
Abstract
Perfectionism is a multidimensional personality characteristic associated with mental health problems. However, its features are commonly misunderstood, and many people are unaware of the risks it can pose. This study aimed to develop the first self-report measure of perfectionism literacy. That is, the degree of knowledge someone has about perfectionism, its features and consequences, and when and where to seek help if needed. The Perfectionism Literacy Questionnaire (PLQ) was validated over four stages using four samples of community adults (N = 1078 total; Mage = 37.17 years). In stage one, we generated a pool of items. In stage two, we used exploratory and confirmatory factor analysis to derive a 29-item, seven-factor measure. In stage three, we assessed relationships between the PLQ, perfectionism, and attitudes toward help-seeking for mental health support and found the PLQ is distinguishable from these constructs. In stage four, we examined whether the PLQ was responsive to change following an educational video on perfectionism. We found tentative evidence that minimal intervention can increase perfectionism literacy. Our findings suggest that the PLQ is valid and reliable and may be useful for educational purposes and primary prevention of mental health problems.
Introduction
Mental health problems are increasing worldwide (World Health Organization, 2022). In search of possible explanations for this trend, meta-analytical data suggests that perfectionism – a risk factor for mental ill-health – is also increasing (Curran & Hill, 2019). Research on the efficacy of individual and group-based interventions to reduce perfectionism is accruing (see Suh et al., 2019). However, for larger-scale support, other forms of primary intervention are required to prevent difficulties associated with perfectionism before they arise. While the benefits of increased knowledge of mental health issues – or mental health literacy – have been noted in this regard (e.g. Freţian et al., 2021; Perry et al., 2014; Smith & Shochet, 2011), no measures exist that examine perfectionism literacy. A perfectionism literacy measure is central to assess knowledge of perfectionism, promote understanding of perfectionism, and support primary prevention of mental health issues associated with perfectionism. Here, we apply the concept of mental health literacy to perfectionism to create a novel measure of ‘perfectionism literacy’ that can aid researchers and practitioners in assessing the benefits of their educational and preventive work.
Multidimensional Perfectionism and Mental Health
Current understanding of multidimensional perfectionism is underpinned by Hewitt et al.’s (2017) Comprehensive Model of Perfectionistic Behavior. This model includes trait dimensions of perfectionism, perfectionistic cognitions, and self-presentational facets of perfectionism. We focus on trait perfectionism in the current research as the most extensively researched and longstanding aspect of the model. Hewitt and Flett (1991) conceptualized trait perfectionism as consisting of three dimensions: self-oriented perfectionism (requiring perfection of the self), socially prescribed perfectionism (perceiving others to require perfection of oneself), and other-oriented perfectionism (requiring perfection of others). These are three distinct, but related, personal and interpersonal dimensions of perfectionism that co-occur and interact to determine the effects of a perceived need to be perfect.
Perfectionism is best understood as a transdiagnostic risk factor for mental health problems (Egan et al., 2011). Based on extensive meta-analytical evidence, this includes depressive symptoms, disordered eating, and suicidal ideation (e.g. Limburg et al., 2017; Smith et al., 2016; Smith et al., 2018). Of the three trait dimensions, socially prescribed perfectionism has consistently been shown to be a concomitant of mental health problems (see Limburg et al., 2017). By contrast, self-oriented perfectionism acts as a vulnerability factor for mental health problems when paired with stress or failure (Flett et al., 2016). Other-oriented perfectionism is inconsistently related or unrelated to personal mental health problems, such as depressive symptoms, but contributes indirectly to problems for others via conflict and disrupted relationships (e.g. Smith et al., 2019).
Mental Health Literacy and Perfectionism Literacy
According to Jorm et al. (1997), mental health literacy pertains to knowledge and attitudes regarding mental health that assist in mental health problems. It includes: (a) the ability to recognize specific mental health disorders; (b) knowledge of how to seek mental health information; (c) knowledge of risk factors and causes of mental health; (d) knowledge of self-treatments; (e) knowledge of professional help; and (f) attitudes that endorse recognition and help-seeking. Following the development of a valid and reliable measure of mental health literacy (see O’Connor & Casey, 2015), research has illustrated that educational interventions can increase mental health literacy (e.g. Potvin-Boucher et al., 2010), and that mental health literacy is related to greater help-seeking behaviour and reduced stigma of mental health problems (Perry et al., 2014; Suka et al., 2016). Understandably, then, increasing mental health literacy has become a key focus in organizations responsible for promoting mental health (LaMontagne et al., 2014).
Notably, mental health literacy has been applied to other concepts such as ‘depression literacy’ and ‘eating disorder literacy’ (Singh et al., 2019). The development of valid and reliable measures of these derivatives has allowed researchers and practitioners to study the benefits of specific types of mental health literacy. In support of this approach, research suggests that the general population, and healthcare professionals, differ in their knowledge of general and specific mental health problems, and knowledge of more general issues do not equate to knowledge of specific issues (e.g. Hadjimina & Furnham, 2017). In addition, there are often low levels of literacy of specific mental health issues among those who may encounter these issues regularly and would be able to direct people to appropriate support (e.g. Worsfold & Sheffield, 2018). Against this backdrop, the development of a novel measure of perfectionism literacy will offer researchers and practitioners the opportunity to study and promote understanding of perfectionism and its risks, and support primary prevention of mental health issues associated with perfectionism.
