
Abstract
This paper explores disparities in health outcomes among Hispanic older adults living near the United States (U.S.)-Mexico border. Hispanic older adults face significant barriers to healthcare access, stemming from multiple factors: limited income, high medical costs, elevated rates of chronic disease and dementia, and greater reliance on public insurance programs, relative to other racial, ethnic, and age groups. Likewise, Hispanic older adults diagnosed with dementia near the U.S.-Mexico border face documented barriers to healthcare, including higher costs, fewer adult day care centers, and a lack of health insurance. We use a health disparities and dementia care conceptual framework to explore the interactions of these social determinants of health for the older Hispanic American population. Using data from the Hispanic Established Populations for the Epidemiologic Study of the Elderly (HEPESE, waves 8–9, 2012–2013 and 2016), complemented by the American Community Survey (ACS, 2011–2022), we conduct descriptive and regression model analyses to explore the relationship between living in U.S. counties and states that border Mexico and health outcomes such as mobility difficulties, self-care, self-reported health, and issues with activities of daily living (ADL) and instrumental activities of daily living (iADL). We control for demographic, health, and social support characteristics to account for individual level differences. We also examine how proximity to the border and caregiver and community resources affect outcomes for Mexican American older adults aged 80 and older—a growing demographic with limited data and a higher risk of health disparities. Our findings show that Hispanic older adults who reside closer to the border rely more on caregivers for instrumental and emotional support, report worse self-reported health, experience more difficulty paying bills, report lower independence in both ADL and iADL measures, and face an increased risk of dementia diagnosis, relative to their counterparts further from the border. Our findings suggest the urgency for better policies to address the needs of older Hispanic Americans with dementia in the border region. These policies require a focus on primary care, benefits counseling, and assistance in locating and accessing community services. The long-term focus should be to support flexible caregiving arrangements that increase the autonomy of both the care recipient and caregiver, community support, culturally competent caregiving, infrastructural improvements, and in-home support services for families coping with a dementia patient.
Introduction
This paper explores disparities in health outcomes among Hispanic older adults in states that include portions of the U.S.–Mexico border. This border extends for approximately 1,954 miles; on the U.S. side, it crosses California, Arizona, New Mexico, and Texas, and it is one of the most significant international boundaries in the world from the standpoint of economic activity and the dense population residing around it (Taylor, 1988). Older adults near the border are vulnerable, with Mexican American residents showing lower physical activity rates (65.6% vs. 80.9% for non-Hispanics), higher Alzheimer’s rates (13%–18% among those 65+), lower cognitive function, and greater difficulty with ADLs (Texas Tribune, 2023).
Populated by about 19 million inhabitants, the border region faces significant socioeconomic challenges. While 12% of people living outside the four border states live at or below the poverty line, about twice as many live at or below the poverty line within the border region (Migration Policy Institute, 2023). In addition, Mexican Americans in California, Arizona, New Mexico, and Texas often face challenges related to healthcare and education access, food insecurity, and a lack of recreational infrastructure (U.S. Census Bureau, 2022b). According to the U.S. Census Bureau’s Community Resilience Estimates, 25.3% of people in border counties are categorized as High Risk based on factors like caregiver support, crowding, and the presence of older adults, compared to 21.6% in non-border counties within border states (U.S. Census Bureau, 2022b). The documented vulnerabilities in the border region make it crucial to examine disparities in healthcare access and caregiving among Hispanic older adults, and how these factors influence health outcomes (Quiroz et al., 2022).
About 50% of the people living in California, Arizona, New Mexico, and Texas identify as Hispanic. In urbanized areas of these states, the percentage ranges from 64% to 97% (Southern Border Communities Coalition, 2023; Weigel & Armijos, 2019). Moreover, Hispanics in border states face distinct challenges in healthcare access, caregiving, lower overall incomes, lower-quality education, and constrained employment opportunities compared to non-Hispanics in the region (NBC News, 2024). Much as in the U.S. overall, Hispanics in the four border states have the highest uninsured rate of any racial or ethnic group in the country, more than triple that of non-Hispanic Whites (U.S. Census Bureau, 2022a). Hispanics are also more likely to use public insurance programs such as Medicare and Medicaid than non-Hispanics, making them more vulnerable to policy changes and related uncertainty. Barriers related to culture and language, migration status, mobility, preventive health care, caregiving, and community support are also common among U.S. Hispanics (U.S. Department of Health and Human Services, 2024).
Older adults living on the U.S.-Mexico border often face more adverse socioeconomic conditions, relative to non-border residing older adults, due to a confluence of structural and geographic factors (Bastida et al., 2011). Border regions tend to have higher poverty rates, limited access to healthcare, and lower educational attainment, reflecting systemic underinvestment in these areas (Bastida et al., 2011). Employment opportunities in border communities are often concentrated in low-wage industries, such as agriculture and the service sector, which can perpetuate economic inequality (Flota & Mora, 2001; Mora & Dávila, 2006). Additionally, border residents may experience challenges related to immigration policies, language barriers, and social marginalization, further exacerbating socioeconomic disparities (Bruhn, 2014; Tenorio et al., 2024). Border communities frequently face the challenges of being on the periphery of two distinct economic and political systems, leading to gaps in healthcare access and economic opportunities. These factors combine to create environments where individuals are more likely to experience financial strain, limited healthcare access, and consequently, poorer health outcomes.
Hispanics over 80 years old, the focus of this study, experience compounded risk. Overall, improved medical care and a higher quality of life have led to increased life spans, but these improvements have led to the emergence of new challenges such as geriatric care, specifically for those living with dementia and their ability to access affordable and quality health care (Angel et al., 2022). Demographic projections indicate that given their lower socioeconomic status and aging population, Mexican-origin older adults will be disproportionally affected by increases in chronic diseases such as Alzheimer’s disease and related dementias (ADRD) in the coming decades (Mejia-Arango et al., 2020). The U.S.–Mexico Border Health Commission, formed between the U.S. Secretary of Health and Human Services and the Secretary of Health of Mexico in 2000, summarized these challenges in the Healthy Border 2020 report, identifying chronic and degenerative diseases among its top five public health priorities. The report also defined evidence-based research as one of the key strategies to address these health disparities (U.S. Department of Health and Human Services, 2021).
