
Abstract
The time of eating has been considered to have an important role in weight regulation. However, it is unknown if there are specific daily patterns of energy and macronutrient distribution that could be more beneficial for metabolic outcomes, especially obesity. This study aimed to assess the effect of time-of-day energy and macronutrient intake at 4 y of age on the weight status at 7 y of age. The study sample included 1961 children from the population-based birth cohort Generation XXI, with data on 3-day food diaries at 4 y and body mass index (BMI) z-scores at 7 y. Dietary patterns based on the collected data were obtained for the distribution of energy and macronutrients across eating occasions. Having a relatively higher energy intake at lunch and supper (OR = 1.19, 95% CI = 1.05 to 1.34) or at mid-afternoon (OR = 1.18, 95% CI = 1.05 to 1.34) at 4 y was associated with higher odds of becoming overweight/obese at 7 y. A relatively higher intake of fat at lunch was positively associated with later children’s odds for being overweight or obese (OR = 1.17, 95% CI = 1.03 to 1.32). These associations were independent of the effect on children’s eating behaviors related to appetite. Our results also show a detrimental relation between skipping breakfast and eating late in the day and children’s body weight. Considering all daily eating occasions, a higher proportion of energy and macronutrient intake at the main meals and a lower proportion during the afternoon and evening seems to be more beneficial for children’s weight. These results emphasize the important role of daily food intake rhythm on excessive weight gain in childhood.
New research areas have emerged to tackle the high prevalence of obesity. In that sense, accumulating evidence has suggested the importance of the time of eating in weight regulation (Almoosawi et al., 2013; Almoosawi et al., 2016; Kupek et al., 2016; Thompson et al., 2006). The circadian rhythm controls several physiological functions, including feeding. Parallel to “chrono-pharmacology,” used to determine the best time to take a medication according to the circadian system of drug functions, the term “chrono-nutrition” has been used to account for the relationship between food intake and the circadian clock (Tahara and Shibata, 2014).
The SCN of the hypothalamus is believed to be the location of the master clock system in mammals, which rules the circadian rhythms (Tahara and Shibata, 2013). The SCN receives LD information through the retinal-hypothalamic tract and organizes the peripheral clocks located in other parts of the body, such as the pancreas, liver, and adipose tissue (Albrecht, 2012). In addition to light, other factors, such as timing and type of nutrient intake, temperature, or exercise, can be a synchronizer for the circadian clock (Tahara and Shibata, 2013). In particular, meal timing might interfere with synchronization of peripheral circadian rhythms in humans (Wehrens et al., 2017). In that way, poor nutrition (including unusual eating times) can disrupt homeostasis, resulting in disturbances in leptin release, glucose and energy metabolism, as well as insulin sensitivity (Cagampang and Bruce, 2012; Hutchison and Heilbronn, 2016). Hence, unusual feeding practices can disrupt clock systems and nutrient metabolism, which may increase the risk of developing diseases like obesity or diabetes (Cagampang and Bruce, 2012; Hutchison and Heilbronn, 2016).
A previous review of observational studies (Almoosawi et al., 2016) on time-of-day energy intake and its association with obesity included evidence from 8 cross-sectional studies (3 in children) and 2 longitudinal cohort studies (one in children). Overall, the studies reported a positive association between evening energy intake and obesity. However, a more recent meta-analysis of observational and interventional trials among adults (Fong et al., 2017), analyzing the association between large evening meals and body mass index (BMI) in adults, showed conflicting evidence and failed to find a significant association between evening intake and BMI. Still, in children, a cross-sectional study (Coulthard and Pot, 2016) also did not find any evidence that eating an evening meal after 2000 h is associated with excess weight in UK children aged 4 to 18 y.
Almoosawi et al. (2016) highlighted that it is still unclear if there are specific patterns of energy distribution that could be more beneficial for metabolic outcomes, especially obesity. Because little evidence exists on how macronutrient distribution influences BMI, and given that lipid and glucose metabolism is influenced by the circadian clock, the authors stressed that the evaluation of time-of-day macronutrient intake is a critical point to consider in future studies (Almoosawi et al., 2016).
Considering the gaps in the literature, this study aimed to assess prospectively the association between time-of-day energy and macronutrient intake at 4 y on BMI at 7 y. Moreover, we sought to assess if the effect of time-of-day intake on obesity is independent of children’s appetite.
Methods
Participants are from the population-based birth cohort Generation XXI (G21), assembled in the public maternity units of the Porto Metropolitan Area (Portugal) during 2005/2006 (n = 8647 newborns) (Larsen et al., 2013). These maternity units were responsible, at enrollment, for 91.6% of the deliveries in the whole eligible population.
The present study included all children evaluated at both 4 and 7 y of age by face-to-face interviews, providing complete 3-day food diary data from age 4 and objective measures of weight and height at 7 y (n = 2035). We excluded twins (n = 60) and children with congenital anomalies or diseases that might influence dietary intake (n = 14), achieving a final sample of 1961 children. In all evaluations, the information regarding socioeconomic characteristics, dietary intake, and medical history were collected by trained interviewers.
