
Abstract
Since the beginning of 2020, the COVID-19 pandemic has placed additional pressure on the supply of healthcare services. This study aims to explore profiles of public service motivation among healthcare workers during a pandemic. A total of 318 questionnaires were completed for two measurement times (T1, n = 171 and T2, n = 147). The study’s mixed-method design identified three profiles: (1) The devoted, (2) the disenchanted, and (3) the limited self-sacrificing. Results also revealed three main factors that may affect motivation in healthcare workers during the COVID-19 pandemic: (1) valorization, (2) leadership, and (3) job design. This study contributes to a better understanding of the organizational and human issues of motivation for public service during a pandemic.
Points for Practitioners
Public organizations’ managers should assess job applicants’ motivation when making selection decisions. This assessment can be done in the job offer, in the application analysis, or through questions during interviews.
Public organizations should use management practices such as employee appraisal, transformational leadership, or person-job fit to maintain a certain level of public service motivation.
Organizational policies should focus on preventing presenteeism by reducing excessive stress, enhancing public service motivation, and improving the health and well-being of healthcare professionals.
Introduction
Frontline workers are critical to effective healthcare delivery in public services (Bielicki et al., 2020). In particular, the COVID-19 pandemic highlights the importance of reliable and responsive healthcare systems (Di Ruggiero et al., 2020). Since the beginning of 2020, the COVID-19 pandemic has placed additional pressure on health services. This public health emergency generated new stresses, emotions, and concerns among healthcare professionals (Bielicki et al., 2020).
The desire to serve the public, interact directly with citizens to make a difference, or contribute to the public interest is deeply connected to the notion of Public Service Motivation (PSM). PSM is defined as “the beliefs, values, and attitudes that go beyond self-interest and organizational interest, that concern the interest of a larger political entity, and that motivate individuals to act accordingly whenever appropriate” (Belrhiti et al., 2019, p. 1).
The concept of PSM emerged during the 1970s in the United States (Perry & Wise, 1990; Rainey, 1982) and, since then, has spread to several public administrations worldwide (e.g., Mussagulova & van der Wal, 2021; Perry et al., 2010; Ritz et al., 2016). PSM brings a counter view to the dominant and somewhat cynical view of self-interested and extrinsically motivated public servants (Mussagulova & van der Wal, 2021). However, PSM and its contextual specificity in the Western healthcare system during a pandemic remains poorly understood (Raven et al., 2018, p. 2).
This study explores PSM in frontline healthcare workers (e.g., nurses, medical attendants, physicians, paramedics, and technicians) during the COVID-19 pandemic in Quebec, Canada. Overall, this study has two primary objectives. First, it aims to explore profiles of PSM and their evolution among frontline healthcare workers during the pandemic. Second, it seeks to explore contextual factors that can affect PSM of frontline healthcare workers during the COVID-19 pandemic. Given the paucity of literature on healthcare worker PSM during pandemics and the few longitudinal studies (Christensen et al, 2017; Hameduddin & Engbers, 2022), this study aims to address this knowledge gap by exploring factors that may affect motivation according to the PSM (Bland et al., 2021). This new knowledge could enable better PSM and encourage policymakers to implement behaviors that support healthcare workers’ motivation to provide care during pandemics. To achieve these objectives, this study uses two time points for measuring PSM to better understand the effects the pandemic context has had on PSM. Still, too few studies have used longitudinal approaches to study PSM, and this study addresses that gap (Christensen et al., 2017; Hameduddin & Engbers, 2022; Harari et al., 2017; Piatak et al., 2021).
Moreover, a broader range of contextual elements is considered to provide relevant information on the factors influencing PSM’s impacts on various outcomes. This study responds to invitations from Awan et al. (2020, p. 633) and Mussagulova and van der Wal (2021, p. 23) to conduct studies in this area. Furthermore, Harari et al. (2017) explained in their meta-analysis the need to develop strategies for using the knowledge generated in the PSM literature to advance public management practices. This research also responds to this invitation by exploring PSM profiles that can simplify managers’ use of this concept. The complexity and interconnectedness of the many decisions made by public sector managers require empirical researchers to make simplifying assumptions about measuring and categorizing individuals’ behavior (Pedersen et al., 2019). On this basis, the profiles we bring to the categorization of PSM are justified both empirically and theoretically. The profiles are empirically justified because they enable a finer categorization of individuals’ PSM (e.g., Raven et al., 2018). They are theoretically justified because the profiles highlight PSM variability among individuals that previous studies had not explored much.
Moreover, the cluster approach allows researchers to better understand the similarities between individuals (e.g., Harari et al., 2017; Pedersen et al., 2019). In this article, cluster analysis is used to explore types of PSMs of frontline health workers reflecting patterns of PSM combinations. This new approach to the empirical study of PSM is helpful for extending and complementing the results of studies using other sets of simplifying empirical assumptions (Pedersen et al., 2019). This classification allows for an initial model to investigate PSM in pandemic-like settings and a limited number of individuals to be circumscribed. This new classification allows for the definition of baseline profiles, which can be examined in light of empirical data and, thus, clarify the results obtained with measurement scales that are often difficult to interpret for practitioners.
The results of this study highlighted three profiles of PSM and three determining factors in the evolution of PSM during the pandemic. The profiles include; (1) the devoted, (2) the disenchanted, and (3) the limited self-sacrificing. Conversely, the three evolutionary determining factors include; (1) valorization, (2) leadership, and (3) job design. This article’s main contribution to the literature on PSM is to clarify its evolution and contributing factors among frontline workers during pandemics, such as COVID-19. Previous research has not paid sufficient attention to the contextual factors that interact with PSM during a crisis like the pandemic of COVID-19 (Bland et al., 2021, p. 1). Additionally, as Raven et al. (2018, p. 2) highlighted, there is little research on how healthcare workers experience and cope with epidemics, and this research also addresses this gap.
The remainder of this article is divided into four sections. The first section introduces the PSM model and the context of the study. The second section explains the study’s methodology, and the third section provides the analyses of the results. Finally, the last section presents the study’s discussion, limitations, and conclusions.
PSM; the Heart of Public Management
An important development in PSM research is a scale to measure public service motivation (Perry, 1996). A short form of the scale was first fielded prior to the publication of the full scale in 1996. This scale stimulated a relatively large body of subsequent research on PSM (Perry, 2014; Wright et al., 2013). PSM is viewed as an individual’s orientation toward providing services to people to do good for individuals and society (Hondeghem & Perry, 2009, p. 6). It was initially conceived as a predisposition rooted in public institutions and organizations (Perry & Wise, 1990). Since that time, considerable evidence suggests that PSM exists in the nonprofit sector (Lee, 2012; Park & Word, 2012) and in socially oriented businesses (Hameduddin & Engbers, 2022). PSM can thus be viewed as a broader set of beliefs, values, and motives that lead individuals to look beyond self-interest to a larger political entity (Vandenabeele, 2007). When viewed as a more general non-public structure, it is similar to pro-social motivation (Wright et al., 2013).
Researchers from many countries have also contributed to the literature about the antecedents and consequences of PSM. Some models have focused more on actors’ reward preferences (e.g., Gabris & Simo, 1995), while others have focused on employee behaviors (e.g., Brewer & Selden, 1998; Kjeldsen, 2012; B.Liu & Perry, 2016). PSM has been the subject of much scientific research and has been linked to a wide range of desirable behaviors, such as job performance (Alonso & Lewis, 2001; Andersen et al., 2014; Kroll & Vogel, 2014; Wright & Grant, 2010), organizational commitment (e.g., De Simone et al., 2016), job satisfaction (Taylor & Westover, 2011; Wright et al., 2013), attraction to public service (Carpenter et al., 2012), and ethical behavior (Hameduddin & Engbers, 2022).
The research interest in PSM underscores the potential of this motivation for public sector organizations (e.g., Awan et al., 2020; De Simone et al., 2016) and may explain the effort of healthcare workers in personal care or service activities (Piatak & Holt, 2020; Prebble, 2016). PSM leads public sector workers to a higher level of enthusiasm and dedication, leading them to work harder and be socially engaged (De Simone et al., 2016). This enthusiasm and dedication thus increase the likelihood of presenteeism (Jensen et al., 2019). Presenteeism is “the tendency to show up for work even though one is feeling unwell” (Johns, 2006, p. 396). Public leaders can also change their employees’ PSM through leadership by getting them to see beyond self-interest and be motivated by experiences and identities (Paarlberg & Lavigna, 2010). Leaders who clarify their vision can better get employees to see what they are contributing to and thus are more motivated by public service (Andersen et al., 2016; Johnston et al., 2001).
Although public service motivation may exhibit consistency as a universal phenomenon (Vandenabeele et al., 2006), the concept takes on a unique flavor depending on the national context (Hameduddin & Engbers, 2022; S.Kim & Vandenabeele, 2010). Much of the research on PSM has been conducted in different countries with numerous cultures. However, this multicultural body of literature raises several important questions regarding PSM’s cross-cultural applicability ( S.Kim et al., 2013). For instance, S.Kim et al. (2013) conducted a survey (n = 2,868) in 12 countries. The revised dimensions and items were then tested internationally to isolate a set of universal dimensions. The authors also determined how much these dimensions’ average was shared across the surveyed countries. They then proposed a four-dimensional model and a 16-item measurement scale ( S.Kim et al., 2013). These dimensions are very similar to the ones initially proposed by Perry (Meyer-Sahling et al., 2020).
The first dimension is Attraction to Public Service (APS), referring to the rational motive. This dimension emphasizes the willingness to serve the public, work for the common good, and participate in public policy development and implementation processes. The second dimension refers to the level of Commitment to Public Values (CPV). This dimension assesses how much individuals share a set of values (equality, continuity, and consideration for future generations and ethics). Commitment to the public interest refers to normative motives regarding civic duty and social justice. The third dimension is compassion (COM). While this dimension is also based on Perry’s (1996) scale, the items consider identification with others’ suffering. Compassion refers to affective and benevolent motivation, defined as love and the desire to protect fellow citizens. Schott and Ritz (2018) argue that the PSM dimension of compassion “captures the emotional state of empathy and identification with specific unprivileged or weak groups” (p. 34), and is likely to play a stronger role than the other three PSM dimensions. The last dimension is self-sacrifice (SS). More than the third dimension, this one is strongly informed by Perry’s (1996) scale. It refers to people’s willingness to substitute intangible rewards for tangible rewards for service to others. Self-sacrifice includes affective and normative components and refers to altruism, which is at the heart of PSM.
