
Abstract
Latinos have seen a 30% increase in autism spectrum disorder (ASD) since 2018. However, Latino children are diagnosed later and remain underdiagnosed compared to Whites. Later diagnosis of autism or failure to receive a diagnosis of autism into adulthood is associated with negative outcomes. From 2012 to 2022, in specialty clinic diagnosing autism in adulthood, Latino adults (n = 31) were older than White adults (n = 323) and, using 2020 Census data, severely underrepresented despite experiencing similar distress and symptoms of autism to White adults. Latino adults with a first-time diagnosis of autism were also nearly 2.5 years older than White adults. Recommendations are provided to service providers to improve access to services for Latinos. Recommendations provided include making changes at an organizational level to improve access to high quality healthcare services for Latinos. Other recommendations include translating services for Spanish-speaking Latinos and advertising these services. Finally, service providers should culturally adapt services to ensure they are appropriate for Latinos.
Autism spectrum disorder (ASD) 1 is a neurodevelopmental disorder marked by impairments in social communication and the presence of restricted and repetitive behaviors and interests (American Psychiatric Association [APA], 2022). Currently, it is estimated that 2.26% of U.S. adults are diagnosed with autism (Dietz et al., 2020). Most individuals diagnosed with autism experience difficulties in social communication and co-occurring issues in executive function (Haigh et al., 2018; Johnston et al., 2019). Compared to individuals without autism, adults with autism experience significant difficulties associated with co-occurring mental health conditions (Lake et al., 2014; Mazzone et al., 2012), poorer health-related quality of life (Kamp-Becker et al., 2010), and significantly more premature deaths by suicide compared to the general population (Hedley & Uljarević, 2018). However, for a variety of reasons, a subset remains undiagnosed into adulthood.
Experts estimate that for every three diagnosed cases of autism, there are two additional undiagnosed cases (Lewis, 2018). One possibility is that adults with undiagnosed autism may achieve optimal functional outcomes (i.e., academic achievements, living, relational, or educational; Lehnhardt et al., 2011). However, a missed diagnosis of autism may result in adults receiving treatment for mental health conditions that do not fully capture their clinical picture (Crucitti et al., 2018; Jadav & Bal, 2022; Lehnhardt et al., 2011; Pehlivanidis et al., 2020; Russell et al., 2016) and social isolation (Lewis, 2016). Undiagnosed adults with autism have been found to fear that professionals may not take their symptoms of autism seriously (Lewis, 2017). Thus, researchers have begun to examine individuals diagnosed with autism in adulthood (Lewis, 2016, 2017, 2018). Those who seek a diagnosis of ASD in adulthood typically do so seeking to better understand themselves (de Broize et al., 2022). However, little is known regarding marginalized populations diagnosed with ASD in adulthood.
Latinos are the fastest growing ethnic marginalized group in the United States (Pew Research Center, 2017). Nearly eight million (18.4%) Latino adults reported having a mental illness in 2020 (National Survey on Drug Use and Health [NSDUH], 2020) and Latinos experienced a significant increase (30%) in children diagnosed autism between 2018 and 2020 (Maenner et al., 2023). However, studies show that Latinos receive mental health services at half the rate of non-Latino Whites (White; Office of Mental Health, 2019; Substance Abuse and Mental Health Services Administration, 2018) and Latinos with autism are often under-identified, underserved, and diagnosed at a later age than their White peers (Mercadante et al., 2009; Travers & Krezmien, 2018; Valicenti-McDermott et al., 2012). Disparities in access to equitable care (e.g., un- or under-insured, language and cultural barriers, lack of proximity to services; Arredondo et al., 2014) is particularly relevant given the ongoing downstream inequities in health, education, and income Latino adults with intellectual and developmental disabilities experience (Magaña et al., 2016).
Several factors may explain these concerning trends. For example, studies show that Latinos have restricted access to mental health professionals from their communities (Alarcón, 2001; APA, 2017). Latinos also experience significant disparities in autism-specific services (e.g., more obstacles to services, decreased access to autism-specific knowledge, interventions, and support; Bernier et al., 2010; Bishop-Fitzpatrick & Kind, 2017; Dudley et al., 2019; Ratto et al., 2016). Angell et al. (2018) also note that disparities in access to services are caused by a lack of bilingual service providers. Even when Latinos do receive care, they receive inferior care (Shepherd et al., 2018). Thus, Latinos experience obstacles in receiving the specific care they need.
