
Abstract
As the world celebrates unprecedented advancements in medical technology, such as personalized medicine and gene editing, actors in health markets face growing pressure to ensure that these high-cost treatments are distributed in ways that are moral, fair, and inclusive. Achieving this goal requires more than expanding consumer access to treatments: Public and private stakeholders must develop a deeper understanding of the sociocultural factors that shape consumer inclusion. One such factor is consumer competence, which has been defined in literature as an individual's ability to mobilize knowledge, skills, and resources in using products and services to accomplish their life projects (Longo 2014).
Thus understood, consumer competence is often interpreted as a static indicator of how capable a consumer is of mobilizing and combining resources in ways that are meaningful within their lived environments and available opportunities. The limits of this individual and static view are that perceived (in)competence is often used to classify consumers as deserving or undeserving of treatments. When market access policies are implemented, consumer competence risks being reduced to an externally assessed, decontextualized, one-size-fits-all criterion that does not account for the important work of developing competences.
This commentary aligns with Longo's (2014) reconceptualization of consumer competence as a dynamic, socioculturally embedded practice that is difficult to assess, either internally or externally. It draws on the provision of innovative medical technology for the treatment of Type 1 diabetes within the U.K. and Chilean public health systems to argue that marketplace inclusion requires more than evaluations of individual (in)competence to determine access to products. We introduce the concept of near inclusion, in which consumers are promised the prospect of free access to a market resource but are effectively excluded (e.g., when patients qualify to apply for free access to a health technology in principle, but their applications are denied after being assessed).
More than 9.2 million people live with Type 1 diabetes globally (International Diabetes Federation 2025). Through government-led health initiatives, the United Kingdom and Chile have two inclusion programs that provide Type 1 diabetes patients, free of charge, with a smart insulin pump that enables more efficient management of their condition. Smart insulin pumps represent the most advanced glucose-control technology available to people with Type 1 diabetes. Also known as hybrid closed loop (HCL) systems or “artificial pancreas,” this technology comprises a continuous glucose monitor, an insulin pump, and software running on the device or a smartphone. By automating monitoring of glucose levels and insulin delivery, tasks that are typically done manually, the HCL system can significantly reduce the risk of life-threatening hypoglycemic or hyperglycemic episodes (NHS England 2024). This eases patients’ and families’ burden by making diabetes-care routines less stressful and more discreet.
Despite expanding access to this technology, the U.K. and Chilean systems face important challenges in terms of inclusivity. Successful care provision with available technologies is unequally distributed, disadvantaging the most vulnerable patients (Cabieses et al. 2025; Seidu et al. 2025). In principle, all patients with Type 1 diabetes in both countries have access to HCL technology. In practice, however, as demonstrated by recent studies (Cabieses et al. 2025; Seidu et al. 2025), these programs’ complex, multicriteria decision-making process results in many patients remaining excluded. Consequently, consumers who need the products most are often offered only near inclusion: They are promised the prospect of free access to a market resource yet remain practically excluded. In the United Kingdom, “nearly half of those who have tried to get diabetes tech have been refused it at some point” (Diabetes UK 2025).
In the Chilean health system, those who may be struggling with diabetes management due to the lack of adequate support networks or income (e.g., a child with a working single parent who cannot regularly manage the child's glucose levels) may fail to meet the diagnostic criteria that would grant them access to the smart pump. As specified by the Chilean Ministry of Health, patients must demonstrate adherence to diabetes management and adequate blood glucose control to qualify for HCL technology (Ministerio de Salud 2019). Patients must also demonstrate that they have exhausted all available treatment options without achieving adequate control of the illness. Families whose children face the greatest health risks (e.g., those living in remote locations and/or lacking the financial means to purchase treatment) find their children denied access. This happens precisely because the children's diabetes is poorly controlled due to a lack of resources (Cabieses et al. 2025). Similarly, in the U.K. public health system, it has been recognized that “people from socially deprived areas, some ethnic minorities, or those who don’t own smartphones—which are essential for using HCL systems—are at a disadvantage” in obtaining the pump (National Institute for Health and Care Excellence 2023).
