
Abstract
Mexican American caregivers of individuals with Alzheimer’s Disease face unique stressors and challenges, which may be influenced by cultural, socioeconomic, and systemic factors. This population often assumes caregiving responsibilities based on strong cultural values of familismo which emphasizes family duty and collective care. However, this commitment can lead to increased emotional strain, mental health concerns, financial and physical strain, particularly when caregivers have limited access to healthcare resources, financial support, or respite. Language barriers and a lack of culturally competent healthcare services can further exacerbate stress, making it difficult to navigate the complex healthcare system. The purpose of this study was to identify key stressors and challenges affecting Mexican American caregivers of Alzheimer’s Disease patients. A qualitative approach was employed to capture the lived experiences of Mexican American caregivers. To analyze the data, researchers used the Stress and Coping model. Two overarching themes identified were adjusting to caregiving and the impact on the caregiver’s life. Addressing the unique needs of Mexican American caregivers requires culturally sensitive interventions, resources, support systems to reduce stress and improve caregiving outcomes. The study emphasizes the need for systemic change to better support Mexican American caregivers.
Introduction
Caring for loved ones with Alzheimer’s Disease presents unique challenges that extend beyond routine care, demanding both emotional and physical endurance from caregivers. Because Alzheimer’s Disease is a progressive, neurocognitive disorder that leads to a decline in memory, cognitive abilities, and behavior, this process makes patients increasingly dependent on others for activities of daily living. As the disease progresses, caregivers often find themselves navigating complex medical, emotional, and social needs while managing their own well-being.
It is not unusual for caregivers to change one or more aspects of their lives to accommodate the needs of their loved ones. Some of these changes can include anything from reducing their work hours to quitting their jobs altogether. For others, it could mean having to leave their home possibly leaving their own children and spouse behind and moving to another state (Perry & Thiels, 2016). Whatever the changes might be, they often create stress for the caregiver, even when the caregiver has wholeheartedly made the decision to serve in this capacity. Frequently, caregivers find themselves with little or no support as they begin these duties; thus, the combination of the caregiving stress and the lack of support can lead to the caregiver experiencing their own physical and mental health challenges (Anderson & White, 2018; Corvin et al., 2017).
According to the Alzheimer’s Association (2024), almost 6.9 million older adults suffer from Alzheimer’s Disease or a related dementia. Older Latinos are particularly vulnerable as they are 1.5 times more likely than non-Hispanic whites to be diagnosed with the disease (Turner et al., 2015). By the year 2060, the prevalence of Alzheimer Disease in older Hispanics is projected to increase sevenfold over current estimates. Considering that Hispanics are the fastest growing ethnic group in the nation (Pew Research Center, 2025), it is important to study the factors that contribute to ethnic and racial disparities in the Alzheimer’s Disease diagnoses (Rodriguez et al., 2024). This increase in the number of older Latinos diagnosed with Alzheimer’s leads to many Hispanics/Latinos who will assume the role of a caregiver (Llanque & Enriquez, 2012). There is growing evidence that Latinos have the highest percentage of family caregivers over all other ethnic groups including non-Hispanic Whites (Turner et al., 2015).
The South Texas-Mexico border is largely Hispanic with percentages varying from 89% to 95% in counties situated along the border (U.S. Census, 2020). Compared to the percentage of Hispanics/Latinos in Texas (39.3%), these numbers are almost three times the number of individuals who identify as Hispanic/Latino. This area is largely low income with an average household income of $55,300 with about 25% of the population living in poverty (U.S. Census 2020). This is approximately $20,480 less than the average household income in the state of Texas as a whole. The area also has high rates of uninsured individuals when compared to the State of Texas (18%). On average, 26% of the population living in the counties along the South Texas border are uninsured. Finally, the language spoken at home is often a language other than English (mostly Spanish) with an average of 76%, compared to 35.4% average in the state of Texas.
