
Abstract
This study examines the impact of migration experiences—specifically undocumented status and informal sector participation—on the cognitive aging of Mexican return migrants. Using data from 6,277 participants in the 2018 Mexican Health and Aging Study (MHAS), we assess the likelihood of dementia among return migrants relative to non-migrants. The findings reveal that undocumented return migrants who later work in Mexico’s informal sector have significantly worse cognitive outcomes than both non-migrants—Mexican individuals whom never left Mexico—and undocumented return migrants working in the formal sector. Factors such as rural residency, lack of health insurance, and limited education further exacerbate cognitive decline in this population. Legal precarity, economic insecurity, and limited access to healthcare, accelerates cognitive aging for older return migrants, especially those in the informal sector. These results underscore the importance of formal sector participation, especially in contexts where healthcare access is tied to formal employment. The study adds to the growing body of research underscoring the long-term impact of migration on health and emphasizes the need for inclusive health and social policies to benefit aging vulnerable populations in both the United States and Mexico.
Introduction
About 11 million unauthorized immigrants live in the United States (Passel & Krogstad, 2024). A significant portion of this population is aging, facing unique challenges related to economic security and retirement (Ro et al., 2022). These challenges are often amplified among return migrants to Mexico, especially those who spent significant time in the United States. For these migrants, legal status plays a critical role in shaping access to healthcare, economic stability, and social services (Aguila & Angel, 2021; Carrasquillo et al., 2000). Legal precarity—the uncertainty stemming from undocumented or temporary immigration status—has been shown to negatively impact health and well-being (Hacker et al., 2015). Additionally, labor sector participation—whether in the formal or informal sectors—can influence long term health outcomes (Aguila & Angel, 2021).
Migration, Legal Precarity, and Health Outcomes
Mexican migration to the United States has historically been driven by significant economic and social disparities between the two countries (Aguila et al., 2023; Durand et al., 2001; Hanson, 2006; Massey et al., 2002). U.S. immigration laws have increasingly restricted immigrants’ access to public benefits. For example, the Illegal Immigration Reform and Immigrant Responsibility Act and the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) significantly reduced immigrants’ eligibility for healthcare and other resources (Rodriguez et al., 2017). Historically, unauthorized migration was seasonal and cyclical, with migrants moving freely across the border. However, stricter border enforcement in the 1990s, and escalating during the Great Recession, curtailed this mobility and prompted many families to settle permanently in the United States (Martínez et al., 2018; Massey et al., 2015).
Despite their marginalization, undocumented immigrants make substantial economic contributions, paying an estimated $11.64 billion annually in state and federal taxes (Gee et al., 2016). Yet, they remain excluded from critical safety net programs such as Social Security and Medicare, rendering them economically vulnerable as they age (Zallman et al., 2013). Fear of deportation often prevents them from seeking health care services, resulting in untreated health conditions and significant psychological stress, which in turn can contribute to various physical and mental health issues (Ayón, 2020; Rodriguez et al., 2017). Exposure to the health context in the United States can expose migrants to poor dietary and health behaviors leading to higher rates of obesity and smoking for men with migration experience compared to those with no migration experience (Ullmann et al., 2011). Lack of legal status is also associated with lower educational attainment, reduced social capital, and language barriers, further limiting access to healthcare and social services (Angel & Berlinger, 2019; Jiménez-Rubio & Vall Castelló, 2020; Orrenius & Zavodny, 2009).
For undocumented immigrants, the barriers are even greater, precluding access to employer-provided pensions and U.S. Social Security Benefits (Aguila & Vega, 2017; Gonzales, 2015; Herd et al., 2018). Consequently, many U.S. immigrants rely more on family support than on savings for their retirement plans, (Fontes, 2011) often motivating them to return to Mexico, where the cost of living is lower (Massey et al., 2002). Many older adults in Mexico also receive remittances from family members living abroad, particularly in the United States. Migrant children of non-migrant parents often bear the responsibility of supporting their aging parents back in Mexico (Carling, 2014). In 2012, U.S. remittances to Mexico were $22.4 billion (Maldonado & Hayem, 2013); altogether, 16.2% of older adults in Mexico receive remittances (Aguila, 2011).
Although, return migration has become more common in recent years—many returnees face significant challenges reintegrating into Mexican society including limited access to health care and social systems, exacerbated by their previous undocumented status in the United States and their unfamiliarity with Mexican bureaucracy (Medina & Menjívar, 2015). Previous research has found that return migrants have worse mental health and higher rates of psychiatric disorders and this is especially true for those who were deported (Hamilton et al., 2023; Ullmann et al., 2011). Studies indicate that undocumented return migrants experience worse health outcomes compared to both legal migrants and non-migrants in Mexico, largely due to factors such as legal precarity, chronic stress, and limited access to and utilization of healthcare services. (Amuedo-Dorantes et al., 2013; Berk & Schur, 2001; Cleaveland & Ihara, 2012; Ferraro & Shippee, 2009; Garcini et al., 2021; Hamilton et al., 2023; Wallace et al., 2013). Return migrants are also more likely to be divorced and have smaller households, which may limit the support networks available to them (Mudrazija et al., 2016). Nonetheless, research on the cognitive health of return migrants remains limited, particularly regarding how their migration experiences and labor sector participation impact their risk of developing dementia.
Migration and Cognitive Function
Immigrants, especially those who migrate in midlife, have lower rates of cognitive impairment than U.S.-born older adults (Downer et al., 2016). Male Mexican immigrants have cognitive function similar to that of male non-Hispanic whites of comparable socioeconomic status (Casanova & Aguila, 2020). Among Mexicans in Mexico and the United States, a higher proportion of older adults in Mexico—non-migrants—have experienced cognitive decline (Mejia-Arango, Singelmann, & Saenz, 2020). Based on previous research, there are clear social risk factors for dementia that are particularly relevant for undocumented migrants. There are also disparities between documented and undocumented immigrants in cognitive function and mental health as they age (Casanova & Aguila, 2020).
