
Abstract
Despite extant research suggesting the important role of family in supporting youth with disabilities (e.g., learning disabilities) making the transition to university, family relational influences on youth with mental illness undergoing this transition remains unclear. Adopting a family resilience perspective, this mixed-methods study aimed to examine (a) how parent-child relationship factors relate to youths’ mental illness symptoms and well-being and (b) youth and parent perspectives on how parents can best support youth in this transition. A total of 225 youth with mental illness (aged 17–23, M = 18.43, SD = 0.91, 87% white) completed questionnaires assessing parent-child relationship satisfaction, depressive and anxiety symptoms, and life satisfaction. For 22 of these youth, a parent (aged 45–57, M = 49.77, SD = 3.57, 100% white) completed questionnaires assessing caregiver burden and reward. Parents (and their child) completed written responses addressing what youth most need from parents during this transition. Parent-child relationship factors were moderately associated with youth mental illness and well-being. Thematic analysis indicated much agreement and some difference between youth and caregivers on the aspects of parental support most valued during this transition. Implications for supporting such youth as they adapt to university are discussed.
Keywords
The transition of a child to university often represents a major shift in the family life cycle (Mattessich & Hill, 1987) with children embarking on a “launching process” and perhaps living away from home for the first time. Families 1 must adjust to changes in routines and relationships, along with the youth facing a host of new demands inherent to being a university student (Pitt et al., 2018; Wintre et al., 2011). For families in which a child has a pre-existing mental illness, the ability to successfully manage this transition is multifaceted, with the normative stressors of student life compounded by managing their mental illness and/or recovery (Auerbach et al., 2016; Davis & Vander Stoep, 1997). From a family perspective, youth are expected to be less dependent on parents and to take on increasing levels of autonomy (e.g., living away from home, managing professor-student relationships, self-advocacy with regards to mental illness). The clash between blossoming youth autonomy and ongoing family involvement may be especially marked given that caregiver involvement is established to be more intensive for youth with disabilities than for typically developing youth (Wagner et al., 2005).
Parenting during this period of development is marked by unique challenges (e.g., university environment which tends to exclude parent participation, increased parental distress about their nonresident child’s well-being, and changes in child autonomy regarding decision-making). These challenges may upset the equilibrium within the family system with commensurate impact on caregiver perspectives (e.g., caregiver burden and caregiver reward) and youth well-being (e.g., symptoms of mental illness, indicators of positive functioning). Despite the increasing number of youth with mental illness attending university (Auerbach et al., 2018), little research considers the impact of family-level factors (e.g., the parent-child relationship, caregiver burden/reward, parental support) on these youth and their well-being. Such research may contribute to knowledge regarding both family and youth resilience during this important developmental phase, as well as provide recommendations for families and university settings increasingly grappling with how to best support (and prevent negative sequelae for) these youth.
Transitions to Adulthood for Youth with Mental Illness
Research on the transition to university for youth with mental illness is sparse. However, extant work on this transition among youth with other disabilities, including autism (Defur et al., 2016) and learning disabilities (Smith et al., 2002), underscores the important role of family relationships and supports in promoting a successful transition. Furthermore, the broader research on families of youth with mental illness navigating the transition from adolescence to young adulthood suggests that this period in the family is often marked by distress, anxiety, and challenges for parents and youth alike (Davis & Butler, 2002; Vander Stoep et al., 2000). In their national survey of parents of youth with “serious emotional difficulties” transitioning to adulthood, Davis and Butler (2002) found that a lack of information regarding available services or resources for their child at this stage of development was identified as highly frustrating for parent participants. Also, families often felt jettisoned from their child via institutions and services that did not “sufficiently or appropriately include parents” (Davis and Butler, 2002 p. 18). In another qualitative study of parents of youth with mental illness making the transition to young adulthood, parents reported feeling that service providers under-utilized parents as an important resource to promote youth well-being (Jivanjee et al., 2009). Traditionally, university environments have been quite disparaging of parental involvement in student life (Agliata & Renk, 2008). Such a stance may be particularly problematic for youth with mental illness, as caregiver support and relationships may be important resources both to promote youth well-being and to protect against negative outcomes (e.g., substance use, drop-out).
Parent-Child Relationships and Youth Well-being
Parent-child relationships may be an under-recognized and potentially under-utilized protective factor for youth with mental illness attending university. Broadly, the quality of these relationships are well-established to have important implications for youth functioning (e.g., McLeod et al., 2007; Pettit et al., 2001) and for university youth specifically, contribute to more positive student outcomes (Kenny & Donaldson, 1991; Wintre & Yaffe, 2000). Despite this, the particular impact of parent-child relationships for students with mental illness remains unclear. From a foundational perspective, examining the relation between parent-child relationship satisfaction and youth functioning for these students would begin to better illuminate this potential protective factor.
Another aspect of the parent-child relationship which may influence students with mental illness is the caregiver experience of caregiving burden and reward. Researchers postulate that the well-being of children with mental illness highly depends on parental ability to adapt to the role of caregiving (Anuradha, 2004), as is seen in families dealing with children’s physical illnesses (Thompson & Gustafson, 1996). Decades of research have shown that caring for a family member with a mental illness can create a significant burden for caregivers (e.g., Mitsonis et al., 2012; Nehra et al., 2005). In contrast to mental health professionals, family members who face the challenge of caring for a relative with a mental illness typically have no formal training, are “on call” at all times, and are emotionally connected to the individual they are caring for (Wing, 1982). This can result in both subjective burden (i.e., the caregiver’s personal appraisal of burden; Heru, 2000; Ricard et al., 1998) and objective burden (i.e., the observable forms of burden; Scheirs & Bok, 2007). Higher levels of burden have been associated with less-effective parenting practices, poorer family relationships, and lower-quality care (Athay, 2012; Gerkensmeyer et al., 2011), all of which may have a significant impact on youth well-being.
Despite the challenges, sacrifices, and disruptions that are associated with caring for an individual with a mental illness, many caregivers also report experiencing caregiver rewards (i.e., positive outcomes related to this role; Bauer et al., 2012; Heru & Ryan, 2004). From a family resilience perspective, caregivers whose perspectives encompass a compassionate view of child strengths, satisfaction from fulfilling their parental duty, and a deeper understanding of life priorities (i.e., caregiver rewards; Schwartz & Gidron, 2002) may contribute to promoting a resilient process within their families. Examining relations among caregiver burden/reward and aspects of youth functioning may be important for understanding resilience in the transition to university for youth with a mental illness, as well as their families (Greeff et al., 2006; Nehra et al., 2005).
