
Abstract
Introduction
Facial nerve palsy may lead to significant functional facial and ocular morbidity. The loss of midfacial tone exacerbates paralytic ectropion, and thus isolated lateral canthoplasty is often insufficient for long-term rehabilitation of a paralyzed lower eyelid. In patients who are not seeking complex dynamic facial restoration, static soft tissue resuspension may improve both functional and aesthetic deficits in facial palsy. 1 Previously described suspension techniques are limited by alloplastic implants, with risk of infection and extrusion. 2 We have adapted a minimally invasive midface suspension,3,4 which can be easily combined with routine paretic periocular rehabilitation to optimize outcomes.
Materials and Methods
We performed a retrospective review of patients who underwent midcheek suture suspension for unilateral facial nerve palsy by American Society of Ophthalmic Plastic and Reconstructive Surgery (ASOPRS)-trained surgeons at 2 centers (1 private practice and 1 academic institution) from 2004 to 2019. Patient demographic and perioperative data were retrospectively reviewed to assess outcomes. Institutional Review Board approval was obtained and research was performed in accordance with the Declaration of Helsinki. The study performed in a HIPAA-compliant manner and written patient consent was obtained for inclusion of facial photographs.
This midface suspension procedure is most commonly performed concurrent to periorbital rehabilitation of paralytic lagophthalmos, which may include upper or lower eyelid recession, upper eyelid weighting, and/or lateral canthoplasty. Following instillation of local anesthetic to the periorbital region, tumescent anesthetic is infiltrated into the ipsilateral temple and cheek. Direct eyelid rehabilitation procedures are first performed, followed by the midface elevation procedure.
A subcutaneous temporal flap is initiated via a 1- to 2-cm temporal elliptical incision. The superficial temporalis fascia is exposed with tenotomy scissors, and the dissection toward the malar region is carried out directly over the deep temporalis fascia to the lateral orbital rim and zygoma, while remaining deep to the intermediate fat pad. In cases of complete facial palsy, the anterior two thirds of the zygoma may be exposed to maximize elevation, in a subperiosteal plane deep to the temporal branch of the facial nerve.
Depending on the goals of the surgery, the dissection can be performed via the temporal incision alone or, in more severe cases, a second incision via the superior buccal sulcus can aid in maximizing cheek soft tissue mobilization. In such cases, a 1-cm incision is made within the superior buccal mucosa, slightly above the mucogingival junction, using monopolar cautery. Care should be taken to avoid injury to Stensen’s duct. The periosteum of the maxilla is exposed and incised using monopolar cautery, and then a subperiosteal dissection is carried superiorly along the anterior face of the maxilla. The release should be extended from the piriform aperture medially, and through the incised masseteric ligament laterally until the primary temporal dissection plane is reached at the lateral orbital rim and anterior zygoma.
Three distinct stab incisions of 0.5 cm from the patient’s nasolabial fold or midcheek are made with a No.-11 blade (Figure 1A). A 0-0 permanent braided suture such as silk is threaded onto a Keith needle, and inserted into these entrance sites (Figure 1B.) Next, the cheek soft tissues are engaged, and the needle is externalized through a lateral canthal incision (Figures 1C and 1D). The needle is then redirected through the lateral canthal incision and guided along the preformed dissection plane to exit through the temporal incision (Figure 1E). The distal end of the suture is then swaged onto the Keith needle, inserted through the same entrance, passed through an adjacent cheek soft tissue tract, and similarly externalized through the temple. An identical procedure is performed along the 3 separate entrance sites. Next, the braided suture is purposefully cheesewired through the dermis via manual vacillating saw action under tension. Tension is adjusted to achieve adequate midface suspension with the goal of initial overcorrection (Figure 1F). Finally, each suture is secured to the deep temporalis fascia using a free needle. When indicated, the superficial musculo-aponeurotic system may be independently elevated and secured to the deep temporalis fascia using a 3-0 polydioxanone (PDS) suture to achieve additional temporal support. The temple incision is then closed in a layered fashion using deep 4-0 Monocryl sutures in deep interrupted bites, and superficial 5-0 fast-absorbing plain gut suture in a running fashion. The oral incision, when present, is closed with a 5-0 chromic suture in a running locking fashion. The patients are instructed to apply antibiotic ointment over area of incisions 4 times daily and oral antibiotic rinse twice daily for 1 week.