Given its rise in popularity, a number of researchers have synthesized existing research on PSM to identify gaps in the literature and suggest future research (e.g., Hameduddin & Engbers, 2022; Harari et al., 2017; Piatak et al., 2021; Ritz et al., 2016). Researchers have engaged in much debate, found inconsistent results, and have accumulated numerous unanswered questions (Awan et al., 2020; Piatak & Holt, 2020; Piatak et al., 2021; Ritz et al., 2016). One such question is whether PSM evolves or remains stable over time. First, the theoretical orientation associated with social learning results in a dynamic view of PSM (Hameduddin & Engbers, 2022). Conversely, personality theory suggests a more static orientation, which independently predicts a range of occupational behaviors (Hough et al., 2015). Personality theory suggests that early life experiences and perhaps even biological influences (Bouchard et al. 1990; Charbonneau & Van Ryzin, 2017; Funder, 2001) are critical to the development of PSM and that this trait has behavioral ramifications for later attitudes and behaviors in people’s work life. Although contextual differences are important in predicting individual behavior, traits have been shown to consistently predict behaviors too, such as job performance (Hameduddin & Engbers, 2022; Judge & Ilies, 2002). Given this predominant view of PSM (Perry & Wise, 1990), and its association with personality traits (Jang, 2012), many authors report that PSM would be relatively stable over time despite environmental influences (Jeong et al., 2022; McCrae, 2000; van Loon et al., 2020; Vogel & Kroll, 2016). For example, Vogel and Kroll (2016) examined MSP-related values of three cohorts of individuals across time and found general stability.
Finally, it is important to note that the pandemic has fundamentally altered the nature and demands of public sector work. Moreover, few PSM studies have been conducted in the context of this pandemic (Ye et al., 2021). However, the pandemic presents new challenges for healthcare professionals. For instance, it creates a dilemma for healthcare professionals between self-protection and service delivery (Møller, 2021). Second, it creates significant organizational pressures (Ghanayem et al., 2020) that can lead to burnout (Bakker et al., 2017), sick leave (Petersen et al., 2019), demotivation (Parker et al., 2017), and declines in performance (Schuster et al., 2020). Additionally, pressures outside the workplace (e.g., daycare and school closures) force healthcare workers to find a way to balance work and personal obligations during work hours (Ye et al., 2021). Throughout the COVID-19 pandemic, work demands on PSM increased while work resources, such as equipment and co-worker support, decreased (Ye et al., 2021). As a result, healthcare workers may exhibit less commitment and motivation to work (Bakker et al., 2014; Parker et al., 2017). The following section further describes the unique context of this study.
Evolution of the Government Response to the First Two Waves of COVID-19 in Quebec
The first case of COVID-19 reported in the Canadian province of Quebec was on February 27, 2020. Only 2 weeks after these events, the Quebec Government adopted sanitary measures, attempting to control the spread of the virus. These measures included directives concerning the isolation of travelers, prioritization of teleworking, and restrictions on gatherings and travel (Institut national de santé publique du Québec [INSPQ], 2022). Despite the various implemented measures, cases multiplied due to community transmission, reaching over 10,000 infected in Quebec by April 7. However, the situation seemed to be under control then, and the provincial government announced a softening of sanitary measures at the end of April (INSPQ, 2022). The government authorities announced on July 11 the end of the first wave of COVID-19 (February–July 11, 2020).
The second wave began at the end of August of the same year (August 2020–March 2021), which was virulent and spread rapidly (INSPQ, 2022). Thus, new sanitary measures, such as wearing masks in public places, became a daily reality for the population. In September 2020, a new regional alert system to adjust health measures according to risk levels became operational (INSPQ, 2022). Despite all these efforts, the number of active cases exceeded 100,000 by October. The Minister of Health and Social Services asked the population to limit their physical contact as much as possible for 28 days (October 1–28, 2020). The second wave was also associated with increased coercive measures (INSPQ, 2022). For example, police checkpoints were deployed all over Quebec to limit travel between regions and enforce compliance with sanitary measures. Health professionals were also very affected by this second wave. According to data from a study conducted by the National Institute of Public Health (INSPQ, 2021), nearly half of healthcare workers (48%) during the second wave reported a high or very high level of psychological distress. Many workers with COVID-19 reported not having the resources to do quality work (75%) or having to work inconsistently with their professional conscience (52%) (INSPQ, 2021). The absenteeism rate in the latter wave reached nearly 8,000 workers in January 2021 (Bélair-Cirino, 2021). These absences, combined with the nearly 100% increase in COVID-19 cases requiring hospitalization in the second wave compared to the first, put a strain on the continuity and quality of healthcare services. Despite the significant changes in the work context of healthcare workers, to our knowledge, no study had previously examined the impact of the healthcare crisis on the evolution of motivation for public service.
Methodology
The primary objectives of this study are to (1) to explore PSM profiles and (2) contextual factors that can affect the PSM of frontline healthcare workers during the COVID-19 pandemic. This study uses a mixed-method design with a nested concurrent strategy to achieve these objectives (Newman et al., 2003; Tashakkori & Teddlie, 2003). For this design, data are collected and analyzed concomitantly. In other words, qualitative and quantitative approaches are employed simultaneously. This strategy has the advantage of integrating multiple perspectives to study interventions, particularly in the healthcare field (Guével & Pommier, 2012; Johnson et al., 2007).
Sample and Data Collection
Potential participants were recruited on Facebook through posts on ten dedicated closed Canadian healthcare worker groups (Appendix 1). These groups aim to promote a coherent collective movement of healthcare workers throughout Quebec. This includes all the actors who collaborate with nurses to offer quality care, such as orderlies, ambulance attendants, radiology technicians, laboratory technicians, and physicians. Similar to several other studies, respondents were selected non-randomly through convenience and snowball sampling methods (e.g., Bujold et al., 2022; Halley et al., 2018; Leighton et al., 2021; McRobert et al., 2018). Snowball sampling is the most widely used sampling method in qualitative research in social science (Dosek, 2021; Noy, 2008). The use of digital social media to reach potential respondents provides a broad opportunity to reach a large number of respondents (Bujold et al., 2022; Evans & Mathur, 2018). Indeed, Leighton et al. (2021) have demonstrated that collecting data using snowball sampling via social media is an effective and efficient way to increase sample size and reduce completion time. Several authors have previously used this recruitment method in their studies (e.g., Halley et al., 2018; King et al., 2014; McRobert et al., 2018).
To participate in the study, individuals had to meet the following criteria: (1) be 18 years or older; (2) be a frontline healthcare worker; and (3) have worked in the public sector during the COVID-19 crisis. A distinction was made regarding participants who work in hospitals and those who work outside of hospitals (e.g., long-term care facilities, paramedics, outpatient clinics, and medical clinics).
The preferred collection tool is the questionnaire. The questionnaire consists of two sections. The first section contains S. Kim et al.’s (2013) 16-item Likert scale of PSM measurement, including four questions per dimension. The second section has seven open-ended questions allowing respondents to elaborate on their thoughts (e.g., Would you mind doing the same job in the private sector for the same salary and why? Have your perceptions changed since the pandemic began?). These questions were designed to better understand the dimensions of the PSM and the context associated to COVID-19 pandemic. A table of these questions is available in Appendix 2.
To recruit participants, we proceeded in two steps. First, we identified Facebook pages dedicated to frontline healthcare professionals and applied to join the group. To gain access to the members of a page, one must first be a member of the page. After being accepted by the groups’ administrators, Facebook posts were made to ten previously identified groups. For social media groups requiring approval to post a recruitment post, group administrators were contacted by private message to post an invitation on their page with the link to the survey. The ten Facebook groups reach a potential 106,000 healthcare workers (Appendix 1). It is important to note that although some groups have several thousand members, this number does not guarantee that they are active members or that members see the publication in their Facebook news feed inviting them to participate in the study. The number of publications can sometimes reach 70/day, depending on the group.
A total of 2,903 participants viewed the publication and accessed the questionnaire during the study period. Participants retained for the remainder of the study were those who had fully completed the questionnaire and submitted their consent forms (n = 318). In the end, 11% of potential participants who saw the publication and accessed the questionnaire participated in the study. Calculating the number of potential participants by clicks is a recognized approach in studies based on social media data collection (e.g., Evans & Mathur, 2018; Halley et al., 2018).
Additionally, data collection was conducted in two phases; T1 in April 2020, which was the first wave 1 of COVID-19, and T2 in October 2020, the second wave. A total of 318 questionnaires (n = 318) were completed for both measurements (T1, n = 171; and T2, n = 147). Of the 318 completed questionnaires, 66 participants (21%) responded to both measurement times. T1 participants who agreed to be contacted again for a second survey voluntarily provided their email addresses. T1 participants were used to develop PSM profiles (n = 171), and T2 participants were employed to validate the profiles and address the factors influencing PSM. Table 1 presents the participants’ characteristics.
