
Abstract
The dim light melatonin onset (DLMO) is the most reliable measure of central circadian timing in humans. However, it is not always possible to measure the DLMO because sample collection has to occur in the hours before usual sleep onset, it requires staff support and considerable participant effort, and it is relatively expensive. Questionnaires that ask people about the timing of their behavior, such as their sleep, may provide an easier and less expensive estimate of circadian timing. The objective of this analysis was to compare the MEQ score derived from the Morningness-Eveningness Questionnaire (MEQ) and the MSFsc derived from the Munich ChronoType Questionnaire (MCTQ) to the DLMO in the largest sample to date (N = 60). Our hypothesis was that MSFsc would correlate more highly with the DLMO than MEQ score. Our sample of 36 healthy controls and 24 patients with delayed sleep phase disorder ranged in age from 18 to 62 years. All participants slept at times of their own choosing for a week before the assessment of their DLMO. The DLMO correlated significantly with both the MEQ score (r = −0.70, p < 0.001) and MSFsc (r = 0.68, p < 0.001). A linear regression using MEQ, MSFsc, and age to predict the DLMO explained 60% of the DLMO variance. The strongest predictor of the DLMO was MSFsc (beta = 0.51, p = 0.001), followed by MEQ (beta = −0.41, p = 0.004), and age (beta = 0.26, p = 0.013). The beta values for MSFsc and MEQ score were not statistically different from each other. Nonetheless, around a 4-h range in the DLMO was observed at a given MEQ score and a given MSFsc, indicating that neither questionnaire should be exclusively used to time light or exogenous melatonin treatment, as this could result in the mistiming of these treatments relative to the DLMO, thereby potentially worsening circadian misalignment.
The most reliable measure of central circadian timing in humans is the onset of melatonin secretion when measured in dim light conditions (dim light melatonin onset, DLMO) (Klerman et al., 2002; Lewy et al., 1999). The DLMO is believed to accurately represent the timing of the central circadian clock (suprachiasmatic nucleus, SCN), as the secretion of melatonin from the pineal gland is controlled by the SCN (Moore, 1996). On average, melatonin levels begin to increase 2 to 3 h before the usual onset of nocturnal sleep (Burgess and Fogg, 2008), but melatonin must be measured in dim light as otherwise its secretion is suppressed by light (Lewy et al., 1980). The DLMO can be obtained noninvasively from half-hourly or hourly saliva samples, collected in the 6 h or so before habitual sleep onset (Burgess and Fogg, 2008). However, it is not always possible to measure the DLMO, because the procedure requires staff support and considerable participant effort, and the melatonin assay is relatively expensive (~$US13 per sample). Thus, there remains a need for low-cost alternatives that can estimate circadian timing with little participant burden and under less artificial conditions.
One alternative is to simply ask people about the timing of their behavior using questionnaires. Several such questionnaires are used in the field and have recently been reviewed in detail (Di Milia et al., 2013). The first was the Morningness-Eveningness Questionnaire (MEQ) (Horne and Ostberg, 1976), which consists of 19 questions that ask people to consider their “feeling best” rhythms and indicate preferred clock time blocks for sleep and engagement in various hypothetical situations (e.g., physical exercise, tests, work), in addition to assessing morning alertness, morning appetite, evening tiredness, and alarm clock dependency. Thus, the MEQ score can be considered as a psychological preference for behavior (diurnal preference) (Di Milia et al., 2013). MEQ scores can range from 16 to 86, with lower scores indicating evening types and higher scores indicating morning types. The Munich ChronoType Questionnaire (MCTQ) (Roenneberg et al., 2003) instead focuses primarily on sleep timing and with 14 questions assesses the regularity of one’s work schedule, number of workdays per week, sleep timing on workdays and work-free days, and alarm clock use on workdays and work-free days. Chronotype is estimated as the midpoint of sleep on work-free days minus half of the difference between sleep duration on work-free days and average sleep duration of the week to control for sleep debt (midpoint of sleep on work-free days, sleep-corrected, MSFsc). Thus, the MSFsc is in essence a subjective report of sleep timing (Di Milia et al., 2013). Importantly, MSFsc can only be calculated when individuals do not use an alarm clock on work-free days (Roenneberg et al., 2012). Previous work compared the MEQ score with midpoint of sleep on work-free days (MSF) (not MSFsc) in a large sample of mostly Dutch students (N = 2481) and found reasonable convergence (e.g., r = −0.73) (Zavada et al., 2005).
