
Abstract
The capabilities approach is useful for evaluating progress toward the just city. We report how a Participatory Action Research consortium studying neighborhood change and well-being designed a survey instrument measuring respondents’ ability to fulfill a set of common life priorities. We present data on priority endorsement and fulfillment, and conduct a factor analysis to explore the underlying structure of the instrument. We argue that the instrument operationalizes the capabilities approach and serves as a model for using participatory methods to evaluate the impact of planning interventions on social justice and health equity.
Introduction
To advance justice, planners need frameworks for evaluating whether and how planning processes and outcomes are just. In 2010, planning theorist Susan Fainstein developed a theoretical framework for “the just city” focused on three principles: equity, democracy, and diversity (Fainstein 2010). Fainstein observed that these principles often come into tension with one another in practice, and suggested that planners turn to the “capabilities approach” (CA) for guidance adjudicating between conflicting goals and principles in efforts to plan just cities (Fainstein 2010, 54). The CA is a philosophical framework for justice which posits that justice should be understood in terms of well-being and that well-being is determined by an individual’s freedom to do or be those things that they value doing or being, and thus the kind of life that they are able to lead (Nussbaum 2001, 2011; Robeyns 2016, 2017; Sen 1979, 2000).
Operationalizing the CA—a necessary step for application in planning practice—is notoriously challenging because the freedom to do or be something is difficult to measure (Nussbaum 2011, 62; Shinn 2015). As of yet, there have only been a handful of attempts to operationalize the CA to evaluate interventions into the built and social environments of cities and their effects on the well-being of affected communities (e.g., Frediani and Hansen 2015). Nevertheless, there is support for the case that the CA can be operationalized in a participatory manner, rooted in Sen’s argument that which capabilities matter in any context ought to be the outcome of public reasoning (Clark, Biggeri, and Frediani 2019; Sen 2000).
This paper reports how community residents and academic researchers collaboratively operationalized the CA as part of a larger, long-term Participatory Action Research study investigating the relationship between urban development and health in nine Boston-area neighborhoods experiencing increased investment in transit-oriented development real-estate projects (Arcaya et al. 2018). First, we explain the CA and review how planners have used the CA to date. Then, we describe how our study team developed a survey instrument that we argue partially operationalizes the CA: a “prioritization inventory” that assesses an individual’s priorities and their ability to fulfill those priorities that are of most importance to them. We present data from the prioritization inventory gathered via a community survey and conduct an exploratory factor analysis to understand the underlying constructs measured by the instrument.
We argue that the prioritization inventory partially operationalizes the CA by measuring the extent to which individuals have the freedoms in place to fulfill priorities that they value. Using our tool to operationalize the CA affords planners a means to better understand well-being, and design and evaluate planning processes (e.g., community engagement), interventions (e.g., climate adaptation), and policies (e.g., rent control) in terms of the extent to which they enhance the capabilities of disadvantaged populations and thus make cities more just.
Measuring Well-Being Via the Capabilities Approach
The CA was introduced by economist Amartya Sen (1979) in response to shortcomings he perceived in utilitarian and Rawlsian theories of justice, both of which have informed contemporary notions of justice in planning (Reece 2018; Steil and Connolly 2009). First, Sen argued that the utilitarian emphasis on equality of marginal utility as the basis of justice was insufficient because it ignored differences in levels of disadvantage and intensities of need. Then, he argued that Rawls’s (1971) framework of justice makes the mistake of being “concerned with good things rather than what these good things do to human beings” (Sen 1979, 219). He insists that Rawlsian justice also renders disadvantage irrelevant, assumes that people’s needs are fundamentally similar when in reality they are fundamentally diverse, and ignores the importance of happiness and desire-fulfillment.
Sen (1979) contends that a notion of basic capabilities, or some reflection of a person’s ability to do basic things that they value, is necessary for a theory of justice. Focusing on capabilities shifts the locus of justice from goods themselves to what goods enable for human beings, he argues, which is necessary because the conversion of goods to capabilities varies substantially from person to person (Sen 1995a). Sen (1995b, 2000; 2004a, 2004b, 2005) subsequently developed the framework that has come to be known as the “capabilities approach.” His work has been complemented and further developed by philosopher Martha Nussbaum, who has sought to refine the CA for application in human development (Nussbaum 2001, 2002, 2003, 2006, 2013).
The CA has two central concepts: functionings and capabilities (Sen 1979). Functionings are the various things a person may value doing or being, which may range from meeting basic needs like food and shelter to experiencing complex psychosocial states like a sense of belonging or leadership. Capabilities are a person’s real freedoms to achieve those functionings that they value (Hick 2012; Sen 1979, 2000). For example, if learning to play the piano is a functioning that someone values, the capabilities required to do so may include access to a piano, time and space to practice, and/or the availability of instruction. As a framework for evaluation and comparison, the CA thus offers both a metric of achieved well-being, in the form of functionings, and a metric of the freedom to pursue well-being, in the form of capabilities (Robeyns 2016).
Applying the Capabilities Approach to Urban Planning
In developing her concept of the “just city,” Fainstein (2010) argues that the basic elements of justice are democracy, equity, and diversity, but shows that there are tensions between these values that planners must navigate. The CA, she suggests, is well suited to (1) figuring out how to apply these norms within particular contexts to realize the just city, and (2) evaluating plans, policies, and programs from the perspective of whether the outcomes enhance the capabilities of the relatively disadvantaged. She argues that the CA is “the most fruitful of the various philosophical strategies regarding justice applicable to urban governance” (Fainstein 2010, 54). Similarly, Deneulin (2014) has suggested that the concept of the “right to the city” can be understood in terms of the CA, and argues that the CA can make important contributions to right to the city movements, including improved tools for well-being evaluation and a better understanding of how different dimensions of well-being positively or negatively affect each other.
The CA can help planners shift their focus from understanding justice in terms of how spatial goods are distributed, to whether the distribution of spatial goods makes people more capable of realizing functionings that they value and which respond to their demands for justice (Basta 2016; Mukhija and Takahashi 2022). The CA also affords planners the ability to sustain plural conceptions of justice when evaluating whether processes and outcomes are just, which is advantageous in diverse contexts. The key insight from the CA for planners is that it is not spatial goods themselves that guarantee well-being and equality of opportunity, but what these goods do for those they are provided to.
Scholars are beginning to apply the CA to evaluate progress on planning-related issues such as housing, transportation, and community development. For example, Frediani (2019) has applied the CA through participatory methods to examine the impact of squatter upgrading initiatives on residents’ “housing functionings” in Brazil. Fennell et al. (2018) use the CA to put forward a model of urban inclusion to guide housing policy, encouraging planners to distinguish between shelter as a good, on one hand, and on the other hand the act of habitation as mediated by built structures, and to focus on the latter to ensure well-being. Other recent applications of the CA in planning scholarship include Zitcer, Hawkins, and Vakharia’s (2016) use of the CA to understand the contribution of arts and culture to community development, Hananel and Berechman’s (2016) framework for incorporating the CA into transportation planning to reach more just outcomes, Doussard and Yenigun’s (2022) use of the CA to offer solutions to longstanding problems in economic development, and Mukhija and Takahashi’s (2022) use of the CA to show how housing interventions can improve health. All of these scholars have suggested that the CA can help planners extend the impact of their investigations or interventions to ensure that spatial goods expand the capabilities of residents in ways that allow them to achieve functionings of value and achieve greater well-being.
Allied fields have also made progress incorporating the CA as a normative and empirical tool for understanding when harm and injustice occur, how justice can be attained, and how doing so can advance well-being. For example, environmental justice scholars have advocated for the use of the CA as a conceptual tool to expand the field’s notion of justice beyond the distributional concerns in which the field has its origins, and posit well-being as the ultimate goal of environmental justice (Edwards, Reid, and Hunter 2016; Schlosberg 2007; Walker 2009). Moreover, they have argued that the CA is useful in helping to know when and how different environmental outcomes should be understood as injustice, and how to accommodate pluralistic justice claims made in everyday practice across grassroots environmental justice movements.
