
Abstract
Digital media use is central for youth as a means to facilitate identity development, social connection, and vocational competence. Emerging literature suggests that the influence of digital media use is more nuanced than the contemporary risk/benefit discourse, particularly for youth who experience social and emotional vulnerability. This youth-centered, developmentally informed study attends to the gap in literature addressing the digital media use experiences among youth in residential treatment (RT). McCracken’s Long Interview Method was utilized to conduct and analyze in-depth interviews with youth (n = 15) aged 13 to 18 in RT. The analysis involved movement from particular to general coding, applying categorical observations, and thematic comparison of transcripts. Consistent with existing literature on other youth populations, participants reported that digital media use had both beneficial and problematic implications for their well-being. Internet access decreased experiences of isolation and stigma and increased capacity to contend with marginalized identities (e.g., disability, Lesbian, Gay, Bisexual, Transgendered, Queer, Two Spirited Plus [LGBTQ2S+], child welfare guardianship). They reported that following an initial digital disconnect and stabilization, digital media use facilitated pathways toward agency, leadership, and community engagement (e.g., LGBTQ2S+ community, recovery blogs, animal advocacy). The findings suggest that supporting youth in RT to identify their online opportunities and needs can encourage individual growth, wellness, and participation in social change.
Introduction
Internet-enabled digital tools (cell phones, tablets, gaming consoles, and PCs) offer pathways for communication and virtual social spaces that have become central platforms for adolescent developmental tasks such as social connection, identity development, and health and wellness information-seeking by youth (Borca et al., 2015; Davis, 2013; Middaugh et al., 2017; Shifflet-Chila et al., 2016). Opportunities for adolescent developmental growth often include exposure to risks and digital media use is no exception (Masten, 2004; Ungar, 2001). Online risks include content exposure, conduct, and contact-related experiences online (Livingstone et al., 2012). Extant literature has focused on four key categories of online risk: (a) harassment and cyberbullying, (b) privacy and information breaches, (c) sexual solicitation and encounters, and (d) exposure to explicit content (Pinter et al., 2017). Additional areas of concern include internet and video game overuse (Kuss & Lopez-Fernandez, 2016).
While experiences of online harm among youth vary significantly based on age, amount of time spent online, and types of activities (Livingstone & Helsper, 2013; Selwyn, 2009), some groups of youth encounter more harm from online risk exposure. For example, compared with general youth populations, youth with learning, behavioral and mental health challenges (Carson et al., 2018; Good & Fang, 2015; Rafla et al., 2014), and marginalized groups including, Lesbian, Gay, Bisexual, Transgendered, Queer, Two Spirited Plus (LGBTQ2S+) youth and those involved with child welfare organizations (Badillo-Urquiola & Wisniewski, 2017; Schimmel-Bristow & Ahrens, 2018) are more negatively affected by online risks, particularly cyberbullying, exploitation and the emotional impact of social comparison (Abreu & Kenny, 2018; Kowalski et al., 2018; Schimmel-Bristow & Ahrens, 2018; Stathopoulou et al., 2018). Paradoxically, these same groups of youth have been shown to use and benefit from digital media to contend with social isolation, express themselves, maintain contact with friends and family, enact skills and competencies, and access information and resources to promote health and well-being (Badillo-Urquiola & Wisniewski, 2017; Craig et al., 2015; McInroy, 2018; Regan, 2017; Rideout & Fox, 2018).
Despite an emerging body of literature addressing digital media use among child welfare involved youth in out-of-home placements (Denby Brinson et al., 2015; Gustavsson & MacEachron, 2015), literature focused on the media practices of youth requiring admission to mental health-based residential treatment (RT) remains in its infancy (Good & Mishna, 2021). More specifically, the gap of empirical knowledge derived from the firsthand perspective of youth has been identified as important and needed to generate effective practice and policy approaches in RT settings. The purpose of the current study is to explore how youth understand and describe the interplay between digital media use and wellness, prior to admission and during their time in RT.
Youth in RT and Digital Media Use
While the degree of vulnerability among youth in RT varies in severity and complexity, they share characteristics that are associated with youth who are more affected by online harm (Anderson, 2017; Pridgen, 2010). Typically, between the ages of 13 and 18 years, youth in RT often have encountered adversity associated with traumatic experiences and/or characteristics increasing their vulnerability. These characteristics may include depression, anxiety, difficulties with emotion regulation and impulse control, substance abuse, learning and communication difficulties, and psychosis (Good & Mishna, 2021; Lyons et al., 2015; Trout et al., 2009; Vural et al., 2015). Safety issues among youth in RT can include self-harm, suicidal ideation, aggression toward others, running away, and sexual aggression (Lyons et al., 2015). Historically there has been a problem-focused lens applied to the literature addressing youth in RT (Ungar, 2001). This problem-focused frame of youth in RT can result in missing the existing strengths that have supported youth to navigate very complex life pathways. A growing body of literature, however, has shown that resilience-based approaches to skill development both online and offline can safeguard marginalized youth, including those in RT, from harm by generating and nurturing pre-existing hope for the future, agency and social connection with adults and peers (Asakura, 2017; Lou et al., 2018; Ungar, 2004; Vissenberg & d’Haenens, 2020).
With early parental mediation, education, and peer-based discussions about safety, the majority of youth is able to safely navigate online risk (Livingstone et al., 2017; Odgers, 2018; Shin & Lwin, 2017). Rather than focusing on risk prevention, experts recommend a risk resilience approach to online safety (Hinduja & Patchin, 2017; Pinter et al., 2017; Wisniewski, 2018). Resilience is defined as protective patterns used by youth to avoid adopting problem behavior in the face of risk (Catalano et al., 2004; National Research Council Institute of Medicine, 1996). In the context of online safety, resilience suggests that pre-existing strengths and resources can be used to successfully traverse online risk (Good & Mishna, 2021). In addition, resilience can be used to mitigate negative effects of online risk exposure including cyberbullying and internet addiction (Wisniewski et al., 2015).
Empowerment-based approaches to online risk resilience development among youth have been promoted by Vissenberg and d’Haenens (2020). Their study looked at EU Kids Online 2018 data of 1,436 Flemish youth and showed that highly engaged youth encounter more distressing online content than less digitally engaged youth, but their increased online engagement provided skill-building and problem-solving opportunities that permitted them to mitigate the degree of harm due to their degree of online risk resilience. Consistent with previous studies, Vissenberg and d’Haenens also reported that youth who are more negatively affected by online risks may require more adult support to develop skills to decrease the impact of online harm. Consistent with this, Good and Mishna (2021) focused on the perspective of service providers. They suggest applying concepts from positive youth development theory to promote online safety among youth in RT regardless of levels of internet access.
Developmental Tasks and Youth in RT
The use of strength-based and resilience-informed interventions with high-risk youth is well reflected in the child and youth care and social work literature (Baber & Rainer, 2017; Lou et al., 2018). One example of such a model is positive youth development, applied to interventions targeting youth identified as high risk (Catalano et al., 2004; Lerner, 2005; Sanders et al., 2015). It attends to the complex interplay of individual characteristics, relationships, and contexts belonging to youth while simultaneously promoting agency, competency, and growth. Within positive youth development, five key tasks are framed as pathways for positive development: (a) competence or a sense of mastery and self-efficacy, (b) confidence or a feeling of self-worth, (c) connection or a sense of belonging to a family or community, (d) character or a sense of possessing values and a social conscious, and (e) caring or a sense of compassion (Gustavsson & MacEachron, 2015; Lerner, 2005). Healthy development is promoted by aligning the strengths of youth with the resources found in their physical and social ecologies (Lerner, 2012).
The notion of social ecology associated with positive youth development derives from systems theory (Lerner, 2005). One example is Bronfenbrenner’s Ecological Model of Human Development that suggests that development occurs through interactions between and through these multi-level interrelated social systems. This framework emphasizes supporting the individual strengths and needs of each youth within their particular life spaces or social ecology. The microsystem is defined as “a pattern of activities, roles and interpersonal relations experienced by the developing person in a given setting with particular physical and material characteristics” (Bronfenbrenner, 1979, p. 22) such as home, school, or workplace. The mesosystem is a system of the microsystem that is formed or extended when a person moves into a new setting. The mesosystem addresses the interrelations among two or more settings where the individual actively participates such as home, school, and neighborhood peer group. The extosystem also addresses the interrelation between the individual and one or more settings but does not involve the individual as an active participant. However, the events that occur within the extosystem affect or are affected by what happens in the setting containing the individual (Bronfenbrenner, 1979). For example, within RT, clinical decisions made at a staff team meeting would be based on events that took place in the (treatment setting) microsystem of a client and affect the client within the microsystem but the client is not involved in the meeting and decision-making.