The family resilience perspective emerges from family stress theory (Boss, 2001) and considers “protective factors and processes that moderate the relationship between a family’s exposure to significant risk and their ability to show competence in accomplishing family functions” (Patterson, 2002, p. 356). One such important family function is the ability to successfully launch child members into an increasingly independent adult role (e.g., attending postsecondary institutions). Family relational patterns are a key aspect of understanding both family and individual-level resilience (Walsh, 2012) and may illuminate how a family navigates stressors that occur at major transitions within the family life cycle (Patterson, 2002).
Capabilities and Coping: What Youth Need During this Transition
Another aspect of family resilience are a families’ capabilities in the form of resources (e.g., financial stability) and coping practices (e.g., providing emotional support). With regards to families in which a youth with mental illness is transitioning to university, little is known about what youth and their caregivers believe is most required for the youth to be successful during this launching process. Extant research in typically developing samples has suggested that while having highly involved parents is related to positive student outcomes (e.g., student engagement, life and college satisfaction, social development; Shoup et al., 2009), having overly involved and/or controlling parents (i.e., helicopter parents) is associated with negative student outcomes, such as decreased well-being and increased psychopathology (e.g., Schiffrin et al., 2014). At the same time, the level of parental involvement that is beneficial in the context of managing a mental illness in university may be different than for general student populations. Extrapolating from research on youth with other disabilities (e.g., Defur et al., 2016), youth with existing mental health difficulties attending university may have unique or more intensive parenting needs. Parental involvement and support must also be considered within a campus environment that typically strives to promote autonomy of its students and often struggles with how to address the role of parents (e.g., parent requests for information/advocacy on behalf of their child). In fact, there has been a growing concern and negative perception among postsecondary administrations regarding parental involvement in their youth’s university life (e.g., Hunt, 2008; Somers & Settle, 2010). Thus, understanding the role that parents may play in promoting positive outcomes for youth with mental illness attending university stands to contribute important knowledge for parents, youth, and campus support services regarding appropriate parental support for this population.
The Current Study
In line with Patterson’s (2002) recommendation for family resilience research, the current mixed-methods study focuses on families experiencing significant risk in the form of a transition to university for a child member with an extant mental illness. It is under such risk conditions that a family and individual resilience processes may be operative (Patterson, 2002). This study thus aims to further understanding of parent-youth relationship variables (i.e., parent-child relationship, caregiver burden/reward) and their association with youth well-being for these families. Although families have been historically sidelined by the traditional university constellation of supports, family relationships may continue to play an important role for these youth. By examining lived experiences of youth and their caregivers from a resilience perspective, this research aims to contribute a broader understanding of how parental involvement/support may affect the well-being of these youth and their families.
To accomplish these aims, this study examines the following research questions: (a) How does parent-child relationship satisfaction relate to youth’s experience of mental illness (i.e., depressive and anxiety symptoms) and well-being (i.e., life satisfaction)? Within dyads in which both a parent and their child participated in the research, two additional questions were examined, (b) How does the caregiver’s experience of reward and burden relate to their youth’s experience of mental illness (i.e., depressive and anxiety symptoms) and well-being (i.e., life satisfaction)?, and (c) How can parents best support their youth with mental illness while at university? Based on previous research, it was hypothesized that higher parent-child relationship satisfaction, as reported by youth, would be associated with lower levels of symptomology and higher life satisfaction. Across informants, it was also hypothesized that lower levels of caregiver burden and higher levels of caregiver reward would be associated with greater youth endorsement of life satisfaction and lower youth psychopathology. Finally, given that limited research has considered the supports that may be most beneficial to youth with mental illness as they transition to university, the final research question was exploratory with no specific hypotheses determined a priori. This study seeks to give voice to the perspectives of both youth and their parents using qualitative methods.
Methodology
Participants
Participants were university students recruited for a larger study through a public university’s introductory psychology course participant pool. Potential participants (N = 441) were screened for young adults (age < 26) in their first or second year of university who reported having a diagnosed mental illness. The resulting sample of 225 students were aged 17 to 23 (M = 18.43, SD = 0.91) with the vast majority of participants reporting their race as white (n = 195, 87%). See Table 1 for sample characteristics of the larger youth sample as well as the characteristics of the subset of youth whose parent also participated in this study.
