
Abstract
In rural Mozambique, girls commonly marry and have children before age 18. We use a Positive Youth Development lens to examine how constructs of confidence and competence were related to adolescent girls’ ability to and progress toward achieving their future aspirations. As part of an intervention evaluation, we used a longitudinal qualitative design, conducting in-depth interviews with 47 adolescent girls aged 13 to 19 at the end of the intervention and 1 year later. We explored adolescent girls’ future aspirations and examined their progress toward achieving their goals and three distinct groups emerged: (a) hopeful with self-efficacy, on track to reach goals; (b) hopeful with mixed levels of self-efficacy, not on track to reach goals; and (c) lacking hope and self-efficacy, not taking any actions to reach goals. Having hope and self-efficacy and behavioral competence enabled progress toward achieving goals, but poverty, early marriage, and childbearing were major obstacles. We conclude that fostering individual-level protective factors (e.g., hope and self-efficacy) is useful in interventions targeted toward young women to prevent pregnancy and child marriage, but that external assets (e.g., community, structural interventions) should be promoted to facilitate girls staying in school, provide sustainable economic opportunities, and improve adolescent contraceptive access and use.
Keywords
Introduction
There are more adolescents in the world than ever before and the majority live in low- and middle-income countries (LMIC) (United Nations, 2012). In 2015, United Nations member states agreed to promote 17 sustainable development goals (SDGs), which focus on economic, social, environmental, and sustainable development by 2030. Achieving the SDGs, especially those related to improving health and gender equality and reducing poverty, will not be possible without investing in adolescent health and well-being (Cluver et al., 2016; Gates & Graca, 2015; World Health Organization, 2017). Investing in adolescent health, education, and economic opportunities will enable adolescents to become healthy adults who can contribute positively to society and have their own healthy children, leading to a more sustainable future (United Nations, 2012; World Health Organization, 2017). Early marriage and childbearing significantly impact adolescent girls’ development in many LMIC because of serious health consequences, including maternal and infant morbidity and mortality, low birth weight (The United Nations International Children’s Emergency Fund [UNICEF], 2015; World Health Organization, 2018), and broader social impacts, such as decreased autonomy and self-efficacy to continue education or work outside of the home due to deeply pervasive and inequitable gender norms (Phillips & Mbizvo, 2016; Sawyer et al., 2012).
Youth risk-reduction programs have often focused on youth’s negative behaviors and vulnerability, especially related to sexual and reproductive health (SRH). Empirical evaluation of such programs have traditionally hinged on individual-level, SRH-specific outcomes (such as increased self-reported condom use or increased knowledge of a specific health topic) alone as markers of success or failure (Chandra-Mouli et al., 2015; Glinski & Petroni, 2014). The positive youth development (PYD) field challenges the view that young people are inherently risky and focuses on promoting protective factors to prevent risk behaviors and achieve positive outcomes. These protective factors are sometimes referred to as developmental assets and include both internal assets (e.g., youth’s personal skills and values) and, equally as important, external assets (e.g., community and social systems) (Benson et al., 2011). PYD promotes five positive developmental outcomes for youth: competence, confidence, connection, character, and caring (Lerner & Thompson, 2002). Increasingly, efforts to help adolescents thrive worldwide are incorporating PYD approaches (Ahorlu et al., 2015; Blum et al., 2012; Gavin et al., 2010; Mathur et al., 2001; Rew & Horner, 2003). Rather than being incompatible, PYD approaches can be considered an evolution of historically problem- or risk-focused programs and program evaluations (Plourde et al., 2016).
We conducted a secondary analysis using data from an evaluation of an economic and social empowerment intervention implemented with adolescent girls in Zambézia Province, Mozambique, to explore ways in which individual-level protective factors related to competence and confidence impacted adolescent girls’ ability to make progress toward achieving their future goals. The Strengthening Communities through Integrated Programming (SCIP) project, funded by the United States Agency for International Development, implemented the women first (WF) intervention among many other interventions from 2010 to 2015 in Zambézia, Mozambique (Moon et al., 2015). The WF intervention included adolescent girls aged 13–17 (particularly targeting orphans and vulnerable children) and combined an economic package that trained girls to sell products in their communities with group education using the Go Girls! life skills curriculum (Johns Hopkins Bloomberg School of Public Health/Center for Communication Programs, 2011) and a locally tailored gender-based violence (GBV) curriculum. While the primary evaluation focused on changes in self-reported knowledge and behavior related to HIV, GBV, and school attendance, aspects of the intervention echo core constructs from PYD approaches, which we wished to explore further through secondary analysis of the qualitative data. Specifically, the WF intervention included content that can be seen as targeting two individual-level PYD developmental outcomes: confidence and competence.
Through a PYD lens, we examine two core constructs of confidence—belief in the future and self-efficacy—and one core construct of competence: behavioral competence (Gavin et al., 2010; Gloppen et al., 2010). Belief in the future is the “internalization of hope and optimism about possible outcomes” and is related to long-term goal setting and beliefs that support higher education, employment, or work values (Gavin et al., 2010). Self-efficacy—believing one is in control of one’s own life, being motivated and able to persevere in difficult situations, and exhibiting problem-solving and goal-setting skills (Bandura, 1997)—has been described as a goal for healthy adolescence (Blum et al., 2012) and as a core aspect of adolescent development (Greve et al., 2001; Tsang et al., 2012). Youth self-efficacy is seen as a positive factor, or asset, that helps youth overcome risk and enact health-promoting behavior (Fergus & Zimmerman, 2005). As adolescents develop to become more autonomous, they need to believe that they are capable of doing the behaviors that will lead to their desired futures (Greve et al., 2001). Behavioral competence is defined as “effective behavior choices and action patterns” (Gavin et al., 2010) and can be described as taking meaningful or concrete actions such as attending school or using contraception. These constructs were selected because they emerged during initial qualitative analysis and because of their links to the intervention content. Related to self-efficacy and belief in the future, the WF intervention encouraged girls to have self-confidence to make healthy decisions, define personal goals, and identify available resources to enable them to achieve their goals. Related to behavioral competence, the WF intervention sought to provide participants with education, encouragement, and skills to delay marriage until age 18; stay in school; prevent unintended pregnancy, HIV, and GBV; and to become financially self-sufficient. The WF intervention did not directly engage communities or parents/guardians.