The macrosystem addresses subculture or culture as a whole that informs belief systems and ideology “that are consistent within the form and content of the lower order system levels (micro, meso and exto)” (Bronfenbrenner, 1979, p. 26). Policy and legislation are examples of the application of macrosystem ideology being implemented within the lower order system (Pence, 1988). There is a differential influence of macrosystem values and practices on various groups within society. Bronfenbrenner added a final system called the chronosystem to incorporate the influence of history and time, both of which shape development.
Over the past several decades, academics have addressed technology and media in relation to a social-ecological framework. New digital tools and associated virtual contexts create pathways and spaces that interact with the pre-existing ecological systems identified by Bronfenbrenner. The influence of digital tools and context (digital sub-space) within each pre-existing subsystem has been incorporated into ecological models and has been applied to youth digital media use and well-being (Johnson, 2010; Martin & Stuart, 2011). Increasingly, literature on positive youth development and research addressing youth digital media use emphasizes the importance of attending to the digital subspace as integral to the social ecology of youth (Martin & Stuart, 2011; Middaugh et al., 2017; Shifflet-Chila et al., 2016). This is particularly important considering identity expression and peer connection are both integral to adolescent development and are increasingly facilitated through mobile devices and digital media use (Davis, 2013; Davis & Weinstein, 2017).
Literature focused on residential addiction programs for both youth and adults, suggests there are some benefits to restricting online access, but long-term restriction comes with negative consequences (Anderson, 2017; Collier & Gavriel, 2015; Sanders et al., 2017). Some studies suggest the ubiquity and potential resourcefulness associated with digital media use makes restricting it an ineffective long-term solution for youth in RT (Anderson, 2017; Good & Mishna, 2021; Lim et al., 2013). One recent study focused on RT service providers’ perspective suggests applying positive youth development to promoting online safety among youth in RT is important regardless of levels of access or restriction during treatment (Good & Mishna, 2021). In addition, this study recommends including perspectives from youth in RT to inform future research, practice, and policy development.
It is important to gain a better understanding of the experiences and needs of youth in RT when it comes to digital media use and access. This is relevant, considering the growing relevance of digital media use coupled with the lack of research focused on the digital media use among youth in RT. This is particularly relevant considering the absence of youth perspective in the research exploring the opportunities and obstacles associated with supporting youth with serious mental health and behavioral challenges. The aim of the current study is to address the lack of research addressing digital media use in RTs by contributing exploratory, descriptive research that amplifies the voices and experiences of youth in RT (Nolas, 2011; Sprague Martinez et al., 2018).
The overarching research question addressed in this study is:
The resulting youth-driven data can inform practice approaches to supporting the developmental pathways of digitally engaged youth within RT programs. A positive youth development model is applied to the discussion of the results, offering insight into the tension experienced among participants between digital media use as a risk for increased harm and as a facilitator of wellness and development, providing strength-based approaches to digital literacy and online safety for youth in RT.
Method
McCracken’s Long Interview Method of data collection and analysis (McCracken, 1988) was utilized in this study. An initial “analytic review” of literature was conducted to generate a core research question and develop a rich interview guide focused on soliciting youth perspectives related to their experiences of digital media use prior to and during their time in RT. This process contributed to interview guide questions that moved past pre-existing definitions related to youth digital media use (such as the current focus on digital media “risks” and “opportunities” both examples of adult, and professional framing of youth digital media use rather than how youth define and describe their relationship to digital media use) and moving past pathology-based formulations of problems related to digital media use among youth with mental health difficulties. This was done by exploring constructivist ethnographic research literature (boyd, 2010; 2014; Ito et al., 2010; Mesch, 2009; Mesch & Talmud, 2010; Rideout, 2015). This was coupled with the primary investigator (PI) applying McCracken’s phenomenological approach to qualitative inquiry, which emphasizes recognizing the researcher’s positionality to the subject being examined and described below.
Prior to recruitment and data collection, a “cultural review” of the identified research categories related to youth in RT and youth digital media use was conducted whereby the PI positioned herself as an “instrument of inquiry,” unpacking familiarity with the topics in a systematic and reflexive process. This was achieved through reflexive memo-taking, and academic peer and mentor consultations. These steps focused on taking stock of the PI’s personal and professional assumptions and associations derived from lived experience, working with youth in RT and her past experience and knowledge of previous research related to youth digital media use (McCracken, 1988; Merton et al., 1956).
Following ethics approval from the two participating agencies and the PI’s university Research Ethics Board, purposeful sampling was used to solicit participation from youth ages 13 to 18 years who were in RT for at least 1 month or had been admitted to one of four participating RTs in Ontario, Canada, in the past year. All recruitment, data collection, and analysis were conducted by the PI, who had no relationship with youth in any of the participating programs. Following an introduction to the project in a group meeting, youth were invited to take information packages to review and sign-up to participate. Youth assent and parental consent were obtained prior to interviews (in accordance with each agency’s consent/assent guidelines). Youth ages 16 and over from all four participating programs were able to consent without parental authorization. Parental consent and youth assent were required for youth ages 15 and under at Agency A (rural and urban multi-gender hospital-affiliated programs) and youth 12 and under at Agency B (the female residence and the male residence in urban neighborhoods; see Figure 1).
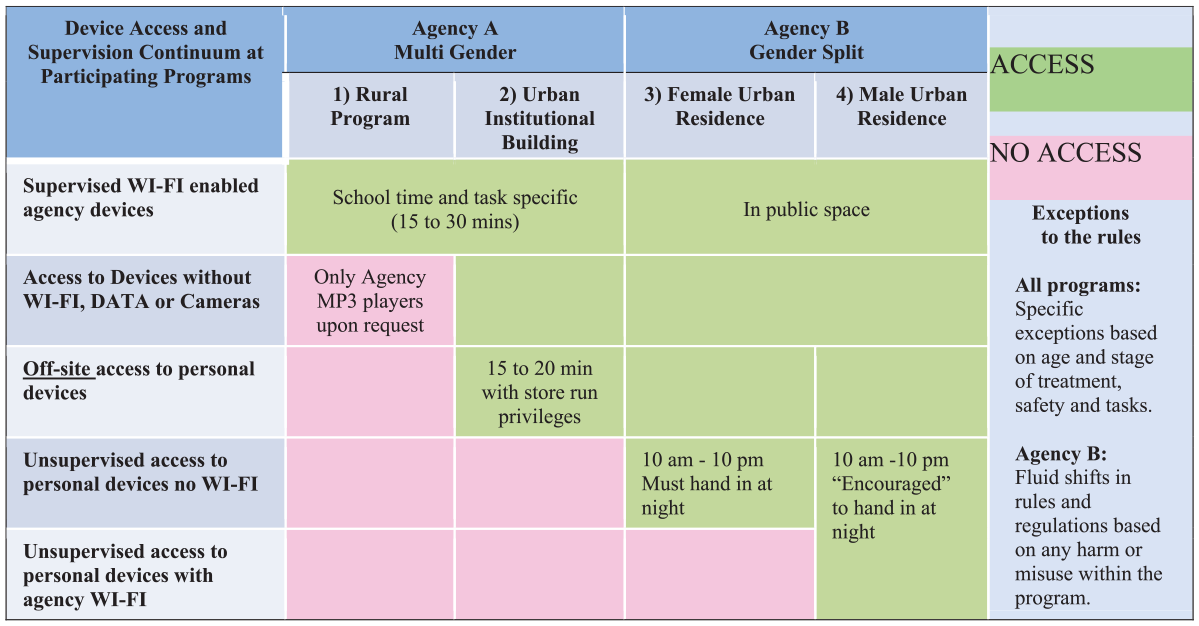
Device access and supervision continuum at participating programs.