This study compares the health outcomes of Mexican Americans aged 80 and older who live in California, Arizona, New Mexico, and Texas–both near and far from the border–with those who live in all other, non-border states elsewhere in the U.S. The 80+ age group is of particular interest, as older adults in the U.S.-Mexico border region may experience compounded vulnerabilities related to socioeconomic status, healthcare access, and other social determinants of health over the life course. For example, this group typically experiences an intersection of challenges associated with aging, such as higher rates of chronic conditions, mobility limitations, caregiving needs, and other barriers linked to being a historically underserved population (Angel et al., 2012). Moreover, adults aged 85 and older are projected to increase from 6.7 million in 2020 to 19 million in 2060, an almost 200% increase (Vespa et al., 2020). By narrowing our focus to this demographic, we aim to provide nuanced insights into the unique health and social needs of oldest-old Hispanic adults, contributing to targeted interventions and policies that can improve their quality of life.
We use an adapted version of the chronic care conceptual model for dementia care, combined with the health disparities conceptual framework (Angel et al., 2022; NIMHD, 2023; Wagner et al., 1996). The resulting conceptual model focuses on care which combines both individual-level characteristics and policy and structural domains such as community resource policy and caregiving assistance (Gassoumis et al., 2016). The individual-level domains are concerned with inequities related to housing access, chronic conditions, caregiving support, and food security, while the structural-level domains are focused on the inequities of the healthcare system; Medicare (and its potential inefficiencies), given a vast majority of older adults in the U.S. participate in it (Vega & Wallace, 2016).
The literature on health disparities near the U.S.-Mexico border highlights the challenges faced by older Hispanic populations. For example, Salinas et al. (2013), use a similar measure of distance to the border from previous HEPESE waves (waves 1–7, 1993–2011), to illustrate the health challenges faced by older Mexican Americans living in border regions, showing higher rates of disability and chronic conditions compared to non-border counterparts (Angel & Rote, 2021).
Our analysis considers border effects at multiple distances up to 100 miles from the border, enabling us to examine how health disparities may vary with increasing distance from the U.S.-Mexico border. Bastida et al. (2011), use the Border Epidemiologic Study on Aging to document that adults aged 45+ who live in Texas near the border with Mexico often cross into Mexico for health care, driven by high costs and accessibility issues in the U.S. They also find that uninsured individuals are more likely to engage in such medical tourism. These findings illustrate the complex interplay between insurance coverage, healthcare costs and access. Taken together, the literature highlights the need for targeted interventions to address the unique healthcare needs of Hispanic older adults in border regions, considering demographic and structural factors such as gender, nativity, and community support systems.
Our research seeks to expand on this literature with updated estimates from more recent waves of data and to compare our findings with nationally representative data beyond the border states. Moreover, we aim for our research to scaffold on the International Conference on Aging in the Americas, which provides a broader sociological context on the subject, emphasizing the intersecting social, economic, political, and environmental factors influencing health among aging Hispanics (Angel & Whitfield, 2007).
To explore the health challenges and disparities faced by Mexican American older adults in the four U.S. border states, we compare data from the HEPESE (wave 8, 2012–13; wave 9, 2016) to the American Community Survey (ACS). The HEPESE data allows us to explore the specific aging challenges of Mexican American older adults in the four bordering states, such as mobility difficulties, measures of likely dementia, cognitive function, ADLs, and iADLs, while the ACS provides nationally representative demographics, such as age, marital status, employment, Hispanic proportions of the county/state, income, Medicaid participation, mobility difficulties, and self-care difficulties. In that sense, the ACS is useful both as a comparison group to the U.S. more broadly, and the overall demographic characteristics of the four border states.
Our results indicate that Hispanic older adult populations, in particular, are at risk of experiencing barriers to care due to low earnings, higher health expenditures, chronic disease, and participation in public insurance programs. Findings indicate that closer proximity to the border—both in the form of living in a border state and of living in a border county—correlates with difficulties with IADLs, poorer overall health, lower exercise rates, and higher financial strain when receiving medical care, relative to non-border states, and relative to non-border counties in border states. Proximity to the border also correlates with higher rates of dementia, based on a self-reported diagnosis by a physician and other markers of likely dementia. These results have policy implications as they highlight the need for targeted programs to increase affordability of medical care in border states, and better data collection of cross-border treatment of older adults to assess the extent of disparities in cross-national older adult care.
Data and Methods
The HEPESE survey has been underway since 1993, funded by the National Institute on Aging. It provides data on risk factors for mortality and morbidity among a representative sample of Mexican-Americans aged 65 years and older who reside in five southwestern U.S. states: Arizona, California, Colorado, New Mexico, and Texas. We restrict our analytic sample to those who reside in a border state (drop Colorado) and who responded to either wave 8 (2012–13) or wave 9 (2016). The two waves were linked based on the geographic location and questionnaire number of the respondents (Markides et al., 2016, 2024). We further restrict the sample to adults 80 years and older who have non-missing geographic data on their county of residence and other relevant demographics Our final analytic sample consists of 452 unique, older Mexican-Americans.
We operationalize the distance to the border as residing within 100 miles or less of the border. In our analytic sample, all states have a combination of bordering and non-bordering counties. Figure 1 shows counties by their border status; 262 (58%) respondents reside in a border county, while 190 (42%) reside in a non-border county. However, it is important to note that not every county in every state has respondents in the HEPESE, so several counties within border states are not included in the sample (gray counties in Figure 1).
