
Abstract
Habitus is society inscribed on the body, but Bourdieu does not explore how biological processes interact with habitus, namely, how action flows from a bio-habitus. I engage pain science to illustrate this point. First, I document how dispositions—specific components of habitus—mediate pain both before and after its onset. Second, I explain how pain alters cognition and affect, an interaction I contend inhibits the habitus. Far from placing the biological over the social, my discussion illustrates how the two are inseparable, a unity underlined by the term bio-habitus. I demonstrate how this concept intervenes in Bourdieusian debates over social reproduction and how the biological inhibition of habitus compares to work on hysteresis. I end by discussing resonances with and implications for disability studies.
To build a theory on habitus is to build a theory on the body, a move that locates the social where one least expects it. Just as Durkheim (1979) illuminated social forces within the seemingly private act of suicide, Bourdieu argues that what is between the head and the toes is an expression not just of DNA but the history of one’s movement across social space. Resisting the dominance of the biologizing view, Bourdieu (2000:141) insists, “The social order inscribes itself in bodies.” What is inscribed—marked on the body—is habitus. There is much to learn from this perspective—for example, how the broad shoulders and upright heads of the powerful are held aloft not by gifts of nature but via costly gym memberships and the discipline of boarding schools. Bourdieu (2000:136) routes biological determinism, but despite underspecified references to “synaptic connections,” he never circles back to fully consider how the body has implications for socialization.
Because Bourdieu moves down from the social to the body, he does not consider the ways one’s socially acquired dispositions may bend and squirm against a body in revolt. Consider the common refrain, “I’m not myself”—whether declared in the throes of pain or hunger, old age or pubescence, what this phrase reveals is the ability of the body to impede the habitus. In short, society’s imprint is entangled with a biological organism so that action always flows from a bio-habitus. It is useful, analytically, to discuss the socialized habitus and biological processes separately, but individuals act from the dash at the heart of bio-habitus. This emphasis on the dash echoes Latour’s (1993) insistence on hybridity, but my aim is not to upend the Bourdieusian project—as Latour might hope—but to advance it.
As a path into the complexity of the bio-habitus, I explore how pain science demonstrates the imbrication of the socialized habitus with the biological organism. To enter on terrain accessible to sociologists, I discuss how the habitus can moderate the biological by reviewing the effects of socialization on the experience of pain. I then reverse course and explain how pain impacts cognition and affect, a pathway that inhibits the expression of habitus. Separating these discussions is necessary for the sake of clarity, but it risks suggesting an ontological distinction between habitus and biology—the point is precisely the opposite. One discussion explains the role of socialization in pain, the other the effect of pain on socialization, but both processes are always simultaneous. Pain is processed by a socialized mind at the same time as pain dulls the mind’s acuity. The habitus may be inscribed on the body, but the body pushes back. I retain and employ the term habitus, shorn of a prefix, to indicate the embodiment of socialization, but my argument is that action flows from a bio-habitus.
Engaging pain science to develop the concept of bio-habitus is not just an exercise in complicating a famously slippery concept—the effect of pain on brain functioning helps mount a defense against those who criticize Bourdieu for explaining social reproduction and nothing else. Because pain can inhibit the expression of one’s habitus—and the timing of pain can vary among those with similar pain risk factors—it is a source of noise between the socializing effects of structures and the actions of individuals. As a result, the bio-habitus perspective helps defend Bourdieu against “the problem of particularity” (Singh 2022), namely, the charge that his theory cannot explain difference among individuals with similar social origins.
Beyond fashioning a defense, the inhibition of habitus by pain is further a theoretically insightful foil to hysteresis, Bourdieu’s term for a state where the habitus persists longer than the field conditions that imprinted it. Both hysteresis and inhibition create a mismatch between habitus and the social environment, a gap that engenders a reflexive awareness that something is amiss. But because hysteresis is driven by structural change, it can generate a sense of reflexivity shared among those holding the impacted class of habitus. Instead of being rooted in a change to the field, inhibition is driven by the biological interruption of habitus, producing a type of reflexivity where one’s sense of self becomes weighted by the experience of pain. Far from creating conditions for solidarity, this is an alienating process that amplifies suffering.
The interaction of the “bio” with “habitus” echoes earlier efforts by Bourdieusian-inspired disability scholars (Edwards and Imrie 2003) to overcome the dualism of the social model and medical perspectives. One achievement of the disability literature is to demonstrate the symbolic violence of medical knowledge, a classification scheme that categorizes bodies as normal and abnormal, healthy and sick—while I embrace this insight, the bio-habitus also demonstrates the importance of learning from biomedicine. If we are always socialized and biological—if we can only act through the bio-habitus—we ignore the biological at our peril.
I begin with a brief critical overview of habitus, focusing on Bourdieu’s (2000) use of the concept in his culminating work, Pascalian Meditations, where the pampered body of the academic is central to his resolution of the tension between objectivist and subjectivist accounts of action. Because Bourdieu focuses on the comfort of the academic, he considers the advantages a body can confer without exploring how a body in pain can inhibit habitus. I then review the secondary literature, including criticism that habitus can only explain reproduction, and extant work on the body and habitus. To set the ground for the bio-habitus, I offer an overview of biomedical understandings of pain and chronic pain, focusing on recent advances in neurology. Building on this literature, I explain how pain is mediated by dispositions within the habitus. Pain beliefs such as “catastrophizing” demonstrate how cognitive dispositions can amplify or moderate the experience of pain, whereas the development of avoidance behavior is an example of pain generating tertiary habitus formation at what Wacquant (2014) calls the “conative” level. I then review evidence documenting the cognitive and affective impacts of pain. In particular, pain taxes the attentional bandwidth of the brain, thus limiting an individual’s ability to respond to stimuli—an interaction I conceptualize as inhibiting the habitus. Taken together, these perspectives demonstrate the imbrication of the social and biological in the bio-habitus. I next elaborate the significance of this insight for Bourdieusian sociology by specifying how inhibition interrupts social reproduction, exacts a social cost, and compares to hysteresis. To conclude, I unpack the implications for a Bourdieusian perspective on disability.
Habitus in Pascalian Meditations
Bourdieu (2000:138) argues that habitus allows him to dispel with two fallacies, what he terms in Pascalian Meditations “mechanism” and “finalism.” 1 The former “holds that action is the mechanical effect of the constraint of external causes” and the latter “that the agent acts freely, consciously, and . . . ‘with full understanding’” (Bourdieu 2000:138). When analysts embrace mechanism, they perceive actions as rote and mechanical; when finalism is one’s guidepost, actions appear strategic and reasoned. In between these two extreme accounts—humans as automatons, humans as free will—Bourdieu slides habitus, a structured spontaneity. It is structured because “schemes of perception, appreciation and action” (Bourdieu 2000:138) are imprinted as one is socialized, a marking that reflects one’s origin in a particular family and subsequent trajectory across social space. It is spontaneous because the unfelt presence of these schemes enables “acts of practical knowledge” (Bourdieu 2000:169) that, sans effortful calculation, generate a range of available actions that feel naturally suited to one’s social environment. Bourdieu stresses the social and structural ancestry of habitus—its internalized dispositions are the result of contact with society—but its medium is the individual body (for an excellent overview of habitus, see Benzecry 2018).