Having a low socioeconomic position throughout life has been shown to be associated with a greater risk of dementia among Mexican Americans in the United States (Zeki Al Hazzouri et al., 2011). Family support can help offset some of these disadvantages, but return migrants, especially those who have spent extended periods in the United States, often live in smaller households and have fewer female family members—which limits the availability of informal caregivers—or other family members for financial and emotional support (Mudrazija et al., 2016). Return migrants may also face more pronounced problems in readjusting to a new environment, where feelings of isolation and loss of independence can adversely affect their psychoemotional health (Sadarangani & Jun, 2015).
The Informal and Formal Sectors’ Impact on Health Disparities
In both the United States and Mexico, lower educated workers, including U.S. immigrants, are overrepresented in informal sector jobs such as house cleaning, gardening, agriculture, hospitality, and construction (Aguila & Angel, 2021). The informal sector comprises between 11% and 40% of the U.S. labor force and 58% of that in Mexico (Smith Nightingale & Wandner, 2011). U.S. Hispanics are particularly likely to work in the informal sector compared to other U.S. workers (Pisani, 2021). Informal sector jobs typically pay lower wages, limiting workers’ ability to escape poverty and increasing their financial insecurity (Smith Nightingale & Wandner, 2011).
In Mexico, informal sector workers face similar challenges. Most lack access to social security benefits and health insurance, leaving them financially unprepared for retirement (Aguila et al., 2011; CONSAR, 2016). Formal protections are limited to those in the private sector under IMSS (Mexican Social Security Institute) or in the public sector mainly under ISSSTE (Social Security Institute for Public Sector Workers). Workers must contribute for decades—24 years for IMSS and 25 years for ISSSTE—to qualify for benefits (Alonso et al., 2015). Informal workers, by contrast, rely on non-contributory pensions that provide minimal support (Lee et al., 2023).
Efforts to address healthcare disparities in Mexico, including Seguro Popular (2001–2018), INSABI (2020–2022), and the current IMSS Bienestar Program, have faced challenges in providing consistent coverage for uninsured workers. Seguro Popular was launched in 2001 as a public program for low-income families without access to any healthcare coverage. Initially implemented as a pilot program in five states, it expanded to 15 additional states in 2002, four more in 2003, and the remaining eight states by 2005. By 2018, the program provided coverage to 53.5 million individuals (Centro de Estudios de las Finanzas Públicas, 2023). In 2020, Seguro Popular was replaced by INSABI, which only covered 32.8 million individuals. In 2023, INSABI was substituted by IMSS Bienestar, a program managed by IMSS providing primary, secondary, and more advanced medical care for the uninsured (Centro de Estudios de las Finanzas Públicas, 2023). Nonetheless, these persistent gaps in healthcare access leave return migrants, especially those who spent years without formal protections in the United States, particularly vulnerable to poor health outcomes.
The Connection Between the Informal Sector and Cognitive Decline
Upon returning to Mexico, return migrants, often re-enter the informal sector without health insurance or social security benefits, exacerbating their financial and health vulnerabilities. We argue that the lack of preventative services, prompt detection, and disease management of chronic conditions because of informal sector access to low quality health care and stress related to lack of income stability during their working life and retirement, may increase the risk of cognitive decline and dementia in older age. While previous research has examined return migration (e.g., Aguila et al., 2023; Aguila & Vega, 2017), there is limited attention to the intersection of legal status, informal sector participation and its impact on cognitive health. This leaves significant gaps in understanding how legal status and working in informal or formal sectors impacts the risk of dementia in older adults. This study highlights the urgent need for policies that address the unique vulnerabilities of aging return migrants, shedding light on the transitional effects of migration and legal precarity on late-life health outcomes.
Using data from the 2018 Mexican Health and Aging Study (MHAS), this study investigates how migration and formal or informal sector participation influence the cognitive health of Mexican older adults. We hypothesize that return migrants—particularly those who were undocumented in the United States and are now involved in Mexico’s informal sector—have worse cognitive outcomes than both non-migrants in the informal sector and return migrants in the formal sector. By examining differences in health, family, and economic circumstances, this study seeks to address critical gaps in the literature on the long-term health consequences of migration.
Data and Methods
To test our hypotheses, we use data from the 2018 wave of the Mexican Health and Aging Study (MHAS). The MHAS is a nationally representative survey of the population 50 years old and older collected in 2001, 2003, 2012, 2015, 2018, and 2021, with information on respondents’ income, wealth, health, and health insurance (Wong et al., 2017).