The project G21 was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Ethical Committee of the São João Hospital and the University of Porto Medical School. The project was approved by the Portuguese Authority of Data Protection. We have complied with requirements of Portuguese law for pediatric populations. Parents or legal guardians of each participant received an explanation of the purposes and design of the study and gave written informed consent at baseline and at follow-up evaluations.
Dietary Intake
At the 4-y follow-up evaluation, parents or another main caregiver were asked to provide a detailed description of all foods and drinks consumed by the child, in 2 weekdays and 1 weekend day, in a format of a food diary (Vilela et al., 2018). Oral and written instructions were given for the correct completion of food diaries, including information on the estimation of the size of the food portions. Caregivers were also asked to provide a description of the method of food preparation, recipes, place and time of consumption, whenever possible. In case the child was out of the home during the day, parents were advised to ask for the help of other caregivers.
A team of trained nutritionists was responsible for the codification process, using an age-specific food coding manual previously developed by our research team. Nutrient intake was estimated using the software Food Processor SQL (2004-2005 ESHA Research, Salem, Oregon), based on the Food Composition Table of the United States of America Department of Agriculture (US Department of Agriculture and Agricultural Research Service, 2003). For typical Portuguese foods or culinary dishes, new codes were created with national nutritional information.
Meal Definition
The meal definitions have been described previously (Vilela et al., 2019). Briefly, an “eating occasion” was any occasion when food or drink was consumed 30 min apart and provided a minimum of 210 kJ (50 Kcal) of energy. As caregivers did not distinguish the meals in the food diary, the team of trained nutritionists classified and distinguished meals (e.g., breakfast, supper) according to the types of food, the period, and place of consumption. Using this variable, a decision tree (Hearty and Gibney, 2008) was applied to define the best period for breakfast, mid-morning, lunch, mid-afternoon, dinner, and supper. Main meals were unique and considered as breakfast, lunch, and dinner, and the eating occasion with the highest energy contribution was chosen among 0600-0930 h, 1100-1430 h, and 1900-2130 h, respectively. All the other eating occasions were considered as mid-morning, mid-afternoon and supper, and could be chosen more than once. Patterns of time-of-day energy and macronutrient intake according to the meals were identified by factor analysis using standard principal component analysis (PCA).
Anthropometrics
Children’s anthropometric measurements were performed by a team of trained examiners, according to standard procedures. Children’s weight was measured in underwear and without shoes using a digital scale and was recorded to the nearest 0.1 kg. Height was measured as the distance from the top of the head to the bottom of the feet without shoes, using a fixed stadiometer to the nearest 0.1 cm. Children’s BMI, defined as weight in kg divided by height in m2, is often used as a proxy of adiposity in children (Freedman et al., 2005). Age- and sex-specific z-scores were established according to the World Health Organization criteria (WHO Multicentre Growth Reference Study Group, 2006), allowing us to have indirect age- and sex-specific measures of relative adiposity.
Children’s Eating Behaviors Related to Appetite
A Portuguese version of the Children’s Eating Behavior Questionnaire (CEBQ) (Albuquerque et al., 2017) was used to evaluate parental reports (94% of the questionnaires were answered by mothers) regarding their child’s eating behavior at 7 y. This 35-item instrument is rated on a 5-point Likert scale (never, seldom, sometimes, often and always; scored 1 to 5), and includes 8 subdimensions of eating behaviors, containing 3 to 6 items each. In individuals with missing data for less than 50% of the items, missing data (around 3%) were handled by imputation, replacing the average of the remaining questions within each subdimension. These subdimensions were included as potential confounders of the association between time-of-day energy and macronutrient intake and children’s BMI.
Statistical Analysis
Characteristics of children who were normal weight or underweight were compared with those who were overweight or obese using the chi-square test for categorical variables and the Student t test for 2 independent samples.
Patterns of distribution of daily energy and macronutrient intake according to meal type were identified by factor analysis using PCA without rotation and using the co-variance matrix. This methodology was applied separately for absolute intake of energy (kcal), protein (g), carbohydrate (g) and fat (g), performing 4 different PCAs and using all samples. The criteria used were the eigenvalue (>1-times the mean of eigenvalue), scree plot, and interpretability of the components. Principal components are linear combinations of the input variables (6 variables in each pattern) and explain as much of the variation in the data as possible (percentage explained by the component). Each component describes a dietary pattern, and the linear combination allows the calculation of a component score for each child; the higher the score, the more likely this pattern is present in the child’s diet.
The factor score for each child was obtained by summing observed dietary intake weighted by the factor loading, applying the following formula:







The patterns described by each component may be interpreted by its factor loadings, which are the correlations between the component and each input variable. Higher loadings (absolute value) indicate a stronger positive or negative correlation between intake at a specific meal and pattern. Energy or nutrient intake at specific meals with loadings above ±0.3 on a component was considered to have a strong correlation with that component. Labeling of the patterns was based on the highest component loadings within each pattern.