Participant Characteristics
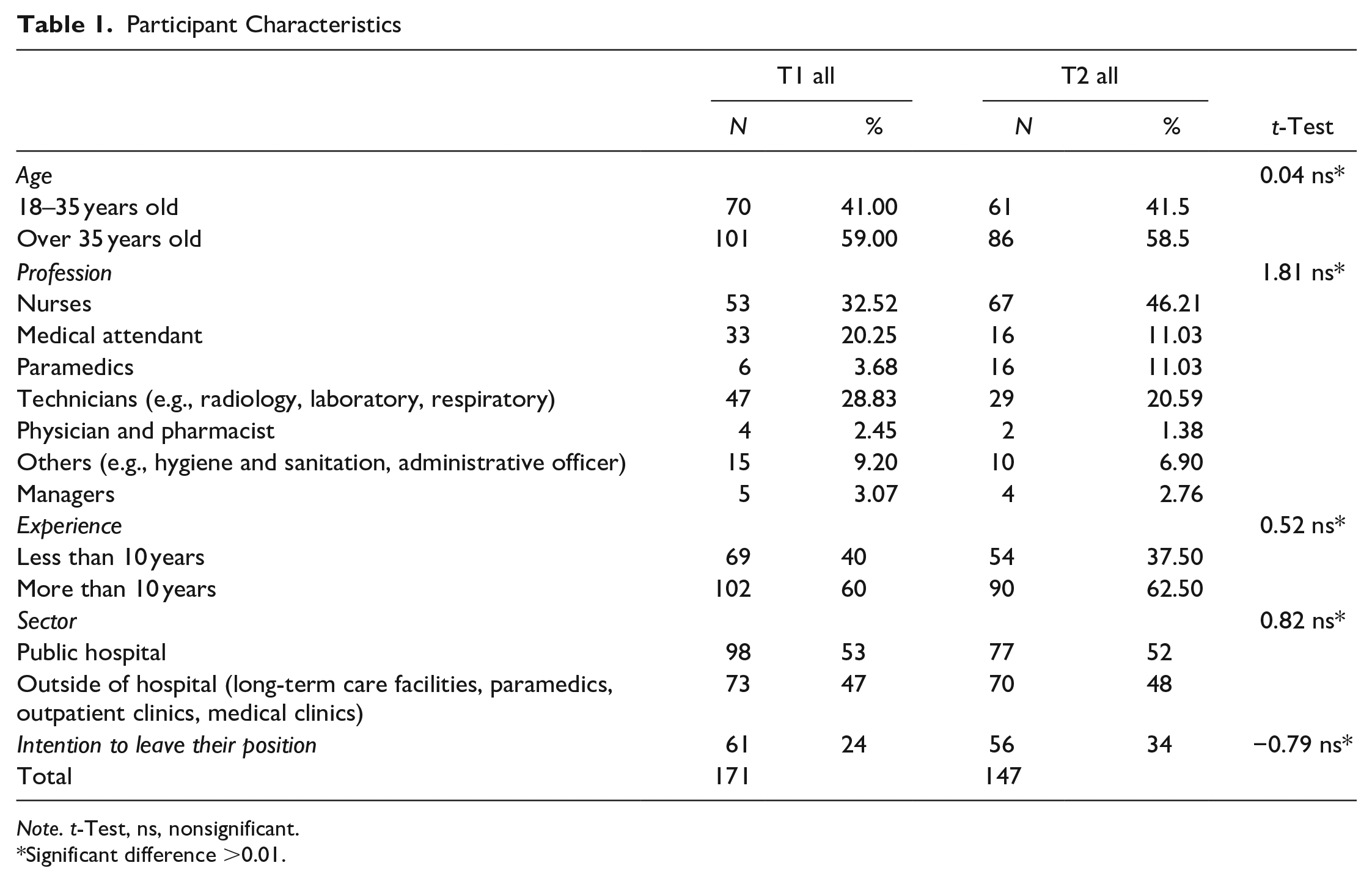
Note. t-Test, ns, nonsignificant.
Significant difference >0.01.
Table 2 shows the mean results obtained for the four PSM dimensions and global PSM at the first and second measurement times.
Descriptive Statistics for Indices
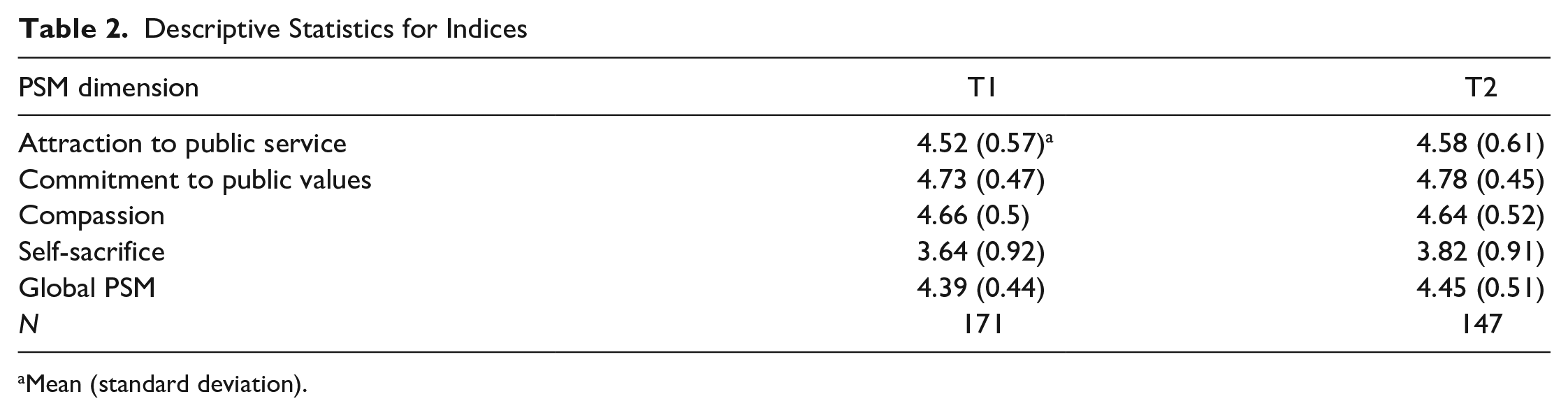
Mean (standard deviation).
Data Processing and Analyses
Data analyses were performed in two stages: (1) cluster analyses and (2) qualitative analyses using inductive coding.
Cluster Analyses
The results obtained with the PSM measurement scale were compiled (creation of indexes) for each scale dimension. Cluster analyses were performed using STATA version 16.0.810 to create PSM profiles. This statistical analysis method was chosen because it organizes the raw data into homogeneous silos by creating groups that share similar characteristics (Everitt et al., 2006). These silos can, in turn, highlight subsets and subconcepts that would otherwise be indistinguishable and thus capture their particularities (Everitt et al., 2006; Hair et al., 2019). Specifically, cluster analyses were conducted in four steps: (1) purpose and clustering variables; (2) sample and data preparation; (3) clustering strategies; and (4) group interpretation and classification validation (Hair et al., 2019; Lestage et al., 2014).
First, the exploratory perspective was favored over the confirmatory perspective because it is the most frequently used approach for cluster analysis (Lestage et al., 2014). Next, the sample was defined, and the data were prepared. Cluster analyses were conducted on the participant sample from T1 (n = 168). Formann (1984) suggested that the minimum sample size for cluster analyses should be no fewer than 2k cases (k = number of variables), and preferably 5 × 2k. Therefore, the minimum sample size for this study is 40 (i.e., 5 × 2[4]). The data were then prepared for analysis. The Euclidean distance was used to measure distance because it allows a simple interpretation of the distance between two observations (Hair et al., 2019). The four indexes, which are continuous variables, were created with the four items in a Likert scale from 1 to 5 for each of the four dimensions. To create profiles as close to the measurement scale as possible, the complete set of PSM variables was retained. Then, a correlation matrix and VIF analysis were performed. No variable showed a multicollinearity problem when analyzing variance inflation (VIF).
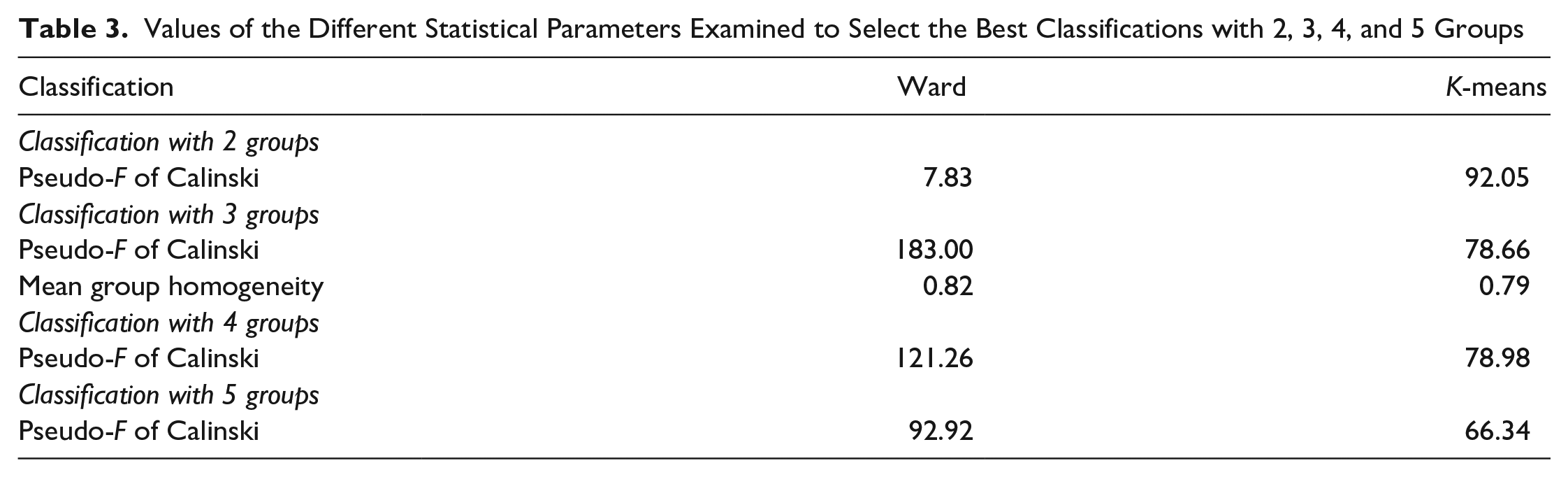
The clustering strategy used to classify the 168 healthcare workers is cluster analysis (Hair et al., 2019). This strategy was chosen because it creates homogeneous groups. The average value of the cluster centers provides specific profiles for each cluster. Specifically, Ward’s hierarchical method was used to produce potential classifications (Hair et al., 2019). However, different classification methods and clustering strategies were tested for the analyses to justify this choice. First, the statistical parameters presented in Table 3 were considered the best classification. We compared two types of classification analysis: Ward’s method and the K-means method, which consist of two different algorithms. The K-means method limits the number of clusters to ten, which is different from Ward’s method, as it does not limit the number of clusters. In Ward’s method, each observation is considered a cluster, and the clusters are joined hierarchically. Ward’s method is an algorithm for finding a partition with a small sum of squares. Another distinction is that K-means is intended for unsupervised classification, but Ward’s method is not. Calinski’s pseudo-F was used to guide the optimal number of groups. The best results came from the three-group Wards classifications, for which the pseudo-F value was maximized (Calinski’s Pseudo-F = 183.00). This choice resulted from a balance between statistical and practical considerations (Hair et al., 2019; Kettenring, 2006).