Following Sen’s (2002) argument that health equity should be understood in terms of capabilities, scholars in health-related fields have employed the CA with implications for how planners understand the relationship between health and place and our role in improving urban health equity. For example, Hopper (2007) argues that the CA enables researchers to account for the contextual dynamics of health outcomes, and R. G. White, Imperiale, and Perera (2016) observe that the CA can help health scholars consider how space and place can afford opportunities to enhance mental well-being. Whitehead and colleagues (2016) have used the CA to understand how lack of “control over destiny” underlies socioeconomic inequities in health outcomes. In community psychology, Shinn (2015, 247–48) has considered how settings such as neighborhoods can foster capabilities by acting as “mediating structures” between individuals and society, while others have operationalized the CA via participatory methods to measure community mental health (Sacchetto et al. 2018). Finally, we note that some approaches to planning for health equity, such as Trauma Informed Community Building, do not explicitly employ the CA but are nevertheless aligned with underlying tenets like fostering self-determination (Falkenburger, Arena and Wolin 2018; Reece 2020).
These developments provide important footholds for planners to extend the normative and practical application of the CA in the planning process. They show how planners could use the CA to understand when, how and for whom injustices arise during or as a result of planning processes, and what just outcomes might in turn look like; accommodate diverse conceptions of justice from different stakeholders in planning processes; assign value to agency and self-determination in efforts to build more just cities; and articulate well-being as a planning goal. Given the foundational link between well-being and justice in the CA, we see such contributions as particularly relevant for burgeoning efforts to use planning as a tool to achieve health equity (Corburn 2013).
One barrier to applying the CA to planning is the critique that the CA is overly individualistic and elides structural considerations. Fainstein (2010) responds by arguing that while the CA does emphasize the individual, it also understands individuals as existing within a network of social and emotional relationships, not as atomized entities whose freedom and well-being are independent of that of others. Others have argued that the CA’s focus on individuals should actually be understood as an emphasis on understanding justice and well-being in terms of agency (Fennell, Royo-Olid, and Barac 2018; Frediani 2010). The extent to which the CA is individualistic depends on how it is used, and numerous scholars have demonstrated the importance of understanding and collective capabilities (Alkire 2008; Evans 2002; Ibrahim 2017). Fainstein (2010) recommends that planners employ the CA via a communal ethic, and environmental justice scholars have similarly suggested that the CA should be extended to include functionings at the collective level (Schlosberg 2007; Walker 2009). A relational, communalistic application of the CA accommodates group-level desires to be free from racial or class-based oppression, to exercise self-determination, or to be safe from gender-based violence, for example.
The adoption of a communalistic ethic in relation to the CA is being advanced by a growing body of work that explores the relationship between participatory methods and the CA. Frediani, Clark, and Biggeri (2019) contend that participation has both intrinsic and instrumental value for the expansion of capabilities, and that the CA can contribute to the elaboration of what Paolo Freire (2000) called “critical consciousness,” an in-depth understanding of the world that fosters the confidence and ability to alter unjust conditions. Scholars working at the intersection of participatory methods and the CA have demonstrated that participation is a powerful means for identifying functionings that communities value and exploring the processes that shape the capabilities available to them (Clark, Biggeri, and Frediani 2019; Frediani 2010). In the “Discussion” section, we offer our own call for a relational and collective approach to applying the CA in planning practice.
Study Context: Rapidly Developing Neighborhoods in Metropolitan Boston
The Healthy Neighborhoods Study takes place in nine communities across the Boston metro area experiencing rapid real-estate development rippling out from transit hubs: the Boston neighborhoods of Roxbury, Dorchester, and Mattapan; and the cities of Lynn, Everett, Chelsea, Brockton, Fall River, and New Bedford (Figure 1). The study sites are places where large investments in transit-oriented development were expected to occur at the outset of the study in 2015, and were chosen via a multistep screening process based on built environment characteristics, urban development trends, and health outcomes (Arcaya et al. 2018). The nine study sites are all dense, socioeconomically marginalized, racially/ethnically diverse urban neighborhoods experiencing high real-estate development pressures, with socioeconomic change, gentrification, and displacement. In six of the nine study neighborhoods, the majority of the population are people of color. In all but one study neighborhood, the poverty rate is higher than the state average, and in three study neighborhoods, at least one in four residents live below the poverty line.
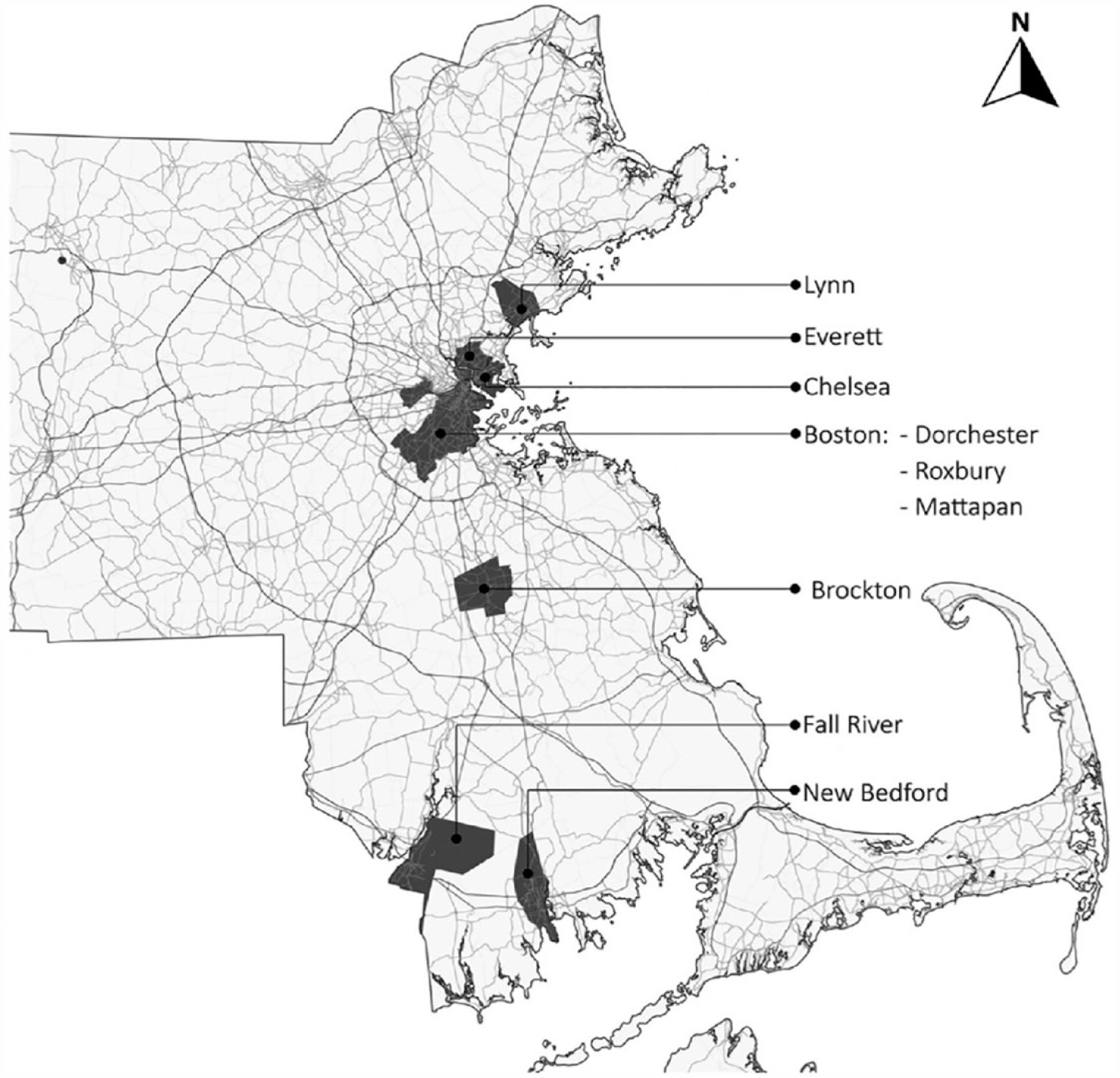
Healthy neighborhoods study sites in Eastern Massachusetts.