Sociodemographic characteristics for the full sample of youth (n = 225) and the subsample of youth with participating caregivers (n = 22).
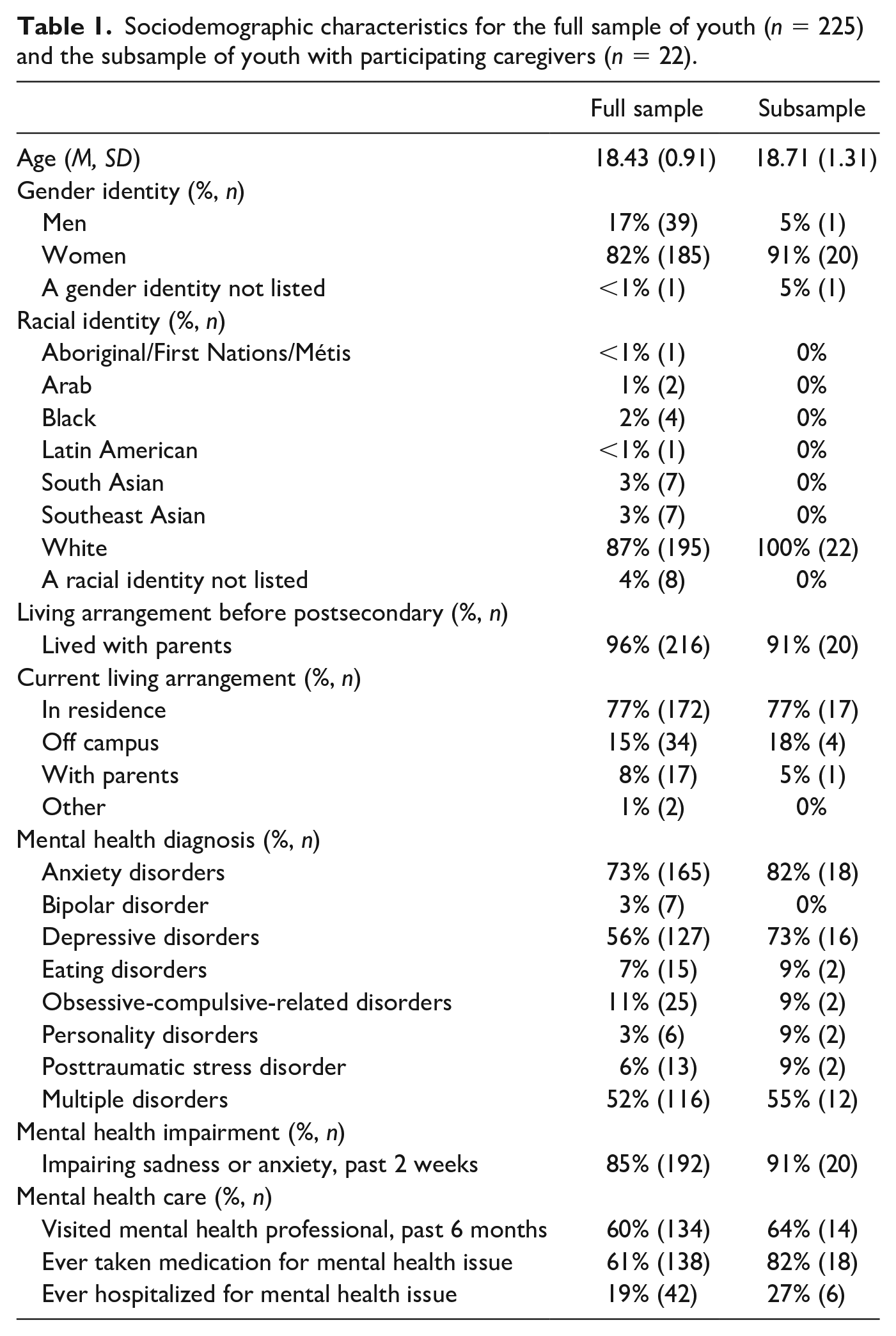
Of the 225 youth participants, 67 consented for parents to participate and provided contact information. Of the parents who were contacted, 22 participated in the study. The caregivers were aged 45 to 57 (M = 49.77, SD = 3.57). Parents’ gender identities were men (n = 3, 14%) and women (n = 19, 86%). Parents endorsed the following relationship statuses: in a relationship (n = 2, 9%), married (n = 17, 77%), single (n = 1, 5%), and a relationship status not listed (n = 2, 9%). All parents identified as white (n = 22, 100%). Parents indicated the following as their highest level of education: high school (n = 3, 13%), college or university (n = 13, 59%), graduate school (n = 5, 23%), and a professional degree (n = 1, 5%). Students with versus without participating caregivers were compared. There were no significant differences other than those with participating caregivers were more likely to be female and to use medication for a mental illness (p values < .05).
Measures
Mental health screen
The Mental Health Questionnaire (Lumley & McArthur, 2016) is a 9-item questionnaire examining self-reported recent history of contact with mental health professionals, use of medication to treat mental health issues, and mental health diagnoses. Eight items are answered in a “yes” or “no” format and one question asks to indicate frequency of contact with a mental health professional.
Parent relationship satisfaction
To assess satisfaction with the parent-child relationship, student participants completed a modified version of the Relationship Assessment Scale (Hendrick, 1988), adapted to be appropriate to nonromantic relationships (RAS-G; Renshaw et al., 2010). The RAS-G is a 7-item self-report scale, with each item scored on a 5-point scale ranging from 1 (Not Satisfied) to 5 (Very Satisfied) (e.g., How well does your caregiver meet your needs?). The modified version has demonstrated good internal consistency, item reliabilities, test-retest reliability, and factorial validity across various close relationships (Renshaw et al., 2010). In this study, the Cronbach's alpha was .89.
Caregiver burden
Objective and subjective burden associated with caring for a child with mental illness were assessed using the 19-item Burden Assessment Scale (Reinhard et al., 1994). Participants rated the extent to which they have experienced each item related to caring for a child with a mental illness within the past 6 months on a 4-point scale ranging from 1 (Not at All) to 4 (A Lot) or 0 (Not Applicable) (e.g., “Because of your child’s mental health challenges, to what extent have you found it difficult to concentrate on your own activities”). Higher scores on this measure indicate higher levels of burden. The Burden Assessment Scale evidences adequate internal consistency, content and construct validity, reliability, and sensitivity to change over time (Reinhard et al., 1994). In this study, the Cronbach's alpha was 0.91 for total burden.
Caregiver rewards
The caregiver’s perceived rewards associated with caregiving were assessed with 10 questions adapted from Green’s (2007) measure of perceived benefits of mothering a child with a disability and based on the authors’ suggestions for additional items to apply to caring for a youth with mental illness. Caregivers were asked to indicate the degree to which they agreed with each statement on a 5-point scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree), with higher scores indicating higher levels of reward (e.g., “The pride and joy my child feels with each accomplishment makes all the work I do worth the effort”). In this study, the Cronbach's alpha for caregiver rewards was 0.78.
Youth psychopathology and well-being
These variables were assessed via youth self-report. Youth depressive symptoms were assessed using the Beck Depression Inventory-II (BDI-II; Beck et al., 1996). The BDI-II is a widely used 21-item self-report scale designed for individuals 13 years of age and older to assess the number and severity of depression symptoms over the preceding 2 weeks (e.g., “loss of pleasure”). Each item contains four statements scored on a 4-point scale with higher scores indicating higher severity of depression symptoms. The BDI-II evidences high internal consistency, test-retest reliability, and construct validity (Beck et al., 1996). In this study, the Cronbach's alpha for the BDI-II was .92.
Youth’s anxiety symptoms were assessed using the Beck Anxiety Inventory (BAI; Beck & Steer, 1993). The BAI is a widely used 21-item self-report scale designed for individuals 17 years of age and older to assess the number and severity of anxiety symptoms over the preceding week (e.g., “fear of the worst happening”). Each item contains four statements scored on a 4-point scale with higher scores indicating higher severity of anxiety symptoms. The BAI evidences good internal consistency and test-retest reliability (Beck et al., 1988). In this study, the Cronbach's alpha for the BAI was 0.93.
Youth’s life satisfaction was assessed using the Brief Multidimensional Students’ Life Satisfaction Scale (BMSLSS; Seligson et al., 2003). The BMSLSS is a 6-item self-report scale that asks participants to indicate their current level of satisfaction in various aspects of their life (e.g., family life) using a 7-point scale ranging from Very Dissatisfied to Very Satisfied. The BMSLSS has been found to show adequate psychometric properties (Athay et al., 2012). The Cronbach's alpha in this study was 0.75.
