
Abstract
Melatonin is secreted systemically from the pineal gland maximally at night but is also produced locally in many tissues. Its chronobiological function is mainly exerted by pineal melatonin. It is a feedback regulator of the main circadian pacemaker in the hypothalamic suprachiasmatic nuclei and of many peripheral oscillators. Although exogenous melatonin is approved for circadian rhythm sleep disorders and old-age insomnia, research on endogenous melatonin in humans is hindered by the great interindividual variability of its amount and circadian rhythm. Single case studies on pinealectomized patients report on disrupted but also hypersomnic sleep. This is the first systematic prospective report on sleep with respect to pinealectomy due to pinealocytoma World Health Organization grade I without chemo- or radiotherapy. Before and after pinealectomy, 8 patients completed questionnaires on sleep quality and circadian rhythm (Pittsburgh Sleep Quality Index, Epworth Sleepiness Scale, and Morningness-Eveningness Questionnaire), 2 nights of polysomnography, salivary evening melatonin profiles, and qualitative assessment of 2 weeks of actigraphy and sleep logs. Six patients were assessed retrospectively up to 4 years after pinealectomy. Before pinealectomy, all but 1 patient showed an evening melatonin rise typical for indifferent chronotypes. After pinealectomy, evening saliva melatonin was markedly diminished, mostly below the detection limit of the assay (0.09 pg/mL). No systematic change in subjective sleep quality or standard measures of polysomnography was found. Mean pre- and postoperative sleep efficiency was 94% and 95%, and mean sleep-onset latency was 21 and 17 min, respectively. Sleep-wake rhythm during normal daily life did not change. Retrospective patients had a reduced sleep efficiency (90%) and more stage changes, although this was not significantly different from prospective patients. In conclusion, melatonin does seem to have a modulatory, not a regulatory, effect on standard measures of sleep. Study output is limited by small sample size and because only evening melatonin profiles were assessed.
Keywords
Introduction
The human pineal gland is involved in circadian regulation. In both diurnal and nocturnal vertebrates, it synthesizes and releases the indoleamine melatonin (N-acetyl-5-methoxytryptamine) in a rhythmic fashion, with a peak during the dark period and with almost undetectable amounts during daytime (Adrendt et al., 1977; Lewy and Markey, 1978). Pineal melatonin secretion is regulated by the main endogenous circadian pacemaker, the hypothalamic suprachiasmatic nuclei (SCN), and by light via a multisynaptic pathway starting from retinal ganglion cells (Klein et al., 1971; Lucas et al., 1999). On the contrary, melatonin is a feedback regulator of the SCN and of many peripheral oscillators (McArthur et al., 1991).
Although it is now well known that melatonin is produced in many tissues, systemic melatonin that is detectable in blood and saliva is mainly derived from the pineal gland, and pineal-derived melatonin is mainly responsible for its chronobiological function (Binkley, 1993; Lewy et al., 1980).
Between-subject comparison of the melatonin profile is hindered by great interindividual variability: morning chronotypes have an advanced and evening chronotypes a delayed melatonin profile, and there are up to 5-fold differences between “low” and “high secretors” (Arendt et al., 1979; Bergiannaki et al., 1995; Burgess and Fogg, 2008). Because of these obstacles, the hypotheses that endogenous melatonin is important for (1) circadian sleep-wake rhythm and (2) sleep quality were not consistently confirmed in humans.
Pharmacological doses of exogenous melatonin have been proven to be effective in disorders of the circadian rhythm such as jetlag, shift work, delayed sleep phase syndrome, or irregular rhythm in blind people (Arendt et al., 1986; Arendt et al., 1988; Arendt and Skene, 2005; Dawson et al., 1995; Sack et al., 2000). More doubts exist on the soporific effect of melatonin (Brzezinski et al., 2005; Ferracioli-Oda et al., 2013). In diurnal vertebrates, the endogenous melatonin profile is strongly related to sleep (Shochat et al., 1997), and its prolonged-release formulation is approved for the treatment of old-age insomnia (Garfinkel et al., 1995; Lemoine et al., 2007; Wade et al., 2011).
In the rat, the diurnal sleep-wake cycle and sleep architecture are unchanged after experimental pinealectomy (Fisher and Sugden, 2010). Also, the diurnal sleep-wake cycle is normal in the inbred mouse strain C57BL/6J, which carries a natural “knockdown” of melatonin (Roseboom et al., 1998). However, both of these animals are nocturnal species in whom high melatonin concentrations are related to the period of activity, rather than sleep. In humans, pinealectomy has to be performed only rarely if there is a tumor in the pineal region. Pineal region tumors constitute only 1% of all brain tumors (Grimoldi et al., 1998; Leston et al., 2009). Most are germinomas but also pineal parenchymal tumors, meningeomas, glial tumors, craniopharyngeomas, lymphomas, and teratomas. Melatonin can be produced by the tumor (in the case of germinomas). The physiological rhythmic pattern can be maintained or secretion can be diminished due to an undifferentiated and invasive tumor (Barber et al., 1978; Grimoldi et al., 1998; Leston et al., 2009; Miles et al., 1985; Murata et al., 1998; Walker et al., 1996). Melatonin depletion can be used to confirm complete tumor and pineal gland resection (Leston et al., 2009; Murata et al., 1998; Neuwelt and Lewy, 1983).