The Boston metropolitan area has witnessed significant economic and population growth in recent decades. Despite rapid real-estate development, the supply of affordable housing has not kept up with growth and remains inadequate, and the region is one of the country’s most expensive housing markets. Almost half of renters in Greater Boston are housing cost-burdened (Calef et al. 2022). High housing costs and economic inequality are contributing to financial insecurity and health risks among low-income residents (Arcaya et al. 2020; Binet et al. 2021). Housing and economic pressures are disproportionately severe for residents of color, racial residential segregation is persistent, and Boston’s racial wealth gap is among the widest in the nation (Calef et al. 2022; Muñoz et al. 2015).
Methods
In this section, we describe how community residents and academic partners collaborated to develop a survey tool to measure respondents’ current priorities in life and their perceived ability to fulfill them, as part of a broader Participatory Action Research study. These priorities represent a set of “beings and doings” that can be considered “central functionings” within the study communities.
The Healthy Neighborhoods Study PAR Approach
The Healthy Neighborhoods Study (HNS) is a multisite, longitudinal Participatory Action Research (PAR) study in the nine Boston-area neighborhoods described above (Arcaya et al. 2018). Our team has a broad multiyear (2015–present) research agenda exploring how experiences of neighborhood change affect community health and well-being (e.g., Arcaya et al. 2020; Binet et al. 2021, 2022). Through partnerships with community-based organizations in each of the nine study communities, the HNS is driven by a network of forty-five “Resident Researchers,” who are involved in all aspects of the research process, including study design, data collection, data analysis, knowledge dissemination, and community action (Binet et al. 2019; HNS 2020).
Resident Researchers are residents of the study communities who vary widely in age, background, life experiences, and familiarity with research. Resident Researchers are recruited by community partner organizations, trained in PAR methods and research ethics by academic members of the study team, and are registered as institutional review board (IRB)–approved study personnel. There are approximately four Resident Researchers for each of the nine study communities at a given time. Resident Researchers are paid a stipend of $20 per hour (increasing according to number of years as a Resident Researcher) and work approximately 175 hours per year across all HNS activities. In their own lives, all Resident Researchers are active in their communities, for example, through volunteering, community organizing, service provision, and/or program leadership. Resident Researchers have shared their experiences working on the HNS in a variety of public-facing blog posts (e.g., Morales 2021; Morris 2020; Seeder 2020).
A basic tenet of PAR is that measurements used to study people must be meaningful and useful to those people, and the only way to ensure this is to co-create the measures with the communities being researched (Minkler 2000, 2010). Thus, because a central aim of the HNS is to understand resident experiences of neighborhood changes, our research design is driven by Resident Researchers who are experiencing and trying to influence the changes we are investigating together. We do so via our collaborative research design process, which centers residents’ experiential knowledge and emphasizes reflexivity among community and academic participants, with the goal of building collective critical consciousness. This process is part of a cycle of inquiry, action, analysis, and reflection that our team conducts on roughly an annual basis (Figure 2). The process of developing these measures together has empowered Resident Researchers and community partner organizations to confidently use the data and knowledge they have generated to affect change in their communities in line with their values via community action projects undertaken as part of our PAR process. Indeed, Boni and Frediani (2020) have argued that aspects of PAR such as the development of collective awareness enhance participants’ capabilities.
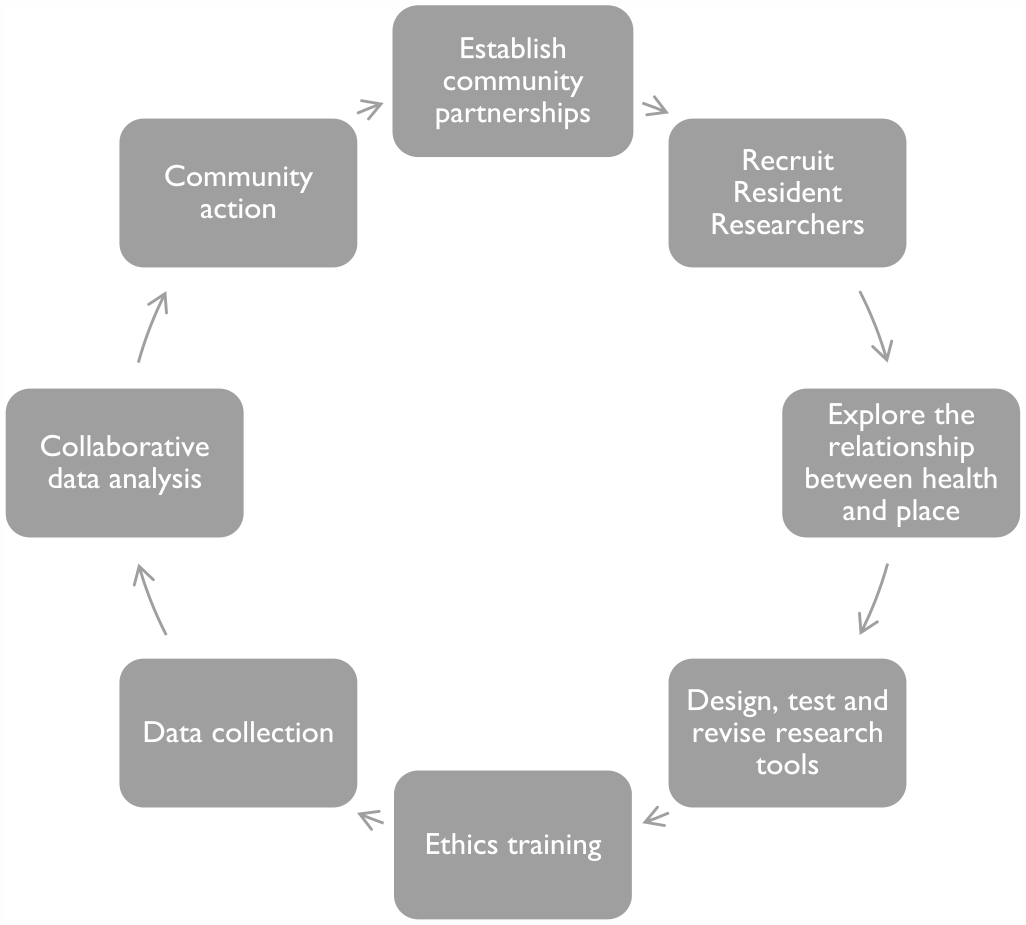
Healthy neighborhoods study Participatory Action Research (PAR) process overview.
Collaboratively Designing a Survey Instrument That Operationalizes the Capabilities Approach
Through a series of collaborative research design workshops, Resident Researchers designed a multidimensional survey instrument to explore salient connections between health and neighborhood change by employing or slightly modifying previously validated and reliable measures, and fielding new questions to attempt to capture constructs lacking strong precedents in the literature. The initial collaborative research design process consisted of five workshops, each three hours in length. Academic members of the study team facilitated the series of five workshops in each of the nine study sites across overlapping periods of six to eight weeks from March to August 2016. Each workshop had between four and eight participants comprising the Resident Researchers and community partner organization staff from that community. Workshops were typically held at the community partner organization’s office or at a nearby location with meeting space such as a library.
The first workshop focused on introducing participants to PAR and discussing core study themes (Figure 3). The second workshop focused on generating research questions and hypotheses about the relationship between health and place. The third workshop focused on identifying data that could be collected to answer questions raised by the team. The fourth workshop involved choosing previously validated measures or designing new measures for variables of interest, and the fifth involved finalizing new measures and making final revisions based on feedback from practice administering the survey. To facilitate the development of a common survey tool across each of the nine communities, during each workshop facilitators reported key ideas and contributions from other communities, and participants highlighted important points to convey about their own community’s conversations to participants in subsequent workshops.