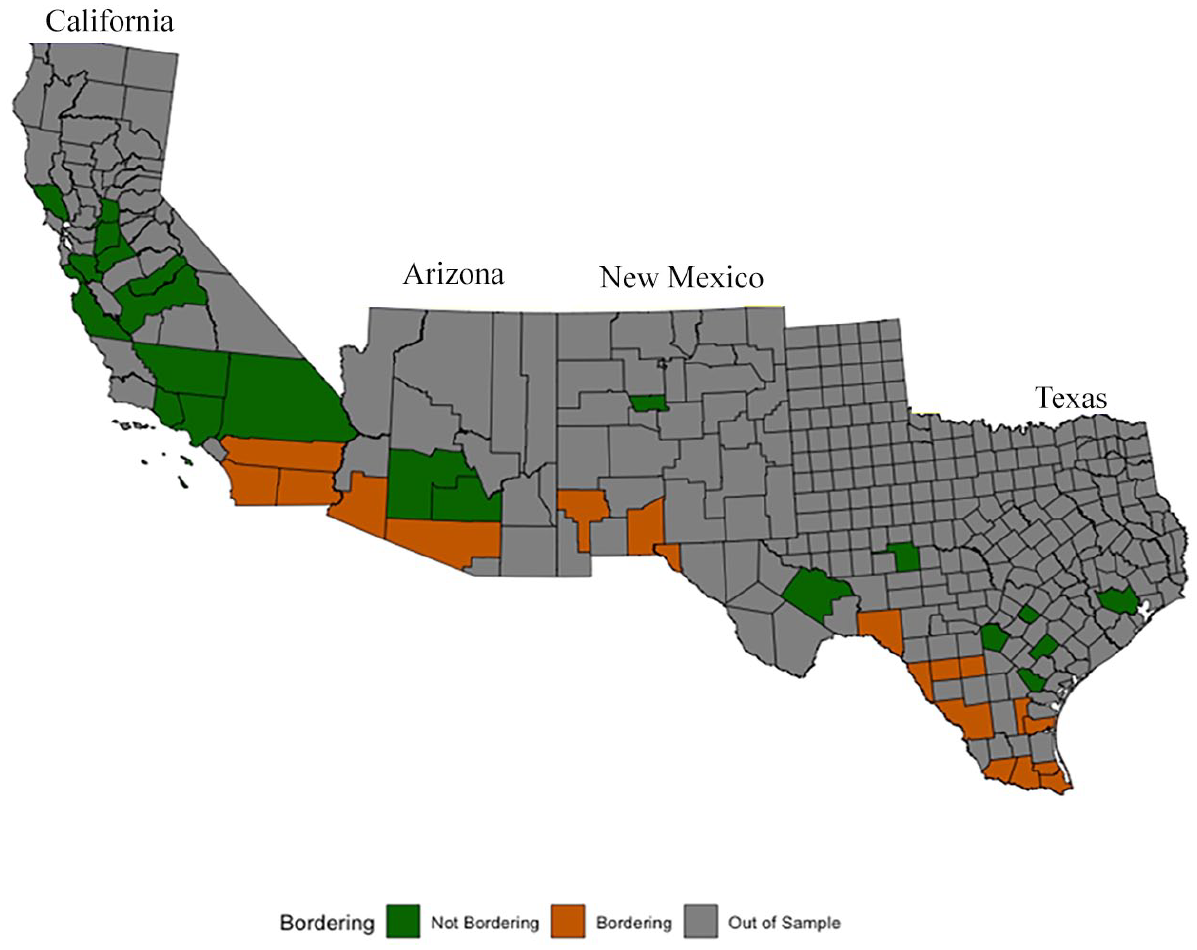
Counties by border status.
To complement the HEPESE data, we use data from the ACS (2011–2022), accessed from the U.S. Census Bureau via IPUMS (Ruggles et al., 2024). We restrict the ACS to Hispanic adults aged 80 years and older (n = 1,679,872), providing us with a comparison sample representative of all 50 states over a period of 10 years.
The key variables of interest represent health outcomes associated with difficulties faced by older adults and include the following:
Activities of Daily Living (ADL): tasks that individuals perform daily to maintain personal health and well-being such as dressing, bathing, toileting, and eating (Kim, 2021). We use the variable Total ADL, which sums the number of seven basic activities for which the respondent either reports they are unable to do or need help. The ADL index ranges from 0 to 7 (higher scores imply higher need for support).
Social Support: respondents were asked how often they can count on at least some of their family or friends in times of trouble. The social support index ranges from 1 to 4.
Emotional Support: respondents were asked how often they can talk about their deepest problems with at least some of their family or friends. The emotional support index ranges from 1 to 4.
Instrumental Activities of Daily Living (iADL): more complex tasks necessary for independent living like managing finances, transportation, shopping, preparing meals, and managing medications (Kim, 2021). The IADL index ranges from 1 to 10.
Self-reported help: self-reported health, with a range from 1 to 4 (poor, fair, good, excellent).
Number of minutes spent walking: reported number of minutes spent walking on each occasion.
BMI: body mass index, a measure of body fat based on height and weight, with a higher BMI indicating poorer health.
Financial Difficulty: reported financial difficulty meeting monthly bills, with a range from 1 to 4 (none, a little, some, a great deal).
Mental Incapacitation: reported reason for proxy interview because of mental incapacitation (Alzheimer’s or Dementia).
Alzheimer’s Disease or related Dementias (ADRD): respondent has been diagnosed by a physician for Alzheimer’s disease and related dementias.
We also use individual-level demographic controls in our regression models, including age in years (continuous), an indicator for female (1 = female; 0 = male), and indicator for living alone (1 = lives alone; 0 = no), and an indicator for U.S. born (1 = yes; 0 = no).
We hypothesize the direction of the association to be positive between border status and all our outcomes of interest, but higher for financial strain and worse overall health given the existing disparities to economic and health support resources in the border region.