The association between energy and macronutrient intake throughout the day, summarized as the meal pattern score (factor score, continuous variables) at 4 y, and the children’s z-score BMI (non-overweight vs. overweight/obese) at 7 y, was examined using logistic regression models; odds ratios (OR) and respective 95% confidence intervals (95%CI) were obtained. The following potential confounders were tested as potential influencers of either food intake (meal patterns) or BMI and tested statistically in the final models: children’s sex, maternal age and education, child’s z-score BMI, number of meals, total daily energy intake, practice of structured physical activity and sedentary lifestyle at 4 y (Model 1), and CEBQ subdimensions’ score at 7 y (Model 2). Model 2 aims to test the potential mediating effect of children’s eating behaviors related to appetite on the association between time-of-day intake and BMI. The subdimensions included as confounders in Model 2 were the ones statistically significant for the model (p < 0.05).
The Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, Version 23.0. IBM Corp., Armonk, NY), and R language and software environment for statistical computation (version 3.4.1, R Foundation for Statistic Computing, Austria, 2010) software were used. For the Student t test, a significance level of 0.1% was assumed to allow for multiple testing (Feise, 2002). For all other analyses, a p value of <0.05 was used to determine significance.
Results
The prevalence of 7-y-old children as overweight or obese was 36.7%. The characteristics of children classified as normal/underweight and overweight/obese are presented in Table 1. The mean energy intake was higher in the overweight/obesity group than in the normal weight/underweight group; although, this did not achieve statistical significance (p = 0.069). The proportion of energy intake at dinner was higher in the normal/underweight group compared with the overweight/obesity group (p = 0.006). On average, maternal education was higher in the normal/underweight group compared with the overweight/obesity group (p < 0.001).
Characteristics of the children according to body mass index categories.
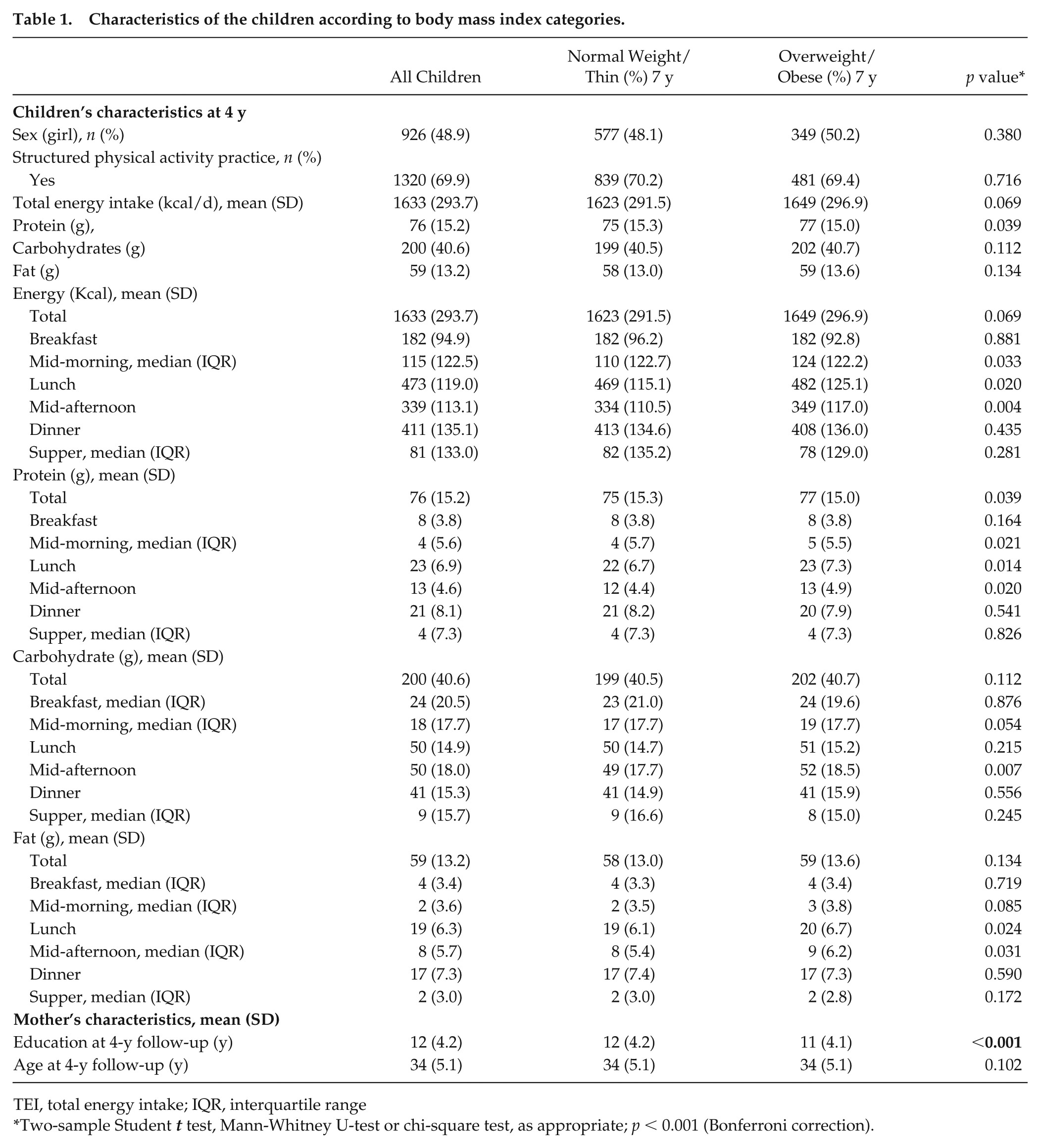
TEI, total energy intake; IQR, interquartile range
Two-sample Student t test, Mann-Whitney U-test or chi-square test, as appropriate; p < 0.001 (Bonferroni correction).
