
Abstract
Workers involved in crushing, milling, screening, and bagging of mica scrap are at increased risk to develop pneumoconiosis, a progressive material overloading of the lung that can lead to fibrosis and, in the later stages, to dyspnea. Pneumoconiosis is only seen after 10–20 years of respiratory mica exposure, and it can have a latency period of up to 40 years—today’s cases date back to exposures during the second half of the 20th century. An occupational lifetime exposure level of 3 mg/m3 respirable mica dust has been considered to present no risk of pneumoconiosis since 1951 when the American Conference of Governmental Industrial Hygienists (ACGIH) established a 20 million particles per cubic foot (mppcf) (3.5 mg/m3 respirable particles) exposure limit. As a result, numbers of unspecified and other pneumoconioses in the United States have steadily declined since the early 1970s. Data from the National Institute for Occupational Safety and Health documents a 91% decrease between 1972 and 2014 (i.e., the peak of documented cases and the latest reported data) for combined cases of aluminosis, berylliosis, stannosis, siderosis, and fibrosis from production and use of bauxite, graphite fibers, wollastonite, cadmium, Portland cement, emery, kaolin, antimony, and mica. Ample evidence indicates that the 70-year-old occupational lifetime exposure level of 3 mg/m3 respirable mica dust is protective of workers’ health.
Introduction
Occupational exposure limits for mica.
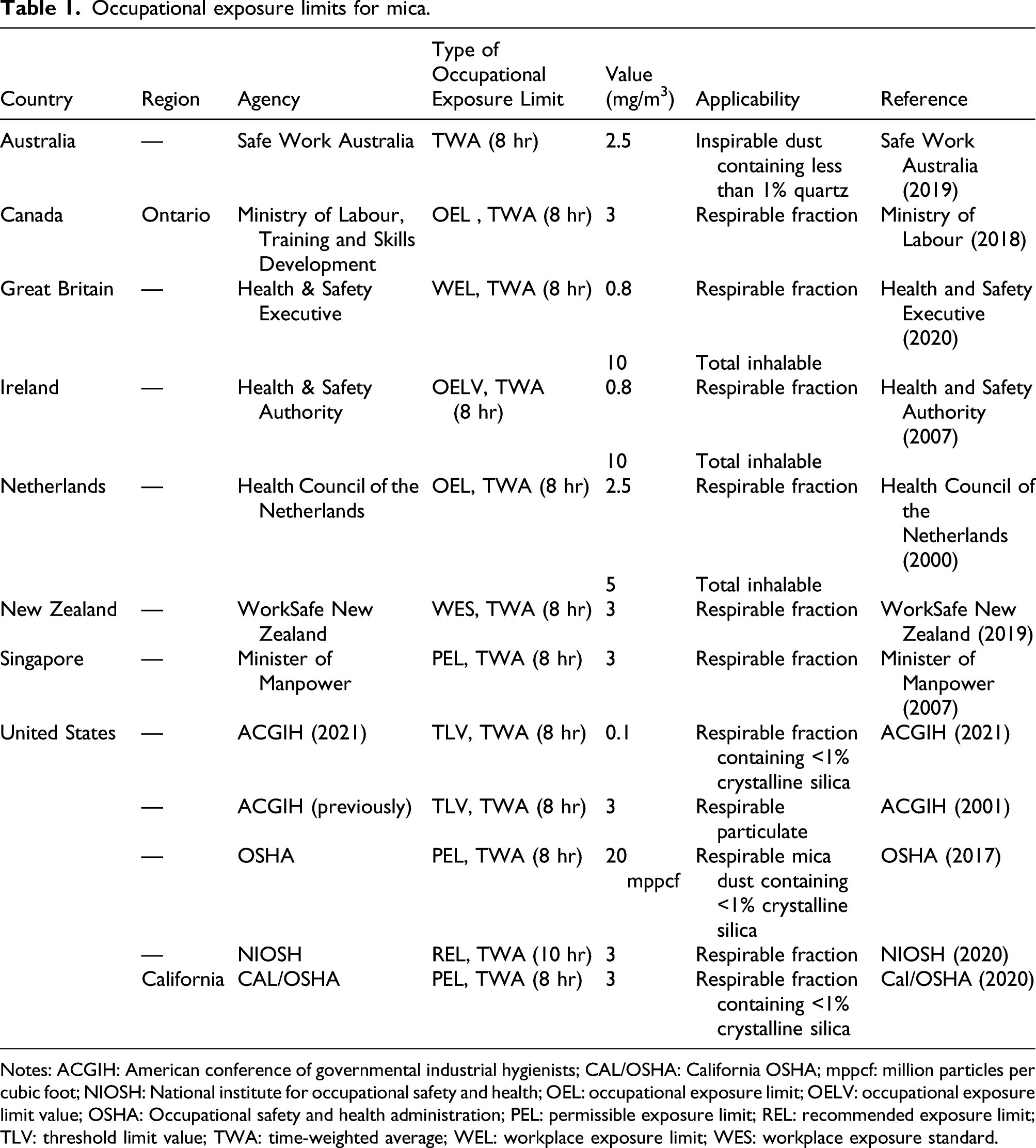
Notes: ACGIH: American conference of governmental industrial hygienists; CAL/OSHA: California OSHA; mppcf: million particles per cubic foot; NIOSH: National institute for occupational safety and health; OEL: occupational exposure limit; OELV: occupational exposure limit value; OSHA: Occupational safety and health administration; PEL: permissible exposure limit; REL: recommended exposure limit; TLV: threshold limit value; TWA: time-weighted average; WEL: workplace exposure limit; WES: workplace exposure standard.