Only a few unsystematic, retrospective, mainly single case studies have reported on the outcome of pinealectomized patients regarding sleep (Etzioni et al., 1996; Jan et al., 2001; Lehmann et al., 1996; Petterborg et al., 1991; Quera-Salva et al., 2011). These studies report on insomnia and sleep continuation problems but also on hypersomnia or somnolence: in 5 of the 6 reported patients, the sleep abnormalities were improved by melatonin replacement (Etzioni et al., 1996; Jan et al., 2001; Lehmann et al., 1996; Petterborg et al., 1991; Quera-Salva et al., 2011). However, only positive results of melatonin treatment might have been published in single case studies. Methodological shortcomings and heterogeneity of treatments add to the weakness of these studies: sleep was mainly assessed by actimetry or sleep log, and patients received chemotherapy or radiotherapy, had hydrocephalus or postoperative aseptic meningitis, or received only partial pinealectomy. More systematic studies show that far from all pinealectomized subjects have sleep problems. Two retrospective cohort studies report on subjective sleep complaints: one study reported on 14 patients with pineal and/or hypothalamo-neurohypophyseal tumors who were assessed up to 11 years after partial pineal resection, chemotherapy, and radiotherapy, with 3 (21%) reporting sleep problems that were confirmed by polysomnography (PSG) in 2 patients (Murata et al., 1998). Another study reported that 6 months to 6.5 years after pinealectomy, 54% of the patients (n = 13) complained of nighttime wake periods that lasted longer than 1 h (poster presentation only; Macchi and Bruce, 2004).
We conducted the first prospective study on the effect of pinealectomy on sleep in humans. Sleep was assessed by means of questionnaires and PSG, and pre- and postoperative salivary evening melatonin profiles were determined. Although evening partial melatonin profiles are usually used to determine the circadian phase of the individual (i.e., its chronotype; Pandi-Perumal et al., 2007), we used it as an approximation for the endogenous pineal melatonin secretion. The 24-h melatonin profiles after pinealectomy and the consecutive depletion of melatonin have already been published in several studies (Jan et al., 2001; Kocher et al., 2006; Lehmann et al., 1996; Leston et al., 2009; Murata et al., 1998; Neuwelt and Lewy, 1983; Quera-Salva et al., 2011). However, this was not assessed together with a systematic evaluation of sleep. Physiologically, the majority of melatonin is produced after midnight, with peak concentrations occurring between 0200 and 0400 h, and some individuals have almost undetectable concentrations of melatonin (Burgess and Fogg, 2008). However, in most people, the onset of nightly melatonin secretion occurs before midnight, usually 2 h before sleep onset (Burgess and Fogg, 2008; Leston et al., 2009; Neuwelt and Lewy, 1983). Fourteen days of actimetry and sleep logs both before and after pinealectomy were judged qualitatively as patients continued with their daily routines. Only patients with pinealocytoma World Health Organization (WHO) grade I who did not have to undergo chemo- or radiotherapy as confounding factors were included. To examine long-term effects of pinealectomy, the same protocol was applied to 6 retrospectively assessed patients up to 4 years after pinealectomy.
Materials and Methods
Patients
From July 2010 to October 2012, 8 consecutive patients who had been scheduled for complete pinealectomy due to a suspected pineocytoma WHO grade I were prospectively assigned to the study. Except for 1 patient aged 14 years, all were adults. All enrolled patients underwent complete pinealectomy via an infratentorial supracerebellar approach. Diagnosis and indication for surgery were based on clinical symptoms and on a contrast-enhanced magnetic resonance imaging (MRI) scan with a 3 Tesla MR scanner (Achieva 3T; Philips Medical Systems, Eindhoven, the Netherlands B.V.).
Ethical Standard
The study is well in accordance with ethical standards of our university and the Declaration of Helsinki. It was approved by the local ethics committee (registration number: prospective study: 5225/11, retrospective study: 3094/11). Informed consent was obtained from every participating patient.
Study Procedures
Each participant underwent a detailed clinical assessment of sleep before and after pinealectomy: the preoperative assessment was conducted between 1 and 3 weeks prior to surgery. The postoperative assessment was conducted when the patient had recovered from the acute postoperative phase and was stable in his or her daily life and sleep habits.
Questionnaires
Participants completed questionnaires on their sleep quality and sleep habits (Pittsburgh Sleep Quality Index [PSQI]; Buysse et al., 1989), on daytime sleepiness (Epworth Sleepiness Scale [ESS]; Johns, 1991), and on their chronotype (Horne-Östberg Morningness-Eveningness Questionnaire, German version [D-MEQ]; Horne and Östberg, 1976).
As clinically significant depressive symptoms were reported to be highly prevalent after pinealectomy (58%; Macchi and Bruce, 2004) the Beck Depression Inventory–II (BDI-II) was applied (Beck et al., 1996).
Salivary evening melatonin profiles
Salivary evening melatonin profiles were determined for each participant on both nights of PSG following the protocol of the manufacturer (Bühlmann Laboratories, Schönenbuch, Switzerland). Participants were in dim light (<10 lux) 3.30 h before bedtime. The first sample was collected 2.30 h before bedtime and every 30 to 45 min thereafter. Melatonin content was determined by means of a direct double-antibody radioimmunoassay in an external laboratory (Synlab, Munich, Germany) (Voultsios et al., 1997). A saliva melatonin concentration of 3 pg/mL was defined as the threshold for the evening dim-light melatonin onset (DLMO) (Molina and Burgess, 2011; Nagtegaal et al., 1998).
To control for measurement errors, we assessed an additional 4 patients who have had craniotomy for other reasons, 3 patients who have had lumbar hernial disk resection, and 4 prospectively assigned pinealectomy patients who participated in preoperative assessments but either did not undergo pinealectomy or refrained to do postoperative assessments (2 patients each). We obtained physiological evening melatonin profiles and an appropriate DLMO in all of them (n = 11; data not shown).