Sample
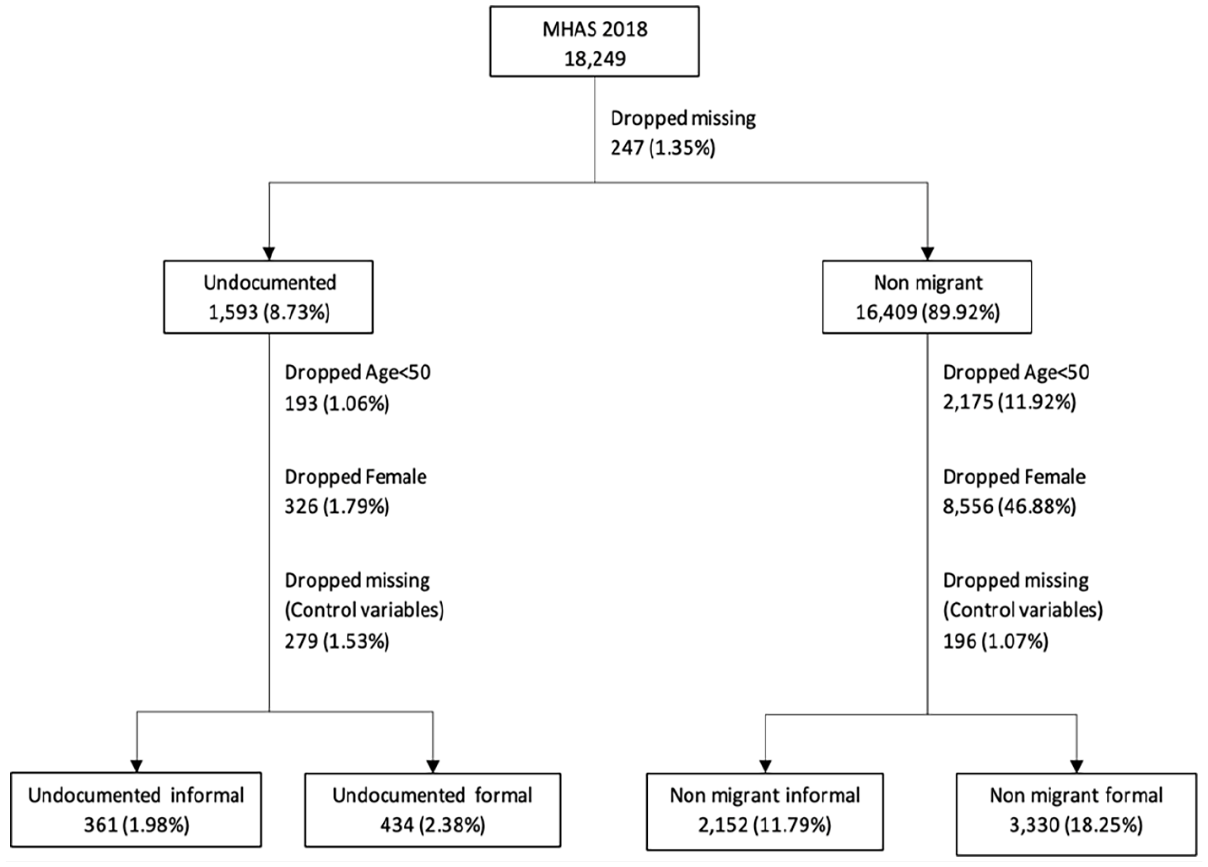
Our sample includes males 50 or older who are undocumented return migrants and non-migrants. Return migrants are MHAS respondents who migrated to the United States and returned to Mexico. We used previous MHAS waves (2001–2015) to classify respondents as return migrants and construct variables related to their migration history (Figure 1). Non-migrants are respondents who never migrated. We also classified return migrants by their legal status while living in the United States. Documented return migrants are those who reported being permanent residents or citizens of the United States or contributed to the U.S. Social Security system using their name or own social security number. Documented migrants are a very small share of the sample (N = 127) and a very small share of historical migration flows to the United States. Therefore, they are too small of a group to include in our analyses. Undocumented migration has almost always been much more prevalent than documented migration from Mexico (Durand & Massey, 2019). And based on descriptive analysis of our data, we do find they are more likely to be in formal employment, however again the sample is too small to conduct meaningful comparisons across groups in our analysis. Further, documented migrants may be less likely to return and only comprise a small share of return migrants in surveys (Hazán, 2014). Undocumented return migrants are classified here as those who do not report being permanent residents or citizens and do not report contributing to the U.S. Social Security system or report contributing but not with their own name or social security number. 1
MHAS data and sample.
We also constructed a variable to identify respondents in the formal and informal sectors of the Mexican economy. Respondents in the formal sector were those who self-reported contributing to the Mexican social security system during their working life or who receive benefits from that system. Additionally, we used data from the MHAS linked to IMSS’s administrative records to check the respondents with a labor history in the formal sector. We used information from all MHAS waves (2001–2015) to build a variable of labor history in the formal sector in Mexico. Respondents without contributions to the social security system were considered to be in the informal sector. 2 We exclude women from the analysis because they comprise a very small share of the return migrants. Furthermore, previous research on cognitive functioning tends to run stratified analyses because of the different cognitive health trajectories; women on average live longer and have higher prevalence of cognitive impairment than men (Mielke et al., 2014). Women also have different reasons for migrating and therefore understanding the role of migration on their wellbeing may be quite different (Donato, 2010; Massey et al., 2006). For instance, research on the mortality of migrants suggests the effect of migration on health is moderated by gender (Reyes & Garcia, 2020).
Our final analytical sample is 795 undocumented return migrants and 5,482 non-migrants. In the analysis, we compare respondents in the formal and informal sectors in Mexico. Our sample includes 361 undocumented returnees in the informal sector in Mexico and 434 in the formal sector. Among non-migrant respondents, 2,152 are in the informal sector and 3,330 in the formal sector. We use a similar approach to previous literature that has compared return migrants and non-migrants to understand differences between population that has never migrated with population with migration history to the U.S. (e.g., Campos-Vazquez & Lara, 2012; Lacuesta, 2010).
Outcome Variable
As our main outcome variable, we classified cognitive status as a binary variable: cognitively normal (=0) or likely dementia (=1). We used MHAS validated cognitive function classification, by which respondents with likely dementia are those with cognitive impairment no dementia (CIND) or dementia. Normal corresponds to those classified as normal or normal with instrumental impairment (Mejia-Arango, Singelmann, & Saenz, 2020). For direct respondents, MHAS employs a modified version of the Cross-Cultural Cognitive Examination (CCCE) including verbal learning, delayed memory, attention, constructional praxis, visual memory, verbal fluency, orientation, and processing speed domains. For proxy respondent, MHAS employs the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE). MHAS classifies with likely dementia direct respondents with at least two cognitive domains scores ≥1.5 SDs below norms and with at least one difficulty performing an instrumental activity of daily living (IADL). For proxy responses, MHAS classified with likely dementia when the IQCODE scores were ≥3.4 (Mejia-Arango, Aguila, et al., 2020).
