
Abstract
Adaptive behavior, self-determination, and health are important areas of body functions and activities identified by autistic adults as priorities for research. Past research has suggested that autistic adults have high support needs in adaptive behavior and self-determination, and have poor physical and mental health outcomes. This study included 211 autistic young adults 18–25 years old (Mage = 20.93) and their caregivers who completed questionnaires and interviews on adaptive behavior, self-determination, and physical and mental health. Correlations were examined among adaptive behavior, maladaptive behavior, self-determination, and health outcomes controlling for IQ. Adult self-reports of self-determination capacity were associated with maladaptive behavior. Reports of self-determination by caregivers were associated with adaptive behavior and maladaptive behavior. Caregiver reports of maladaptive behaviors were associated with physical health outcomes. Findings provide an initial understanding of activities, participation, body functions, and their interactions among autistic young adults.
Challenges for autistic youth during the transition to adulthood are well documented, including difficulties that are linked to contextual factors, such as limited housing options and lack of employment supports, and personal and health factors, such as mental health and interpersonal skills (e.g., Gray et al., 2014; Taylor & Seltzer, 2011; Wei et al., 2015). Viewing these challenges from a biopsychosocial framework may be helpful when considering how to support autistic individuals in their goals for adulthood. The International Classification of Functioning (ICF) uses a biopsychosocial perspective to describe the complexities underlying an individual and their contexts. The ICF conceptualizes functioning as “a dynamic interaction between a person’s health condition, environmental factors, and personal factors” (World Health Organization, 2013, p. 5). Examining the interaction between functioning and disability and contextual factors can help understand an individual better. Functioning and disability include body functioning and activities, task completion, and participation or involvement in life situations (“International Classification of Functioning, Disability, and Health: ICF,” 2001). Literature on autistic adults has identified adaptive behavior and self-determination as essential areas of activities and participation and physical and mental health as body functions (Amaral et al., 2019; Roche et al., 2021).
Adaptive behavior includes skills that individuals use in their daily lives, including conceptual skills, such as concepts of numbers, literacy, and time; social skills, such as interpersonal relationships; and practical skills, such as occupational skills and safety (Schalock, 2010). Adaptive behavior is associated with employment outcomes in adulthood. However, there is less research on adaptive behavior skills during the transition period across the range of the autism spectrum despite being ranked as a high research priority by autistic adults (Gotham et al., 2015). Self-determination, or an individual’s agency in causing things in their lives to occur, is one malleable factor suggested as another potential mechanism for improving transition outcomes in autistic adults (Shogren et al., 2018). Self-determination includes making decisions, setting and achieving goals, planning, and self-management (Shogren et al., 2018).
Furthermore, the role that adaptive behavior and self-determination may play for autistic people in health is minimally understood. Health encompasses both physical health conditions, such as obesity and diabetes, and mental health conditions, such as depression and anxiety. Autistic adolescents are more likely to have physical and mental health conditions compared with the general population (Powell et al., 2021). However, few studies have examined how adaptive behavior, self-determination, and health outcomes are related in the period of transition. This study seeks to address this gap by examining the relationships among adaptive behavior, self-determination, and health during the transition years and examining the associations.
Adaptive Behavior
A growing body of literature has identified the critical role that adaptive behavior can play in adult life for autistic individuals. Several studies have found significant associations between daily living skills and adult outcomes, such as employment and postsecondary education (e.g., Clarke et al., 2021; Farley et al., 2009; Mazzotti et al., 2021; Test et al., 2009). Higher levels of daily living skills have also been linked with higher quality of life for autistic adults (Bishop-Fitzpatrick et al., 2016) and lower caregiver burden (Marsack-Topolewski et al., 2021). Parents of autistic youth have also reported daily living skills as a primary challenge during the transition into postsecondary education (Elias & White, 2018).
Notably, adaptive behaviors are not static and may fluctuate during the transition to adulthood for autistic youth. Improvements in daily living skills during childhood may be followed by plateaus or declines, with significant variability in individual trajectories and with generally low attainment of these skills relative to neurotypical peers (e.g., Bal et al., 2015; Clarke et al., 2021; Meyer et al., 2018; Smith et al., 2012). In a sample of 179 autistic children followed longitudinally from age 2 to 21 years, Bal and colleagues (2015) found that even autistic young adults classified as having “high daily living skills” remained an average of 7 years behind typical development at age 21 years. Furthermore, autistic adults often have lower adaptive behavior skills than cognitive ability (Kraper et al., 2017; Viezel et al., 2022). Although there is some evidence that higher levels of vocational engagement may lead to improvements in daily living skills over time for autistic adults (e.g., Taylor & Mailick, 2014), few studies have explored factors that might lead to better attainment of adaptive behavior during the transition to adulthood.
Self-Determination
Self-determination refers to an individual being a causal agent in their daily activities, including the ability to express their own needs, interests, and wants, make choices, and set goals. Self-determined individuals set and take action to achieve goals based on their interests and values. Opportunities to develop self-determination during the transition to adulthood are critical (Wehmeyer & Shogren, 2017). For example, in a study examining outcomes for young adults with disabilities, Shogren et al. (2015) found that student reports of self-determination during high school were a strong predictor of employment and community living outcomes. However, only 47 of the 779 youth in the sample had a categorical label of autism. Among autistic young adults without intellectual disability, higher levels of self-reported self-determination have been associated with higher perceptions of life satisfaction (White et al., 2018) and lower levels of anxiety symptoms (Capriola-Hall et al., 2021).
Similarly, White and colleagues (2021) found parent-reported self-determination to predict gains in self-reports of college adaptation among autistic young adults with at least average range IQ. Few studies include multiple perspectives of self-determination (Morán et al., 2021). Adaptive behavior reported by teachers in high school was associated with student, teacher, and educator reports of self-determination. However, there remains a gap in knowledge regarding how self-determination may be linked to adaptive behavior and health in autistic adults across the full range of the autism spectrum.