Polysomnography
PSG was performed for 2 consecutive nights. To exclude first night effects, only the second night was used for statistical analysis. Polysomnography included electroencephalography (EEG), electro-oculography (EOC), 2-sided submental electromyography (EMG), pectoral electrocardiography (ECG), nasal airflow assessment via thermistor, snoring microphone, thoracic and abdominal belts to assess breathing motion, pulse oximetry, anterior tibial EMG on both legs, and video monitoring. Recording was performed within an 8-h time frame on individually identical pre- and postsurgery bedtimes from 2200–0000 h until 0600–0800 h. Scoring of sleep stages was performed by the same experienced scorer following the criteria of Rechtschaffen and Kales; limb movements were scored following the criteria of the American Academy of Sleep Medicine (AASM) (Iber et al., 2007; Rechtschaffen and Kales, 1968).
Actigraphy and sleep logs
As a measure of circadian rhythm, participants wrote sleep logs and wore a piezo-sensitive electronic wrist actigraph (3D Biolog; Gefatec, Tiefenbach, Germany) for 2 weeks before and after surgery.
Retrospectively Assessed Patients
To examine long-term effects of pinealectomy, the same procedures were applied to 6 retrospectively assessed patients after pinealectomy due to WHO grade I pineocytomas.
Statistical Analysis
Statistics were performed in Microsoft Excel for Windows, version 14.0 (Microsoft, Redmond, WA), and IBM SPSS Statistics for Windows, version 19.0 (SPSS, Inc., Chicago, IL). Pre- and postsurgery results were compared with paired t tests. Polysomnographic data of retrospective patients were compared with prospective presurgery results by unpaired t tests. Because of the small sample size, data were also analyzed by nonparametric Mann-Whitney U tests, which revealed similar results (not shown). All results are presented as mean ± standard deviation (SD). A value of p < 0.05 was considered significant.
Results
Patient Characteristics
Of the 8 prospectively assigned patients, 6 were women and 2 were men. In the retrospective patient group, gender was equally distributed (3:3). Prospective pinealectomy patients were examined around 11 ± 7 days before surgery and 237 ± 210 days (i.e., around 8 months) after surgery. Retrospective patients were examined after a mean of 32 ± 9 months after pinealectomy. The mean age of participants was in the range of young to middle-aged adulthood, except for 1 patient who was only 14 years of age; prospective patients were 29 ± 11 years old, and retrospective patients were 30 ± 5 years old.
Salivary Evening Melatonin Profiles
Preoperative salivary evening melatonin profiles were obtained from 6 of the prospective patients. Five subjects showed salivary evening melatonin profiles typical for indifferent chronotypes (the DLMO occurred between 2030 and 2300 h; Figure 1a) (Bergiannaki et al., 1995; Lewy and Sack, 1989). The 14-year-old patient did not show detectable melatonin concentrations until 0:30 a.m. (sample collection until 0030 h was performed at a third night at home).
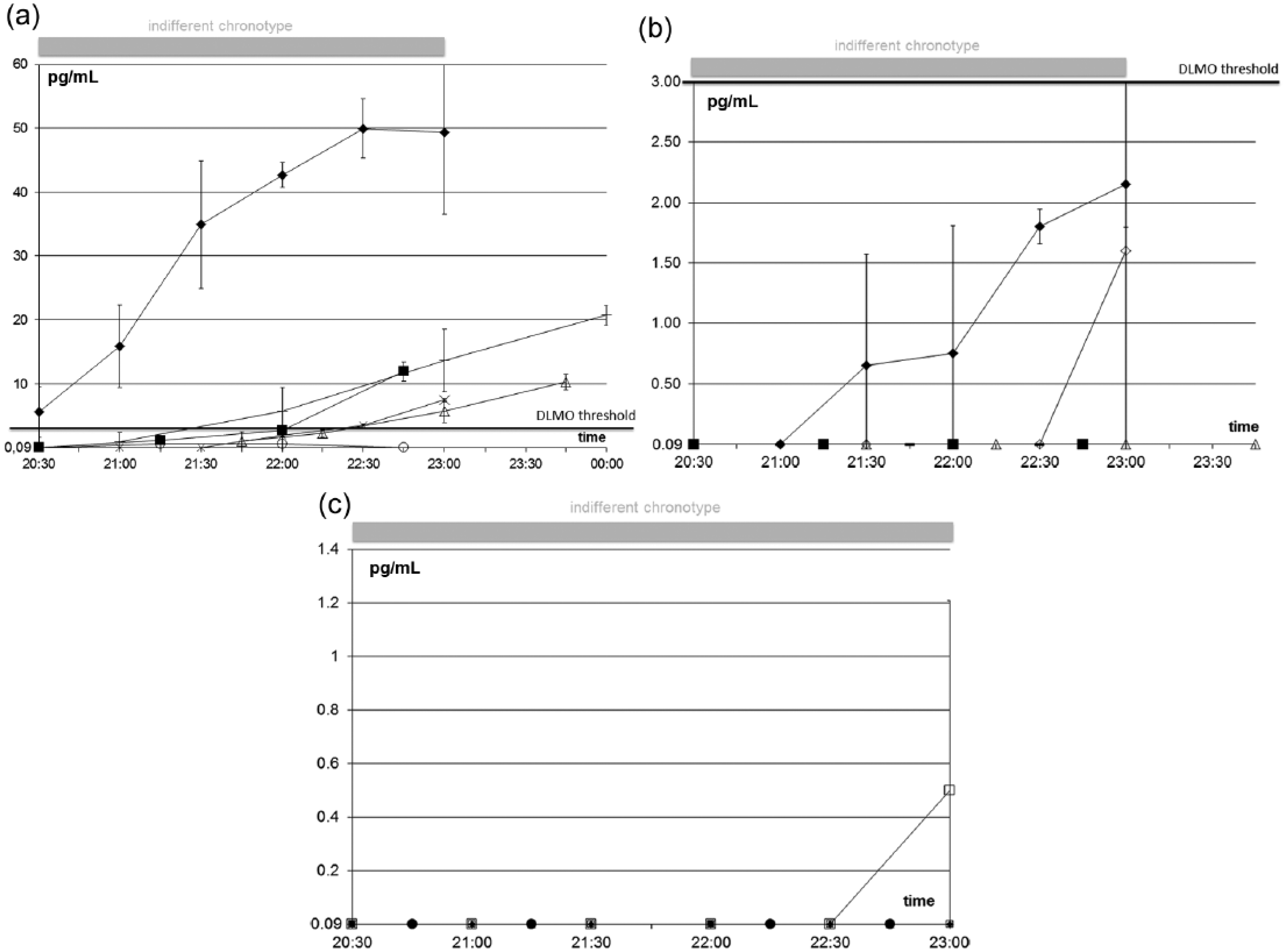