Only one study to date has compared the MEQ, MCTQ, and the DLMO in the same individuals (Kitamura et al., 2014). The initial sample consisted of 44 middle-aged to older Japanese adults (34-68 years) of both sexes. The working status of the subjects was not reported. The DLMO was determined from hourly saliva samples that the subjects collected unsupervised in their homes. Seven subjects had undetectable DLMOs, resulting in a final complete sample of 37 individuals. Relatively early ranges of MEQ scores (~41-76), MSFsc (~0.5-5.0 h), and DLMOs (~1830-2400 h) were observed (Figure 2 in Kitamura et al., 2014). Indeed, there were some very early sleepers in the sample, with ~20% reporting MSF of 0200 h or earlier. If one assumes a sleep episode of 8 h, this sleep timing corresponds approximately to 20% of the sample sleeping 2200 to 0600 h or even earlier on work-free days. Results indicated a stronger association between MSFsc and the DLMO (r = 0.54, p < 0.001) than between the MEQ and the DLMO (r = −0.40, p = 0.055). These results suggest that MSFsc derived from the MCTQ better reflects endogenous circadian timing compared with the MEQ score. However, the results should be interpreted with caution as unsupervised saliva collection at home with no measures of compliance to procedures can result in inaccurate DLMOs (Burgess et al., 2015). Thus, the objective of our study was to compare the MEQ score and MSFsc to the DLMO in a larger sample (N = 60) with a broader range in MEQ score, MSFsc, and DLMO. Additionally, all of the DLMOs were collected in more controlled sampling conditions (Burgess et al., 2015; Crowley et al., 2015; Burgess et al., unpublished data collected in 2012–2013). Our hypothesis was that as observed by Kitamura et al. (2014), MSFsc would correlate more highly with the DLMO than MEQ score.
Our sample consisted of not only healthy controls (n = 36) but also individuals diagnosed by a board-certified sleep clinician with delayed sleep phase disorder (DSPD) as per ICSD-2 criteria (American Academy of Sleep Medicine, 2005) (n = 24). There were 31 women (10 women with DSPD) and 29 men (14 men with DSPD) in the final sample, and age ranged between 18 and 62 years. The sample was also varied in terms of work status (27% not working, 30% part-time workers, and 43% full-time worker). All subjects slept at times of their own choosing for a week before the assessment of their first DLMO, but alarm clock use was not recorded on a daily basis. All subjects included in the final analysis reported not using alarm clocks on their work-free days.
The first baseline DLMO assessed in each research protocol was selected for this analysis, such that the DLMO was not influenced by any research protocol intervention (Burgess et al., 2015; Crowley et al., 2015; Burgess et al., unpublished data collected in 2012–2013).All subjects refrained from caffeine and alcohol in at least the 24 h before saliva collection, refrained from nonsteroidal anti-inflammatory drugs for at least 72 h before saliva collection, and passed a urine drug test. The baseline DLMOs were carefully assessed either in the laboratory (n = 39) according to standardized procedures (Burgess et al., 2015; Crowley et al., 2015) or at home (n = 21) with objective measures of light exposure (photosensors) and sample timing to confirm the validity of each home DLMO (Burgess et al., 2015). Home DLMOs that were verified as valid using objective measures of light exposure and sample timing were highly correlated with laboratory DLMOs (r = 0.91, Burgess et al., 2015). Saliva samples were collected at half-hourly intervals starting 6 or 7 h before the average weekly bedtime and continuing until 2 or 3 h after average weekly bedtime (Burgess et al., 2015; Crowley et al., 2015). The saliva samples were radioimmunoassayed by Solidphase Inc (Portland, ME) using a commercially available kit (ALPCO Inc, Salem, NH) (Burgess et al., 2015; Crowley et al., 2015). The DLMO was calculated as the clock time (with linear interpolation) when the melatonin concentration exceeded the mean of 3 low consecutive daytime/early evening values plus twice the standard deviation of these points (Voultsios et al., 1997). This low threshold more closely tracks the initial rise of melatonin, when the SCN triggers the release of melatonin from the pineal gland (Molina and Burgess, 2011). The Rush University Medical Center Institutional Review Board approved all of the study protocols from which the data were pooled, and the study protocols followed the principles of the Declaration of Helsinki. All subjects gave written informed consent prior to participation. All data were analyzed using IBM SPSS Statistics Version 22.