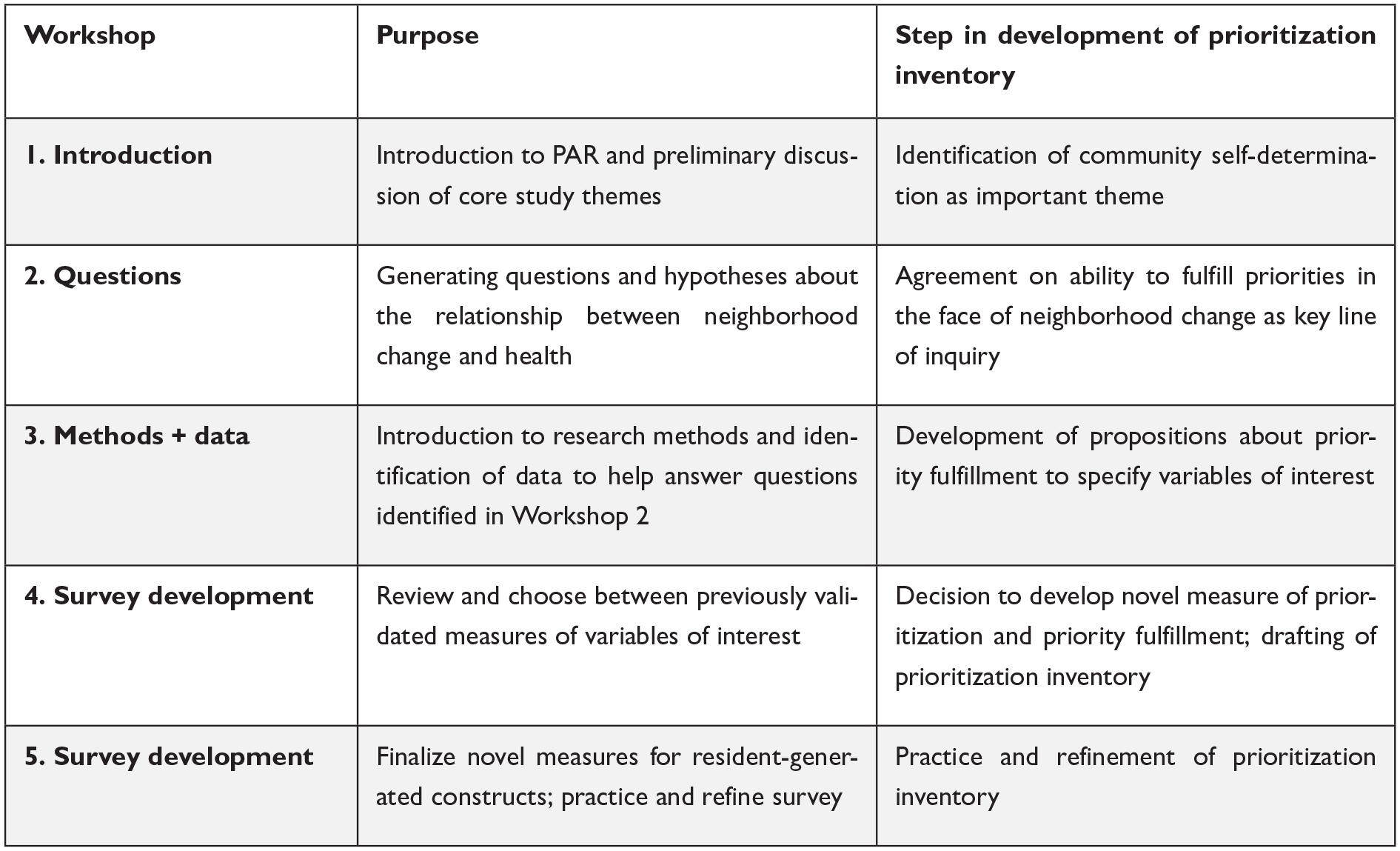
Developing the prioritization inventory through collaborative research design workshops in 2016.
A detailed description of our process for designing and facilitating this initial series of collaborative research design workshops, including sample facilitation guides and key lessons learned, has been published elsewhere (Binet et al. 2019). In subsequent years of the study, the collaborative research design process has been condensed to two to three workshops focused on revisions to data-gathering instruments and adjustments to community-specific sampling plans.
During the initial collaborative research design process, via reflective journaling and storytelling activities, Resident Researchers highlighted individual and community self-determination as important themes for this research. The group then pursued two lines of facilitated discussion on this theme. The first considered community residents’ sense of ownership over the changes taking place in their community (see Binet et al. 2022). The second line of conversation, which we focus on here, concerned individuals’ priorities in life, their ability to fulfill these priorities, and the ways in which their neighborhood helped or hindered their efforts to fulfill their own priorities.
Next, Resident Researchers, with support from academic and organizational partners, articulated three reasons it was important to study community residents’ priorities: (1) ability to fulfill one’s important priorities could be good for overall health; (2) sets of priorities likely vary over time and by age, place, and socioeconomic position, making it important to ask about priorities rather than assume residents were all pursuing the same things; and (3) intensive urban development and its consequences (such as displacement, cultural change, and changes in access to sources of social and material support) could affect residents’ ability to meet their stated priorities, with effects modified by individual-level characteristics. We report these propositions to disclose Resident Researcher motivations, but note that testing them as hypotheses is beyond the scope of this paper.
To gather data on resident priorities, the Resident Researchers constructed a “Prioritization” inventory to include as a part of the HNS community survey. This inventory was developed during collaborative research design workshops that included reviewing other scholarly attempts to measure what people valued, and whether they were able to achieve or otherwise have their desired outcomes (e.g. Rosenblatt and DeLuca 2012). Resident Researchers chose to write a survey question that could generate data on the range of priorities a respondent might have, how important each priority is at the time of the survey, and whether respondents are able to fulfill the priorities that are important to them. Resident Researchers collectively identified and agreed upon a list of seventeen priorities that members of their communities were likely to prioritize at some stage of their life. In 2018, after two rounds of data collection, Resident Researchers agreed to narrow the list of priorities down to thirteen to eliminate uncommon priorities and condense priorities with highly correlated responses, with the ultimate goal of reducing respondent burden.
The inventory asks respondents to indicate whether each priority is Most Important/Important/Not Important/Not applicable to them at this time. On all items marked Most Important or Important, respondents are also asked to indicate whether they currently feel able to fulfill this priority (Appendix A).
Data Collection
This analysis uses HNS survey data collected annually between 2016 and 2020 in the nine study neighborhoods. The HNS survey asks a range of questions developed by Resident Researchers in collaboration with other members of the HNS team to explore the relationship between urban development and community health; survey topics included demographic characteristics, household composition, housing tenure and history, neighborhood belonging, financial security, social support, health, food security, discrimination, prioritization, and ownership of change. To be eligible to participate in the survey, respondents needed to: be over the age of eighteen, reside in a study neighborhood, and be able to complete the survey in English or Spanish.
Because a central purpose of the HNS is to understand the impacts of transit-oriented development patterns on the health and well-being of preexisting neighborhood residents, data collection focused on those who live within a half-mile radius around a major public transit hub (i.e., train station or bus depot). Within study sites, we adopt a participatory heterogeneous purposive sampling approach based on locally variable definitions of what representativeness means (Arcaya et al. 2018; Shadish, Cook and Campbell 2002). Resident Researchers in each community work together to identify four population characteristics that they deem essential to ensuring representation of their community in the sample (e.g., age, race, language spoken at home, and neighborhood tenure). Then, they map where in the study site residents with different levels of the selected characteristics live. Within the areas identified on their maps, Resident Researchers reached respondents through a mix of door-knocking and convenience sampling at local events, parks, libraries, and businesses. Surveys typically take about twenty-five minutes to complete, and respondents were thanked for their time with a $20 gift card.
Analysis
Below, we present baseline data on respondents’ self-reported priorities as measured by the HNS prioritization inventory. First, we provide selected descriptive statistics on the analytic subsample of 2,564 HNS survey respondents from 2016 to 2020 who completed the entire prioritization inventory (Table 1), highlighting demographic, socioeconomic, housing, and health variables to give readers further context on the sample population, and because we conceptualize these variables as drivers of prioritization and priority fulfillment. We present sample sizes, means for all continuously measured variables, and frequencies for categorical data. We compare the sample characteristics with census data for the nine study sites. Details on the number of responses collected in each survey year and from each study community are provided in Appendix B.
Sample Characteristics.