Youth interview
Youth provided a report of their perspective regarding parental support while attending university using written open-ended interview questions. Participants were asked the following questions: (a) “How has your mother and/or father been supporting you while attending University?,” (b) “What would be most helpful to you from mother and/or father to support you while attending University?,” (c) “What do you need most from your mother/father while attending University?,” and (d) “Is there anything different you wish your mother/father could do to support you?”
Parent interview
Caregivers provided written responses to a series of interview questions delivered via a survey link through their email. For the purpose of this study, parent responses to the following question: “In what ways will you support your child while they are attending University?” were of particular interest.
Procedure
This study was approved by the institutional ethics review board at this university in Ontario, Canada. Youth were recruited through the Introductory Psychology course participant pool and screened regarding mental health history. Those indicating mental illness were invited to complete a larger online youth survey, including the study measures described above. Youth were provided course credit for their participation. Following completion of the survey, youth were given the option to have their parent contacted to participate in the study. Parents were contacted at the email address that was provided by their child and if willing to participate, accessed the study measures (described above) online. After completion of the survey, parents were sent an electronic gift card by email.
Quantitative Results
Quantitative Data Screening
Missing data were handled per Newman’s (2014) procedures. Since less than 10% of the sample had construct-level missing data, pairwise deletion was employed. The affected participant skipped all constructs, resulting in a final sample of 224. No outliers were observed for relationship satisfaction, depressive symptoms, anxiety, or life satisfaction. Data were also examined for normality. All of the variables were above or below an absolute value of 1.5 for both skew and kurtosis. Finally, the data of the parent-youth dyads were examined. There was no missing data and normality assumptions were met. Multicollinearity was examined and, in all analyses, tolerance was greater than 0.1 and variance inflation factor (VIF) was less than 3.0, suggesting no issues with multicollinearity.
Relations Between Parent-Child Relationship and Youth Functioning
Relations among parent-child relationship satisfaction and youth’s experience of depressive symptoms, anxiety, and life satisfaction were explored via bivariate correlations (Table 2). Higher youth-reported parent-child relationship satisfaction was associated with higher levels of youth life satisfaction, r = .44, 95% CI [.33, .54], lower levels of anxiety, r = −.25, 95% CI [−37, −.13], and lower levels of depressive symptoms, r = −.39, 95% CI [−.49, −.27] (all p < .001).
Means, standard deviations, and correlations with confidence intervals among satisfaction with caregiver relationship, psychopathology, and well-being in a clinical sample of university students.
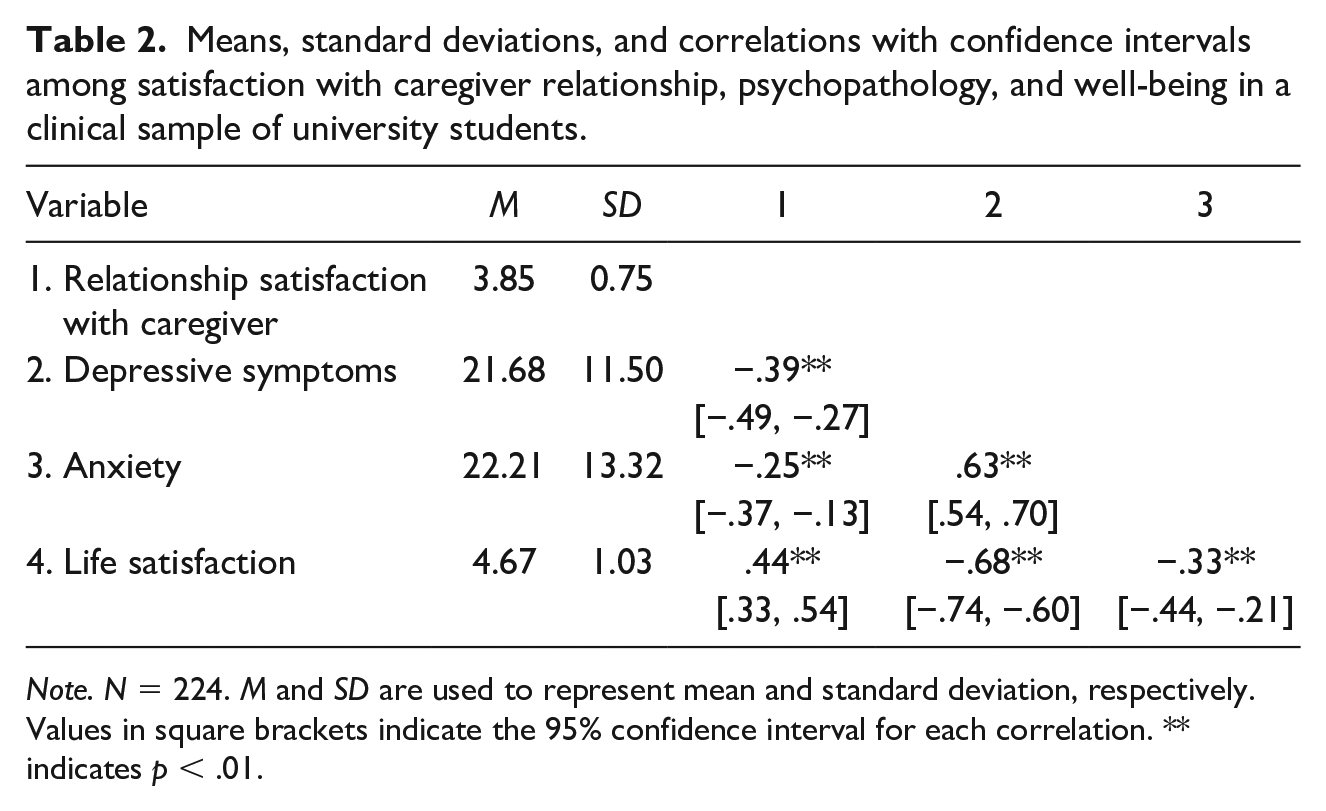
Note. N = 224. M and SD are used to represent mean and standard deviation, respectively. Values in square brackets indicate the 95% confidence interval for each correlation. ** indicates p < .01.
Relations Between Caregiver Reward and Burden with Youth Functioning
Cross-informant relations among caregiver reward, caregiver burden, and youth’s report of their own functioning were explored by examining the bivariate correlations (Table 3). Higher reported rewards of caregiving were associated with higher levels of youth-reported life satisfaction, r = .49, 95% CI [.08, .75], p = .022. Higher reported caregiver burden was associated with higher youth-reported depressive symptoms, r = .56, 95% CI [.17, .79], p = .007, and anxiety r = .48, 95% CI [.08, .75], p = .023, and lower youth-reported life satisfaction, r = −.49, 95% CI [−.75, −.08], p = .022.
