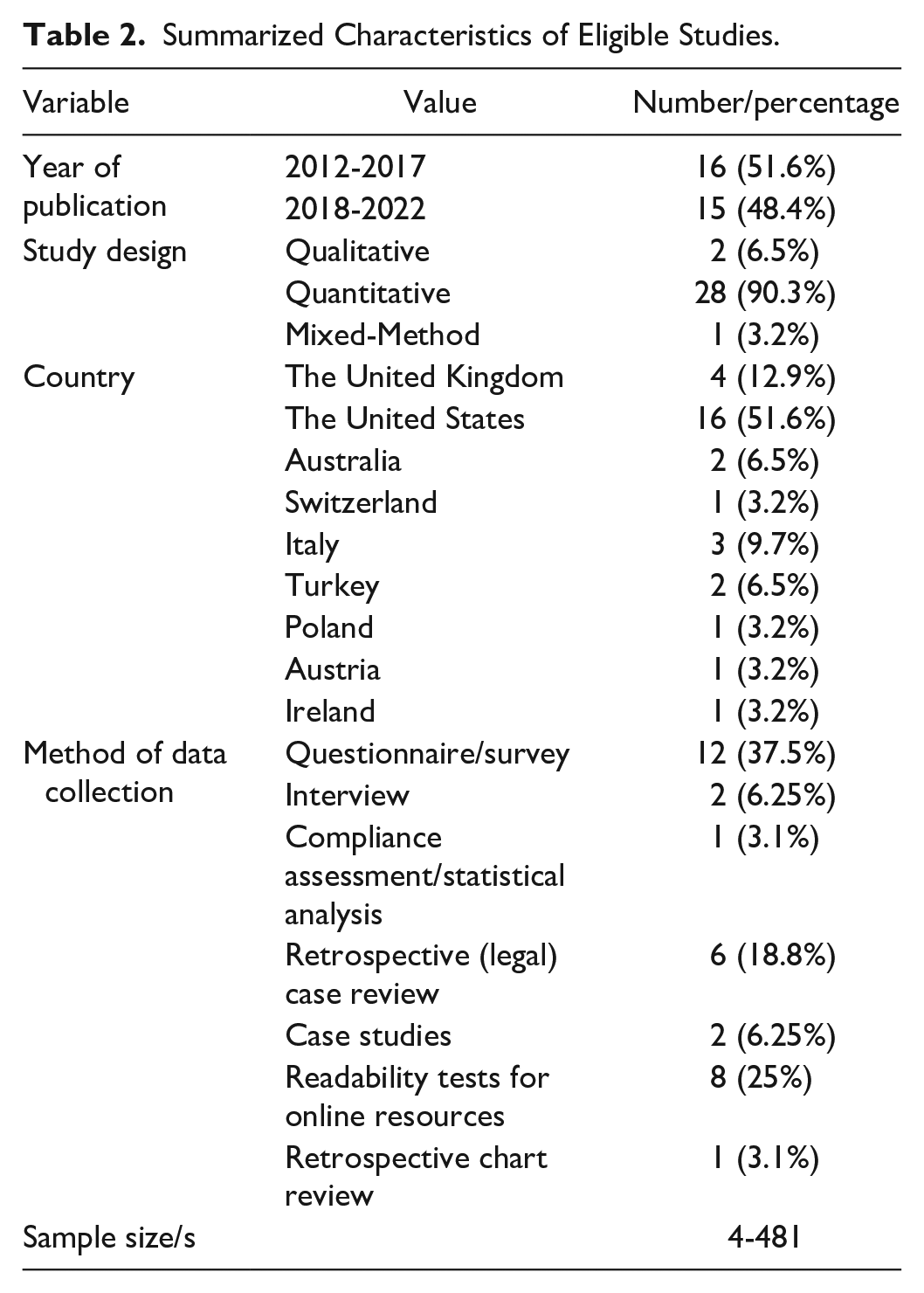
An additional 20 studies were identified as eligible for this study and screened for quality as part of the MMAT appraisal. The characteristics of all included studies are presented in Table 2. Most of the studies included in this review are quantitative. Just over half of the studies included (51.6%) were conducted in the United States, followed by the United Kingdom (12.9%). The dominant methodology employed throughout these studies were questionnaires (37.5%). Table 3 provides a further breakdown of the characteristics of each study.
Summarized Characteristics of Eligible Studies.
Characteristics of Eligible Studies.
Results of the Findings
What information should be communicated to the patient during the consent process?