The baseline distributions of the MEQ, MSFsc, and DLMO are shown in Figure 1. All variables were normally distributed (Kolmogorov-Smirnov test p > 0.05). There was slight positive skew in MSFsc and the DLMO, but this did not warrant transformation. Kitamura et al. (2014) also did not transform their data. The ranges in MEQ (20-69), MSFsc (3.0-9.7 h), and DLMOs (1830-0238 h) were larger than those observed by Kitamura et al. (2014). Our subjects, in addition, slept later on their work-free days, with reported sleep onsets on work-free days ranging between 2300 and 0530 h, and they reported wake-up times on work-free days ranging between 0645 and 1500 h. The DLMO correlated significantly with both the MSFsc (r = 0.68, p < 0.001) and the MEQ (r = −0.70, p < 0.001), as shown in Figure 2. Additionally, a linear regression analysis (enter method) using MEQ, MSFsc, age, and sex to predict the DLMO explained 60% of the variance in the DLMO (p < 0.001). The strongest significant predictor of the DLMO was MSFsc (beta = 0.51, p = 0.001), followed by MEQ (beta = −0.41, p = 0.004) and age (beta = 0.26, p = 0.013). Sex was not a significant predictor of the DLMO (beta = 0.00, p = 0.99). The beta values for MSFsc and MEQ score were not statistically different from each other (p = 0.84). Applying additional linear regression analysis using the backwards or forward method did not substantially alter these findings.
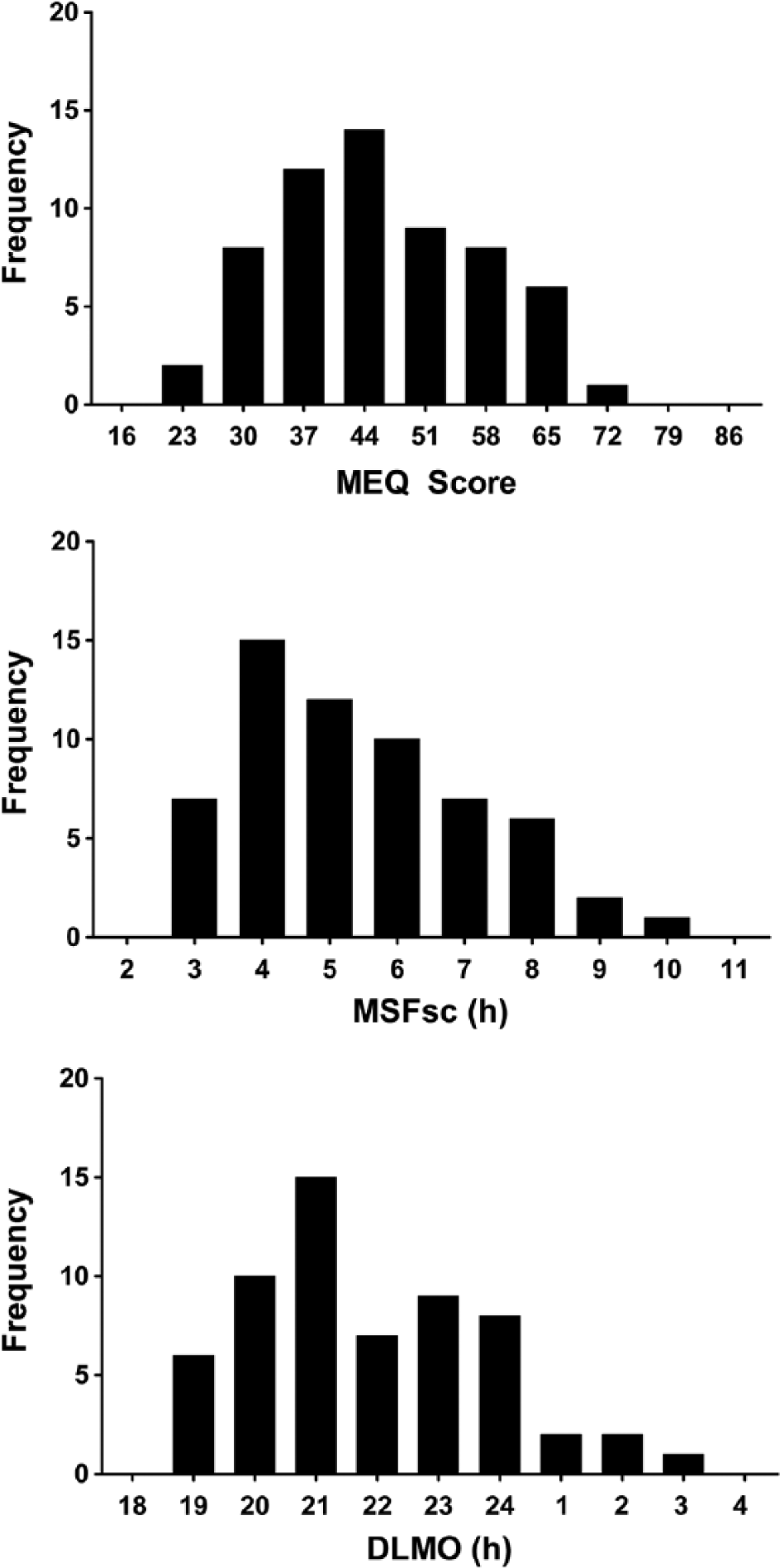
Frequency histograms of MEQ, MSFsc, and DLMOs calculated from the final sample of n = 60.