Cultural factors may also explain disparities in services for Latinos (Alegría et al., 2007; Zuckerman et al., 2014). For example, Alegría et al. (2007) found that language barriers, age at migration, years of residence in the United States, generational status, fear of exposing immigration status, and few services that take into account cultural differences were some of the reasons for these disparities. Zuckerman et al. (2013) provided more information on the cultural factors related to service disparities, adding that Latino parents may accept the behavior of their children with autism as normal due to several factors, including providers dismissing parents’ concerns about their children. Thus, not only do not only do Latino families lack resources but they may never seek out services, thereby increasing the probability of Latinos with autism reaching adulthood undiagnosed.
Further exacerbating these disparities are the findings that Latino children are more likely to receive an alternative diagnosis to autism, such as specific language impairment (Mandell et al., 2007, 2009). Latino children are also diagnosed almost 1 year later than White children, receive fewer specialty services, and have higher unmet service needs (Liptak et al., 2008; Magaña et al., 2012, 2013; Parish et al., 2012; Ratto et al., 2016). Factors that contribute to differences in the number of services received are maternal level of education and the number of sources of knowledge about autism (Magaña et al., 2013). Socioeconomic status (SES) has also been shown to account for delays between the time mothers report concerns and the time of autism diagnosis (Ratto et al., 2016).
In sum, given these concerning trends in the missed diagnosis of autism in Latino children, many Latinos are likely reaching adulthood with a missed diagnosis of autism. While many studies have investigated the first-time diagnosis of autism in Latino children (Alegría et al., 2007; Angell et al., 2018; Zuckerman et al., 2014), little is known regarding Latino adults presenting for a first-time diagnosis of autism. Best practice guidelines for psychological evaluations include the collection of information on the client’s developmental and social history, as well as self- and informant-rated measures on the client’s social skills, and emotional and behavioral functioning (Perry et al., 2002; Pilling et al., 2012). The assessment used to aid in the diagnosis of autism in adulthood is the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; Lord et al., 2012), which has shown to have adequate psychometric properties in predicting autism in adults and is as a well-researched, valid and reliable instrument for diagnosing autism in general and for diagnosing autism in cognitively able adults (Bastiaansen et al., 2011; Langmann et al., 2017). Self-report measures of autism typically utilized include the Social Responsiveness Scale, 2nd Edition (SRS-2; Constantino & Gruber, 2012) and others (Baron-Cohen & Wheelwright, 2004; Baron-Cohen et al., 2001; Nylander & Gillberg, 2001; Ritvo et al., 2011). However, no studies to date have examined these measures in Latino adults with a first-time diagnosis of autism.
In the present study, the characteristics and symptoms of autism in Latino adults and White adults with a first-time diagnosis of autism were compared. Both groups were made up of adults and thus represent a specific subset of adults with autism who were undiagnosed as children. The present study sought to examine whether Latino adults are diagnosed at later ages than White adults and experience similar distress and symptoms of autism as White adults. The present study sought to answer this question by examining demographic characteristics, autism measures, and distress/dysfunction in Latino and White adults with a first-time diagnosis of autism. Finally, in an exploratory step, Latino population rates were compared to Latinos in the present study, using 2020 Census data to evaluate whether Latinos are underserved in receiving critical autism assessment services.
Method
Participants
The current sample comes from a clinical sample from an outpatient clinic specializing in the diagnosis of autism in adults in the South-Central United States of adults presenting for an evaluation for autism from 2012 to 2022. The clinic is housed in a psychiatry and behavioral sciences department in a large medical center. The center is housed in a large metropolitan area with nearly 45% of the surrounding area identifying as Hispanic/Latino. Patients can be seen utilizing private or public health insurance but were limited to English-speaking Latinos due to the lack of bilingual staff at the clinic. The typical evaluation in this clinic lasts approximately 1.5 hr and includes specific diagnostic measures discussed below, as well as self- and informant-report measures. Measures include assessment of psychological functioning, adaptive functioning, and executive functioning. Patients are typically self-referred to the clinic and speak English. Thus, the current sample includes English-speaking Latinos.
The study received IRB approval and participants provided informed consent. The sample includes a total of 31 self-identified Latino adults (41.9% female) ranging from 20 to 55 years of age (M = 30.94, SD = 9.35) compared to 323 White adults (32.8% female). Demographic information was collected via record review and semi-structured interviews with participants (see Table 1 for full demographic information). Participants were mostly employed full-time (48.4%), college graduates (38.7%), never married (41.9%), and living independently (61.3%). All participants were evaluated for autism using an autism-specific diagnostic instrument, the Autism Diagnostic Observation Schedule (ADOS-WPS; Lord et al., 2000) or the Autism Diagnostic Observation Schedule-2nd Edition (ADOS-2; Lord et al., 2012). To aid in the diagnosis and provide tailored recommendations, self- and informant-report questionnaires were collected, including the Social Responsiveness Scale, 2nd Edition (SRS-2; Constantino & Gruber, 2012), Autism Spectrum Quotient (AQ; Baron-Cohen et al., 2001), Empathy Quotient (EQ; Baron-Cohen & Wheelwright, 2004), and the Ritvo Autism Asperger Diagnostic Scale-Revised (RAADS-R; Ritvo et al., 2011).