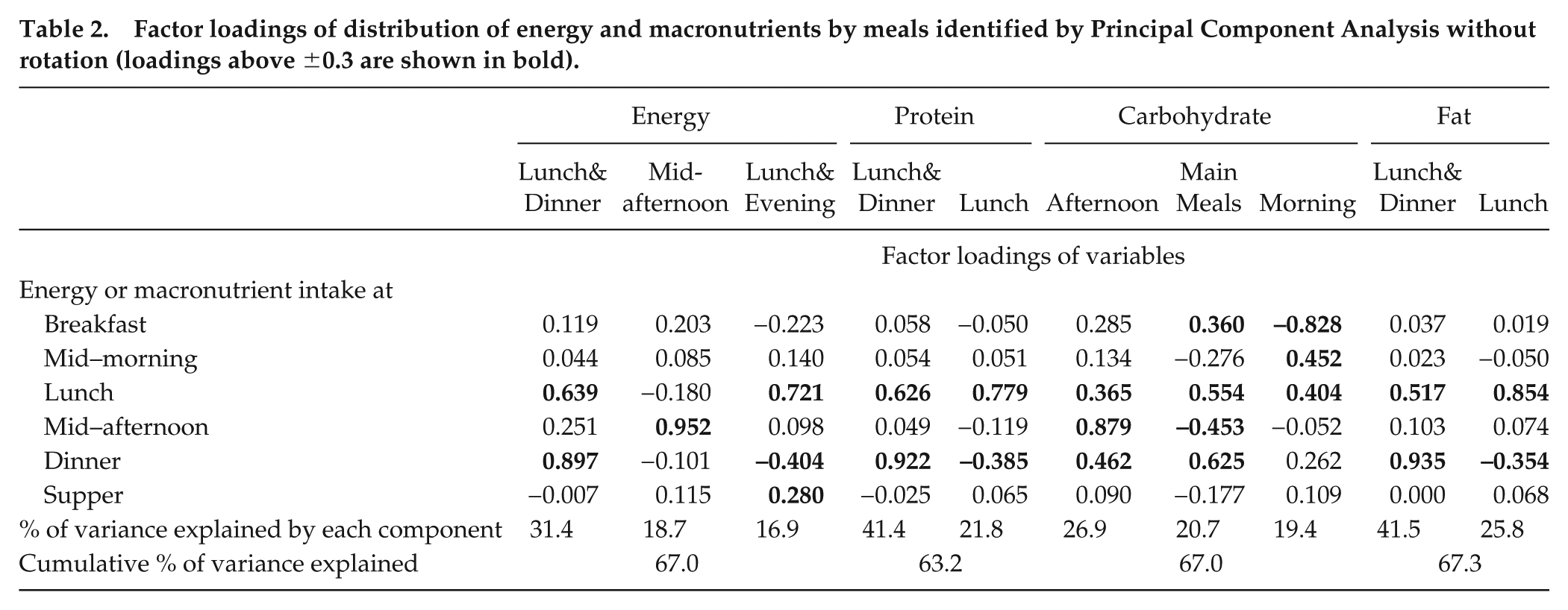
An overview of the component loadings identified by PCA per meal pattern (according to energy and macronutrient distribution by meals) is shown in Table 2 and Figure 1. Three distinct patterns (factors) were identified for energy intake, explaining 67% of all data variance. The first pattern, labeled “Lunch&Dinner,” is characterized by higher energy intake at lunch and dinner and represents children who start and finish eating earlier; i.e., they have breakfast and do not eat anything else after dinner. The second pattern was labeled “Mid-afternoon” based on its high loadings of energy intake in the mid-afternoon. Children from this pattern start eating earlier, have a late lunch and finish eating later. The last pattern was labeled “Lunch&Evening,” and is characterized by higher energy intake at lunch and supper but lower energy intake at dinner. This pattern seems to combine breakfast skipping with a late eating pattern. For protein intake, 2 patterns identified explained 63% the total data variance. The patterns were “Lunch&Dinner,” characterized by a higher intake of protein at lunch and dinner, and “Lunch,” characterized by higher intake at lunch but lower intake at dinner. Three distinct patterns were identified for carbohydrate intake, namely, “Afternoon,” “Main Meals,” and “Morning,” and together they explained 67% of the total variance. The first pattern is characterized by a higher intake of carbohydrates at lunch, mid-afternoon and dinner. The second pattern is characterized by a higher intake of carbohydrates at all main meals but a low intake at mid-afternoon. Finally, the last pattern is characterized by a higher intake at mid-afternoon and lunch but a lower intake at breakfast. Two patterns were identified for fat intake, similar to the patterns observed for protein intake: higher fat intake at lunch and dinner (“Lunch&Dinner”) and a higher intake at lunch but lower intake at dinner (“Lunch”). These 2 distinct patterns explained 67% of the total data variance.