Means, standard deviations, and correlations with confidence intervals among caregiver-reported burden and reward and youth-reported psychopathology and well-being.
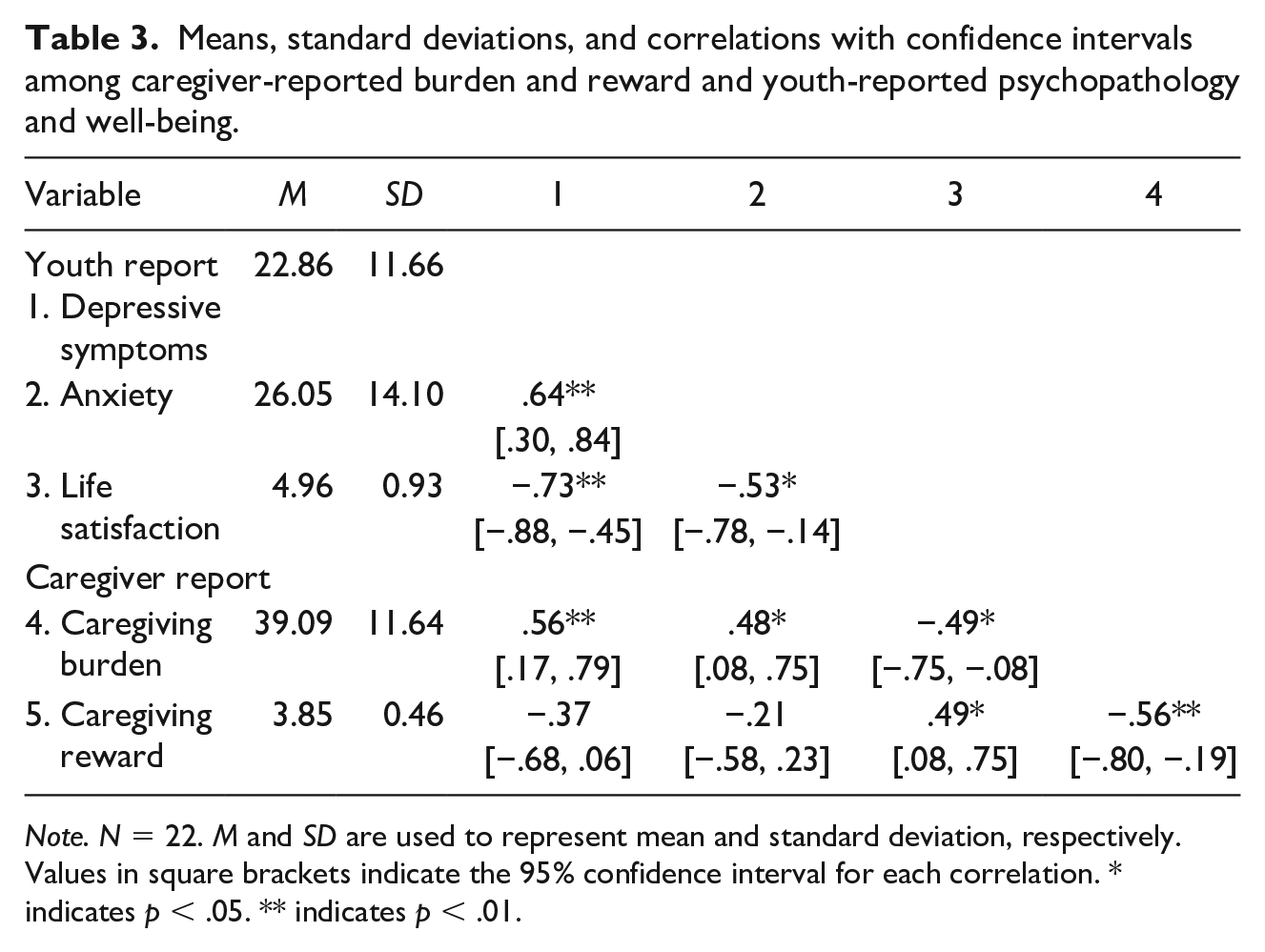
Note. N = 22. M and SD are used to represent mean and standard deviation, respectively. Values in square brackets indicate the 95% confidence interval for each correlation. * indicates p < .05. ** indicates p < .01.
Qualitative Results: What do Youth Need from Parents?
To explore how parents can best support their child with mental illness transitioning to university, both youth and their parent provided written responses to open-ended questions regarding parental support during the youth’s transition to university. After data were collected, analysis followed a thematic analysis approach (Braun & Clarke, 2006). Analysis began with youth responses, and upon completion, the process was repeated with parent data, finally both youth and parent responses were reviewed to refine the thematic map. To enhance reliability, themes and subthemes were developed through discussion and consensus-building among two researchers. The first researcher (K.B.) was a senior doctoral student in clinical psychology and this study formed part of her dissertation. She has several years of clinical and research experience working with youth with mental illness and their parents. The second researcher (M.L.) served as KB’s dissertation supervisor and is an established researcher in the field of youth mental health. She has extensive experience studying and advocating for student mental health supports during the transition to university.
First, to become familiarized with the data, the researcher (K.B.) read through participant responses to each question twice and, during the second reading, began thinking about and noting commonalities that appeared to be present across responses. In the second phase of analysis, initial codes were manually generated. Each response was re-read and each specific element of the response that was relevant to the question(s) asked were identified and given a code (e.g., “care packages”; “feel loved”), as were the overarching ideas communicated within the response (e.g., “talked about balance between support and independence”). A comprehensive list of all codes was generated. The next phase of analysis involved sorting this list of codes into potential themes by placing codes that were similar or appeared to be related together. These potential themes were further refined by examining whether data in each category appeared to be meaningfully related, whether each quote fit within the category, and whether categories were too broad (i.e., could be separated into smaller categories) or too narrow (i.e., could be combined into a broader theme). Following this refinement, the responses of all participants were re-read by the researchers to examine whether the potential themes appeared to capture the ideas expressed by the participants or whether other potential themes could be identified. Themes were then named, described, and subthemes were identified (e.g., theme of “instrumental support” with subthemes of “financial support,” “practical support,” and “problem-solving”) with quotes that exemplified each subtheme. Themes are depicted in Figure 1 and described in depth below.