Literature Review
According to the literature, caregivers of patients with Alzheimer’s Disease and other dementias experience higher rates of depression, role stress, family conflict, poorer self-rated health, alterations in immune functioning, and even increased mortality (Arevalo-Flechas et al., 2014; Brodaty & Donkin, 2009; Gelman, 2010; Schulz & Sherwood, 2008). Latino caregivers have reported unique challenges when providing care for patients with Alzheimer’s disease, which differ significantly from those faced by White or Caucasian caregivers. These differences are crucial for understanding the Latino caregiving stress process. Latino caregivers are more likely to quit their jobs to provide care and often share caregiving responsibilities more than other racial and ethnic groups (Hilgeman et al., 2009). Caregiving within Latinos is shaped by distinct cultural themes that play a significant role. These themes, which include denial, family obligation, and the utilization of formal services, contribute positively to how caregiving is approached and managed (Nair et al., 2013). Understanding these influences can help enhance the support systems and resources available to Latino caregivers.
Furthermore, the literature also indicates that Latino caregivers have experienced health disparities in accessibility of appropriate health services resulting in inequitable service use (Smedley et al., 2003). This is also associated with dementia behavioral problems and caregiving distress among Latino caregivers (Gelman, 2014; Gurland et al., 1999; Pinquart & Sorensen, 2005). Increasing numbers of older persons in the Latino population places unforeseen long-term care demands on Latino caregivers (Aranda & Knight, 1997; Mage et al., 2024; Rote et al., 2015). Prior studies on Hispanic and Mexican American families have emphasized the role of cultural values, namely familismo in the role of caregiving (Hahn et al., 2011; Hernandez & Bigati, 2010; Herrera et al., 2013).
The value of familismo is the belief that family ties are very strong among Mexican American families, and there is an expectation (this can be both spoken and unspoken) that family members will prioritize family needs above all else, and that family members will be both dedicated and loyal. In a study conducted by Jaldin et al. (2023), researchers found that the cultural value of familismo influenced the decision to serve as caregivers for loved ones. Gouveia Marques et al. (2017) found that familismo was largely related to the older adult’s desire to remain in their home rather than moving to a care facility.
It is often stated that Hispanics and, particularly Mexican Americans place family interest above individual interest (Aranda & Knight, 1997; John et al., 1997; Sayegh & Knight, 2011). Caregiving may represent filial duty and be seen as an expected part of the life course, especially for women. Indeed, a large percentage of Latino caregivers in the United States believe their role is an expectation within their upbringing (Evercare and National Alliance on Caregiving, 2008). In addition, past research also suggests that Hispanic/Latinos endorse family centered care, meaning that caregivers may prefer the person with dementia to be cared for by family members rather than professional caregivers (Llanque & Enriquez, 2012; Martinez & Acosta Gonzalez, 2022; Mendez-Luck & Anthony, 2016). While these values can serve as protective factors, they may also contribute to increased caregiver burden when formal support services are underutilized due to cultural stigma, denial of the disease, or mistrust in institutional care (Martinez & Acosta Gonzalez, 2022).
Despite the long-held view that Latinos’ values and reliance on family leads to greater involvement of extended family in caregiving for sick members and reduced perception of burden, some research also supports low levels of social support and high levels of distress among Latino caregivers (Gelman, 2014; Mendez-Luck et al., 2020). The literature also indicates that Latino caregivers have health disparities associated with dementia behavior problems and caregiving distress and depression (Carmin & Ownsby, 2010; Turner et al., 2015). Although there has been extensive research on the phenomenon of dementia caregiving, the impact of cultural influences on caregiving has been less explored (Neary & Mahoney, 2005). Additionally, given the continued, expected growth of the Latino population (Pew Research Center, 2022), it is important to explore the impact of these challenges and stressors experienced by familial caregivers.
Considering the limited literature on Mexican American caregiving experiences, the purpose of this study was to explore the caregiving experience of Mexican American caregivers along the South Texas border. This study aims to answer the research question: What are the stressors and challenges faced by Mexican American caregivers of patients with Alzheimer’s Disease?
Methodology
The ways in which Mexican Americans view Alzheimer’s Disease caregiving and create meaning from their caregiving experience is best studied using a qualitative approach, according to Padgett (2016). In this study, a qualitative methodology was used to explore Mexican American caregivers of loved ones with Alzheimer’s Disease.