Physical and Mental Health
Emerging evidence suggests that autistic individuals have higher rates of physical and mental health problems than non-autistic individuals (Croen et al., 2015; Kohane et al., 2012; Vohra et al., 2017; Weiss et al., 2018). These findings likely reflect contextual factors, such as limitations in the health care system and few health-focused programs designed to meet the varied needs of this population. In a large online survey of college students at 14 public institutions, autistic students reported poorer physical and mental health than their non-autistic peers, with two exceptions. They were less likely to drink heavily and had lower sleep deprivation (McLeod et al., 2019). Similarly, in a large-scale study of electronic health records of autistic individuals ages 14–25 years, Davignon and colleagues (2018) found that more than one-third (34%) of autistic individuals had a co-occurring psychiatric condition. Most psychiatric and medical conditions were more common among autistic transition-age youth/young adults compared with individuals with attention-deficit/hyperactivity disorder (ADHD) and non-autistic controls, even after controlling for sex, age, race, and duration of time within the health care system (Davignon et al., 2018). These studies point to the high risk of co-occurring health problems for autistic young adults. Questions remain, however, regarding malleable factors that might support optimal health outcomes during the transition to adulthood.
Extant research has shown that autistic adolescents and adults are less physically active and spend more time engaging in sedentary behaviors than peers without a diagnosis (McCoy & Morgan, 2020). In a nationally representative survey of adolescents, 23.3% of autistic adolescents were obese compared with 12.5% of adolescents without an autism diagnosis. In addition, 62.5% of autistic adolescents watched more than 2 hr of television per day compared with 52.2% of non-autistic adults (McCoy & Morgan, 2020). There is limited research on health behaviors related to diet that may contribute to co-occurring health conditions.
Current Study
Questions remain about the adaptive behavior, self-determination, and health outcomes in autistic young adults following the exit of high school. Studies have characterized adaptive behavior in adolescents and adults and identified childhood predictors of adult adaptive behavior, such as IQ and language (Bal et al., 2015), and associations with anxiety and depression in adulthood (Kraper et al., 2017). To date, most research on outcomes of autistic young adults has used samples dating back to 2012 (e.g., NLTS-2) and has focused on youth without intellectual disability (Duncan & Bishop, 2015; Glover et al., 2023; Kraper et al., 2017). To our knowledge, this is the first study examining the associations among adaptive behavior, self-determination, and mental and physical health outcomes in autistic young adults across cognitive abilities.
Our research questions are: (a) What are the adaptive behavior, self-determination, and mental and physical health outcomes in autistic young adults? (2) What are the associations among adaptive behavior, maladaptive behavior, self-determination, mental health, and physical health, controlling for IQ?
Method
Participants
Participants included 211 autistic young adults from the Center on Secondary Education for Students with Autism Spectrum Disorder (CSESA) Follow-Up Study (Hume et al., this issue) between 18 and 25 years old (Mage = 20.93 years, SD = 1.49) and their caregivers. Caregivers reported that the autistic young adults in this sample were 69% White, 12% Black, 6% Multiracial, 5% Asian, 3% American Indian or Alaskan Native, 4% Not Listed, and 16% reported being Hispanic. Only 8% of the sample was living independently. See the work by Hume et al. (this issue) for complete sample characteristics and a study description.
Procedures
Measures used in this study were part of the larger assessment battery of the CSESA Follow-Up Study (Hume et al., this issue). Caregivers completed surveys, standardized assessments, and parent interviews. Autistic young adults completed surveys and an interview. Information about health outcomes, adaptive behavior, and self-determination was derived from surveys and standardized assessments. At the beginning of participation in the original CSESA study (Hume et al., 2022), the research team assessed non-verbal IQ. Research staff administered four subscales from the Leiter International Performance Scale–Third Edition (Leiter-3, Roid et al., 2013) with participants to obtain a brief non-verbal IQ.
Measures
Adaptive behavior and maladaptive behavior
During the parent follow-up interview, caregivers provided information about the young autistic adults’ living situation and completed questionnaires on adaptive behavior and maladaptive behavior. Adaptive behavior was assessed using the Scales of Independent Behavior-Revised (SIB-R; Bruininks et al., 1996). The SIB-R tool measures adaptive and maladaptive behaviors and is a comprehensive, norm-referenced assessment. The SIB-R was completed as an interview via phone or in-person or as a checklist. Caregivers are asked to rate how well the autistic young adult can do adaptive behavior tasks without help or supervision from a scale of Never or Rarely, even if asked to Does very well, almost, or almost always without being asked. Adaptive behavior domains include motor skills, social interaction and communication skills, personal living skills, and community living skills. Skills are representative across the lifespan.
The motor skills domain includes gross motor (i.e., pounding a nail with a hammer, doing push-ups, and strenuous physical activity participation on a regular basis) and fine motor (i.e., replacing small screws, nuts, and washers, and assembling objects with small parts). The social interaction and communication skills domain includes social interaction (i.e., entertaining and making plans with friends and having constructive conversations with others during disagreements), language comprehension (i.e., looking up needed information, reading articles, and summarizing details from lectures or speeches), and language expression (i.e., making oral and written reports for community groups, and filling out forms and contracts). The personal living skills domain includes eating and meal preparation (i.e., preparing shopping lists and making meals for self and family), toileting (i.e., using restrooms in unfamiliar places and replacing emptied rolls of toilet paper), dressing (i.e., buying appropriate size clothing and ironing or pressing clothes), personal self-care (i.e., taking own temperature and making medical appointments), and domestic skills (i.e., taking out the trash, performing maintenance around the home). The community living skills domain includes time and punctuality (i.e., setting timers, writing down scheduled events on a calendar), money and value (i.e., budgeting expenses, tipping appropriately), work skills (i.e., discussing criticism with a work supervisor, informing employer when unable to work), and home/community orientation (i.e., giving directions to others when asked, driving, making travel plans).
Caregivers were also asked to rate the frequency of maladaptive behaviors from 1 (Less than once a month) to 5 (1 or more times an hour) and the severity of behaviors from 0 (not serious) to 4 (extremely serious) across asocial, internalizing, and externalizing behaviors. Asocial behaviors include disruptive behavior and socially offensive behavior. Internalizing behaviors include hurtful to self, unusual or repetitive habits, and withdrawal or inattentive behavior. Externalizing behaviors include being hurtful to others, destruction of property, and disruptive behavior. Index scores are created based on the frequency and severity ratings. They range between very serious (−41 and below), serious (−31 to −40), moderately serious (−21 to −30), marginally serious (−11 to −20), and normal (−10 to +10).