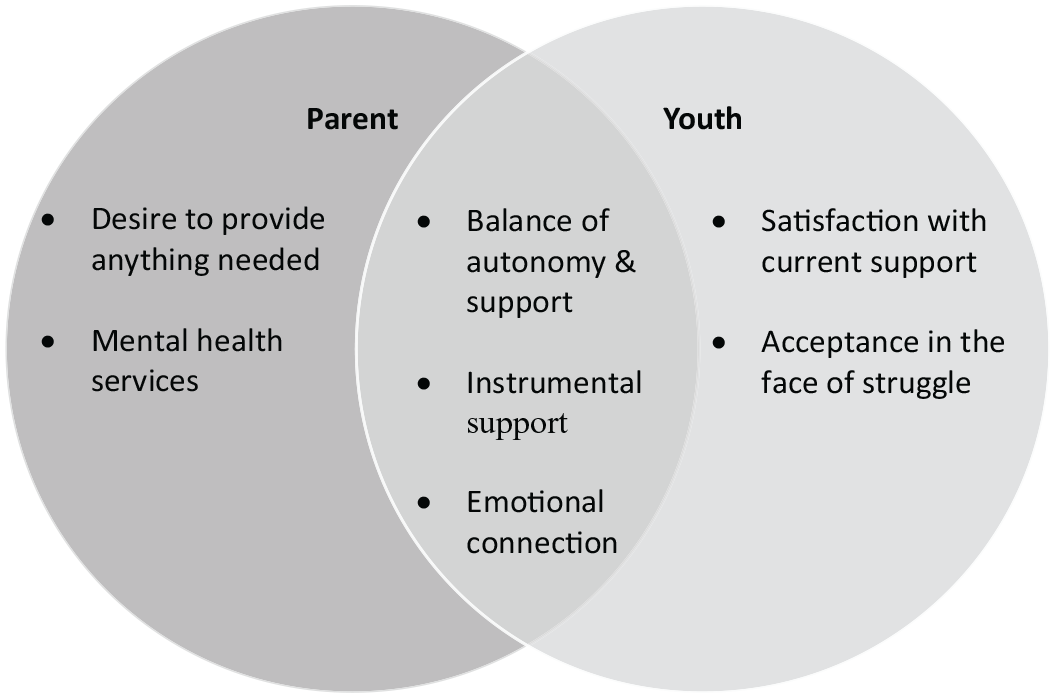
Youth and Parent Perspectives on Parental Support During University.
Youth and Parent Perspectives on Parental Support During University
Seven themes emerged from participant (i.e., parent and youth) responses: (a) balance of autonomy and support, (b) instrumental support, (c) emotional connection, (d) desire to provide anything needed, (e) importance of mental health services, (f) satisfaction with current support, and (g) acceptance in the face of struggle. As depicted in Figure 1, the analysis revealed some overlapping themes across parents and youth (i.e., balance of autonomy and support, instrumental support, and emotional connection), as well as themes uniquely present in parent (i.e., desire to provide anything needed, encouraging access to mental health services) and youth responses (i.e., satisfaction with current support, need for acceptance in the face of struggle). There are types of support that both parents and their youth view as important in helping the youth during their transition to university, as well as unique perspectives provided.
Overlapping Parent and Youth Perspectives on Parental Support
Balance of support and autonomy
Participant responses emphasize the need to find balance between supporting the youth and providing opportunities for their independence. For example, one youth wrote: “If they continue doing exactly what they are doing, no more and no less. They are still there for me, but they are allowing me to become an adult and to learn how to take care of myself.” Trust in the youth also arose within this theme with one youth writing, “I think the most helpful thing my mother and father could do to support me while attending University is support my decisions and if they're concerned about me to tell me.” The youth responses suggest that they want their parents to allow them to become their own adult, while stepping in with appropriate levels of support, when needed. Similarly, parents often explicitly acknowledged the importance of balancing the support they provide while also encouraging their child’s autonomy. For example, one parent shared, “We are available for occasional visits, but try to provide her with as much independence as possible, so that she continues to build a sense of self-worth and ability.” These quotes highlight the sentiments of many participants, which acknowledged the importance of parental support but also the need for youth to learn how to manage their responsibilities, take care of themselves, and make their own decisions to support the transition to becoming responsible and independent adults.
Instrumental support
Some parents and students indicated the importance of instrumental or tangible forms of support within the parent-child relationship. Within this theme, three subthemes emerged, namely financial support, practical support, and problem-solving.
Financial support
Both youth and parents noted the importance of financial support, with a number of students emphasizing that their parents were currently providing this. Both youth (e.g., “money”; “Help me financially”) and parents (e.g., “She has complete financial support and is welcome to live at home during university”; “. . . financial support and boxes of food.”) spoke of parents paying bills or providing them with loans while they attended university. One youth said, “They have been supporting me mentally, financially . . . They have lent me money when I am broke.” For some parents, this financial support was described as a “safety net” should it be needed: One parent shared, “She chooses to work but knows that she does not need to make money if her studies become too demanding to combine with a job.” Taken together, financial support was viewed as a way for parents to decrease the stress and burden of the university experience for their youth.
Practical support
Parent and youth responses also highlighted a variety of other practical supports. For example, one parent reported the following “We set up the house WITH her and I stocked the freezer with her favorites. We pick her up and drive her back when she asks.” Similarly, one youth shared that their parents “drop off a care package of food and other little supplies weekly, which is an enormous help . . .” Thus, providing tangible supports (e.g., food, transportation) were a valued form of support in this sample.
Problem-solving and advice
In addition, youth uniquely emphasized the importance of receiving personal or academic advice from their parents. In fact, many youth reported turning to their parents for help with solving specific problems and described their parents as being available to help them with a wide range of issues, as illustrated in the following quote: My mother has been supporting me a lot throughout University by offering for any clarification or help if I need it. . .My father has been supporting me also quite a bit throughout University by giving me a lot of positive advice and feedback to keep motivated me to work hard but not over work myself.
Parents also reported offering this type of support. For example, one parent reported the following: “I offer to talk to her about her assignments and to help her by reading her drafts and giving her feedback.” Thus, many participants appear to consider parents to be an important and trusted advisor to help the youth navigate academic and personal difficulties within the university context. Parents were also reported to help with stress management and motivation.
Both parent and student responses noted the value of instrumental support, namely they emphasized the role of financial support, practical support, and problem-solving and advice as important forms of parental support.