In Pascalian Meditations, Bourdieu (2000) sets his sights on the body of the scholar. The account is a masterful analysis of the philosopher caught unaware by the spell of skholé, namely, the academic’s projection of their point of view into the mind’s eye of the subject. But because a study of the academic habitus hinges on a pampered body, the account highlights a case where the body and habitus are neatly integrated without considering how a pained body can inhibit one’s habitus. When Bourdieu (2000:13–14) writes that the scholastic position is “a site and a moment of social weightlessness,” he is drawing attention to the safe distance academics enjoy between their self and the realm of necessity, a distance from which one can cast a “sovereign gaze” (Bourdieu 2000:23) to categorize and quantify the ills of the world. This distance entails the material conditions that enable one to be socialized into skholé, namely, “the neutralization of practical urgencies and ends” (Bourdieu 2000:14). Unlike those “ordinary mortals who have to take each day as it comes,” hurdling over contingencies and nagging hazards, the scholar lives in a world of thought defined by “a divorce between the intellect, seen as superior, and the body, seen as inferior” (Bourdieu 2000:23). Although this divorce is made possible by the professional world of the philosopher, it is not an available move for the burdened, which is why it is a grave error for philosophers to project their own relation to the practice of thought into the head of the imagined subject. Bourdieu (2000:50) insists that to overcome this scholastic fallacy, one must “return to the world of everyday existence,” where practice outweighs reflection as a means for moving through the day. In this way, Bourdieu undermines the philosopher’s view of the subject but also the self-perception the academic world holds of itself as being a realm of pure thought. As he illustrates, the philosopher is not above the body—the academic habitus is structured by the comfort the body enjoys. From the embrace of an armchair, comfort induces a relationship to thought that obscures the effects of comfort.
By spotlighting the privilege of the academic, Bourdieu (2000) succeeds in his criticism of skholé. But as a project for establishing the importance of the body to habitus, it is a one-sided case—the privilege Bourdieu exploits to reveal skholé excludes consideration of the pained body. Of course, Bourdieu’s writings on habitus are extensive, and this is far from the only place he interrogates habitus and the body. However, across his work, he emphasizes the effect of the social on the body while only glossing over the effect of the body on socialization. In Distinction (Bourdieu 1984:192), for example, Bourdieu calls the body “a social product” that bears the imprint of the food, leisure, and employment one’s class station affords. The possibility of illness interrupting such reproduction is set aside in a parenthetical wherein he notes the production of classed bodies will proceed “biological accidents apart” (Bourdieu 1984:193). This stress on the social body is also apparent in Masculine Domination (Bourdieu 2001:23), where Bourdieu details the “somatization of the social relations of domination,” namely, the process by which symbolic distinctions become embodied through the gendered habitus. Highlighting the socialization of bodies is an important contribution, one that bends the stick against the powerful allure of biology as destiny. But armed with the insights of Bourdieu, this article spotlights biological accidents. What happens to the habitus when a body is in pain, be it the body of a comfortable philosopher or a struggling phlebotomist?
The Problem of Particularity
Because the habitus develops from contact with society, the concept has been criticized for theorizing social reproduction at the expense of individuality, a charge Singh (2022) lyrically calls Bourdieu’s “problem of particularity.” In this critical take, one’s social position imprints a habitus that is the social space in miniature; when in motion, this habitus helps recreate the larger social space—a neat, closed circuit (Dalton 2004; Sewell 1992). The problem of particularity is the challenge of accounting for the fact that individuals with ostensibly similar origins are often quite idiosyncratic. Neighboring the problem of particularity, habitus is also indicted for erasing agency (Alexander 1995; Archer 2007; Crossley 2001; Sayer 1999). As King (2000:427) writes, “since everyone in society has a habitus, individuals will never actually be faced with unforeseen and ever-changing situations, because everyone else, informed by their habitus, would simply go on repeating their social practices and reproducing their social relations.”
The prominence of this critique is in part a result of the contingent diffusion of Bourdieu’s thought into anglophone academia. As has been widely observed (Benzecry 2018; Gorski 2013; Lizardo 2012), Bourdieu’s arrival on the American intellectual scene was marked by attention to his empirical studies of class (Bourdieu 1984) and education (Bourdieu and Passeron 1977), two areas where reproduction is often the phenomenon of interest. The reproduction critique has been rebuked by Wacquant (2014), notably through his genetic argument that Bourdieu’s development of habitus is rooted in fieldwork marked by cultural upheaval, namely, the twilight of colonial Algeria and Bourdieu’s encroached-upon rural homeland of the Béarn (see also Bourdieu 2000:64).
Singh (2022) roots an additional defense from within Bourdieu’s oeuvre, arguing that extant scholarship does not emphasize relational logic. In this take, critics miss the finely textured experience individuals have as they move across social space. Not only does an agent’s trajectory alter the fields they cross, but those fields are continuously in flux due to the actions of others. Given this fluidity, minor differences in the timing of movement across social space could lead two agents with similar origins and trajectories to pass through fields with markedly different effects on the habitus. Aligned with Singh, I show how intimate differences rooted in the bio-habitus can scramble the effects of structure on individuals, adding another tool to reconcile Bourdieu with particularity. Whereas Singh looks to the relational dynamism of fields, I turn to the truculence of pained bodies.
Bodily Advances on Habitus
I am far from the first to consider the role the body plays in habitus (Connell and Mears 2018). A range of work explores its embodied nature, and a few contributions look specifically at pain and habitus. However, this scholarship centers on asking how the body and pain can be a resource for enacting social life—what Bourdieu calls “capital”—a contribution distinct from my emphasis on the bio-habitus.
How can the body be cast as a resource of capital? Some of the theorizations in this approach include erotic capital (Green 2008; Hakim 2011), 2 aesthetic capital (Anderson et al. 2010), gender capital (Bridges 2009), and bodily capital that can lead to economic capital via professions like modeling (Mears 2011). There is much interest in how a fit body can be marshaled to advance cultural capital (Khan 2011), especially in a way that privileges whiteness and heterosexuality (Connell and Mears 2018). In an earlier piece, Williams (1995) drew on Bourdieu to theorize how health behaviors are classed, thus offering an explanation for population-level differences that works down from the structuring effects of class and then up from the perspective of habitus. Anticipating the later work of Mears (2011) and Khan (2011), he specifies how certain lifestyles are used as resources in contests for recognition. In their overview of Bourdieu and the body, Connell and Mears (2018:571) suggest “for all the attention to the accumulation of bodily capital, relatively little attention has been paid to the loss of or absence of such capital and the opportunities that such ‘failures’ may offer.” In the Distinction (Bourdieu 1984:193) passage that references “biological accidents,” Bourdieu briefly explores this point. Whereas social status is assigned to the bodily traits enabled by being in a dominant position (e.g., fitness), Bourdieu notes that biology “sometimes denies the ‘high and mighty’ the bodily attributes of their position, such as height or beauty.” In this aside, Bourdieu demonstrates that he is aware the body can directly shape habitus, as one’s dispositions must accommodate a lack (or excess) of some trait expected to signify one’s standing.
Beyond the bodily capital perspective, prior work has used Bourdieu’s toolkit to explore the role of pain, examining its social origin and function in specialized communities. In Wacquant’s (2004) classic account, learning to endure pain is a stepping-stone toward acquiring the boxer’s pugilistic habitus. Moving from boxing to ballet, in Turner and Wainwright’s (2003) study, pain is accepted and managed as part of the dancer habitus, whereas debilitation—an acute risk for dancers—is cushioned by the community norms of a field premised on the threat of sudden and tragic injury. Instead of interrogating habitus, this article works with the concept to criticize a social construction perspective on dance taken to excess, one that treats the body as text without accounting for the experience of pain. Alford and Szanto (1996) make a similar argument about pain among piano players, showing how the acceptance of pain is naturalized by the musician habitus, although their interest lies in demonstrating how the political economy of the elite piano field is organized in a way that produces such pain. Vandebroeck’s (2017) ambitious contribution to the study of class embodiment takes a wider perspective, emphasizing how the dominated are conditioned to ignore pain via the careers open to them.
Biomedical Understandings of Pain
To illuminate the bio-habitus, I move in two directions. First, my aim is to illustrate how socialization mediates pain, an enactment of what Latour (1993) calls the denunciation of nature by society. To do this, I show how an agent’s habitus impacts the cognitive processing of pain and how the impacts of chronic pain spur tertiary habitus formation, a step that shapes downstream pain. Second, I reveal how pain impacts cognition and affect, a move that denounces society with nature. This interaction, centered in the anterior cingulate cortex, inhibits the expression of habitus by reducing one’s ability to process environmental signals that trigger dispositional action. Although separate in presentation, these are simultaneous processes—a point that should demonstrate the imbrication of the terms in bio-habitus and warn off reifying what Latour calls dualism.