Methods
U.S. mining records for mica from the U.S. Geological Survey were reviewed and compared to mortality records of the National Institute of Occupational Safety and Health (NIOSH) (NIOSH 2017a) where unspecified pneumoconiosis was identified as a contributing or underlying cause of death. Sheet mica production was excluded from consideration because it does not involve the primarily dust-generating steps of crushing, milling, screening, and bagging. In addition, a literature review was conducted for respiratory health effects in workers globally who were occupationally exposed to mica dust. The literature cited in the American Conference of Governmental Industrial Hygienists’ (ACGIH) historical decision to justify an exposure limit of 3 mg/m3 respirable fraction as well as that in the 2021 ACGIH publication of the lowered threshold limit value over a time-weighted average (TLV-TWA) of 0.1 mg/m3 respirable mica dust was reviewed. All scientific publications were assessed for reliability, temporality, exposure information, potential or reported compounding co-exposures to other mineral dusts, and nature and severity of effects.
Results
In 1951, ACGIH published a 20 million particles per cubic foot (mppcf) exposure limit for mica dust. This equals approximately 3.5 mg/m3 respirable particles, using an empirical conversion factor of 5.65 mppcf = 1 mg/m3 by Tomb and Haney (1988), also used by ACGIH (2021). That year, the U.S. production of scrap and flake mica was 63,600 t. Mica production more than doubled over the next 30 years, and it reached its peak at 132,000 t in 1984. Production of mica started to decline in the following years falling to 35,000 t in 2020 (U.S. Geological Survey, online only).
NIOSH (2020) has been tracking work-related respiratory diseases among other endpoints dating back to 1968. Respiratory diseases specific to production and use of minerals such as asbestosis, coal worker pneumoconiosis, byssinosis, and silicosis are singled out, whereas “unspecified and other pneumoconiosis” refers to pooled data on aluminosis, berylliosis, stannosis, siderosis, and fibrosis from production and use of bauxite, graphite fibers, wollastonite, cadmium, Portland cement, emery, kaolin, antimony, and mica. Figure 1 shows a dramatic decline of the pooled total numbers of unspecified and other pneumoconioses after the peak at 1548 cases in 