Factor loadings of distribution of energy and macronutrients by meals identified by Principal Component Analysis without rotation (loadings above ±0.3 are shown in bold).
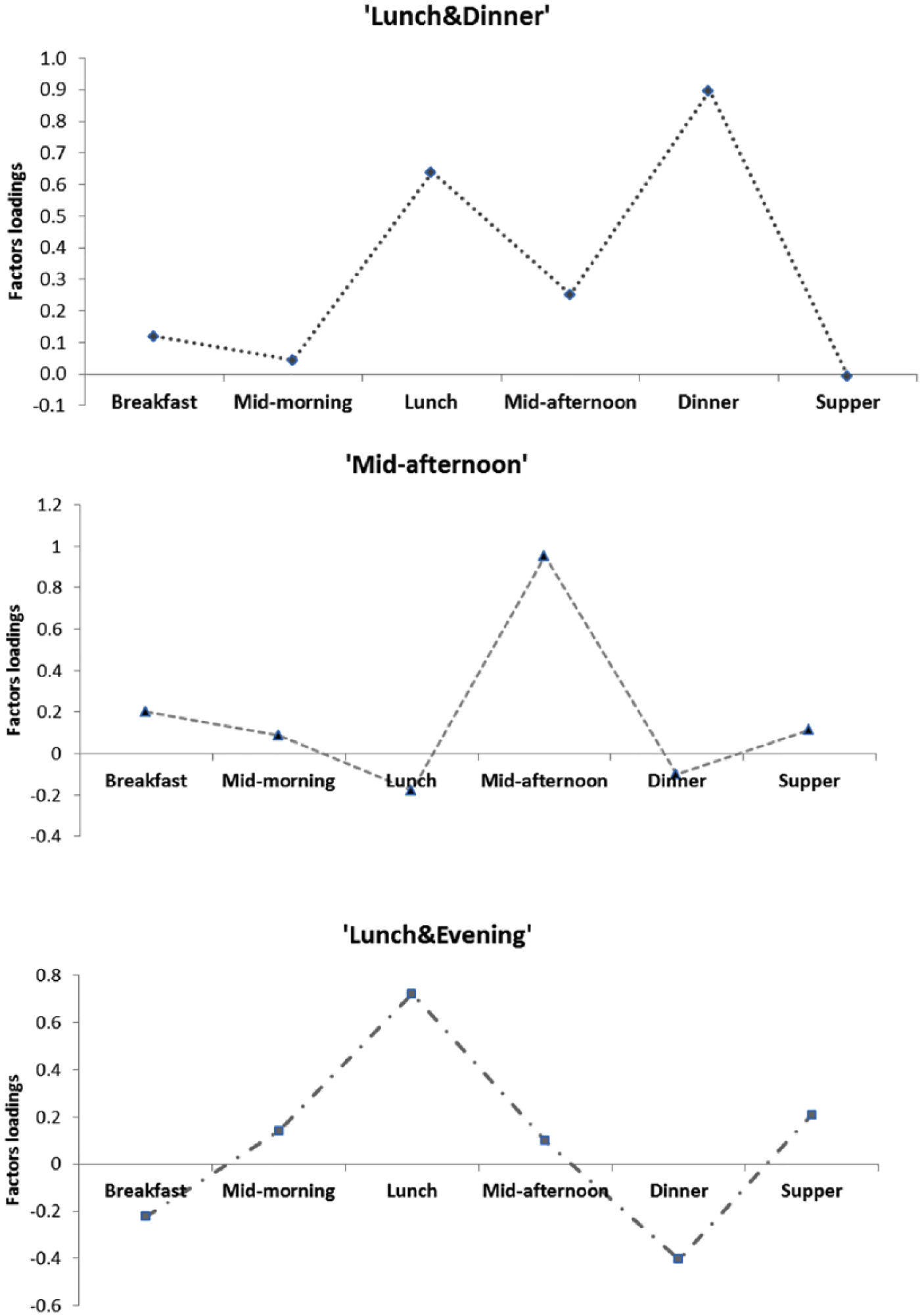
Graphic illustration of the factor loadings of energy distribution by daily meals identified by principal component analysis.