Background on Zambézia Province, Mozambique
Mozambique has one of the highest rates of child marriage in the world, with almost half of women aged 20 to 24 years marrying before age 18 (UNICEF, 2015). Adolescent girls in Zambézia Province, one of Mozambique’s most rural provinces that depends almost exclusively on subsistence farming and fishing (Victor et al., 2014), are at especially high risk for early marriage (before age 18). This is largely due to social norms such as considering young adolescent girls ready for marriage and childbearing after completing traditional initiation rites and lobolo, or bride price, paid to the girl’s family, which gives families an economic incentive to marry their daughters. Child marriage is often synonymous with pregnancy, as girls in Mozambique typically have their first child 15 months after getting married (UNICEF, 2015). Overall, 76% of adolescent girls in Mozambique have experienced a pregnancy by age 19 (Ministério da Saúde, Instituto Nacional de Estatística, e ICF, 2015).
Method
We conducted a secondary analysis using qualitative data collected from 47 adolescent girls who participated in a mixed–methods evaluation of the WF intervention conducted by FHI 360, Vanderbilt Institute for Global Health and Friends in Global Health. Further information on the methodology and primary results from the evaluation is reported elsewhere (Burke et al., 2018, Burke, Field, et al., 2019; Burke, Packer, et al., 2019). The primary evaluation was designed to assess whether the WF intervention reduced adolescent girls’ vulnerability to HIV and to describe potential pathways that explain the intervention’s effects on girls’ HIV vulnerability. The evaluation began after the intervention had started, and, in some communities, after the intervention had ended. Most girls had finished the intervention by the first round of qualitative data collection and were interviewed 1 year later to look at sustainability of intervention effects.
Sample Selection and Data Collection
For the qualitative component of the primary evaluation, we randomly selected two communities in each of the six districts in Zambézia Province that participated in the WF intervention (this resulted in 12 communities out of 22 which participated in the WF intervention). We then generated a list of the adolescent girl WF participants aged 13 to 19 years who participated in a quantitative survey in April to May 2015 (n = 151), and randomly selected four girls in each of the 12 communities to invite to participate in qualitative interviews at two time points. The data collection team went to the communities and followed up with potential participants in-person. We planned to interview a total of 48 adolescent girl participants (four per community) but interviewed one extra girl due to miscommunication during data collection. Five originally selected girls were replaced using the next eligible girl on the list (three had moved out of the province and were not able to be contacted, one girl’s husband refused to let her participate, and one did not participate in most of the intervention and could not answer any questions). We conducted interviews with 49 selected girls from August to October 2015 and a second interview with 47 of the 49 girls from August to October 2016, approximately 1 year after the intervention had ended. The participant who was mistakenly interviewed the first time was not re-interviewed, and the husband of another participant refused to let her participate. This article includes data from the 47 girls who completed two interviews.
Trained female interviewers fluent in Portuguese and Lomué, Sena, and/or Chuabo local languages used semi-structured in-depth interview guides (see Supplemental Appendix A). Interviews were conducted one-on-one in a private location and lasted approximately 1 hour. Specific to this secondary analysis, we asked girls at both time points questions about their opinions on the ideal age, actual age, and age that they thought they would have sex, get married, and have children; about current and future contraceptive use; how they envision their futures; and what steps they were taking to achieve their future goals. All questions were open-ended and respondents were probed about why they considered a certain age ideal for such life events and what age and why they expected to experience these events. A question about the actual age that girls in their communities begin these life events was added to the interview guide used in Round 2 to gain a deeper understanding of the social context of the communities where respondents lived and to enable comparisons between respondents’ ideal ages, the actual ages of girls in their communities, and the ages respondents thought they would have sex, get married, and have children.
The study was reviewed and approved by FHI 360’s Protection of Human Subjects Committee, the Vanderbilt University Institutional Review Board, and the National Bioethics Committee for Health in Mozambique. All respondents gave written informed consent or assent with parental/guardian consent for respondents under 18 years. Respondents did not receive compensation for participating in the interviews.
Data Analysis
All interviews were audio recorded with respondents’ permission, simultaneously transcribed and translated from local languages into Portuguese, and then translated into English. All English transcripts were carefully reviewed by the co-authors and if questions related to accuracy or translation arose, transcripts were sent back to the study coordinator who contacted the interviewers to review the original audio file and correct the transcript as needed. For each interview round, we developed initial codebooks with structural and thematic codes based on the interview guides and review of preliminary data. Two analysts (co-authors K.R. and R.L.) conducted initial coding of the transcripts using NVivo qualitative software (QSR International Pty Ltd. Version 11, 2015). To assess intercoder reliability, both analysts independently coded 9% of the transcripts and resolved coding discrepancies through discussion (Guest et al., 2012). Analysts used an iterative process to update the codebooks based on these meetings, add new codes as new themes emerged, and re-code transcripts when necessary.
We used an inductive approach for data analysis where the analytic concepts and categories were directly grounded in the data (Charmaz, 2006). During the analysis for the primary evaluation, themes related to hope for the future, self-efficacy, and crushed dreams emerged, which we felt aligned with the PYD outcomes of competence and confidence and warranted further investigation. We then conducted a secondary analysis which forms the basis of this article using a process similar to focused and axial coding (Charmaz, 2006). The first author generated coding reports from initial coding from the primary analysis for all relevant topics related to future goals, ideal and actual age of starting to have sex, getting married, and having children. She then read these coding reports, went back to the transcripts, and summarized them thematically in structured matrices, by interview round and basic demographics. She compared the data between girls and within girls between interview rounds to link having hope and/or self-efficacy to categories of being “on track” or not to achieve their goals. Inductive thematic saturation was reached in that no new themes emerged from the data after the described analysis process (Saunders et al., 2018). During analysis, we considered communities respondents came from, and the few differences between communities are noted in the text.
Classifications of hope, self-efficacy, and being “on track” to achieve goals
For this analysis, we categorized respondents as “hopeful” (belief in the future) if they used optimistic language when talking about their futures (e.g., stating that had set goals and they believed they could achieve their goals) (Table 1). Respondents were categorized as “lacking hope” if they used pessimistic language (e.g., explicitly stating that they did not believe it was possible to achieve their goals).
Connecting PYD Outcomes to Analysis Categorizations.