1972. This steep decline occurred 21 years after the ACGIH’s 20 mppcf limit, or 26 years after the first ACGIH exposure limit for mica. This duration is approximately when the protective effects of implemented exposure controls could be expected to manifest, a delay based on induction period and latency period. However, any assessment of a correlation would have to consider other confounding factors and other environmental exposures. Annual U.S. production volume of mica (U.S. Geological Survey, 2021) and unspecified and other pneumoconiosis as underlying or contributing causes of death, U.S. residents age 15 and over, 1968–2004 (NIOSH 2017a).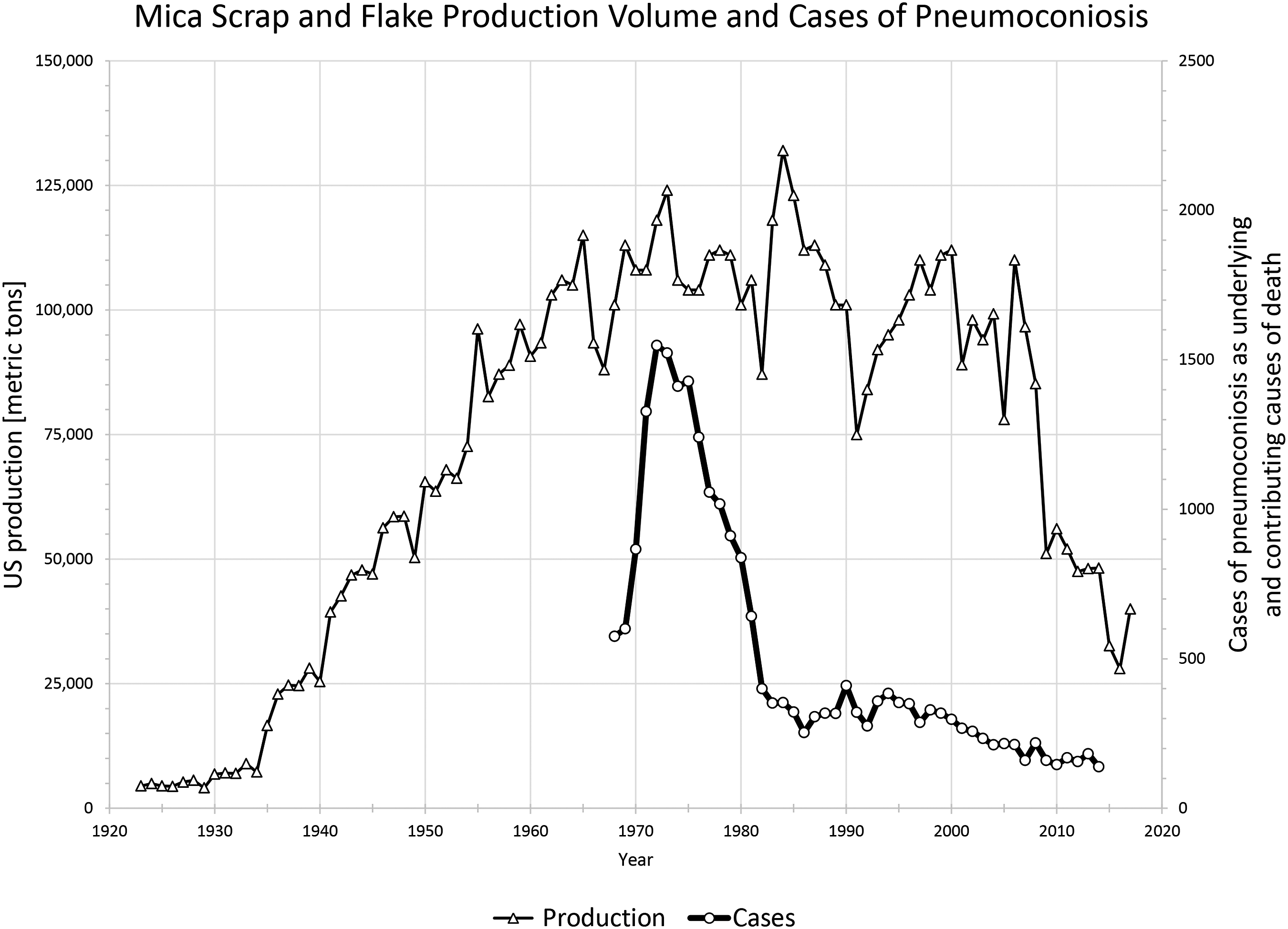
While pneumoconiosis was identified as a contributing or underlying cause of death, it is further of note that this is not necessarily indicative of impaired respiratory function during the workers’ lifetimes, and the average median age of the deceased workers was 79.6 ± 1.4 years between 1995–2014 (calculated from NIOSH 2007 and NIOSH 2017b). This is equivalent to the overall life expectancy in the United States of 78.8 years in 2014 (Kochanek et al., 2016). As the U.S. Centers for Disease Control and Prevention also remarked in the Morbidity and Mortality Weekly Report 17 years ago (CDC 2004), “new technologies such as computed tomography are used increasingly, resulting in increased diagnostic sensitivity for pneumoconiotic diseases.” Despite this improvement in diagnostics, reported cases have continued to fall. The latest reported number of all combined unspecified and other pneumoconiosis was 139 U.S. workers in 2014. Even with a significant increase in mica production in prior decades and taking the long latency period for disease manifestation into account, the rates of pneumoconiosis declined (Figure 1). Mica production makes up a fraction of 1% of the sum of the other elements and minerals that are listed as co-contributors to the “unspecified and other pneumoconiosis” cases (data not shown, fraction calculated from production statistics on respective elements and minerals published by the U.S. Geological Survey, online only).
With general pneumoconiosis being the well-established occupational hazard of respiratory exposure to mica dust, any review of safe occupational exposure levels should focus more on dose response assessment than on hazard identification.