Analytic Approach
We first show summary sample statistics, stratified by county-level border status (Table 1). We use statistical tests to explore whether the differences between the groups are statistically significant. Then, to build on the bivariate analysis and to control for confounders, we estimate the below regression model:

We estimate OLS and logistic regressions (for binary outcome variables), where outcomeic represents the health outcome for an individual i, in county c, and state s. Borderingics is a binary indicator for whether the respondent i lived in a bordering county c, and state s. A statistically significant
Summary Statistics of Mexican American Older Adults by Bordering County (HEPESE Waves 8–9, 2011–2013, 2016).
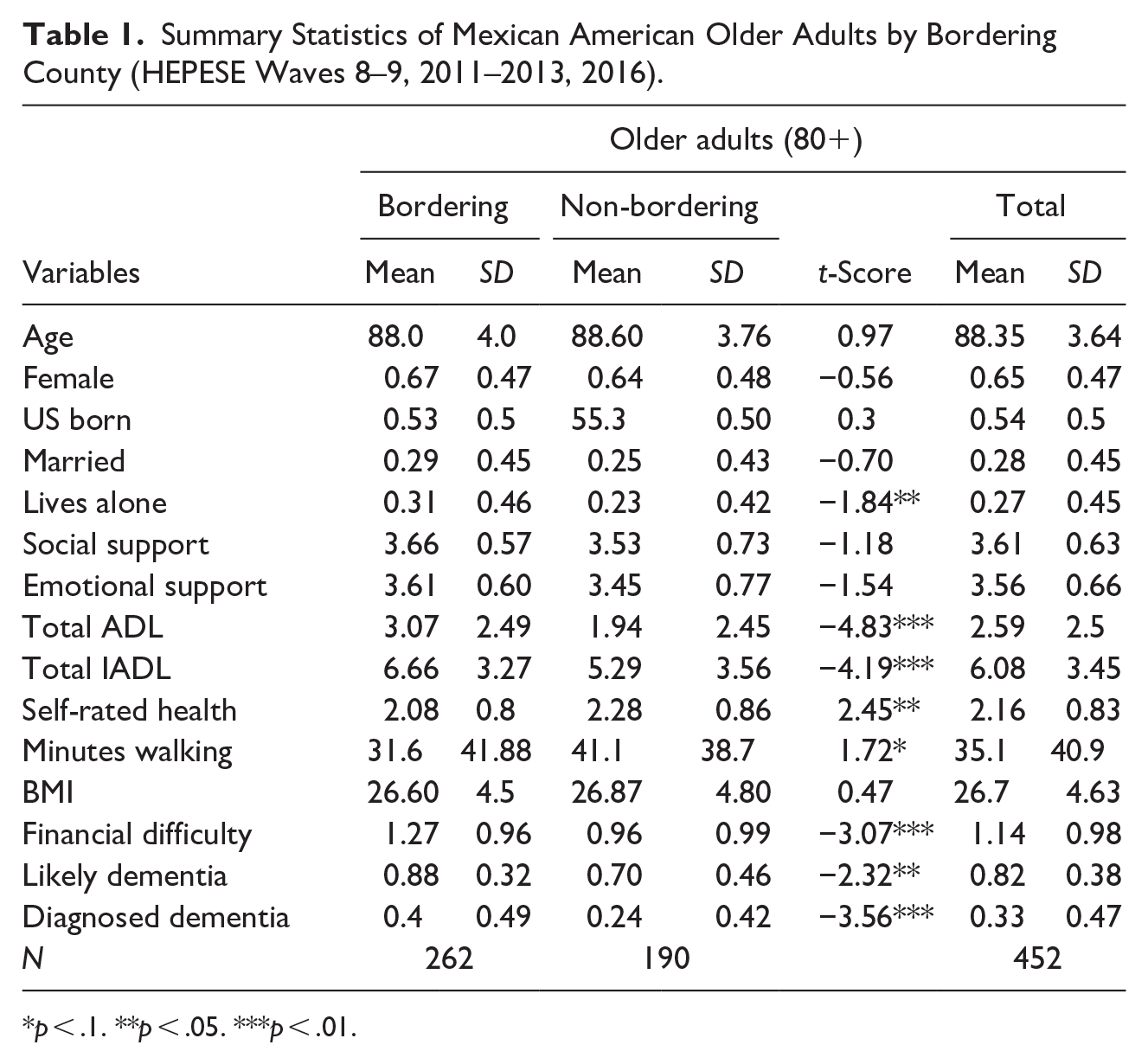
p < .1. **p < .05. ***p < .01.
The vector Xics represents individual-level demographic characteristics. The coefficients on State (
Results
Table 1 shows summary sample statistics and tests of statistical significance by bordering county status. Demographically, the average age is 88 years old, with no significant difference between those residing in bordering counties and those in non-border counties. Similarly, the proportions of U.S. born residents and respondents who identify as female are not statistically different between both samples. Respondents in border counties are more likely to live alone (31%) compared to those in non-bordering counties (23%), a statistically significant difference. Similarly, respondents living in border counties report having higher levels of emotional and social support than those in non-bordering counties, although neither difference is statistically significant.
In terms of ADLs, there is a sharp difference between those in bordering and non-bordering counties. Those in bordering counties reported a statistically significant difference in the need for assistance of an average of 3.07 activities, compared to 1.94 for those living in non-bordering counties. A similar significant result is shown with iADLs, where those in bordering counties require assistance for an average of 6.66 activities, while those in non-bordering counties require assistance for an average of 5.29 activities.