Demographic Characteristics of Adult ASD Cases.
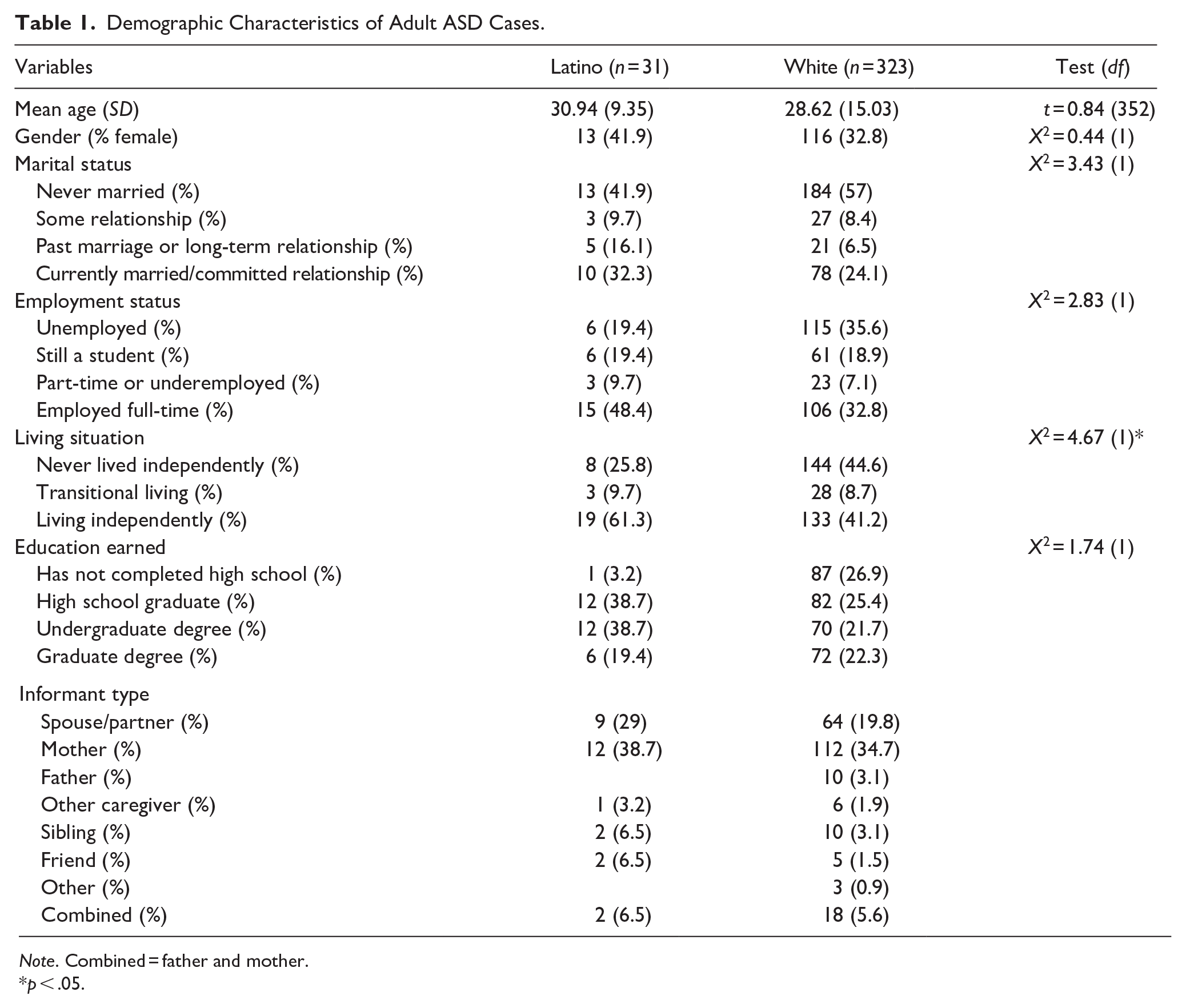
Note. Combined = father and mother.
p < .05.