Individual salivary evening dim-light melatonin profiles in prospectively assigned patients before pinealectomy (a, n = 6), after pinealectomy (b, n = 7), and in the retrospectively enrolled patients after pinealectomy (c, n = 6). The threshold for the dim-light melatonin onset (DLMO) was defined as 3 pg/mL. It occurs between 2030 and 2300 h in indifferent chronotypes (gray bar). (a) Preoperatively, all but 1 patient (open circle) reached suprathreshold melatonin concentrations within the expected time frame. (b) After pinealectomy, melatonin concentrations were below the detection level of the assay for most patients (<0.09 pg/mL); in the 2 patients with detectable melatonin concentrations (filled and open rhomb), it was still below the threshold for the DLMO. (c) None of the retrospectively assigned patients after pinealectomy had a concentration above the defined threshold for the DLMO. In all but 1 (open square) patient, melatonin concentration was below the detection level of the assay (data are presented as mean of 2 measurements on the 2 consecutive nights in the sleep laboratory ± SD).
After pinealectomy, we obtained saliva samples from all patients except from the 14-year-old patient who lacked detectable melatonin concentrations before surgery and refused sample collection thereafter. In all other patients, salivary melatonin concentrations were below the DLMO threshold (<3 pg/mL), and in 5, they were below the detection level of the assay (<0.09 pg/mL) (Figure 1b).
Moreover, in all 6 retrospectively assigned pinealectomized patients, evening salivary melatonin concentrations were below the DLMO threshold, and in 5, melatonin was undetectable (Figure 1c).
Questionnaires
Prospective patients
Paired t tests did not reveal any significant differences between average questionnaire scores after pinealectomy compared to the presurgical state (n = 8, Table 1).
Questionnaire Results of Prospectively and Retrospectively Assigned Patients (n = 8 and 6).
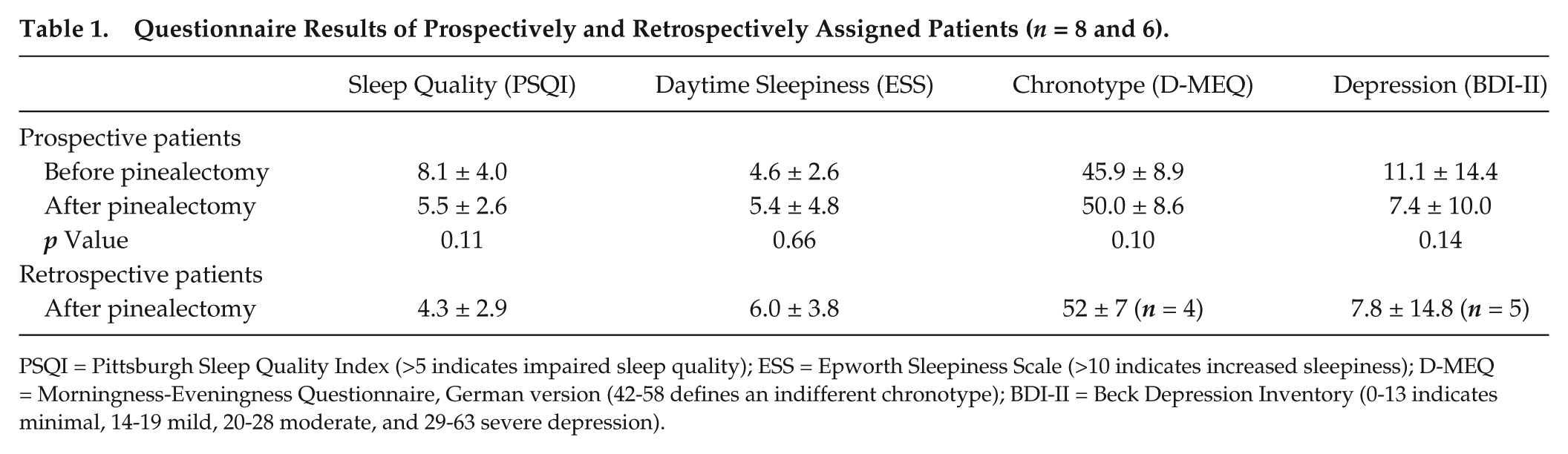
PSQI = Pittsburgh Sleep Quality Index (>5 indicates impaired sleep quality); ESS = Epworth Sleepiness Scale (>10 indicates increased sleepiness); D-MEQ = Morningness-Eveningness Questionnaire, German version (42-58 defines an indifferent chronotype); BDI-II = Beck Depression Inventory (0-13 indicates minimal, 14-19 mild, 20-28 moderate, and 29-63 severe depression).
Before pinealectomy, 6 of 8 patients showed increased insomnia symptoms (PSQI score >5); the average PSQI score was in the range of mildly impaired sleep quality. After pinealectomy, these symptoms slightly but not significantly improved to a borderline average PSQI score and an increased score in 4 of the 8 patients. Average daytime sleepiness was not increased both before and after pinealectomy; individually, 2 patients showed postoperatively increased daytime sleepiness. D-MEQ scores were mostly in the range of indifferent chronotypes (D-MEQ score 42-58). The average BDI-II score was minimally elevated before pinealectomy and slightly but not significantly lower after pinealectomy (BDI score >13 in the same 2 of 8 patients both before and after surgery).