Table 3 shows the associations between meal patterns for daily energy and macronutrient distribution and the odds for being overweight/obese at 7 y. After adjustment, higher scores in the pattern “Mid-afternoon” (OR = 1.18, 95% CI = 1.05 to 1.34) and “Lunch&Evening” (OR = 1.19, 95% CI = 1.05 to 1.34) for energy intake at 4 y were associated with a higher odds of being overweight/obese at 7 y (model 1). Relatively higher fat intake at lunch but lower intake at dinner (“Lunch pattern”) at 4 y was positively associated with being overweight/obese at 7 y (OR = 1.17, 95% CI = 1.03 to 1.32). After adjustment, neither carbohydrate nor protein daily distribution at 4 y was associated with being overweight/obese at 7 y (model 1). The adjustment for children’s eating behaviors (model 2) did not change significantly the associations described before.
Association between meal patterns at 4 y and BMI at 7 y.
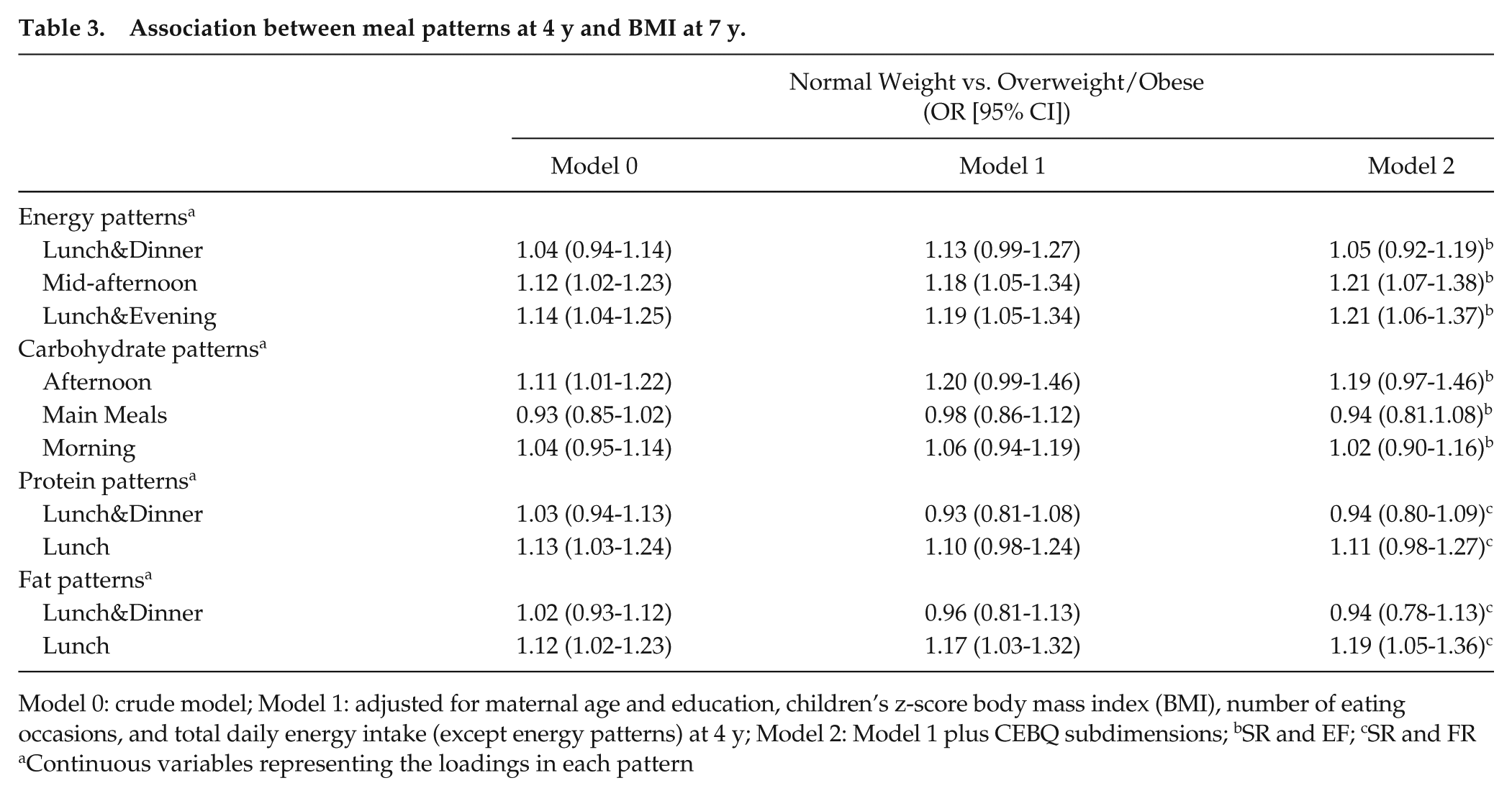
Model 0: crude model; Model 1: adjusted for maternal age and education, children’s z-score body mass index (BMI), number of eating occasions, and total daily energy intake (except energy patterns) at 4 y; Model 2: Model 1 plus CEBQ subdimensions; bSR and EF; cSR and FR
Continuous variables representing the loadings in each pattern
Discussion
To our knowledge, this is the first study to consider meal patterns of energy and macronutrient distribution and their association with children’s body weight status using a prospective approach. After adjusting for potential confounders, we found that having a relatively higher energy intake at lunch and supper or in the mid-afternoon was positively associated with later children’s BMI. Similarly, a relatively higher intake of fat at lunch at 4 y increased the odds of becoming overweight/obese at 7 y. These associations were independent of the effect on children’s eating behaviors related to appetite. No association was found between time-of-day protein or carbohydrate intake and BMI.