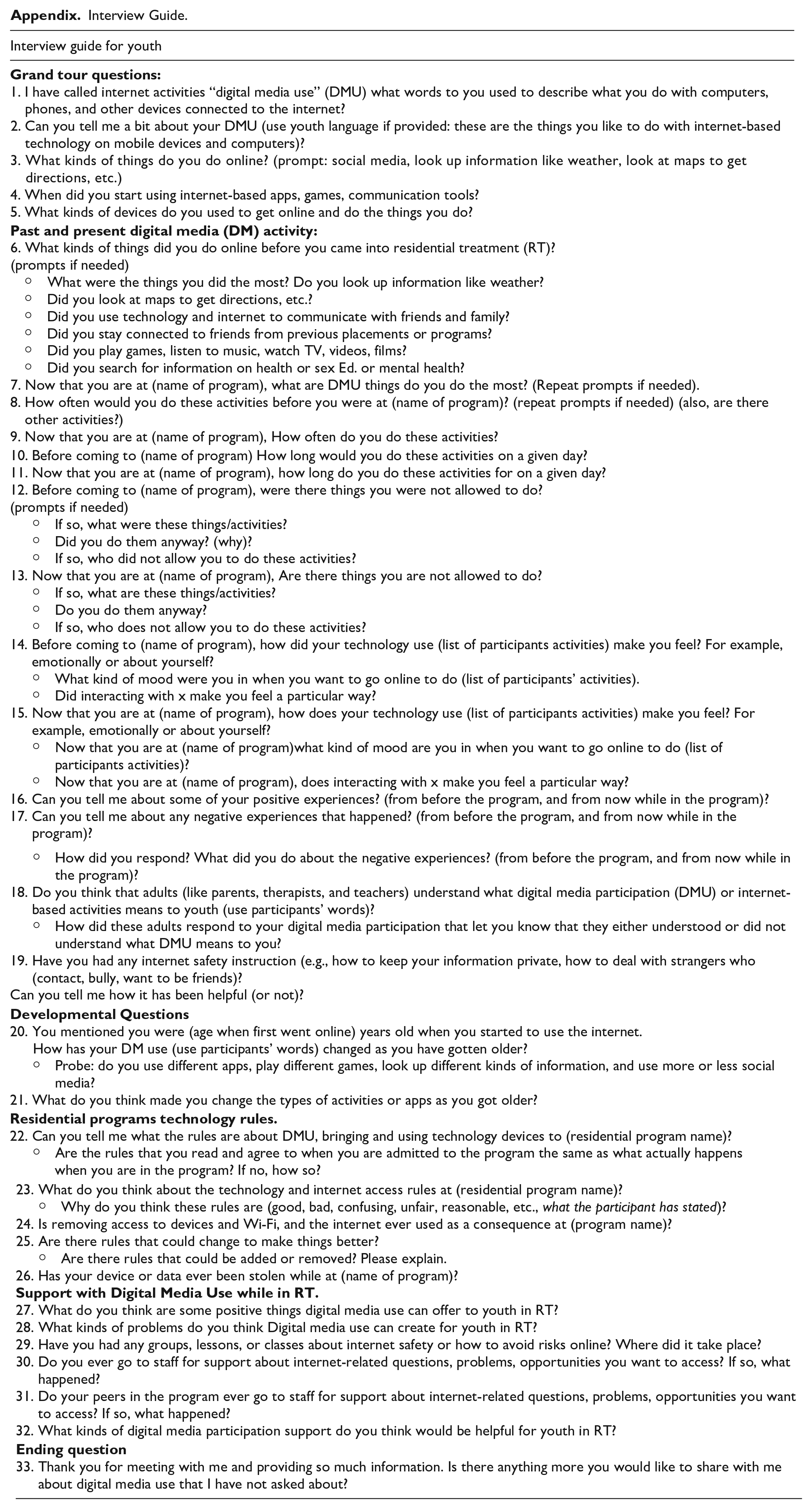
Semistructured interviews, as defined by the long interview method (McCracken, 1988), took place with youth at participating RT programs for more than 8 months between November 2017 and June 2018. Following review of consent documents, youth were asked to answer brief demographic questions pertaining to gender identity, ethnic or racial identity, and duration of time in RT. Questions about technological device ownership and use were asked to gauge participants’ personal use and familiarity with digital media use. Participants were asked to describe their general online experiences and how their emotional well-being was related to their digital media use prior to and during their time in RT. For example, participants were asked questions related to the meaning and role of digital media use within different domains of their lives (e.g., hobbies, recreation, education, relationship development and maintenance, family connections). They were asked when they started using digital media and the types of device(s) to which they had access. They were asked how different activities affected their well-being and to talk about activities that resulted in positive and negative experiences, emotions, and lessons learned. Aligned with the ecological and developmental research frameworks, youth were asked questions associated with changes to their perspective toward online experiences from a developmental timeline within different social and relational domains (e.g., family, friends, school, home, and RT). Youth were also asked how they experience adults’ attitudes toward youth digital media within their family and RT settings. This included soliciting details and descriptions of experiences of negotiating digital media use while participating in RT. (More examples of interview guide questions can be found in the Appendix).
Interviews were digitally recorded and ranged in length between 25 minutes and 2 hours based on the level of detail youth were willing to provide and interest in the subject matter. The PI documented reflexive journal and observational memo writing following each interview to generate contextual details and provide observations of similarities and differences between interviews and existing literature. Recordings were transcribed by a research assistant and reviewed by the PI to ensure accuracy. Participants were offered the opportunity to review their interview transcript or recording for accuracy and feedback. Two of the 15 participants completed this member checking process.
Data Analysis
Verbatim transcripts of the recorded interviews were analyzed using McCracken’s five-stage model. NVivo software was used to execute the qualitative analysis process, moving from particular to general. Beginning with Stage 1, there was an observation of individual utterances isolated from each other. In Stage 2, the initial utterances were assessed for ways they were linked to each other, to become expanded observations. At this stage, core themes were emerging from youth’s nuanced descriptions of mental health challenges and online activities. For example, there were indications of awareness among youth of times when digital media was experienced as both attractive and detrimental to them. These expanded observations were then compared with other transcripts, the literature, and the cultural review (reflexive analysis by the PI) to contextualize and situate assumptions or PI influence (Good & Mishna, 2021). For example, to avoid premature conclusions based solely on youth-reported risks and endorsement of digital media restrictions, a more in-depth analysis of thematic categories was employed to reflect the nuances of youth experience. Upon further analysis, it became clear that youth were asserting two messages: (a) It is hard not to have DM access, but the break can be good to create safety. (b) A return to digital media access informed by youth needs and strengths was important to their recovery, and sense of inclusion in adolescent life and development.
The third and fourth stages focused on the interconnections, consistencies, and contradictions within participants’ descriptions of unique digital media experiences. For example, the review of participants with differing experiences was undertaken, to examine context and nuance in descriptions of challenges and benefits related to the limiting of digital media access and the opportunities associated with access. This was followed by an additional comparison to the literature and a reflexive cultural review initiated by the PI. At this stage, the PI identified the significance of resilience-based developmental tasks as described by the positive youth development framework, which fit within the third identified thematic category in the results. Finally, the fifth stage entailed returning to the transcripts and to review the patterns and themes that emerged and were linked to the earlier analysis stage of observations and themes (Good & Mishna, 2021; McCracken, 1988).
Coupled with the long interview method’s multistep process, four criteria of trustworthiness were employed to ensure validity through the qualitative analysis of this study (Creswell & Miller, 2000; Good & Mishna, 2021; McCracken, 1988). Credibility was achieved through, prolonged engagement, consistency, triangulation, and the use of dependability and confirmability. The PI’s previous 13 years of professional involvement with youth in RTs provided evidence of prolonged engagement. In addition, the use of illustrative quotes from participants’ descriptions of their lived experiences provided a further demonstration of prolonged engagement. Consistency was demonstrated by having the PI conduct all data collection and analytical steps. Triangulation of the findings was provided by having 25% of transcripts coded by four doctoral students, to ensure thematic consistency. This triangulation process took place at the third and fourth stages of analysis where coding observations by the four doctoral students were compared. The coding nodes and emerging initial themes identified by the doctoral students and the PI were found to be consistent. Dependability and confirmability were enacted by providing a description of analytic steps taken, including an audit trail and reflexive journaling and memo writing (Antle et al., 2008; Good & Mishna, 2021).