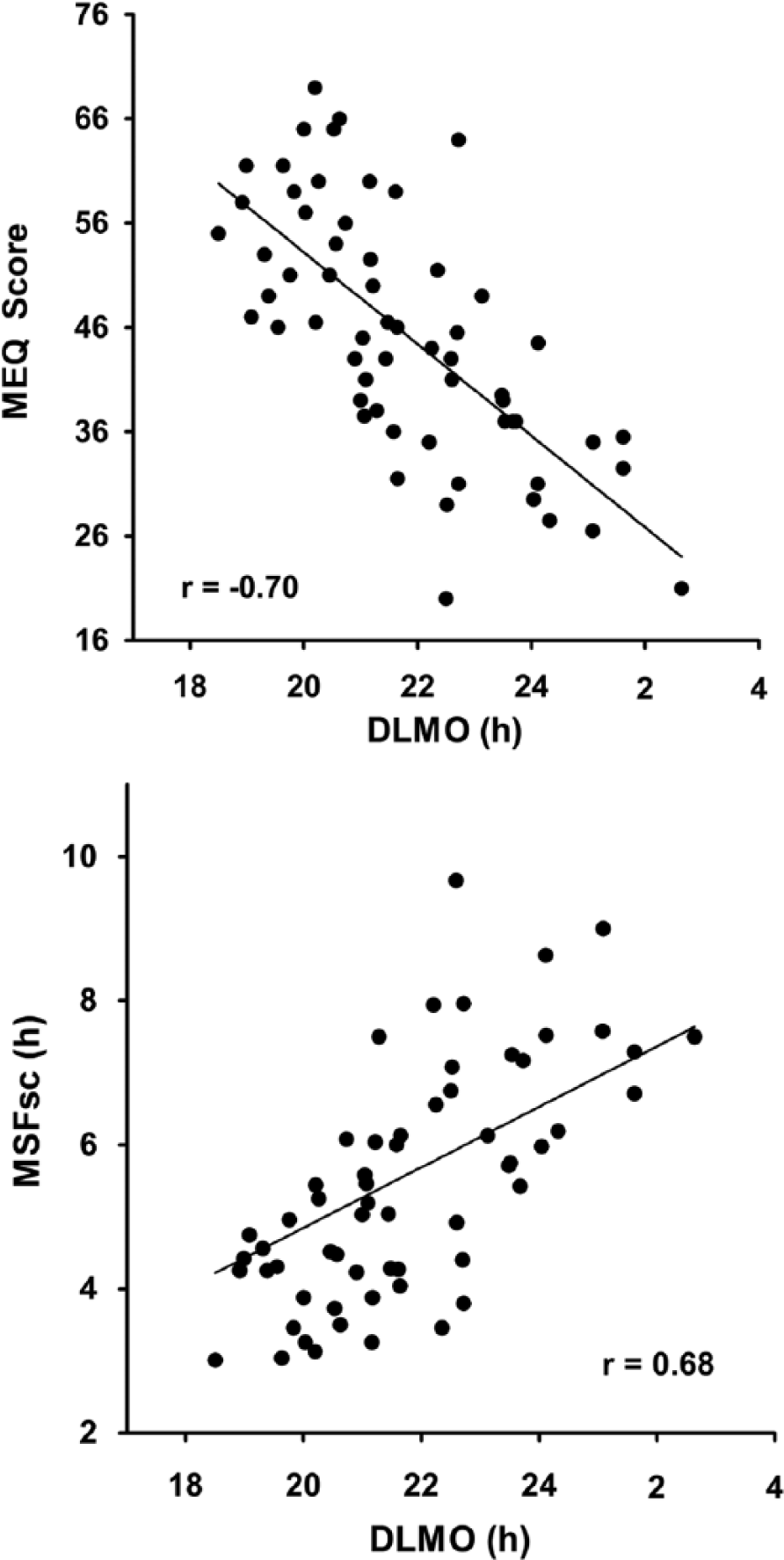
Associations between the MEQ and DLMO and between the MSFsc and DLMO in the final sample of N = 60. The solid line represents the linear associations between each pair of variables. Both correlations were statistically significant (p < 0.001).