For the concept of perfectionism literacy, we propose a definition based on Jorm et al. (1997) – knowledge and beliefs about perfectionism, which aid in the recognition, management, and prevention of perfectionism. We also include components that mirror O’Connor and Casey’s (2015) work on the development of the Mental Health Literacy Scale. As such, perfectionism literacy includes (a) the ability to recognize perfectionism, (b) knowledge of how to seek information regarding perfectionism, (c) knowledge of risk factors and causes of perfectionism, (d) knowledge of self-treatment and professional treatments available for perfectionism, and (e) attitudes that endorse recognition and help-seeking behaviour for perfectionism. Utilizing O’Connor and Casey’s (2015) approach helps ensure coverage of key aspects of health literacy and that the concept and subsequent measure of perfectionism literacy closely aligns with general mental health literacy and research that has adapted the concept to specific mental health issues (e.g. Hart et al., 2014).
The Present Study
The aim of the study is to develop the first psychometric instrument measuring knowledge and attitudes relating to perfectionism – termed the Perfectionism Literacy Questionnaire (PLQ). To do so, we divided the study into four stages. The first stage consists of initial item generation and refinement. The second stage involves exploratory and confirmatory factor analysis of the factor structure of the PLQ. The third stage assesses the construct validity of the PLQ. The fourth stage adopts an experimental design in two independent samples to examine whether perfectionism literacy (measured by the PLQ) increases after viewing of an informational video on perfectionism.
Ethical Approval
This study received ethical approval from York St John University’s research ethics committee.
Stage One
The purpose of stage one was to generate items that capture components of perfectionism literacy and to assess and refine the initial PLQ item pool.
Initial Item Generation and Item Refinement
Item generation was undertaken by the study authors who hold doctorates in perfectionism-related topics and have conducted perfectionism research for >8 years. Operational definitions of the five perfectionism literacy components were developed based on Jorm et al.’s (1997) conceptualization of mental health literacy. The items generated were guided by Hewitt and Flett’s (1991) conceptualization of perfectionism given that it includes both intra- and interpersonal expressions of perfectionism and provides a comprehensive theoretical framework (Hewitt et al., 2017). While we considered including other facets of perfectionism (i.e. perfectionistic self-presentation) from this framework, we felt that they are not well recognized or understood compared to trait dimensions of perfectionism. Hence, the first component, recognition of perfectionism, was formed into three separate facets: recognition of self-oriented perfectionism, recognition of socially prescribed perfectionism, and recognition of other-oriented perfectionism.
For the second component and knowledge on how to seek information for perfectionism subscale, the items generated were based on the notion that if people needed to seek support for perfectionism there were a number of sources of information that would be appropriate and inappropriate. We listed appropriate sources of information in our items. For the third component, risk factors and causes, we focused on parental behaviours as these are the most plausible explanation and well-studied antecedents of perfectionism in research (Curran & Hill, 2022; Flett et al., 2002). For the fourth component, knowledge of treatments, we focused on the availability of general professional treatments for perfectionism which again we believe better reflects the current evidence base. Finally, for the fifth and final component, as in O’Connor, Casey, and Clough (2014), we listed beliefs we believed would encourage people to seek help (e.g. it could be bad for mental health).
Based on the devised definitions of the seven scales of perfectionism literacy, we generated an initial pool of 84 items. These items were then reviewed on their clarity, readability (based on Flesch-Kincaid grade level scores; Kincaid et al., 1975), relevance, similarity to other items generated and items of existing perfectionism scales and their appropriateness for lay populations. This process resulted in a revised pool of 76 items.
Expert Review
The 76 items were reviewed by two experts with extensive experience in perfectionism. The experts hold doctorates in psychology research with a focus on perfectionism, are employed at universities in senior academic roles, and have published research on perfectionism for over twelve years. The experts were asked to provide comments on specific items, propose new items where relevant, and provide more succinct wording for existing items. Following this, there was a total of 56 items.
Stage Two
The purpose of stage two was to explore the factor structure of the 56 PLQ items. We aimed to identify a parsimonious model which: (a) adequately accounts for the correlations among the set of items; and (b) incorporates interpretable factors. We also aimed to identify a scale which was stable across samples (subsample one vs. subsample two) and analyses (exploratory vs. confirmatory factor analytical techniques).
Participants and Procedure
The sample were 506 community adults (206 = male; 298 = female; 2 = nonbinary; M age = 40.80 years, SD = 13.41; range 18–77; 87.90% White British) recruited via Prolific Academic. We undertook extensive research in choosing Prolific as a recruitment platform for our study. Prolific was chosen as the preferred recruitment platform as it was designed for the scientific community and addresses limitations of other recruitment platforms (e.g. MTurk; Palan & Schitter, 2018). Prolific has been found to be superior to other recruitment platforms in relation to higher quality data (i.e. participants meaningfully responding to the researchers’ questions; Albert & Smilek, 2023). Notably, research has found that compared to other platforms, participants on Prolific are more likely to pass attention checks, provide meaningful answers, follow instructions, remember information, and work at an appropriate pace when responding to questions (Douglas et al., 2023).
All samples in the study were from the United Kingdom and were predominantly White British. Once recruited, participants completed an online consent form and the PLQ on Qualtrics on one occasion, which took approximately 10 minutes to complete. Attention checks were included to ensure high-quality responses. Participants were compensated with a small fee for completing the study questionnaires (∼£1.00). The sample was split into two (approximately equal) subsamples (n1 = 248 and n2 = 258) via SPSS (random sample of cases function). The first subsample was reserved for exploratory factor analysis (EFA), while the second subsample was reserved for confirmatory factor analysis (CFA).
Measures
Participants were instructed to answer questions on the construct ‘perfectionism’, specifically their knowledge, attitudes, and perceptions of perfectionism, and rate the extent to which they agree or disagree on a five-point scale (1 = strongly disagree to 5 = strongly agree).