RT Settings and Sample Population
The participants in this study were associated with four distinct programs. Each program serves youth (with and without child welfare involvement) who require RT, a high level of staff support, and separation from their home environments. Participation in these programs is voluntary and typically youth have formal diagnoses of at least one mental health, learning, and/or behavioral difficulty, with the exclusion of a primary diagnosis of autism or developmental delay (Good & Mishna, 2021). Programs 1 and 2 were delivered by Agency A, a pediatric hospital-affiliated community mental health center. Both cater to male, female, and gender variant youth and have a capacity for 10 youth each in the age range of 13 to 18 years. Program 1 was located in a rural setting 2 hours from an urban center, while Program 2 was located within a downtown urban community mental health institution. Agency B was responsible for Programs 3 and 4. Both were gender-split, in a home-based community setting run by a children’s mental health center, each with the capacity for six youth in the age range of 12 to 18 years (Good & Mishna, 2021). In this study, Program 3 is referred to as the Female Urban Residence and Program 4 as the Male Urban Residence. All four programs offered some digital media use to the youth in their care, however, the frequency and duration of access to personal devices and degree of supervision varied by program and treatment approach (see Figure 1). Program 1 offered the least amount of digital media use, while Program 4 offered the most unrestricted digital media use.
Youth Demographics
Fifteen youth were recruited and completed the consent process. The majority of participants (n = 12) were older than 16 years. The remaining (n = 3) were between 14 and 15 years. The duration of time in RTs among participants ranged between 1 month and 2 years with the following breakdown: <3 months (n = 3), 3 to 6 months (n = 5), 6 to 12 months (n = 3), 1 to 2 years (n = 4). Gender identity among the participants included (n = 4) male youth, (n = 10) female youth, and (n = 1) nonbinary youth. Among the 15 youth, five identified as belonging to a visible minority group (e.g., racialized youth including, Black, Asian, Latinx, mixed race). During the interviews, four self-identified as belonging to the Lesbian, Gay, Bisexual, Transgendered, Queer, Two Spirited Plus (LGBTQ2S+) community. The majority of youth had a smartphone with a data plan (n = 12). Among the participants, two had a cell phone without a data plan and one youth had no cell phone. All youth identified as having participated with digital media since at least the age of 12 with some reporting unsupervised digital media use at 7 years old. The descriptions of mental health and behavioral challenges described by youth participants were consistent with the heterogeneity in the demographic literature on youth in RT. Unique characteristics of youth challenges requiring admission to RT and their positive and difficult digital media use experiences are reflected within the narratives described in the “Results” section.
Results
The analysis and interpretation of these data revealed three core thematic categories, which follow the shifts in digital media use and well-being reported by youth in RT. The first thematic category, “A Problematic Solution: Experiences with Digital Media Use Among Youth Pre-admission and While in RT,” highlights pre-admission digital media use and early experiences of digital media use in RT. The second thematic category, “‘It’s hard’: Experiences of Digital Media Use Restrictions and Digital Disconnect,” offers descriptions of participants’ mixed feelings about limitations on digital media access while in RT. The third thematic category, “Pathways to Wellness: (Re)connecting in Mindful Ways,” provides examples of experiences demonstrating how digital media access facilitated pathways to wellness and offers descriptions of how participants’ digital media use shifted during RT.
A Problematic Solution: Experiences With Digital Media Use Among Youth Pre-Admission and While in RT
Youth reported that digital media use helped to distract them from depression and anxiety and to decrease their experiences of social isolation by helping them stay informed about pop culture and the news. One youth stated, “Being able to keep up on world events. That’s kind of big for me . . . I’m a pretty political person” (Y49). 1 Another youth highlighted how being informed helped them remain connected and in touch with youth culture, “I think involved, or just like kind of like not ignorant . . . I think it makes me feel like I’m not an outsider being a part of all that. Just important to me” (Y48). Social media “likes” and posts were identified by one youth as helping her to feel cared for and valued, stating, “Well it kind of built my self-confidence . . . just makes me more happy when people are commenting . . . It just makes me feel like more special and makes me feel like they actually care” (Y55).
Beyond offering a sense of connection and a method for remaining informed, participants reported finding social media important as a way to contribute, have purpose, express themselves, and motivate them to persevere through times of distress and adversity. On one hand, digital media use was depicted as a default activity to entertain and distract participants. For example, in reference to not attending school for extended periods of time, one participant stated, I mean I didn’t feel like I had much else to do so might as well kill time online . . . But I mean of course some of us like that’s like why we’re in here because we’re on the internet all the time and stuff. (Y21)
On the other hand, this same youth and several others described digital media use as a way to have purpose and feel less alone with difficulties.
One youth who shared she had 3,000+ followers on a mental health support Instagram account described the value of social media use before and during treatment this way: Treatment often feels so overwhelming and for me having a bit of, a, it almost gives me like purpose like something to do that I like that’s going to keep me going and that for me is a little bit fulfilling. It really does make me happy. It makes me feel proud about myself, that’s not easy for me to do but I try. I’m really happy that I get to have it [social media] . . . Whenever I would feel like horrible about myself or I was anxious, whatever, I would just go on my Instagram and just feel,. . . I guess, at peace and just a little more grounded, a little less lonely. (Y26)
Participants who were less active social media contributors also reported going online to learn more about their mental health difficulties and to feel less alone and more hopeful. One youth attributed their agreement to get treatment to inspirational video content by social media influencers who have contended with mental health difficulties: I kind of, somewhat found motivation online to help me decide on coming here . . . I like kind of see these people [internet personalities] and, . . . I kind of want to be like them and they talk about how they somewhat struggled like how I did and then turned out the way they did because they motivated to work hard. So, in a way that also motivated me to work hard so that someday I could have a better life. (Y24)
A participant who was employed as a professional gamer and coach prior to admission to RT shared experiences of being negatively affected by disability-related and transphobic prejudice in middle and high school leading to extensive absences from school. This youth reported finding people who understood her and valued her leadership and expertise within the online gaming community. Her role as a team leader reportedly provided a source of purpose, competence, and independence: I’ve had a job since I was 12 that’s awesome. . . . I bought a PC with my own shit. I got this like thousand-dollar gaming PC that I built myself and I bought all the parts with my own money . . . I feel like a lot more independent than a lot of the people here [RT]. And being independent is frickin’ nice because you can do your own thing . . . It makes me feel good. (Y49)
Paradoxically, a number of youth reported that extended amounts of online activities heightened experiences of boredom, loneliness, anxiety, and sadness. For some, digital media use was described as a segue to self-harm. Some participants described a process, whereby exposure to social media and digital media use started as a coping strategy and gradually became part of the problem. For example, youth reported social media use generated a negative effect on their emotions, a sense of obligation to engage, and increased stress and social comparison: Social media can make it worse for sure and I remember about a year ago, when I was hospitalized for the first time I decided when I left the hospital that I was gonna quit social media for a while and it was the best thing I ever did. It was literally so much less stress. So much like less bad feelings about jealousy for other people and just comparing your life to theirs and stuff like that. (Y47)
Several youth reported that seeking mental health content and connections with others with similar difficulties promoted suicidal ideation, depressive states, and self-destructive behaviors, including self-harm. “Yeah. OK so there are accounts out there like that but, there’s also accounts out there, kind of like almost pro-depression, pro-suicide, pro-self-harm but, they all kind of merge into one . . .” (Y57). Another youth attributed adopting self-harm as a way to cope with her mental health problems to these self-destructive online communities: And honestly my phone has been a huge segue into some of the stuff that I do like cutting and stuff like that I saw it on the internet, and I thought, “Oh my God I’m going to try this,” . . . Yes, but I know now that it is really bad to do because then once you start doing that then you start thinking that self-harm is more OK. (Y47)
Overall, participants reported a strong awareness of the influence of digital media use in their day-to-day lives leading to admission into RT. Moreover, youth reflected that they often engaged with digital media as a strategy to address a problematic emotional state. For some youth, digital media use was a positive tool that supported their well-being. In many instances, youth commented, however, that their use of digital media as a solution for problems actually increased their distress. Other participants described digital media use as a problematic solution with simultaneously beneficial and problematic influences on their well-being. The next theme explores the diverse experiences and reactions of the youth participants to the varying degrees of digital media use restriction prescribed by their RT program.