Before making these arguments, I provide an overview of the processes that generate the experience of pain. My review is not exhaustive but intended to provide an intuition for the biomedical logic that informs my argument. Although focused on the state of pain science today, I am aware that biology and medicine are fields of struggle—far from understanding current knowledge as final, I stress their provisional nature. This remark could seem to undermine my project, but I believe there is value in provisional findings. I base this stance on Bourdieu’s (2004:62) argument that scientific fields can be sites of “regulated struggle.” In short, Bourdieu argues that such fields can achieve autonomy through a high barrier to entry in the form of scientific capital (as in research skills) and internal norms that value rigorous debate. These social conditions of autonomy, although never perfect, can “rescue scientific reason from relativistic reduction and explain how science can constantly progress towards more rationality without having to appeal to some kind of founding miracle” (Bourdieu 2004:54). Knowledge may never be final—and there is good reason to be skeptical of Bourdieu’s use of the adverb “constantly”—but it can still progress.
From a Thorn Prick to the Neuromatrix
What is pain? To appreciate the complexity of this question, consider the gardener. In a rush, they do not bother to grab gloves before heading out to deadhead a rose. Reaching toward a stem, a thorn catches their right index finger, drawing blood. Almost instantly, they draw their hand away from the thorn and emit a pained yelp.
When the thorn punctures skin, cells are destroyed, releasing cellular material into what biologists call the extracellular space (Ambron 2022). 3 One thing that gets released is ATP—adenosine triphosphate, a molecule that, within cells, provides energy to power many basic functions. Released into the intercellular space by the thorn, ATP binds to the terminal membrane of nociceptor neurons, which initiates a series of electrical signals called “action potentials.” These signals travel up the arm and enter the spinal cord at the C6 vertebrae. Here, the signal splits in two, with one path heading back toward the right hand via a motor neuron. This stimulates muscle contractions, leading to the quick withdrawal of the hand away from the thorn—a mechanical reaction that prevents further damage. The other path enters a second-order neuron and crosses to the left side of the spinal column, continuing up into the brain. Here the signal enters third-order neurons in the thalamus, a structure that generates the sense of pain (as well as the other sensations we call “senses,” minus olfaction) in concert with structures deeper in the brain.
This description glosses over the biochemistry that drives action potentials up to the brain and once there, how and by what mechanisms the signal radiates along a tangled path. Complicating matters further, the process initiated by a thorn is distinct from that started by a flame, which is driven by the opening, at a specific temperature threshold, of a family of ion channels in the nerve terminal. Internal pain, such as from a kidney stone, is also wired through distinct visceral neurons, as opposed to nociceptor neurons. Given this complexity, biomedical scholars have theorized pain models to simplify the underlying processes.
Early models viewed pain as a signal that moved from tissue damage to the brain, but a breakthrough came with Melzack and Wall’s (1965) gate control theory. This recast pain as a two-way path, with information passing from the injury to the brain and from the brain down through the nervous system (Gatchel et al. 2007; Moayedi and Davis 2013). After an injury, nociceptive neurons transmit information from the site of tissue damage to “gates” in the spinal column, which pass information up to the brain. In the second, simultaneous step, “the other sensations we experience (fear, shock, anxiety) result in information being passed in the opposite direction, from the brain to the gate” (Denny 2018:21). This downward path moderates how the upward path is communicated and is vital for theorizing the bio-habitus.
Within medicine, gate control theory was essential for integrating affect into pain science, but it failed to account for a long-standing puzzle—phantom limb pain (Keefe, Lefebvre, and Starr 1996). Why do patients feel severe pain in a limb that has been amputated and more specifically, when there is no spinal cord connection? Accounting for this anomaly led Melzack (1990) to posit that a diffuse network of structures inside the brain ultimately generates the experience of pain. Whereas gate control theory emphasized the role of affect in pain, this later development, termed the neuromatrix, suggested an even more prominent role for socialization.
Much of what is known about the neuromatrix is enabled by functional magnetic resonance imaging (fMRI). Such imaging can detect “changes in blood flow or oxygen usage” in the brain, which, assuming activated neurons require an increased supply of energy, indicates how involved distinct regions are in neurological processes (Ambron 2022:144). The exact mechanisms underlying these connections are elusive, but the relationships of structures in the neuromatrix to the experience of pain are increasingly understood via fMRI studies. When an action potential reaches the thalamus, it radiates into the brain through the anterior cingulate cortex (ACC). The ACC processes sensory inputs like pain, sound, and light in a hierarchical manner, meaning the pain the gardener experiences can be lessened if they are distracted by a passing ambulance. The shifting of attention to the ambulance is driven by another structure of the brain that acts on the ACC, the amygdala, which stores traumatic memories and applies them reflexively when related information presents itself. To simplify, the amygdala has learned that ambulances can signal danger, so it directs the ACC to ignore the prick and focus on the siren. But the brain “also contains a group of neurons that provide positive reinforcement and motivation for behavior based on whether or not there is a sufficient reward for ignoring the hurtfulness” (Ambron 2022:148). Identified as the nucleus accumbens, this structure can moderate pain if the rose is destined for a horticulture competition. Taken together, the experience of pain is the result of affect, motivation, and action potentials interacting—namely, the bio-habitus.
Chronic Pain
Chronic pain is treated by the medical field as an illness unto itself. The term is used in contrast to acute pain, namely, fleeting pain, such as from a rose prick. To assess the prevalence of chronic pain at the population level, the Centers for Disease Control (CDC) defines it as pain on “most days” or “every day” in the past three months. In 2019, chronic pain afflicted 20 percent of U.S. adults (CDC 2020). Just as there is variety among the processes driving acute pain, chronic pain can be rooted in a range of biological mechanisms. As one example, following injury, a phenotypic change can occur that affects a first-order nociceptive neuron and thus the pathway by which activation potentials reach the brain. Such changes include the production of new ion channels that amplify action potentials moving up the neurons (Ambron 2022). As a result of the additional ion channels, the individual becomes sensitized to what otherwise would have been negligible sensations, producing a chronic pain state called hyperalgesia.
How Habitus Mediates Pain
To clarify how habitus mediates pain, I draw on Wacquant’s (2014) three-part schematization. Wacquant (2014:8) argues that his work demonstrates “one may analytically differentiate and empirically document three ‘components’ to habitus.” These components are cognitive, conative, and affective. Mirroring the evaluation of pain in brain structures like the amygdala and nucleus accumbens, the cognitive level concerns “the categories of perception through which agents cut up the world, make out its constituents, and give them pattern and meaning” (Wacquant 2014:8). Conative, which evokes the nociceptive neurons that signal tissue damage, “consists of proprioceptive capacities, sensorimotor skills, and kinesthetic dexterities that are honed in and for purposeful action” (Wacquant 2014:8). Finally, affective, which aligns with the role emotions play in gate control theory, concerns “the vesting of one’s life energies into the objects, undertakings, and agents that populate the world under consideration” (Wacquant 2014:9). As I demonstrate, cognitive dispositions shape the experience of pain, and pain itself can spur the development of conative dispositions that have downstream effects on health.
In medicine, “pain beliefs” are cognitive dispositions that mediate the experience of pain (Baird and Sheffield 2016; Williams and Thorn 1989). Social scientists have conducted complementary research, documenting cultural practices that underlie distinct reactions to and understandings of pain (e.g., Bendelow and Williams 1995; Zborowski 1952). Such research often concerns the interconnections between belief and institutionalized actions, but in medicine, research is focused on smaller-scale cognitive constructs. A major aim in this field is to identify constructs ripe for clinical intervention, often through cognitive behavioral therapy. Although much could be learned from a dialogue between cultural studies of pain and clinical studies of pain beliefs, here I focus on the latter to emphasize what may be least familiar to sociologists. 4
Catastrophizing, a well-established construct in psychology (Ellis 1962) used to identify a general tendency toward “an irrationally negative forecast of future events” (Quartana, Campbell, and Edwards 2009:745), illustrates the compatibility of habitus with research on pain beliefs. Applied to pain, catastrophizing is the “tendency to magnify or exaggerate the threat value or seriousness of pain sensations” (Quartana et al. 2009:745), a cognitive disposition that affects experienced pain intensity, anxiety, and hypervigilance toward pain (Sullivan et al. 2001). The concept is widely studied, but there are disagreements about whether it should be further decomposed into more specific dispositions and processes. Despite such debates, “[w]ithin pain literature, catastrophizing emerges as one of the most robust and reliable predictor[s] and correlate[s] of adverse pain experience” (Petrini and Arendt-Nielsen 2020).