Self-determination
Self-determination was assessed using a self- and caregiver-reported questionnaire, the American Institutes for Research Self-Determination Scale (AIR-SDS; Wolman et al., 1994). This tool measures individuals’ capacity and opportunity for self-determination. The current study used the Capacity subdomain, which consists of 12 items (for autistic young adults) and 6 items (for caregivers) on a five-point rating scale. The AIR-SDS demonstrated high reliability for the self-report (Cronbach’s alpha = .92) and caregiver report (Cronbach’s alpha = .91).
Health outcomes
Health outcomes were included as part of the Demographic Form and Parent Follow-Up Check-In. On the Demographic Form, caregivers reported the presence of mental health or other conditions (anxiety, ADHD, bipolar disorder, depression, obsessive-compulsive disorder, and schizophrenia). Body mass index (BMI) was calculated based on caregiver reports of height and weight. On the Parent Follow-Up Check-In, caregivers reported the presence of 10 physical conditions the young autistic adults were diagnosed with or treated for in the past 12 months (e.g., asthma, gastrointestinal [GI] issues, sleep disturbance). Caregivers also rated the autistic young adults’ health on a four-point scale (1 = poor, 2 = fair, 3 = good, 4 = excellent). Considerable previous research has provided evidence of the validity of such health ratings in the general population (Idler & Benyamini, 1997) and in autistic adults (DaWalt et al., 2019).
Engaging in health behaviors
Caregivers were asked to think about a typical week in the autistic young adults’ lives to provide information about exercise, diet, and the impact of health on adaptive behavior. Exercise questions asked included “How many times in one week does [the autistic young adult] exercise (e.g., walking, jogging, jumping rope, karate) or go to a fitness center to work out?” and “How many times in one week does [the autistic young adult] work, play, or exercise hard enough to make them sweat and breathe heavily?” Response options included from 0 to 8 or more times.
Diet questions included “How many regular(non-diet) sweetened drinks does [the autistic young adult] have in one week?” and “How many days in one week does [the autistic young adult] eat fast food from restaurants?” Response options ranged from 0 to 11 or more. Caregivers were also asked, “On average, how many hours per day does [the autistic young adult] watch television or videos, play video games or use a computer, tablet or smartphone?” with response options from 0 to 5 or more hours. Caregivers were also asked whether the autistic young adults’ health limited their ability to do school or work, household chores, shopping or errands, and personal care or hygiene.
Data Analyses
Descriptive statistics were used to characterize adaptive behavior, self-determination, and physical and mental health outcomes and health behaviors of autistic young adults (Research Question 1). Partial correlations were conducted to examine the associations among adaptive behavior, maladaptive behavior, self-determination, and mental and physical health controlling for IQ (Research Question 2)
Results
Adaptive Behavior Profile
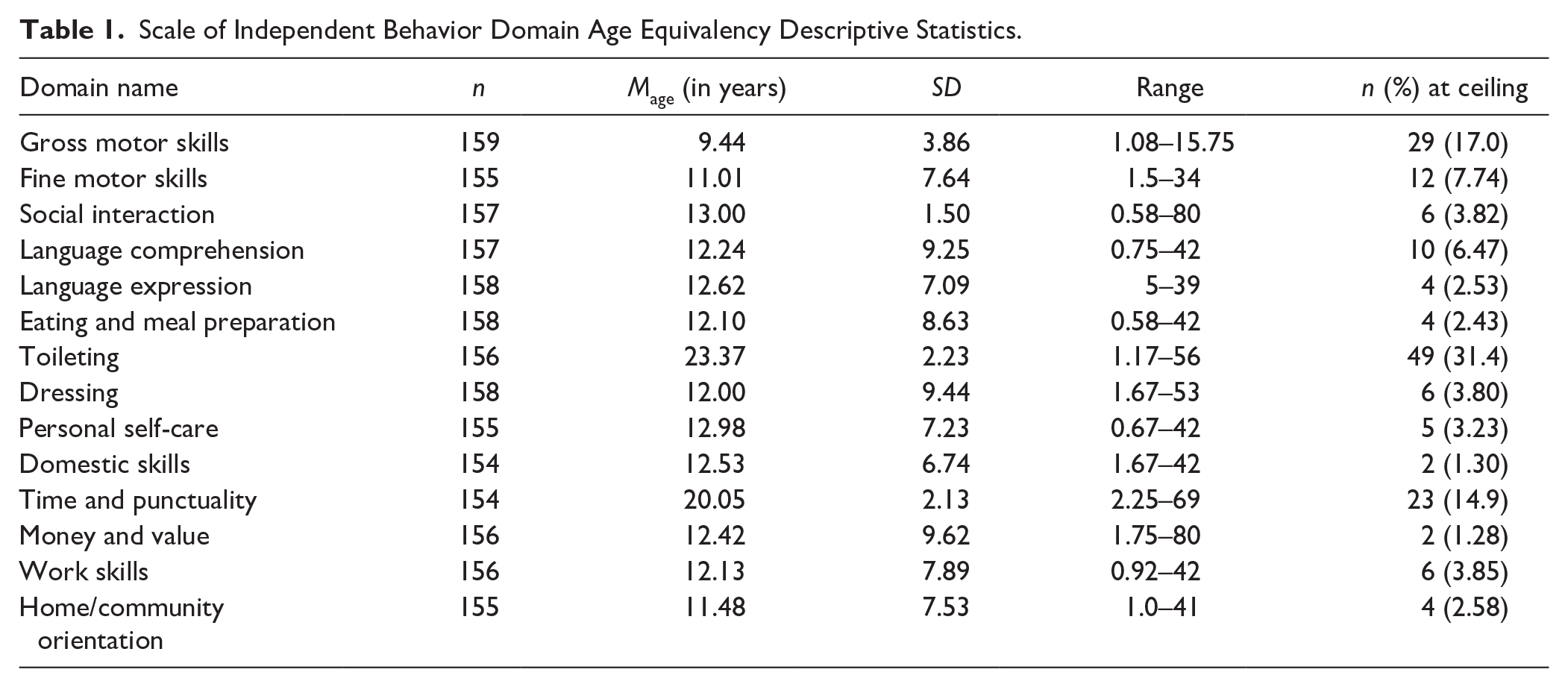
Table 1 shows the age equivalence scores on the SIB-R domains. A repeated-measures multivariate analysis of variance (MANOVA) was conducted to identify within-domain differences on adaptive behavior age equivalency scores on the SIB-R. Overall, the tests of within-subjects effects using Greenhouse–Geisser estimation due to violation of sphericity were statistically significant, F(4.16, 120) = 24.05, p < .001, n2 = .15. Autistic young adults had statistically significant differences across adaptive behavior. On average, autistic young adults demonstrated the highest age equivalency scores in Toileting and Time and Punctuality. These two area age equivalency scores were close to their chronological age (20–23 years). The remaining domains had lower age equivalency scores than chronological ages. The domains of social interaction, language comprehension, language expression, eating and meal preparation, dressing, personal self-care, domestic skills, money and value, work skills, and home/community orientation age equivalency scores did not significantly differ from each other (age equivalency ranges = 11–13). Motor skills were significantly lower than the social interaction, personal living, and community living domains (age equivalency = 9).