Setting
The study consisted of 15 telephone interviews with Mexican American caregivers of Alzheimer’s Disease recruited along the South Texas/Mexico Border. This study took place during the COVID lockdown so finding the sample came with some difficulties because community organizations and providers like the Alzheimer’s Association and Caregiver Support groups were not open to the public. Instead, these caregivers were recruited with assistance from the Promotoras (Community Health Workers) who work in the Rio Grande Valley and the Laredo communities and/or colonias. Colonias are defined as neighborhoods in the lower South Texas-Mexico border whose majority population is comprised of individuals and families with low to very low income (Texas Department of Housing and Community Affairs, 2025). After Institutional Review Board (IRB) approval, the primary author met with the Promotoras staff to explain the study’s purpose, the sample selection criteria, and the researchers’ contact information. Those promotoras contacted potential participants who were identified and provided the researcher’s contact information to schedule an interview.
Participants
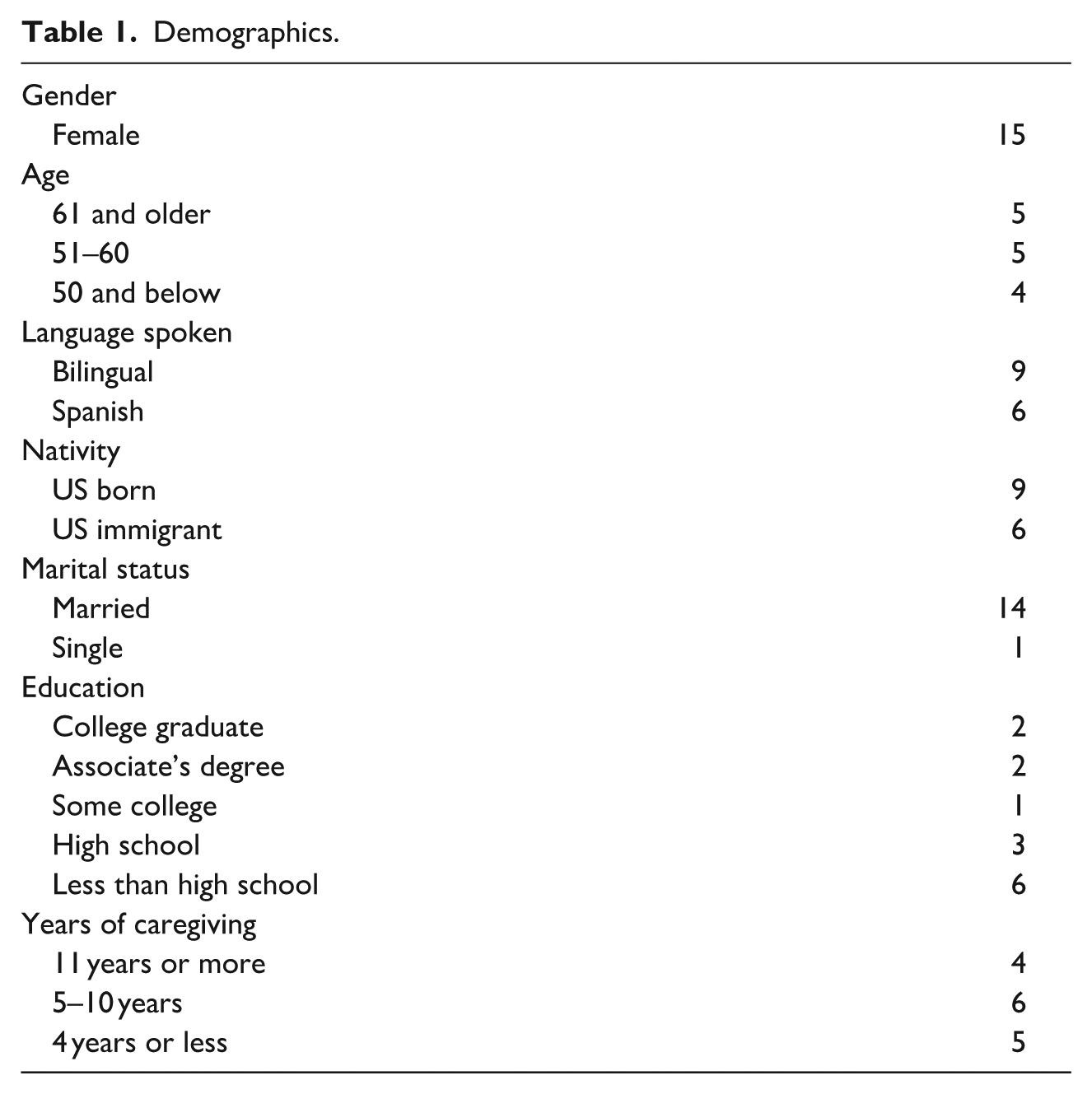
The sampling began as purposive and because of the lockdown, snowball sampling was also employed as some participants recommended other participants to the study. Some participants also shared the research study information from other promotoras that fit the study sample. Demographic information of the participants (Table 1) included the following: all caregivers were Mexican American females born in the United States who live in the Rio Grande Valley or Laredo areas whose ages ranged from 29 to 78 years old with a mean age of 53. The number of years being a caregiver for a family member ranged between 2 and 30 years. The marital status of the participants included 12 married and 3 single participants. The level of education for 13 of the participants was primarily receiving only an elementary education and 2 participants having a college degree (1 participant had an associate degree and the other had a bachelor’s degree.)
Demographics.
Measurement
A semi-structured interview guide was used with the participants. The initial questions dealt with the collection of basic demographic information from each participant. Once this information was obtained, the researcher(s) then proceeded to use open-ended questions regarding the experiences of being a caregiver. More specific questions included information about some of the stressors of becoming a caregiver and the experience of being a caregiver. Other questions dealt with coping with the challenges they had to overcome. Lastly there were questions about the involvement of the family and the influence of culture.