Values of the Different Statistical Parameters Examined to Select the Best Classifications with 2, 3, 4, and 5 Groups
Finally, the analyses were redone on the sample of T2 (n = 147). This analysis allowed us to assess the stability of the cluster solutions proposed in T1. Several general validation techniques have been developed for cluster analysis that can be used independently of the clustering method used (Grün, 2019). These measures can be used to assess the stability of cluster solutions (Hennig, 2007). For example, the extent to which a cluster solution depends on a specific dataset and how much it varies if a new dataset is used can be assessed. Dolnicar and Leisch (2010) pointed out that these stability assessments allow researchers to infer whether cluster solutions can be constructed stably when natural clusters (i.e., density clusters) are not contained in the data. They proposed using stability as a criterion for selecting an appropriate clustering solution when no natural clusters are contained in the dataset.
Qualitative Analyses
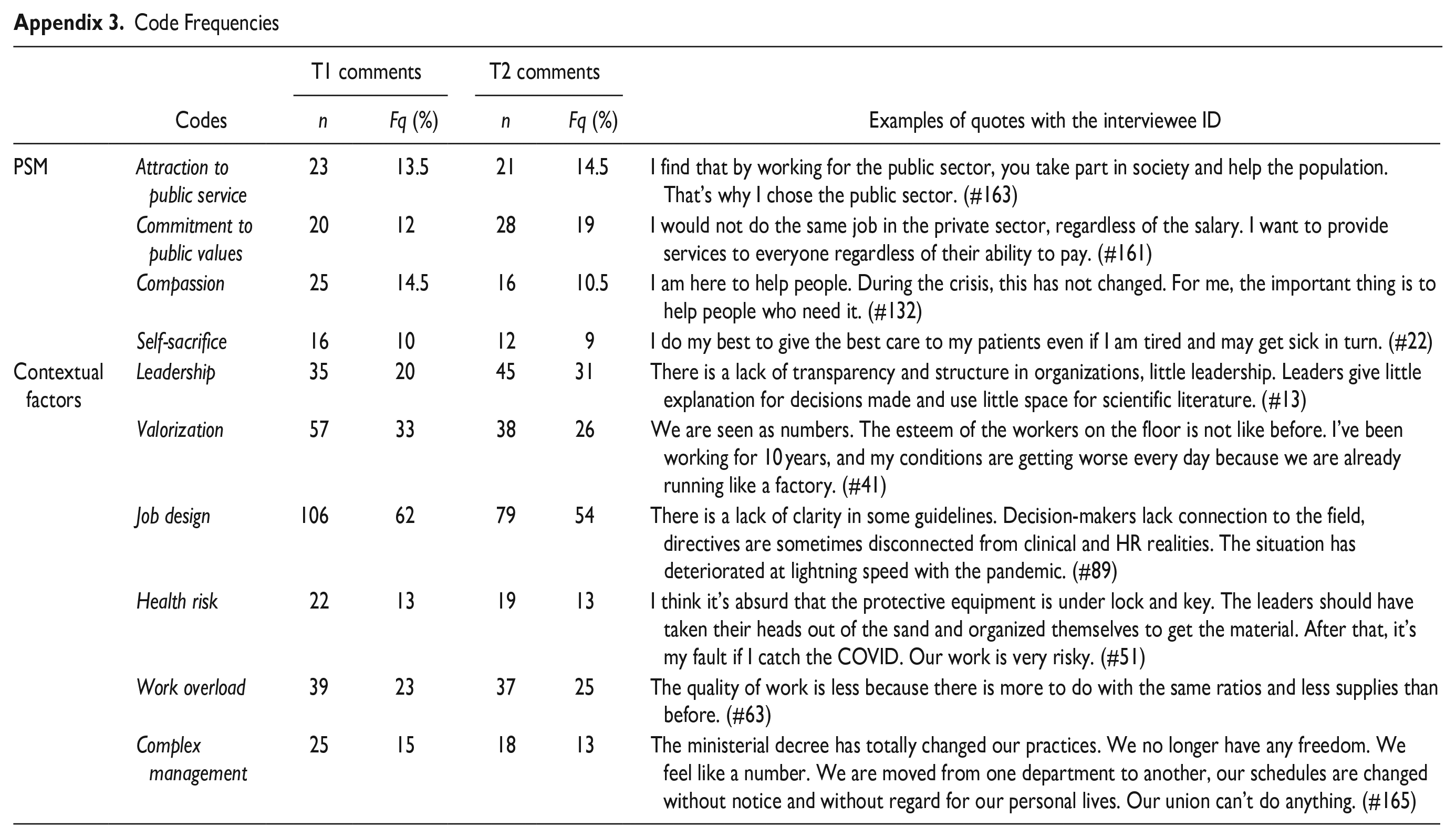
A general inductive content analysis was conducted to identify major themes in the textual data (Thomas, 2006). Specifically, the data collected by open-ended questions were coded using a three-step inductive approach (Thomas, 2006). First, the responses to the open-ended questions were downloaded and collated into a Word document to make the responses visibly accessible through text. Then, once the data were adapted to this format, the analyses began with a close reading of the texts. During this reading, thematic analysis was used to detect critical ideas reported by the healthcare workers. Third, the content of the responses was classified and systematized into different thematic categories. A total of 3,464 excerpts were coded, and then further qualitative analyses (e.g., the frequency of the codes obtained by the inductive analysis and the descriptive statistics associated with the themes) were conducted using Dedoose v. 8.3.40 software.
These steps resulted in the identification of two categories; PSM and contextual factors. Categories allow multiple codes to be grouped together under a single topic, refining the coding tree (Saldaña, 2014). The above steps also helped to uncover ten codes. These codes include valorization, leadership, health risk, work overload, complex management, job design, attraction to public service, commitment to public values, compassion, and self-sacrifice. Appendix 3 presents the respondents’ coded frequencies and percentage of comments. Qualitative analyses focused on all respondents’ answers to the two measurement times.
The items relating to PSM help to illustrate the differences between the three healthcare worker profiles. The contextual factors allow exploration of the potential explanations for the changes in the profiles. Subsequently, a comparative analysis of the 68 participants who changed profiles between T1 and T2 was conducted to understand the contextual factors influencing the MSP profile. The present longitudinal analysis aims to identify and assess the changes for each participant and compare them to each other (Calman et al., 2013).
This study also employed three validation strategies to ensure the reliability of the qualitative data. First, both researchers defined and discussed codes (Miles & Huberman, 2003). They met several times to discuss emerging codes and analysis strategies during the research process. Second, independent parallel coding was conducted for the first 25 respondents. This exercise allowed two coding trees to be developed and compared to identify similarities and differences (Thomas, 2006). After five meetings, the researchers agreed on the codes and themes included in the rest of the analyses. Subsequently, the remaining responses were coded using independent parallel coding with the consolidated coding tree (Thomas, 2006). Third, the qualitative data were used as a data validation strategy. Thus, the different data (qualitative and quantitative) were triangulated to reduce the biases inherent in each research method used (Miles et al., 2018). This triangulation of the data resulted in a rich description of the profiles (Yin, 2011).
Results
The results of this study are presented in three subsections. The first subsection explores the PSM profiles obtained from the inductive analyses. Next, the PSM profiles’ evolutions are described for respondents who participated in both questionnaire phases (October and December 2020). Finally, the three main factors influencing PSM evolution are presented.
PSM Profile of Healthcare Professionals
The cluster analyses identified and described three profiles of frontline healthcare professionals, including: (1) the devoted, (2) the disenchanted, and (3) the limited self-sacrificing. The results of the comparison of the variable groups used to construct the final classifications are presented in Table 4. The results of the ANOVA test demonstrate a significant difference between the three profiles on each of our independent variables.
Comparison of Variable Groupings Used to Construct the Final Classifications for T1 and T2
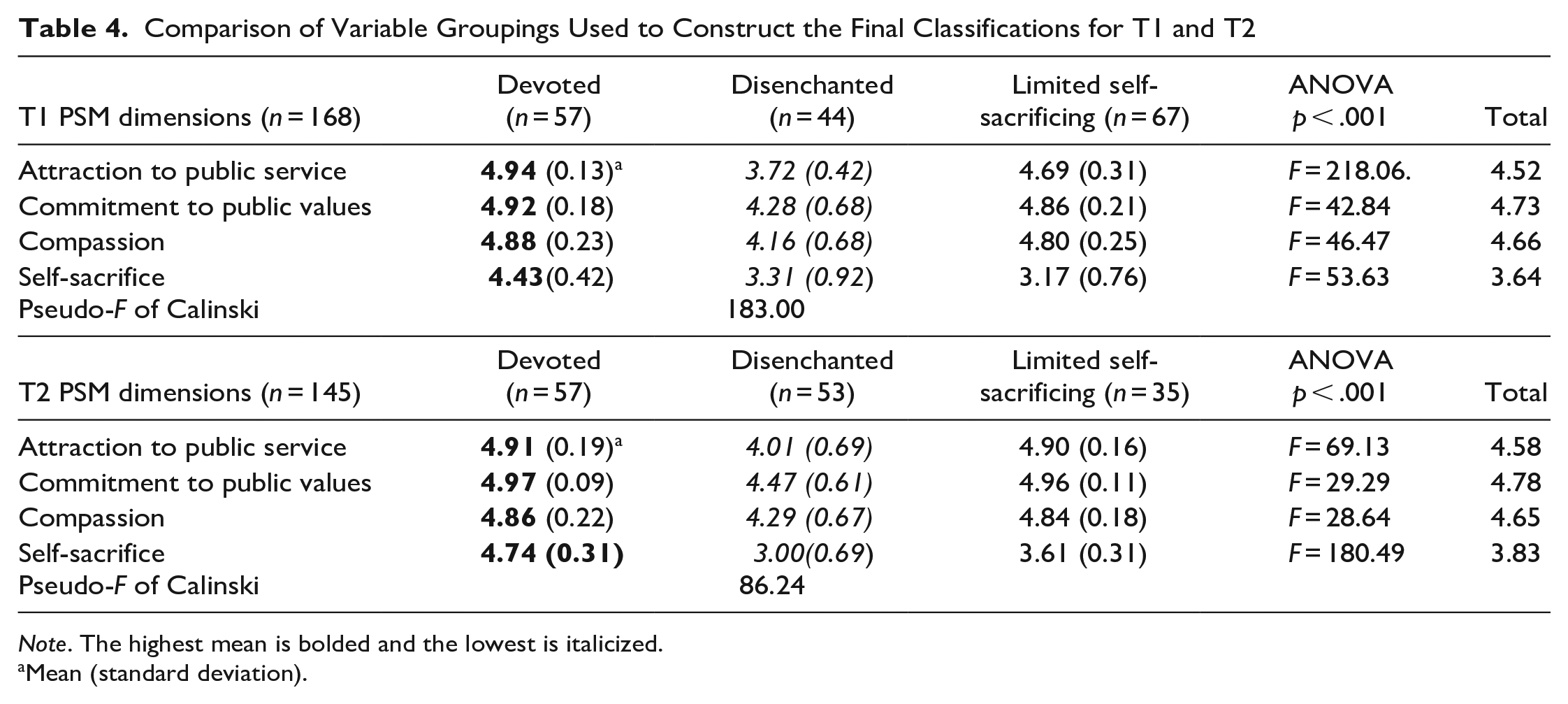
Note. The highest mean is bolded and the lowest is italicized.