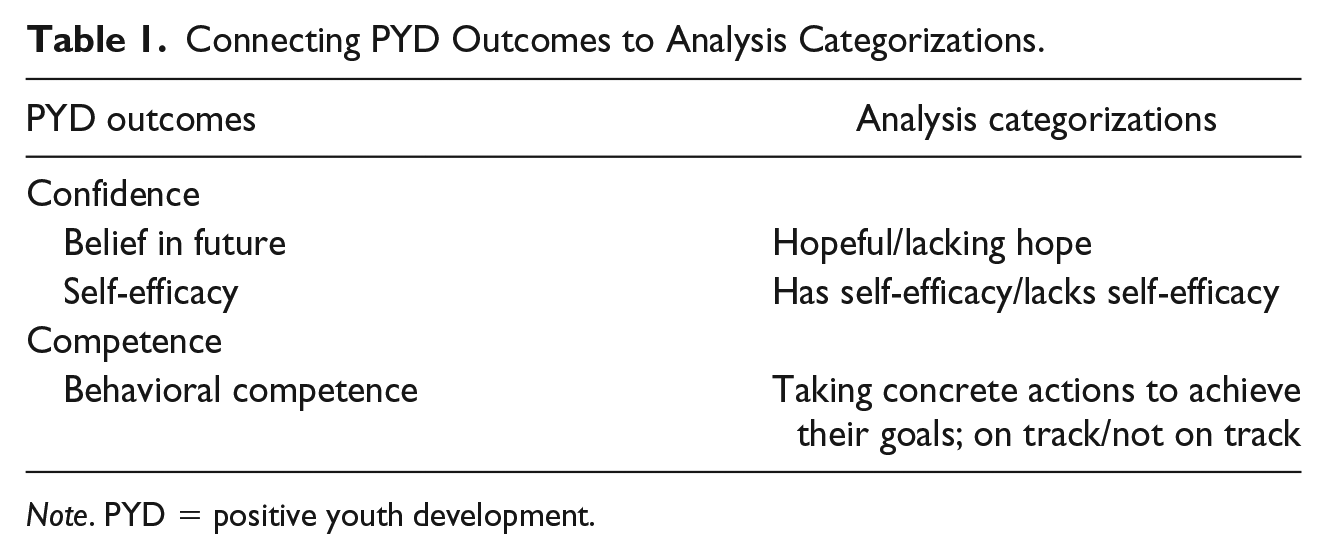
Note. PYD = positive youth development.
Respondents who expressed confidence that they would and could do what is needed to achieve their goals were considered to have self-efficacy (e.g., that they could stay in school if their goal was to study; or that they could delay pregnancy if they desired to delay childbearing). Those who expressed lacking control over their ability to do things to achieve some or all of their goals were considered to have no or mixed self-efficacy.
Being “on track” to achieving their goals took into consideration hope, self-efficacy, and behaviors toward reaching their goals. Those who were hopeful and described having self-efficacy were categorized as being on track to reaching their goals if they were also taking concrete actions (demonstrating behavioral competence) to achieve their goals, that is, attending school (if goal was to study), doing business (if goal was related to business), not having sex (if desired delaying marriage and childbearing), or, if sexually active, using contraception (if desired delaying childbearing). Those who lacked hope, expressed a lack of self-efficacy, and were not currently taking actions to achieve their goals were considered “not on track.” Table 1 outlines the linkages between PYD outcomes and our analytical categories.
Results
Respondent Characteristics and Changes Over Time
Respondents’ self-reported average age was 16 years at the first interview (Table 2). We found different patterns in the data for “younger” (13–16 years old) and “older” respondents (17–19 years old); thus, these terms will be used to describe respondent age throughout the “Results” section.
Self-Reported Respondent Characteristics.
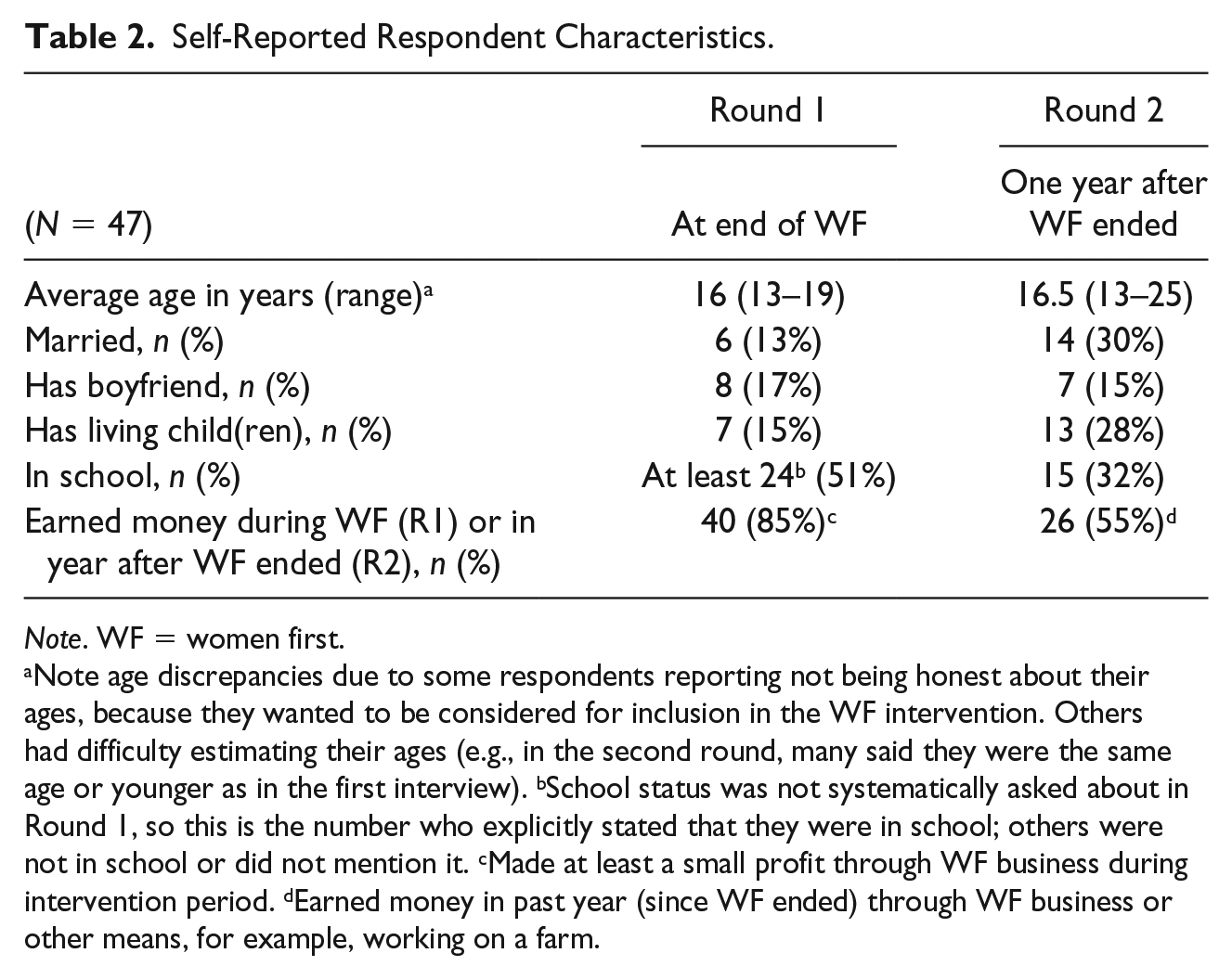
Note. WF = women first.