Scale of Independent Behavior Domain Age Equivalency Descriptive Statistics.
Self-Determination
A repeated-measures MANOVA was conducted to identify within-item differences in self-determination for students and caregivers. For autistic adults, the overall test of within-subject effects using Greenhouse–Geisser estimation due to violation of sphericity was significant, F(8.40, 1,150.7) = 10.34, p < .001, n2 = .07. Autistic adults rated themselves the highest on, “I know what I need, what I like, and what I’m good at,” “I feel good about what I like, what I want, and what I need to do,” “I believe that I can set goals to get what I want,” and “I like to make plans to meet my goals” in the capacity domain and all items on the opportunities at home domain, with the exception of “At home, I have learned how to make plans to meet my goals and to feel good about them.” See Tables 2 and 3 for descriptive statistics of AIR-SDS. Overall, autistic young adults rated opportunities at home domain as higher (M = 4.15, SD = .80) than the capacity domain (M = 3.84, SD = .77, t(141) = 4.29, p < .001, Cohen’s d = .84).
AIR-Self-Determination Capacity Scale Descriptive Statistics.
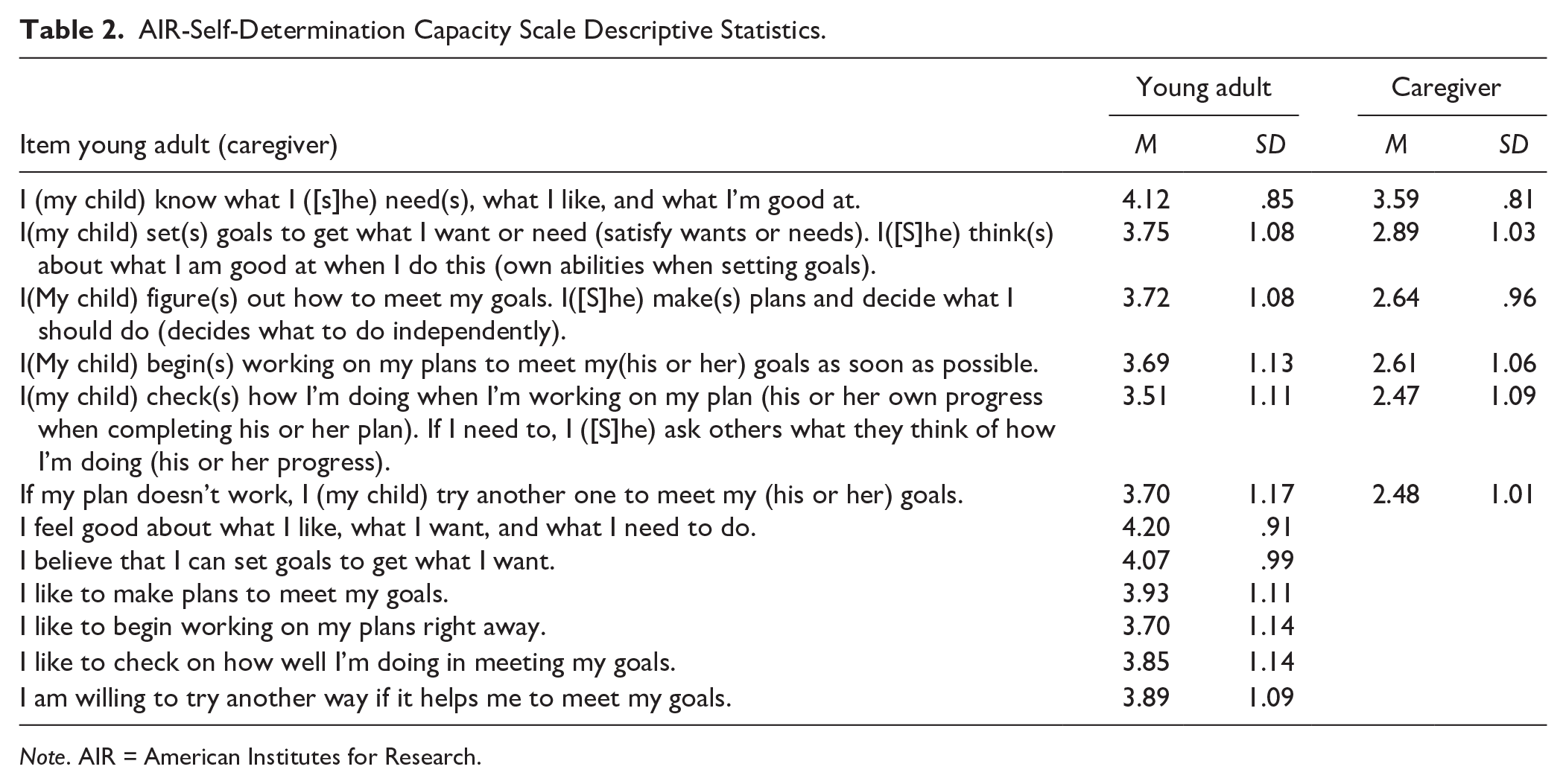
Note. AIR = American Institutes for Research.
AIR-Self-Determination Opportunity at Home Scale Descriptive Statistics.