“It’s Hard”: Experiences of Digital Media Use Restrictions and Digital Disconnect
On one hand, youth reported that lack of access to cell phones and social media was a consistent concern that contributed to their sense of relational disconnection and isolation as well as fear of missing out (FOMO). One youth described this by stating, “You feel like living you’re living under a rock, and then you feel excluded” (Y53). Youth acknowledged having access to a telephone and land/snail mail but explained that most of their friends used social media, texting and FaceTime to communicate. The lack of contact with peers, therefore, resulted in many participants describing an increased sense of isolation: I think it should be addressed because it sucks if you’re losing friendships because . . ., you’re never able to talk to them. So, it’s like you lose friendships over that sometimes or relationships or whatever. And that in itself can make you feel more depressed. (Y26)
On the other hand, while there were few enthusiastic endorsements for restricting digital media use among participants, many said they understood the rationale for limits to digital media use access, particularly in relation to privacy and confidentiality within RT settings. As one youth stated, It would be really hard [to let youth have cell phones] and also the confidentiality stuff like we can’t take pictures of each other, things like that. So, I kind of fully understand that . . . Doesn’t mean that I like it, it’s just I understand it. (Y47)
Despite this resignation to accepting the digital media use rules, several participants in programs with very limited access to social media and gaming reported that after some time, they adjusted to the limits. For example, one youth commented that, “At first it was really hard, especially being a teenager . . . but the program is very busy, and I eventually didn’t ever think about my phone” (Y26). Furthermore, this participant and others reported that they eventually found the disconnection to devices and the internet valuable reporting, “It was hard at first, but you get used to it. Honestly, I kind of like not having my phone” (Y26).
The reported benefits of a disconnection from devices were particularly evident according to the youth who had been hospitalized prior to their RT admissions, older youth who could reflect on their digital media use in relation to their treatment issues and youth who had been at RT for more than 6 months. The youth explained that the digital disconnect allowed them to pay attention to their own thoughts and feelings and avoid distractions such as peer drama and feelings/FOMO in relation to fun with their home friends. The following two quotes illustrate how a disconnect from their regular cell phone use offered youth time to focus on themselves: It’s a part of everyone’s life now at this point all of the teens at least. And maybe taking a break from it and just kind of looking back and just kind of reflecting on like what’s up with yourself or whatever. I think that’s useful. (Y21) I just kind of felt like I was behind society and then . . .—it really makes you realize that you are isolated when you come here, that you are in the middle of nowhere, and you’re—but it also makes you think that this is a treatment for yourself and not the world you know. Like it’s supposed to be that you’re here, focus on you. (Y48)
Regardless of digital media use rules in each program, some of the participants reported that they and other youth actually had their own cell phones or access to the internet without authorization. One youth expressively stated, “It’s happening right under their noses” (Y49). According to participants, as they became more familiar with the RT program and rules over time, the youth found loopholes to rules making it possible for them to sneak internet access and “forget” to hand in devices. One youth stated, “Let me see. It’s very easy to get away with it though once you’ve been here a while” (Y51). Some youth expressed concerns that younger youth in RT were also using the internet without permission and participating in risky behaviors without staff awareness. In summary, participants identified a range of experiences when access to digital media was limited in RT. Some youth resented the requirement to pass in their devices, while others found digital media use limits helpful. Still, others had conflicting feelings about digital media use restrictions. They understood the rationale, gained benefits from the disconnection from their devices and appreciated having limited access at particular times, and yet they disclosed keeping their devices when they should have been turned in, or sneaking them into their dorm rooms.
Pathways to Wellness: (Re)connecting in Mindful Ways
The third thematic category provides examples of how the youth adapted their digital media use or applied their pre-RT positive online activities to their recovery. This included how varying degrees of digital media use access supported adolescent developmental pathways toward identity, recovery, leadership, and community engagement. It emerged that limits to digital media use access helped the participants become aware of the dominant role of digital media use in their lives and shifted their relationship to digital media use, whereby they (re)connected in purposeful, wellness promoting, and intentional ways that were consistent with mindfulness practices being taught in their respective RTs.
Some youth in RT programs in which some digital media access was allowed, described how their online activities shifted or were addressed in their treatment. For example, one 16-year-old youth shared that she had experienced a difficult childhood including child welfare guardianship and mental health difficulties that led to a number of hospitalizations. Prior to her hospitalizations, she described her digital media use access as predominantly negative and focused on self-destructive and eating disordered content: There’s a community of people who . . . post pictures of their self-harm and pictures of themselves calling themselves fat when they’re vastly underweight. It’s community and I was part of . . . I think it made me more depressed . . . and it normalized self-harm to the nth degree, and it glamourized and romanticized it and suicide. . . . and when that is something that you are exposed to so much, you see it as this kind of thing that is like possibly beautiful or makes you special or something. Especially if you haven’t had attention in your life for one reason or another. People want that, right? (Y57)
After a digital disconnect associated with a lengthy hospitalization, this participant reported that she began to shift her focus toward animal protection and advocacy, healthy eating, vegetarianism, and the vegan online community, “I’m a vegan so there aren’t a lot of vegans out there especially when you’re 16 but, on the internet like on Instagram there’s a humongous vegan community” (Y57). This participant reported that the break from social media during her hospitalization helped her to recognize how her digital media use was contributing to her problems. Her focus on making changes for suffering animals coupled with an emphasis on wellness and health was reported to be important for her socially, emotionally, as well as to her sense of purpose and identity: Well, I spend a lot of time on Instagram because now, this has nothing to do with mental health but it makes me feel like I belong kind of sort of . . . it was really nice to find other people who believe the same way and it made me feel less alone because that’s a really large part of my identity . . . (Y57)
She also reported that belonging to a group of people who cared for vulnerable animals increased her sense of optimism about society and humanity, which was particularly significant given her child welfare involvement: It really reaffirmed some of the hope and my faith in humanity just because I was surrounded by people who literally care so much about the most innocent beings on this earth who can literally do nothing for them but, they’re still being compassionate towards them. Oh! And and from that I was able to go to vigils like I went to—I was able to feed pigs water. (Y57)
Being a part of a community of people who shared her values and demonstrated altruistic behaviors was a positive influence for this participant.
In an example that appears counterintuitive, a youth with an online pornography addiction was permitted to maintain internet access despite the illegal and problematic nature of his online activities. He talked about how although addressing his problematic digital media use is ongoing, the treatment resulted in his developing self-awareness. This youth reported that some overnight digital media use restrictions at the beginning of his treatment plan with increasing unsupervised access were helpful. The following quote shows the participant’s understanding of not having access overnight: I had to hand my phone in originally and that was, so I didn’t like—because like an addiction to porn. Well, I still do. Like it caused me to not sleep at night and like I guess looking up dark content or just like pornography content in general and because of that like constant exposure to that kind of stuff like all night long as you can imagine is like not just unhealthy . . . (Y14)
He stated that over the span of his 2-year stay in RT, he gained awareness of how his addiction to online pornography was a means of coping with sexual and physical abuse trauma. Conversation with service providers regarding the time, he spent isolated in his room viewing violent and sexually explicit content provided the youth insight into his addiction and his motivations to view predatory content: . . . like a lot of people that come into here like have like a piece of past where they were once like I guess a lot of us see ourselves as, well at least I do, a sad, little vulnerable child and it’s that whole vow that . . . I’ll never be weak again. And that’s where that desire of like control and power comes from . . . Yeah. Like if I’m feeling like very . . . angry at the fact that I’m vulnerable I look up anything that can make me feel more like a predator than a domicile sheep. . . . So that like instead of being the prey you become the predator. (Y14)
The therapeutic work in which this youth engaged with RT staff to address his digital media-related behaviors resulted in him gaining understanding about his interactions with youth in the RT. He described his insight into the persona he was trying to project and how this manifested at the RT: I wanted to like people to be afraid of me and like behaviors I displayed here [at RT] at certain points of time did work to my favour . . . Like yelling at someone, . . . them afraid of me and what I might do to them like it wasn’t healthy. Like farthest thing from it. (Y14)
This participant’s insight into his efforts to protect himself from revictimization by becoming an unpredictable aggressor began with him understanding his media consumption and extended to his offline social interactions. The youth stressed that his exposure to graphic content had decreased significantly but had not yet been eliminated at the time of the interview. He attributed this motivation to find alternative ways of coping to the supportive way the RT staff approached him and his problems, which included having digital media access: I guess as I got older, they didn’t want it to be like a battle and plus my behavior did gradually change over time so that’s a reason they allow me to have my phone . . . I would say that that was a good thing because it built the habit up to monitor myself instead of having someone else to do it. (Y14)
He stated that he was working hard to find more life affirming and adaptive coping strategies when confronted by trauma triggers and feeling under threat in social situations.