Mean (standard deviation).
The Devoted
Data analyses identified 57 professionals at T1 and 57 professionals at T2, with the devoted profile. The characteristics associated with this profile translate into higher scores on all four PSM dimensions. Frontline professionals in this category strongly emphasize their readiness and willingness to serve the public and work for the common good (Attraction to Public Service). They promote a set of shared values, including equality, continuity, consideration for future generations, ethics, and commitment to public values. Devoted healthcare professionals identify with the suffering of others and are caring and protective of their fellow citizens. These qualities demonstrate a strong capacity for compassion. Finally, these professionals report a willingness to substitute intangible rewards for tangible ones in the service of others, which refers to altruism (Self-Sacrifice). The comments of professionals presented in Table 5 illustrate this profile’s characteristics.
Representative Quotes for the Devoted Profile

The Disenchanted
The data analyses identified 44 professionals at T2 and 53 professionals at T2 with the disenchanted profile. This profile’s associated characteristics result in the lowest scores on the four PSM dimensions than the other profiles. Frontline professionals in this category emphasize their readiness and willingness to serve the public and work for the common good, but with some reservations (Attraction to Public Service). They have a set of shared values, including equality, continuity, consideration for future generations, and ethics. Still, they do not feel recognized by the system (Commitment to Public Values). Disenchanted healthcare professionals identify with others’ suffering and care about and protect their fellow citizens. These qualities demonstrate their facility for compassion. Furthermore, these professionals also express their willingness to substitute intangible rewards for tangible ones in the service of others (Self-Sacrifice).
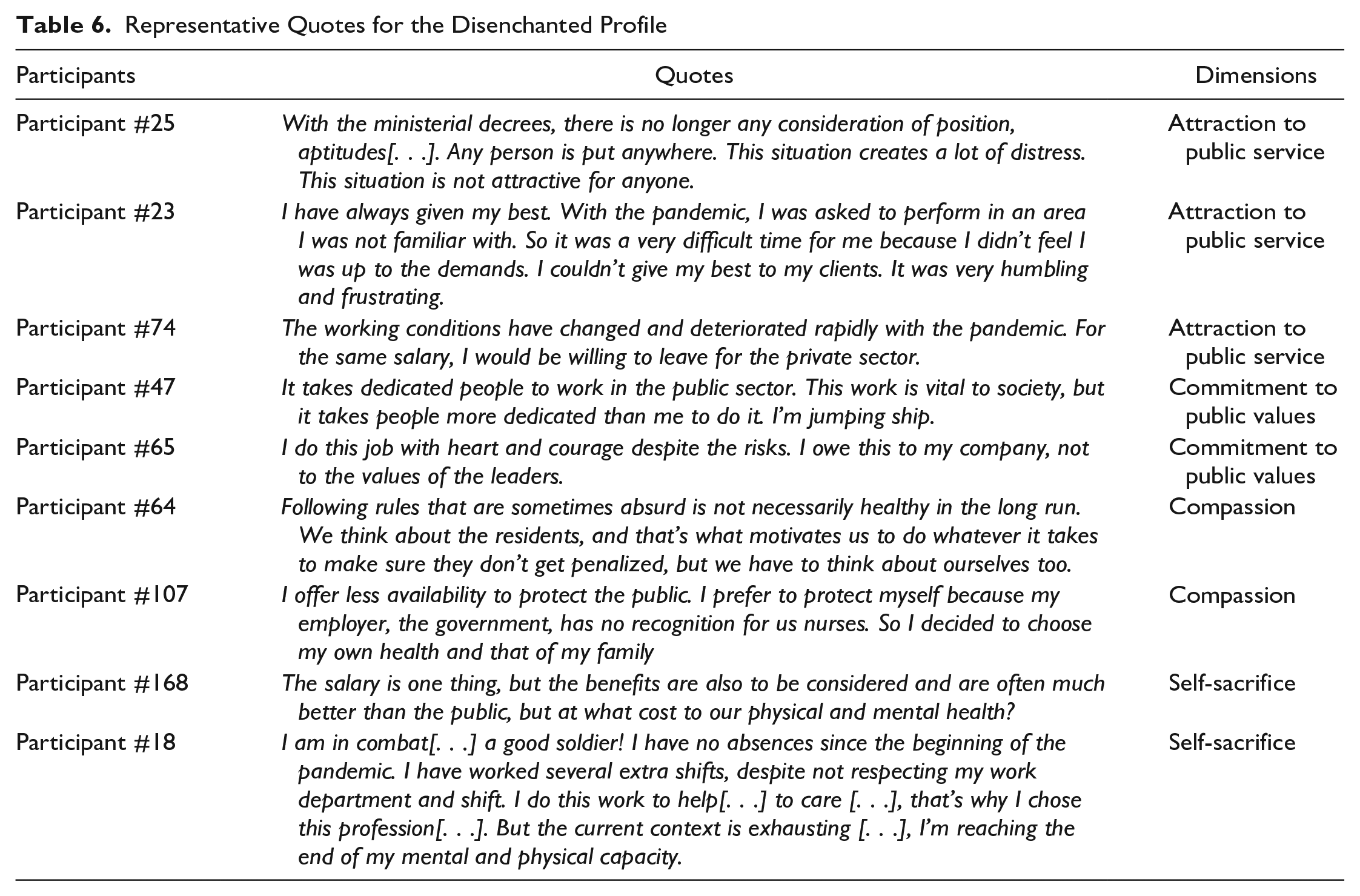
Therefore, healthcare professionals in this profile are also altruistic. However, they perceive that this is to the detriment of themselves, their family, and their personal life. They question the system and its ability to provide quality care that meets the needs of their fellow citizens. In particular, they feel disillusioned, exhausted, and undervalued. The response excerpts presented in Table 6 illustrate aspects of the disenchanted profile.
Representative Quotes for the Disenchanted Profile
Limited Self-Sacrificing
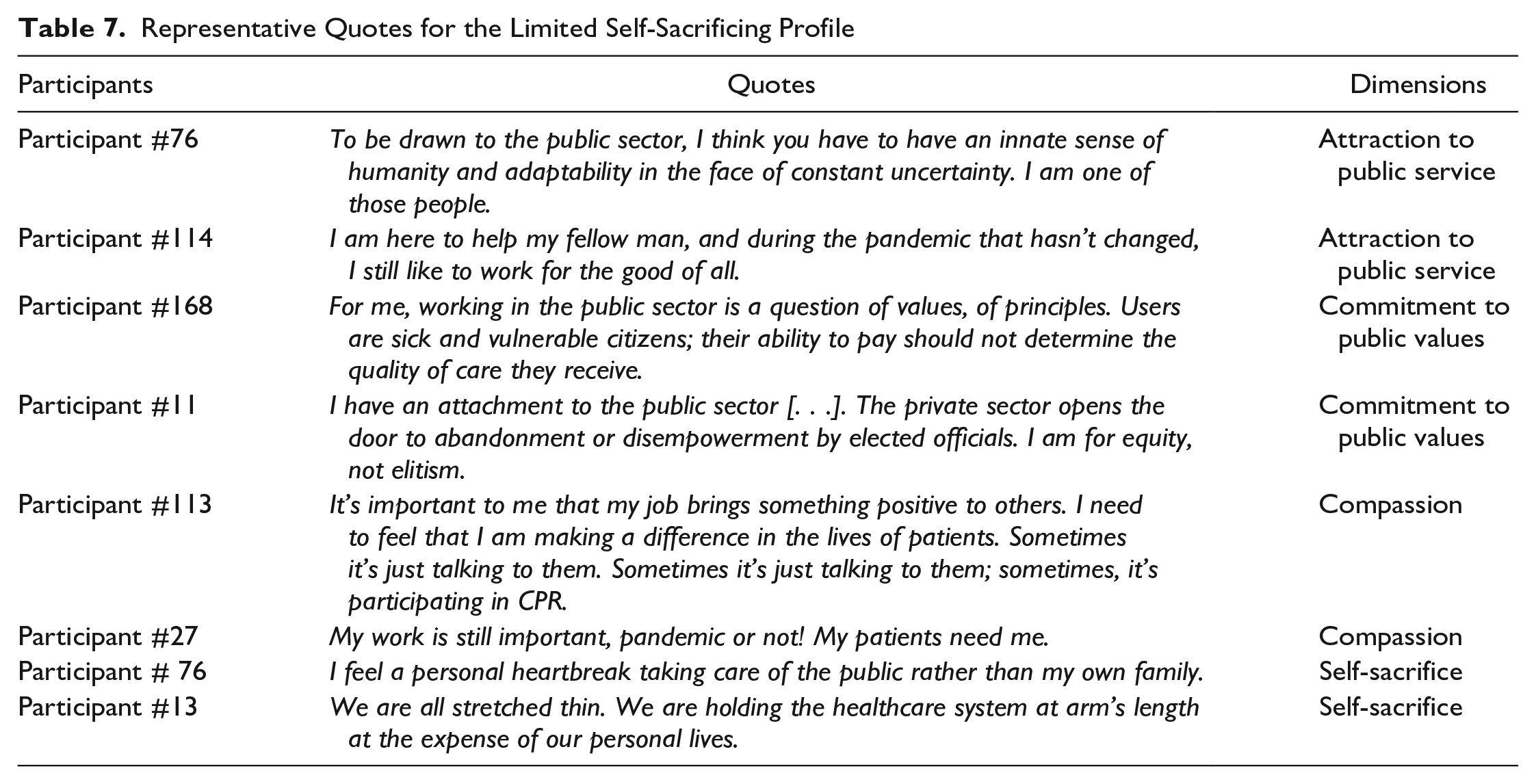
Data analyses identified 67 professionals at T1 and T2 with the limited self-sacrificing profile. This profile’s associated characteristics result in a lower PSM score for the “selflessness” dimension. Frontline healthcare professionals in this category emphasize their readiness and willingness to serve the public and work for the common good (Attraction to Public Service). They promote a set of shared values (e.g., equality, continuity, consideration for future generations) and ethics (e.g., commitment to public values). They also identify with others’ suffering and care for and protect their fellow citizens, showing compassion. However, they allege that service to others is at the expense of themselves, their families, their personal lives (Self-Sacrifice). Healthcare professionals with this profile feel instrumentalized, disillusioned, and exhausted. They also feel like they have to choose between their quality of life and work. The comments of professionals presented in Table 7 illustrate this profile’s characteristics.