The Guidelines by the Medical Board of Australia indicate that the practitioner should communicate patient specific risks to their patient. 4 Winter et al 9 retrospectively reviewed the charts of 804 patients within the 18-81 years age range, who underwent a bilateral reduction mammoplasty between 2005 and 2015. Although this age range is outside the core criteria, the premise and themes within this article are somewhat unique and highly relevant, warranting consideration. The data gathered were divided into 3 groups including patient specific data; treatment specific data; and complication specific data. The risk factors associated with the personalized patient chart for the most recurring complications which influenced pre-surgical consent were operative technique, smoking, resection weight for wound healing issues, body mass index (BMI) and allergies for wound infections; patients’ age; and resection weight for fat tissue necrosis. The graphical template produced from the most common complications based on individual risk factors will be useful when obtaining informed consent. However, Winter et al 9 note that the effectiveness of this resource in influencing patient information retainment, number of filed lawsuits or identifying changes related to behavior, needs to be tested in future studies.
Forster et al 10 stated that breast augmentation with implants is a common cosmetic procedure. However, the authors identified that the risk of complications prompting revision surgery, resulting in inadequate outcomes is not sufficiently emphasized. Forster et al 10 evaluated the instances of implant removal or replacement and the resulting complications and follow-up interventions after primary breast augmentation surgery. This was a 10-year retrospective study of patients who attended the Department of Plastic Surgery and Hand Surgery at the University Hospital in Zurich, Switzerland. The cases identified were grouped into aesthetic, transsexual, and malformation based on their main reason for the procedure. Although patients undergoing surgery for malformations were excluded, the dominant group identified was primarily for aesthetic reasons. A total of 230 patients were included in this study. The authors identified that it is common to have revision surgery after breast augmentation; there is a high risk of further revision procedures after the first. 10 The authors conclude that patients should be selected carefully and provided with comprehensive information to reduce complication rates and produce greater patient satisfaction. Forster et al 10 also conclude that the high risk of revision surgery and associated consequences should be stated in the written consent for breast augmentation surgery in a routine manner.
Expertise is a significant factor in determining what constitutes adequate information for patient decision-making and informed consent (Hagopian et al 11 ). Regulations and laws outline broad categories of information for informed consent. Hagopian et al state that it is the duty of the relevant medical practitioner to define the specific information they provide to their patients before performing their procedure. The scope of the study conducted by Hagopian et al was limited to informed consent for primary breast augmentation with breast implants. The authors sought to establish an expert consensus on what procedure-specific information is essential. 11 The authors sent a survey via the Survey Monkey platform to select individuals part of The Aesthetic Society. Their target participants were board-certified plastic surgeons who identify as having an aesthetics-focused practice. Their primary demographic was based in the United States. Consensus by participants was achieved for 16 risk items, 1 risk factor, and 8 expectations. This included benefits and burdens. The authors acknowledge that the results may not account for varied international surgical approaches to primary breast augmentation. The information presented is specific to a certain procedure, opposed to all procedures. 11
Patient selection
Dilger and Sykes suggested that patient satisfaction is the primary measure of success in cosmetic facial plastic surgery. Successful outcomes in aesthetic surgery depend on a number of factors including patient selection. 12 Montemurro et al stated that psychology and aesthetic surgery have a complex relationship. The authors considered 4 case studies of women who requested immediate removal of their breast implants following their surgery. The authors stress the importance of patient selection. Pre-operatively, these 4 patients did not raise any concerns about their mental state. Although immediately following their surgery, they had a negative psychological reaction to the augmented shape. These patients demanded the immediate removal of their implants because they found it difficult to cope with their changed body image. 13 These findings are consistent with Milothridis who identified that it may be difficult to identify patients with underlying psychological issues. 14