When patients are assessed for the disposition before surgery, those who reveal a tendency to catastrophize have worse “postsurgical pain ratings, narcotic usage, depression, pain-related activity interference and disability levels” (Quartana et al. 2009:747). The disposition can develop in response to pain, but when it exists prior to pain’s onset, it has been found to predict a longer persistence of pain symptoms. Specifying how exactly catastrophizing is related to such a wide array of findings is unsurprisingly complicated. One view is that the disposition influences the ability to discriminate between different sensations. As discussed previously, perception is hierarchical, with the ACC spotlighting sensations that a subject considers important. This effect has led some pain scholars to argue that “pain catastrophizing amplifies the experience of pain via exaggerated attention biases to sensory and affective pain information” (Quartana et al. 2009:748; see Figure 1). Catastrophizing has also been connected to physiological stress responses, such as muscle tension, which can amplify pain. This perspective connects to the intuition behind gate control theory, where affective states influence how pain signals are transmitted to the brain.
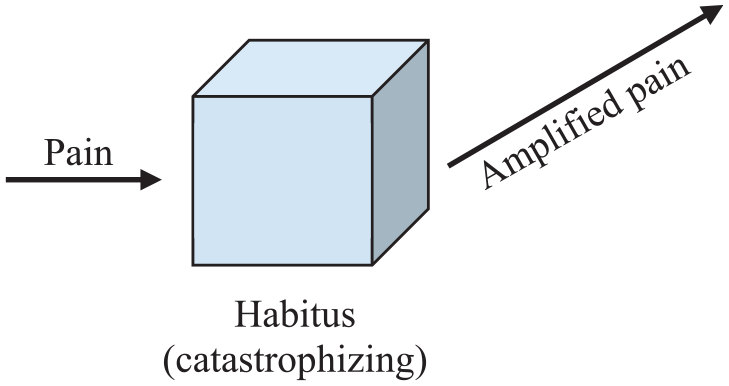
The effect of pain beliefs on experienced pain.
The poor health outcomes tied to catastrophizing are mirrored by the therapeutic effects of self-efficacy beliefs, namely, an evaluation that one can achieve a goal despite obstacles (Bandura 1977). Just as catastrophizing is linked to a range of negative health outcomes, self-efficacy has been shown to decrease the experience of pain and disability. For example, a study of individuals with lower back pain found that self-efficacy beliefs moderated the negative influence of pain intensity on disability (Costa et al. 2011). Although these findings may strike one as sanguine, they generalize to the well-known placebo effect, wherein positive expectations initiate neurotransmitters that lessen the experience of pain (Dodd 2017).
In light of this research, Main, Foster, and Buchbiner (2010:207) argue for the importance of understanding the “style of response to pain and the threat of pain.” Such a style implies the working of habitus at the cognitive level, namely, the influence of one’s socialization on dispositions that guide reactions to pain. The importance of cognitive dispositions to the experience of pain has led to public health campaigns that attempt to rework public perceptions of pain. Such a popular classification struggle, to invoke Bourdieu, occurs through “knee schools,” a preoperation training for people set to undergo knee replacement (Lalkhen 2021). What’s more, “[s]everal countries have now performed mass media campaigns in an attempt to shift beliefs about back pain” (Main et al. 2010:213).
Tendencies toward catastrophizing and self-efficacy demonstrate how cognitive dispositions can influence the experience of pain, revealing the compatibility of habitus on the cognitive level with biomedical research. To broaden this discussion to the conative level, I briefly turn to the literature on avoidance behavior, a type of habit formation that impedes recovery from injury and can exacerbate the experience of pain. Avoidance behavior refers to the evasion of routine action due to the anticipation of pain. Such a conative tendency is implicated in the etiology of chronic pain when it persists beyond healing or generalizes to behaviors beyond those implicated in injury (Vlaeyen, Crombez, and Linton 2016). For example, a back injury may lead one to limit their range of motion to, in the mind of the agent, prevent further strain. This could initially be medically justified, but if the limitation becomes ingrained—if the disposition enters the habitus on the conative level (see Figure 2)—it can induce harm. Research on avoidance behavior, tied mostly to musculoskeletal pain, suggests that avoiding certain motions, what is called “disuse,” can lead to deconditioning and maladaptive movements (Leeuw et al. 2007).
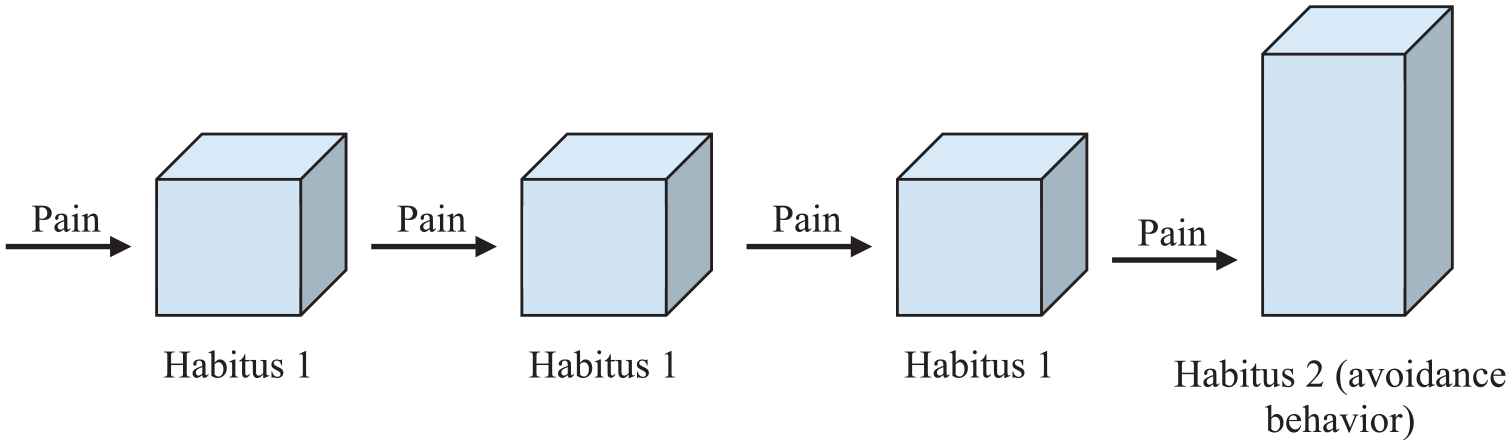
The formation of avoidance behaviors.
Whereas avoidance behavior can be understood as conative tertiary habitus formation, it also entails a state of anxious monitoring of pain, and the affective charge of this behavior has been found to have debilitating effects. For example, the fear of lower back pain can have a significant effect on the use of sick days (Turk and Wilson 2010). One treatment for avoidance behavior is exposure therapy, in which patients are encouraged to engage in a feared behavior, such as lifting a heavy object. Such a procedure “provides a disconfirming experience and offers corrective evidence, which reduces fearful responding and ultimately inhibits further avoidance behavior” (Volders et al. 2015:34). Just as public health campaigns attempt to shift cognitive dispositions concerning pain, exposure therapy can be seen as the intentional reworking of the habitus at the conative (and affective) level.