Data Analysis
The first step was to explore the factor structure of the item pool using data from the first subsample (n1 = 248). The EFA procedure was conducted in Mplus 8.0 using maximum likelihood estimation and default oblique (GEOMIN) rotation. The procedure was iterative and followed several recommendations (Fabrigar & Wegener, 2012). Factor retention was explored using eigenvalues (in combination with parallel analysis), goodness of fit statistics for competing models, and model interpretability. The pattern of factor loadings from each model was assessed based on magnitude (≥.30 was considered meaningful), degree of cross-loading (number of items loading meaningfully on more than one factor; <.30), and interpretability (Morin et al., 2020).
The second step was to confirm the factor structure of the model identified from the EFA process. This step used data from the second independent subsample in this study (n1 = 258). The CFA was conducted in Mplus 8.0 using maximum likelihood estimation. We specified a first-order model in which: (a) items were constrained to load on target factors; and (b) all latent factors were specified to covary. We assessed the CFA model in relation to goodness of fit statistics and the magnitude and statistical significance of factor loadings (≥.30 was considered meaningful).
In both the EFA and CFA models, we used multiple fit indices to help evaluate overall model fit: chi-square statistic (χ2), comparative fit index (CFI), Tucker-Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root-mean-square residual (SRMR). In line with established guidelines, we considered models meeting the following criteria to reflect at least adequate model fit: >.90 CFI, TLI, <.08 RMSEA, 90% CI < .05 to <.08; <.08 SRMR (Marsh et al., 2004).
Results
EFA
In the first EFA model tested (using all 56 items), seven eigenvalues from the sample correlation matrix exceeded the corresponding eigenvalues derived from the parallel analysis. We therefore explored the seven-factor model. In this model, well-defined factors for recognition of self-oriented perfectionism, recognition of socially prescribed perfectionism, recognition of other-oriented perfectionism, seeking information on perfectionism, risk factors for perfectionism, treatments for perfectionism, and attitudes that promote help-seeking behaviour for perfectionism were evident. While this model was interpretable and in keeping with the item generation process, it provided suboptimal model fit (χ2/df = 2.10, CFI = .84, TLI = .79, RMSEA = .07 [.06, .07], SRMR = .04).
Geomin Rotated Loadings for the Seven-Factor EFA Model of the Final Perfectionism Literacy Questionnaire Items in Stage Two.
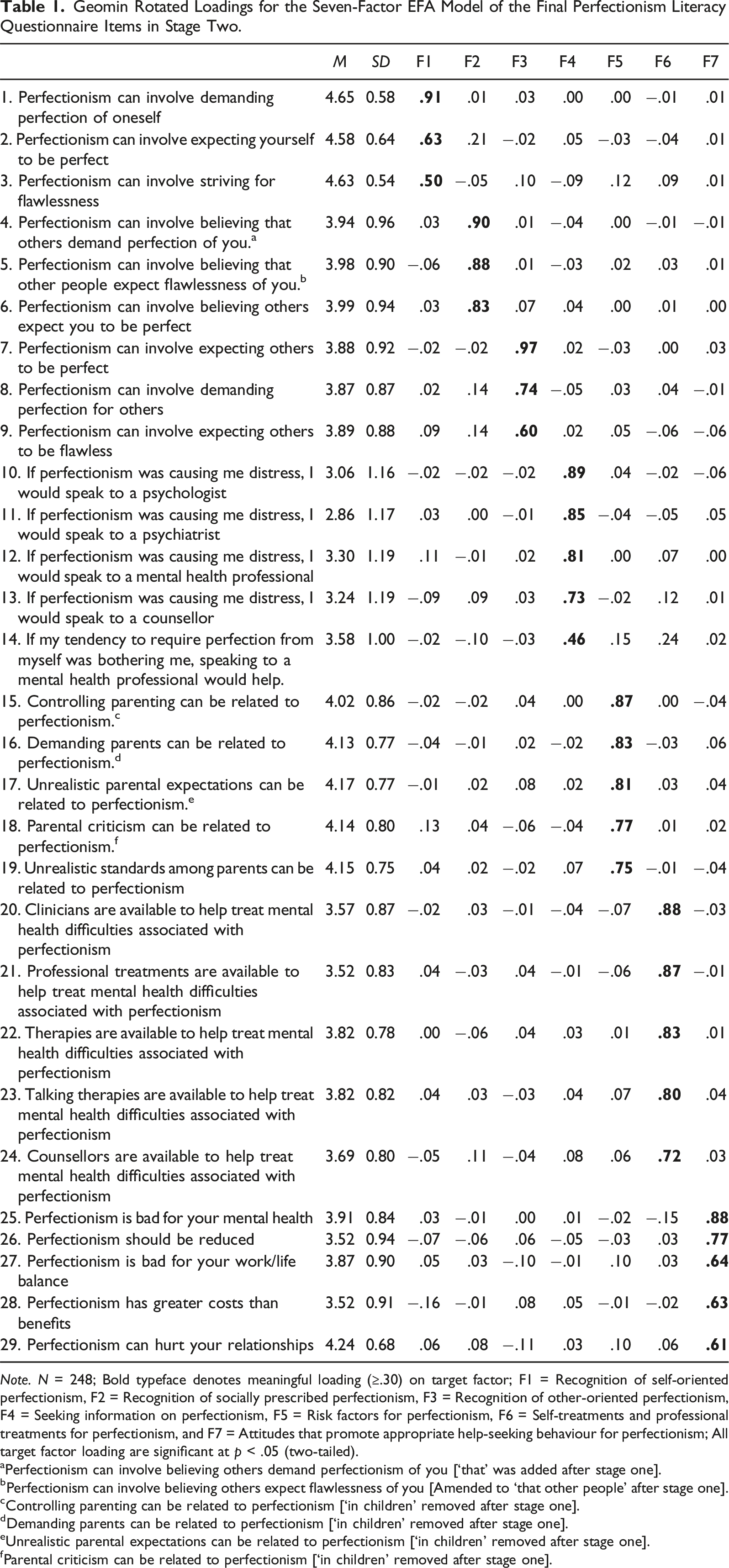
Note. N = 248; Bold typeface denotes meaningful loading (≥.30) on target factor; F1 = Recognition of self-oriented perfectionism, F2 = Recognition of socially prescribed perfectionism, F3 = Recognition of other-oriented perfectionism, F4 = Seeking information on perfectionism, F5 = Risk factors for perfectionism, F6 = Self-treatments and professional treatments for perfectionism, and F7 = Attitudes that promote appropriate help-seeking behaviour for perfectionism; All target factor loading are significant at p < .05 (two-tailed).