Bonell, Austen, and Griffiths explain that the experiences of women having cosmetic surgery are to their knowledge, missing from existing discourse. Understanding these experiences is important especially when it comes to certain points in their pre-operative surgical process including the initial surgical consultation. 5 It is important to explore how women experience cosmetic surgery to assist in determining the reasons for why some women report having greater positive psychosocial changes than others who have also undergone cosmetic surgery. 5 The authors of this study interviewed 15 Australian women on their motivations for undergoing cosmetic surgery and their experiences throughout the surgery process. The surgical procedures underwent by these 15 patients was varied. One of the more significant procedures among this sample was breast augmentation. The authors identified a series of themes and subthemes based on these interviews. A key theme identified was the normalization of cosmetic surgery among locations and social groups. Some participants spoke of how their surgery influenced others in their social circle to undergo cosmetic surgery. This raises questions on consent and whether patients overlook key information related to the risks and expectations of the surgery based on this normalization in society and their social circle. 5
Bonell et al 5 identified further that some women spoke of having positive experiences with their surgeon. However, the majority reported mixed or negative experiences. Numerous patients mentioned that their appointments prior to their operation were rushed, and surgeons did not give them enough time to voice concerns or ask questions. Various patients expressed concerns about the minimal or lacking communication by their surgeon regarding their aftercare. Several patients also concerningly explained that their surgeon did not sufficiently outline the complications which could arise from their surgery. Another key theme the authors identified throughout the interviews was the feelings of extreme depression or regret in the days after having undergone their cosmetic surgery. 5 The shift in the psychological state of these patients is somewhat on par with the case studies described by Montemurro et al as they also exhibited negative emotions following their surgery. 13
It is not uncommon for patients to experience strong emotions during pre-operative, operative, and post-operative phases of their cosmetic surgery. Aysel et al 15 aimed to evaluate the anxiety levels of patients who were undergoing rhinoplasty surgery at different times throughout their journey; compare information methods and establish recall rates of the complications explained to them during the informed consent process. Aysel et al explain that pre-operative interviews and good communication with the patient by the operating surgeon reduces patient anxiety. The patient should have adequate time to discuss and understand their procedure. 15 This is consistent with the patients who expressed negative experiences with their surgeon in the study conducted by Bonell et al, 5 especially regarding the patients who expressed that they felt rushed and therefore unable to raise all their concerns during their pre-operative consultations. 5 Aysel et al conclude that the verbal information and consent form process should be carried out over a longer period, as this increases the patient’s cooperation in treatment and decreases their anxiety levels. The authors conclude that this may result in a reduction of potential legal actions (Aysel et al 15 ).
What are the extent of claims based on a lack of “informed consent” against cosmetic and plastic surgeons?
Medical malpractice claims
Numerous articles within this review have explored claims against plastic and aesthetic surgeons. Kandinov et al 16 assessed the financial implications of medical malpractice litigation in the United States associated with rhytidectomy procedures and the factors contributing to litigation. Patients were aged between 40 and 76 years across a total of 89 cases. The most common allegations for the plaintiff’s claims were intraoperative negligence (69%); poor cosmesis or disfigurement (64%); inadequate informed consent (34%). Claims based on informed consent were significant in the scope of this study, although not the most significant. The authors note that the number of claims based on inadequate informed consent should stress to surgeons the significance of explaining possible complications with their patients. 16 The authors continue that adequate informed consent requires disclosure of information to a patient which is significant to their decision to undergo the procedure. Most informed consent disputes were due to undisclosed risks. This stresses the importance of preoperative discussions to manage the patient’s expectations and communicate the risks and limitations associated with the procedure. 16
Paik et al, 17 like Kandinov et al, 16 found that inadequate informed consent was a significant factor or basis for claims, however not the most significant. This was also an American study which examined litigation in cosmetic breast surgery and identified the factors which influenced the malpractice litigation decisions. 17 Of total, 292 matched the search criteria. The age range was 14 to 72 years. California in the United States had the greatest number of cases. 17 The most common procedures these claims centered on were breast augmentation and reduction. The most common cause of action was negligence, followed by a lack of informed consent. A lack of informed consent was mentioned in 128 cases, amounting to 43.8%. 17 Paik et al 17 explain that cases reporting inadequacies in informed consent were generally found in instances that although they signed the consent form, the discussion of the risks of the procedure were not discussed in sufficient depth.