Both the United Kingdom's and Chile's public health systems have a carefully designed procedure for pump approval on a case-by-case basis. These procedures include a multidisciplinary team working in authorized specialized centers composed of nurses, doctors, diabetologists, and psychologists that assess the patients and submit a recommendation to an independent panel of experts for final approval. However, their capacity to overcome traditional market inequalities has proven limited. Among the identified reasons for this issue are limitations of the infrastructure available (e.g., distance from specialized clinics with well-trained personnel, availability of mobile phones) and gatekeepers’ perceptions of patients and caregivers as potentially incompetent managers of the technology, with implications for their perceived capacity to benefit from it (Cabieses et al. 2025).
Improvements in infrastructure are essential for successful treatment provision and for leveling the playing field for all patients. Nonetheless, infrastructure improvement will only be effective when the market ecosystem is capable of genuinely including consumers. Thus, it is not only important to provide consumers with the opportunity to acquire resources such as knowledge and administrative support to develop specific abilities (Griffin et al. 2023). It is also necessary to create contexts in which patients and caregivers can “transcend their life circumstances” and orchestrate a provision of care that is anchored in the context of their own daily routines and challenges (Cardoso, Rojas-Gaviria, and Scaraboto 2020, p. 917). As Le Boterf (2008, p. 2, translated and cited by Longo [2014, p. 55]) emphasizes, “the development of competences depends not only upon acquiring resources (knowledge, abilities …) but also being trained in building suitable combinations of them. Competence is, hence, a combination of varied resources that can be put in practice.”
When consumer competence is treated as a perceived prerequisite rather than a supported outcome of consumer inclusion, it risks reproducing structural inequalities by excluding those with the fewest resources and the fewest opportunities to orchestrate those resources into new practices (see Figure 1). Our problematization of the use of competence as a criterion for granting access to life-changing products raises fundamental questions for policymakers and other health market actors. We argue that partnerships among these actors are needed to build a more nuanced view of consumer competence and achieve genuine inclusivity in health markets. To advance in this regard, the role of innovators in health markets must be more strongly recognized and mobilized.