Retrospective patients
Results of the PSQI and the ESS of retrospectively assigned patients have already been published in a larger cohort elsewhere (Krieg et al., 2012). Results of our subsample, together with the results in additional questionnaires, are summarized in Table 1.
The PSQI and ESS revealed low average scores of insomnia or daytime sleepiness (PSQI >5 in 2 of the 6 patients, ESS score >10 in 1 patient). According to the D-MEQ, retrospective patients mostly scored in the range of indifferent chronotypes (D-MEQ score 42-58). The mean BDI-II score was in the range of minimal depressive symptoms (<13). One patient had a BDI score above 13.
Polysomnography
Prospective patients
No patient had signs of a sleep apnea syndrome or periodic limb movement (PLM) disorder (respiratory distress indices [RDIs] and PLM arousal indices were all <5/h and <10/h, respectively).
Mean values of all sleep parameters were in the physiological range, and paired t tests did not reveal significant changes in objective sleep quality after pinealectomy (n = 8, Table 2).
Polysomnography Results of Prospective and Retrospective Patients (n = 8 and 5, mean ± SD).
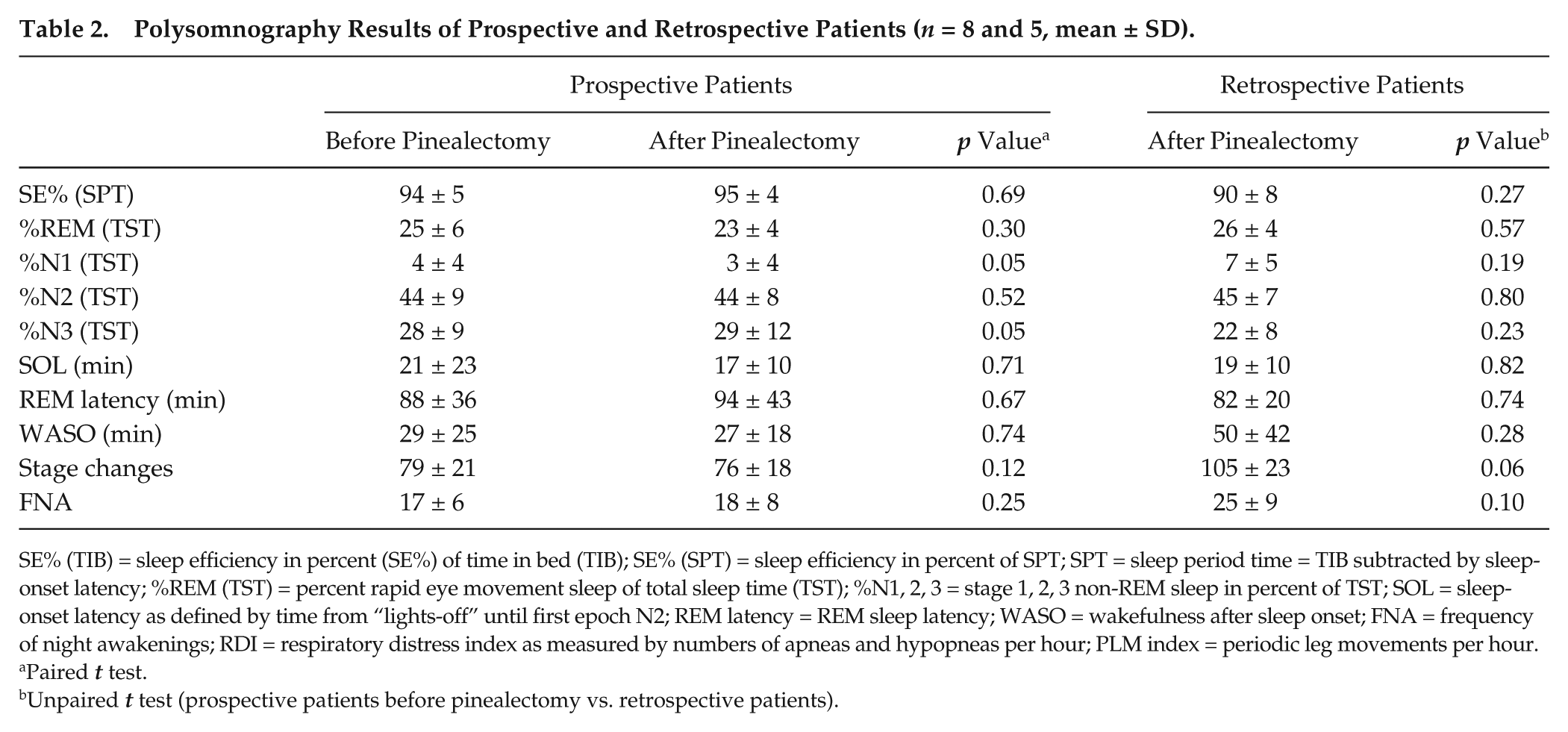
SE% (TIB) = sleep efficiency in percent (SE%) of time in bed (TIB); SE% (SPT) = sleep efficiency in percent of SPT; SPT = sleep period time = TIB subtracted by sleep-onset latency; %REM (TST) = percent rapid eye movement sleep of total sleep time (TST); %N1, 2, 3 = stage 1, 2, 3 non-REM sleep in percent of TST; SOL = sleep-onset latency as defined by time from “lights-off” until first epoch N2; REM latency = REM sleep latency; WASO = wakefulness after sleep onset; FNA = frequency of night awakenings; RDI = respiratory distress index as measured by numbers of apneas and hypopneas per hour; PLM index = periodic leg movements per hour.