A further American study by Svider et al 18 explores malpractice litigation for facial plastic surgery procedures. This study considered reconstructive and other non-aesthetic procedures; however, it remains important to consider how a lack of informed consent fit into these claims. Svider et al 18 also separate some of their data on cosmetic procedures such as blepharoplasty and rhinoplasty, as they were 2 of the most litigated procedures. The age range was 2 to 81 years across all procedures in 88 claims. Svider et al note that most cases involving blepharoplasties and rhinoplasties were resolved in the defendant’s favor. The authors identify further that a lack of informed consent was a contributing factor for litigious claims in a significant number of cases assessed (38.6%). This study found that “informed consent” was the most mentioned factor in these 88 cases. 18
Like the preceding studies, Ong et al 19 explore the motivating factors in medical malpractice litigation following rhinoplasty in the United States. Of total, 23 cases met the authors’ inclusion criteria. The plaintiffs in these matters were primarily female. New York had the highest number of cases. 19 The patients’ ages were hardly mentioned within the identified cases. The age range for the few cases which mentioned the patient’s age was 19 to 41 years. All cases brought claims based on negligence, and 5 cases amounting to 21.7% additionally alleged that there were issues with the informed consent process. Ong et al asserted that although the percentage of cases identified based on a lack of informed consent was less than that stated in Svider et al 18 and Kandinov et al, 16 pre-operative discussions and emphasis on informed consent remain highly significant. 19
All articles identified thus far have centered on data from the United States (Kandinov et al 16 ; Paik et al 17 ; Svider et al 18 ; and Ong et al 19 ). Bismark et al 20 reviewed 481 malpractice claims and serious health care complaints finalized in Australia from 2002 to 2008, which alleged inadequacies with the informed consent process for cosmetic and other procedures. 77 of the 481 (16%) informed consent claims involved cosmetic procedures. Most patients in these cases were female. 20
Marchesi et al 21 evaluated different errors attributed to plastic surgeons through a case analysis. This was an Italian study which focused on mammoplasties. The 50 cases identified were composed of 34 instances of mammoplasty augmentation; 11 cases of mammoplasty reduction; and 5 cases of mastopexy. Five cases of the 50 selected for analysis (10%), based their complaints on the informed consent provided. 21 The authors conclude that this figure on informed consent must be interpreted as an artifact, due to the nature of the study and the fact the analyzed cases were related to first instance trials. They affirm that most patients contest based on informed consent to obtain compensation because they believe no one may produce evidence of complete consent. 21
The studies thus far have assessed case law/claims involving aesthetic procedures. Boyll et al 22 aimed to better understand the elements of the informed consent process which may assist in minimizing malpractice claims in plastic surgery. The authors designed a questionnaire comprised of multiple-choice style questions and sent this to 1694 practitioners who were members of the American Society of Aesthetic Plastic Surgery (ASAPS). The questionnaire intended to evaluate the attitudes and practices of informed consent on medical malpractice. 22 A total of 129 completed questionnaires were analyzed. Interestingly, although the number of female patients make up the majority of the patients bringing claims against their medical practitioner.16,17,19 -21 Boyll et al 22 identified that the majority of plastic surgeons who responded to their survey were male. 88 of the 129 respondents (68%) acknowledged they had been a defendant in medical malpractice at some point in time. 22 The respondents who indicated they had no experience with medical malpractice lawsuits provided procedure-based brochures to their patients (97.6%). Further guidance for medical practitioners and plastic surgeons practicing in aesthetic surgery on obtaining informed consent is required. 22 Although claims based on a “lack of informed consent” or “inadequate informed consent” are not the most dominant basis for seeking compensation or making a claim, it remains to be a significant issue in the literature discussed.
What are the sources of information cosmetic surgery patients access to become “informed”?
Information sources for decision-making
There were several studies which did not meet the study criteria most notably due to the age range requirement. However, these are important to consider in the context of this question and were therefore included in this review. Patients access information for aesthetic procedures through a variety of means and for a wide range of reasons. Patients may consider different sources of information pre-consultation and post-consultation. Nejadsarvari and Ebrahimi 23 highlight that there is a divide in the information available to plastic surgeons and patients. The authors acknowledge that the stage of providing information to the patient is highly important. Advertisements for aesthetic procedures and the circulation of insufficient or incorrect information may impact the patient’s decision-making autonomy. 23
Barone et al 24 assessed how informed and aware patients of cosmetic surgery are using a questionnaire to be completed by patients prior to their surgery. The sample size was comprised of 72 patients with the primary distribution being women (60/72). This study required participants to be older than 18 years of age, of Italian nationality, and have requested cosmetic surgery. 24 The most significant procedures undergone by these patients were surgeries in the face and neck areas. The authors found that almost all patients under the age of 40 years had sought additional information in the pre-operative period. 24 This was significantly higher than those in the over 40 age brackets. The Internet was the most common source of information in patients under 40 years old (93.3%). 30% of participants with a lower educational background perceived the information provided during the pre-surgical consultation to be adequate. Questionnaires seeking to understand patient engagement with alternate sources of information pre-surgery and post-surgery are important in understanding what has influenced the patient’s decision to have the surgery. 24 Barone et al 24 note that the reliability of online information may significantly influence the patient’s expectations and lead to disputes with their medical practitioner.