Control Variables
We included the following demographic and socioeconomic variables: age, years of education, number of household members, and marital status (where married or in a civil union was coded as 1, and any other marital status, such as single, widowed, or divorced, was coded as 0). Rural residence was coded as 1 for those living in localities with fewer than 2,500 inhabitants, and 0 for those in larger localities. We also controlled for chronic conditions, including hypertension, diabetes, cancer, respiratory illness, heart attack, and stroke, with two or more conditions coded as 1, and one or less as 0. Current access to health insurance in Mexico was represented by four binary variables: receiving health insurance from the Social Security system (coded as 1 for receiving, 0 otherwise), receiving private health insurance (1 for receiving, 0 otherwise), receiving Seguro Popular (1 for receiving, 0 otherwise), and being uninsured (coded as 1 for uninsured, 0 otherwise). We measured respondents’ mental health with a modified CES-D depressive symptoms count (0–9 scale), based on the self-reported frequency of experiencing in the past week feeling depressed, feeling that everything was an effort, restless sleep, feeling unhappy, feeling alone, not enjoying life, did not have energy, feeling sad, or feeling tired.
We classified respondents with a score ≥5 as having high depressive symptoms based on a clinical validation study (Aguilar-Navarro et al., 2007). We also control for a set of variables to capture the health behaviors of respondents that have been associated with cognitive functioning and may also vary by immigration status (Aggarwal et al., 2006; Lenoir et al., 2011; Wright et al., 2006). For instance, smoking is less common among Mexican immigrants than non-migrants, suggesting migrants may be more selected on their health choices (Fleischer et al., 2017). To account for health behaviors, we included dummy variables for obesity, smoking, and alcohol consumption. Obesity was defined with a body mass-index (BMI) ≥ 30 (WHO, 2024), whereas smoking now and drinking alcohol in the last 2 months are defined as 1 = Yes, and 0 = No. Additionally, previous studies have documented that social engagement could be a dementia protective factor (e.g., Livingston et al., 2020). Social engagement here is identified as having social contact with friends or relatives. To account for different migration experiences we include variables on age at first migration and years lived in the United States.
Methods
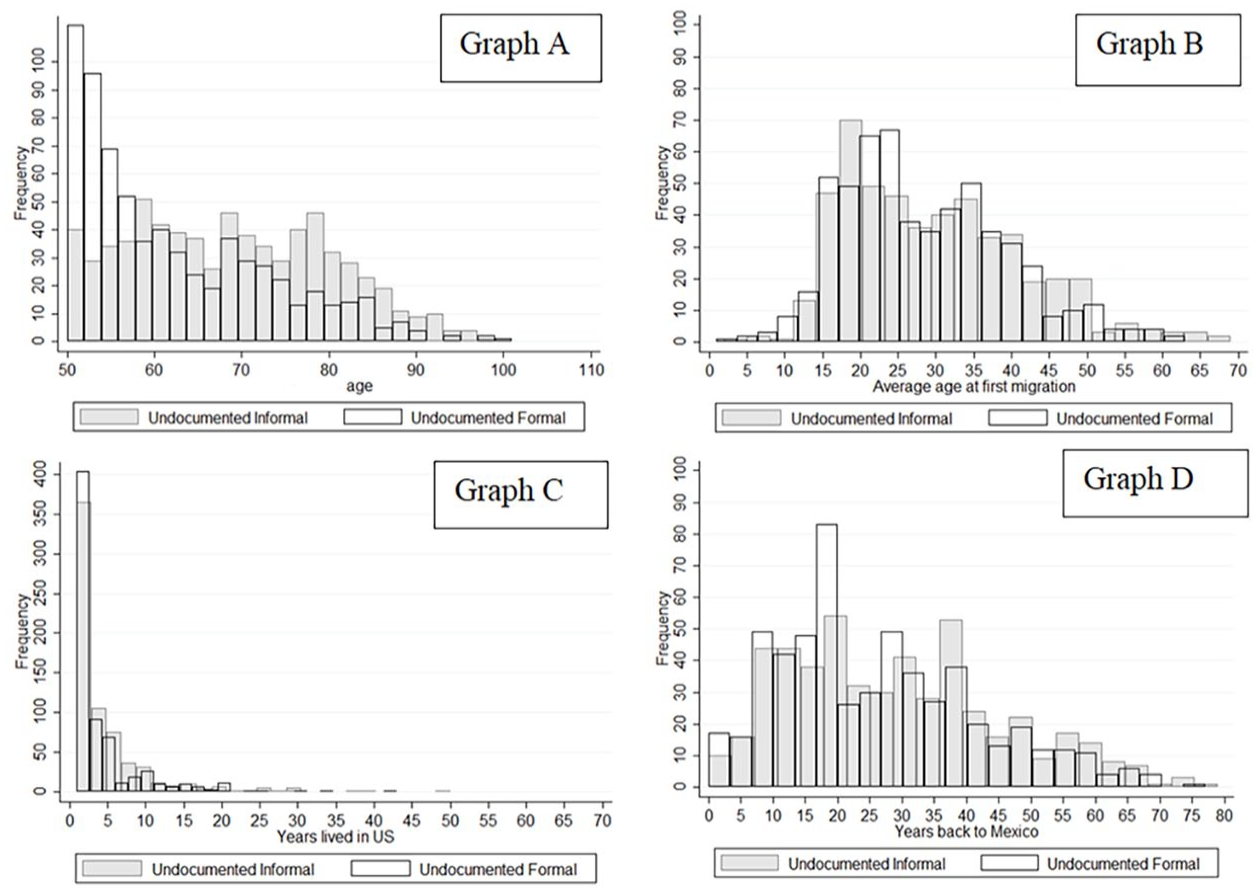
We obtained histograms for the migration history variables of undocumented return migrants by formal and informal sectors, as well as their age, as shown in Figure 2. We examine differences of mean outcome variables and covariates between respondents in the formal and informal sectors using a t-test for continuous variables and a Chi-square for categorical variables. Table 1 shows the descriptive characteristics of the sample. We employ logistic regression models with standard errors clustered at the household level to analyze the likelihood of likely dementia for undocumented return migrants relative to that for non-migrants and stratified by formal and informal work history in Mexico. Among undocumented return migrants, we also estimate logistic regression models by formal and informal work history in Mexico to assess the relationship migration experience and likely dementia. In all our regression analyses, we show two specifications. The first specification includes sociodemographic and health insurance variables, and a second specification adds other known risk factors of dementia (two or more chronic conditions, depressive symptoms, obesity, smoking, alcohol, and social engagement). In addition, for the regression analysis among undocumented return migrants (Table 3), we also include migration history variables. For ease of interpretation, we present estimates from logistic regression models as odds ratios (OR). An OR greater than 1 indicates the independent variable is associated with higher odds of the dependent variable; an OR less than 1 indicates the independent variable is associated with a lower odds of the dependent variable. For example, an Odds Ratio of 1.258 for age would imply one additional year of age results in a 25.8% increase in the odds of the outcome variable. Conversely, an Odds Ratio of 0.259 implies that one additional year of age results in a 74.1% decrease (1 − 0.259 = 0.741) in the odds of the outcome variable. We use Stata SE v18 for the analysis.