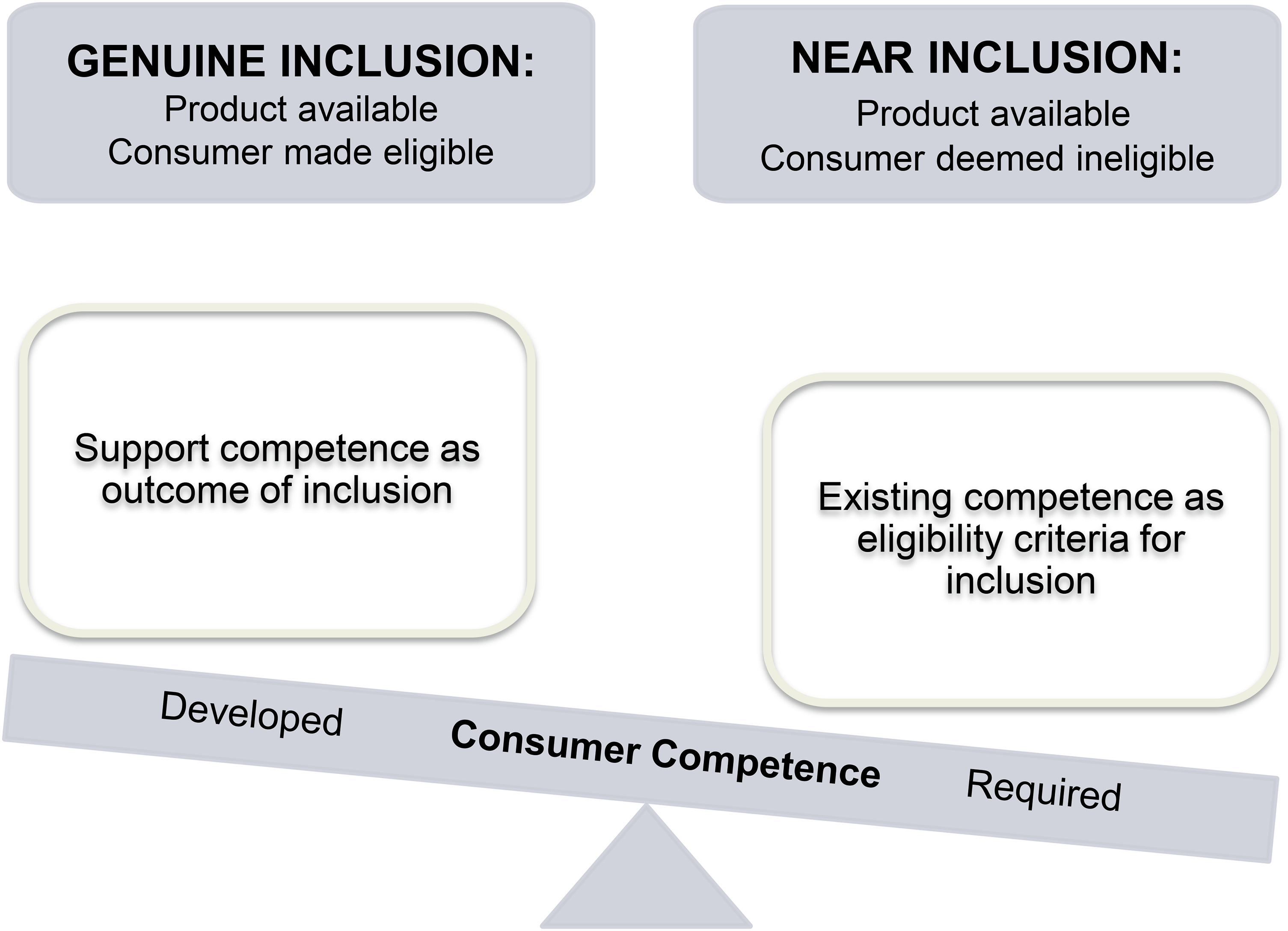
The Role of Competence in Genuine Versus Near Inclusion.
Take, for example, CamDiab, one of the leading manufacturing brands in the HCL systems market. CamDiab frames its app CamAPS FX as “sophisticated … easy to set up” (CamAPS FX - CamDiab 2021). A patient testimonial on the brand's website reads: “To anyone considering the CamAPS FX app my advice is quite simple, go for it. It really is transformational and if I can do it anyone can” (CamDiab 2026). Medtronic (2026), maker of the MiniMed 780G insulin pump system, uses the tagline “Life with diabetes just got easier.” Similarly, Dexcom (2026) markets its continuous glucose monitoring systems as “Easy. Accurate. Better health outcomes.” This market-led construction of competence imaginaries (“anyone can”) positions families and patients as capable and deserving actors in their own processes of care. These narratives emphasize product development and technology support rather than consumers’ responsibility to become competent. This contrast matters because such imaginaries shape expectations, aspirations, and claims to access, thus amplifying the harm caused by denial of formal inclusion. Policies of marketplace inclusion must, therefore, recognize consumer competence as dynamic, relational, and shaped by sociocultural contexts, markets included. Ideally, access programs should be designed in collaboration with other market actors to actively support consumers in building embedded capacities through the design, training, and ongoing use of the medical technologies. This approach acknowledges that consumer competence, as traditionally understood, is a poor basis for determining who gets to access life-changing market resources.
Our analysis of near inclusion in the context of HCL technology shows that market entanglements continue to sustain exclusion, even as market narratives and product innovation seem to facilitate the development of consumer competence. These dynamics underscore the intersectional nature of systemic exclusion, revealing that inclusion cannot be reduced to mere product provision or very specific functional training. Instead, genuine inclusion requires careful attention to how the competences demanded by markets can emerge within systems of collaboration.
Footnotes
Joint Editors in Chief
Jeremy Kees and Beth Vallen
Special Issue Editors
Samantha N.N. Cross, Rebeca Perren, Eileen Fischer, and Anders Gustaffson
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
No data were created or analyzed for this article.