Overall self-reported health is lower (2.08/4) for those in bordering counties compared to those in non-bordering counties (2.28/4). Similarly, bordering residents reported walking an average of 31.6 min compared to 41.1 min for those in non-bordering counties, a significant difference that is a predictor of worse health outcomes. Financial difficulties are also significantly higher in bordering counties (1.27/4 in border counties, relative to 0.96/4 in non-border counties). Examining dementia measures, we report two different measures that show similar trends, but different results. The first, Likely Dementia measure, is based on a question of whether the respondent needs a proxy to participate in the HEPESE survey due to ADRD. We take this measure as a revealed need for care, where 88% of respondents in bordering counties require that assistance, compared to 70% of those in non-bordering counties. In regard to a stated need for care, the Diagnosed Dementia question directly asks respondents if they have been diagnosed dementia by a physician. This result is also large and significantly higher for those in bordering counties (40%) compared to non-bordering counties (24%). We use both measures to account for differences in measurement errors that could arise from either of the questions, but in both cases, it is evident there is a disparity between those in bordering and non-bordering counties.
Overall, in all the health outcome measurements we track using the HEPESE survey, those in bordering counties have higher vulnerability and worse outcomes that those in non-bordering counties. Figure 2 illustrates the correlations between the key variables of interest for the full sample. Emotional support and social support are positively correlated, while higher levels of these indicators are negatively correlated with higher scores of total ADL and iADL. Similarly, better results in self-rated health and minutes walking also correlate negatively with total ADL and iADL, while financial difficulties are negatively correlated with both social support and emotional support. The strongest correlations we found relate to the likely dementia and diagnosed dementia variables, which correlate higher with higher needs in total ADL and iADL.
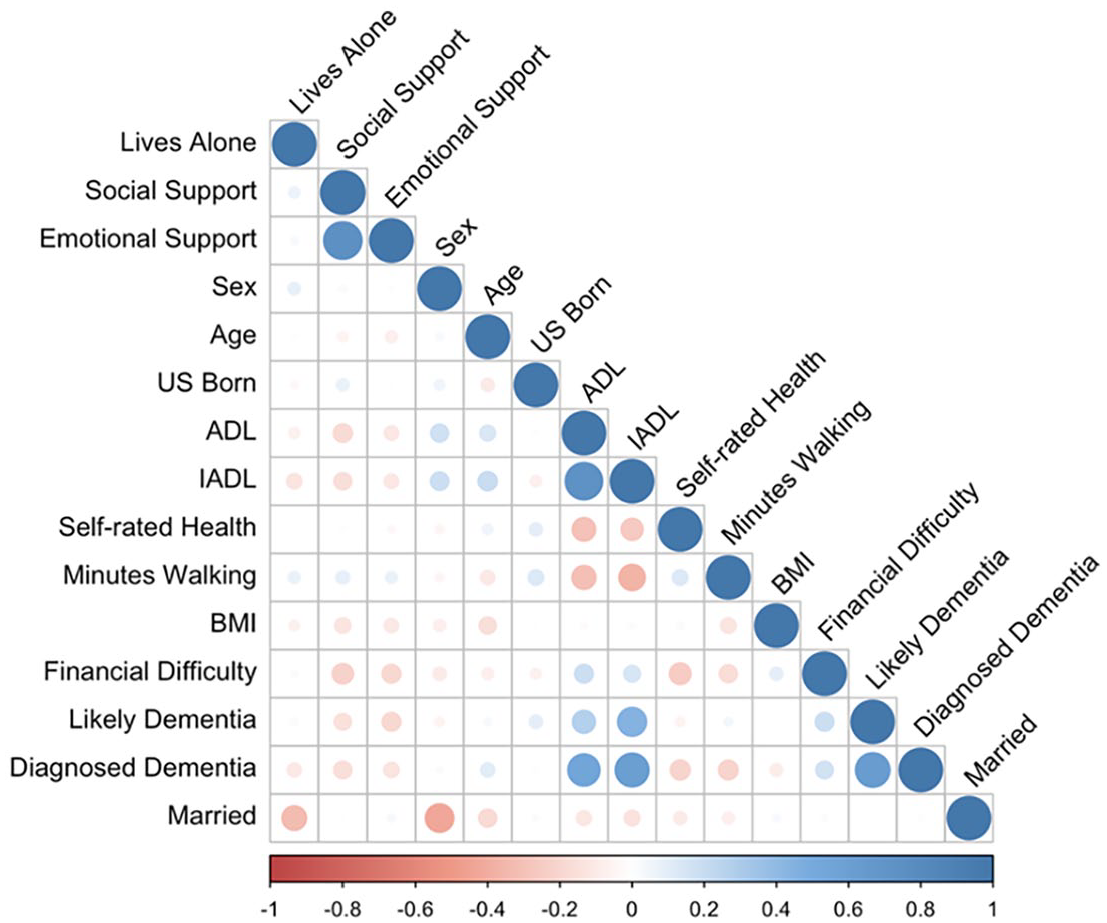
Correlation matrix of Hispanic older adults, HEPESE, Waves 8–9.
In Table 2, we contrast these results with demographic measures obtained from the ACS, stratified by bordering status.
Summary Statistics by Bordering States, Older Adults National Sample.