Parmeshwar et al 25 acknowledge that patients have access to a wide variety of information prior to meeting with their cosmetic surgeon. The authors acknowledge that despite the use of this information, they remain undefined in the patient’s decision-making process. This study partly considered the experiences of patients undergoing breast reconstruction. The total sample size was composed of 58 patients. The most significant procedure within this group was breast reconstruction (60.3%). However, it was one of the only studies located which provided detailed insight into the kinds of information sources patients access and their uses for this information within the context of invasive aesthetic surgery. 25 It is therefore important to include in this review. Consistent with Barone et al, 24 a significant number of patients sought information through the Internet/online. 25 Parmeshwar et al 25 found that the most useful sources of information following the patient’s initial consultation were primarily plastic surgeons, followed by the Internet.
Janik et al 26 explain that social media is rising in popularity. The use of social media has increased among potential patients. Most of these patients use the Internet to do research before consulting with their surgeon or practitioner. The authors conducted a study across the Public Plastic Surgery Department and Private Aesthetic Plastic Surgery Clinic. 26 This study included both aesthetic and nonaesthetic patients. Participants were asked about which social media platforms they use including Facebook, Twitter, LinkedIn, YouTube, or other. Patients were also asked to identify the source of information which was the most or least helpful for them. 26 A total of 313 questionnaires were collected (200 in the aesthetic group). Facebook was found to be the most popular social media platform for both the aesthetic and public groups. Twitter was identified as the least popular platform. Aesthetic patients were found to use Instagram more than patients in the public group. 26 Similarly, Sorice et al surveyed social media use by patients of a single aesthetic practice run by 2 plastic surgeons. The sample size was 100 patients; however, the findings are consistent with Facebook being the most popular platform and Twitter the least popular. 27
Sonmez and Esiyok 28 explored the significance of media (including social media) on the decision to have a cosmetic surgery procedure. This study was refined to female patients who decided to have cosmetic surgery (without any health problems). It was requested that participants complete the survey 1 day after their surgery. Data were collected from 82 patients through face-to-face interviews. 28 Patients were aged between 21 and 69 years; however, only 1 patient fell into the 60 to 69 years age bracket. Data were collected from different clinics in Ankara, Turkey. The main reason for wanting to undergo surgery was dissatisfaction with appearance. The study found that the Internet was a prominent source in influencing patient decision-making; notably through the celebrities the patients followed on social media. 28 Cosmetic surgery news on social media was also found to be influential. Television was second to the Internet. 24% of participants stated that TV was a key source for them when deciding to undergo their procedure. Additional sources which assisted with the patients’ decision-making process are celebrities on television and television programs centered on cosmetic surgery. The third most significant source was magazines. 28
Rufai and Davis 29 explain that the Department of Health within the United Kingdom and Professor Sir Bruce Keogh published a review in 2013 of guidelines to help regulate cosmetic interventions. Rufai and Davis’s study assessed the level of compliance with these national guidelines by aesthetic surgery providers in the United Kingdom. The authors used the Google search engine to mimic a patient searching for information on cosmetic surgery. The search terms “cosmetic surgery UK” were input into the UK version of Google to examine cosmetic surgery providers in this location. The top 50 websites of cosmetic surgery providers that appeared in this Google search were assessed in this study. The recommendations were identified in 2 national guidelines published by the Department of Health and the Cosmetic Surgical Practice Working Party. The recommendations were grouped into one of the 3 sections including consultations, promotions, and consent. Information was obtained from the websites of these 50 providers, and where the information required was unavailable online, the researchers called the company and mirrored their process of reviewing the websites to obtain the unidentifiable information. 29 Ultimately, this study found that there was low compliance by cosmetic surgery providers with the national guidelines used in this study. The authors explain that aggressive forms of selling are significant. These may take the form of time-sensitive deals and incentives to tempt vulnerable patients. 29
Genuine informed consent is achieved through the effective communication of medical information by a provider and the ability of patients to process this information to guide their decision-making. 25 If appropriately achieved, it has strong links with patient satisfaction. Thus, to determine how informed patients are when they provide consent for aesthetic procedures, it is important to understand their experience with different sources of information and their purpose for seeking out these sources. Minimal empirical literature has assessed experiences throughout the surgery process including at the consultation, aftercare, and recovery stages (Bonell et al 5 ). Very little Australian data (both qualitative and quantitative) were located depicting the experiences of cosmetic surgery patients undergoing invasive surgeries. A significant gap in current discourse centers on where Australian aesthetic patients (invasive) are sourcing their information from and for what purpose.