For youth in programs that limited recreational media participation, having access had to be requested and negotiated. Two youth (one who was a professional online video gaming team leader and one who had a popular mental health wellness recovery Instagram account) advocated for daily internet access to continue activities, which they believed helped them to maintain wellness and self-esteem. After reviewing each request thoroughly, the respective programs approved the requests, which meant allowing greater access. For example, while the professional gamer agreed to be in the RT in order to help her re-establish routine and regular school attendance, she did not want to lose access to digital media. With the support and understanding of her parents, this youth was able to advocate for daily access from the time of her admission to RT. She described how participating in treatment was contingent on having regular access: So, I was like, “I will not come to this program if I do not have the opportunity to work,” . . . so yeah, I wanted to keep my job. So that’s how I got that [permission]. As well as the fact that I’m significantly older because I’m 17 almost 18 . . . And my parents are also like really good at advocating for it. They’re like, “No we get it now. We used to be like you,” which is helpful. (Y49)
This youth explained that having internet access contributed to her feelings of purpose and allowed her connection to peers who depended on her leadership, and this increased her self-esteem: I like taking on leadership roles those make me happy. . . . Even if it’s stressful . . . I feel like I can cope pretty well under pressure. I tend to play really well under pressure . . . so it all kind of fits together. (Y49)
The social connection and responsibility to others coupled with income were important to this youth, It’s just it’s important to keep my job. I like having money and I like my team a lot. I think they are . . . counting on me to pull through and I’m counting on them . . . they’re very good and so I want to in return do that too. (Y49)
As someone who was struggling with a myriad of complex mental health and learning issues as well as stigma, digital media access was understood to be critical to maintaining the strengths and gains she had made.
The participant with 3,000+ Instagram followers on her mental health wellness and recovery account regularly posted inspirational, and informative content offering teens coping skills and motivation to stay safe and well. This teen was anonymous on her account and reported that she avoided all social media engagement with her friends. She found social media activity anxiety-provoking and was distressed by observing others being cyberbullied. Her Instagram activities were specific and focused on the wellness of others and herself. She felt understood, trusted, and supported by the RT staff who allowed her digital media access: I do have access to my phone. It’s kind of like an exceptional case. . . . I want to use my Instagram during the time that I’m here just because it’s so helpful for me and they kind of said, “We trust you. Let’s do it, let’s try it.” (Y26)
At the same time, this participant reported valuing the disconnection which the program provided, outside of her daily Instagram use, “And it’s nice to realize that you can live your life without your phone being God” (Y26).
These examples highlight how digital media use can complement identity development, treatment, and civic engagement while in RT. These youth advocated for themselves or had a treatment plan that was implemented to attend to the ways digital media use was related to their difficulties. Not all participants advocated for digital media use access. Many participants, however, reported that the digital media use rules and limits actually helped them become aware of the dominant role of the internet and cell phones in their lives. This was most notable in relation to social media. One youth stated, “I had to be a part of social media and now I care less about that being in residential. Like I feel like my priorities have been put in check a little more after having a phone less” (Y48). Some youth reported that not having immediate access to their phones resulted in using digital media in moderation and in a more intentional, rather than automatic way: I used to be on it all day, but I was also pretty bored of it too . . . It just became a whole lot more enjoyable since I’ve been away from it so long. Kind of being here kind of feels like somewhat of a rehab from like the internet . . . I still watch long videos, but I don’t really binge watch them as much anymore. (Y24)
Another youth reported that not having access to their device at the RT program forced them to engage with others and address their social anxiety and chronic boredom, “I was bored a lot, but I didn’t know exactly why . . . Then in residential . . . I was able to work on social skills and stuff be able to not be bored. But there was definitely an adjustment period” (Y21). This youth described gaining capacity to self-regulate digital media use after participating in the day program, once they returned home. “My mom used to have to take away all my electronics every night. Now I can be trusted on my own. Yeah, definitely helped me” (Y21). Within this theme, youth explained that having internet access and limits at different stages of their treatment contributed to them gaining self-awareness, increased capacity for emotion regulation and engaging in online activities in a more purposeful and mindful way.
Discussion and Implications
Promoting the Five Cs of Positive Youth Development Through Digital Media Use Among Youth in RT
Positive youth development emerged from the analysis as relevant to how youth navigate both their self-defined challenges with digital media use and how digital media and online contexts were catalysts for their developmental growth. The findings of this study demonstrate that to varying degrees, digital media use among participants facilitated elements of the five Cs associated with positive youth development: connection, confidence, competence, character, and caring (Gustavsson & MacEachron, 2015; Lerner, 2005). The participants’ narratives indicated that through their online activities, they were able to transcend their mental health challenges and view themselves as active members of society. Within this sense of social connection, they were able to gain confidence, exercise competence and express their character and caring for others. Maintaining connection emerged as a central motivation for digital media use, as it linked youth in RT to people, information, and resources. These connections included family and friends as well as online communities with shared values and experiences. According to participants, information that was available online was critical in increasing their social awareness and in promoting a sense of connection to communities of caring and compassion such as the vegan community as well as online mental health promotion and recovery groups. This finding is consistent with studies addressing the role of digital media use among other marginalized youth populations, such as those with mental health difficulties, disabilities, and LGBTQ2S+ (Belfort & Miller, 2018; McInroy, 2018; Vural et al., 2015). As Davis’ (2013, 2017) research has highlighted, digital media is used as a platform for both social and relational connections and affiliations as well as supporting identity development among youth. The digital domain has become a primary context and tool for adolescent development.
Beyond connection, the participants reported that digital media use facilitated opportunities for them to build confidence and demonstrate their leadership, competence and caring. For example, one participant employed as a gaming expert and team leader with LGBTQ2S+ online peers, applied gaming skills that she developed through hours of online gameplay, to enhance her sense of confidence, character, purpose, and well-being. Despite the problems associated with gaming overuse reported in the literature, online video game playing has been associated with positive youth outcomes (Adachi & Willoughby, 2017). Research has emphasized the importance of optimizing health promotion among youth in RT through a focus on resilience and positive youth development (Baber & Rainer, 2017). An example that corresponds to this outcome was youth who used Instagram to solicit and contribute to mental health wellness and recovery content.
Findings indicated that connecting to causes other than mental health was facilitated through digital media, which is consistent with research that identifies digital media as a pathway for civic or community engagement and positive youth development (Middaugh et al., 2017). An instance of such an outcome was the participant, who during her time in RT, shifted from engaging with pro-self-harm, and pro-eating disorder online communities to becoming involved in environmental and animal protection and veganism groups. The findings of the current study suggest that digital media use was an important means for the participating youth to address marginalized and stigmatized components of their lives and maintain pre-existing strengths while developing adaptive pro-wellness focuses that extended to actively caring for others, and demonstrating character and confidence to assert and share their values. The online activities described by several of the participants contributed to promoting the five Cs of positive youth development—connection, competence, confidence, character, and caring.
The youth reported that digital media was important to support their wellness and yet recognized that it could also negatively affect their well-being. This mixed finding is consistent with a recent study addressing digital media practices and youth well-being. Rideout et al. (2018) reported that overall youth do not see digital media as either harmful or beneficial to their well-being. In comparison to the overall sample of youth, those who were reported to have moderate to severe depression stated that digital media was both highly important to maintaining their well-being and negatively affected their well-being. While all youth noted using digital media to address health and wellness, those who reported moderate to severe depression were twice as likely to use digital media to seek support with mental health (Rideout et al. 2018).