Note age discrepancies due to some respondents reporting not being honest about their ages, because they wanted to be considered for inclusion in the WF intervention. Others had difficulty estimating their ages (e.g., in the second round, many said they were the same age or younger as in the first interview). bSchool status was not systematically asked about in Round 1, so this is the number who explicitly stated that they were in school; others were not in school or did not mention it. cMade at least a small profit through WF business during intervention period. dEarned money in past year (since WF ended) through WF business or other means, for example, working on a farm.
At the first round, few respondents were married (13%) and/or had children (15%), whereas by the second round, almost one third were married (30%) and more than one quarter had children (28%). School attendance and earning money decreased substantially between the first and second interviews and were often interconnected. Respondents generally stopped attending school due to lacking money to pay for school-related costs or because they got married or pregnant. Illustrating this, only one married respondent and no respondents with children were in school by the second interview. In addition, secondary schools were only available in five of the 12 study communities, so to continue secondary education, adolescents often had to travel significant distances or move to other communities to go to school. Although the WF intervention had a business component, not all respondents engaged in business or made a profit during the intervention, and in many cases, those who made a profit did not sustain their businesses, usually because of factors outside of the girls’ control (e.g., higher product prices after the intervention stopped subsidizing products). Less than one third of respondents (14) said they were earning money at the second interview (data not shown).
The remainder of the “Results” section describes respondents’ stated future goals, their desired timing of marriage and childbearing, contraceptive self-efficacy and behavior, and being on track to achieving their goals.
Girls’ Stated Future Goals
Participating in the WF intervention gave many girls new hope for their futures. Regarding the social context of their communities, respondents talked about how there were few economic opportunities for girls beyond working on a farm, having transactional sex, or getting married (to receive lobolo). However, after learning that they had more options during the intervention, respondents generally expressed belief in their futures by describing optimism that they could “be someone” beyond a housewife and mother, and become financially self-sufficient through business, giving them the means to pursue their goals (e.g., paying for school-related expenses).
Many respondents expressed that they felt they could become autonomous after taking part in the intervention. For example, one married respondent said, “The program opened our vision. Before we were blind and didn’t know our rights. We didn’t know we were able to do business, study, be respected and make decisions.” Indeed, the most common future goal, mentioned by almost all respondents, was having paid work, often so they would not have to rely on others (husband, family, transactional sex). Another married respondent said, “It is through this income that I will make my house and will continue to study without depending on others.” More than half of respondents described wanting to continue or expand their businesses, and more than half specifically described wanting to become a teacher or, less commonly, a nurse. About two thirds of respondents said a future goal was to “study” or complete secondary or higher education. About one third of respondents said that they wanted to build their own house or improve their existing one. Several respondents also talked about wanting to own things like a bicycle, motorcycle, car, or television. A few mentioned wanting to be healthy or happy.
Many respondents described having multiple goals and often described doing business as its own goal or to generate money to achieve other goals. The majority of respondents expressed hopefulness and self-efficacy that they could achieve their goals. An unmarried respondent said, “I would like to graduate and have a job . . . Graduate as a teacher . . . Thanks to the program today, I have the strength to continue studying and graduate.”
Most respondents discussed the same or similar goals in both interview rounds; however, for some, goals changed between rounds (e.g., in Round 1, wanted to continue to study and have her own home and in Round 2, wanted to resume or continue doing business). There was no clear pattern of respondents’ characteristics who changed their goals and whether their goals became more or less ambitious.
Preferences for Timing of Marriage and Childbearing
In general, the desire to get married and have children was universal; however, most respondents expressed wanting to delay these life events for at least a few years. For example, an unmarried respondent wanted to wait 5 years before getting married, saying, “I don’t think about getting married early because I want to study first and only get married when I’m a grown up. I still have my money to buy my school supplies.” Although premarital sex was viewed very negatively, respondents typically reported an ideal age of 18 for girls to start having sex and 19 to get married (Table 3). They also said that girls should have children only after marriage.
Respondents’ Reported Ideal and Actual Ages to Have Sex, Get Married, and Have Children.