aPerfectionism can involve believing others demand perfectionism of you [‘that’ was added after stage one].
bPerfectionism can involve believing others expect flawlessness of you [Amended to ‘that other people’ after stage one].
cControlling parenting can be related to perfectionism [‘in children’ removed after stage one].
dDemanding parents can be related to perfectionism [‘in children’ removed after stage one].
eUnrealistic parental expectations can be related to perfectionism [‘in children’ removed after stage one].
fParental criticism can be related to perfectionism [‘in children’ removed after stage one].
CFA
Standardized Model Results and Factor Correlations for the Seven-Factor CFA Model of the Final Perfectionism Literacy Questionnaire Items in Stage Two.
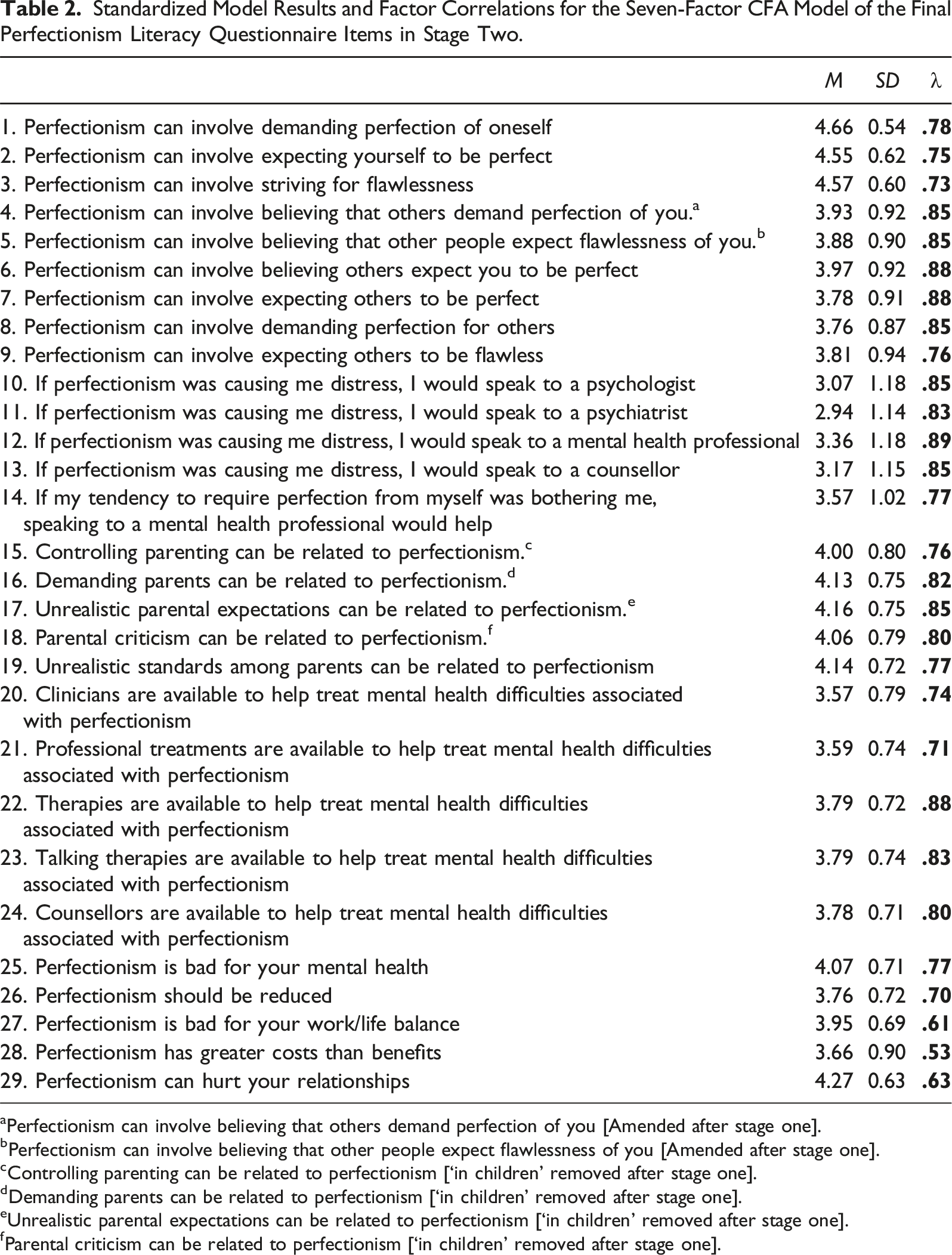
aPerfectionism can involve believing that others demand perfection of you [Amended after stage one].
bPerfectionism can involve believing that other people expect flawlessness of you [Amended after stage one].
cControlling parenting can be related to perfectionism [‘in children’ removed after stage one].
dDemanding parents can be related to perfectionism [‘in children’ removed after stage one].
eUnrealistic parental expectations can be related to perfectionism [‘in children’ removed after stage one].
fParental criticism can be related to perfectionism [‘in children’ removed after stage one].