Are patients able to comprehend the information available to them on aesthetic procedures?
Patient comprehension/understanding/readability
The Internet is a primary source of information for patients seeking cosmetic surgery.24,25 Barone et al note that the reliability of online information may significantly influence the patient’s expectations and lead to disputes with their medical professional. 24 Therefore, the ability of patients to comprehend this information is an important consideration.
Hoppe et al 30 state that surgeons have an obligation to ensure that their patients are aware of the risks, benefits, and potential complications associated with their procedure/s. Traditionally, when this information was provided by the patient’s surgeon or associations and societies, the validity and thoroughness of the information patients had access to were controlled and disseminated by medical professionals and their community. The authors explain further that the validity and comprehensiveness of information found online are questionable. However, patients may believe the online information they locate to be reliable and true. 30
Hoppe et al evaluated resources on breast augmentation and rhinoplasty. The American Society of Plastic Surgeons (ASPS) and the ASAPS websites were used to research these 2 procedures. 30 The information was then provided to participants within this study. Questionnaires were distributed to patient’s assessing their understanding of this information. The authors located 4 passages and developed 2 questionnaires based on the 2 websites and procedures. A total of 100 patients from a plastic surgery clinic at the University Hospital in Newark took part in this study. The patient age range was between 18 and 68 years. 30 Although this age range fell outside the inclusion criteria for this review, the key theme of understanding made it important to include and the age range was not too far from the 19 to 64 criteria. Participants were placed into 1 of 4 groups; each group had a total of 25 patients. The participants were asked to read their assigned passage. The passage was removed, and then the patients were asked to complete the questionnaire. One point was awarded for each correct response to the first 5 questions. There were no significant differences on patients’ understanding and knowledge of the considerations associated with their surgery between the websites. 30 The authors conclude that patients are capable of understanding information shared on the Internet by professional societies about their procedures (breast augmentation or rhinoplasty). Two key limitations of this study were that most participants completed a high school level education, and the focus was on the websites of professional societies. 30
Vargas et al 31 explore the most popular mastopexy resources in relation to their overall readability. A Google search for “breast lift surgery” led to the identification of the 12 most popular websites on this surgery. Ten different readability tests were performed, with each one evaluating different aspects of text difficulty. The online resources for mastopexy information evaluated produced an average which corresponded to a university freshman level. 31 All articles extracted went beyond the American Medical Association (AMA) and National Institutes of Health’s (NIH) recommended sixth-grade level. The authors note that discussion about information from these websites with patients who have different literacy skills requires plastic surgeons to be aware of their level of difficulty. 31
Vargas et al 31 conclude that the patient’s physician should acknowledge that some information online could be harder to read than others; this could create issues during the patient’s consultation and obtainment of informed consent. Patients may seem well informed about a procedure when presenting for an elective procedure; however, the online resources they access to read about their procedure may not lead to an equally distributed understanding of information related to their surgery such as the risks and benefits of the procedure. The authors acknowledge that there are limitations to this study. Their analysis focused on the readability of this online information; however, this does not replace comprehensibility. 31
Kennedy et al 32 evaluated the readability of, and quality of websites centered on breast reduction. Location filters were disabled and the terms “breast reduction” were input into the Google search engine. The search yielded 112 articles from the first 10 search results for assessment. Private or commercial cosmetic surgery websites were excluded. The authors used 10 established readability tests for their evaluation. The authors found that all websites included in their analysis were of a reading grade (16- to 17-year-old reading level) level too high for all patients to understand. 32 Similarly, Vargas et al conducted an Internet search using the term, “liposuction” through Google. The 10 most accessed websites were identified. A total of 80 articles were gathered from these websites. These articles were assessed using 10 established readability tests. The readability analysis showed that all articles were beyond the target sixth-grade reading level. The authors concluded that liposuction websites may be too difficult to read, and aesthetic surgeons should discuss with patients the kinds of resources they use. 33 Phillips et al 34 also found that online resources about abdominoplasty (tummy tuck) were above the recommended readability level, and patients are likely to find these resources too difficult to understand. In common with the studies examined thus far, Ricci et al 35 found that the 110 articles extracted from the 12 most popular sites for “breast implant surgery” were above the recommended reading level and were therefore determined to be difficult to read. The authors used 10 established readability tests to evaluate these articles.