Once a participant contacted the researcher, the interview was scheduled at a time chosen by the participant. Interviews lasted 60 to 90 min and were conducted either on Zoom or via telephone interviews because of COVID precautions. All interviews were recorded with field notes as part of the researcher’s subjective documentation of participant-observation, and memo-writing to capture emergent patterns, categories and subcategories, themes, and concepts derived that could lead to a possible theory (Saldana, 2009). The primary author, who is bilingual and bicultural, conducted the interviews. Interviews were conducted in the language the participant preferred, English or Spanish or both. Interviews were audio recorded and transcribed in the language used in the interviews.
To analyze the data, the researchers used the Stress and Coping model as a framework. The Stress and Coping model begins with an event that is then appraised as harm, a threat, or a challenge. Coping is the next stage that involves problem-focused coping and emotion-focused coping. Coping leads to the event’s outcome, which can be viewed as favorable or unfavorable; this, in turn, leads to an “emotion” outcome. A favorable outcome leads to positive emotion. An unfavorable outcome leads to distress that leads back to another event and a new cycle of the model. In the revised Stress and Coping Model, Folkman (1997) added “meaning making coping” from distress that can lead to positive emotion which helps sustain coping and restore resources (Folkman, 1997; Lazarus & Folkman, 1984).
Analysis began during data collection. Because of the qualitative nature of the study, the analysis was inductive. Three researchers who participated in the analysis process have a PhD and the fourth researcher holds a DSW degree. All researchers have several years in the field as social workers practicing in the mental health arena. Adjustments to the survey protocol were not needed. Ethnographic content analysis was used to analyze the transcripts. Ethnographic content analysis centers on concept development, data collection, and emergent data analysis through repeated study of the content or text. Ethnographic content analysis follows a recursive and reflexive movement between data collection, coding data, and analysis and interpretation of the data (D. Altheide et al., 2008; D. L. Altheide, 1996; Altheide & Schneider, 2013; Stark & Roberts, 2005). Atlas.ti, a qualitative software data analysis, was used with the analysis. Data quality was through interrater reliability of multiple coders. Each author reviewed the transcriptions and recordings multiple times, coding common as well as unique themes separately, and then the authors compared and reached consensus about the emergent themes within and across the interviews. Coding and discrepancies were reconciled through these discussions. A description and interpretation of the themes, and quotations that reflected the themes are presented in the findings section.