These results indicate that MCTQ-derived MSFsc (chronotype) may be a slightly better proxy measure of central endogenous circadian timing as measured by the DLMO, compared with the MEQ score. This finding is consistent with the interpretation of the MEQ as a psychological preference for behavior, whereas MSFsc is a subjective report of sleep timing (Di Milia et al., 2013). We have previously found that sleep timing, objectively verified with wrist actigraphy, in young adults sleeping at times of their choosing (as opposed to study protocol mandated times), correlates highly with the DLMO (e.g., sleep midpoint and DLMO, r = 0.69, p < 0.001; Burgess and Eastman, 2005). This close association between sleep timing and the DLMO makes intuitive sense, as sleep (eyes closed) gates exposure to environmental light, which is the strongest entraining signal to the circadian clock. Indeed, shifting bedtime (with light outs) or wake-up time shifts the DLMO, presumably due to the accompanying shift in light exposure (Burgess and Eastman, 2004, 2006). Thus, perhaps by focusing primarily on sleep timing, the MSFsc measure somewhat more closely tracks endogenous circadian timing. Nonetheless, one key point is that while both MEQ score and MSFsc significantly predicted the DLMO, around a 4-h range in the DLMO can be seen at a single MEQ score (e.g., MEQ score of 46 in Figure 2) and at a single MSFsc (e.g., MSFsc of 4 in Figure 2). This indicates that neither the MEQ score nor MSFsc should be used solely to time light or exogenous melatonin treatment, as this could result in the mistiming of these treatments relative to the DLMO, thereby potentially worsening circadian misalignment.
There are some limitations to our study. We included data from DSPD patients to broaden the range in the MEQ score, MSFsc, and DLMO and to increase our sample size. Without the DSPD patients, our sample of healthy controls is smaller than that in Kitamura et al. (2014), with the additional loss of statistical power. Thus, the relationships observed between these variables in our sample may not generalize to other samples without more extreme chronotypes. We also found in our sample that we could not derive the MSFsc from the MCTQ in subjects who reported using an alarm clock on work-free days (Roenneberg et al., 2012), causing us to lose 13 subjects from our original sample. Seventy percent of these 13 subjects woke at 0900 h or later on work-free days, suggesting that MSFsc may be harder to assess in later chronotypes. There may also be some people who set an alarm clock on their work-free days but actually wake prior to their alarm. These people may indicate “woke with an alarm clock on work-free days” on the MCTQ, when in fact they woke prior to the alarm, and thus in principle could have their chronotype calculated.
Furthermore, the hand scoring of both the MEQ and MCTQ can be time consuming and somewhat complicated; to avoid errors, we recommend that automated scoring be used. The MCTQ can be completed online, or alternatively automated scoring can be generated from the scoring rules provided previously (Roenneberg et al., 2012). A further advantage of the MCTQ is that it can be used to calculate social jetlag, the difference between the timing of midsleep on work days and work-free days (Wittmann et al., 2006). Social jetlag represents chronic circadian misalignment, and because social jetlag is associated with depression, cardiometabolic health, health behaviors, and academic performance, it is a useful additional circadian measure to extract from the MCTQ (Kantermann et al., 2013; Levandovski et al., 2011; Roenneberg et al., 2012; van der Vinne et al., 2015; Wittmann et al., 2010). Thus, if one is forced to pick between the MEQ or the MCTQ due to concerns about subject burden and time taken to complete questionnaires, we recommend the MCTQ because (1) our results suggest that MSFsc is a slightly better proxy of central endogenous circadian timing than MEQ score, (2) the MCTQ also permits the calculation of social jetlag, and (3) the MCTQ consists of only 14 questions compared with 19 questions in the MEQ. Future work should continue to examine the relationships between circadian questionnaires and the DLMO in large representative samples (Di Milia et al., 2013). Our sample was one of convenience and is not necessarily representative of the general population, particularly as DSPD patients were included.
Footnotes
Acknowledgements
This research was supported by National Institute of Health R01 grants HL083971 and AT007104 to HJB. TK is supported by the Technology Foundation STW grant P10-18/12186. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.