Paired t test.
Unpaired t test (prospective patients before pinealectomy vs. retrospective patients).
Retrospective patients
One pinealectomized patient had a mildly increased respiratory distress index (RDI = 9) and an increased PLM arousal index (PLM-A index = 17/h). Neither the ESS nor the PSQI score indicated increased daytime sleepiness or insomnia (3 and 4, respectively). All others had normal RDI and PLM arousal indices (<5/h and <10/h, respectively).
PSG analysis revealed a reduced sleep efficiency in the retrospective patients that was associated with a prolonged wakefulness after sleep-onset (WASO) and a high number of stage changes (n = 5, Table 2). However, neither unpaired t tests nor Mann-Whitney U tests (not shown) revealed significant differences compared to prospective patients before pinealectomy.
Actigraphy and Sleep Logs
As all subjects maintained their daily routines with alternating working-day and weekend bedtimes, actimetry and sleep logs were only judged qualitatively and are not shown. In none of the patients did we observe any irregularity or shift of the rhythm compared to the preoperative state.
Discussion
Limitations
Before interpreting the results, it is necessary to consider several limitations of our study. First, study output is limited by small sample size and missing data. Therefore, less pronounced effects of pinealectomy might have been masked. We included as many subjects as possible of this rare cohort. Additional data from 6 retrospectively assessed patients confirm the results of the prospective study.
Second, we only assessed partial melatonin profiles, which are usually used to determine chronotype (Lewy and Sack, 1989; Nagtegaal et al., 1998; Pandi-Perumal et al., 2007). Reasons for this were discussed earlier. Therefore, we cannot be sure that our subjects were melatonin free. We found physiological evening melatonin profiles in all but 1 prospective patient before pinealectomy. Also, we found this in additional prospective subjects who did not undergo pinealectomy or declined postoperative assessment and in additional control subjects after craniotomy for other reasons or after lumbar hernial disk resection (n = 11, as mentioned in the Materials and Methods section). Our success rate to determine the DLMO is quite high. It is very unlikely that melatonin detection failed only in pinealectomized patients but not in preoperative patients or in additional controls. A large retrospective study in the Netherlands (n = 1848) has shown a success rate of 76% of home collection of saliva samples within a 5-h time frame (Keijzer et al., 2011). In one-third (7%), this was due to very low or undetectable melatonin concentrations, and this was correlated to old age.
Third, we cannot exclude that locally produced melatonin in some ways supports or can take over the chronobiological function of pineal-derived melatonin. There are many extrapineal melatonin-producing sites such as skin, eye, brain, lung, gastrointestinal tract, reproductive organs, and many endocrine tissues (Acuna-Castroviejo et al., 2014). Locally produced melatonin can reach much higher concentrations intracellularly compared to the physiological systemic concentration of melatonin. As yet, it is not entirely understood what mechanism regulates the high intracellular as opposed to relatively low systemic concentrations of this highly lipophilic molecule. The existence of melatonin-binding proteins is discussed (Laudon and Zisapel, 1991; Messner et al., 1998). Also, melatonin is subject to a high hepatic first-pass effect, leading to the known short half-life of melatonin of around 30 min (Weitzman et al., 1978). In the gastrointestinal tract, melatonin concentration is 10 to 100 times higher than in the plasma and 400 times higher than in the pineal gland (Huether, 1993; Messner et al., 2001). In fact, melatonin is not only produced by enterochromaffin cells in the mucosa, but the gastrointestinal tract can accumulate melatonin from the circulation (Messner et al., 1998; Messner et al., 2001). Gastrointestinal melatonin serves not only endocrine but also auto- and paracrine and luminal functions and is not regulated by the photoperiod but by food (Huether, 1993; Ozaki and Lynch, 1976). In diurnal vertebrates such as humans, the low systemic level of diurnal melatonin is mainly derived from gastrointestinal and nocturnal melatonin from the pineal. Also, depletion of pineal melatonin by continuous light exposure or by pinealectomy increases intracellular melatonin in the brain, thymus, and liver of rats, thus indicating an inhibitory effect of pineal melatonin on intracellular melatonin (Jimenez-Jorge et al., 2005; Venegas et al., 2012), but in another study did not change gastrointestinal melatonin (Bubenik and Brown, 1997).
In the end, we had no possibility of assessing sleep and melatonin profiles prospectively before tumor growth.
Salivary Evening Melatonin Profiles
According to our observations, preoperative salivary evening melatonin profiles in patients with pineocytoma WHO grade I showed the characteristic physiological pattern in 5 of 6 cases. After pinealectomy, evening salivary melatonin profiles were below the DLMO threshold in all prospectively assigned patients as well as in all retrospectively assigned patients. As mentioned, melatonin depletion can be used to confirm complete resection of the tumor but has never been determined systematically together with sleep parameters (Leston et al., 2009; Murata et al., 1998; Neuwelt and Lewy, 1983). There is one report on a pinealectomized patient who had normal melatonin concentrations (Krahn et al., 2002). Most likely, pineal tissue has been only partially resected in this patient.
It remains unknown if the 14-year-old, prospectively assessed girl who rated herself as a definite evening chronotype (D-MEQ) did not show suprathreshold salivary melatonin concentrations because the tumor had depleted melatonin secretion or because sample collection was not performed at the appropriate time for this chronotype, although we extended collection until 0030 h. Alternatively, this subject might belong to the few people with constitutively low melatonin levels (Burgess and Fogg, 2008). A depletion of melatonin secretion had particularly been shown for undifferentiated and invasive rather than WHO grade I tumors (Grimoldi et al., 1998; Leston et al., 2009). Physiologically, melatonin secretion is maximal between the age of 3 and 6 years and gradually decreases to 20% by adulthood (Waldhauser et al., 1988).