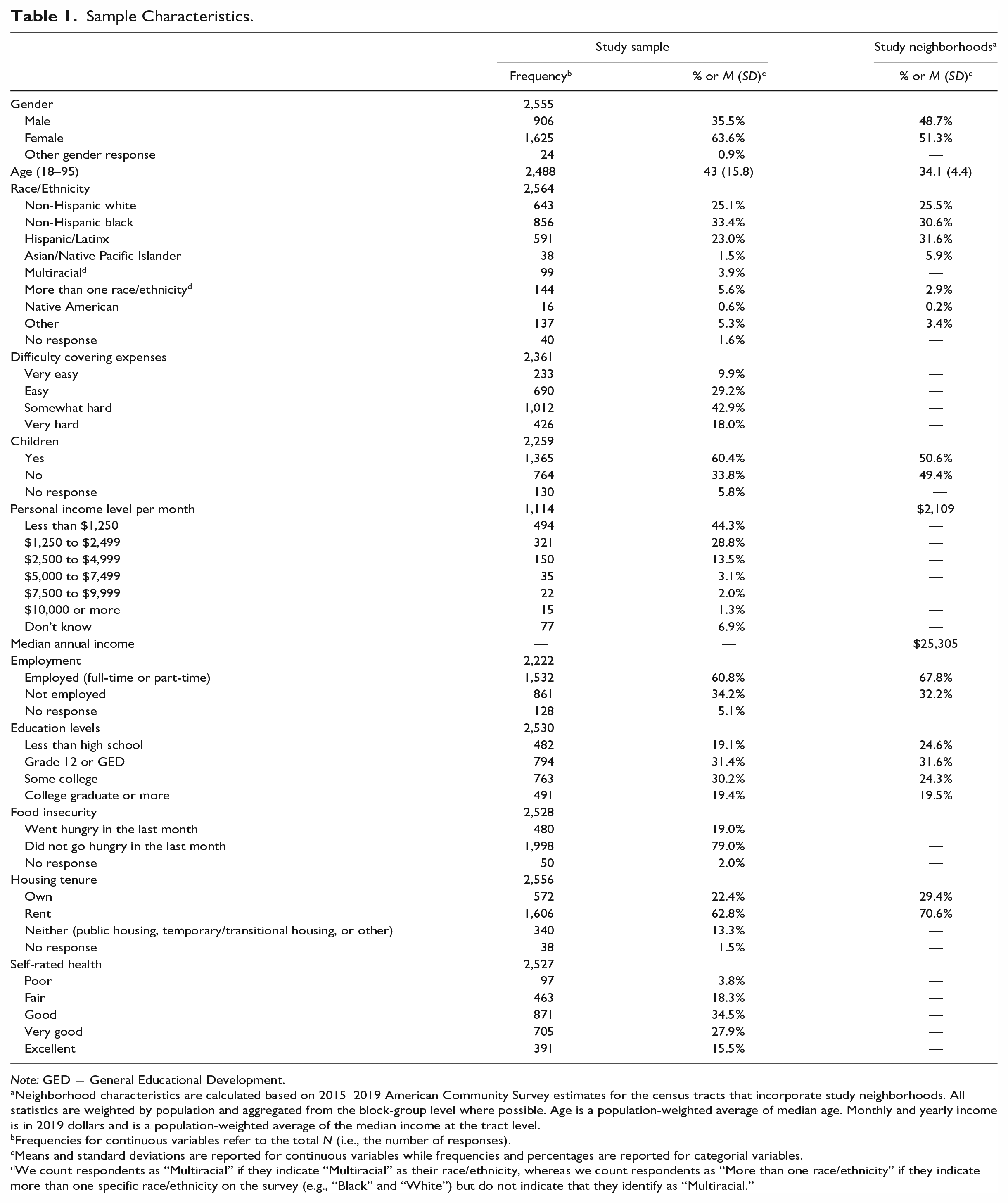
Note: GED = General Educational Development.
Neighborhood characteristics are calculated based on 2015–2019 American Community Survey estimates for the census tracts that incorporate study neighborhoods. All statistics are weighted by population and aggregated from the block-group level where possible. Age is a population-weighted average of median age. Monthly and yearly income is in 2019 dollars and is a population-weighted average of the median income at the tract level.
Frequencies for continuous variables refer to the total N (i.e., the number of responses).
Means and standard deviations are reported for continuous variables while frequencies and percentages are reported for categorial variables.
We count respondents as “Multiracial” if they indicate “Multiracial” as their race/ethnicity, whereas we count respondents as “More than one race/ethnicity” if they indicate more than one specific race/ethnicity on the survey (e.g., “Black” and “White”) but do not indicate that they identify as “Multiracial.”
To explore whether patterns of prioritization revealed underlying “central functionings” that were not measured directly, but which may explain why people who prioritize one item may also prioritize another, we used exploratory factor analysis to examine the factor structure of priority endorsement (Table 2). The factor structure represents the intercorrelations among variables, and groups of variables with strong intercorrelations are said to “hang together” to represent a factor. Factors indicate latent constructs measured by the group of variables that load on to that factor.
Polychoric Factor Loadings.
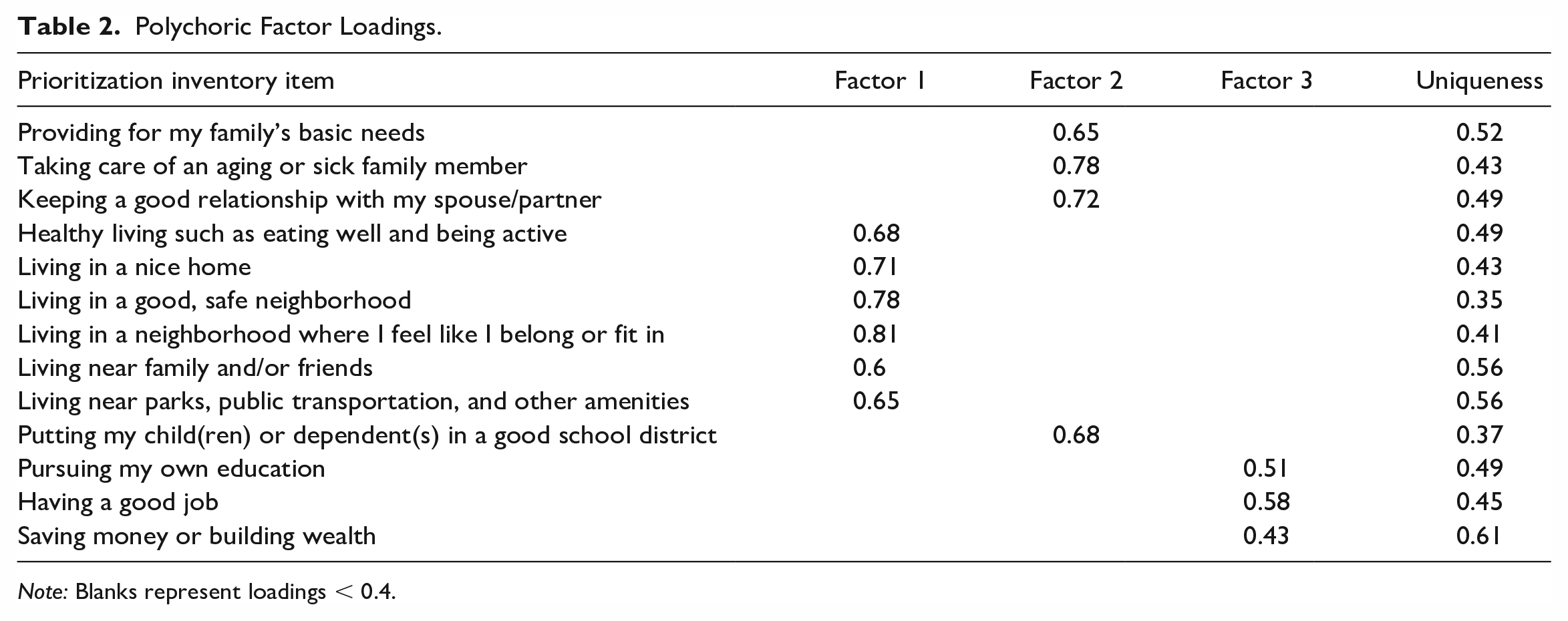
Note: Blanks represent loadings < 0.4.