Scale Readability
The Flesch-Kincaid grade level scores of the final items in the PLQ ranged from 5.2 (5th-11th grade, 11-17 year-olds) to 18.5 (11th-18th grade, 17 year-olds and above). Most items were between 11th-18th grade (N = 20), whereas the remaining items were between 5th-11th grade (N = 9). Based on these scores, the PLQ is likely to be most appropriate for those aged >17 years.
Stage Three
The purpose of stage three was to examine the construct validity of the seven-factor 29-item structure of the PLQ in relation to multidimensional perfectionism and attitudes towards help-seeking for mental health services. We had two exploratory aims in mind. The first was to examine whether perfectionism literacy is sufficiently distinct from these related constructs. The second was to identify the various ways these constructs link together.
Participants
The sample for this stage were 250 community adults (84 = male; 164 = female; 2 = nonbinary; M age = 37.10 years, SD = 13.34; range 18–82; 80.40% White British) recruited via Prolific Academic.
Measures
Perfectionism Literacy
Perfectionism literacy was measured using the seven-factor 29-item PLQ created in stage two.
Trait Multidimensional Perfectionism
Multidimensional perfectionism was measured using a 15-item short form of Hewitt and Flett’s (1991) Multidimensional Perfectionism scale (HF-MPS-SF; Hewitt et al., 2008). The HF-MPS-SF is formed of three subscales: self-oriented perfectionism (5 items; for example, ‘I must work to my full potential at all times’), socially prescribed perfectionism (5 items; ‘The better I do, the better I am expected to do’), and other-oriented perfectionism (5 items; for example, ‘I have high expectations for the people who are important to me’). Participants rated items on a 7-point scale from 1 (strongly disagree) to 7 (strongly agree). The HF-MPS-SF has high internal consistency (α ≥ .70) and exhibits similar psychometric properties to the original scale (Stoeber, 2018). Dimensions of the HF-MP-SF, for instance, are strongly correlated with self-oriented perfectionism (r = .91), socially prescribed perfectionism (r = .90), and other-oriented perfectionism (r = .81) of the original scale (Hewitt et al., 2008).
Attitudes Towards Seeking Mental Health Services
Attitudes towards mental health utilization were measured using the 24-item Inventory of Attitudes Toward Seeking Mental Health Services (IASMHS; Mackenzie et al., 2004). The IASMHS is formed of three subscales: psychological openness (8 items; e.g. ‘There are experiences in my life I would not discuss with anyone’), help-seeking propensity (8-items; e.g. ‘I would want to get professional help if I were worried or upset for a long period of time’), and indifference to stigma (8-items; e.g. ‘Having been mentally ill carries with it a burden of shame’). Participants rated items on a five-point scale from 1 (disagree) to (agree). The IASMHS exhibits good reliability and validity. For instance, three-week test-retest reliabilities ranged from (r = .64 to .91) across subscales (Mackenzie et al., 2004). Evidence supports the three-factor structure of the IASMHS (Hyland et al., 2015).
Data Analysis
A multi-stage procedure was implemented to analyze the data. The first stage involved screening the data (evaluating missing data and screening for outliers) and running a series of preliminary analyses (computing descriptive statistics, bivariate correlations, and scale reliability estimates). These analyses were conducted in IBM Statistics SPSS 28.0.
The second stage involved using network psychometrics to test the main study aims. We started by computing a graphical Gaussian model (GMM) via the ggmModSelect algorithm implemented in the qgraph R package (Epskamp & Fried, 2018). In a single stage estimation, the ggmModSelect algorithm automatically searches for the most optimal unregularized GGM model. This process involves: (a) generating a range of regularized network structures (100 by default) by varying the Least Absolute Shrinkage and Selection Operator (LASSO) tuning parameter; (b) re-estimating each network without regularization (non-zero edges are freely estimated and zero edges are fixed to zero); (c) selecting an optimal model based on the extended Bayesian information criterion (EBIC); and (d) further evaluating the selected model by stepwise adding and removing edges until the EBIC is optimized.
The final network structure includes study variables (depicted by nodes) and their pairwise relationships (depicted by edges connecting nodes together). The edges are weighted by partial correlation coefficients (with stronger relationships depicted by wider and more saturated edges). To provide a further visual aid, we identified clusters of nodes that are highly interconnected with one another using exploratory graph analysis (EGA; Golino & Epskamp, 2017) and coloured the nodes based on cluster membership. To identify important relationships between clusters, we computed network loadings and identified nodes with network-cross loadings that are substantively meaningful (>.10; Christensen et al., 2021). This process can be helpful in identifying relationships that are important from an intervention perspective (e.g. aspects of perfectionism literacy that share meaningful relationships with more general positive attitudes toward help-seeking behaviour).
Results
Data Screening and Preliminary Analyses
Descriptive Statistics, Bivariate Correlations, Edge Weights (Partial Correlation Coefficients), and Scale Reliability Estimates in Stage Three.