Age and migration characteristics of undocumented return migrants Graphs A-D.
Descriptive Characteristics for Formal and Informal Sectors.
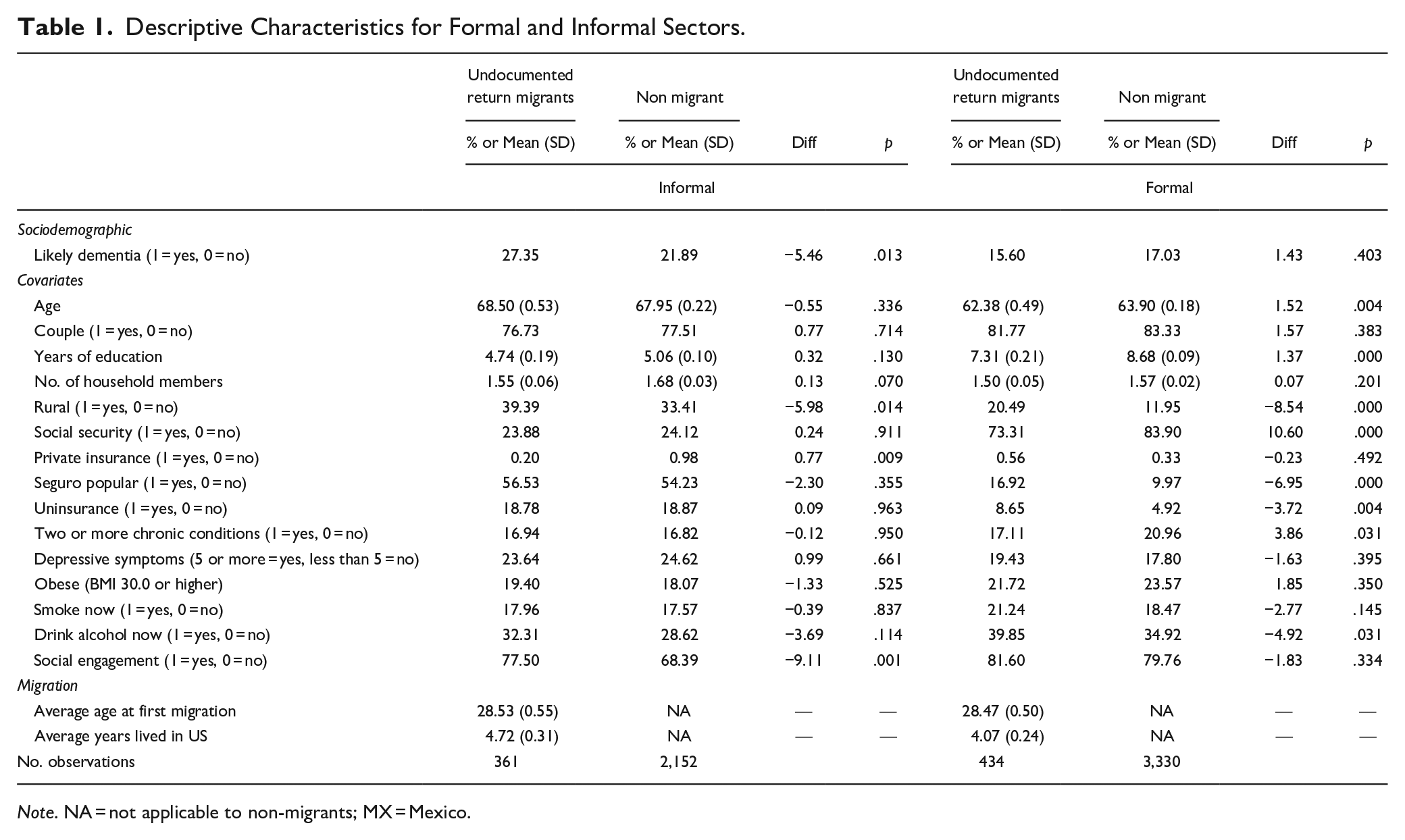
Note. NA = not applicable to non-migrants; MX = Mexico.