My read of the literature on catastrophizing and avoidance behavior is meant to demonstrate that the dispositions contained within habitus can mediate pain. The doctor-patient interface may not be the place for invoking habitus, but this discussion shows the potential for habitus to serve as a heuristic for the social elements of pain within medical research—indeed, Oerther and Oerther (2018) make just this point in the context of treating patients adjusting to disabilities. Whereas this use of pain research affirms habitus as Bourdieu theorized it, I now look more closely at how pain impacts the brain to underline the “bio” in the bio-habitus.
How Pain Inhibits Habitus
Bourdieu describes habitus as being “a sort of spring that needs a trigger” (Bourdieu and Wacquant 1992:135). The trigger is an external stimulus that unlocks the spring’s tension, propelling it in a direction it was predisposed to take. I argue that pain can interrupt this process by interfering with the trigger. In Bourdieu’s model, the triggering of the spring sends it on a path determined by one’s socialization; but in the presence of pain—the “bio” in bio-habitus—the trigger is altered, sending the spring along a different path, one that uncouples the identity between socialization and action. To illustrate this point, I discuss pain’s impact on the cognitive level of habitus through its effects on attention, memory, and other functions. I then turn to the affective level and discuss the influence of chronic pain on mood and mood’s relationship to cognition. Through these interactions, the brain’s attentional capacity is taxed, thus limiting one’s openness to stimuli that could trigger the habitus.
The cognitive impairments caused by chronic pain are diverse, including a diminished ability to toggle between tasks and assess the consequences of one’s actions (Moriarty, McGuire, and Finn 2011). At the center of these deficiencies is the effect of pain on attention—in populations with a range of illnesses, the presence of pain has been correlated with a decreased ability to focus on and respond to everyday responsibilities. Evidence for this finding is based on patient reports (e.g., Muñoz and Esteve 2005) and tests designed to measure attention (e.g., Oosterman et al. 2011), such as having subjects complete timed problem-solving tasks. Beyond attention, there is evidence documenting the ability of pain to interfere with short-term memory. Park et al. (2001) found negative effects of fibromyalgia pain on a range of memory tests, results that are echoed in other chronic pain populations, such as those with rheumatoid arthritis (Brown, Glass, and Park 2002). Pain also increases reaction times following a stimulus (Antepohl et al. 2003) and the time required to complete simple computer tasks (Harman and Ruyak 2005). Given that habitus is meant to emphasize the unthinking and spontaneous nature of practical action, these studies are of special interest. However, pain has also been demonstrated to decrease executive functioning skills (Verdejo-García et al. 2009).
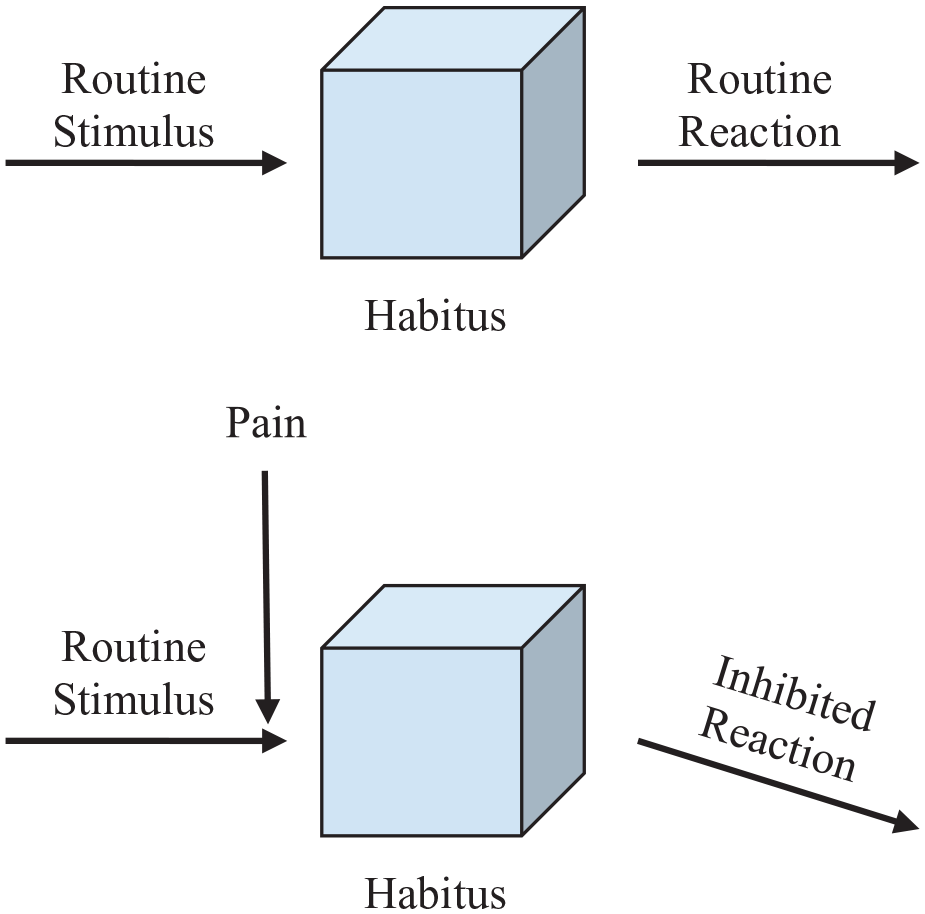
My argument does not require conceptually distinguishing attention, memory, reaction time, executive functioning, and other cognitive traits—these concepts are deeply related and overlap. Instead, the point is to document the immense evidence for pain’s ability to diminish cognitive acuity and thus inhibit habitus at the cognitive level. What drives this effect? One mechanism is pain’s impact on the ACC, which can be understood through the heuristic of attentional bandwidth. Pain is a signal that eats away at one’s attention, thus decreasing the ACC’s bandwidth available to devote to other signals. As the pain from an aching back or a persistent headache monopolizes attention, it interferes with the perceptual inputs that would otherwise trigger one’s habitus (see Figure 3). In short, it is not the self that is changing—as in the formation of avoidance behaviors—but rather one’s openness to the world. However, in their review of chronic pain and cognition, Moriarty et al. (2011) note two additional possibilities that suggest an altered biology. First, chronic pain may change brain structures in a way that diminishes cognitive capacity. Second, chronic pain may dysregulate the production of neurotransmitters, a process that can impair brain activity and amplify pain via the gates of gate control theory, which, in turn, would further limit attentional capacity.
Habitus and inhibition.
Cognition studies match patients on a range of factors—such as root illness or the use of a particular medication—to isolate the effect of pain on cognition, but they are typically limited to a single national context, raising the question as to whether the “national habitus” (Bourdieu 2014:361) could influence findings. To frame this objection, perhaps the internalization of a particular national culture—class and other differences aside—and the cognitive dispositions it entails could underlie the effect of pain on cognition. As Bourdieu (2014:216) argues, the state’s monopoly on symbolic violence positions it to generate “a unified cultural habitus.” In a study motivated by the literature’s narrow emphasis on the pain experience of Western European and U.S. subjects, Nadar, Jasem, and Manee (2016) found that chronic pain reduces the cognitive abilities of Middle Eastern patients in a similar manner to that found in the extant literature: “The similarity of these findings, along with the control for psychosocial variables, suggests that chronic pain contributes directly to cognitive impairments regardless of cultural differences.” This supports the view that a biological process is involved in pain’s effect on cognition distinct from the role of cognitive dispositions rooted in socialization.
Moving from the cognitive level of habitus to the affective, it should come as no surprise that there is a strong relationship between pain and negative changes to one’s affective state, although the causal relationship is deeply complex (Hart, Wade, and Martelli 2003). As one example, although it might seem obvious that pain would lead to a change in mood, it is also true that pain impacts sleep, which can impact mood by producing anxiety and irritability (Burgess et al. 2019). If one’s investment in the game—what Bourdieu calls illusio—is a key component of habitus, then pain’s negative effect on motivation vis-à-vis emotional change points to another route to the inhibition of habitus.