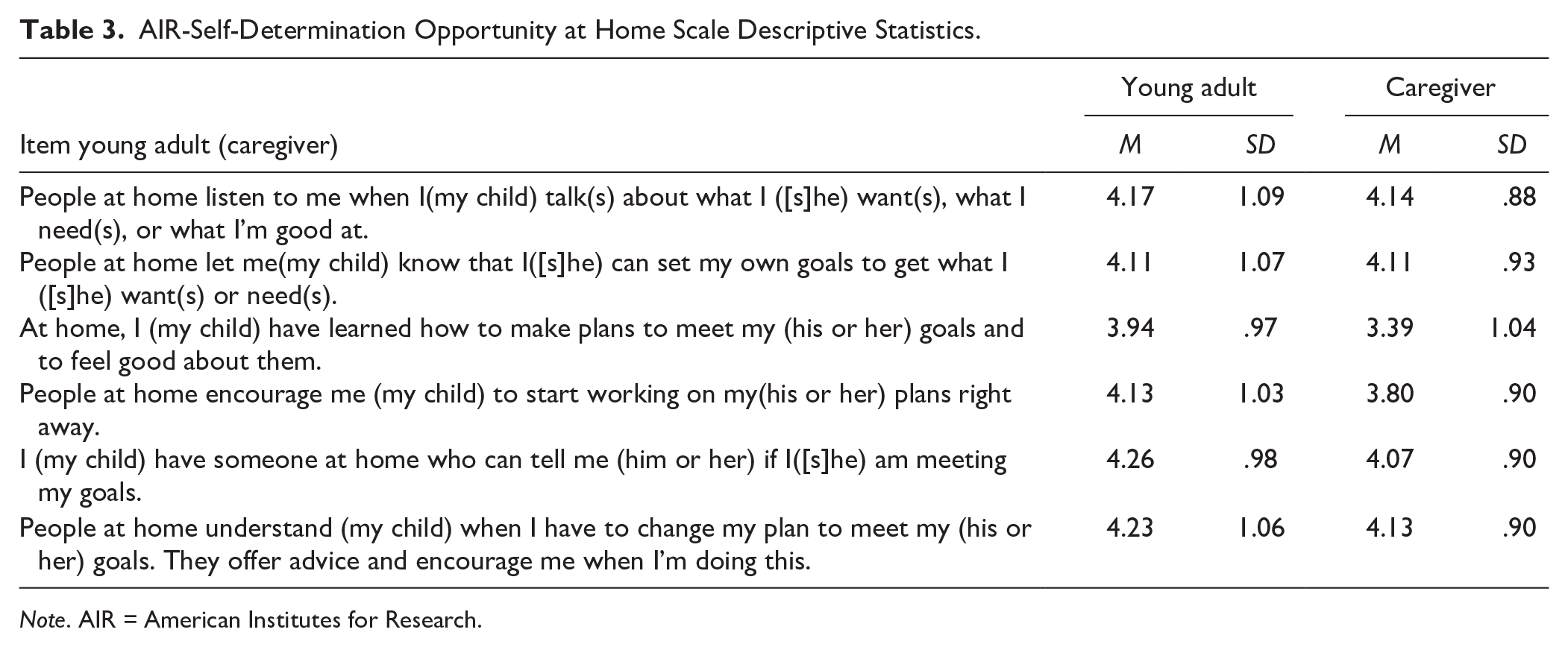
Note. AIR = American Institutes for Research.
For caregivers, the overall test of within-subject effects using Greenhouse–Geisser estimation due to violation of sphericity was significant, F(4.91, 913.80) = 183.83, p = 001, n2 = .50. Caregivers rated “My child knows what (s)he needs, likes, and is good at.” as higher than all other Capacity domain items, and caregivers rated Opportunity at Home items as significantly higher than all Capacity items. “My child checks his or her own progress when completing his or her plan. (S)he asks others what they think of his or her progress.” In addition, “If my plan doesn’t work, my child tries another one to meet his or her goals” were the lowest Capacity items. On the Opportunity at Home domain, “At home, my child has learned how to make plans to meet his or her own goals and to feel good about them.” In addition, “At home, my child is allowed to act on his or her plans right away.” were the lowest. Overall, caregivers rated Opportunities at Home as higher (M = 3.93, SD = .73) than Capacity (M = 2.78, SD = .80), t(189) = 19.74, p < .001, Cohen’s d = .81.
Mental and Physical Health Outcomes
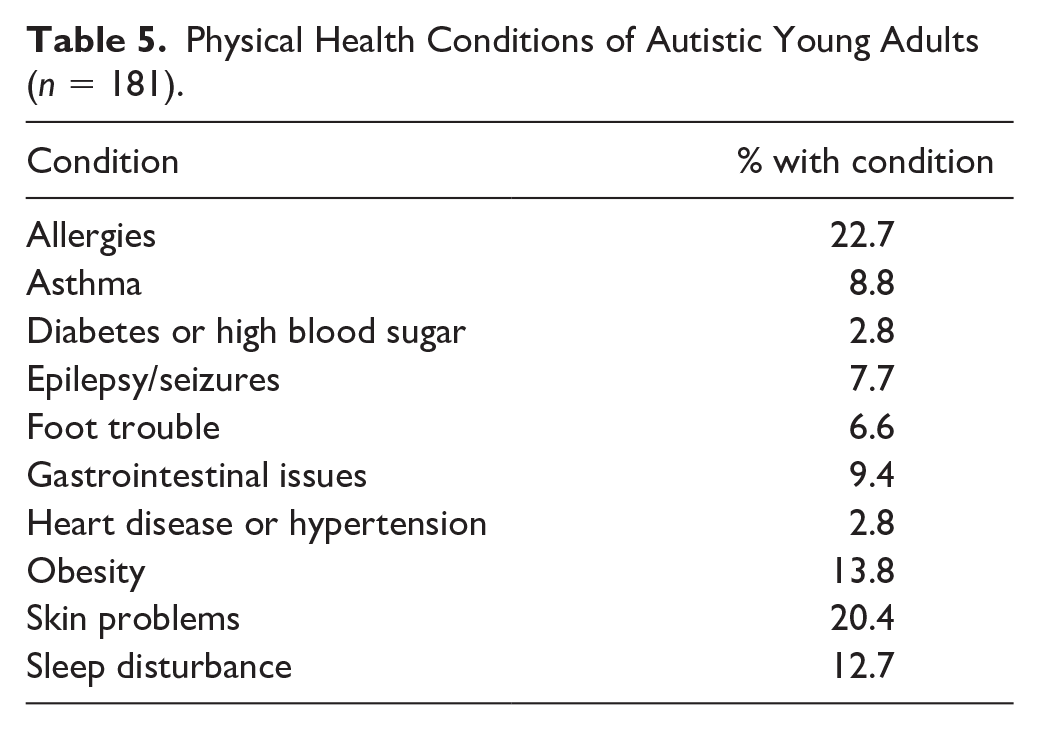
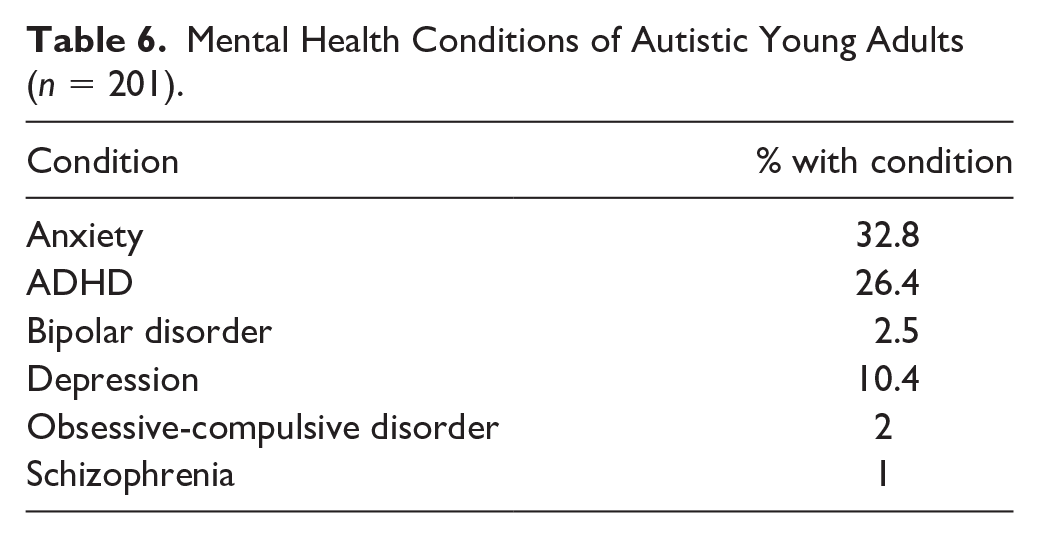