Representative Quotes for the Limited Self-Sacrificing Profile
Evolution of PSM Profiles
For participants who completed the questionnaire at both phases, the Wards cluster analyses were rerun to see if their results had changed over time. Of the 66 participants who had completed both measurement times, 44% (n = 29) of them showed a change in PSM profile. The most common scenario (38%) was a shift from limited self-sacrificing to disenchanted (n = 11). In other words, 11 participants with the limited self-sacrificing profile had a decrease in self-sacrifice between the two measurement times. Table 8 shows the results of the student’s t-statistic. The paired samples t-test was used. Specifically, we compared the means of each individual between the two measurement times according to the profiles. The results show significant changes between the two measurement times for the commitment to public values and self-sacrifice dimensions for participants in the devoted group and attraction to public service for participants in the disenchanted group.
Paired t-Test by Profil (n = 66)
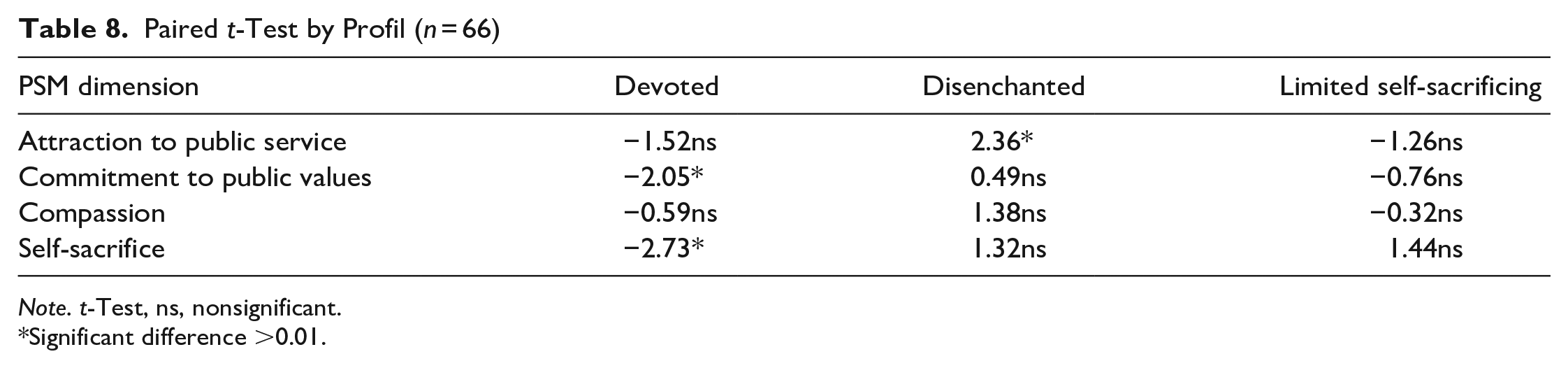
Note. t-Test, ns, nonsignificant.
Significant difference >0.01.
The remaining participants showing a decrease in PSM changed from (1) a devoted to a disenchanted profile (n = 4) and (2) a devoted to a limited self-sacrificing profile (n = 6). Few participants showed an improvement in PSM during the study period (n = 8). Those few participants (28%) showing an increase moved from (1) the limited self-sacrificing to the devoted profile (n = 3); (2) the disenchanted to the limited self-sacrificing profile (n = 1), and (3) the disenchanted profile to the devoted profile (n = 4). Figure 1 shows the five different scenarios of PSM profile change.
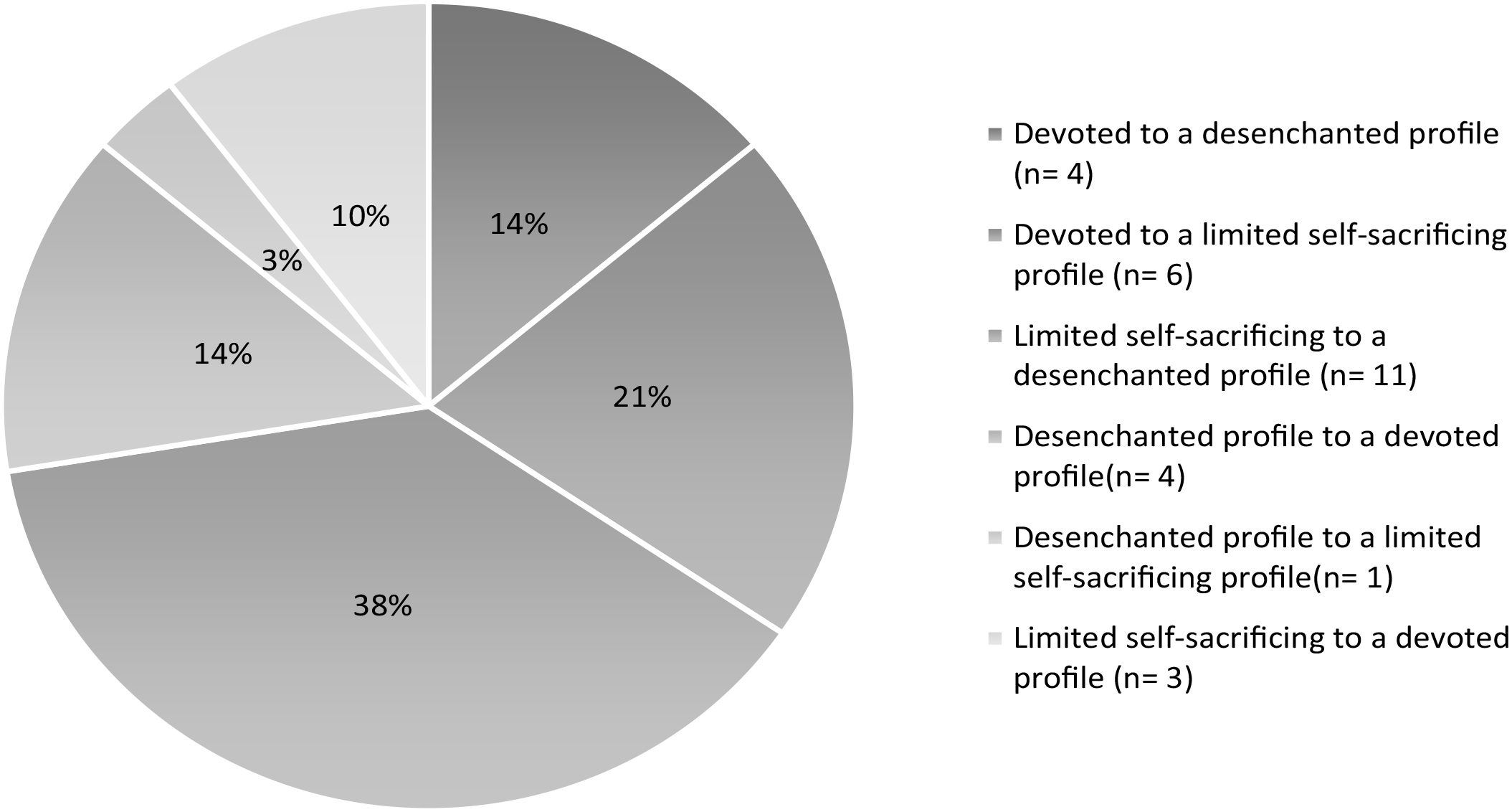
Scenarios for changing PSM profiles (n = 29)
The exploratory qualitative analyses identified three interrelated factors of workers’ PSM development: (1) valorization, (2) leadership, and (3) job design. For this study, valorization is defined “as a process of mobilizing socially constructed attitudes in the collective elevation of the value and image of certain types of work (and the individuals performing it) that are traditionally devalued” (Hennekam et al., 2020). Leadership refers to the meta-leadership defined by Marcus et al. (2019). Relatively new to the leadership theory family, the meta-leadership framework is becoming more widely recognized and adopted, particularly for leading in emergency preparedness and response, such as the COVID-19 pandemic (Hayes et al., 2021). Meta-leadership is defined via three dimensions: (1) the person or personal characteristics of leaders who exhibit emotional intelligence, and who develop credibility, and trusting relationships; (2) the situation and the leader’s grasp of the complex problem and the actions taken through communication and decision-making; and (3) connectivity and how the leader builds networks through partnerships, collaboration, and work with stakeholders (Hayes et al., 2021, p. 3). Job design is “the process of organizing tasks, duties, and responsibilities, along with the associated required skills, knowledge, abilities, and competencies, into a coherent structure that will drive the work of the individual in the position” (Piatak et al., 2021, p. 90). Table 9 presents different quotations from healthcare workers who contributed to the identification of factors.