Measures
The Social Responsiveness Scale, 2nd Edition (SRS-2; Constantino & Gruber, 2012) is a 65-item adult self- and informant-report questionnaire that assess traits associated with autism on a 4-point scale from 0 (“Not True”) to 3 (“Almost Always True”). Scores on the SRS-2 are reported as t-scores (M = 50, SD = 10) with scores of 60 or higher indicating mild (or greater) social difficulties related to autism (Constantino & Gruber, 2012). The SRS-2 provides subdomain scores in the areas of social awareness, social information processing, capacity for reciprocal social communication, social anxiety/avoidance, and preoccupations and traits related to autism. The original SRS data found strong 3- to 6-month test-retest reliability (r = .88–.95; Bruni, 2014). Across various samples, the SRS-2 has also demonstrated strong internal consistency (α = .94–.96; Bruni, 2014).
The Autism Spectrum Quotient (AQ; Baron-Cohen et al., 2001) is a 50-item questionnaire for adults with five subscales associated with autism spectrum disorder (i.e., social skill, attention switching, attention to detail, communication, and imagination). Each question is answered using a 4-point Likert scale that ranges from 0 (“Definitely Agree”) to 3 (“Definitely Disagree”) and then summed to create a total score. In order to avoid response bias, approximately half of the items are worded to produce a “disagree” response, and half an “agree” response. Baron-Cohen et al. (2001) found 80% of adults with autism spectrum disorder scored above a critical minimum of 32, whereas only 2% of control adults received that score. Baron-Cohen et al. (2001) found good 2-week test-retest reliability (r = .70) and moderate to high internal consistency across subscales (Communication = .65; Social = .77; Imagination = .65; Local Details = .63; Attention Switching = .67).
The Empathy Quotient (EQ; Baron-Cohen & Wheelwright, 2004) is a questionnaire for adults with 60 items, with 20 of the 60 items serving as “filler” items that do not contribute to the total sum score of 80. Answers are provided on a 4-point scale ranging from 0 (“Strongly Agree”) to 3 (“Strongly Disagree”) with approximately half of the items being reverse scored. Baron-Cohen and Wheelwright (2004) found 81% of adults with autism spectrum scored equal to or less than 30 points compared to 12% of control adults. The EQ demonstrates strong test-retest reliability (r = .97) and moderate internal consistency (Sreehari et al., 2016).
The Ritvo Autism Asperger Diagnostic Scale-Revised (RAADS-R; Ritvo et al., 2011) is an 80-item self- and informant-report questionnaire for individuals over the age of 16 years old. The RAADS-R consists of four subscales (i.e., social relatedness, circumscribed interests, language, and sensory motor) associated with autism spectrum disorder. Responses are scored on a 4-point scale with the following response options: “True now and when I was young,” “True only now,” “True only when I was younger than 16,” and “Never true.” Sixty-four questions describe symptoms of autism and 16 questions describe normative behaviors. Scores are summed to produce a total score with higher scores indicating more symptoms of autism. The cutoff score associated with a clinical diagnosis of autism is 65. Ritvo et al. (2011) found strong concurrent validity with the SRS-2 (95.59%), strong sensitivity (97%) and specificity (100%; with a score of 65), strong test–retest reliability (r = .99), and moderate to strong internal consistency across subscales (circumscribed interests = .90, language = .79, sensory motor = .91, social relatedness = .92).
The Adult Self Report (ASR; Achenbach & Rescorla, 2003) is a self-report measure that contains 123 problem items which can be combined to create several distress scales (e.g., depression, anxiety, ADHD symptoms). Items are rated over the last 6 months from 0 (“not true”) to 2 (“very true”). The ASR was utilized to identify underlying concerns regarding internalizing and externalizing issues as part of the standardized battery of the intake evaluation. The ASR is standardized against a community-based sample with t-scores (M = 50, SD = 10). The Spouse and Tobacco/Alcohol/Drug Use subscales were omitted given many adults did not endorse them.