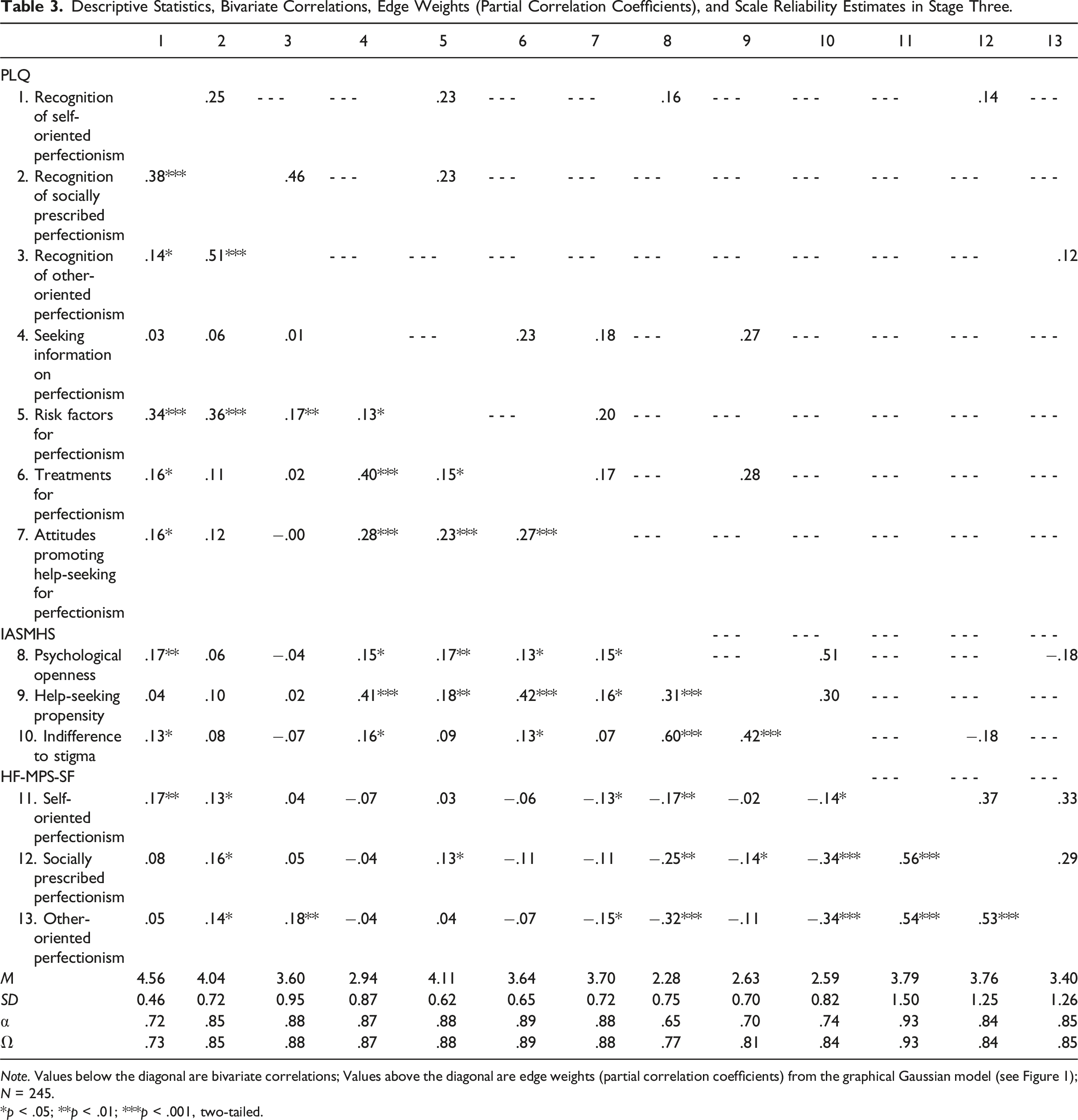
Note. Values below the diagonal are bivariate correlations; Values above the diagonal are edge weights (partial correlation coefficients) from the graphical Gaussian model (see Figure 1); N = 245.
*p < .05; **p < .01; ***p < .001, two-tailed.
Primary Analyses
The network structure is displayed in Figure 1. The network features 13 nodes and 20 edges (25.64% of all possible associations). The EGA identified four clusters. The first cluster is comprised of PLQ subscales that capture recognition of perfectionism characteristics and factors relevant to their development. The second cluster is comprised of the PLQ subscales that capture awareness of the negative consequences of perfectionism and how to seek help when in distress. The additional node that also loaded on the second cluster was the help-seeking propensity subscale of the IASMHS that captures willingness to seek professional help for psychological problems. The third cluster is comprised of the remaining two IASMHS subscales that capture willingness to openly acknowledge psychological problems without shame or a sense of disapproval. The fourth cluster is comprised of the HF-MPS-SF subscales that capture levels of trait perfectionism. Graphical Gaussian model (GGM) in stage three. Note. The network contains nodes representing perfectionism literacy (as measured by the PLQ), attitudes toward seeking mental health services (as measured by the IASMHS), and trait perfectionism (as measured by the HF-MPS-SF). Solid lines represent positive partial correlation coefficients; Dashed lines represent negative partial correlation coefficients; The width and saturation of an edge represent the magnitude of the partial correlation coefficient (see Table 3 for edge weight estimates).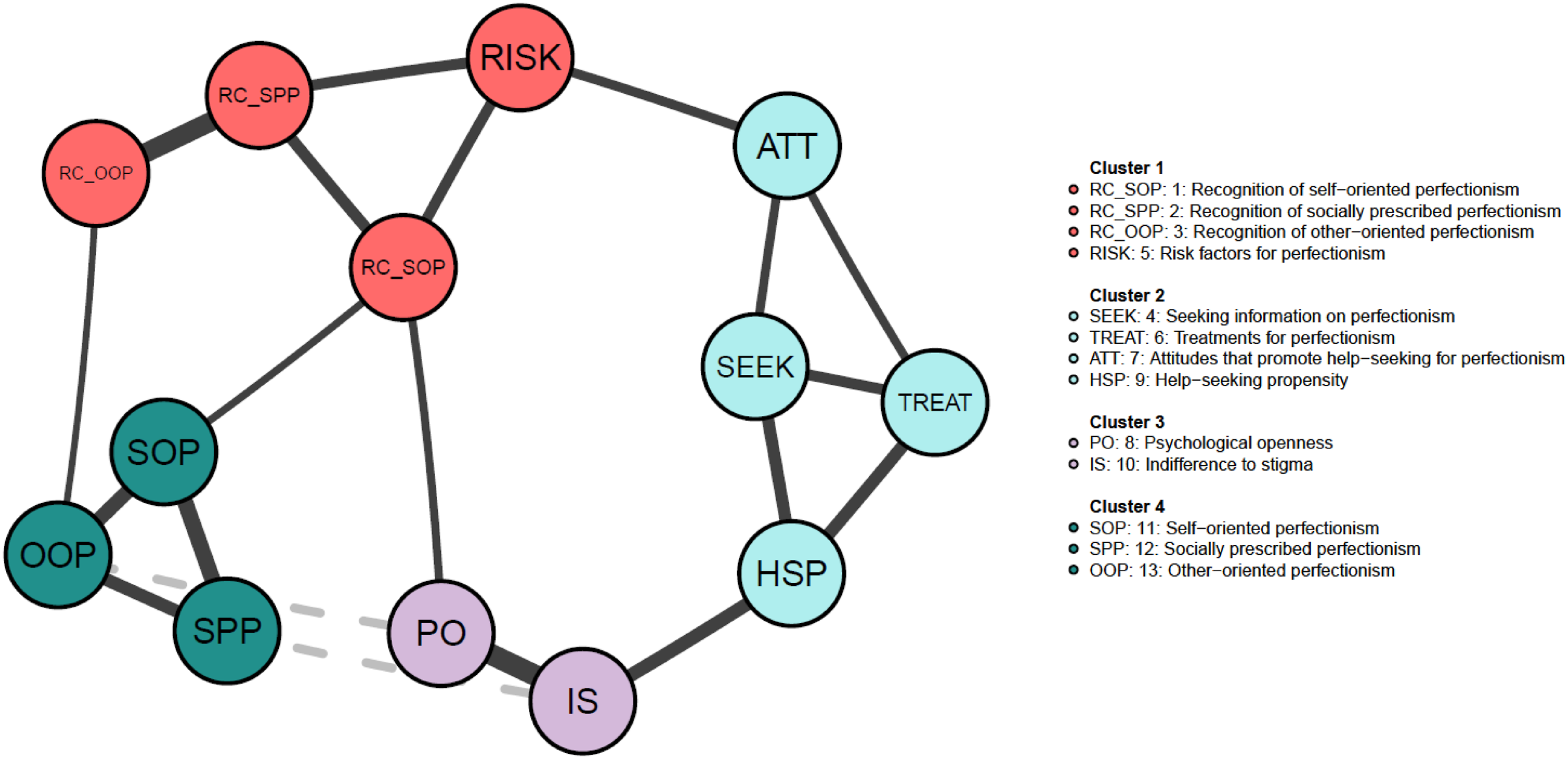
The edge weights are reported in Table 3. We were interested in connections between nodes belonging to independent clusters (i.e. bridges). The network loadings suggest that the following bridges are substantively meaningful. Help-seeking propensity was positively associated with indifference to stigma (r = .30). Risk factors for perfectionism was positively associated with attitudes that promote help-seeking behaviour for perfectionism (r = .20). Indifference to stigma was negatively associated with socially prescribed perfectionism (r = −.18). Psychological openness was negatively associated with other-oriented perfectionism (r = −.18). Recognition of self-oriented perfectionism was positively associated with psychological openness (r = .16).