Emotional connection
Another theme that emerged in participant responses was the importance of emotional connection. Responses emphasized the importance of the youth feeling that their parents are there for them, thinking about them, and that they are loved and cared for. For example, one youth expressed that “Their love is the most important thing I need as it helps me to know I can always count on my family to be there.” Another reported that their parents provided “reassurance that they are there and everything will be OK.” For a number of other youth, staying emotionally connected to their parents was reflected in responses that mentioned love being what they need most from their parents (e.g., “love and support,” “knowing that they love me”). Many parents echoed the importance of maintaining an emotional connection with their child and described seeking to ensure that their child knows that they are there for them and available if needed, as illustrated in the following quotes: “I try to be emotionally available if ever and whenever I am needed.” and “by being available when and how she needs me.” Parents also described ensuring that their child knows they are loved and that they are thinking of them: “I tell her about home life here let her know she is still part of our family here.”
Youth and parent responses also described tangible and explicit ways that parents demonstrate this form of emotional support and strive to maintain an emotional connection with their child (e.g., texts, phone calls, check ins). For example, one youth reported that “Lots of facetime and phone calls, visiting me or bringing me home as much as possible and as needed by myself” was an important form of emotional support for them. This was similarly described by parents. As an example, one parent reported that “Keeping in regular contact (phone, text, skype and visits) to ensure that she is handling university,” was particularly salient to them. Another parent shared, “I maintain communication with her always. I know her schedule and ask about her activities and experiences.” These quotes highlight consistency across the emotional support that parents strive to provide to their youth and what many youth described to be important to them.
Overall, many participants highlighted the importance of maintaining an emotional bond or connection through a variety of means (e.g., facetiming, texting, calling to check-in, providing reassurance, letting youth know they are loved/missed) to ensure that the youth continue to feel loved and know that parents are available when needed.
Unique Parent and Youth Perspectives on Parental Support
While there was considerable overlap between the themes present in the youth and parent responses, some additional themes were unique to either the youth or parent perspective.
Importance of mental health services to parents
Parents specifically discussed wanting to ensure that their child was continuing to access mental health services when needed. For example, one parent reported that they provided support to their youth “By encouraging counseling when she needs it, . . .” Another parent expressed that an important form of support is providing “Daily contact, reminders of where to seek assistance, encouragement to advocate as appropriate, visits and comfort, connections to Health office.” These parents recognize the importance of mental health services in helping their child manage their mental illness and succeed in postsecondary education.
Youth need for parental acceptance in the face of struggle
Some youth described that what they needed most was their parents’ understanding of the challenges that they experience as they attend university while managing a mental illness and for their parents to be accepting of them even in the face of these struggles (e.g., “to know that they are not disappointed in me ever if I am struggling with my mental health.,” “I wish they could be able to talk to me without judgment . . .”). These youth expressed a strong desire for their parents’ unconditional love, respect, and acceptance even if they potentially make mistakes or fail. For example, one youth expressed wanting their parents “to be understanding of me getting marks lower than expected and not getting mad.” Finally, the youth also reported wanting their parents to understand the difficulties they face in relation to their mental illness, as evidenced by the following quote: I wish my parents could understand that my mental illness isn't something that I want to have. I wish that they realized that some days, getting out of bed is all I can do, and it's a huge accomplishment. I wish they realized how much I was struggling, but how much I am succeeding in dealing with the various struggles.
It appears important for youth to not feel that their parents are disappointed, angry, or judging them as they cope with these challenges. These youth reported wanting their parents to understand the various demands that they are juggling and to acknowledge that they are doing the best they can to successfully manage this.
Parent desire to provide anything needed
Overall, many parents indicated that they were willing to do anything that their child needs to support them through university. One parent said, “In any way she needs me too!! The sky is the limit!!” and this sentiment was echoed by many other parents (e.g., “In any way she needs. Emotionally, mentally, financially or otherwise.”). The majority of parents reported a willingness to provide anything that their child feels that they need as they attend university.
Youth satisfaction with current support
Given parents’ expressed willingness to support their youth in any way needed, it is perhaps unsurprising that many youth indicated that they felt their parents were already providing the support they needed or that would be the most helpful. One participant responded, “Just to keep doing what they are doing . . .,” and others with, “What they’re currently doing,” and “Exactly what she’s doing.” These quotes are representative of the majority of youth’s responses, and findings suggest that within this sample, youth were generally satisfied with the level of support their parents were currently providing for them and felt their needs were being met by their parents.
Discussion
This study aimed to develop understanding regarding how family relational factors (i.e., the parent-child relationship, caregiver burden/reward, and parental support) affect youth with mental illness making the transition to university. Results ought to be interpreted with the characteristics of the student sample in mind in that the majority reported female gender, white race, having lived with parents prior to university admission, currently living in residence, and having taken medication for a mental health issue.
First, within the larger youth survey sample, we examined the associations between parent-child relationship satisfaction and youth’s experience of mental illness (i.e., depressive and anxiety symptoms) and well-being (i.e., life satisfaction). Consistent with hypotheses, higher youth-reported parent-child relationship satisfaction was associated with higher levels of life satisfaction and lower levels of anxiety and depressive symptoms for these youth. Thus, results are consistent with research in general student samples (e.g., Kenny & Donaldson, 1991; Wintre & Yaffe, 2000), in those with other disabilities (Defur et al., 2016), and, with replication, extend these findings to a sample of youth experiencing mental illness. Positive parent-child relationship (as perceived by the youth) may be one important resilience resource for promoting positive youth functioning during this developmental transition.
Examining another aspect of the parent-child relationship, and consistent with expectations, lower levels of caregiver burden were also associated with better youth functioning (i.e., lower depressive and anxiety symptoms and higher youth life satisfaction). Caregiver reward was associated with higher youth life satisfaction. These are novel contributions to extant literature, expanding research linking caregiving experience to child well-being in the context of physical child illnesses (e.g., Thompson & Gustafson, 1996) to mental illness in youth that are in the process of launching within the family life cycle. In the context of this study, having a parent whose perspectives regarding caregiving during this developmental phase are reward centered (e.g., see strengths in their child and benefits of having a child with unique challenges) may be one factor that promotes resilience in youth and their families during an often challenging transition. Further research to explore the potential mechanisms through which caregiver reward and burden affect youth functioning, as well as transactional analyses of these variables, will aid in further clarifying these relations. The homogeneity of the current sample with respect to race and the lack of additional data regarding family social class/socio economic status suggests that care need be taken with regards to generalizing findings about caregiving rewards to other diverse communities (e.g., racial minorities, first generation, and immigrant families). Parental striving for caregiving reward perspectives may be particularly challenging for parents experiencing multiple and often intersecting forms of oppression in addition the experience of mental illness within the family. Family social capital (Coleman, 1988) and parental privilege (Kwate & Goodman, 2014) may well have affected these results.