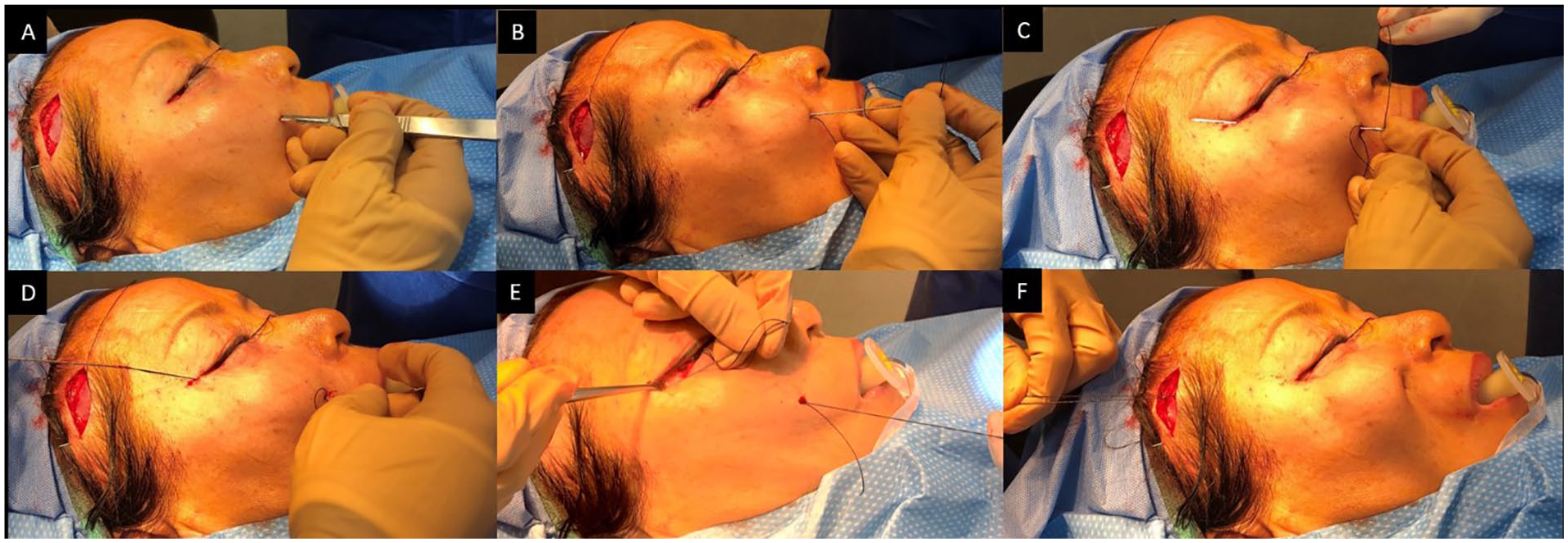
Intraoperative photographs demonstrating (A) a stab incision made along the patient’s midcheek, followed by (B) insertion of a 0-0 silk tie threaded onto a Keith needle. (C) The cheek soft tissues are engaged, and (D) needle is externalized through a lateral canthal incision. (E) The needle is then redirected through the lateral canthal incision and guided along the preformed dissection plane to exit through the temporal incision. (F) Tension is adjusted to achieve adequate midface suspension and suture secured to the deep temporalis fascia.
Results
Seven patients of median age 65 years (range 55-85 years) with unilateral facial nerve palsy and bothersome, symptomatic facial droop were identified. All patients underwent simultaneous eyelid reconstructive procedures, including upper eyelid gold weight implantation (n = 5, 71.4%), lateral canthoplasty (n = 3, 42.9%), ipsilateral brow lift (n = 2, 28.6%), and lower eyelid filler (n = 1, 14.3%). The midcheek release and suture suspension were concomitantly performed, customized based on individual patient needs.
All patients demonstrated lasting improvement in facial asymmetry (Figure 2) and reported satisfaction with their results at an average follow-up of 8.7 months (range 3-24 months). There were no significant postoperative complications, although 3 patients experienced transient cheek paresthesia, which spontaneously resolved over the course of the healing period.
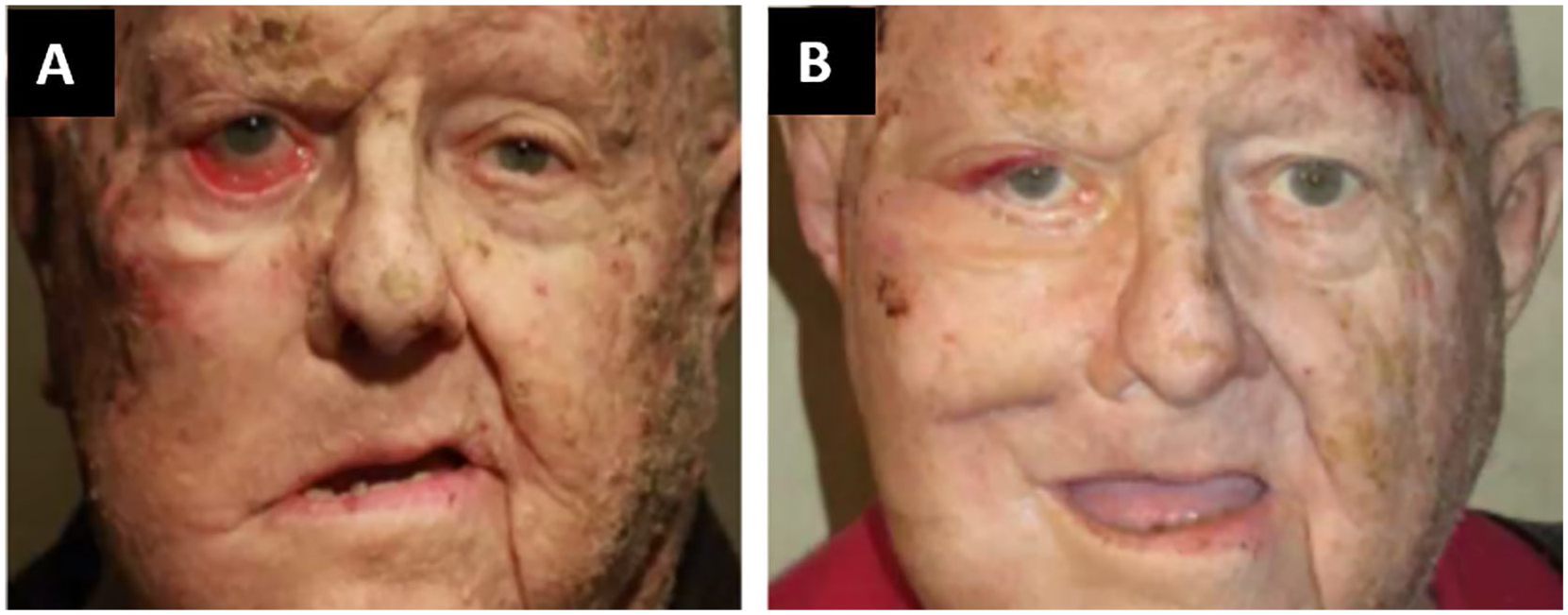
Representative patient’s (A) preoperative and (B) postoperative photographs.