Procedure
As part of the comprehensive psychological evaluation at an outpatient clinic specializing in the assessment and treatment of autism across the lifespan, participants and their informants completed measures assessing personality traits, emotional and behavioral functioning, executive functioning, and traits related to autism. The current variables of interest were autism measures and demographic characteristics associated with the participant’s current level of functioning. All data were de-identified prior to data analysis. Participants were asked at the time of the assessment whether de-identified data from their assessment could be used for research purposes. All participants in this sample gave written informed consent for data to be used for research purposes. The evaluations occurred from 2012 to 2022. For samples collected prior to 2013, when the DSM-IV-TR (4th ed., text rev.; APA, 2000) and the original version of the ADOS (ADOS-WPS; Lord et al., 2000) were being used, only cases that conformed to the autism diagnostic criteria of the DSM-5-TR (5th ed., text rev.; APA, 2022) and ADOS-2 (Lord et al., 2012) were included. Participants included in the autism sample also met criteria per the International Statistical Classification of Diseases and Related Health Problems (ICD) 10th edition (ICD-10; World Health Organization, 1992) and 11th edition (ICD-11; World Health Organization, 2019). Exclusion criteria included: (a) cases of individuals under the age of 18 years old, or (b) individuals with suspected or confirmed intellectual disability. Because some adults did not have a parent available to aid in the diagnosis of autism and the presence of symptoms in childhood, those with an intellectual disability were excluded. Inclusion criteria included: (a) a current diagnosis of autism, (b) being able to read and write in English, or (c) cases of individuals at or above 18 years of age.
Data Analysis
Data were analyzed for the presence of outliers and normality to confirm whether the assumptions for parametric testing were fulfilled. No violations of the assumptions of normality, linearity, multicollinearity, and homoscedasticity were observed. Outliers were examined but none were identified in the data set. Additionally, no distribution demonstrated abnormal levels of skew or kurtosis with the exception of age. Data were analyzed utilizing Version 28 of SPSS (IBM Corp, 2021). Descriptives and frequencies of variables of interest included outcome measures (i.e., SRS-2, AQ, EQ, RAADS-R, and the ASR) and demographic variables (i.e., sex, education, relationship status, employment status, and living situation). Using 2020 US census data from Houston, Texas (U.S. Census Bureau, n.d.), a chi square goodness of fit as calculated based on expected population values.
Results
Demographic characteristics were compared between Latinos in the present sample to the White sample across a 10-year period. For the purposes of the chi square analyses, a participant’s living situation was categorized as independent living (i.e., living alone or with a partner) or supported living (i.e., never lived independently or in transitional living), employment status was categorized as either employed (i.e., full- or part-time) or unemployed (i.e., still a student or unemployed), and marital status was categorized as currently married/committed relationship or not currently married/committed relationships (i.e., never married, some relationship, past marriage, or long-term relationship). Overall, participants looked similar across many categories, including marital status, employment status, and education earned. However, some key differences were observed in other demographic characteristics. For example, Latino individuals with a first-time diagnosis of autism in adulthood were nearly 2.5 years older than the White in the present sample (t = 0.84, p = n.s.). Furthermore, a larger proportion of the Latino sample was female (X2 = 0.44, p = n.s.). Significantly more Latinos in the present sample were also living independently when compared to the White sample (X2 = 4.67, p < .05). Overall, over the same 10-year period, 323 White adults were diagnosed with autism in the present clinic and only 31 Latino adults were diagnosed with autism.
Independent samples t-tests were utilized in order to examine whether differences in autism measures and ASR scales were associated with ethnicity (see Table 2). No significant differences were noted across measures. Thus, Latino adults experienced a similar amount of distress and autism symptoms across measures compared to White adults. However, of note is that ADOS-2 total scores were higher on average for the Latino group when compared to the White group (t = 1.30, p = n.s.).
Measures of Distress and ASD Symptoms for Adult ASD Cases.

Note. ADOS-2 = Autism Diagnostic Observation Schedule, Second Edition; AQ = Autism Spectrum Quotient; EQ = Empathy Quotient; SRS-2 = Social Responsiveness Scale, 2nd Edition; RAADS-R = Ritvo Autism Asperger Diagnostic Scale-Revised; ASR = Adult Self-Report; ADHD = attention-deficit/hyperactivity disorder.
Finally, a Chi-Square Goodness of Fit Test was performed to determine whether the proportion of Latinos with a first-time diagnosis of autism matched the proportion of Latinos in the broader population of Houston, Texas. Using 2020 Census data (U.S. Census Bureau, n.d.), the present study found the proportions diagnosed with autism in adulthood significantly differed by ethnicity (X2 = 184.37, p < .0001; see Table 3). These results indicate a statistically significant discrepancy, suggesting that the proportion of Latinos diagnosed with autism in adulthood does not reflect the ethnic distribution within the broader population of Houston, Texas.
Chi Square Goodness of Fit Test Comparing First Time Diagnosis of ASD Among Latinos Versus Whites.