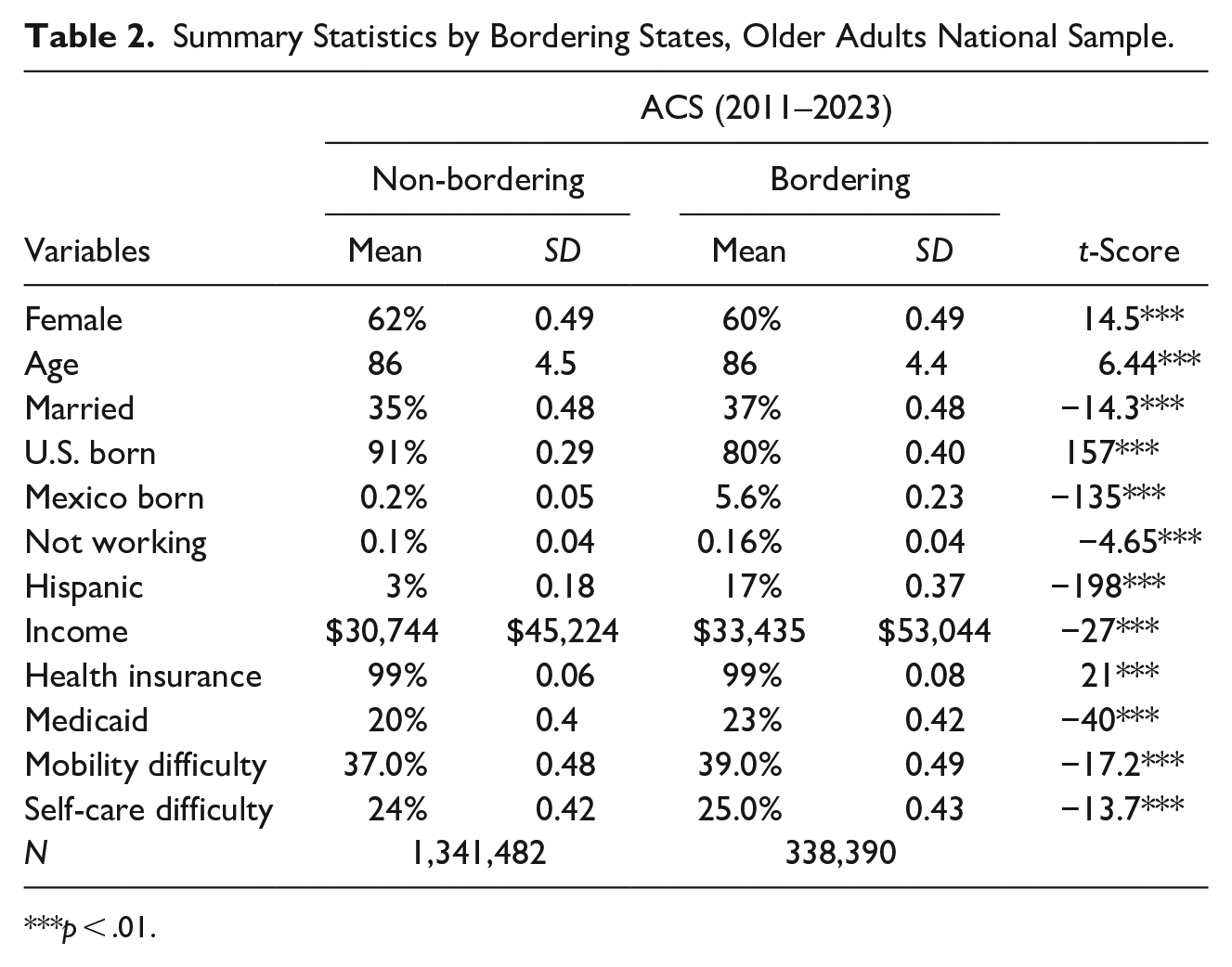
***p < .01.
When comparing general demographic characteristics of older adults who live in bordering states to those who do not live in bordering states, we find notable differences. There is a higher proportion of Hispanics, higher percent with mobility difficulties, and a higher proportion of those reporting self-care difficulties in border states. Regarding nativity status, major differences are found; 91% of those in non-bordering states report being U.S. born compared to 80% in bordering states, a significant difference. Similarly, 0.2% of those in non-bordering states report being born in Mexico compared to 5.6% of those in bordering states, a proportion 28 times higher between the groups. These results suggest the role of multi-layered disparities at the national level: those in bordering states have worse outcomes than those in non-bordering states, and within the bordering states, those in bordering counties have worse outcomes than those in non-bordering counties.
We also explore the relationship between bordering counties and key health outcomes using regression analyses. Table 3 shows the fixed-effects regression results, revealing that proximity to the border is associated with ADL, IADL, exercise, and diagnosed dementia outcomes after controlling for demographic variables and clustering standard errors. We expect these relationships to be more robust than the exploratory summaries presented in the previous tables. In addition, we run a sensitivity analysis with alternative definitions of border proximity, by changing the threshold from 0–100 miles to 0–62.5 miles, 1 0–50 miles, and 0–25 miles in different specifications.
Regression Model Results for Health Outcomes by Distance Specification.