Discussion
Facial nerve dysfunction may lead to significant functional disability and cosmetic disfigurement of the periocular region and midface. Inadequate periocular reconstruction can extend ocular surface morbidity risks in these patients. Dynamic facial restoration can sometimes be achieved with cross-facial nerve grafting, microneurovascular free flaps, and regional muscle transfers.2,5 However, these procedures are technically challenging, require longer anesthesia time, and carry increased risk of surgical morbidity including significant failure rates. 6 In addition, older patients and those requiring radiation therapy have been found to have less success in dynamic rehabilitation. 7 Thus, for patients who are elderly, have an oncologic comorbidity, or simply prefer a less-invasive surgical rehabilitation strategy, static soft tissue mobilization may be an ideal choice.
Various suspension materials have been used for facial soft tissue elevation, including suture, wire, autologous fascia lata, silastic rubber, Marlex mesh, and Gore-Tex.1,4,8-10 Although autogenous and alloplastic sling suspension has some reported success, disadvantages include an additional fascia lata harvesting site (for cases of autologous fascia use), risk of infection and extrusion, and limited durability.1,8 Suture suspension for cheek elevation in facial palsy has been a reconstructive tool for more than 50 years. 9 Alex and Nguyen 1 reported a multi-vectored suture suspension using polypropylene sutures, anchoring the midcheek tissues to the malar eminence using a Mitek screw. Disadvantages of suture suspension relate primarily to the cheesewiring of the suture in the postoperative healing phase, reducing efficacy. With subperiosteal release, durable midface elevation is more effectively achieved with suture suspension. Malar fat pad elevation to the level of the temple using polypropylene suture, without need for hardware, was additionally proposed for cosmetic age-related face rehabilitation. 3 We describe a modified minimally invasive technique to achieve midface suspension in cases of cranial nerve (CN) VII palsy using a complete subperiosteal release, suspended by semipermanent braided suture tie on a Keith needle, that can be easily performed at the time of periocular rehabilitation. We have found that braided silk suture resists cheesewiring compared with monofilament suture, acts as slow nidus of inflammation that anchors the lift long term, and maintains the benefits of the minimally invasive suture suspension approaches. When combined with periocular rehabilitation, this procedure improves the efficacy and durability of the eyelid reconstruction by robustly mobilizing midfacial tissues toward the lower eyelid.
Limitations of this study include the retrospective nature of review, limited patient cohort, and variation in specific surgical dissection adjusted for patient-specific anatomy and degree of paresis. However, we believe the wide applicability of this technique lies in its malleability in the treatment of a diverse spectrum of patients. In addition, this technique is principally one of static rehabilitation that does not perfectly reestablish a symmetric facial architecture, particularly apparent with facial animation. Invasive dynamic rehabilitation may be preferred by some patients.
Conclusions
We have found this midface soft tissue suture suspension was effective for improving long-term facial symmetry and function in 7 patients with facial paralysis of various etiologies. The suture suspension technique is an effective and safe maneuver that can be included in the oculoplastic surgeon’s toolbox at time of periocular tissue reconstruction for patients with facial nerve palsy.
Footnotes
Meeting Presentation
This project was shared as a poster at the ASOPRS 2019 Fall Symposium in San Francisco, California.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: T.N. is a shareholder of Global Beauty Science, Inc. N.H. is a consultant for Pulse Biosciences. No direct conflicts of interest are present with the content of this article. The remaining authors have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Human Investigation Committee (IRB) of University B approved this study.
Informed Consent
Patients signed informed consent regarding publishing their data and photographs.