The final aim of this study was to better understand what youth with mental illness need from their parents while attending university and how parents may best support them. From a family resilience perspective, parental involvement and support may be conceptualized as “capability and coping” resilience resources (Patterson, 2002) for families adjusting to their child with mental illness attending university. Qualitative responses indicated much overlap between youth and parents’ perceptions of the importance of a variety of types of parental support. Both parent and youth reported the value of having balanced parental support and youth autonomy. This suggests that both youth and parents recognize the need for youth independence and for parents to provide appropriate and adaptive support as their youth move toward this goal. Results here are consistent with research with families in which a child with other disabilities is making the transition to university (e.g., Smith et al., 2002), underscoring how challenging, delicate, and important this normative developmental process can be in populations of youth with unique needs. Instrumental support, in the form of financial support, practical support, and problem-solving, was identified as important by both youth and parent participants. Parents may be in a unique position to provide such foundational supports which may in turn reduce overall stress burden such that youth are freed up to focus on the challenges of being a student (e.g., navigating new relationships, completing coursework). Finally, Emotional connection was a particularly salient theme within both parent and youth responses. This emotional connection was evidenced by the parent creating a sense of being there for the youth and communicating support and/or love to their youth. Participants reported that emotional connection was maintained by the parent via frequent check-ins, being available when needed, and ensuring their child knows they love/are thinking of them.
Beyond this, youth uniquely reported wanting to be accepted unconditionally even when they face obstacles and challenges. Youth also spoke of being satisfied with the support their parent was providing. Parents specifically identified the intention to provide whatever is needed and supporting their youth in continuing to access needed mental health services. The parent focus on access to mental health services is unsurprising, given the salience of challenges regarding the availability and appropriateness of mental health supports (e.g., psychotherapy), as well as the importance of parental involvement, at this stage of development (e.g., Davis & Butler, 2002).
The themes present in youth and parent responses are informative in a number of ways. Regarding advising how parents may best support their youth, providing basic instrumental supports, maintaining a sense of connection, feeling loved, and perceiving unconditional acceptance from parents appear to be important for many youth. This is also consistent with extant research suggesting that a positive and supportive relationship with parents can serve as a protective factor in promoting youth well-being (Armsden & Greenberg, 1987; Kenny & Donaldson, 1991; Masten et al., 1999; Wintre & Yaffe, 2000). While knowing how to provide positive support, particularly during times of heightened stress and difficulty, can be challenging for parents, it is possible for parents to further develop skills to achieve these aims (e.g., improved communication, active listening, validation). Although not directly assessed, it must be mentioned that the socio-economic privilege of the current sample may well have influenced study findings (e.g., parental intrinsic knowledge about the University experience, sufficient parental financial resources). Thus, care must be taken in generalizing findings to families with less-privileged or more-oppressed experiences within society.
To postsecondary institutions, the present research speaks to these parents’ willingness to do anything needed to support their child with mental illness while at university. Even when parents are perceived as overinvolved or potentially providing support in ways that are perceived to be less adaptive, this is likely well-intentioned. Second, parents are a source of support with a vested interest in the success of their child (Small et al., 2011). As such, the potential of parental support for these vulnerable students could perhaps be better utilized. In line with the perspective of many postsecondary institutions, both parents and youth speak to the importance of balancing this support with promoting autonomy. Yet parents may not know what the optimal balance is or how to achieve it. In particular, for youth already struggling with mental illness, it may be even more difficult for parents to promote independence, as parents may fear the consequences of providing insufficient support (e.g., higher risk of suicide, higher likelihood of risky behavior, and negative avoidant coping strategies). In addition, parents may feel less able to “take a step back” when they feel as though their role as a caregiver is devalued or discounted altogether by postsecondary institutions (e.g., Agliata & Renk, 2008). Better acknowledgment and integration of parent support by postsecondary institutions may reduce demands for other support services and provide better direction for parents. In addition, such efforts may reduce the burden of caregiving during this time of transition, and increase perceived parenting rewards, which in line with the results reported above, may further positively impact youth adjustment and well-being.
Strengths and Limitations
Use of a difficult-to-recruit clinical sample of youth and their parent that might be seen in clinical practice is a strength of this study. The focus on parent-child relational impacts on these youth during a key period in the family life cycle is important and the transition to university is an ideal time in development to examine resilience-related processes. Examining youth well-being more holistically by including psychopathology symptoms and an indicator of “mental health” (i.e., life satisfaction) is also a strength and follows recommendations for a more “positive” clinical psychology approach to research (see Wood & Tarrier, 2010). Furthermore, the multimethod approach employed allowed a multifaceted exploration of this transition for youth with mental illness.
Conclusions are limited by several factors including the cross-sectional quantitative approach, as well as the size and potential generalizability of both the larger survey and parent-child dyad samples. All participants in the parent-child dyad sample and the vast majority of the larger sample reported white race. The experience of parents and youth from diverse racial and socio-economic identities within society may diverge from results described here in important ways. For example, it may only be from a position of racial/socio-economic privilege that parental emphasis on providing “anything needed” seems possible. Additional stressors and forms of oppression affect youth with mental illness and their families who may hold multiple intersecting minoritized or oppressed identities. Such differences in positionality may generate important differences in how to best support the youth making the transition to postsecondary environments (Kao & Rutherford, 2007; Keels, 2019). Further nuanced research with diverse samples of families is needed to more fully consider these possibilities.
Only a small proportion of study participants agreed to have a parent participate in this study, and of those who did only one parent, who was selected by their child, participated. Although the demographic and descriptive characteristics of youth who did versus did not have a parent participate in the study were quite similar (e.g., severity of mental illness indicators), it may be that the relational quality of nonparticipating youth-parent dyads was quite different and would have resulted in divergent perspectives emerging. Participating parents were mainly mothers, more likely to have a child who identified as female (vs. male), and this child was more likely to be taking medication to treat their mental illness than youth from the sample whose parents did not participate. It is possible that the observed associations may have differed significantly if relationship, reward, and burden measures were collected for nonparticipating parents and children with other genders. Nonetheless, the effect sizes of many of the relations reported here suggest value of replication and a deeper exploration within broader samples, extending this work by ideally tracking participants over time in longitudinal research.
This study suggests that while transitioning to university with a mental illness presents a number of unique challenges, positive parent-youth relationships, and specific forms of parental involvement appear to be beneficial to student adjustment and well-being. As postsecondary institutions continue to grapple with addressing the challenges of student mental illness, efforts to cultivate a university climate that acknowledges the importance of ideal levels of parental support may be a beneficial strategy to better pursue.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.