The pattern that combines breakfast skippers and late eaters (“Lunch&Evening” energy pattern) shows a connection between these 2 behaviors. Many studies have previously assumed these are independent exposures (McCrory, 2014; Pendergast et al., 2016); however, this pattern analysis shows they are inherently linked. Overcompensation for the energy missed at breakfast seems to occur in these children. This might be explained by the lower satiety associated with skipping breakfast (compared with children who have breakfast) that leads to overeating later in the day. Over time, this would result in an unhealthy weight gain (McCrory, 2014). Another explanation might be that children who eat later in the night are not hungry in the morning when they wake up and, therefore, they skip breakfast. Indeed previous studies have described that the energy or nutrients consumed at certain times of day influences subsequent eating occasions (Almoosawi et al., 2016; Thompson et al., 2006). For example, in a longitudinal study among girls aged 8-12 and 11-19 y, the mean energy consumed in the evening period during weekdays was negatively correlated with the mean energy consumed in the mornings and afternoons during weekdays (Thompson et al., 2006). The overall results indicated that the mean percentage of daily energy intake at night was positively associated with changes in the girls’ BMI (Thompson et al., 2006).
Studies among shift workers suggest that nocturnal eating could result in metabolic disruption (Holmback et al., 2003; Al-Naimi et al., 2004), partly explained by a decrease in glucose tolerance and insulin resistance at night (Boden et al., 1996; Morris et al., 2012). Accordingly, changes in the levels of circulating leptin or ghrelin by circadian disruption could influence energy intake and expenditure. Moreover, research also suggests that energy metabolism is less efficient during the evening, as morning diet-induced thermogenesis is significantly higher than night-induced thermogenesis (Bo et al., 2015). In this way, eating late in the day or at night may disrupt circadian rhythms leading to excessive weight gain. One of the meal patterns described in our study and positively associated with the odds of being overweight/obese was having a higher energy intake at lunch and supper.
A more holistic approach has been encouraged for exploring complex issues, such as nutrition-related health outcomes, before addressing any specific questions (Fardet and Rock, 2014). Traditional analysis of isolated foods or nutrients has been relevant, for instance, in decreasing the prevalence of hypovitaminosis; however, due to the complex nature of diet, this approach seems to fail to adequately describe the diversity of metabolic effects on the entire organism (Hoffmann, 2003). An analysis at the level of meal pattern allows for an assessment of the combined effects of compound food synergy and translation into meaningful results, such as dietary guidelines (Jacobs and Tapsell, 2013). In the present study, the patterns of energy and macronutrient distribution by meal were examined in relation to obesity likelihood and appetite control in children, as previously recommended (Almoosawi et al., 2016).
Previous studies have focused on breakfast (Deshmukh-Taskar et al., 2010; Timlin et al., 2008) or evening meals only (Coulthard and Pot, 2016), failing to capture how energy intake at one meal is associated with intake at other times. Our study has overcome these limitations by examining the prospective association between timing of energy and macronutrient intake and obesity in children, using all eating occasions.
Previous research has shown that specific appetite-related traits (e.g., high response to environmental food cues) are positively associated with a child’s weight, whereas other traits, such as “satiety responsiveness” (perception of internal satiety cues) are inversely associated with a child’s weight (Carnell and Wardle, 2007). Moreover, the influence of the circadian clock on hunger and appetite has been previously suggested (Scheer et al., 2013). This endogenous control seems to be independent of other behaviors, such as the duration of time since waking up (Sargent et al., 2016; Scheer et al., 2013). Experimental studies have also shown an effect of varying the macronutrient intake of a meal or of the overall diet on appetite, with a more pronounced effect from proteins on suppressing appetite (Beasley et al., 2009; Dougkas and Ostman, 2016). The further adjustment of CEBQ’s subdimensions to the association between meal patterns and children’s BMI showed that the effect of time-of-day energy and macronutrient intake on obesity was independent of the effect on children’s appetitive behaviors, and thus these behaviors do not seem to be mediating factors in those associations.