Factors Influencing PSM Evolution
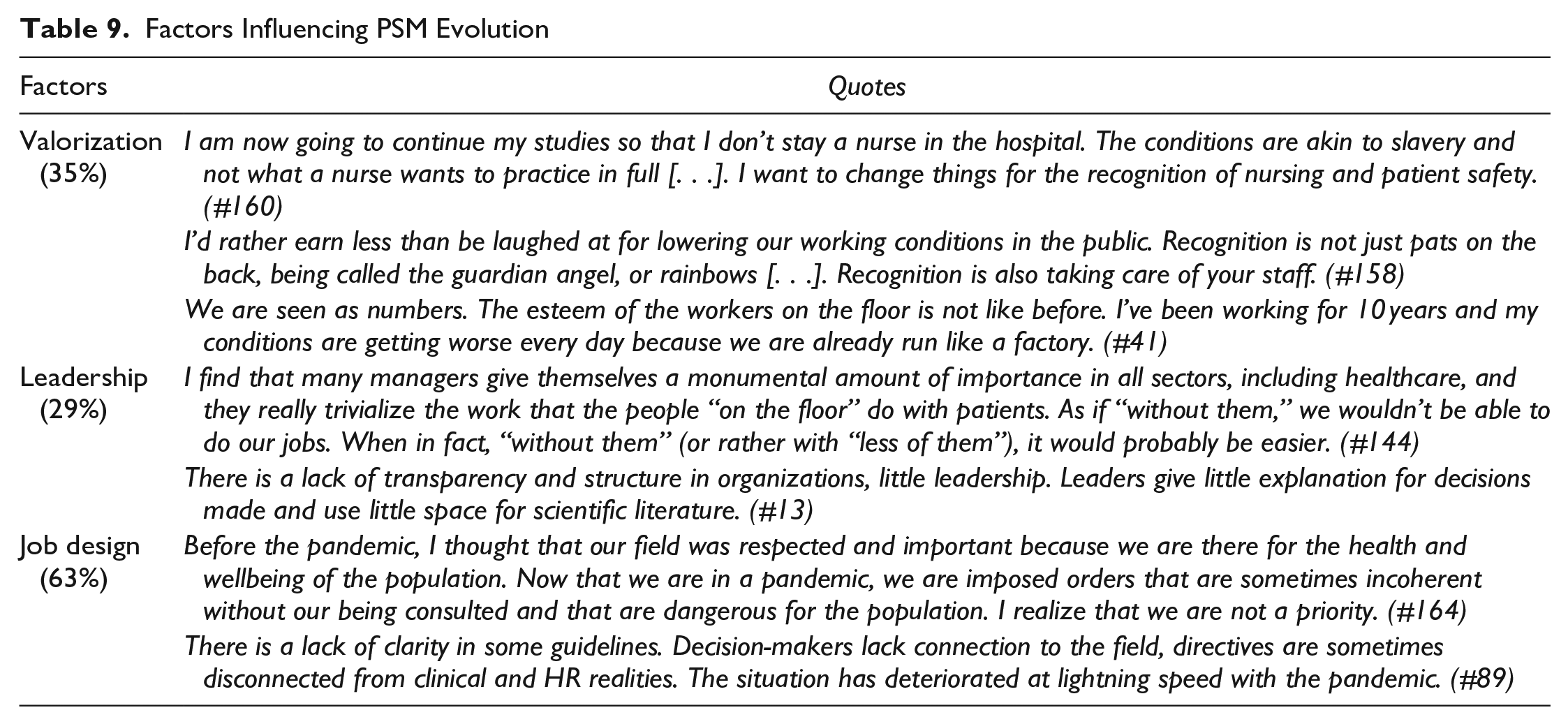
Valorization
Social valorization is a process of mobilizing socially constructed attitudes (Wolfensberger & Thomas, 2005). It is based on the collective elevation of the value and image of certain types of work—and the individuals who perform them—that are traditionally devalued (e.g., doctors vs. nurses). In this study, 33% of respondents reported feeling poorly valued in the first wave of questionnaires, increasing to 35% in the second wave. This factor increases to 43% in the second wave for participants with the limited self-sacrificing profile. The existence of rigid organizational policies results in limitations or barriers to the autonomy of professionals. This factor could explain both the low satisfaction with administrative policies and the need to increase the value of autonomy. Employees are attentive to the words and actions of their supervisors. Therefore, supervisors must ensure that they value employees’ suggestions, supportively accept their feedback, and lead by example.
Leadership
Leadership promotes a sense of cohesion, personal development, and higher satisfaction levels among subordinates (Van Wart, 2003, p. 216). In this study, 20% of the respondents mentioned that the leadership did not allow them to reach their full potential as healthcare professionals, and that number rose to 29% during the second wave. This factor decreased to 9% for participants with the limited self-sacrificing profile. Respondents explained that their leaders lack knowledge and sensitivity to the frontline realities. They also have conflicting values, do not heed their employees’ feedback, and must improve transparency.
Job Design
Job design is the process of organizing the tasks, duties, and responsibilities for a position (Piatak et al., 2021). Furthermore, job designers must identify the required skills, knowledge, abilities, and competencies needed for each role (Piatak et al., 2021, p. 90). In this study, 62% of the respondents mentioned differences related to job design, and this number increased to 63% in the second wave. This factor was mentioned by 92% of the devoted profile participants. Researchers studying employee motivation have highlighted how job design and attention to job characteristics can influence employee motivation. They also point out that this is a critical element to understand in the context of PSM because, from a human resources management (HRM) perspective, job design is the start of the HRM process (e.g., Grandey & Diamond, 2010; Piatak et al., 2021).
Finally, although exploratory, the second measurement period allowed us to investigate the factors (Table 10) that might have influenced these changes among the workers who had shifted profiles (n = 29). In the open-ended questions, 41% of these workers spontaneously mentioned leadership, 45% mentioned valorization, and 76% mentioned job design. For leadership, 25 of the 66 respondents mentioned this factor. In terms of proportions, 12/29 (41%) of the workers who changed their profile and 13/37 (35%) who did not change their profile addressed leadership. As for valorization, 28 of the 66 (42%) respondents spontaneously addressed this factor. In terms of proportions, 13/29 (45%) of the workers who had changed their profile and 15/37 (41%) of the workers who had not changed their profile discussed valorization. For job design, 49 of the 66 (74%) respondents addressed this factor. Regarding proportions, 22/29 (76%) of the workers who changed their profile and 27/37 (72%) of the workers who did not change their profile addressed job design. In all cases, although these differences were minimal, a higher percentage of workers who changed their profile mentioned the factors compared to those who had not.
Factors’s Evolution
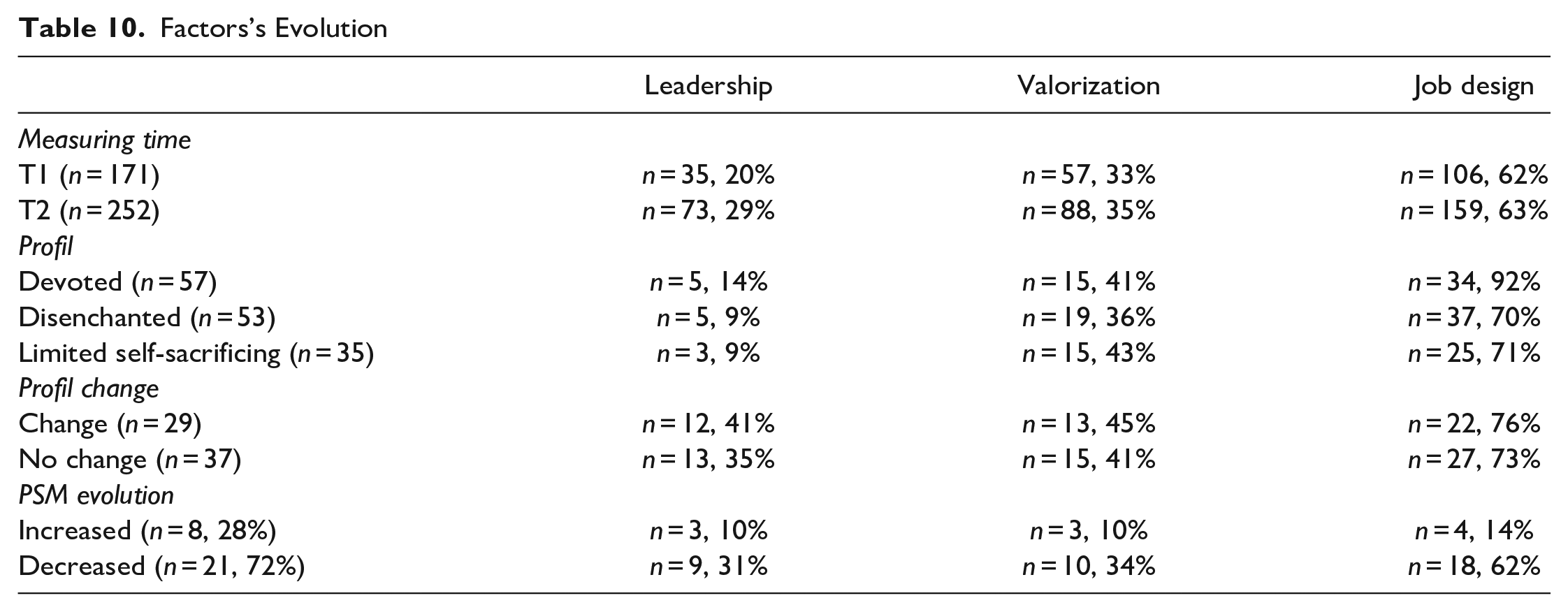
Similarly, despite the minimal changes, the use of quantitative data allowed us to identify changes that were not apparent simply from the unquantified qualitative data (Maxwell, 2010, p. 479; Sadker & Sadker, 1995, p. 2). These analyses allowed us to reveal a higher percentage of these factors among workers who changed their profile.
Discussion and Conclusion
The objectives of this study were to (1) develop PSM profiles and (2) explore PSM’s evolution and its contributing factors during the pandemic. Using data obtained with S. Kim et al.’s (2013) PSM measurement scale, cluster analyses highlighted three profiles sharing similar PSM characteristics. These profiles include: (1) the devoted, (2) the disenchanted, and (3) the limited self-sacrificing. The four dimensions of PSM helped define the profiles, and the qualitative analyses enabled their identification and description. Second, the COVID-19 pandemic provided an opportunity to explore principal determinants for preserving PSM, such as valorization, leadership, and job design. Analyses of the responses of healthcare workers who participated in both measurement periods revealed that self-sacrifice is the most context-sensitive dimension.
This study has three main contributions to the literature on PSM, motivation, and public sector health service management, especially during a public health crisis (e.g., a pandemic). First, rather than pursuing more familiar actions focusing on industrial models of motivation (Perry & Porter, 1982), this study contributes to the scientific literature on public sector health service management by exploring a typology of PSM profiles. This typology helps describe and clarify PSM among health professionals during the pandemic by identifying three key contextual factors. Based on the three PSM profiles, managers and policymakers can draw on these results to develop alternative patterns and visions. They can also seriously consider the three contextual factors that potentially undermine professional motivation. Managing contextual factors is fundamentally a matter of interaction between PSM and human resource practices (Bland et al., 2021).