Subjective Sleep Quality and Depression
Our study did not reveal a significant difference in subjective sleep quality before and after pinealectomy.
In our study, the percentage of patients with insomnia symptoms according to the PSQI was 50% (4 of 8) in prospective patients and 33% (2 of 6) in retrospective patients. Macchi and Bruce (2004) found similar patient numbers (54%) with impaired subjective sleep quality as defined by nighttime wake periods longer than 1 h. In a retrospective study on patients with pineal and/or hypothalamo-neurohypophyseal tumors that were assessed up to 11 years after partial pineal resection, chemotherapy, and radiotherapy, 21% (3 of 14) reported unspecified sleep problems (Murata et al., 1998). We used a rather low PSQI cutoff score (>5), and most of our subjects had mild insomnia symptoms. We have shown earlier in a retrospective study on subjective sleep in pinealectomized patients that the rate of insomnia symptoms is comparable to those after craniotomy for other reasons (Krieg et al., 2012). Also, our prospective study allowed us to show that sleep quality was already impaired before pinealectomy in 6 of 8 patients (75%). Therefore, insomnia symptoms do not appear to be related to systemic melatonin depletion in the evening. We cannot exclude an effect of tumor growth on sleep. Alternatively, preoperative insomnia might be caused by personal concerns about the upcoming surgery and the diagnosis of a brain tumor. Postoperative increased sleepiness in 2 patients who did not have increased PSQI scores indicates that sleep was not restorative for these 2 additional patients, although they did not have complaints of a disturbed nighttime sleep.
As only 2 of 8 of the prospective patients (25%) and 1 of 5 of the retrospective patients (20%) had depressive symptoms that were at least mildly elevated according to the BDI-II (BDI-II >13), our study could not confirm the high prevalence of depression after pinealectomy that had been reported previously in a retrospective study (54%; Macchi and Bruce, 2004) and in a single case study (Jan et al., 2001). Again, in our prospective design, depressive symptoms were already present before pinealectomy and were not related to depletion of evening melatonin. It is controversially discussed whether nightly melatonin levels are reduced in depressed patients (Cryan, 2010; Kennedy et al., 1996).
Objective Sleep Quality
For the first time, our study presents systematically assessed polysomnographic data on the effect of depletion of evening melatonin in humans. It does not provide evidence for any systematic change of standard objective sleep variables due to pinealectomy and depletion of systemic evening melatonin. One previous report performed polysomnography in 2 of 14 retrospectively assessed pinealectomized patients (Leston et al., 2009; Murata et al., 1998; Neuwelt and Lewy, 1983). These were 2 of 3 patients who had complained of sleep difficulties, and PSG showed poor sleep efficiencies of around 60% (Etzioni et al., 1996; Jan et al., 2001; Lehmann et al., 1996; Murata et al., 1998). Another study delivered contrasting results in a single patient in whom PSG revealed prolonged nighttime sleep duration, which was slightly improved by melatonin treatment (Kocher et al., 2006). Again, the power of these retrospective studies on selected patients is very limited not only since the tumor growth was not restricted to the pineal gland area but also because combined treatments of pinealectomy together with radiotherapy (and chemotherapy) were applied.
Retrospectively assessed patients of our study seem to have a reduced sleep efficiency due to an increased WASO and to have more stage changes. This indicates a negative impact of pinealectomy on sleep in the longer term. However, this was not a significant effect and awaits replication in prospective patients.
The multisynaptic pathway that regulates pineal melatonin secretion by light ultimately leads to sympathetic noradrenergic stimulation of the pineal gland by innervation from the superior cervical ganglia. Our results are in contrast to a retrospective study that described a decreased sleep efficiency in 3 patients who had melatonin depletion after cervical spinal cord injury (Scheer et al., 2006) and to another study in which systemic melatonin depletion by application of the β1-blocker atenolol led acutely to increased wake time at night, which was reversed by simultaneous application of exogenous melatonin (n = 10) (Van Den Heuvel et al., 1997).
We can also consider pinealectomy as the reverse situation of exogenously applied melatonin—although these studies investigate more acute effects of melatonin and although pharmacological but not physiological concentrations of systemic melatonin are used. Meta-analytic investigation with a great heterogeneity concerning also dosage and time of administration has shown that the soporific effect of melatonin is modest. In one meta-analysis with a total number of 284 subjects (mainly healthy volunteers or with insomnia only), exogenous melatonin led to a reduction of sleep onset latency of 4 min and an increase in sleep efficiency (total sleep time/time in bed) of 2% and of total sleep time of 13 min (Brzezinski et al., 2005). In a more recent meta-analysis of almost 1700 patients with primary insomnia, a reduction in sleep onset latency of 7 min and an increase in total sleep time of 8 min were found (Ferracioli-Oda et al., 2013). However, the effect of exogenous melatonin treatment was strong enough to show improved sleep by means of actigraphy in a recent study on 36 type 2 diabetic patients in a randomized, double-blind, crossover study (Garfinkel et al., 2011) and as determined by polysomnography in 16 hypertensive patients treated with beta-blockers in a randomized double-blind, placebo-controlled, parallel-group design (Scheer et al., 2006). In conclusion, our patient numbers might have been too small to detect any statistically significant differences. Alternatively, melatonin might only be soporific at nighttime when sleep is impaired (Macchi and Bruce, 2004). The latter is also supported by the reports of a successful treatment of those pinealectomized patients who have sleep problems (Etzioni et al., 1996; Jan et al., 2001; Lehmann et al., 1996; Petterborg et al., 1991). In one case, the successful melatonin treatment could even be discontinued and sleep remained stabilized (Quera-Salva et al., 2011).