Caregivers of autistic adults reported that 50.9% of the sample were in good health, 36.4% were in excellent health, 11.0% were in fair health, and 1.7% were in poor health. Participants were, on average, in the overweight category on the BMI (M = 26.58, SD = 6.83). Approximately, 54% of the sample were either overweight or obese, with 39% of the sample in the normal category and 6% underweight. Caregivers reported 1.23 total health conditions on average (M = 1.23, SD = 1.45, range = 0–8), with 59.7% reporting at least one physical or mental health condition and 25% of the sample reported at least one mental health condition. Table 4 shows the overall descriptive statistics of health conditions. Table 5 shows the prevalence of physical health conditions in the sample. The most commonly reported physical health conditions included allergies (22.7%), skin problems (20.4%), sleep disturbance (12.7%), and GI issues (9.4%). Table 6 shows the prevalence of mental health conditions in the sample. The most frequently reported mental health conditions were anxiety (32.8%) and depression (10.4%)
Descriptive Statistics.
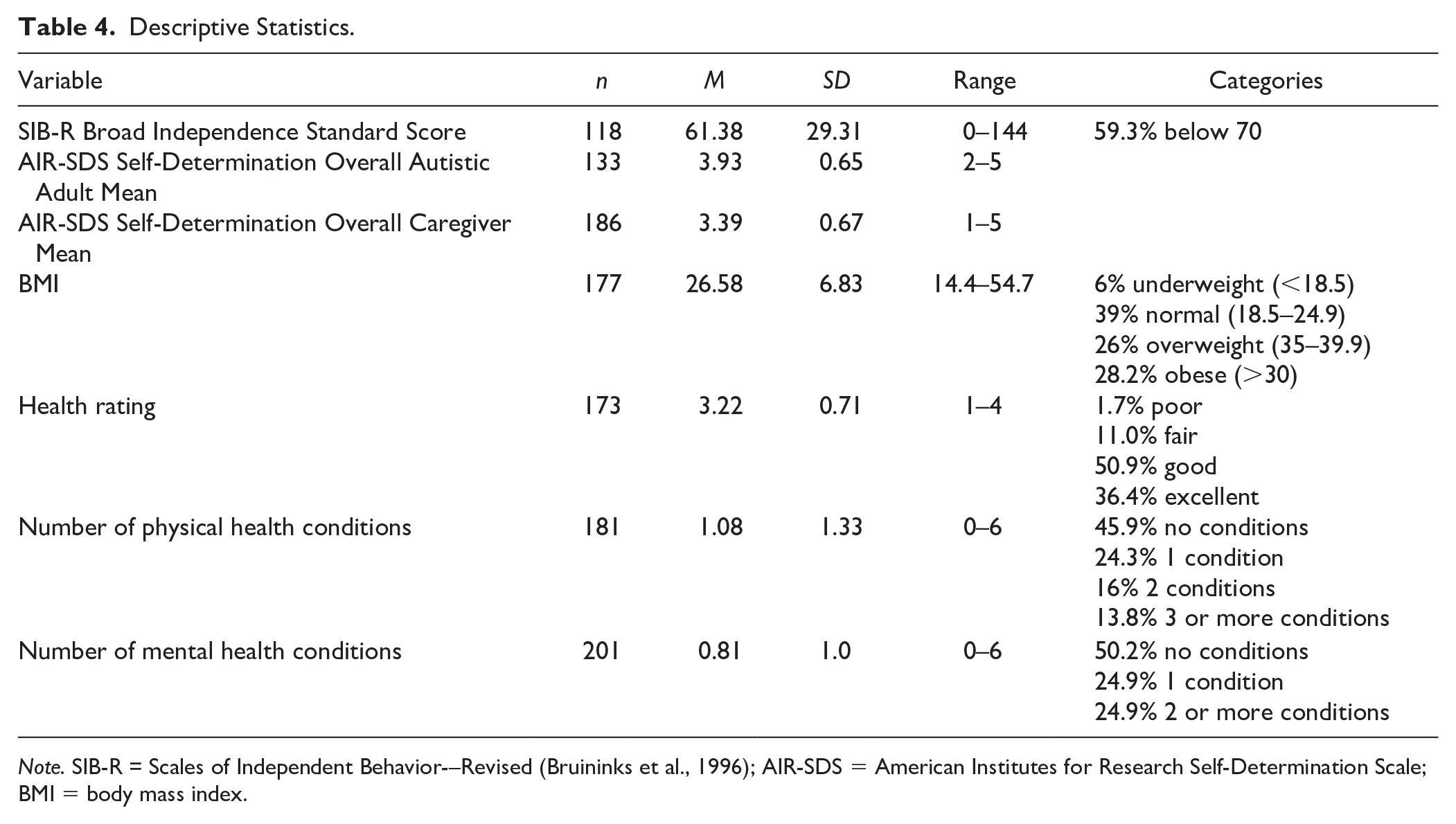
Note. SIB-R = Scales of Independent Behavior-–Revised (Bruininks et al., 1996); AIR-SDS = American Institutes for Research Self-Determination Scale; BMI = body mass index.