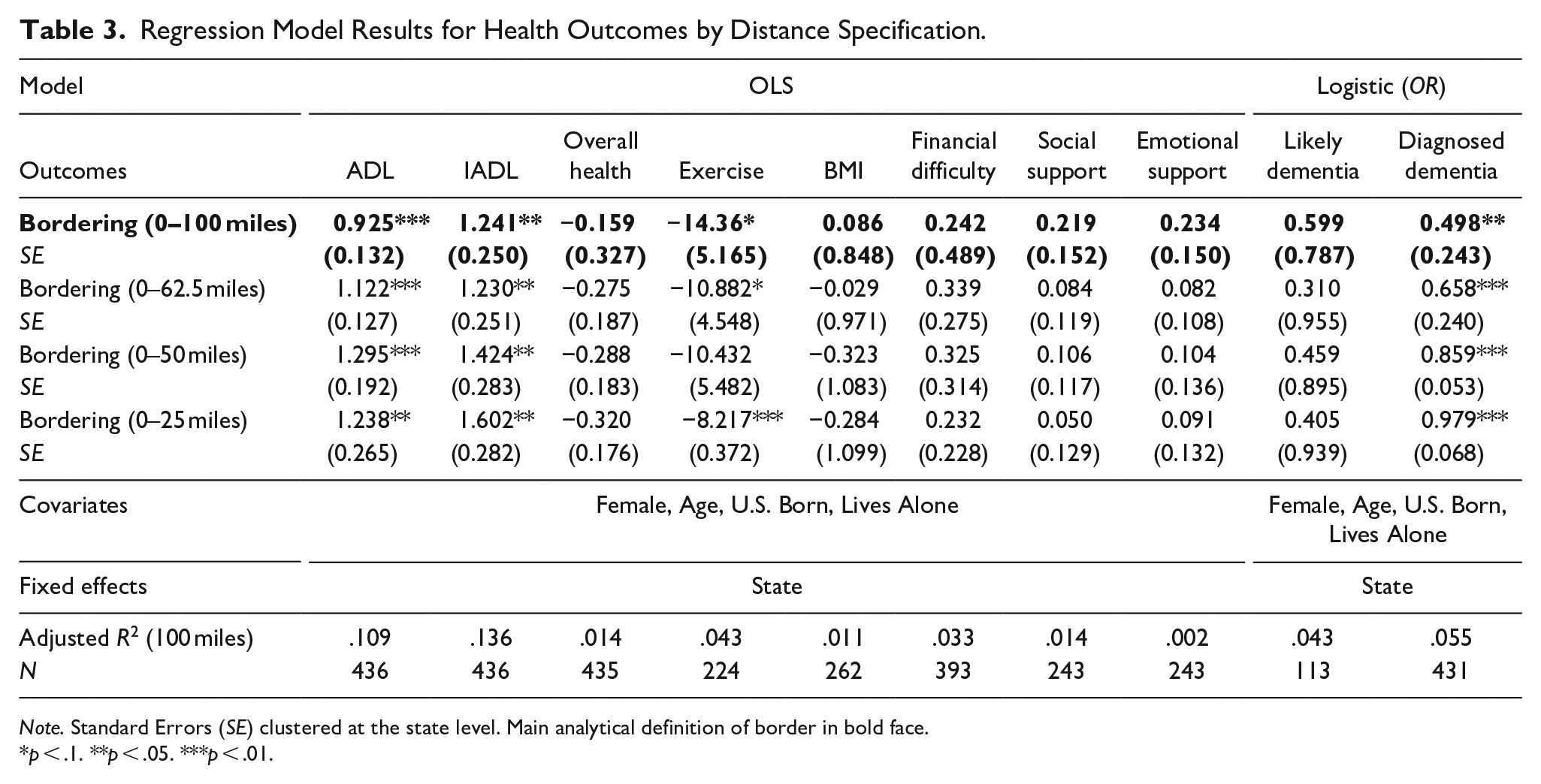
Note. Standard Errors (SE) clustered at the state level. Main analytical definition of border in bold face.
p < .1. **p < .05. ***p < .01.
We find that regardless of the definition of a bordering county, in all cases the results for ADL and IADL imply that those residing closer to the border require higher assistance on average than those in non-bordering counties. The 100 miles border specification is associated with an increase of 0.79 in the ADL index (out of 7) and an increase of 1.05 in the IADL index (out of 10). The stricter the border definition, the higher the association between both ADL and IADL, which emphasizes that the existing health disparities are moderated by proximity to the border.
In terms of exercise, we find that individuals in border counties walk significantly less than those in non-border counties—14.36 min less using the 100-mile definition, 10.88 min less using the 62.5-mile definition, and 8.22 min less using the 25-mile definition. For levels of social support and emotional support, living in a bordering state is correlated with an increase in both measures, although these relationships are not statistically significant.
Regarding measures of dementia, we were only able to corroborate the bivariate analysis of the relationship between distance to the border and diagnosed dementia, but not for likely dementia. The coefficient for diagnosed dementia gets larger as the distance threshold gets smaller, suggesting stronger effects closer to the border. For example, under the 100-mile definition, the odds of being diagnosed with dementia among older adults are 50.2% lower, relative to older adults living more than 100 miles from the border. For the 62.5-mile definition, the odds are 34.2% lower (relative to more than 62.5 miles), 14.1% lower for the 50-mile definition (relative to more than 50 miles), and 2.1% lower for the 25-mile definition (relative to more than 25 miles), all statistically significant. These findings suggest a protective “distance gradient” in dementia diagnosis, where the odds of being diagnosed with dementia decrease significantly as distance from the border increases. With regards to likely dementia, the much smaller sample size (n = 113) compared to diagnosed dementia might explain the null findings.
However, it is important to note that this pattern might reflect healthcare access disparities rather than actual dementia prevalence. For example, individuals living closer to the border may have different patterns of healthcare access, including diagnostic resources, language barriers, or cultural attitudes toward seeking care. Taken together, these results suggest that proximity to the border significantly increases the odds of diagnosed dementia, potentially due to variations in healthcare access, diagnostic practices, or other contextual factors. Moreover, the lack of significance for likely dementia warrants further investigation to understand these dynamics more fully. One caveat is that a small number of respondents (26%) get asked this question (only those who are unable to respond to the survey).
Discussion
The findings presented in this study highlight significant disparities in health outcomes for Hispanic older adults residing in the U.S.-Mexico border region. From a bivariate analysis, there is a higher proportion of older adults living alone, higher needs in activities of daily living (ADL), instrumental activities of daily living (iADL), worse self-rated health, less minutes of exercise, more financial difficulties, and higher percentages of both likely dementia and diagnosed dementia. Furthermore, for the multivariate analysis we provide evidence of these disparities across various health indicators, including activities of daily living (ADL), instrumental activities of daily living (iADL), minutes of exercise, and diagnosed dementia. The results, which reinforce previous findings using earlier waves of the HEPESE data (Salinas et al., 2013) underscore the urgent need for targeted policies and health equity initiatives to address the unique challenges faced by older Hispanic adults with ADRD, which get compounded by the challenges of providing caregiving to older adults in underserved and marginalized communities.