Results
Figure 2 illustrates the distribution of key migration and demographic characteristics among undocumented return migrants, comparing those in the informal and formal sectors. Graph A shows the age distribution of the sample. It indicates that undocumented migrants in the informal sector tend to be slightly older than those in the formal sector, with the majority clustered between ages 50 and 70. Graph B displays the age at first migration. It demonstrates that first-time migration is concentrated in early adulthood (ages 15 to 30), with some variation between the two groups. Graph C highlights the number of years lived in the United States. It shows most return migrants lived in the United States for fewer than 10 years. Finally, Graph D shows the years since return to Mexico. There is a broad range here, with notable peaks at 10 and 20 years since return.
Table 1 presents the descriptive characteristics of undocumented return migrants and non-migrants across the informal and formal sectors. Among informal sector workers, a significantly higher proportion of undocumented return migrants exhibit signs of dementia (27.35%) compared to non-migrants (21.89%; p = .013). In contrast, among formal sector workers, there is no significant difference in dementia likelihood between undocumented return migrants (15.60%) and non-migrants (17.03%; p = .403). Educational attainment is consistently lower among undocumented return migrants in both sectors, with the difference reaching statistical significance among formal sector workers (7.31 vs. 8.68 years; p < .001 in the formal sector).
Rural residency is significantly more common among undocumented return migrants in both sectors (p = .014 for informal workers; p < .001 for formal workers). Social security coverage is low for both groups in the informal sector but is significantly higher in the formal sector. Among formal sector workers, undocumented return migrants are 10.60% less likely to have social security coverage than non-migrants (p < .001). Seguro Popular usage is higher among informal sector workers but, in the formal sector, undocumented return migrants are more likely to rely on Seguro Popular or remain uninsured compared to non-migrants. A higher proportion of those in the informal than in the formal sector report depressive symptoms. There are no differences within sectors between undocumented and non-migrants. A higher proportion of formal than informal sector has obesity, smokes, and drinks alcohol. Respondents in the formal sector have more social engagement than those in the informal sector. The average age at first migration is similar for undocumented return migrants across sectors (28.53 years for informal workers; 28.47 years for formal workers). Undocumented return migrants in the informal sector report having spent more years living in the United States (4.72 years) compared to those in the formal sector (4.07 years).
Table 2 presents the results of logistic regressions examining the likelihood of dementia among undocumented return migrants and non-migrants in the informal and formal sectors. The odds of likely dementia are significantly higher for undocumented return migrants compared to non-migrants in the informal sector (Odds Ratio [OR] = 1.289, p < .05) but not in the formal sector (OR = 0.838, p > .1). These findings are consistent also in the second specification that includes health, health behaviors, and social engagement. Among covariates, age is significantly associated with a higher likelihood of dementia for in the informal sector, with each additional year of age increasing the odds of likely dementia by 1.019%, but there appears to be no association between age and dementia in the formal sector.
Logit Likely Dementia Undocumented Versus Non-Migrants in the Informal and Formal Sectors.
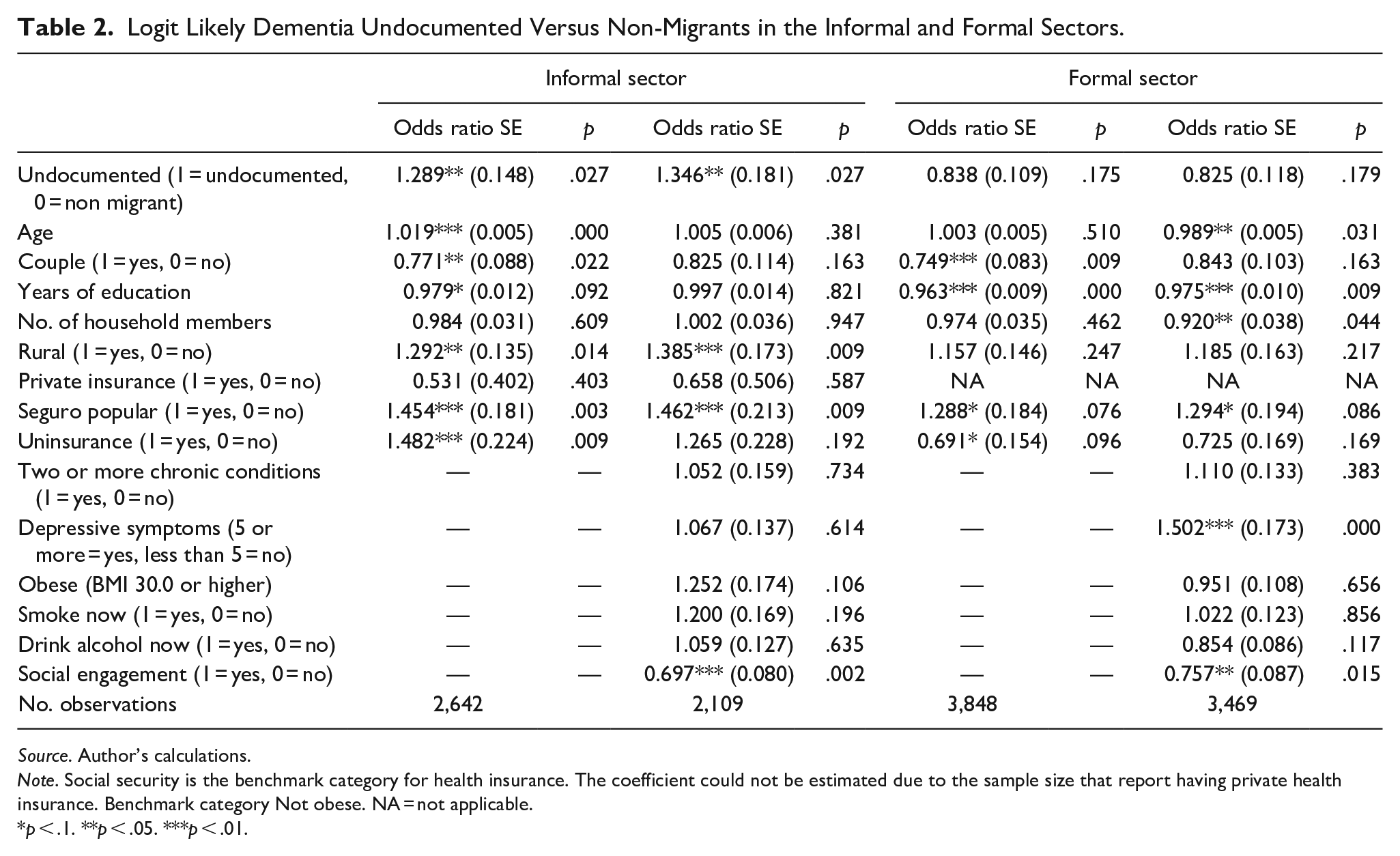
Source. Author’s calculations.