Researchers employed several strategies to mitigate bias throughout data collection, and analysis processes. To enhance trustworthiness or rigor in this study, the researchers employed peer debriefing and an audit trail. The researchers met bi-weekly for peer debriefing sessions to serve as a check on the study. These sessions were a chance for feedback on interpretations and an opportunity to explore new ideas for data analysis (Creswell & Poth, 2024; Padgett, 2016). Debriefing sessions provided fresh eyes and a fresh perspective for the analysis. These sessions helped determine when the researcher’s reached saturation. The audit trail consisted of steps taken in data collection and data analysis, as well as interview transcripts, field notes, notes from peer debriefing sessions, and coding and analysis (Creswell & Poth, 2024). The audit trail helped the researchers look back at the steps in this process and review directions that might need consideration in analysis.
Subjectivity Statements
We understand that the interpretation of the data is a construct from our identities and lived experiences. The first two authors are bilingual male and female Latinos with practice and research experience in Latino mental health. Both are clinical social workers, primarily servicing Latinos. The third and four authors are bilingual male and female Latinos, with practice and research experience in Latino mental health. Both are LMSWs. The researcher’s experiences inform their approach to Latino dementia caregiving.
Findings/Results
The larger event for participants was accepting that their loved one has Alzheimer’s and becoming a caregiver. This was followed by the event of being a caregiver. These events are challenges according to the Stress and Coping Model. The primary appraisal of these events, stressors and challenges, was personally significant because it was a family member. The secondary appraisal was to learn how to cope with challenges that came with negative emotions like anxiety and fear. Caregivers had to adjust their lives to the needs of their loved ones. Caregiving was a family responsibility. This adjustment was meaningful to the participants, even though the event was stressful. Participants found meaning in coping with this particular event. The stressful event turned out to be meaningful as the caregivers coped with this experience each day.
Two overarching themes identified were adjusting to caregiving and the impact on the caregiver’s life. Adjusting to caregiving included the themes learning about Alzheimer’s Disease and coping with challenging behaviors. The impact on the caregiver’s life included the themes of geographical changes, family sacrifices, and simultaneous caregiving. Additionally, the lack of support and commitment from family members was another theme. Finding ways to cope with these stressors and challenges became a meaningful responsibility.
The participants experienced various stressors and challenges that required problem-focused coping and emotion-focused coping strategies. Through the care of their loved one came a sense of accomplishment and love for their family member making caregiving more meaningful. These emotions helped the participants through the stress of caregiving. Even though the experience was challenging and stressful, caregiving had a meaning. This responsibility and its meaning helped fuel the participants through the process of caregiving.