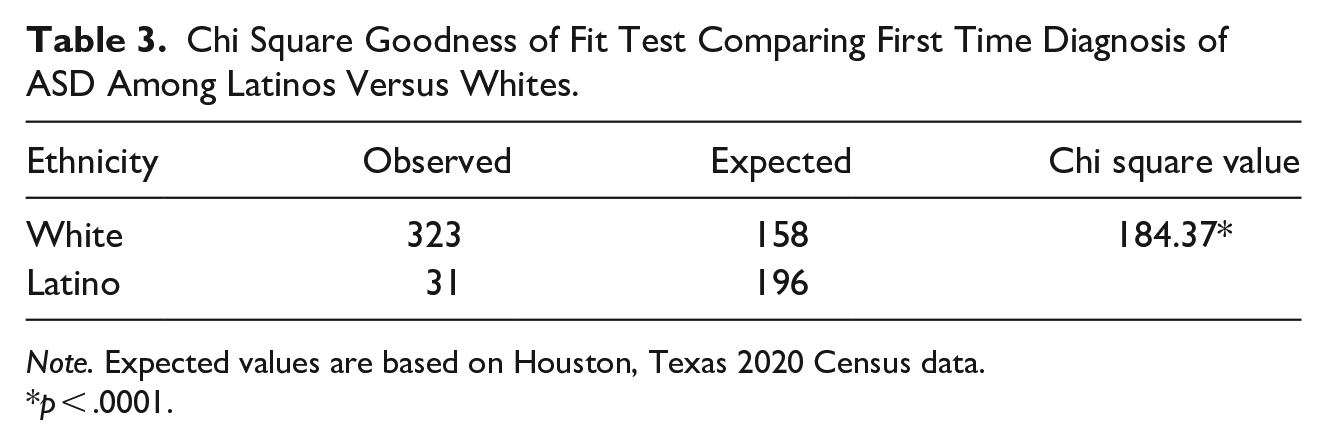
Note. Expected values are based on Houston, Texas 2020 Census data.
p < .0001.
Discussion
To our knowledge, this is the first study to date to specifically examine a sample of Latinos with a first-time diagnosis of autism in adulthood. Racial and ethnic marginalized children, including those who are Latino, experience delays in first time diagnosis of autism (Liptak et al., 2008; Magaña et al., 2012; Parish et al., 2012). The present study found that Latino adults are also diagnosed at later ages than White adults, which extended and replicated findings from past studies in children (Magaña et al., 2013; Ratto et al., 2016). Furthermore, a larger proportion of females with autism was observed in the Latino adults compared to the White adults. This contrasts with Zuckerman et al.’s (2017) findings that Latino females were diagnosed less frequently than White. A recent collective case study found a Latina female’s pathway to diagnosis may be inhibited by familial factors, tension surrounding autism knowledge, cultural stigma, and a female autism phenotype (Moreira & Angell, 2020). Other research in the general population has found that females may be under diagnosed in childhood due to differences in symptom manifestation (Kreiser & White, 2014), which could be a result of females’ higher self-reported “camouflaging” of autism symptoms (McQuaid et al., 2022). The present study was the first to examine differences in autism diagnosis in Latina females. As researchers seek to understand the unique reasons for this difference (Hull & Mandy, 2017; Kanfiszer et al., 2017), it is imperative that Latina females be identified in both community and clinical settings to provide effective and timely treatment and supports.
The present study also found that significantly more Latino adults with autism lived independently when compared to White adults with autism. This was a surprising finding given past studies have found culturally and linguistically diverse autistic individuals experience even higher rates of chronic unemployment (e.g., 66%) compared to the national average (Nord et al., 2016). This could be the result of the present sample consisting mostly of intellectually able adults with autism. Further, those who are employed are more likely to have access to private health insurance. In fact, one study found a higher percentage of Latino adults with autism were using public health insurance compared to non-Latino adults with autism (Ames et al., 2022). The present study also found that Latinos with a first-time diagnosis of autism did not significantly differ from White individuals with a first-time diagnosis of autism across measures symptoms of autism symptoms and distress. Findings like these are often referred to as the Hispanic paradox (Franzini et al., 2001), where Latinos may self-report better outcomes despite lower SES.