Note. Social security is the benchmark category for health insurance. The coefficient could not be estimated due to the sample size that report having private health insurance. Benchmark category Not obese. NA = not applicable.
p < .1. **p < .05. ***p < .01.
Being in a couple is associated with lower odds of dementia in both sectors (OR = 0.771, p < .05 informal and OR = 0.749, p < .01). Years of education is protective against dementia in both sectors, with stronger effects in the formal sector (OR = 0.963, p < .01) compared to the informal sector (OR = 0.979, p < .1). Rural residency significantly increases the odds of dementia in the informal sector (OR = 1.292, p < .05) and to a lesser extent in the formal sector, where the result is not statistically significant (OR = 1.157, p > .1).
Regarding health insurance, having Seguro Popular significantly increases the likelihood of dementia in both sectors (informal: OR = 1.454, p < .01; formal: OR = 1.288, p < .1). Uninsurance is also a significant risk factor in the informal sector (OR = 1.482, p < .01) but appears to have a protective effect in the formal sector (OR = 0.691, p < .1). Private health insurance could not be reliably estimated due to the small sample size.
Depressive symptoms and social engagement emerge as significant factors in the formal sector. Depressive symptoms are associated with higher odds of dementia (OR = 1.502, p < .01), while social engagement is protective (OR = 0.757, p < .05). Social engagement is also protective in the informal sector (OR = 0.697, p < .01).
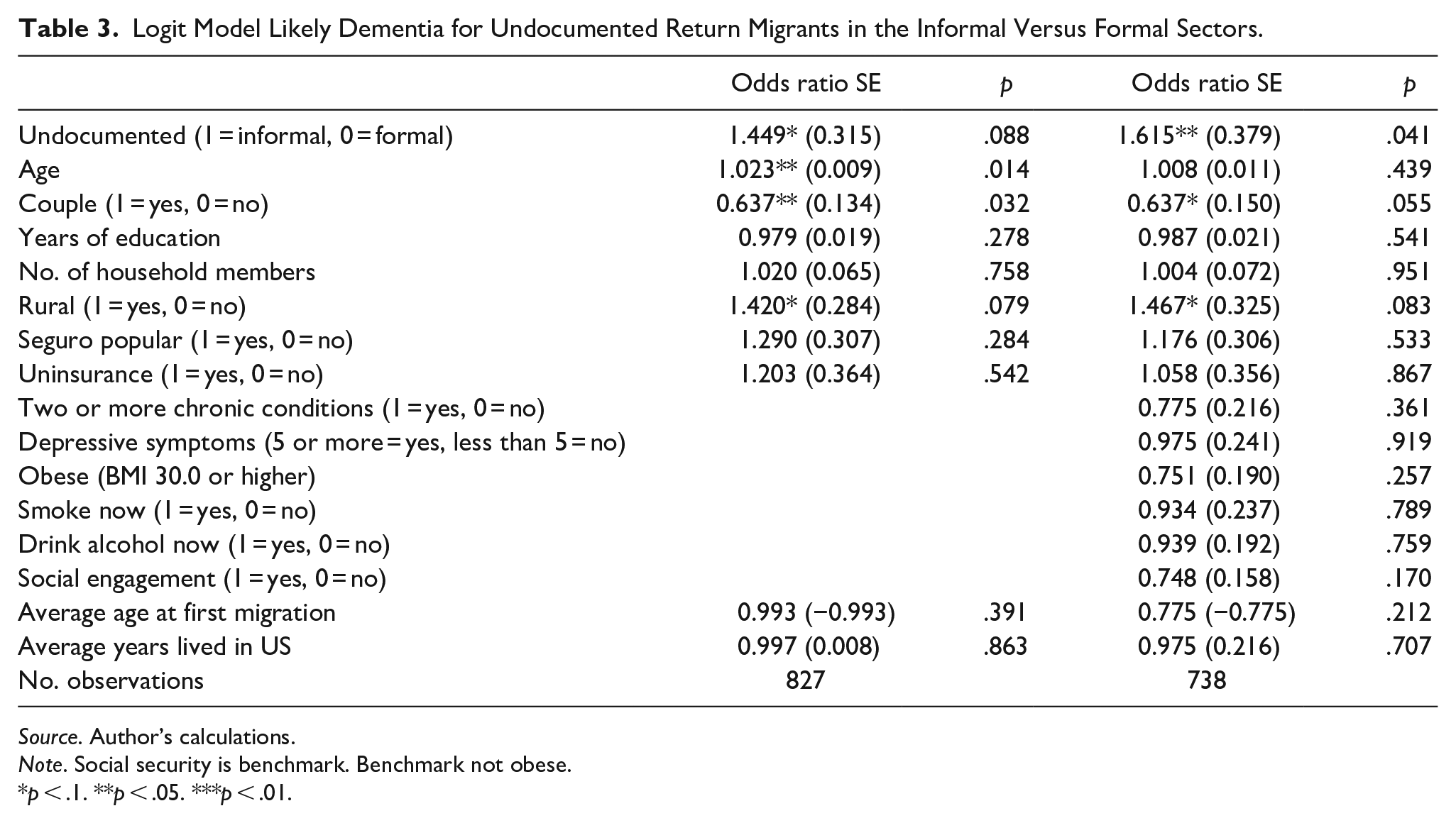
Table 3 presents the results of the logistic regression model comparing the likelihood of likely dementia among undocumented return migrants in the informal and formal sectors. The odds of dementia are significantly higher for undocumented return migrants in the informal sector compared to those in the formal sector. In the first model, the odds of dementia are 1.449 times higher for informal sector workers (p < .1). This effect is higher in the second model, where the odds are 1.615 times higher (p < .05). Being in a couple is significantly protective against dementia, while years of education, household size, and health insurance coverage (Seguro Popular and uninsurance) do not show significant associations with dementia likelihood. Age and rural residency are associated with higher dementia risk (OR = 1.023, p < .05) for age and OR = 1.420, p < .1 for rural residency); undocumented return migrants living in rural areas are 42% more likely to show signs of dementia. Migration-related factors, including average age at first migration and average years lived in the United States, are not statistically significant predictors in either model (p > .1). Health and health behavior related variables such as the presence of two or more chronic conditions, depressive symptoms, obesity, smoking, and alcohol consumption included in the second specification show no statistically significant associations. Social engagement is also not statistically significant in the second specification (OR = 0.748, p > .1).