Stage Four
The purpose of stage four was to examine whether the PLQ can capture changes in perfectionism literacy after watching an educational animation on perfectionism (Hill et al., 2021). This minimal intervention was selected for an initial test of the scale as it is a cheap, easily administered, accessible, and scalable resource that might be used by others to improve perfectionism literacy. Similar educational animations have also been shown to be effective in regard to knowledge, attitudes, and willingness to seek support in previous research (e.g. Curran et al., 2023).
Participants and Procedure
We recruited two samples for this study from Prolific Academic. The first sample were 173 community adults (38 = male; 135 = female; Mage = 35.81 years, SD = 11.65; range 18–78; 83.20% White British).
The second sample were 149 community adults (47 = male; 102 = female; Mage = 34.95 years, SD = 11.62; range 18–68; 78.50% White British).
In both samples, we assigned participants to an intervention group (watched the perfectionism animation) or control group and used repeated measures (pre-test, post-test measurement). We only employed randomization in the second subsample. In the first sample, there were 94 participants assigned to the intervention group and 79 to the control group. In the second sample, there were 74 participants randomly assigned to the intervention group and 75 to the control group.
Participants completed the PLQ on two measurement occasions. Immediately after completion of the questionnaire, the intervention group watched a perfectionism animation video (02:27 [min: sec]). The animation: (a) defines perfectionism (‘having unrealistic expectations and thinking and feeling negatively when those expectations aren’t met’); (b) highlights that perfectionism is dimensional (continuous) rather than taxonic (categorical); (c) introduces three core dimensions (‘flavours’) of perfectionism (‘expecting yourself to be perfect’, ‘expecting others to be perfect’, and ‘thinking other people expect you to be perfect’); (d) highlights that perfectionism can impact negatively on mental health; (e) provides help-seeking advice for when perfectionism is distressing (e.g. ‘speak to someone you trust’); and (f) offers some tips on how to become less perfectionistic (‘don’t base your self-esteem on how you perform’, ‘cut yourself some slack’, and ‘getting things done is better than getting things perfect’). The control group completed the PLQ only.