Another study using dietary patterns based on time-of-day eating events described that Brazilian children having a traditional lunch with rice and beans as the main meal of the day had the lowest obesity risk (Kupek et al., 2016). These results highlight the importance of considering both when and what is eaten for weight regulation. The irregularity of energy intake, especially at breakfast and between meals, appeared also to be related to a higher cardiometabolic risk in adults, including an increased waist circumference and BMI (Pot et al., 2014). The time of day and the nutrient composition of the meals were also associated with other chronic diseases, such as metabolic syndrome and its individual components, including abdominal obesity (Almoosawi et al., 2013). Results from this research show that carbohydrate intake at breakfast or mid-morning is protective against abdominal obesity (Almoosawi et al., 2013). In our study, we found a positive association between consuming carbohydrates in the afternoon and BMI in children, but after adjustment for total daily energy intake, the association was no longer significant.
Similar to our results, a previous study showed that the timing of lunch in a Mediterranean adult population influenced weight loss during a 20-week dietary intervention in overweight or obese adults (Garaulet et al., 2013). Late lunch eaters lost less weight, independent of the total energy intake, dietary composition, estimated energy expenditure, appetite hormones, and sleep duration (Garaulet et al., 2013). In parallel, our results showed an effect of time-of-day energy and fat composition on adiposity that was independent of appetite control (using CEBQ as proxies). Changes in chronotype, genetic background, and/or function of the circadian system may be implicated in these associations (Garaulet and Gomez-Abellan, 2014).
Some strengths of this study were the prospective design based on a large population-based birth cohort, the age frame considered, the detailed measures of dietary intake, and the objective measures of children’s weight and height. The use of a prospective cohort also allowed testing a wide set of potential confounders. Some limitations of this study need further discussion. Misreporting of dietary intake among individuals with excessive weight has been previously described in the literature (Wehling and Lusher, 2017), which might affect the association between eating habits and BMI. However, there is no evidence of a misreporting of the time of eating, and we believe that, in this particular study, misreporting might have been minimized as the parents were the ones reporting the children’s dietary intake, and not the children themselves. Additionally, selection bias may have occurred due to the high burden related to the completion of food diaries. Comparing the children included in our study with the remaining cohort, we did not find statistically significant differences regarding sex and BMI (at 7 y); although, mothers included in this study were slightly older (30.0 [5.09] vs. 28.7 [5.70] y, p < 0.001) and more educated (11.5 [4.25] vs. 10.1 [4.21] school y, p < 0.001) in comparison with the mothers included at baseline. However, these differences are more likely to be due to a large sample size rather than to considerable differences. Despite adjustment for relevant confounders, some residual confounding cannot be excluded. Lastly, future work as more birth cohorts become available would make it possible to replicate these findings in an independent Portuguese cohort, which was not possible here.
In conclusion, considering all daily eating occasions, our results suggest that a higher proportion of energy and macronutrient intake at the main meals and a lower proportion at the afternoon and evening snack times are more beneficial for children’s body weight. This study increases our understanding of the potential importance of the daily rhythm of food intake on childhood overweight/obesity development. Although the mechanisms associated with meal timing and weight regulation are not fully understood yet, our results suggest that new therapeutic strategies, as well as preventive measures, should consider not only the nutrient composition of the diet but also the timing of feeding.
Footnotes
Acknowledgements
S.V. contributed to the design of the study, conducted the statistical analysis and interpretation of data and drafted the initial manuscript. M.S. contributed the statistical analysis and to the interpretation of data. A.O. and C.L contributed to the design of the study and discussion of results. All authors were involved in writing the paper and had final approval of the submitted and published versions. The authors gratefully acknowledge the families enrolled in Generation XXI for their kindness, all members of the research team for their enthusiasm and perseverance, and the participating hospitals and their staff for their help and support. The authors acknowledge the support from the Epidemiology Research Unit (EPI-Unit: UID-DTP/04750/2013).
Generation XXI was funded by the Health Operational Programme – Saúde XXI, Community Support Framework III and the Regional Department of Ministry of Health. It was also supported by the Calouste Gulbenkian Foundation, by FEDER from the Operational Programme Factors of Competitiveness – COMPETE, and by national funding from the Foundation for Science and Technology – FCT (Portuguese Ministry of Education and Science) under the projects PTDC/SAU-EPI/121532/2010 (FEDER-Operational Programme Factors of Competitiveness – COMPETE – FCOMP-01-0124-FEDER-021177) and POCI-01-0145-FEDER-030334); by the Unidade de Investigação em Epidemiologia - Instituto de Saúde Pública da Universidade do Porto (EPIUnit) [Ref. UID/DTP/04750/2013]. This research was also supported by the PhD Grant SFRH/BD/92389/2013 (SV) co-funded by the FCT and the POPH/FSE Program, and by the FCT Investigator contract (IF/01350/2015) (AO)
Data Sharing and Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflict of Interest Statement
The author(s) have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.