Adjustments by the Caregiver
Within the overarching theme, there were several themes identified. The themes included accepting a family members Alzheimer’s diagnosis, learning to be a caregiver, and being a caregiver. Coping with the stress of becoming a caregiver and the disease of Alzheimer’s was a challenge to participants. Participants discussed the difficulty of seeing their loved one’s cognitive health deteriorate. Adjusting to becoming a caregiver and the disease of Alzheimer’s was a challenge to several participants. Many participants discussed the difficulty of seeing their loved one’s cognitive health deteriorate and accepting that something was wrong. “I had a denial problem . . . I didn’t want to see her like that. I kept saying she’s going to be well; she’s going to snap out of this you know.” For some family members, it was difficult to admit their loved one had Alzheimer’s. As a means of coping, the participants dedicated themselves fully to care with the underlying belief that their efforts would lead to an improvement in their loved one’s condition. Non-acceptance or denial seemed to serve as a coping mechanism when dealing with the decline of their loved one; this helped them by remaining hopeful that their loved one’s health could improve. For some family members, it was difficult to admit to themselves that their loved one was experiencing cognitive decline. One participant shared what she still wanted to see from her mother, “I wanted to get her out of the diapers; I wanted to get her walking again; I wanted to get her to at least being mobile.” Participants had to learn how to accept their loved one’s diagnosis; acceptance was their way of coping with the distress from caregiving to continue helping their family members. Another event that was a challenge was the change in the caregiver’s life. The caregiving experience changed participants’ lives including daily activities and routines. The added caregiving experience required a lot of patience and added more responsibility when caring for a patient with Alzheimer’s Disease, especially as the disease progressed. “Tuve que tratar de acomodar mi vida; que voy hacer.” (I had to figure out how to adjust my life and what I was going to do). She tried different ways to figure out how to make it work. Coping with caregiving was challenging and stressful emotionally. Participants shared how they developed coping skills through the process and found meaning in their caregiving. Participants learned how they needed to cope by practicing patience. Because they were taking care of a loved one, participants lost focus on the stressful and challenging part of the disease and focused on coping with the caregiving. They turned the challenge into a meaningful event, or something that they wanted to do because it was a family member. Participants agreed caregiving was a learning experience, “vas aprendiendo poco a poco y con mucha paciencia.” (You are learning a little bit at a time and with a lot of patience).Participants agreed that accepting a family member’s behavior was challenging and distressing. The loved one’s behaviors required that participants learn to understand the physiological changes their loved one was going through and to cope with these behaviors emotionally and cognitively in a manner that made the challenge less distressing. Understanding this and applying coping strategies learned helped create meaning of their loved one’s behavior changes.
Behaviors included the patient hallucinating and being aggressive at times. One participant stated, “decía que veía cosas y veía bultos o personas.” (At times, my loved one would say they were seeing things – shapes or people.) Another challenging behavior was being accused of taking things, which is not uncommon in dementia caregiving. Caregivers had to learn to be aware of these behaviors and not personalize them. Participants needed to learn that these behaviors were characteristic of the disease, not the actions of their loved ones and avoid internalizing these behaviors as a means of making caregiving challenging or distressing.
Impact on the Caregiver’s Life
The overarching theme regarding the impact on the caregiver’s life included the geographical changes, stress on familial relationships, loss or change of employment, and balancing work and caregiving schedules. Participants dealt with the impact on their life as they became caregivers in several ways. They learned what was needed to help provide care. They adapted as needed to manage the challenges that resulted from geographical changes, an impact on familial relationships, and managing their work and caregiving schedules. At times life completely changed for families, and they had to make sacrifices. Some respondents were impacted geographically because they had to travel, move closer, or move in with their loved one. Participants described having to travel from one state to another to provide caregiving, and when this became unmanageable, they had to either move in with the loved one or have the loved one move in with them. In either case, it presented challenges. Coping with the challenge of caregiving became a meaningful choice. One respondent had to choose between taking care of her mom and taking care of her family and children. Participants explained how they handled these demands. In some cases, the children became a part of the process, thus adding meaning to the responsibility of caregiving. Now the coping skill had meaning for the entire family. The family made sacrifices for their caregiving parent.
For one participant, caregiving was so meaningful that she lived next door to her mother and would care for her when she arrived home from work until the next day when she went to work. This kind of schedule was her way of coping, and with the assistance of her loved one’s provider, this schedule created a less distressing caregiving responsibility.
The impact of caregiving was exacerbated when individuals had to simultaneously provide caregiving. This concept of coping expanded to include the need to support multiple individuals. For some caregivers, the challenge extended beyond simply providing care; it also involved managing the needs of several family members. This simultaneous caregiving presented significant difficulties for many caregivers.
Participants also reported the added challenge of caring for more than one individual such a special needs child, more than one parent, or a parent and spouse. “It’s very difficult to handle two people at the same time.” Some caregivers described the experience, “Emotionally it’s been very challenging.”
One participant discussed taking care of her mother until her death and now she is taking care of her father. Participants focused on multiple distress and used all their resources including family and social networks to provide care for all family members.