Logit Model Likely Dementia for Undocumented Return Migrants in the Informal Versus Formal Sectors.
Source. Author’s calculations.
Note. Social security is benchmark. Benchmark not obese.
p < .1. **p < .05. ***p < .01.
Discussion
This study highlights the significant health challenges faced by undocumented return migrants, particularly their increased likelihood of cognitive decline compared to non-migrants. The findings are especially stark among those involved in the informal sector in Mexico, where precarious work conditions and limited access to social protections exacerbate vulnerabilities. This suggests that the combination of legal precarity and economic insecurity accumulated over the life course contributes to worse cognitive outcomes. These results are consistent with research linking the chronic stress associated with undocumented status and limited access to healthcare in the United States to long-term health consequences (Cheong & Massey, 2019; Garcini et al., 2021). Our analysis underscores the importance of legal and economic contexts in shaping health outcomes for aging populations, particularly those who have experienced migration.
The Protective Role of Formal Sector Employment
The protective effects of formal sector employment observed in this study, suggests that labor sector attachment is critical in moderating the health risks associated with migration. Undocumented return migrants in the formal sector in Mexico, who have access to social security benefits and healthcare services, show significantly better cognitive outcomes than their counterparts in the informal sector. This finding points to the broader role of institutional support in mitigating some of the health risks related to undocumented status and the life-course stressors experienced by migrants.
This employment dynamic leaves many aging migrants without adequate resources to address health challenges or secure financial stability in retirement. The finding that rural residency significantly increases the odds of dementia that is particularly prevalent for undocumented return migrants further underscores the compounding effect of geographic and structural disadvantage. Rural areas often lack access to quality healthcare and employment opportunities in the formal sector, worsening health disparities among vulnerable populations.
Policy Implications
In Mexico, expanding access to formal sector employment or providing more robust health coverage for informal workers, including return migrants, could help reduce health disparities among aging populations. Similarly, in the United States, immigration reforms that allow undocumented migrants to access healthcare and social safety nets could alleviate some of the long-term cognitive health impacts observed in this population. Our findings support the argument for more inclusive policies that provide economic and healthcare protections for migrants across their life course.
Additionally, binational efforts between the United States and Mexico could play a pivotal role in supporting return migrants. Bilateral agreements could facilitate the portability of retirement benefits, ensure continuity of healthcare coverage, or provide targeted reintegration programs for aging returnees. Addressing the transnational nature of migration and health outcomes requires coordinated policies that consider the cumulative effects of migration on vulnerable population.
Study Limitations and Future Research Directions
While this study provides important insights, it is not without limitations. First, we rely on self-reported data for migration history and legal status. The constructed measure of legal status to identify undocumented respondents can introduce a degree of uncertainty, as this status is classified by the authors rather than directly reported by the respondents. Future studies should aim to refine measures of legal precarity to improve the accuracy of such classifications. Second, the cross-sectional nature of the data limits our ability to draw causal inferences about the relationship between undocumented status, labor sector participation, and cognitive decline. Longitudinal studies are needed to track health outcomes over time and better understand the life-course effects of migration and legal status on aging. Such studies could explore how cumulative stress, occupational exposures, and social support networks interact to shape cognitive health outcomes. Third, due to the small sample size of documented migrants (N = 127), we excluded this group from our analyses. While this decision was necessary to maintain statistical robustness, it limits the generalizability of our findings to documented migrants, who may have different health trajectories. Finally, because of sample size constraints, our analysis focuses primarily on male return migrants. Future research should explore gender differences in health outcomes and incorporate larger samples of documented migrants to allow for broader comparisons.
Conclusion
This study underscores the profound health challenges faced by undocumented return migrants, particularly those in the informal sector. The combination of legal precarity, economic insecurity, and limited institutional support creates significant barriers to healthy aging. By highlighting the protective role of formal sector employment and the detrimental effects of participating in the informal sector, these findings call for targeted interventions and inclusive policies that address the unique vulnerabilities of this population. Addressing the structural determinants of health for migrants across their life course is essential to reducing health disparities and promoting equitable outcomes for aging populations in both Mexico and the United States.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge support from the Center for Advancing Sociodemographic and Economic Study of Alzheimer’s Disease and Related Dementias (CeASES) funded by NIA grant 5P30AG066589, the USC AD/ADRD Center on Minority Aging Research (RCMAR) funded by NIA grant P30 AG043073.