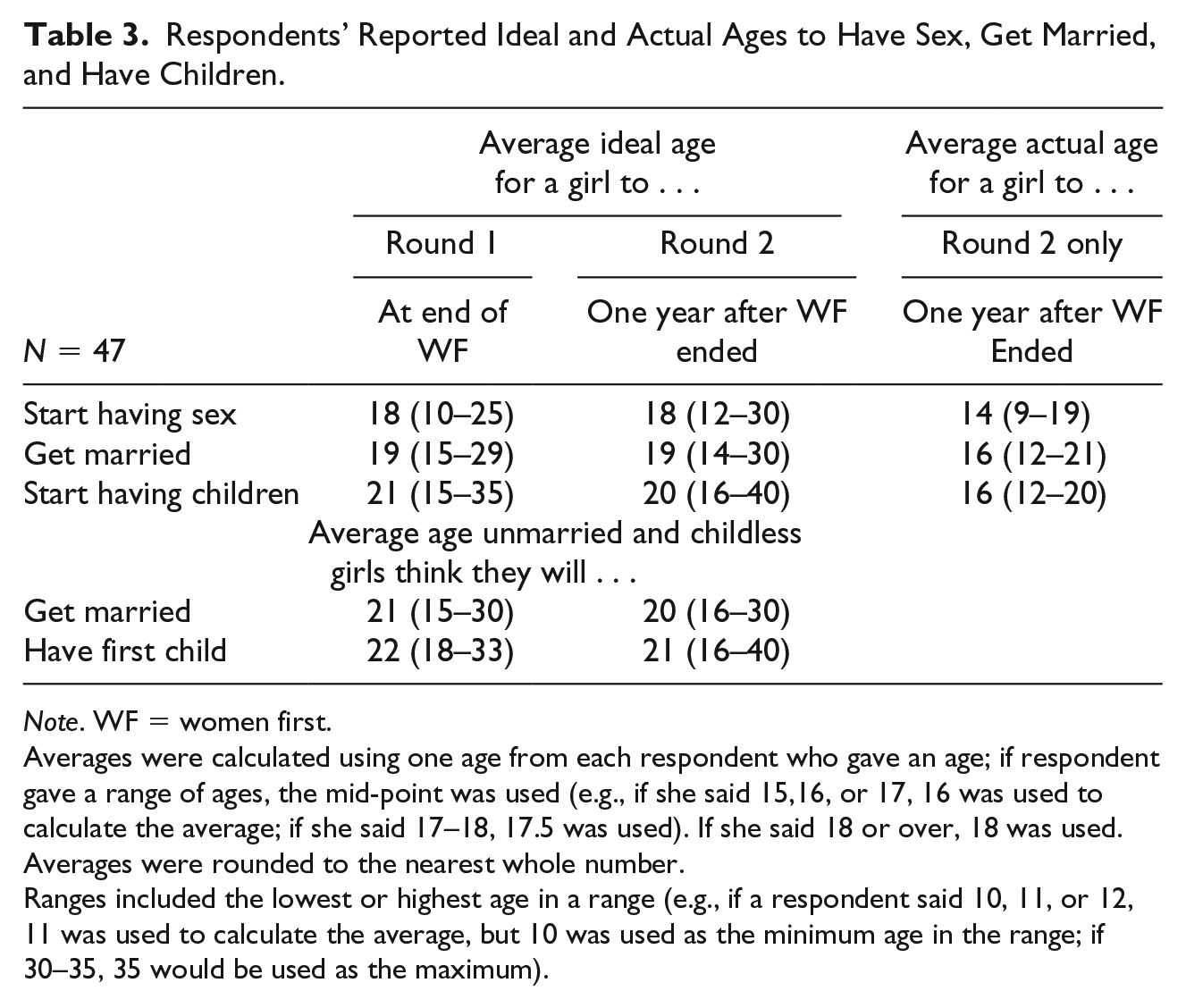
Note. WF = women first.
Averages were calculated using one age from each respondent who gave an age; if respondent gave a range of ages, the mid-point was used (e.g., if she said 15,16, or 17, 16 was used to calculate the average; if she said 17–18, 17.5 was used). If she said 18 or over, 18 was used. Averages were rounded to the nearest whole number.
Ranges included the lowest or highest age in a range (e.g., if a respondent said 10, 11, or 12, 11 was used to calculate the average, but 10 was used as the minimum age in the range; if 30–35, 35 would be used as the maximum).
Despite expressing that girls should ideally wait to start having sex, get married, and have children at Rounds 1 and 2, respondents at Round 2 said girls in their communities generally started these life events 3 to 4 years younger than the ideal ages they stated. Respondents often explained that due to poverty, girls start having sex (e.g., “in exchange for money, food, and clothing”) or get married.
At Round 1, unmarried respondents and those without children typically said they thought they would get married around age 21 and have their first child around age 22, often saying that they wanted to wait until they finished their studies before getting married and wait to have children until after they were married. Although respondents gave similar ideal ages in Round 2, those who were still unmarried and childless at Round 2 said they thought they would get married or have their first child about a year younger on average compared to Round 1, somewhat closer to the actual ages respondents reported girls in their communities got married and had their first child (Table 3). Illustrating this point, one younger unmarried girl said at Round 1 that she thought she would get married at age 19 “after I’m done studying”; however, at Round 2 said she thought she’d get married at age 18 because that age is “old enough.” An unmarried 19-year-old respondent reported at Round 2 that her ideal age of marriage was 23; however, she thought she would get married by age 21 and explained, since I can’t support myself and I want to continue my studies, I have to find a husband who works to help me continue my studies. I’ve completed the 7th grade here in [community name], and we don’t have the 8th grade. I have to study in [different community name], so I have to marry to have some help.
Related to this, eight girls got married between interview rounds (Table 2), most married prior to age 18, and all but one at an age earlier than their stated ideal age at Round 1. Five of these respondents said they got married because they wanted to and one of these became pregnant which also led to her getting married. The other three, who had all stopped doing business after the intervention ended and had not earned money in the past year, said they married because they needed money and two expressed regret for this, “I wouldn’t have gotten married if the program had continued” (married respondent, second interview). Eight respondents had a baby or got pregnant between the first and second interview round, usually at an age earlier than their stated ideal age at the first round. Half said they wanted to get pregnant because they were married. Half experienced unintended pregnancies (all but one of these was unmarried) and said they had not thought they would get pregnant, also indicating low perceived pregnancy risk. A few of these respondents expressed regret for getting pregnant at an early age: [Getting pregnant at age 15] was a failure . . . I never thought I would have sex with someone and get pregnant; I didn’t have sex with the father of my son often, it was only a few times. (Unmarried respondent, second interview)
Contraceptive Knowledge, Self-Efficacy, and Behaviors
Despite respondents’ participation in the WF intervention and their stated desires to delay childbearing, we found large gaps in contraceptive knowledge, low contraceptive self-efficacy, and negative attitudes toward contraception which appeared to affect contraceptive behaviors. During both interview rounds, many respondents stated learning that one should use condoms to prevent HIV and pregnancy, while relatively few spoke about pills, injections, or, more vaguely, “going to the hospital to get family planning.” Respondents also did not seem to have the functional knowledge to know where to obtain and how to correctly use contraception.
Many respondents did not feel that they had control over the timing and number of children they would have, and felt that it was up to God or depended on their husband, indicating general low perceived self-efficacy and interpersonal and social barriers related to contraceptive use and childbearing. For example, “Having children is something that only God knows. I can’t determine” (Married respondent, second interview). And “Using a condom with their wives is abusive to the husbands” (Married respondent with a child, second interview).
Also related to the social environment, misperceptions and negative attitudes toward contraception were prevalent. Many respondents expressed that married women should not or could not use contraception, usually because their husbands did not want to. Other common perceptions were that women should not use contraception until after having a child because it would cause infertility (“I never used any method to avoid pregnancy, because I had never made a baby. Here in our area it is not advisable to take pills to avoid getting pregnant if you never had a child”—Married pregnant respondent, second interview). However, attitudes toward using contraception to space births were more positive, and when asked if they thought they would use contraception in the future, more than three quarters of respondents at both rounds said they thought they would, especially to space births.