Physical Health Conditions of Autistic Young Adults (n = 181).
Mental Health Conditions of Autistic Young Adults (n = 201).
Engaging in Health Behaviors
Caregivers reported whether the health conditions of autistic adults limited the adults’ participation in daily living activities. Caregivers reported that overall, health conditions limited autistic young adults’ ability to participate in at least one activity in 11% of the sample. Specifically, daily participation limitation was reported for things such as going to school or work (9.9%), performing chores or running errands (7.2%), and personal care or hygiene (7.2%). Caregivers also reported health behaviors in exercise frequency, drinking sweetened drinks, eating fast food, and hours spent playing video games or engaging in screen time. Caregivers reported that 19.9% of young autistic adults were not engaging in any kind of exercise and 30.4% were not engaging in moderate to vigorous physical activity. Caregivers reported that 22.5% of autistic young adults were consuming seven or more sweetened drinks, and 18% were eating fast food four or more times a week. However, 44.9% of autistic young adults were spending five or more hours a day playing video games, watching television, or using their phones.
Associations Among Adaptive Behavior, Maladaptive Behavior, Self-Determination, and Health Outcomes
Partial correlations were performed using total scores of caregiver-reported adaptive behavior, autistic young adult self-report of self-determination capacity, caregiver report of self-determination capacity, and physical and mental health outcomes controlling for IQ (see Table 7). Higher caregiver-reported adaptive behavior was significantly associated with fewer maladaptive behaviors and higher caregiver-reported self-determination scores. Lower caregiver-reported maladaptive behavior scores were associated with higher caregiver-reported self-determination, higher adult-reported self-determination capacity, and fewer number of physical health conditions.
Partial Correlations Among Adaptive Behavior, Maladaptive Behavior, Self-Determination, Mental Health, and Physical Health Controlling for IQ.
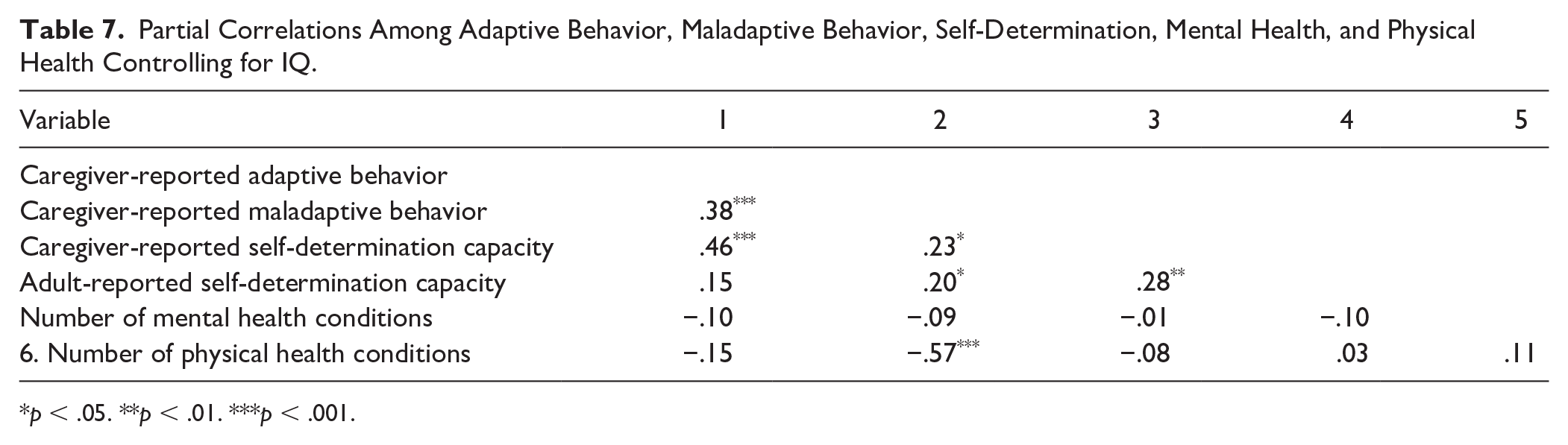
p < .05. **p < .01. ***p < .001.
Discussion
This study characterized the aspects of functioning and disability in autistic young adults through the examination of activities and participation of adaptive behavior and self-determination and body functions of physical and mental health conditions and examining their associations controlling for IQ. Caregivers of autistic young adults reported on the presence of physical and mental health conditions, health behaviors, and adaptive behavior; self-determination and young adults reported on self-determination. Importantly, we found that many young autistic adults in our sample, across the level of intellectual ability level, were experiencing health concerns and limitations in their adaptive behavior.
Adaptive Behavior
This study found that autistic young adults had adaptive behavior significantly below their chronological age regardless of IQ across the majority of areas. Two areas of relative strength were Time and Punctuality, or skills related to keeping track of time and dates, setting dates and appointments, and understanding the passage of time, and Toileting, including using the restroom and identifying the restroom in unfamiliar locations. The gross motor domain was identified as having the lowest mean age equivalency scores in this sample. However, the maximum age equivalency score is 15 years 9 months on the assessment, so it may be that is why the mean age equivalency score was lower. We would expect more individuals to be at the ceiling on this domain and only 17% of the sample was at the ceiling, indicating that fewer autistic adults were taking part “in strenuous activities on a regular basis” and “paint[ing] the inside walls and trim around windows in doors” than anticipated for their chronological age. Therefore, it may be that the lack of participation in exercise as reported by caregivers as well, could be a contributing factor for the lowest scores being in the gross motor domain.