Lack of Family Support
Lack of support was a challenge reported by participants. This stress became another event in caregiving responsibility. Understanding the challenges that arise from a lack of support allows participants to gain valuable insights. This understanding can transform an unfavorable outcome into an opportunity for growth, enabling them to continue in the caregiving process. Some participants were single or not married. These participants did not have any other support, so the caregiving responsibility fell entirely on them. Caregivers that lacked support reported, “I feel very alone because I don’t have family.” They frequently feel like they are on their own. Participants learned to transform the stressor of having no support into a positive emotion by finding additional resources to cope with their caregiving responsibilities.
For many, their family members were not supportive in the caregiving of their loved one. Her family was not supporting her at all with any caregiving duties; she stated that she felt her siblings were, “lost in combat.” Participants and their families gained meaning through the process of dealing with the event, which included both the challenge of their loved one’s health deteriorating due to Alzheimer’s and becoming a caregiver. These challenges affected not only the caregiver, but their family as well. As is the case in many Latino Families, the family member was an older adult that was still considered the center of the family. The coping responses to these challenges were based on caring and love for the family member. The family responded by helping the primary caregiver through their caregiving responsibilities, and the family took on the meaningful responsibility of caregiving for their family member who was providing the caregiving. The burden of caregiving changed from stress to a meaningful responsibility.
Discussion
According to the results from the study, there are several challenges in the role of Latino caregivers that come with providing care for a loved one with Alzheimer’s Disease that led to caregiver burden. Despite the stress and challenges of caregiving, participants were able to give meaning to their experience – a meaning that was grounded in familismo. The caregiver’s psychological and behavioral responses to caregiving assisted in the development of meaningful coping skills and helped them adjust to their personal lives needed to lessen the stress and burden of caregiving.
For most caregivers, caring for a loved one with Alzheimer’s Disease is a new and unfamiliar experience; thus, some of the situations encountered can require significant adjustment. Caring for a loved one with Alzheimer’s Disease can vary greatly, and caregivers often find themselves having to make many adjustments to their approach or lifestyle (Hawken et al., 2018; Perry & Thiels, 2016). Depending on the severity of the dementia and resulting behaviors, the caregiver may be required to assist by driving their loved one to a medical appointment, or they may be required to assist with all activities of daily living, including toileting, bathing, and feeding. Often, caregivers are learning about the disease as they are providing care and new behaviors emerge. Some of these behaviors can be disconcerting to caregivers because their loved ones are suddenly aggressive, hostile, and accusatory (Alzheimer’s Association, 2024) or perhaps even experiencing delusional beliefs or hallucinations (National Institute on Aging, n.d.). The caregiver must quickly learn not to personalize accusations or anger, but rather, recognize that many of the behaviors are related to the disease.
For some caregivers, life is impacted by the need to travel or even move to another place because there is no way to determine how long the caregiving will be required. Since Alzheimer’s Disease progresses as time goes by, caregivers recognize that the level of care will also continue to increase; thus, proximity to the loved one becomes essential. If the distance between the caregiver and their loved one’s home is significant, moving in will sometimes be the best option. This, in turn, can also have an impact on the caregiver’s own family because it can mean leaving a spouse and/or children behind.
In some cases, as discussed by the participants of this study, caregivers must provide care to multiple people, such as a parent or older relative as well as an adult child with special needs. This is referred to as “compound caregiving,” and while it may not increase depressive symptomatology or increased mental health issues, the main problems reported by caregivers were limited personal time and a lack of support from others (Perkins & Haley, 2010). Han’s (2023) study provides strong counterevidence to the notion that the act of caregiving worsens mental health, but the findings by no means nullify the fact that caregivers often face tremendous burdens and psychological distress, which can undermine mental health. According to the Mayo Clinic (2023), it is important for caregivers of multiple family members to recognize that they need help, be willing to ask for it, and then accept it. Because compound caregiving generally includes older adults and other family members it is likely that the care has been ongoing for a very long time. In one study, Lee et al. (2020) learned that approximately 25% of caregivers were caring for more than one loved one. It generally included parents, grandparents, individuals with developmental delays and sometimes children or grandchildren. For some caregivers, it was siblings who were providing the care for family members who had already served as caregivers for many years.