Contraceptive use was low. Nearly half of respondents in Round 1 said they had ever had sex, yet only a few said they had ever used contraception, mostly condoms. By the second interview, slightly more than half of respondents said they had had sex and about half of those said they had used contraception (mostly condoms), which was more than the first round, but still low considering the general desire to avoid pregnancy.
Tying it All Together: Competence and Confidence to Achieving Goals
We examined girls’ progress toward achieving their goals by the second round, in terms of their stated desired age for marriage and childbearing and whether that had affected their other aspirations. Three distinct groups emerged: (a) hopeful with self-efficacy, and on track to reach all of their goals; (b) hopeful with mixed levels of self-efficacy, but not on track to reach all of their goals; and (c) lacking hope and self-efficacy, and not doing anything to reach their goals. Note that there were no differences in types of future goals among the three groups (e.g., girls across all categories wanted to study, become a teacher, and improve their house).
Hopeful with self-efficacy: On track to achieve goals
Just over one third of respondents at the second interview (Figure 1) expressed hope, high levels of self-efficacy, and were doing something concrete to achieve their goals, like going to school or doing business. The majority of these respondents were not married and did not have children, and more frequently stated that they had never had sex or that they were currently not sexually active. For example, an older unmarried respondent who was in school and doing business at both rounds said at the first interview, “I would like to be a nurse or a teacher to teach . . . I will bake my cakes and sell them so that I can study and be able to become a teacher.” At the second interview, she had the same goals and seemed determined to reach them: Before I entered the program, I didn’t have any dreams, but with the training from the program now I want to be a teacher or a nurse. But ever since the program closed I haven’t changed my mind, I want to have a house, and be a teacher or a nurse.
She said she had never had sex and that she wanted to wait until she was 30 years old to get married.
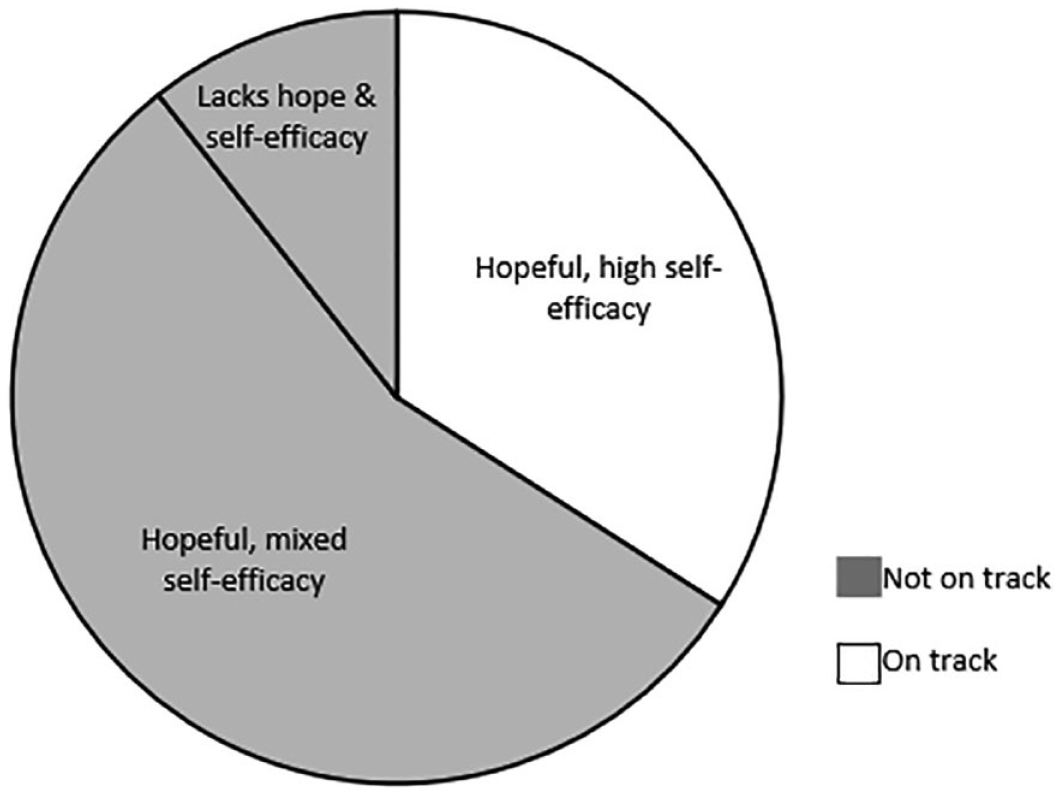
Proportion of respondents with hope and self-efficacy and progress toward achieving goals (N = 47).
Most of these “on track” respondents were younger and in school. Compared to girls in the other categories, more were doing business or making money by working on a farm. In two communities, both of which had secondary schools, almost all respondents were in the “on track” category and all of those in this category whose goal was to study were in school. A younger unmarried respondent who had the same goals at both interview rounds said in the second interview, I’d like to work, have a salary, and buy everything I want with my salary . . . .I want to study, work, then get married . . . when I started doing my business, buying my own stuff, paying my school fees, for my notebooks, my uniform and shoes, I started thinking I should continue to study until the 12th grade, then start working.
She was still in school at the second round (her community had a secondary school), and when asked how she planned to achieve her goals she said, “I am going to work harder at school . . . Be more committed, not failing, so that I can finish school and work.” She also said she had never had sex and wanted to wait to get married until she was 20.
The few sexually active respondents who wanted to delay childbearing in this category said they were using contraception (mostly condoms). The few respondents who were married or had children were already so at the first interview. These respondents were older and were not in school at the second round; however, studying was not their goal (all had the goal of continuing to do business and they were all doing business at the second interview round).
Hopeful with mixed self-efficacy: Not on track to achieve goals
Slightly more than half of respondents at the second interview described hope for their futures but expressed mixed levels of self-efficacy and were not on track to reach some or all of their goals. More than half of these respondents were married or had children, several of whom had gotten married or had a baby in the year since the first interview. Over one quarter said they used contraception, but a similar number said they did not use contraception, usually because they were married and lacked self-efficacy to use contraception. Over one quarter said they had never had sex, and the rest gave unclear answers about having sex or whether they had used contraception.
Most of these “hopeful but not on track” respondents were older. The majority were not in school, usually because they got married or pregnant or did not have money for school fees or uniforms. Most were no longer financially self-sufficient or able to do business from the WF intervention, usually because they stopped receiving subsidized products or their businesses failed.