The ability of pain to diminish one’s investment in the world—to inhibit habitus at the affective level—is suggested by research into the relationship between pain and depression. Robust evidence shows that chronic pain and depressive disorders are linked, but causality is hard to parse—a highly cited longitudinal study of musculoskeletal pain found “the evidence supports both the views that depression promotes pain and pain promotes depression,” with the effect of pain on depression appearing “somewhat more powerful” (Magni et al. 1994:289). Complexity is the rule here—social costs of pain surely play a role in the link between depression and pain, for example, when one has to miss valued activities due to pain. However, the aforementioned cognitive effects of pain have been linked to “a reduced desire for activities,” which is itself an indicator of depression (Hart et al. 2003:118).
Regardless of pain’s ability to inhibit habitus at the affective level, it is also the case that by triggering negative affect, pain can amplify its inhibition of the cognitive habitus. What makes this the case is that negative affect interacts with the ACC in a manner similar to pain. As Hart et al. (2003:121) write, “Because painful stimulation and related emotional distress are attention-demanding, the reserved capacity of the ACC to allocate attentional resources may be limited.” Not only do the cognitive effects of pain and negative affect converge in the ACC, but per gate control theory, negative affect amplifies pain. Although these relationships point to the inhibition of habitus, it is also important to emphasize that cognitive dispositions, such as catastrophizing, can predispose individuals to have a negative affective reaction to pain. As discussed previously, this entails the habitus mediating pain rather than pain inhibiting the expression of habitus. There is also evidence that pain and negative affect can combine to alter the biological body through dysregulation of the hypothalamic-pituitary-adrenal axis (Vachon-Presseau et al. 2013). Such dysregulation could result in excess cortisol, a stress hormone that shifts the body toward its fight-or-flight response. Evidence from both human and animal studies shows the effects of long-term stress on the brain, and thus cognition and affect, are powerful (McEwen 1999).
To return to the rose, as blood drips from the gardener’s hand, they are caught between neurological processes closing the world off, learned investments pushing them toward horticultural glory, and alarm at the passing ambulance siren. Whether they persevere or stall amid the pain, the complexity of their response cannot be understood from the social or biological vantage alone. We are the product of the interaction between the two, the dash at the heart of bio-habitus.
The Significance of the Bio-Habitus for Bourdieusian Theory
If habitus develops from contact with society, how is it that individuals located in the same social space are often quite different? In response to those who indict Bourdieu for failing to explain particularity, Singh (2022) looks to the relational dynamism of fields, arguing that minor differences in the timing of one’s social trajectory can result in a unique socialization experience. This argument looks up from individuals to fields, identifying a source of difference in the complexity of competitive relational structures. By drawing attention to pain’s impact on cognition and affect, I am looking down to the body’s biological ability to inhibit the expression of habitus and engender difference between otherwise similar individuals. As pain taxes the attentional bandwidth of the ACC, the agent’s ability to read the world is diminished, thus altering how contact with the world triggers the spring of habitus. Beyond creating difference within the moment of inhibition, this attentional deficit could also affect the process of “permanent revision” (Bourdieu 2000:161) that ensures the habitus is never final. Whereas Bourdieu (2000:134) describes habitus as entailing “the (biological) property of being open to the world . . . and so capable of being conditioned by the world,” the bio-habitus perspective reveals that such openness is not constant.
Inhibition could be fleeting—a jammed finger diminishing the adroitness with which a parent makes their child breakfast or, with greater consequence, the composure with which a job candidate navigates a slide deck. Acute pain is unlikely to coincide with something as momentous as a career change, but chronic pain definitionally has long-term effects. Following Singh (2022), the timing is crucial—minor differences in the moment of pain’s onset can lead to meaningfully different trajectories. Consider, for example, someone who develops lower back pain one week into a new job versus one year. As I discuss, the distribution of pain is socially patterned, but the particular accidents and illnesses suffered by individuals and their bodies create resistance within a social system that tends toward reproduction.
How does inhibition generate particularity? A disrupted career is one possibility. Another meaningful and intimate route is through the impact on bodily hexis—Bourdieu’s term for the bearing of one’s body, the everyday expression of the habitus at the conative level. Bourdieu (2008:85) argues, “[b]odily hexis is above all a social signum” because it exists in the visual field as a legible record of one’s position in social space (misreadings and deception aside). Because hexis can be a marker of cultural and economic capital, it has consequential effects on social interaction. Analyzing the amorous pursuits of rural French bachelors, Bourdieu (2008:85–86) observes, “in the relations between the sexes, the whole bodily hexis is the primary object of perception,” so that being “clumsy, ill-shaven, ill-attired” can extinguish a romantic flame. Although the dominant inherit the embodiment of ease—and reap the rewards of such a performance—they can still be rumpled by pain. Appearing slow to react, having a hard time focusing, and other effects of pain can manifest at the level of hexis, where they may suggest awkwardness, disinterest, or worse. In typical circumstances, “habitus generates practices immediately adjusted . . . which are therefore perceived, by their author and also by others, as ‘right’, straight, adroit, adequate” (Bourdieu 2000:143). Because the inhibition of habitus by pain has a visually apparent effect on hexis, the signal function of habitus is disrupted, potentially exacting a social cost if one is made to look uncomposed (see Bourdieu 1984:207).
An important contribution to the medical sociology of chronic illness substantiates this point. In line with my argument—although not using a Bourdieusian framework—Kelly and Field (1996:246) emphasize “that to be acknowledged as competent social performers we have to be able to give the impression of some degree of control, use and presentation of our bodies.” The bodies of the chronically ill, they contend, “may inhibit the capacity to play social roles.” Emphasizing the signaling function of bodily hexis, Kelly and Field (1996:252) write, “Biological facts become social facts because others respond to the person in terms of their physicality.” As I argued previously, biological processes also influence tertiary habitus formation because biological facts “are also social facts for the individual because the individual sufferer is aware of, and has to take steps to cope with, that physical reality” (Kelly and Field 1996:252). Such coping strategies are shaped by the particularities of specific impairments. For example, visibly impaired individuals can develop strategies centered on the apparent source of their interpersonal deviance (Davis 1961), but the concealed nature of chronic pain means there is no visible explanation for one’s seemingly off behavior.
Hysteresis and Reflexivity
By arguing that pain can create a mismatch between one’s actions and social expectations, I am calling to mind one of Bourdieu’s central tools for reconciling habitus with broad social change—hysteresis. This is Bourdieu’s term for a habitus that persists in a field undergoing changes so profound and swift as to eliminate the conditions that gave rise to the habitus. 5 As he writes in Pascalian Meditations, “there is an inertia (or hysteresis) of habitus which have a spontaneous tendency (based in biology) to perpetuate structures corresponding to their conditions of production” (Bourdieu 2000:160). Bourdieu’s (2000:160) concept draws attention to the farcical incongruity such a state can entail, an observation that leads him to label hysteresis the “Don Quixote effect,” a nod to the character’s outdated belief concerning the social standing of knights. Although the inhibition of habitus can likewise generate a mismatch, it is not the field that has changed, but the bodily ability to actualize one’s habitus. In this way, inhibition by pain is less situational comedy and more personal tragedy.
Some of Bourdieu’s paradigmatic examples of hysteresis are the bachelors of rural France rendered ill suited for economic and romantic relations by the growing pull of urban life (Bourdieu 2008), the shifting of Algerian social terrain due to the imposition of colonial rule (Bourdieu 1977), and the overproduction of credentials that fueled the discontent of scholarly aspirants, new professors, and down-on-their-luck graduates culminating in May 1968 (Bourdieu 1988). Habitus, by definition, is adaptive, but these cases entail crises that span distinct fields, generating change too vast and sudden for reconditioning to keep pace. As Fowler (2020) argues, if synchronized crises produce a hysteresis effect, that can generate collective resistance to the structural conditions widening the gap between habitus and social space. Underlying this potential for resistance is a reflexive awareness that one was made for different times, a mass recognition Fowler suggests can be key to understanding how the dominated can advocate for change, as was the case in 1968. However, such reflexivity is not a destined byproduct of hysteresis—Strand and Lizardo (2017:180) specify that radical reflexivity arises when a sharply internalized order of succession is broken, a coming apart that reveals society’s arbitrary nature and invites new visions for the world.