We did not detect any significant changes in sleep architecture, although 2 single case studies had reported on increased REM sleep after pinealectomy (Kocher et al., 2006; Krahn et al., 2002). There was an indication that pharmacological doses of exogenous melatonin increase REM sleep in patients with REM sleep behavior disorder (RBD) and in patients with disturbed REM sleep due to unselected neuropsychiatric disorders (Kunz et al., 2004). However, more systematic studies have shown that sleep architecture was unchanged in patients who received evening melatonin for successful treatment of a delayed sleep phase syndrome (Nagtegaal et al., 1998) and in a double-blind placebo-controlled trial of patients with RBD and in a double-blind trial of healthy volunteers and patients with insomnia (James et al., 1987; James et al., 1990; Kunz and Mahlberg, 2010; Zhdanova et al., 2001). In the study on 3 patients after cervical spinal cord injury, an increased REM sleep latency was shown (Scheer et al., 2006). However, in the control group, after thoracic spinal cord injury, REM sleep latency was particularly short (220 min vs. 34 min, p = 0.04). In the 10 patients who received atenolol for melatonin depletion, the amount of REM sleep was reduced acutely by 25% (Van Den Heuvel et al., 1997). However, considering the effect of noradrenaline on sleep, atenolol has a more general effect on sleep as well (Betts and Alford, 1985).
Activity-and-Rest Rhythm
Compatible with the PSG data, we could not observe any irregularity or shift of the activity-and-rest rhythm after pinealectomy. Although we did only qualitatively judge actimetry and sleep log data, our study is the first assessment of a number of consecutive patients. Previous single case studies reported on sleep-wake rhythm irregularity assessed by actimetry in 1 patient and by parental sleep logs in a 14-year-old boy (Quera-Salva et al., 2011). Both patients underwent not only pinealectomy but also adjuvant therapies (radio- and chemotherapy).
Conclusions and Future Directions
Our study is the first prospective evaluation of salivary evening melatonin profiles and polysomnographically recorded sleep related to pinealectomy in humans. We did not find a systematic effect on standard variables of sleep, although salivary evening melatonin levels were diminished below the threshold of 3 pg/mL. Our study expands on previous work that showed deterioration of sleep and circadian rhythm or hypersomnia in selected, retrospectively evaluated patients. It is in line with studies that have shown a modulatory rather than a regulatory role of melatonin in humans in the immune system, the cardiovascular system, and reproduction, as well as have shown that pineal melatonin depletion has no effect on diurnal variation of growth hormone, cortisol, adrenocorticotropic hormone, and thyroid-stimulating hormone (Kocher et al., 2006; Macchi and Bruce, 2004; Murata et al., 1998; Zeitzer et al., 2000).
Pineal melatonin is embedded in a complex network of circadian regulation that includes the central oscillator in the hypothalamic SCN as well as many other central nervous system and peripheral oscillators and pineal but also extrapineal sites of melatonin production. To delete only one output signal of this complex network does not seem to have any major acute effect on sleep. In the long term, particularly when other factors are involved, it might contribute to a clinically relevant sleep problem.
Although pinealectomy is rarely performed, our investigations are important to thoroughly balance potential advantages and disadvantages of pinealectomy before intervention.
Future studies should be conducted multicentrally to increase patient numbers to detect potential subtle effects and for the systematic analysis of an effect of melatonin treatment in those patients with postoperative sleep problems. Long-term follow-up data would be helpful. Macchi et al. (2002) suggested that pinealectomized humans might be less “seasonal.” The existence of some photoperiodic responses in humans is indicated by studies of others who demonstrated an increased duration of nightly melatonin secretion in winter and a phase advance in summer in humans in temperate and polar regions (Wehr, 2001). As can be seen from totally blind people, the main contribution of endogenous melatonin is the stability of the sleep-wake rhythm. Roth et al. (2015) used the day-to-day variability of sleep onset/offset and sleep latency as a marker for this. Another marker that was used by them and that is highly dependent on the circadian variation of melatonin is the number of daytime naps (Lockley et al., 1999; Roth et al., 2015). A quantitative analysis of the actigraphy and sleep log data after the subjects had been under a more standardized protocol of daily routines would be useful for this purpose. Sleep spectral analysis might show more subtle changes: in rats, the only difference observed in pinealectomized animals was a significant decrease in theta power during REM sleep episodes (Fisher and Sugden, 2010). Sleep spindle activity is a potent marker of circadian variation that correlates with the physiological variation of circulating melatonin (Jan et al., 2009). Alternatively, a more detailed analysis of subjective estimates of sleep (e.g., separate components of the PSQI; Buysse et al., 1989) might be helpful in future studies. These might be more sensitive to the restorative aspect of sleep rather than sleep quantity. Preservation of a physiological circadian rhythm of cortisol and adrenocorticotropic hormone levels has been shown in melatonin-depleted pinealectomized subjects and after cervical spinal cord injury, which was the reason why we did not use it as a marker (Kocher et al., 2006; Macchi and Bruce, 2004; Murata et al., 1998; Zeitzer et al., 2000). Others used the circadian variation of core body temperature to show a stabilization of the rhythm by melatonin (Gubin et al., 2006; Kocher et al., 2006).
Footnotes
Acknowledgements
We thank Ingeborg Schlenker for her excellent administrative assistance.
Author Contributions
All authors have contributed to this study in a manner to justify authorship. H.S. performed literature search, figures, study design, data collection, data analysis, and data interpretation and drafted the manuscript. L.R., Z.V., and C.P. participated in data collection and data analysis. M.B., J.L., and B.M. revised the manuscript and corrected the final version. M.S., M.W., and S.K. were responsible for study design, study supervision, and data interpretation and revised the manuscript.
Conflict of Interest Statement
The author(s) have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.