While most of these respondents were not on track to achieve their long-term financial or career goals, they did appear to have self-efficacy and be on track to achieve other goals, such as delaying pregnancy. Several girls in this category, despite impressions of having stalled in their progress, expressed determination to continue to work toward their goals. Some had concrete plans, such as saving money to return to school at a certain time point, whereas others only had intentions or desires, but no plan. For example, an older respondent who had gotten married and had a child between the first and second interviews said that her goals of studying and becoming a teacher had not changed at the second interview. “Yes, [my goals for the future] are the same, but you know what youth is like. I ended up making some mistakes on the way and I have a daughter and got married. But this doesn’t change anything.” She stopped attending school when she was pregnant, but she seemed determined to return to school: “I’d like to go back to school, complete the 10th grade and do a course to become a teacher to help my family.” She also expressed high contraceptive self-efficacy and a goal to delay having another child, saying, I take [contraceptive] pills for my daughter to grow before I have another baby and for me to be healthy . . . In my house I can buy food, clothes for my child, and I can make decisions without waiting for my husband. And because I have a little baby, I ask my husband to put on a condom to not get pregnant right now.
A few respondents in this category remained hopeful that they could achieve their goals but reported doing no concrete actions at the second interview to achieve their goals. All but one of these was married or had a child at one or both interview rounds and stated that this was part of the reason they were not taking actions to achieve their goals. For example, a younger unmarried respondent who wanted to be a nurse but experienced an unintended pregnancy between interview rounds said in her second interview, I wanted to study, to do Grade 12, to work and get married later . . . I had a dream, to have a child after getting married, but the father of my daughter appeared, I had sex, became pregnant and now I have a child. My dreams have vanished.
She stopped attending school after becoming pregnant and said she was “doing nothing at the present moment” to achieve her goals, but she intended to get back on track: “next year I will study again to reach that objective of mine.”
Lacking hope and self-efficacy: Not on track to achieve goals
In general, in the first interview, most respondents were hopeful that they would reach their goals. By the second interview, more, but still only a handful of girls, expressed lacking hope about their futures and self-efficacy (e.g., had no earnings, married and unable to go to school), and were not doing anything to achieve their goals. A few described experiencing crushed dreams, where they felt that the intervention had given them new hope for a better future, but then, as they became increasingly unable to do anything to reach their goals, they felt very disappointed. For example, a younger respondent said in the first interview that she wanted to continue her business, finish her studies, and become a teacher or nurse. She said she wanted to wait 2 years to get married. However, she had got married by the second interview and felt that her goals were unachievable because she was married: I was not able to accomplish my goals . . . I stopped studying, married at 16 years old, now this is not good. I cry when I see my girlfriends still doing business and studying, some even have bicycles, and I don’t . . . Our life got worse . . . I had the idea of getting married only after the program closed . . . So, when someone showed up and proposed to me, I had no other ideas but to accept it. But when I entered the Women First program the plan was to study.
She was not using contraception with her husband because he refused to, and since she was married she felt like she should have a child, “I just got married and I don’t know if I can have children, that’s why I can’t take anything to avoid pregnancy.”
The respondents in this category were younger. All had stopped attending school in the previous year (usually due to lack of money or getting married), and none were doing business (e.g., because the intervention ended and they were unable to sustain the business). Three said they had never had sex and therefore appeared to be on track to delaying marriage and childbearing; however, they seemed to lack hope that they could reach their other goals, as they did not have the self-efficacy or means to achieve them (e.g., did not have money to stay in school). Two of these respondents got married between the first and second interview rounds because they had no money, and neither were using contraception, because they were married.
Discussion
After participating in the WF intervention, most of the adolescent girls in our study envisioned and were motivated to have better futures for themselves, which they defined as having financial self-sufficiency through paid work, a well-built house, and, eventually, a husband and children. Different aspects of confidence and competence emerged as important individual-level protective factors which helped respondents make progress toward their goals and improve their well-being. Respondents in our study who expressed having hope and self-efficacy and described behavioral competence were more likely to be on track to achieving their goals, reflecting findings from other studies that having high levels of self-efficacy and hope for the future have been associated with reduced risky sexual behaviors (Abousselam et al., 2016; Dudovitz et al., 2017; Gloppen et al., 2010) and better health and well-being among adolescents (Dudovitz et al., 2017), while feeling hopeless has been associated with increased risk behaviors (Bolland, 2003). Similarly, studies have demonstrated that youth with more positive views of their futures may be less likely to take risks that could negatively impact their future goals (Gavin et al., 2010). Early marriage and childbearing, often driven by poverty, appeared to be significant obstacles to achieving future goals for some girls in our study. We found that delaying marriage and childbearing was closely tied to being more hopeful, having higher self-efficacy, and being able to take concrete actions toward achieving future goals. Our findings suggest that this relationship goes in both directions: respondents who delayed marriage and childbearing were more commonly in school and earning money and were therefore generally on track to reaching their goals, and respondents who had high hope and self-efficacy were more commonly delaying marriage and childbearing.
Despite living in very rural areas with few economic opportunities, low school attendance and availability, and high rates of child marriage and early pregnancy, respondents were remarkably optimistic about their futures and most expressed self-efficacy to attain their goals. In contrast, some respondents described crushed dreams, where the WF intervention had raised their hopes for a better future, yet the varying sustainability of the economic component left some girls without hope or the means to fully realize their goals over time. We acknowledge that characterizing respondents as lacking hope or self-efficacy if positive individual outcomes are not observed has the potential to reproduce problematic portrayals of young women, especially in relation to their sexual behaviors, and to blame them for not being able to successfully achieve their goals (Shefer, 2018). The assumption that giving adolescent girls knowledge about health and the ability to make small amounts of money would be enough to change their behaviors and improve their well-being on their own ignores the complexity and constraints of their social and structural environment. We found that limited access to secondary education and health care services impeded girls’ ability to achieve their goals echoing research that access to education, employment opportunities, and health care (e.g., contraception) impacts adolescents’ abilities and behaviors (Sawyer et al., 2012). Other studies have documented that, among adolescent girls, having educational aspirations can be protective against pregnancy and birth (Gloppen et al., 2010); staying in school (Pettifor et al., 2008, 2016) and being financially self-sufficient (S. J. Baird et al., 2012) can be protective against HIV; and staying in school can decrease the onset of sexual activity and reduce early marriage and pregnancy (S. Baird et al., 2010). Adolescent girls in Mozambique who complete secondary school are much less likely to marry by age 18, and on the flipside, child marriage is one of the main reasons adolescent girls stop attending school (UNICEF, 2015). Notably, in our study, almost all respondents from two communities that had secondary schools were on track to reach their goals. However, more than half of the study communities did not have a secondary school, which highlights structural challenges and external influences which make completing secondary education difficult and could explain why many from those communities dropped out of school. Our findings therefore support increasing external assets to improve adolescent girls’ access to higher education and improve social and economic outcomes in order to overcome structural barriers to achieving positive outcomes (Pettifor et al., 2008; Phillips & Mbizvo, 2016; Plourde et al., 2016).