Among the refinements of safe mica levels in air, a most fundamental action is to distinguish the adverse effects of mica from those of other, potentially co-occurring minerals. Specifically, the occurrence of silicosis was considered to be unique and different from mica-based pneumoconiosis, as it could dominate disease development, progression, and complications at lower exposure levels than mica. This important scrutiny was part of the first ACGIH exposure limit in 1946, when ACGIH stipulated a < 5% free silica content in mica dust when the (then) maximum allowable concentration over a TWA for mica was set at 50 mppcf. A reduction of allowable crystalline silica/quartz levels to < 1% was implemented with the subsequent lowering of the TLV-TWA for mica to 20 mppcf. The later 1984/1986 revision of the mica TLV-TWA was not a meaningful lowering of the allowable mica levels in air per se. Rather, it was a unit conversion from number of inhalable particles per volume (20 mppcf mica) to units of respirable mass per volume (3 mg respirable mica/m3). Thus, 3 mg/m3 respirable mica dust has been considered a safe occupational lifetime exposure level since ACGIH established its 20 mppcf (= 3.5 mg/m3) value in 1951.
The 3 or 3.5 mg/m3 standard was set so long ago that its occupational health benefit is clearly obvious today and has been for the past 50 years, even considering that pneumoconiosis is only seen after 10–20 years of exposure and with a latency period of up to 40 years (ACGIH, 2021).
Discussion
Silicosis is a particularly progressive form of fibrotic pneumoconiosis that is histopathologically distinguishable from other pneumoconioses (Chong et al., 2006). The International Agency for Research on Cancer concluded that “Crystalline silica inhaled in the form of quartz or cristobalite from occupational sources is carcinogenic to humans (Group 1),” and, in addition, silicosis carries an increased risk for silicotuberculosis (IARC 2009). As outlined above, ACGIH was an early proponent that toxicity from inhaled crystalline silica minerals carries unique risks for mica workers who are co-exposed. As a logical consequence, any and all case reports, occupational studies, and/or epidemiological assessments that describe or examine mica dust exposures with co-exposures of crystalline silica minerals at or above the ACGIH TLV-TWA of 0.025 mg/m3 should only be used for mica risk assessment or threshold setting after a thorough assessment of the potential confounding effects of such circumstantial co-exposures. Notably, ACGIH (2001) identified the compromising nature of a publication with such co-exposures (i.e., Vestal et al., 1943), and Vestal et al. was the only previously used publication that was not also referenced by ACGIH in 2021. Regrettably, however, ACGIH (2021) introduced newer studies that were compromised for the same reasons (Algranti et al., 2005; Landas and Schwartz, 1991; Raymond, 2014). Respective studies were used by ACGIH (2021) but dismissed from consideration in this review because they must not contribute to a risk assessment for respiratory exposure to mica only. The same applies to studies that did not investigate historical or current co-exposures (i.e., the mere absence of information does not confirm the absence of crystalline silica). Lastly, ACGIH (2021) introduced studies that might be used for hazard identification, but they lack exposure information and/or describe isolated cases that lack statistical significance. Specifically, the publication by Davies and Cotton (1983) lacks exposure information, and the report covers only two individuals; the publication by Skulberg et al. (1985) lacks exposure information, both quantitative and regarding particle size distributions; the publication by Zinman et al. (2002) lacks exposure information for the single individual who was described; the publications by Kobayashi et al. (2004) and Venter et al. (2004) lack exposure information; and the publication by Hulo et al. (2013) described four individuals, of which one was lacking exposure data, one refused continued participation in the study, and one showed a radiological finding that was inconsistent with his peers, potentially indicating other confounding factors. Even though ACGIH (2021) is based on all of these studies, they cannot be considered reliable let alone pivotal because of the identified shortcomings.
Considering all publications available and reviewed by ACGIH, Dreessen et al. (1940) is still one of the most authoritative studies on occupational exposures to mica-only dust, albeit with caveats. Dreessen et al. investigated occupational exposure data collected in 1936. While exceptionally scientific for its time, this study has shortcomings that require careful reinterpretations if applied to define safe exposure levels today, 85 years later. Dust concentrations at the studied work environments were measured using the technology that was standard in the early 1930s (Bloomfield and Dalla Valle, 1935). Considering the progress of quantitative analytical capabilities over the past century, it is not unreasonable to consider that dust levels might have been underreported by Dreessen et al. The best evidence for underreporting by Dreessen et al. is the dust concentrations at bagging, which can be directly compared to the more recent report by Hulo et al. (2013). The highest average dust count reported by Dreessen et al. during machine bagging of mica was equivalent to 9.0 mg/m3 respirable fraction. In comparison, Hulo et al. reported 5.77 mg/m3 respirable dust at the bagging machine. It is extremely implausible that occupational exposure data in a present-day Western European facility is within only twofold of a pre-World War II mining and grinding operation. This common sense level of skepticism is further supported by a publication documenting the decline of respirable dust concentrations within the European minerals sector even as recent as the beginning of the 21st century (Zilaout et al., 2020).