The disparities observed in ADL and IADL among Hispanic older adults in bordering counties compared to non-bordering counties are particularly concerning, given the documented correlation between ADL and IADL abilities and quality of life, especially among older adults (Dahlin-Ivanoff, 2016; Gao et al., 2022). The higher need for assistance in daily activities suggests that older adults in these regions face greater functional limitations, which can significantly impact their quality of life. These findings align with previous research indicating that social determinants of health, such as socioeconomic status, access to healthcare, and community support, play a crucial role in shaping health outcomes, especially when intersected with access to health insurance and caregiving (Perez et al., 2022). The lower self-reported health and reduced mobility among residents in bordering counties further highlights the compounded, cumulative disadvantages faced by this population. The significant difference in walking time between bordering and non-bordering counties is indicative of the broader environmental and infrastructural barriers that limit physical activity and, in effect, contribute to adverse population health outcomes (Jiang et al., 2022).
Dementia and Cognitive Health
The regression results corroborate the relationship between diagnosed dementia, distance from the border, and cognitive health, even if for likely dementia we only observe differences in the bivariate analyses. These higher rates of diagnosed dementia in bordering counties suggest that older adults in these regions are at a greater risk of cognitive decline. This disparity may be attributed to several factors, including limited access to healthcare services, lower socioeconomic status, and higher levels of stress associated with living in a border region (Brady et al., 2023; Carvajal et al., 2013; Duenas et al., 2022). The significant association between residing in a bordering county and the likelihood of a dementia diagnosis, especially under stricter definitions of bordering, underscores the need for targeted dementia care interventions. Furthermore, family structure and sources of support appear to be associated with better health outcomes. Following the dementia care model, these interventions require not only individual level variables such as household self-care and early detection, but community and societal domains of intervention, such as support for families coping with the demands of dementia caregiving, community resource policies, language-appropriate caregiving assistance, and improved public health insurance delivery. Most importantly, research on alternative and innovative options for care is necessary, as well as policies that support families and caregivers, given their association with increased levels of instrumental and emotional support for older adults in the border.
Limitations
This study has several important limitations to consider. First, both datasets we use (HEPESE and ACS) are cross-sectional, which prevents us from making causal inferences about the relationship between border proximity and health outcomes. Longitudinal data would provide greater insight into how proximity to the U.S.-Mexico border is associated with health trajectories, even at the descriptive level. Second, the HEPESE sample does not include respondents from every county within border states, potentially limiting the generalizability of our findings to all border regions, particularly for areas with distinct demographic or socioeconomic characteristics. Finally, comparability between our two data sources is limited by their different population coverage: while the HEPESE specifically samples Mexican-Americans, the ACS includes the broader Hispanic-American population that may differ systematically from the Mexican-American population, potentially masking important subgroup differences. We suggest these areas for future research to improve our understanding of the relationship between border proximity and health outcomes.
Policy Implications
Addressing the health disparities identified in this study requires a multifaceted policy approach that considers the unique needs of Hispanic older adults in the border region, with a special focus on those living with dementia. These actions should be coordinated directly with organizations such as the Area Agencies of Aging in Texas, which provides care coordination, caregiver support services, benefits counseling and focus on those with greatest economic and social need (Texas Health and Human Services, 2024). Previous research has also outlined key policy recommendations (Prince et al., 2016) which can be summarized as follows:
Improving Access to Primary Care: Expanding access to affordable healthcare services is critical. Dementia is currently under-detected, under-diagnosed, and under-treated in primary case (Mitchell et al., 2011). Physicians need training and in-service education to improve their screening capabilities.
Enhancing Community and Family Support: Strengthening community support networks is essential for improving health outcomes. Policies should focus on funding community-based programs that provide social support, health education, and aging resources for older adults and their caregivers. Innovative mechanisms to support families coping with a dementia patient are necessary.
Culturally Competent Caregiving: caregivers must be trained in culturally competent care to effectively address the unique needs of Hispanic older adults. This includes understanding cultural attitudes toward aging and dementia, language barriers, and the importance of family involvement in care.
Economic Support: Addressing the economic challenges faced by older adults in border regions is crucial. Policies should aim to reduce financial barriers to healthcare, increase access to public insurance programs, and provide financial assistance for those with limited incomes.
Environmental and Infrastructure Improvements: Enhancing the built environment to promote physical activity and mobility is vital. This includes improving sidewalks, parks, and public transportation to make it easier for older adults to engage in physical activity and access healthcare services.
Promoting health equity for Hispanic older adults in the border region requires addressing the root causes of health disparities. This involves a commitment to social justice and the recognition that health is influenced by a wide range of social, economic, and environmental factors. Key health equity strategies from the Healthy People 2030 initiative (U.S. Department of Health and Human Services, 2024), adapted to address Hispanic health disparities, include:
Addressing Social Determinants of Health: Policies must address the broader social determinants of health, such as education, housing, and employment, which significantly impact health outcomes. This includes initiatives to improve educational opportunities, increase affordable housing, and create job opportunities in border regions.
Reducing Health Disparities: Efforts to reduce health disparities should focus on targeted interventions for high-risk populations. This includes programs that specifically address the needs of Hispanic older adults, such as dementia care, chronic disease management programs, and mental health services. The example of Mexico provides a helpful reference in a similar region with comparable demographics (Rojas Alvarez et al., 2022).
Promoting Inclusive Research: Research on health disparities should include diverse populations and consider the unique experiences of Hispanic older adults in the border region. This includes collecting qualitative and quantitative data on social determinants of health, cultural factors, and barriers to care to inform evidence-based policy decisions.
Advocacy and Policy Change: Advocacy efforts are essential for driving policy change and promoting health equity. This includes engaging with policymakers, community leaders, and stakeholders to raise awareness of the health disparities faced by Hispanic older adults and advocate for policies that address these disparities.
The disparities in health outcomes for Hispanic older adults in the U.S.-Mexico border region highlight the urgent need for targeted policy interventions and health equity initiatives. The findings of this study underline the importance of a comprehensive and inclusive approach to health policy that considers the unique needs of Hispanic older adults in the border region, particularly those suffering from dementia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the National Institute on Aging at the National Institutes of Health (R01 AG10939) and the UTEP FIRST Grant at the National Institutes of Health(1U54CA280922-01).