Most importantly, the present study found that, over a 10-year period (2012–2022), significantly fewer Latino adults were diagnosed with autism in a specialty clinic for autism than would be expected given nearly 45% of the surrounding population in Houston, Texas identifies as Latino. This is critical given the potential number of Latino adults with autism who remain undiagnosed, the effects of autism on co-occurring mental health conditions (Lake et al., 2014; Mazzone et al., 2012), and most importantly, the risk for suicide in adults with autism (Hedley & Uljarević, 2018). Several factors may explain this finding, including cultural and systemic problems. For example, studies show Latinos have restricted access to mental health professionals from their community (Alarcón, 2001; APA, 2017). Latinos also experience significant disparities in autism-specific services (e.g., more obstacles to services, decreased access to autism-specific knowledge, interventions, and support; Bernier et al., 2010; Bishop-Fitzpatrick & Kind, 2017; Dudley et al., 2019). In studies comparing White children with autism to Latino children with autism, Latino children received fewer specialty services and had higher unmet service needs. Factors that accounted for differences in the number of services received were maternal level of education and the number of sources of knowledge about autism (Magaña et al., 2013). Similarly, Ratto et al. (2016) found that SES can account for delays in reporting autism concerns.
Cultural factors may also explain disparities in services for Latinos (Alegría et al., 2007; Zuckerman et al., 2014). For example, Alegría et al. (2007) found a lack of information, language barriers, age at migration, years of residence in the United States, generational status, fear of exposing immigration status, and few services that take into account cultural differences were some of the reasons for these disparities. Zuckerman et al. (2013) provided more context, adding that Latino parents normalize the behavior of their children with autism (accept the behavior as “normal”) due to several factors, including providers dismissing parents’ concerns about their children. Thus, it is possible that Latino adults do not seek evaluations for symptoms of autism due to a combination of societal and cultural factors.
The present study should be examined in light of some limitations. First, the Latino sample was clinic-based and excluded autistic individuals but did not present for a formal evaluation. Furthermore, comparing the proportion of Latino patients seen in a specialty clinic for autism to census data could yield misleading results. There could be many reasons that the clinic did not see Latino adults in need of an autism diagnosis, and other clinics in the area may have captured them instead. However, we deem this as a low probability as there are no clinics advertising services for adults with autism in this city. Data should be interpreted with caution, as the present sample may not represent the community of all Houston Latino adults with autism. Furthermore, due to the small sample size gender differences were not evaluated, which further limits the generalizability of the findings. Many findings (e.g., age of diagnosis) were not significantly different between groups, which is another limitation of the present study. Second, participants who did not speak English could not be evaluated due to a combination of a lack of translated measures of autism and few Spanish speaking clinicians available. This is a significant limitation that must be addressed in the context of expanding culturally and linguistically appropriate services to this community discussed below and in Table 4. Finally, the present study grouped Latinos from various countries of origin together which may create a false picture of homogeneity despite the various cultural and linguistic differences among diverse groups of Latinos in the United States. Additionally, our sample consisted of English-speaking Latino individuals, which may not fully reflect the broader Hispanic population reported in Census data, as it includes both English- and Spanish-speaking individuals. This limits the generalizability of our findings to the entire Latino community, particularly those who primarily speak Spanish and may experience additional barriers to autism diagnosis and services.