A number of participants in the current study expressed that digital media use during times of mental health difficulties contributed to their problem behaviors and mental distress. This was particularly evident among the youth who reported exposure to online images related to self-harm. These participants shared that although they knew their digital media use was harmful to them, they continued to engage with the content. This finding is consistent with research that found that despite knowing the activities were harmful to their well-being, youth with depression symptoms were more likely than youth without depression symptoms to continue to use digital media use in ways that were not helpful (Rideout et al., 2018). In Rideout et al’s study, those youth without symptoms of depression were more likely to adapt their online use in ways that protected themselves.
Access to Digital Media and Digital Disconnections Can Support Wellness
The current study findings demonstrate that the youth described conflicted experiences in response to varying degrees of digital media restrictions. Those in programs with limited access to social media and news could feel isolated and uninformed about the world. These same youth, however, identified benefits to these restrictions such as gaining insight into their treatment issues. According to the participants’ narratives, experiencing a digital disconnection facilitated this awareness of the relationship between digital media use and well-being. This suggests that despite resistance, youth in RT can benefit from some digital media use restrictions or limitations to access. Digital media was revealed to be a means through which youth could avoid or distract themselves from their distress. The restrictions to digital media use access required youth to remain tuned into their discomfort and use the RT staff for support in order to apply coping skills other than using digital media.
Although digital media can be an important resource, the findings suggest that youth can benefit from a digital media disconnect as a way to strengthen their emotion regulation capacity without their default reliance on digital media. Moreover, these findings suggest developing insight into the relationship between online activities and behaviors with mood, anxiety, and cognition can be facilitated within RT regardless of internet access. The therapeutic benefits to restricted digital media use access during treatment have been reported in previous studies related to youth in RT and in other out-of-home placements (Anderson, 2017; Collier & Gavriel, 2015; Good & Mishna, 2021; Sanders et al., 2017). Like the youth participants in this current study, however, Good and Mishna (2021) found that youth reported feeling isolated and experienced increased anxiety in response to digital media restrictions. Efforts to safeguard youth from danger and harm can have unintended psychological consequences. For example, a study addressing the impact of separating high-risk youth (online and offline) from anti-social peer groups found both positive and negative outcomes (Sanders et al., 2017). This was described as a peer paradox phenomenon whereby disconnecting from anti-social peer affiliations to prevent risky behaviors and harm resulted in increased depression and loneliness (Sanders et al., 2017).
According to youth participants, the value of a digital disconnect was balanced by their equal assertion that some digital media use access was important to help them feel connected and to normalize their identity as teenagers. The significance of normalizing the experience of youth in out-of-home settings has been well documented in the literature and now applies to youth digital media use and access (Badillo-Urquiola et al., 2017; Hammond et al., 2018; Nicholas & Chahauver, 2017; Schuurmans et al., 2018). From the perspective of the participants, it is important for youth in RT to see the light at the end of the digital media use restriction tunnel. Moreover, participants stressed the need to consider age and treatment stage when determining or changing levels of access. Attending to the individual needs, benefits, and risks for each youth can help determine the program’s approach to digital media use access and supervision beginning at intake and assessment (Denby Brinson et al., 2015; Good & Mishna, 2021).
Furthermore, the practicality and feasibility of restricting digital media use are other important considerations. In the current study, older youth participants were more outspoken about the limitations of universal restrictions, disclosing that they did not abide by these restrictions. These participants added that they were concerned about younger youth who were actively engaged in risky online activities. Consistent with this report, service providers in a recent study (Good & Mishna, 2021), reported that youth in RT sneak access to Wi-Fi and cell phone data while in RT programs. Prohibition of digital media access may inadvertently create situations that could increase risk or preclude opportunities for supporting these youth.
The youth participants in the current study suggest that it is complicated to offer internet access and to restrict internet access, with complex and individualized implications for youth well-being. RT service providers may consequently need to assume that all youth in RT will have some degree of access, reinforcing the need to address youth digital media safety regardless of program access rules and expectations. Consistent with a harm reduction approach to digital media access, the approach recognizes that youth in RT belong to the digital world and assumes they require preparation to participate safely both during RT and following discharge to their homes. This approach can facilitate improved safety and generate open discussion between staff and youth. Many youth participants reported they remained connected with concealed mobile devices in spite of program rules.
Treatment Implications: Integrating Treatment Goals and Digital Skills
Residential programs are adapting to the needs of youth in an increasingly networked society. Programs and service providers are tasked with facilitating online opportunities for social connection, learning and digital skill development while safeguarding youth from harm. Although youth were asked about their digital media use in their respective RT programs, responses to these questions focused on individual online activities and motivations for these activities. Some participants reported that they played video games and watched movies with peers and staff. There was a striking absence of participants describing examples of treatment activities using digital media or addressing digital media safety and skills and attending to peer conflict associated with cyberbullying. There were isolated reports, however, of staff supporting youth with anxiety and frustration related to not having digital media access during their time in RT. Despite the fact that some participants received support for internet-related issues, and others successfully advocated for access to social media, and gaming platforms, there remains a gap in access and opportunity for many youth in RTs. The absence of digital media-related RT programming reported by participants demonstrates that addressing youth digital media use in RTs remains in its infancy within the four participating programs.
According to participant reports access to the internet and capacity for digital media use was a central theme in their lives prior to and during their time in RT. Based on what the youth participants assert, it is important that youth in RT not be completely restricted from digital media use, with the exception of crises (at which time they require containment to remain safe). Some access to personal devices and unsupervised Wi-Fi use along with individualized plans for youth in more restrictive RT help youth to be more amenable to accepting the rules and benefiting from the insights generated through participation in RT (Good & Mishna, 2021). The current findings support the application of a harm reduction approach, which attends to the varying degrees of risk among youth in RT. Moreover, offering formal skill development to youth presenting with increased online risk has been recommended. These findings are further supported by the research of Vissenberg and d’Haenens (2020), which reported that youth experiences of online harm can be mediated with empowerment-based approaches to digital media resilience building. As illustrated in the findings and recommendations, while increased degrees of adult support may be needed at times for individual situations or particularly vulnerable youth, supporting them to problem solve as they navigate online opportunities and confront harmful content is recognized as an effective approach. These skills include a combination of digital literacy skills, interpersonal skills, and emotion regulation strategies to address the technical, relational, and emotional elements of digital media use (Denby Brinson et al., 2015; Gustavsson & MacEachron, 2015; Pridgen, 2010).
Gustavsson and MacEachron (2015) recommend addressing the heightened online risk among youth in out-of-home child welfare placements through a collaborative approach between youth and service providers. This approach can address the unique needs of each youth by balancing risk prevention (e.g., restrictions to unsupervised online access) with risk resilience (e.g., facilitating online access through harm reduction). Necessary formal skill training in digital literacy and citizenship can be incorporated in a harm reduction approach to facilitate online positive youth development. Digital literacy concepts include critical thinking, such as how to evaluate the accuracy of information sources and protect oneself and one’s personal information while participating within online platforms (Mihailidis, 2014). Digital citizenship relates to one’s capacity to follow the norms of online behavior or etiquette, respect the rights and responsibilities of online participation and have a sense of communal or civic belonging or membership (Media Smarts, 2013). The characteristics of digital citizenship can help youth consider what and how they communicate in online community chat groups.
Applying digital skills with a focus on treatment goals can increase the effectiveness of youth digital media use safety. Pridgen (2010) suggests that engaging youth in RT with core treatment goals, such as emotion regulation, understanding, and navigating relationships and boundaries, and determining how to effectively access and solicit support can be facilitated through a focus on their digital media practices. Pridgen (2010) contends that treatment approaches such as dialectical behavioral therapy (often adapted for RT) can be applied to youth digital media use and in turn, support increased safety online by targeting their strengths and needs. Core modules of dialectical behavioral therapy for adolescents include mindfulness practices, distress tolerance, emotion regulation, and interpersonal skill development (Linehan, 1995; McCredie et al., 2017), all of which can contribute to more effective digital media use for youth.
Addressing a combination of digital media skills and promotion of treatment goals can complement contemporary family-centered therapy in RT, addressing the needs of youth both in the RT and during home visits (Johnson et al., 2015). For example, during weekend home visits, it was common for youth to have access to digital media and it was an opportunity for them to observe their own digital media use habits and the effects on their well-being. Promoting mindful digital media use through self-awareness and reflection at the RT following home visits coupled with family therapy and parental support to establish digital media use norms for weekend visits can bridge the gap between weekend access and weekday program restrictions. Moreover, this approach provides collaboration and psychoeducation for parents pertaining to both digital media use safety and digital literacy and encourages parental limit-setting and consistency with their child. This approach is consistent with the shift toward more ecologically informed collaborative, family, and community-based approaches to intensive services for youth (Johnson et al., 2015).