We used a parallel analysis approach to determine how many factors were present in the data. Prior studies note that treating ordinal variables as though they were continuous facilitates the use of parallel analysis without sacrificing performance (Cho, Li, and Bandalos 2009), and that the final number of factors may be the estimated number plus or minus one, to be determined on the basis of interpretational validity (Lim and Jahng 2019). Finally, we used polychoric factor analysis to compute factor loadings and uniqueness for each item (Holgado-Tello et al. 2010). We employ promax rotation, which allows factors to be correlated, because our primary goal in this analysis was not to reduce the dimensions of our data for survey development purposes, but rather to substantively explore multivariate response patterns. Previous guidelines suggest that .32 is the lower bound for meaningful item loadings, which translates to roughly 10 percent overlapping with the other items in a factor in terms of variance (Costello and Osborne 2005; Tabachnick and Fidell 2007). To be conservative, we report item loadings of .4 and above.
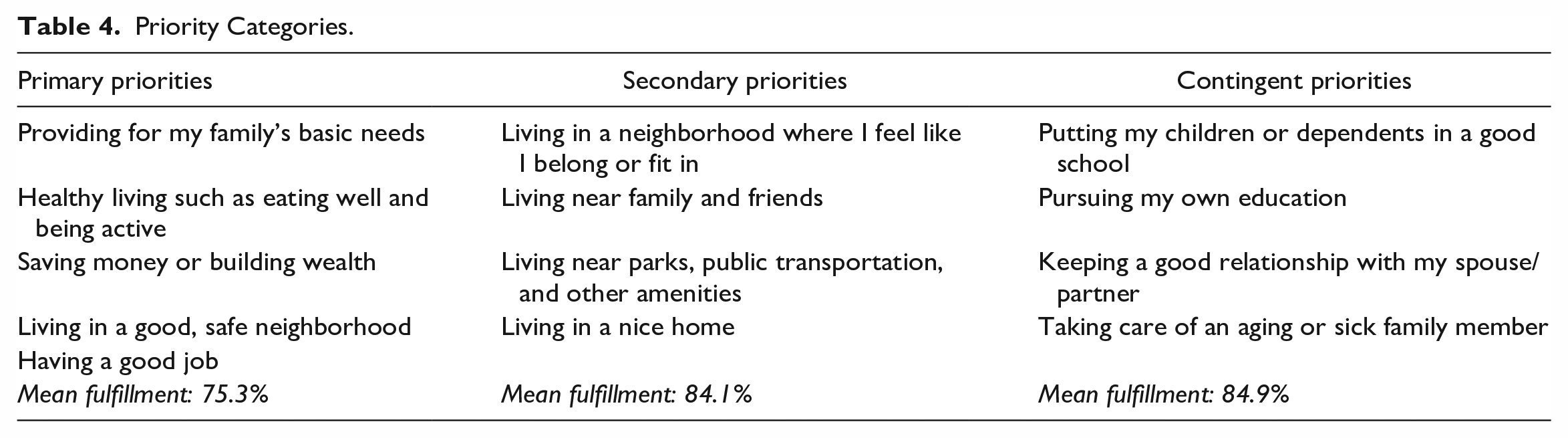
Next, we group the priorities by factor and show the percentage of the sample that endorsed each priority as very important, important, or not important/not applicable, and the percentage of those who endorsed a priority as very important or important who reported being able to fulfill that priority at the time they were surveyed (Table 4). For each factor, we also calculate mean levels of endorsement and fulfillment. This table illustrates the variations in the level of importance of each priority across the sample as well as variation in the extent to which respondents in the sample are able to attain the specific priorities that they value. Finally, we group the priorities into three different categories—primary, secondary and contingent—according to differences in patterns of endorsement, and report mean endorsement levels for each category (Table 4).
We note that the variables for “living near my family and/or friends” and “healthy living such as eating well and being active” have been coded to combine data across waves from the priorities that these variables initially comprised (“living near my family” and “living near my friends” in the former case, and “accessing healthy, affordable food” and “being physically active” in the latter case) before the list of priorities was narrowed down by Resident Researchers in 2018. We also note that we do not report results for the “finding a spouse/partner” priority that was eliminated by Resident Researchers in 2017 due to perceived redundancy with the “keeping a good relationship with my spouse/partner” priority.
Results
Table 1 presents descriptive statistics on an analytic subsample of respondents who completed the prioritization inventory. About 55 percent identified as black or Hispanic/Latinx, and 64 percent of respondents were women. Nearly 45 percent of respondents reported an income of less than $1,250 per month, or $15,000 annually, and almost one in five (19%) said that they or another member of their household had gone hungry in the past month because there was not enough money for food. About two thirds of respondents were renters. The sample reported good health overall, with an average self-reported health score of 3.3, where a score of three corresponds to “good” health and a score of four to “very good” health. Compared with census data from the study neighborhoods, our sample has relatively fewer men, fewer Hispanic/Latinx people, more multiracial people, and more people with children.
Parallel analysis suggested the presence of four factors in the baseline data (Table 2), although no priorities loaded primarily onto the fourth factor. As a result, and in alignment with guidance that the underlying factor count be based on interpretational validity within a range of plus or minus one from the estimated factor count, we retained three factors (Lim and Jahng 2019). Factor 1 captures priorities concerning different dimensions of one’s setting, such as “living in a neighborhood where I feel like I belong or fit in” and “living near parks, public transportation, and other amenities.” “Healthy living such as eating well and being active,” although not an aspect of setting, also weakly loaded onto Factor 1, perhaps because diet and physical activity choices can be highly constrained by setting. Factor 2 included priorities related to family caretaking, such as “providing for my family’s basic needs” and “taking care of an aging or sick family member.” The third factor comprised items related to socioeconomic attainment, including “pursuing my own education,” “having a good job,” and “saving money or building wealth.”
Table 3 reports levels of endorsement and fulfillment for each priority, with priorities organized by factor. Priorities most commonly endorsed as “most important” were “providing for my family’s basic needs,” which was “most important” for 59 percent of respondents; “living in a good, safe neighborhood” (54%); “healthy living such as eating well and being active” (50%); and “having a good job” (50%). Priority fulfillment levels ranged considerably, with the highest being “living near parks, public transportation and other amenities” (92% of those for whom this priority was “important” or “most important” reported being able to fulfill it) and the lowest being “saving money or building wealth” (58%).
Priority Endorsement and Fulfillment.