Second, this study contributes to a better understanding of PSM’s organizational and human issues and provides more clarity on its evolution in frontline workers during a public health crisis like the COVID-19 pandemic. This study identified a broader range of contextual factors influencing PSM’s evolution by exploring the constraining conditions and their impacts on frontline healthcare workers’ PSM. Several previous studies have demonstrated that PSM is stable over time (e.g., Jeong et al., 2022; Toubøl et al., 2022; van Loon et al., 2020). The results of this study differ from previous studies by demonstrating changes in PSM over time in 44% of respondents. This study highlights variability among individuals that previous studies have done little to explore and that the cluster approach provides insight into (e.g., Toubøl et al., 2022; Zhang et al., 2022).
Other previous studies provide some evidence that PSM can change over time. Houston (2000), supported by more recent studies (e.g., M. Y.Kim & Torneo, 2021; Miller-Mor-Attias & Vigoda-Gadot, 2022; Quratulain & Khan, 2015; Wright & Grant, 2010), suggested that organizational factors (e.g., employee-supervisor relationships, leadership, job characteristics, organizational changes, employee role clarity, and task importance) influence PSM over time. Related to these organizational factors, Miller-Mor-Attias and Vigoda-Gadot (2022) urging public sector human resource departments to be aware of the evolution of PSM over time. Future research could further explore this contribution in the context of a crisis to have additional measures 1 or 2 years after the crisis to assess whether respondents are still in the profession or have returned to their original profile.
This study was inspired by other studies that have used clusters to provide a more accurate picture of public service workers (e.g., Baekgaard et al., 2022; Berntson et al., 2012; Pedersen et al., 2019). This technique allows us to demonstrate certain specificities or, as in this case, to show that an individual’s PSM can evolve over time (Miller-Mor-Attias & Vigoda-Gadot, 2022). In summary, the contrast between PSM theory and profile development helps to illustrate that while PSM remains relatively stable over time (see Jeong et al., 2022; van Loon et al., 2020). When examining the pathways of single individuals, there is a change in PSM over time. Previous research on PSM has often focused on the individual (Piatak et al., 2021). Conversely, this study goes further by looking at a particular context to shed light on institutional practices, policies, and procedures.
Third, this work contributes to the literature on healthcare professionals during crises by describing what healthcare workers experience and perceive during a pandemic. Few studies have identified the effects of a health crisis on healthcare workers (Raven et al., 2018). However, major national crises can substantially influence the work of public servants, as was the case for federal employee satisfaction after 9/11 in the United States (van Ryzin, 2014) or various human resource issues in their emergency plans following Hurricane Katrina (Mann, 2014). The present study is one of the first to (1) study PSM in times of crisis and (2) with a longitudinal approach. Results confirm the difficulties of adapting a weak healthcare system on the resilience of organizations in times of global pandemic (Raven et al., 2018). With the help of external partners, government structures in this context need to develop and implement strategies to make their healthcare systems stronger and more resilient to crises (Kruk et al., 2015; Raven et al., 2018). The challenge is integrating mechanisms of organizational resilience, such as benevolent supervision and peer support networks, into existing systems. These systems will help anticipate crises rather than wait until it is too late to respond (Raven et al., 2018). Choosing actions to prepare the health system for health crisis event suggests the presence of anticipatory altruism on the part of decision makers (Le et al., 2021).
Managerial Implications
This study has three main managerial implications. First, public agencies should assess the motivation level of job candidates when making selection decisions (Ritz et al., 2016). This evaluation can be done in the job posting, in the analysis of the application file, or through questions during interviews (Bromberg & Charbonneau, 2020). Second, public organizations should use management practices (e.g., employee valuation, transformational leadership, or person-job fit) to preserve a certain level of PSM. These practices would increase PSM for disenchanted profiles or identify the risks associated with high PSM levels for devoted profiles. Finally, managers should consider PSM profiles and levels at the time of hiring and during employment.
However, PSM should not be the only criterion for selecting an employee. This criterion would not be sufficient to identify high-performing employees (Ritz et al., 2016). Instead, organizational policies should focus on preventing presenteeism by reducing excessive stress, enhancing PSM, and improving the health and wellbeing of health professionals (Jiang et al., 2021).
Limitations and Avenues for Future Research
Although the present study yielded interesting results, several limitations must be considered when interpreting its findings. First, this study is based on self-reported questionnaires and, thus, has the potential for common method, common source, and the social desirability biases (Demetriou et al., 2015). Although we were unable to address these limitations in this study, future research could incorporate surveys collected by other sources. For example, surveys of the observer’s PSM could be collected from peers and/or supervisors, and future studies could use different types of assessments.
Second, the methods and scope of the research are limited by the specific context of the COVID-19 pandemic. First, a nonrandom (snowball or convenience) sampling method was used. This method may cause a sampling bias toward the characteristics of those with an active online presence on social networks, affecting the results of this study. However, during a pandemic, online data collection is a feasible and effective research method (Zhang et al., 2022). Therefore, future research could use an approach with an experimental design with a random sample to reduce the effects of this sampling bias.
In addition, our sample has significant attrition because only 66 of 252 (26%) respondents participated in both T1 and T2. The study lost approximately 62% of the original respondents at T2. Certainly, attrition in a longitudinal survey can lead to bias in estimates of changes in certain behaviors over time. But, without the follow-up of these individuals, our design would have been a short cross-sectional study. Cohort studies are part of the gold standard of randomized and nonrandomized designs because they allow for the comparison of variables within participants, rather than just between participants. In addition, there are procedures that allow for sensitivity testing of the magnitude of this bias (West & McCabe, 2017). Because we collected our data twice, we investigated the existence of attrition bias by following the procedure recommended by Miller and Hollist (2007). We tested for differences in key sample characteristics, such as age, years of experience, employment sector, and occupation type.
Third, clustering classification analysis is a method for exploring results. Individuals in the same cluster are similar only in terms of the information (scores on selected variables) on which the analysis is based. This is why it is recommended to split the sample and apply the method twice. This mixed-method (hierarchical and dynamic clustering) lends itself to testing internal and external validity (Negrini et al., 2020). Therefore, future research could utilize this validity strategy. The reproducibility of the profiles and their interpretation was tested using data from T2. Although it worked well in our study, we recommend future studies to re-test its validity and reliability. This could enrich our understanding of PSM profiles, clarifying their relationships to the contextual factors presented here and those suggested in other studies (e.g., Hameduddin & Engbers, 2022).
Fourthly, our reliance on a sample of Quebec workers may be culturally biased. Thus, we encourage future studies to replicate our study in other regions. Significant cultural differences in both meaning and relationships have been found for some of the core concepts of organizational behavior. For example, research suggests that the definition of job satisfaction may not be equivalent in countries without the same language or cultural history ( C.Liu et al., 2004). The same is true for intrinsic job characteristics, which are more strongly associated with job satisfaction and individualistic values in wealthier countries (Huang & Van de Vliert, 2003; S.Kim et al., 2013). Therefore, future research may reveal additional contextual factors to consider in the evolution of PSM. The exploratory nature of this study limits the scope of the results presented. However, the context of the COVID-19 pandemic lends itself well to exploratory studies. This type of study allows for the development of ideas and hypotheses for the future. Exploratory studies are a key step in assessing the feasibility and value of moving to an efficacy study (Hallingberg et al., 2018). Future research could focus on job design during crises and the importance of redesigning jobs in challenging contexts, such as the one studied in this article. Jobs must be designed to be meaningful so that employees feel competent and valued (Miao et al., 2018). Researchers who have studied employee PSM have highlighted how job design and attention to job characteristics can influence employee motivation (e.g., Piatak et al., 2021; Rainey, 1982; Taylor, 2014). This finding is critical to understanding the PSM framework (Fried & Ferris, 1987; Grandey & Diamond, 2010; Hackman & Oldham, 1976; Piatak et al., 2021).
Footnotes
Appendix
Code Frequencies
| Codes | T1 comments | T2 comments | Examples of quotes with the interviewee ID | |||
|---|---|---|---|---|---|---|
| n | Fq (%) | n | Fq (%) | |||
| PSM | Attraction to public service | 23 | 13.5 | 21 | 14.5 | I find that by working for the public sector, you take part in society and help the population. That’s why I chose the public sector. (#163) |
| Commitment to public values | 20 | 12 | 28 | 19 | I would not do the same job in the private sector, regardless of the salary. I want to provide services to everyone regardless of their ability to pay. (#161) | |
| Compassion | 25 | 14.5 | 16 | 10.5 | I am here to help people. During the crisis, this has not changed. For me, the important thing is to help people who need it. (#132) | |
| Self-sacrifice | 16 | 10 | 12 | 9 | I do my best to give the best care to my patients even if I am tired and may get sick in turn. (#22) | |
| Contextual factors | Leadership | 35 | 20 | 45 | 31 | There is a lack of transparency and structure in organizations, little leadership. Leaders give little explanation for decisions made and use little space for scientific literature. (#13) |
| Valorization | 57 | 33 | 38 | 26 | We are seen as numbers. The esteem of the workers on the floor is not like before. I’ve been working for 10 years, and my conditions are getting worse every day because we are already running like a factory. (#41) | |
| Job design | 106 | 62 | 79 | 54 | There is a lack of clarity in some guidelines. Decision-makers lack connection to the field, directives are sometimes disconnected from clinical and HR realities. The situation has deteriorated at lightning speed with the pandemic. (#89) | |
| Health risk | 22 | 13 | 19 | 13 | I think it’s absurd that the protective equipment is under lock and key. The leaders should have taken their heads out of the sand and organized themselves to get the material. After that, it’s my fault if I catch the COVID. Our work is very risky. (#51) | |
| Work overload | 39 | 23 | 37 | 25 | The quality of work is less because there is more to do with the same ratios and less supplies than before. (#63) | |
| Complex management | 25 | 15 | 18 | 13 | The ministerial decree has totally changed our practices. We no longer have any freedom. We feel like a number. We are moved from one department to another, our schedules are changed without notice and without regard for our personal lives. Our union can’t do anything. (#165) | |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.