Recommendations for Improving Access to ASD Services for Latino Adults.
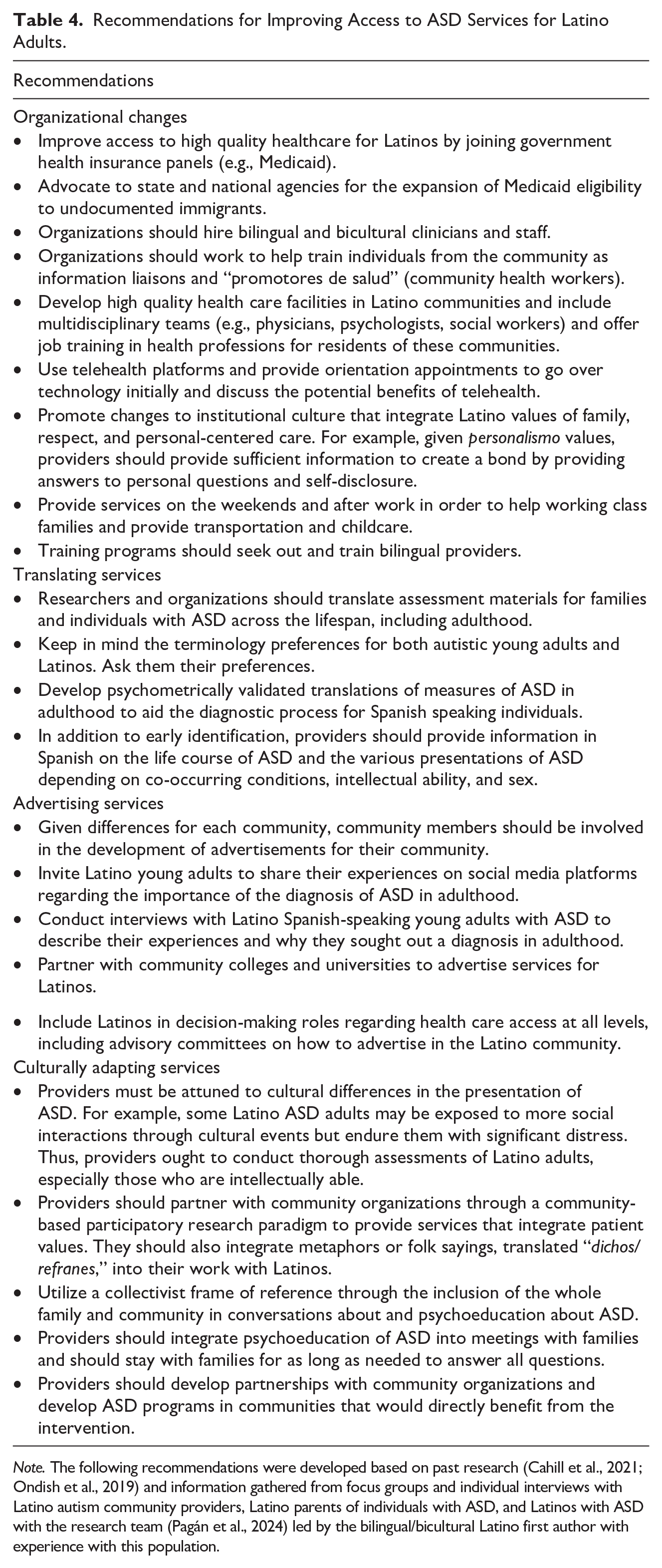
Note. The following recommendations were developed based on past research (Cahill et al., 2021; Ondish et al., 2019) and information gathered from focus groups and individual interviews with Latino autism community providers, Latino parents of individuals with ASD, and Latinos with ASD with the research team (Pagán et al., 2024) led by the bilingual/bicultural Latino first author with experience with this population.
Recommendations to Improve Access Gaps
Despite these limitations, the present study has provided further evidence that Latinos are not accessing vital autism services. Building off previous studies in children (Liptak et al., 2008; Magaña et al., 2012; Parish et al., 2012), the summative results are that, despite experiencing a similar amount of distress and symptoms of autism as White adults, Latino adults were diagnosed at older ages and at a much lower rate than would be expected based on their prevalence of Latinos in the surrounding population. Improving autism service gaps for Latinos requires bold ideas and consistent advocates. Everyone, from organizations to individual service providers have a duty to address these gaps and improve access to high quality evidence-based services for Latinos in the United States. Actionable steps that can be taken are provided (see Table 4) based on information gathered from focus groups and individual interviews with Latino community providers to autistic individuals, Latino parents of children with autism, and autistic Latinos (Pagán et al., 2024). For example, improving education and access to health insurance are important factors that may help Latino adults with autism receive diagnostic services through advertisements (Edward et al., 2018; Flink, 2018). Another important factor that continues to plague the adult autism field is the lack of psychometrically validated translations of measures of autism in adulthood to aid the diagnostic process for Spanish speaking individuals. Consequently, it is vital that researchers and clinicians continue to develop culturally adapted and translated measures for Latino adults seeking a first-time diagnosis of autism. A lack of proficiency in English also makes navigating the health care system more challenging. Individuals from disadvantaged backgrounds deserve equitable access to assessment and treatments, which includes medical facilities hiring bilingual and bicultural clinicians and staff. Services should be advertised specifically to the Latino autism community. Providers and researchers should use community-based participatory research in order to include Latino adults with autism in the research for their communities and as a way to understand the challenges they experience when navigating the health care system as adults and incorporate Latino values into the services provided (Cahill et al., 2021; Ondish et al., 2019; Wallerstein et al., 2017). These are important steps to be taken in order to reach underserved, autistic individuals such as Latinos who remain undiagnosed into adulthood.
Footnotes
Acknowledgements
We would like to thank all those who consented to participate in this study.
Author Contributions
AFP conceived of the original research idea for this study and provided final edits. All authors contributed to the design of the study, and reviewed and approved the article before submission. The article has been submitted solely to this journal and is not published, in press, or submitted elsewhere.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Pagan’s research is funded by an Autism Speaks Postdoctoral Fellowship Grant [#13904], the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health, through UTHealth-CCTS grant number [5TL1TR003169-05 and T32TR004904], and the Eunice Kennedy Shriver National Institute Of Child Health & Human Development of the National Institutes of Health under Award Number K99HD118079. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.