While in general, Bourdieu stresses the unawareness with which people embody their habitus—its doxic character—hysteresis generates an awareness of domination when it draws attention to the distance between what feels natural and what is possible. The core of reflexivity is the recognition that fills the gap, a recognition that what previously felt like one’s nature is actually socially determined and thus precarious. Strand and Lizardo (2017:178) characterize the reflexiveness that derives from hysteresis as a predictable effect of the distinct evolutionary rhythms found in bodies and structures, namely, the “asynchronicity between the (slower) temporality of practice and the (faster) temporality of environments.” If reflexivity can emerge from the relationship between habitus and social structures, could it also emerge from the relationship between biology and habitus? The argument that pain can produce reflexivity is lurking within an influential concept from medical sociology—biographical disruption. Bury (1982) introduced this concept to make sense of how individuals with rheumatoid arthritis navigate a life with chronic pain. Biographical disruption positions scholars to grapple with the impact of chronic illness on both the afflicted individual and the individual’s social network, which is strained by an ongoing need for assistance. Most poignantly, this concept emphasizes that for the ill, one’s well-laid life plans may no longer be feasible. The “disruption” is to a degree forward looking—how a person imagined their biography playing out is disrupted, which has implications for one’s sense of identity. 6
In his original article, Bury (1982:169) emphasized an additional point: In a life with pain, “there is the disruption of taken-for-granted assumptions and behaviours; the breaching of common-sense boundaries. . . . This ‘what is going on here’ stage involves attention to bodily states not usually brought into consciousness and decisions about seeking help.” This language evokes an awareness of the inhibition of habitus, a sense that one is no longer quite themselves. In Bury’s (1982:169) telling, chronic illness renders the previously unfelt structure of habitus tactile because one is no longer able to behave as they are conditioned to do: “My contention is that illness, and especially chronic illness, is precisely that kind of experience where the structures of everyday life and the forms of knowledge which underpin them are disrupted.”
Bury did not explore a connection to Bourdieu, but evidence for this relation is strong. For example, Bury (1982:175–76; emphasis added) found among his subjects that “[m]aintaining normal activities, for example being able to sit in one position for a long period of time at a cinema, or maintaining normal appearances in a social gathering at a club or pub, have to become deliberately conscious activities, and thus frustrating and tiring.” The “normal” is a dispositional investment that lives on through one’s habitus, an investment one is now inhibited from realizing. By “deliberately conscious,” Bury is highlighting the recognition of something previously unfelt and easy but now actively striven for—in this situation, the presentation of self becomes effortful or impossible as inhibition works faster than the revision of habitus. In short, there is a recognition that what felt like one’s nature depended on a particular body.
Why such somatic self-awareness matters for social theory is not obvious. Both hysteresis and biological inhibition dislodge the reciprocity between habitus and social space, but hysteresis does so for a class of social actors all at once. In this way, even if it creates social disorientation, it is a collective experience of disorientation. Under such conditions, there is the possibility that actors will recognize the structural determinants of the hysteresis effect. Although this could lead to resignation—especially for the formerly dominant who benefited from the old ways—it could also lead to collective action (Fowler 2020). This was the case in 1968, but its collectivizing effects are not necessarily revolutionary. Strand and Lizardo (2017:183) note that when hysteresis is marked by a strong, lingering investment in ways of life no longer suited to the environment, then the preservation of such beliefs “becomes a project,” a situation they add is ripe for reactionary politics. Unlike hysteresis, pain is a biological process that individualizes and particularizes; its onset is contained within the organism. On the other hand, it is socially patterned—this is true both in the sense that certain neighborhoods, occupations, and identities have higher rates of pain and in the sense that reactions to pain are socially patterned. Health-seeking behaviors are shaped by class, and the dominant often benefit from these patterns (Allen 2004).
Although the bio-habitus is a tool for explaining individual particularity, it in no way denies the power of social forces to structure society. But the addition of biology to habitus sheds light on the fact that against the patterning of pain, the subjectivity of pain creates a self-understanding dominated by the isolating experience of suffering. This is a process of becoming solitary, an entanglement of identity with pain that clinicians have studied for its pernicious effects. In the field of clinical psychology, Pincus and Morley (2001) 7 term this self-pain enmeshment. The intuition is that for the chronically ill, the routine experience of pain calls to mind the negative consequences of one’s illness. For those who frequently experience pain, this can cascade into a sense of self dominated by the perceived limitations of one’s illness. This resonates with Bury’s (1982) concept of biographical disruption, but Pincus and Morley emphasize a different angle, namely, that the suffering such enmeshment entails will amplify the cognitive effects of pain, an argument borne out by multiple patient studies (e.g., Paschali et al. 2021). The physician philosopher Leder (1990) makes a similar argument about pain in his phenomenological study, The Absent Body. Whereas biological structures generally obscure the body’s presence and enable attention to emanate outward, pain creates “a phenomenologically ‘centripetal’ force, gathering space and time inward to the center. We are ceaselessly reminded of the here-and-now body” (Leder 1990:76). Leder contrasts this experience with outward-oriented pleasures, which “tend to maintain our intentional links with other people” (Leder 1990:75), whether through eating or sex. Whereas pleasure increases social density, “pain tends to induce self-reflection and isolation” (Leder 1990:75). Within pain, a relationship develops, but it is one to a previously unthought body that “emerges as an alien presence” (Leder 1990:76).
This is a form of reflexivity where the self comes to be understood as dominated by pain, a take that is markedly different than the reflexivity that appears in Bourdieu’s research on hysteresis. The closest corollary is the lonely rural bachelor, whose cultural shortcomings are experienced as “an unhappy consciousness of his body” (Bourdieu 2008:86). Even though this is isolating, the bachelor hovers off the dance floor in a crowd of men just like him. Instead of creating the potential for social solidarity, the reflexivity of inhibition pushes one toward identification with their biological organism. The effects of inhibition distinguish it not only from hysteresis but also from Bourdieu’s related concept of cleft habitus, that is, the accumulation of dispositions that work at cross-purposes. Most notably, Bourdieu (2007) identified his own primary habitus acquired through his rural upbringing as being in tension with the secondary habitus he developed through his elite education. A cleft habitus can induce suffering, but it is marked not by isolation but rather, a social overcommitment “to successive allegiances and multiple identities” (Bourdieu et al. 1999:511). In contrast, not only does pain particularize, its centripetal force distances one from the social world.
However, this is only the subjectivity of pain; moving to a structural vantage reveals that although the experience of pain may alienate, the distribution of pain conditions is socially patterned. In the United States, for example, rates of chronic pain are, according to the CDC (2018), “higher among women, adults who had worked previously but were not currently employed, adults living in or near poverty, and rural residents.” This CDC report goes on, evoking the privilege of the unencumbered bodies centered in Pascalian Meditations (Bourdieu 2000): “In addition, the age-adjusted prevalence of chronic pain and high-impact chronic pain were significantly lower among adults with at least a bachelor’s degree compared with all other education levels” (CDC 2018). The role of education in shaping the social patterning of chronic pain has received much recent attention due to the work of economists Case and Deaton (2020). Their research into “deaths of despair” uncovered what one commentator (Epstein 2020) calls the “pain paradox”—pain is higher in each successive generation of non-college-educated white Americans since the Baby Boom despite medical advances and increased workplace safety. This means that, for example, the cohort born in the 1970s had as much pain in their 40s as the cohort born in the 1930s had in their 60s (Case and Deaton 2020:89). This is not the case for college-educated white Americans, whose pain increases with age along a similar path for all recent cohorts.