Limitations
While the constructionist theoretical approach applied to this qualitative study privileged the voices of youth and approached the topic of digital media in RT from their perspective, a limitation of this approach includes not providing diagnostic classifications and demographics due to privileging youth self-descriptions. Moving forward, quantitative research would be beneficial to provide information on youth in RT’s treatment characteristics. Another limitation is that the demographic profile of youth in the study does not reflect the high representation of Black, Indigenous, and people of color (BIPOC) often found within youth out-of-home placements associated with child welfare agencies which support youth with mental health problems (King et al., 2018). This study took place in a province in which mental health services are separate from child welfare, and consequently, the participants do not reflect the over-representation of BIPOC in child welfare, out-of-home placements within Canada (Blackstock et al., 2020; Pon et al., 2011). Future research that is able to capture these systemic realities of overrepresentation of populations in intensive services would be important to better understand the experiences of digital media use among BIPOC youth with mental health and behavioral challenges.
There was a disproportionate number of older youth between 16 and 18 years in the study sample. While the older youth shared experiences from their younger years, the voice of youth between 13 and 15 years is underrepresented. Gaining parental consent from youth in RT contributed to the skew in the sample age. It would be beneficial to gain an understanding of this younger population’s experience with digital media use prior to and during RT. Another limitation associated with data collection was related to the level of comfort youth participants had with disclosing risky online activities. The youth in programs with more digital media use restrictions were less inclined to disclose risky online activities, which may have related to concerns that the confidentiality associated with the study would not apply if they disclosed harm associated with their digital media use. A future consideration is for researchers to conduct the interviews post-discharge, on weekends at the homes of the youth or at off-site locations. This may allow youth to feel less concerned about disclosure of risk having an impact on digital media access during treatment.
Conclusion
The study findings contribute to a small but growing body of literature focused on digital media use among youth within RT contexts. While a previous study by Good and Mishna (2021) focused on the experiences of service providers, the findings from this study address the gap in the literature by providing descriptions of digital media use from the perspective of youth in RT. The study findings demonstrate that digital media use among youth in RT offered pathways toward positive youth development such as connection, wellness, agency, and confidence. Digital media access helped some maintain pre-existing strengths while for others, internet access acted as a catalyst toward positive youth development online. Despite the benefits reported, some youth identified increased potential for harm associated with internet use prior to RT. Youth identified that a digital disconnection was needed for them during periods of mental health crisis and heightened experiences of risk. According to the participants, they gained insight into the association between digital media use and their emotional well-being, even during limited access to digital media. This suggests that youth digital media use can be addressed and understood during a digital disconnect as well as when the youth have varying degrees of access.
For youth with problematic digital media use, the promotion of wellness and safety can support youth to shift their coping strategies by aligning with pro-recovery rather than self-harm and pro-self-destructive content. Likewise, online skills that youth develop can generate pathways to agency and confidence that can be transferred to a future focus on employment or education pathways. Among the youth in the current study, digital media use was a vehicle for positive youth development, which many of them initiated prior to entering RT. Recommendations made by youth participants emphasized the importance of attending to the unique needs and characteristics of the individual. The participants communicated a clear and overarching message that pre-existing coping offered by digital media use should not be removed, rather, RT programs should work with youth to identify risk factors and facilitate needed social-emotional and digital skills to decrease risks online. It is, therefore, important for service providers to engage youth in conversations related to the role of digital media use in their lives, including how it may obstruct and facilitate wellness.
Footnotes
Appendix
Interview Guide.
| Interview guide for youth |
|---|
1. I have called internet activities “digital media use” (DMU) what words to you used to describe what you do with computers, phones, and other devices connected to the internet? 2. Can you tell me a bit about your DMU (use youth language if provided: these are the things you like to do with internet-based technology on mobile devices and computers)? 3. What kinds of things do you do online? (prompt: social media, look up information like weather, look at maps to get directions, etc.) 4. When did you start using internet-based apps, games, communication tools? 5. What kinds of devices do you used to get online and do the things you do? |
6. What kinds of things did you do online before you came into residential treatment (RT)? (prompts if needed) ○ What were the things you did the most? Do you look up information like weather? ○ Did you look at maps to get directions, etc.? ○ Did you use technology and internet to communicate with friends and family? ○ Did you stay connected to friends from previous placements or programs? ○ Did you play games, listen to music, watch TV, videos, films? ○ Did you search for information on health or sex Ed. or mental health? 7. Now that you are at (name of program), what are DMU things do you do the most? (Repeat prompts if needed). 8. How often would you do these activities before you were at (name of program)? (repeat prompts if needed) (also, are there other activities?) 9. Now that you are at (name of program), How often do you do these activities? |
| 10. Before coming to (name of program) How long would you do these activities on a given day? 11. Now that you are at (name of program), how long do you do these activities for on a given day? 12. Before coming to (name of program), were there things you were not allowed to do? (prompts if needed) ○ If so, what were these things/activities? ○ Did you do them anyway? (why)? ○ If so, who did not allow you to do these activities? 13. Now that you are at (name of program), Are there things you are not allowed to do? ○ If so, what are these things/activities? ○ Do you do them anyway? ○ If so, who does not allow you to do these activities? 14. Before coming to (name of program), how did your technology use (list of participants activities) make you feel? For example, emotionally or about yourself? ○ What kind of mood were you in when you want to go online to do (list of participants’ activities). ○ Did interacting with x make you feel a particular way? 15. Now that you are at (name of program), how does your technology use (list of participants activities) make you feel? For example, emotionally or about yourself? ○ Now that you are at (name of program)what kind of mood are you in when you want to go online to do (list of participants activities)? ○ Now that you are at (name of program), does interacting with x make you feel a particular way? 16. Can you tell me about some of your positive experiences? (from before the program, and from now while in the program)? 17. Can you tell me about any negative experiences that happened? (from before the program, and from now while in the program)? |
| ○ How did you respond? What did you do about the negative experiences? (from before the program, and from now while in the program)? 18. Do you think that adults (like parents, therapists, and teachers) understand what digital media participation (DMU) or internet-based activities means to youth (use participants’ words)? ○ How did these adults respond to your digital media participation that let you know that they either understood or did not understand what DMU means to you? 19. Have you had any internet safety instruction (e.g., how to keep your information private, how to deal with strangers who (contact, bully, want to be friends)? Can you tell me how it has been helpful (or not)? |
20. You mentioned you were (age when first went online) years old when you started to use the internet. How has your DM use (use participants’ words) changed as you have gotten older? ○ Probe: do you use different apps, play different games, look up different kinds of information, and use more or less social media? 21. What do you think made you change the types of activities or apps as you got older? |
22. Can you tell me what the rules are about DMU, bringing and using technology devices to (residential program name)? ○ Are the rules that you read and agree to when you are admitted to the program the same as what actually happens when you are in the program? If no, how so? |
| 23. What do you think about the technology and internet access rules at (residential program name)? ○ Why do you think these rules are (good, bad, confusing, unfair, reasonable, etc., what the participant has stated)? 24. Is removing access to devices and Wi-Fi, and the internet ever used as a consequence at (program name)? 25. Are there rules that could change to make things better? ○ Are there rules that could be added or removed? Please explain. 26. Has your device or data ever been stolen while at (name of program)? 27. What do you think are some positive things digital media use can offer to youth in RT? 28. What kinds of problems do you think Digital media use can create for youth in RT? 29. Have you had any groups, lessons, or classes about internet safety or how to avoid risks online? Where did it take place? 30. Do you ever go to staff for support about internet-related questions, problems, opportunities you want to access? If so, what happened? 31. Do your peers in the program ever go to staff for support about internet-related questions, problems, opportunities you want to access? If so, what happened? 32. What kinds of digital media participation support do you think would be helpful for youth in RT? |
33. Thank you for meeting with me and providing so much information. Is there anything more you would like to share with me about digital media use that I have not asked about? |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.