Without outlining each individually reviewed scientific article used by ACGIH in detail, the Dreessen et al. study plays a key role in the determination of a safe exposure level in addition to the fundamental considerations of production volume and occupational disease rates in the U.S., as discussed above. Dreessen et al. state “Above 10 million dust particles per cubic foot, the percentage of workers found to have silicosis or pneumoconiosis increases with increasing dust concentration and with increasing length of employment. Below 10 mppcf no cases were found during the periods of employment represented in this study” (10 mppcf = 1.8 mg/m3). They further note that “No cases of pneumoconiosis were found among 31 men and 78 women engaged in fabricating sheet mica under conditions that generated approximately three million dust particles per cubic foot” (3 mppcf = 0.5 mg/m3). These consistent findings suggest a no-effect level at or above 1.8 mg/m3 respirable fraction—it is not unlikely that these air concentrations were underreported. The absence of other, reliable no-observed-adverse-effect level data in the literature further leads to the conclusion that the Dreessen et al. publication is pivotal.
Scientific evidence, including documentation used by ACGIH, suggests that mica-induced pneumoconiosis is due to lung overload (Hulo et al., 2013). Lung overload is hypothesized to be a threshold phenomenon, where the capacity of alveolar macrophage-mediated clearance is exceeded. Mica particles are not water soluble, are nonreactive, and are of low toxicity (Commission of the European Communities, 1988). As such, mica’s occupational exposure limits should be aligned with those for Particles (Insoluble) Not Otherwise Specified (PNOS), “Inert” dusts, Nuisance dusts, or Particulates Not Otherwise Regulated (PNOR) (e.g., Occupational Safety and Health Administration permissible exposure limit TWA of 5 mg/m3 [resp]) (NIOSH, 2019).
Conclusions
The ACGIH’s allowable respirable particulate fraction of mica in air remained essentially unchanged since 1951. In 2021, however, ACGIH reduced the mica TLV-TWA from 3 mg/m3 respirable fraction to 0.1 mg/m3. Most scientific studies specified by ACGIH (2021) as supporting evidence did not withstand scientific scrutiny for a dose-response assessment because of unaccounted for co-exposures to silica and other dust, non-quantified mica exposure levels, and—for case reports with limited numbers of subjects—the lack of statistical power and disproportional impact of possible idiosyncratic reactions, unique exposure histories, or other compounding factors regarding individual patients. In contrast, this larger scope review of worker health monitoring data, mining records, and the scientific literature concludes that the previous 70-year-old TLV-TWAs of 3–3.5 mg/m3 respirable fraction were scientifically justified and protective of workers’ health. This is consistent with occupational exposure limits by competent authorities globally. Data from NIOSH (2007) documents a steady decline in numbers of unspecified and other pneumoconioses in the United States since the 1970s. American Conference of Governmental Industrial Hygienists’s scientific rationale behind the 30-fold lowering of the TLV-TWA in the absence of compelling new data or new understandings of historical data remains unclear, regrettably because of the lack of transparency and scientific dialog around the ACGIH process, which has been criticized in the past (Smith and Perfetti, 2019; Ziem and Castleman, 1989). Health-effect data in U.S. workers, like the NIOSH data used in this review, has long been postulated to be used for TLV setting (Ziem and Castleman, 1989).
In conclusion, the process of setting occupational exposure limits should not be limited to the peer-reviewed literature but rather should also include the use of legitimate workplace safety data in the context of production volumes, historical regulatory limits, and time (exposure duration and latency). In the present case of a safe occupational exposure level for mica, a broad weight of evidence approach scrutinizing the primary literature and going well beyond it demonstrates that there is ample evidence that an occupational exposure limit of 3 mg/m3 respirable fraction mica is protective of workers’ health, and no evidence suggesting that it should be lower.
Footnotes
Acknowledgments
The authors thank Mr Mark Ellis with the Industrial Minerals Association – North America for sponsorship of this research project. Further thanks go to Ms Monica Carstens for her constructive help and thorough review of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This assessment was funded by the Industrial Minerals Association – North America.