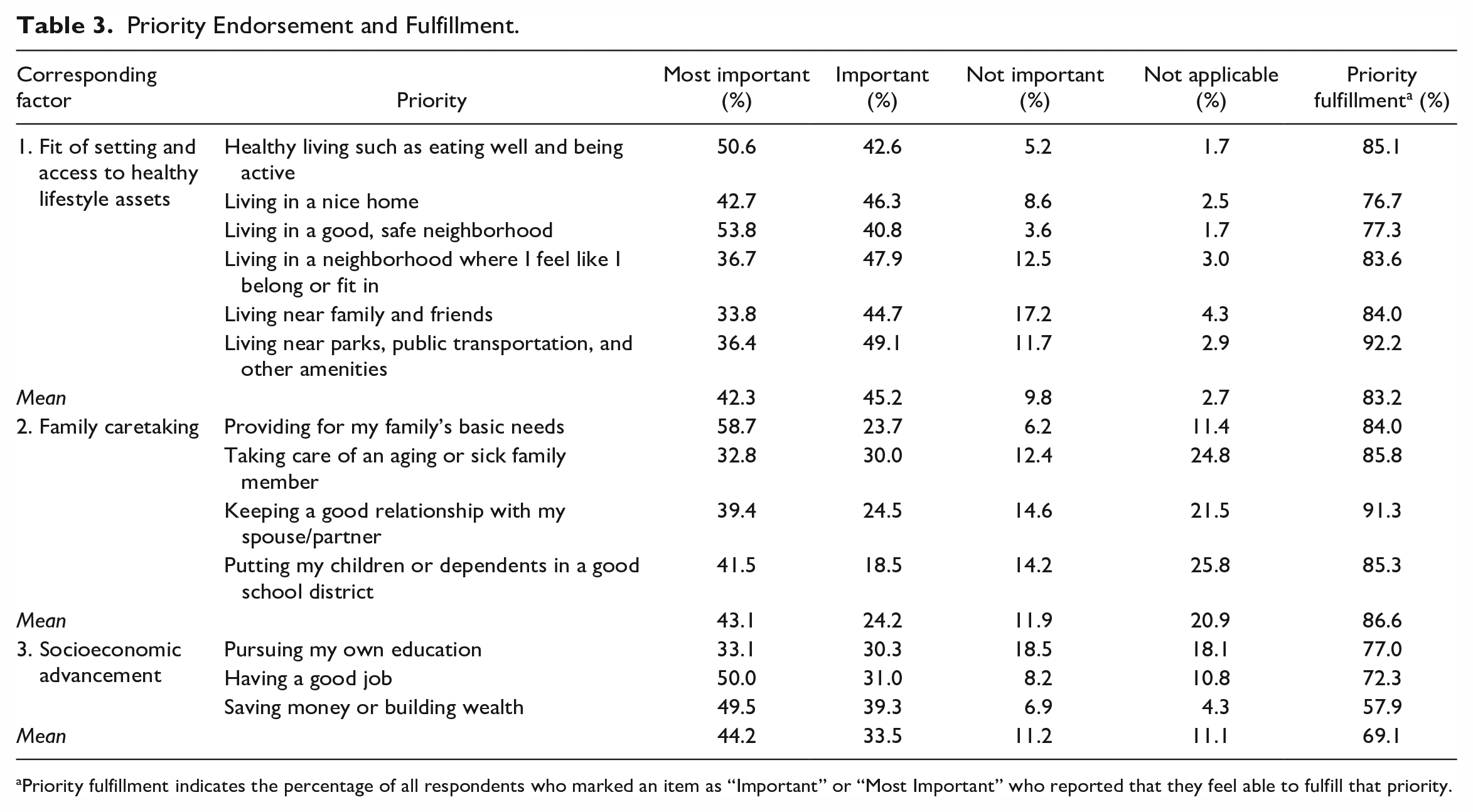
Priority fulfillment indicates the percentage of all respondents who marked an item as “Important” or “Most Important” who reported that they feel able to fulfill that priority.
Different rates and levels of priority endorsement suggest three broad categories of priorities: primary, secondary, and contingent (Table 4). Primary priorities are marked “Most Important” by more than half of respondents and these include fundamental aspects of life such as “providing for my family’s basic needs.” Secondary priorities were more frequently endorsed as “Important” rather than “Most Important,” such as “Living near parks, public transportation and other amenities.” Finally, “contingent” priorities are those that have relatively high levels of endorsement as “Not Important/Not Applicable” but among those for whom these priorities are important, more endorse them as “Most Important” than just “Important.” Contingent priorities include “Keeping a good relationship with my spouse or partner” and “Taking care of an aging or sick family member.” We call these “contingent” because they are contingent on another aspect of the respondent’s life; for example, putting one’s children in a good school district will only be important for respondents who have children. Contingent priorities have the highest mean fulfillment level (84.9%), whereas secondary priorities have a mean fulfillment level of 84 percent and primary priorities have a mean fulfillment level of 75 percent.
Priority Categories.
Discussion
Resident Researchers working alongside academics in a PAR study collaboratively developed a survey instrument that measures endorsement and attainment of a set of functionings—expressed as priorities—as part of a broader effort to understand the impacts of neighborhood changes on well-being. We find that the priorities generated by Resident Researchers vary in importance to respondents, and in rates of fulfillment; for example, those who prioritize “Healthy living such as eating well and being active” are much more likely to report being able to fulfill the priority than those who prioritize “Saving money or building wealth.” The data on levels of priority endorsement suggest that there are three classes of priority—primary, secondary, and contingent—that reflect their relative importance in the respondents’ lives. Parallel analysis suggests the presence of three factors in the data, representing underlying “central functionings” captured by the prioritization inventory: fit of setting and access to lifestyle assets, family caretaking, and socioeconomic advancement. While the first two central functionings had similar mean fulfillment rates of around 85 percent, the fulfillment rate for the priorities capturing socioeconomic advancement was notably lower at 69 percent.
Taken together, our findings have three implications for planners, policymakers, and researchers seeking to impact well-being through interventions in the built and social environments of cities. First, we have demonstrated a replicable process through which planners can operationalize the CA via participatory methods to evaluate well-being at the neighborhood level by measuring residents’ endorsement and attainment of specific functionings. Second, this type of prioritization inventory, especially if deployed across a higher number of places, may contribute to a richer understanding of how neighborhood environments drive health inequities. Third, operationalizing the CA in a place-based, participatory manner can be used to develop evaluative frameworks that facilitate the type of “situated ethical judgment” that is the heart of just planning practice (Campbell 2006).
As planners incorporate consideration of well-being into their work, participatory approaches to assessing well-being will be crucial. Indeed, the capacity to participate is a critical variable in well-being (Nussbaum 2001). Participatory methods have an important role to play in measuring what people do or don’t have, what they can or cannot do with those resources, and the social processes through which they make sense and meaning out of these circumstances (S. White and Pettit 2007). Moreover, co-producing context-specific knowledge about well-being, while as yet still uncommon, is a particularly effective strategy for creating more inclusive spaces for participation in the production of planning knowledge (Woodcraft et al. 2020).
Operationalizing the Capabilities Approach
Given that functionings are “beings and doings” that a person may have reason to value, and that capabilities are a person’s freedom or opportunity to fulfill their desired functionings, the prioritization inventory can be seen as a list of the functionings that Resident Researchers deemed people in their community would be likely to value and seek to fulfill along the life course. By measuring the degree to which these functionings are valued, and the extent to which functionings of value are attained, we can understand whether the capabilities necessary for specific functionings to be attained are present within the community of interest. Thus, we argue that one way to operationalize the CA in planning research and practice is to measure rates of endorsement and attainment of a set of functionings expressed as priorities that people within a community may have. For example, differing rates of priority attainment between highly valued priorities like “healthy living such as eating well and being active” and “saving money and building wealth” suggest that, while just over 85 percent of the people who value “healthy living” have the capabilities in place to attain this desired functioning, 58 percent of those who value saving money and building wealth have the capabilities in place to do so. These differences in levels of priority fulfillment reflect differences in the extent to which the capabilities necessary to attain these functionings are present in the lives of the study population (Shinn 2015).
As the case of the HNS demonstrates, lists of important functionings relevant to assessing the impacts of neighborhood changes can be generated through participatory processes involving residents of multiple communities with a wide range of life experiences and level of exposure to research. While the development of this prioritization inventory took place within a broader PAR process, similar community-based prioritization inventories could be developed during the community engagement phase of planning and design interventions, or by community groups seeking tools through which to hold planning, policy-making, and development institutions accountable to resident well-being. Working with a diverse group of participants can ensure that the inventory includes an appropriate range of priorities capturing the various beings and doings that different community members may value over the life course, and that priorities are expressed in ways that will resonate with community members who value them. Moreover, as Clark, Biggeri, and Frediani (2019) argue, participation helps expand capabilities.
The HNS prioritization inventory has two important limitations when it comes to measuring functionings and, by extension, the presence of capabilities in a neighborhood. First, it does not allow us to measure which specific capabilities are present and to what extent; rather, measuring functionings and their fulfillment allows us to assess the extent to which the set of capabilities necessary to achieve those functionings is present. The set of capabilities underlying any given functioning is not universally consistent, because different sets of capabilities enable different functionings for different people across contexts, and thus cannot be automatically inferred from the functioning itself. Second, this strategy does not indicate which capabilities would need to be added or increased in order for someone to achieve the priorities which they report are important to them but presently feel unable to fulfill. However, within a participatory process, community residents could be engaged in discussion to determine what data on resident’s endorsement and fulfillment of functionings reveal about which capabilities are present or absent and for whom as well as which capabilities would need to be present or expanded to enable community members to attain functionings they value.