Self-Determination
Young autistic adults rated themselves on average, almost always, across self-determination items, and caregivers rated them as sometimes across self-determination items. Autistic adults and caregivers rated opportunities at home as higher than capacity. The highest capacity item for both parents and caregivers was focused on the individual knowing what they need, like, and what they are good at. Autistic adults rated the highest item as one in which they feel good about what they like, want, and need to do. According to young adults and caregivers, they may need more support in making plans, checking progress on their plans, and trying new plans. Young adults and caregivers rated opportunities to make plans as the lowest item on the opportunity at home domain. These findings suggest that planning and self-monitoring of plans may be the important areas in supporting autistic adults.
The Self-Determined Learning Model of Instruction is one evidence-based intervention that supports autistic adolescents in high school settings in setting goals, planning, and evaluating their goals (Shogren et al., 2018, 2019). Students receiving Self-Determined Learning Model of Instruction (SLDMI) report an emerging empowerment, improved grades, and increased engagement in class (Kiblen et al., 2024). Future research should follow students receiving SLDMI in high school and examine the impact on their young adult outcomes. In addition, autistic adults may benefit from the Self-Determined Career Development Model on Self-Determination, which has demonstrated efficacy in adults with disabilities (Shogren et al., 2016).
Mental and Physical Health
Caregivers reported that 36.4% of autistic young adults in the current sample were in excellent health, which is lower than the national samples of health status in adolescents. In the 2020–2021 National Survey of Children’s Health, 86% of caregivers reported that their 12- to 17-year olds were in excellent health (Child and Adolescent Health Measurement Initiative, 2021). Caregivers reported that 12.7% of our sample of autistic young adults were in poor or fair health compared with 3.9% (2018) to 6.5% (2019) young adults 18–24 years of age reported in the National Center for Health Statistics, National Health Interview Survey (National Center for Health Statistics, 2020). Thus, while a majority of autistic young adults in our sample were in good health, caregivers were reporting more individuals in poor or fair health compared with population surveys in children and young adults in the United States. Almost half of the sample had a mental health condition, with close to a third of the sample having a diagnosis of anxiety. This is consistent with prior studies which found higher rates of health conditions for transition-age autistic youth compared with non-autistic youth (Davignon et al., 2018; McLeod et al., 2019). Notably, in the current study, 11% of the caregivers reported that health conditions interfere with their autistic young adult’s ability to do daily activities, such as go to work or school. Furthermore, we found that over half of the sample had at least one physical health condition, with allergies, skin problems, sleep disturbance, and GI problems being the most common.
Of particular concern, our sample had high rates of being overweight (26%) or obese (28.2%) based on their BMI. The prevalence of obesity has risen in the United States from 5.5% to 32.6% since 1976 (Ellison-Barnes et al., 2021), and autistic young adults also experience this high rate of obesity. Although obesity rates in our study are similar to national norms (Aggarwal et al., 2023; Ellison-Barnes et al., 2021), autistic adolescents and young adults often do not engage in recommended physical activity levels and given the current study did not have a comparison group future research is warranted in examining physical activity (Sorensen & Zarrett, 2014). Physical activity engagement levels continue to drop as autistic adults transition to adulthood (Garcia‑Pastor et al., 2019). Autistic children and adolescents tend to be more physically inactive than typically developing adolescents (Broder-Fingert et al., 2014; McCoy & Morgan, 2020). In our study, we found that 19.9% of autistic young adults were not engaging in physical activity of any kind during the week. Furthermore, almost half of the sample spent 5 hr or more a day on screen time and 18% were eating fast food four or more times a week. Future research is needed to identify if these rates are on par with the general population. With rising rates of obesity in the general population, and the potential for additional risk factors and co-occurring health problems for autistic individuals, programs are needed to focus on health and healthy behaviors for autistic young adults. Future research should also examine the environmental context of the ICF framework to identify what environmental factors support or hinder aspects of functioning in autistic adults.
In the current study, we also were able to test for associations of adaptive behavior. We found that higher levels of capacity for self-determination were associated with higher adaptive behavior. Similar to prior studies which documented linkages between emotional and behavioral problems and adaptive behavior in adults (e.g., Gray et al., 2014), we found that lower levels of maladaptive behaviors were associated with higher adaptive behavior. Regarding physical health, we did not find an association between higher youth- or caregiver-reported self-determination capacity and physical health ratings. This slightly diverges from the previous findings that self-determination capacity has a modest positive impact on physical health (Ntoumanis et al., 2021). We did, however, find that higher levels of maladaptive behaviors were associated with a greater number of physical health conditions. This finding aligns with several studies noting the relationship of specific physical health conditions (i.e., GI disorders, epilepsy) and maladaptive behaviors in children with autism (Pusponegoro et al., 2015; Viscidi et al., 2014). The literature on the connection of physical health conditions to maladaptive behaviors in autistic adults is less clear (Forde et al., 2022), and thus, this association warrants further investigation. Nevertheless, these findings highlight the critical intersection of activities and participation and body functions and the importance of continued work examining these constructs.
Limitations and Conclusion
This study has several limitations. Data reported in this study were only collected at one timepoint. Another limitation in this study was the lack of measures of self-report from autistic young adults on health conditions and adaptive behavior. Capturing the experiences of autistic young adults on their perceptions of their health conditions and adaptive behavior is critical in identifying priorities for future programs. Including both caregiver and young adult perspectives in future research is warranted. In addition, future research should include the measures of specific symptomatology for mental health, rather than only a checklist of conditions, and other objective measures of physical health, such as blood pressure, time spent on moderate to vigorous activities through the use of activity trackers, and body composition. The limitations of this study are juxtaposed with several strengths. We were able to examine a wide range of indicators of health, health behaviors, and adaptive behavior in a contemporary, racially, and ethnically diverse sample of autistic young adults. Our main predictor of interest, self-determination, was measured using both young adult and caregiver reports.
This study described and examined the correlations among adaptive behavior, self-determination, and physical and mental health conditions for a diverse sample of autistic young adults. Future research should continue to work to identify the correlates of autistic young adults’ health outcomes as they continue to experience more physical and mental health conditions than their peers without disabilities. The associations found in this study between self-determination capacity and adaptive behaviors may inform future intervention development and implementation. Pairing self-determination capacity building with adaptive behavior programming may bolster the acquisition of skills in both domains.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The work reported here was supported by the Institute of Education Sciences, U.S. Department of Education (grant no. R324A180091) awarded to UNC-Chapel Hill. The opinions expressed represent those of the authors and do not represent the views of the Institute or the U.S. Department of Education. B.T. was supported by the Department of Defense (grant no. W81XWH-19-1-0826).