Respondents expressed personal desires to delay marriage and childbearing, which, given the social context in Zambézia Province of high rates of child marriage, was an ambitious goal. Despite the desire to delay childbearing, our findings related to low contraceptive use reflect nationwide data showing that only 14% of 15- to 19-year-old adolescent girls in Mozambique use modern contraception (Ministério da Saúde, Instituto Nacional de Estatística, e ICF, 2015). In addition, the average ages respondents thought they would get married and begin childbearing were a year younger in Round 2 than Round 1, which may indicate that respondents felt, over time, that delaying marriage and childbearing were less realistic given their circumstances. Although the Go Girls! curriculum included content on the concept of family planning and specific contraceptive methods, it seems respondents had generally low contraceptive self-efficacy and use. Making highly effective long-acting reversible contraception available through youth-friendly services could enable adolescents to delay childbearing and realize their other future goals (Phillips & Mbizvo, 2016; Secura et al., 2014). However, even if girls possess self-efficacy and behavioral competence to obtain a contraceptive method, putting the onus to prevent pregnancy only on young women is problematic as one of the main reasons respondents did not use contraception was partners’ refusal. This likely reflects both traditional gender norms and the norm of newly married girls not using contraception (UNICEF, 2015), thus engaging sexual partners and communities to challenge social norms to facilitate young women’s contraceptive use is also supported by our findings. Furthermore, given that younger girls who had not yet started having sex seemed generally more hopeful and on track toward reaching their goals, programs should also consider targeting this population with efforts to delay sexual debut, keep them in school and engage their peers and communities to address inequitable gender norms.
Overall, in our study inequitable gender norms and low economic status affected respondents’ self-efficacy and ability to achieve their goals, such as staying in school and using contraception to delay childbearing. Our findings are similar to those of a study in Nepal, where girls viewed staying in school and paid work as pathways to opportunities beyond being a wife and mother, but faced restrictive social norms that often led to early marriage and childbearing (Mathur et al., 2001). In addition, respondents in our study were often unable to sustain their businesses after the WF intervention ended, resulting in decreased hope and self-efficacy beliefs as they lost the financial means to achieve their goals, such as attending secondary school. Effective sustainability planning for interventions with economic strengthening components warrant further study.
Limitations
While it would have been useful to interview participants prior to the intervention about their future aspirations and desired timing of marriage and childbearing and then compare their responses after the intervention ended, the evaluation did not take place until the intervention was ending, so this was not possible. However, interviewing the same girls after the intervention and 1 year later enabled us to analyze trends over time and examine how changes in hope and self-efficacy were related to girls’ actions to realizing their goals. In addition, interviewing the same girls at two time points about diverse aspects of their lives and building rapport and trust over time encouraged rich responses. Despite this, recall and social desirability biases may have led respondents to say what they thought the interviewer wanted to hear or avoid discussing topics or admitting behaviors that they perceived would be undesirable to the interviewer. Shame and stigma around young women’s sexuality in this setting may have reinforced negative gender norms among intervention participants and may have made it especially difficult for respondents to talk honestly about sexual behavior during the interviews (Lenzi et al., 2019; Shefer, 2018). In addition, it was somewhat difficult to interpret data related to the girls’ actual or ideal ages. The fact that data were translated from local languages to Portuguese to English also could have affected our interpretation of results. Finally, SCIP implemented many household- and community-level interventions designed to improve health and livelihoods of adolescents, women, and families in Zambézia Province in addition to WF; however, effective tracking of delivery messages was not done so it is unclear whether these interventions impacted our respondents (it did not come up in their interviews) but may have impacted their peers, partners, or families.
Implications
The findings from this analysis have important implications for future interventions that target adolescent girls in low-resource settings that are in line with the United Nations’ (2015) Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030), the World Health Organization’s Global Accelerated Action for the Health of Adolescents guidance, and PYD approaches more broadly. Focusing on cultivating both individual-level protective factors and external assets to overcome structural barriers in programs for adolescent girls in developing countries will be critical to achieving the health and gender-related SDGs (Cluver et al., 2016; Gates & Graca, 2015). Fostering individual-level protective factors such as hope for the future and self-efficacy is useful, but in contexts similar to Zambézia Province, focused efforts to promote external assets to keep girls in school, give them sustainable economic opportunities and access to reproductive health services will likely have greater impacts on pervasive problems such as early pregnancy and child marriage and enable adolescents to thrive.
Research Data
Appendix_A – Supplemental material for Hope, Self-Efficacy, and Crushed Dreams: Exploring How Adolescent Girls’ Future Aspirations Relate to Marriage and Childbearing in Rural Mozambique
Appendix_A for Hope, Self-Efficacy, and Crushed Dreams: Exploring How Adolescent Girls’ Future Aspirations Relate to Marriage and Childbearing in Rural Mozambique by Catherine Packer, Kathleen Ridgeway, Rachel Lenzi, Lázaro González-Calvo, Troy D. Moon, Ann F. Green and Holly McClain Burke in Journal of Adolescent Research
Footnotes
Acknowledgements
The authors thank the research assistants from Friends in Global Health, Mozambique, and field coordinator Samuel Martinho for collecting the data for this study. We appreciate the SCIP staff for their assistance locating the program beneficiaries. We are grateful to staff at Vanderbilt Institute for Global Health for research support and Margaret Eichleay (FHI 360) for training the data collection team and selecting the qualitative sample. We acknowledge Mary Ellen Duke (USAID/Mozambique), Amelia Peltz (USAID/Washington), and Michael Ferguson (FHI 360) for their input on the study design. We are also grateful to Dr. Donna McCarraher, Dr. Natasha Mack, and Emily Namey (FHI 360) for reviewing this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the United States Agency for International Development (USAID) Cooperative Agreement No. AID-OAA-LA-13-00001 and was made possible by the generous support of the American people through the United States Department of State, USAID, and the United States President’s Emergency Plan for AIDS Relief. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.