While this paper only reports on the underlying factor structure of the inventory, we note that the HNS Consortium plans to study determinants of priority fulfillment in future work. In preparation, we conducted two Collaborative Data Analysis workshops in the Spring of 2020 to collectively decide how to score responses to the prioritization inventory. After discussing the implications of several different scoring options, Resident Researchers expressed a preference for creating an unordered four-category outcome defined jointly by whether the number of priorities endorsed as “important” or “most important” was high or low, and whether or not the respondent fulfilled at least half of those important priorities. The four categories are few priorities, low fulfillment; few priorities, high fulfillment; many priorities, low fulfillment; and many priorities, high fulfillment. The Resident Researchers’ intention behind this decision was to recognize, but not judge as better or worse, the differences in having many versus few important priorities, and differentiating between fulfilling most, versus less than half, of priorities for each. We see resident-led scoring decisions as a key step other researcher teams would need to take to adapt our prioritization inventory to their own contexts.
While functionings and capabilities are the two central components of the CA, one additional limitation to note about our approach is that there are other elements of the CA framework that our prioritization inventory does not capture but that planners may be interested in exploring. One example is “conversion factors” that are the personal, social, and environmental factors that enable resources—like a bicycle or an apartment—to be converted into functionings, and which determine how much functioning a specific person gets from a resource (Robeyns 2016). The role of social conversion factors, like public policies or unequal power relations, and environmental conversion factors, like climate or pollution, in shaping functioning attainment may be of particular relevance to urban planners (Frediani 2019). Future efforts to build upon the HNS prioritization inventory and more fully operationalize the CA might experiment with ways of measuring conversion factors, or with incorporating qualitative data about what resources people rely on to fulfill their priorities, to reach a more detailed understanding of the contextual factors enabling functioning attainment.
Understanding How Neighborhood Changes Impact Health Inequities
HNS Resident Researchers developed the prioritization inventory because they reasoned that the ability to meet one’s major priorities in life was an important pathway through which neighborhood changes associated with rapid, gentrifying development might influence health outcomes in their community. Their reasoning echoes major findings from social epidemiology showing that individual and collective powerlessness is seen as a core risk factor for disease and a core driver of socioeconomic inequities in health outcomes (Marmot 2004; Syme 2003). A recent review by Orton and colleagues (2019) found strong evidence that low perceived control in the living environment plays an important role in the pathways leading from lower socioeconomic positions to poorer health. Autonomy, control, and the power to live a life of value, central to the CA, are also central to health equity (Corburn et al. 2015; Sen 2000, 2002). Protecting health and promoting health equity have become priorities for urban planners and policymakers as they recognize the city’s unique role in shaping exposure to social, economic, and environmental determinants of health (Corburn 2009, 2013).
We argue that operationalizing the CA by measuring functioning attainment via tools like the HNS prioritization inventory holds potential to shed light on differences in power, powerlessness, and “control over destiny” within and across neighborhoods. In doing so, the tool can help urban planners and policymakers understand how neighborhood change and interventions in the built environment impact health outcomes and health equity via their effect on residents’ capabilities to fulfill functionings of value. In the future, we plan to explore patterns of neighborhood-level spatial variation in priority fulfillment across the HNS communities as they proceed through different development trajectories, and test the relationship between priority fulfillment and physical and mental health outcomes measured by the HNS neighborhood survey.
Evaluative Frameworks for Just Planning Practice
While the CA has been promoted by planning theorists for its utility as a framework for evaluating whether and how urban interventions advance justice, its application in practice and policy has been more limited. This is due, in part, to the difficulty of measuring capabilities themselves (Brighouse and Robeyns 2010; Nussbaum 2011; Sen 1995b). Shinn (2015) has proposed one way to address this issue that may be of interest to planners: assessing variation in observed functioning at the setting level. She suggests that the greater degree of variety in observed functioning in a setting, the greater the size of the capability set and range of opportunities available to any specific individual within that setting. Based on our analysis of priority fulfillment rates, it is evident that the capability set present across the study communities as a whole is large, but that the presence of capabilities necessary for respondents to attain specific functionings varies, given the different levels of priority fulfillment (functioning attainment) reported by respondents (Figure 3). Future analysis of data from the HNS prioritization inventory could examine geographical inequalities in capabilities by analyzing variation in observed functioning across the nine study communities, as well as social and economic inequalities in capabilities by analyzing variation in observed functioning across populations within the sample according to social and economic characteristics such as race, gender, age, and income. Further research could also explore mechanisms that determine differential levels of functioning attainment across groups or contexts—such as social support or housing affordability—and consider the planning interventions necessary to enhance local capability sets and functioning attainment.
Tools like the HNS prioritization inventory can thus be used to generate data about individual-, group-, and neighborhood-level functioning attainment that would allow planners, policymakers, and other stakeholders to judge interventions according to whether their outcomes enhanced the capabilities of the relatively disadvantaged, which is how Fainstein (2010) argues the CA should be employed in pursuit of the just city. Evaluators could compare the range and levels of functioning attainment in a setting before and after specific planning interventions. For example, an inventory tool like ours could be used to evaluate housing redevelopment programs by assessing neighborhood residents’ functioning attainment prior to, during, and following redevelopment to understand whether redevelopment reduced interneighborhood inequities and/or disparities between specific populations. Similarly, operationalizing the CA using an inventory like ours may also be valuable to planners working on climate adaptation and resilience as a tool for understanding how to plan interventions that enhance the freedoms and well-being of affected groups to ensure that they are both equitable and politically feasible. In addition to measuring functioning attainment and underlying setting-level capabilities, such efforts could also build on this work to explore important conversion factors.
Using the CA to evaluate interventions can help planners ensure that interventions create conditions that link changes in the built environment to enhanced capabilities to actually guarantee greater well-being and equality of opportunity (Basta 2016). By collecting data at the neighborhood level and assessing variation in functioning attainment at the level of setting, such a strategy would facilitate translating the CA from an individualist ethic to a communal one, allowing for collective quality of life to be prioritized over individual material gain, as both planning theorists and those from allied fields like environmental justice have advocated (Fainstein 2010; Schlosberg 2007). A relational, collective approach to using the CA will be particularly necessary for addressing social and economic inequities rooted in structural racism that inhibit progress toward the just city and urban health equity. Evaluative frameworks that help us address such problems must be able to recognize patterns of domination and oppression across groups, because people’s freedoms are generally constrained as a group, rather than just as individuals (Young 2001). Finally, for the practicing planner, we argue that operationalizing the CA in a participatory, context-specific manner can provide the evaluative frameworks necessary to make the sorts of “situated ethical judgements” upon which just planning relies (Campbell 2006).
Conclusion
The capabilities approach has been promoted as a key tool for conceptualizing well-being and the just city. We have described how a PAR consortium conceptualized and developed a survey tool measuring whether respondents are able to fulfill priorities that are important to them. We argue that the HNS prioritization inventory operationalizes the CA by measuring the attainment of functionings, and that operationalizing the CA in this manner provides a practical tool for assessing how neighborhood change and interventions contribute to health equity and progress toward the just city.
In practice, planners, policymakers, and community organizers can operationalize the CA in a relational manner and using participatory methods to: (1) understand the neighborhood landscape of desired and achieved functionings, and the presence and heterogeneity of capabilities, to demonstrate important features of particular communities to elected officials, planners, policy-makers, and community-based organizations; (2) use measures of functioning attainment (or lack thereof) to demonstrate the various impacts of interventions on capabilities at scales ranging from block-level developments to large-scale gentrification; and (3) support the empowerment and mobilization of communities seeking to exercise their right to the city and advocate for healthy and just urban development that meets their needs in ways that correspond with their values.
Footnotes
Appendix A
Acknowledgements
We acknowledge and appreciate the contributions of the entire Healthy Neighborhoods Research Consortium, especially Resident Researchers. We are also grateful to Justin Steil and the anonymous reviewers for their constructive feedback, and to Patrice Williams for assistance with data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Robert Wood Johnson Foundation under grant no. 72369.