Awal and Mills 36 aimed to discern the readability and quality of resources on facial cosmetic procedures including, rhytidectomy; rhinoplasty; orthognathic surgery; genioplasty; malar implants; blepharoplasty; and otoplasty. The authors used Google to search for each procedure and their related terms from London, UK. The searches were conducted without filters. The top 50 results were assessed for each procedure. Quality was determined using the Health On the Net code (HONcode); DISCERN questionnaire; and the Journal of the American Medical Association (JAMA) benchmarks. 36 Readability was assessed using 4 readability tests. The quality of the websites assessed was poor. This was indicated by low mean JAMA and DISCERN scores. The authors noted that quality could be compromised when sites are dominated by sales objectives. The average readability scores mean a higher standard of educational attainment is required. 36
Awal and Mills 36 explained that this is concerning given the low level of health literacy in the United Kingdom. This may limit access to a significant population seeking cosmetic surgery information and lead these patients to become less realistic about the possible outcomes of their surgery. This is also consistent with Rayess et al 37 who assessed the quality, readability and technical aspects of online websites related to neck lifts. The average readability scores were found to be higher than the recommended reading levels by the NIH. 37 Nissan et al 38 found that this also applied to the first 44 relevant websites obtained from a Google search of “otoplasty,” performed in Chicago, Illinois.
The discourse examined indicates that the readability of online information available to patients varies depending on specific cosmetic procedures. Popular or top websites and their associated articles for various cosmetic procedures require a higher reading level and may therefore be too difficult for a significant proportion of populations where the recommended reading level is much lower.
What are the most effective methods of taking consent for cosmetic surgery procedures?
Morselli et al 39 explain that issues may arise when there are difficulties related to communication between the practitioner and different types of patients they need to adapt to. These issues may interfere with the patient’s complete understanding despite their signed consent. Morselli et al recruited 90 patients upon their initial visit to a plastic surgery clinic in Bologna, Italy. The patients included in this study had undergone procedures related to oncological mastectomy; results from trauma; cleft lip; and other medically fuelled surgeries opposed to those characterized as solely cosmetic. 39 These procedures are outside the scope of this review. However, this study was evaluated because the findings are consistent within other scholarly discourse exploring the approach to taking consent. The most effective practice for informed consent in cosmetic surgery is through a process of shared decision-making.39 -42
Morselli et al 39 randomly assigned the 90 patients included in their study to 1 of 3 groups. Each group was comprised of a different method of approaching the patient for informed consent. The first group underwent a standard request for informed consent involving a standard clinical interview. The second group of patients were asked to provide informed consent and supported with a clinical interview based on the principles of shared decision-making, to reach a shared decision. 39 The final group was asked to complete a questionnaire aimed at assessing the patient’s expectations. This was followed by administering informed consent, and as per group 2, these initiatives were combined with a clinical interview based on the principles of shared decision-making. 39 This method was effective for doctors looking into patient expectations, emotions, and preferences. Patients also scored this method much higher than the first method for overall satisfaction. It was also rated higher than the first and second methods in assessing expectations. 39
Similarly, Paraskeva et al note the significance of shared decision-making for aesthetic surgery. The authors state that interventions encouraging patients to identify goals on what they hope surgery will result in, and actively engage in the consultation can improve their satisfaction with the process. 43 Medical professionals tend to support shared decision-making; however, minimal aspects of this approach occur during consultations and patients are not always included to the extent they would like. Paraskeva et al explored the “PEGASUS Intervention” to help facilitate shared decision-making. This mixed-methods study explored the acceptability of the PEGASUS intervention for breast augmentation patients and providers. 43
PEGASUS stands for Patient’s Expectations and Goals: Assisting Shared Understanding of Surgery. 43 This intervention involves the patient listing their goals on an intervention specific sheet and then rating the importance of each on a scale from 0 to 10. The completed sheet is then used as a “tool” during their consultation to encourage discussion around each of their goals. The surgeon then provides a rating on a scale from 0 to 10 on the likelihood of achieving each surgical goal the patient has. Practitioners may use this information to help determine whether the patient has realistic expectations associated with their surgery, and what extent they need to manage them. 43 Providers of aesthetic surgery were recruited through the British Association of Aesthetic Plastic Surgeons in 2014 and 2015. Seventeen women were identified at the participating practices. The age range of the participants involved was 20 to 41 years. The intervention allowed each participant to identify a list of surgical and psychosocial goals for their breast augmentation procedure. The cumulative number of goals was 77, and the ratings on the importance of each of these goals ranged from 5 to 10. Most participants found the PEGASUS intervention to be relevant, helpful, and useful. However, there were some barriers identified by aesthetic providers to the consistent application of PEGASUS in routine practice. 43