Why are non-college-educated white Americans in so much pain? Case and Deaton (2020) argue that a tectonic socioeconomic dislocation predisposes such individuals to pain: This group has been hit hard by the decline of industries that for decades provided stability, if not prosperity; and although non-white Americans have lower wages than white Americans, the former have experienced a relative degree of upward mobility. For non-college-educated white men, income has declined since 1979 (Case and Deaton 2020:7). This history suggests a classic account of hysteresis: Economic conditions and relative social standing shifted faster than a population could be reconditioned. But what does it mean that for a large section of this class, the immediate experience of this shift is mediated by the biological process of pain? The reflexivity engendered by pain entails suffering, but it offers no obvious target for resistance beyond one’s failing body. The students of 1968 could turn on the university that failed to prepare them for the world beyond or the employers who refused to hire them despite their credentials. Lower back pain has no obvious revolutionary implications—as one is pulled toward an identification with pain, the structural source of suffering recedes from view.
This is not to overstate my case and argue that being in pain fully obscures a structural imagination—movements have indeed centered pain conditions (Barker 2002). However, by generating a biological self-consciousness, self-pain enmeshment seems unlikely to produce a reflexivity conducive to solidarity. Instead, it engenders a form of suffering that fosters disengagement and differentiation. The cost of such pain is manifest in this group’s declining longevity due to deaths of despair, whether from alcohol abuse, drug overdose, or suicide. As Case and Deaton (2020) note, the structural forces instigating this suffering recall Durkheim’s (1979) study of suicide—their argument suggests the anomic form is key, although the state of reflexivity produced by inhibition is closer to egoistic suicide. 8 But what about politics? In today’s political moment, the U.S. white working class has become a common shorthand for reactionary populism. The affectivity generated by such suffering may have become articulated into the GOP’s resentment-soaked politics (Silva 2019), but it is also the case this group tends to be politically disengaged—white Americans without a college degree are far less likely to vote than are college-educated white Americans (Frey 2023). Pain may be relevant to the partisan divide, adding fuel to our political fire, but it may also be key to the “the other divide” (Krupnikov and Ryan 2022) shaping national life, that between the politically engaged and the disengaged.
Discussion
In Pascalian Meditations, Bourdieu (2000) includes a footnote directing readers toward L’Homme Neuronal, a 1983 work of pop neurology by his Collège de France colleague Jean-Pierre Changeux. The footnote offers no elaboration, but the suggestion is likely due to the book’s recounting of how neurons are both adaptive and resistant, changing over time but harder to rewire the longer they have been conditioned—in short, Changeux provides a biological basis for habitus. With some reservations, others have advanced this footnote, finding that habitus resonates with the dual process theory of cognition (Vaisey 2009) and the neural basis of learning (Elder-Vass 2007).
Whereas these works pinpoint the biological processes responsible for socialization, I follow pain science into the bio-habitus, demonstrating how the body pushes back against socialization. To illustrate this point, I moved in two analytic directions; although separated for presentational clarity, the key is that action flows from the interaction of “bio” and “habitus.” I first argued that habitus mediates the experience of pain, particularly through the effect of pain beliefs (cast as cognitive dispositions) and the development of avoidance behaviors (tertiary habitus formation) in response to pain. On the other hand, I argued that pain’s impact on cognition and affect demonstrate its ability to inhibit habitus by diminishing one’s attentional capacities. Such an interaction interrupts the link between stimulus and reaction wherein habitus is triggered as well as the ongoing reconditioning of habitus. Pain-driven inhibition offers a novel defense against a major criticism of habitus, namely, that it fails to explain how difference develops among individuals in similar social locations. By inhibiting habitus, pain can disrupt the correspondence between structure and self, thus serving as a source of intimate particularity. Although this self-structure mismatch evokes Bourdieu’s hysteresis, I argue it has an alienating effect, cutting individuals off from the social world as their reflexive self-awareness becomes weighted by the experience of pain.
Given that chronic pain is a condition often studied by disability scholars, there is potential for the bio-habitus to serve as a new topic (Wacquant 2011) of research in this literature. But first, it is important to recognize that disability scholars have made claims that resonate with those I advance here. As one example, whereas the social model perspective pushes against biology’s explanatory power, my description of the bio-habitus echoes Hall’s (1999:144) claim that the body “absorbs and reacts to biological and social processes in a never-ending process.” Such a perspective is also present in the feminist critique of the social model, which spotlights the embodied experience of suffering, an experience the distinction between impairment and disability occludes. As a prominent example, Wendell (1989:107) writes, “I prefer to use a single term, ‘disability,’ and to emphasize that disability is socially constructed from biological reality.” Of course, both Hall and Wendell follow in a much longer tradition aimed at overcoming Cartesian dualism (Merleau-Ponty 2012). Another convergence concerns my argument that as biological impairment disrupts habitual action, it can generate a reflexive awareness that taken-for-granted social arrangements inflict disability. Although I relied on Bury (1982) to substantiate this claim, there is a rich literature documenting the subjectivity of disability. As one example, through interviews with the physically disabled and their caregivers, Engman and Cranford (2016:34) identify the pervasiveness of techniques to “mitigate the failure of the material world to anticipate [impaired] bodies.” The authors stress the sense of precarity such adaptation entails, a state that forces individuals to constantly and effortfully problem-solve an environment made for different bodies.
Engman and Cranford (2016) are interested in habitual action, but their intervention works more through Dewey than Bourdieu. In disability studies, there are scholars working explicitly in the Bourdieusian tradition. Allen (2004) studied class-privileged and disadvantaged children who are visually impaired, finding that his wealthier subjects were trained in bodily techniques that resisted the effects of disability. This points to an important dynamic in the bio-habitus I did not emphasize here, namely, that the habitus shapes health-seeking behavior, which can, in turn, feed back into the “bio” of the bio-habitus. Edwards and Imrie (2003) provide another insightful contribution, documenting the subjectivity of disability and theorizing how habitus moves beyond the tension between the social model of disability and the dominant medical perspective. In the former, disability emerges from social arrangements and norms, whereas the latter attributes it to biological failure. Against the social model, Edwards and Imrie recenter the body, but they do so while retaining a critical view of medical knowledge. As they argue, medical expertise categorizes and reifies “dominant bodily forms” (Edwards and Imrie 2003:245) that accrue capital across a range of fields, a process that devalues impaired bodies. When individuals experiencing disability internalize their devaluation as the natural order of things, they become, in the language of Bourdieu, victims of symbolic violence.
Disability scholars have long chronicled the pernicious effects of medical expertise that classifies bodies as healthy or ill, normal or abnormal (Oliver 1996). But just as Edwards and Imrie (2003) use the concept of habitus to recuperate the body as a tool for a critical perspective on disability, the bio-habitus can recuperate medical expertise for a critical view of impairment. To understand the particularity of the experience of chronic pain, we must reckon with its effects on cognition and affect. This is not because pain can be reduced to a biological process but because the biological process driving pain interacts with the learned dispositions entailed by habitus. Social scientists are adept at studying behaviors and documenting how those behaviors are structured by one’s position in social space, but the bio-habitus invites an exchange with biomedical expertise. Such an exchange will shed light on the give-and-take between the biological organism and the socialized subject and, in this way, offer a deeper understanding of disability. This article begins such an exchange with pain science, but pain is far from the only biological process confronting the disabled. This is not a call to embrace biomedicine at its word—caution is called for, especially when the study of biological processes is heavily clouded by social connotations, as with mood disorders and cognitive impairments. Autonomy is never guaranteed for any scientific field, especially one that generates as much revenue as the biomedical field. Symbolic power lurks within its proclamations, but it is possible the field’s knowledge can be put to critical purposes, too.
Footnotes
Acknowledgements
Thanks to Michael Burawoy for teaching me how to hold a conversation with Bourdieu and for the encouragement to sustain it to the end. Thanks also to Loïc Wacquant, whose bootcamp helped me understand what the exchange means. This article benefited tremendously from feedback offered by Allen Micheal Wright, Isaac Dalke, Emily Ruppel, and members of Berkeley Sociology’s Gender/Sexuality workshop. For their biomedical expertise, I am indebted to Spencer Dunleavy, Lara Berliner, and the team at the UCSF Headache Center. Finally, five anonymous reviewers (one of whom suggested the bio-habitus concept) pushed this article toward greater precision and ambition.