Another challenge identified was the lack of support caregivers received from others. This was similar to findings by Gelman (2014) and Mendez-Luck et al. (2020). In some cases, they identified siblings who were unwilling to help with the caregiving needs of their parents, and in other situations, it was a lack of support from the caregiver’s immediate family such as the spouse or children. Caregivers identified feelings of isolation and abandonment. This is particularly concerning because research has shown the isolation and stress which results from caregiving can lead to bouts of depression, anxiety, and/or other mental illnesses (Broxson & Feliciano, 2020; Cleveland Clinic, n.d.; Lou et al., 2015).
Mexican American caregiver’s access to resources may largely depend on their understanding of the family and community resources available to effectively provide caregiving. For example, having family or community support can provide the caregiver with additional information, resources, and/or respite options. Conversely, a lack of support, low socioeconomic status, limited education, and language barriers can make it difficult for caregivers to identify and access resources. Additionally, it is important to note the interviews were conducted during the peak of the COVID pandemic, so the access to resources could have been affected.
Limitations to the Study
This study was limited to the experiences of Mexican American women serving in the role as caregivers. While one of the purposes was to help fill a gap in the literature regarding this specific population given that the Hispanic population is expected to continue growing, the homogeneity of the participant group presents limitations regarding the generalizability of findings. Specifically, all 15 participants were Mexican American females, which limits the direct applicability of these findings to the experiences of male caregivers or those of other ethnic groups. Another factor which limits the generalizability is the fact that all but two individuals reported an elementary level education; two of the caregivers reported a college education. While this was not addressed or explored in this study, the authors recognized it is information that should be examined in future studies. Caregiving roles and perceived stressors may differ significantly across genders, influenced by societal expectations and cultural norms that were not explored within this exclusive female sample. Moreover, the educational background of all participants was predominately at the elementary level, with only two having a college degree may influence how caregivers access information, navigate healthcare systems, and perceive challenges. Consequently, the findings may not fully capture the experiences of caregivers with different educational backgrounds, potentially impacting generalizability of the results to those with higher education levels who may have different resources or coping mechanisms. Because of these limitations on the specific population studied, some of the findings may not be transferable to caregivers from other racial or ethnic groups, or to broader caregiving populations with diverse characteristics. Future research is needed to explore caregiving experiences across a broader spectrum of genders, educational backgrounds, and cultural contexts to provide a better understanding of Alzheimer’s caregiving.
Implications for Practice
Caregiving for Alzheimer’s patients presents unique challenges that have significant implications for practice. Jaldin et al.’s (2023) qualitative study explored the role of Latino cultural values in caregiving experiences. Within the study four cultural values were identified as meaningful to participants, familismo, fatalismo, marianismo, and machismo. For this study, the researchers focused on the value of familismo. It is noteworthy that future research will need to include how the other three values of fatalismo, marianismo, and machismo influence caregiving with Latinos.
To address the cultural preference for informal, family-based care and the reluctance to use formal services, it is important for individuals who assume the role of a caregiver be provided education to acquire specialized knowledge of dementia-related behaviors, psychological symptoms, and the impact of caregiving on the family. These behaviors often require special skills for families to communicate the needs of their loved ones with health providers. Additionally, caregivers need stress management skills due to the overwhelming results of caring for a patient with Alzheimer’s Disease or a related dementia. Caregivers need to have continuous training emphasizing person centered care, which is critical to help maintain the dignity and autonomy of their loved one with Alzheimer’s Disease.
As their family members decline and caregiving becomes more difficult, support services for caregivers are essential due to the emotional and physical toll from long-term caregiving, and potential burnout. Therefore, integrating support for caregivers who provide care to family members will result in sustaining meaningful caregiving. A last consideration is incorporating the cultural values of familismo, fatalismo, marianismo, and machismo in the creation of programs and services that benefit the care receiver and the health of Latino caregivers and their families.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.