Hagopian et al, 42 like Paraskeva et al, 43 acknowledge that informed consent for aesthetic surgery procedures is best obtained through a process of shared decision-making. However, it is not common practice. 42 The authors aimed to understand the basic attitudes, beliefs, and practices regarding informed consent by board-certified plastic surgeons who have a dominant aesthetic practice. An online survey comprised of 15 questions was distributed through email to the members of the ASAPS. 69% of respondents in this study indicated that they were very or extremely confident that informed consent documents contain information backed by evidence. 63% indicated that their confidence in the effectiveness of informed consent documents, in prompting patients to teach back important fundamental information, was minimal or non-existent. 42 The authors concluded that informed consent documents are centered on disclosure rather than patient understanding. 42
Discussion
Most of the studies explored thus far contain a dominant female population. This is representative of the fact that women tend to undergo cosmetic surgery more than men. 2 To the best of our knowledge, there are few studies exploring the patient experience pre-operatively in Australia. A particular stage in this process centers on informed consent. It is important to better understand how the consent process is experienced because it is a consistent basis across jurisdictions for litigious and malpractice claims.16 -21
Exploring this process is made up of numerous parts. It requires consideration of the types of information patients access prior to and during their consultations and the purpose this serves in their decision-making process; their overall perspective of their surgeon and knowledge of their qualifications; patient recollection and understanding of the risks, benefits, and complications of their surgery; and disclosure of the costs associated with their surgery. Further exploration into how patients and their practitioners experience the consent process for cosmetic surgery procedures is required. It is important to consider the experiences of both stakeholders as the most effective means of taking patient consent is through a process of shared decision-making.39 -42
Most studies discussed have used quantitative methods (90.3%) (refer to Tables 1 and 2) including retrospective reviews and questionnaires/surveys as their dominant methodology. Bonell et al 5 state that inventories and questionnaires containing Likert-scale questions may help in establishing common traits; however, they are limited in providing further insight. Owing to the minimal discourse centered on the “Australian experience,” it may be useful to employ both qualitative and quantitative methodologies to assess the decision-making process of the patient when providing informed consent and to better understand the process from a patient and practitioner point of view. Quantitative surveys inhibit nuance and a comprehensive understanding. 5
A key starting point for exploration of the informed consent process in Australia is the ‘Guidelines for registered medical practitioners who perform cosmetic surgery and procedures’ (2023) developed by the Medical Board of Australia. 4 These guidelines may be useful when developing research tools, particularly, as they relate to consent requirements. Furthermore, it is important to survey the types of information patients access; the purpose of these materials; and the weighting of these materials in their decision to undergo their cosmetic procedure. Patients have access to a wide variety of information prior to meeting their cosmetic surgeon through the Internet and social media. The impact of this information on the patient’s decision-making process is undefined. 25
Limitations
Studies eligible for inclusion in this review may have been overlooked, despite the search strategy implemented. This may be primarily due to the filters applied during the search process. Furthermore, the scope of articles intended to be included was limited further by these parameters which included articles published in the last 10 years (2012–2022) and within the age bracket 19–64 years. Most articles within this review did not meet the intended age bracket (19-64 years); however, the issues and themes they discussed were too pertinent to dismiss; or the findings were consistent with other studies which met the inclusion criteria and therefore warranted inclusion. This may have led to a degree of inconsistency. Not all studies included the age range of the participants or other socio-demographic information. The existing discourse is not extensive and was therefore found to be limiting.
Conclusion
Informed consent may be difficult to discern. “Informed” within “informed consent” requires consideration of the types and sources of information patients’ access, the reasons they access this information, and the weighting they place on it in their decision-making process. Patients are exposed to online information and social media to gather information on their prospective procedures before they meet with their medical practitioner. This may impact their expectations and understanding of their procedure. It is important for practitioners to discern whether their patients have any pre-conceptions of their surgery. Self-assessed patient understanding and satisfaction with their decision to undergo their surgery are important considerations. Dissatisfaction may lead to litigious or other claims based on a lack of informed consent. Based on the results of this literature review, further research on patients’ decision-making process and experiences before and during their cosmetic surgery procedure is required. It is of importance in the context of Australia, as Australian studies on this process for invasive cosmetic procedures are currently limited.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Ethical approval was not required as this study was a review of published studies.