After watching the video on the first measurement occasion, participants in the intervention group were asked to report on the video content (‘According to the video, how many flavours does perfectionism come in?’, ‘Please state a top tip from the video’ and ‘What do you think the take-home message was?’). We used this data to screen for participant engagement (i.e. cases with no responses or irrelevant information across the answers). Both the intervention and control group were instructed that they would be recontacted in three days’ time to complete the second questionnaire. Three days later, both groups were asked to complete the PLQ only.
Data Analysis
We employed a two-way mixed factorial ANOVA (group by time). Our dependent variables were components of perfectionism literacy. Prior to running these models, we confirmed that the dependent variables were approximately normally distributed in each cell of the design (via visual inspection of Q-Q plots). We confirmed homogeneity of variances (Levene’s test for equality of variances) and covariances (via Box’s test of equality of covariance matrices). We report the generalized eta square (η2 G ) as the effect size for main and interaction effects with η2 G denoting small = 0.01, medium = 0.06, and large = 0.14 effects (Cohen, 1988). We also computed independent samples t-tests and Hedges’ g* with 95% CIs using the Shiny app developed by Delacre et al. (2021) for pre- and post-intervention comparison of groups and interpreted effects using common guidelines: small effect = 0.20, medium effect = 0.50, and large effect = 0.80 Cohen (1988).
Results
Sample without Randomization
Mean, Standard Deviation, and Effect Size Estimates for Pre- and Post-intervention Between-Subjects Differences in Perfectionism Literacy in Stage Four.
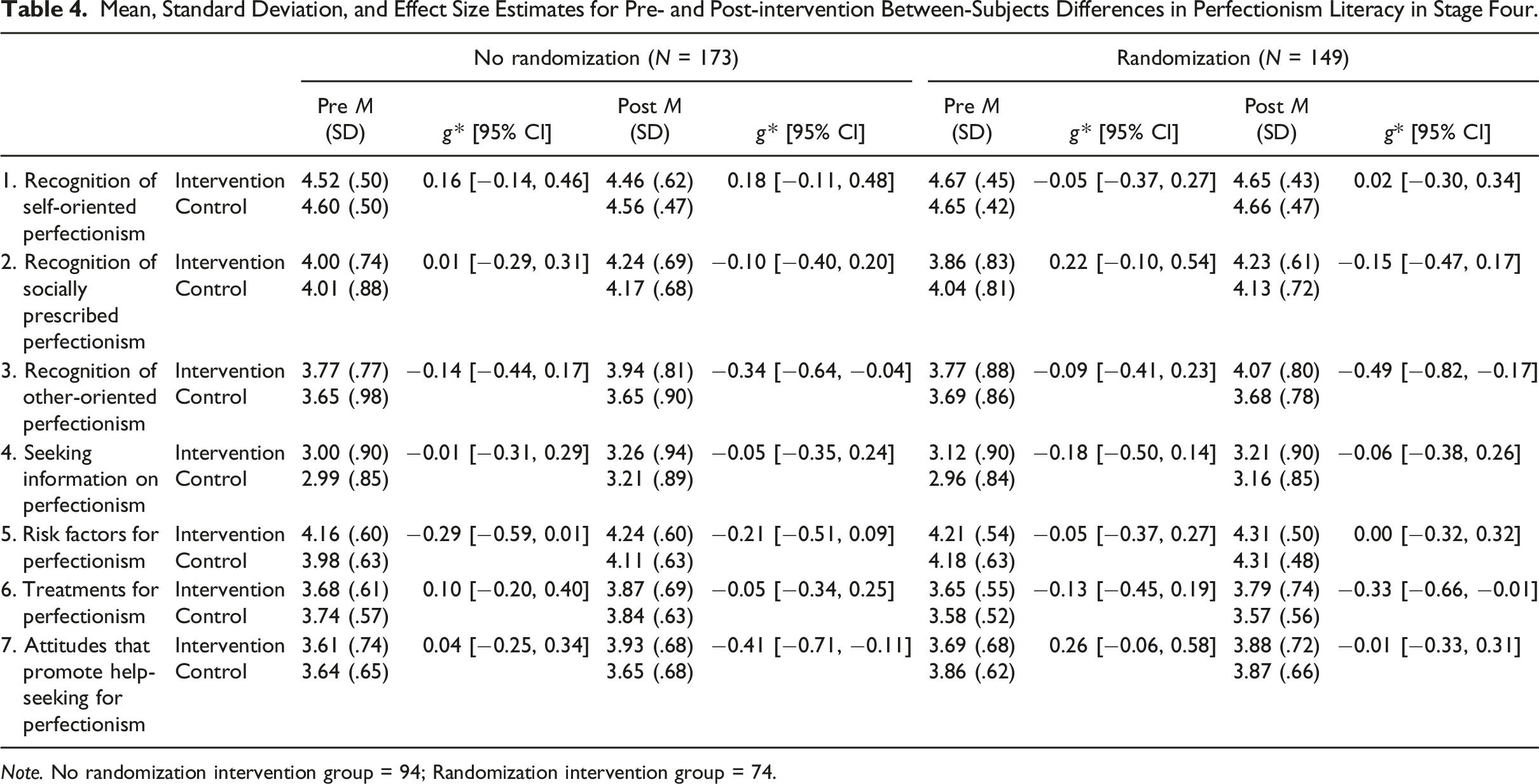
Note. No randomization intervention group = 94; Randomization intervention group = 74.
Main Time, Group, and Interaction (Time X Group) Effects in Stage Four.
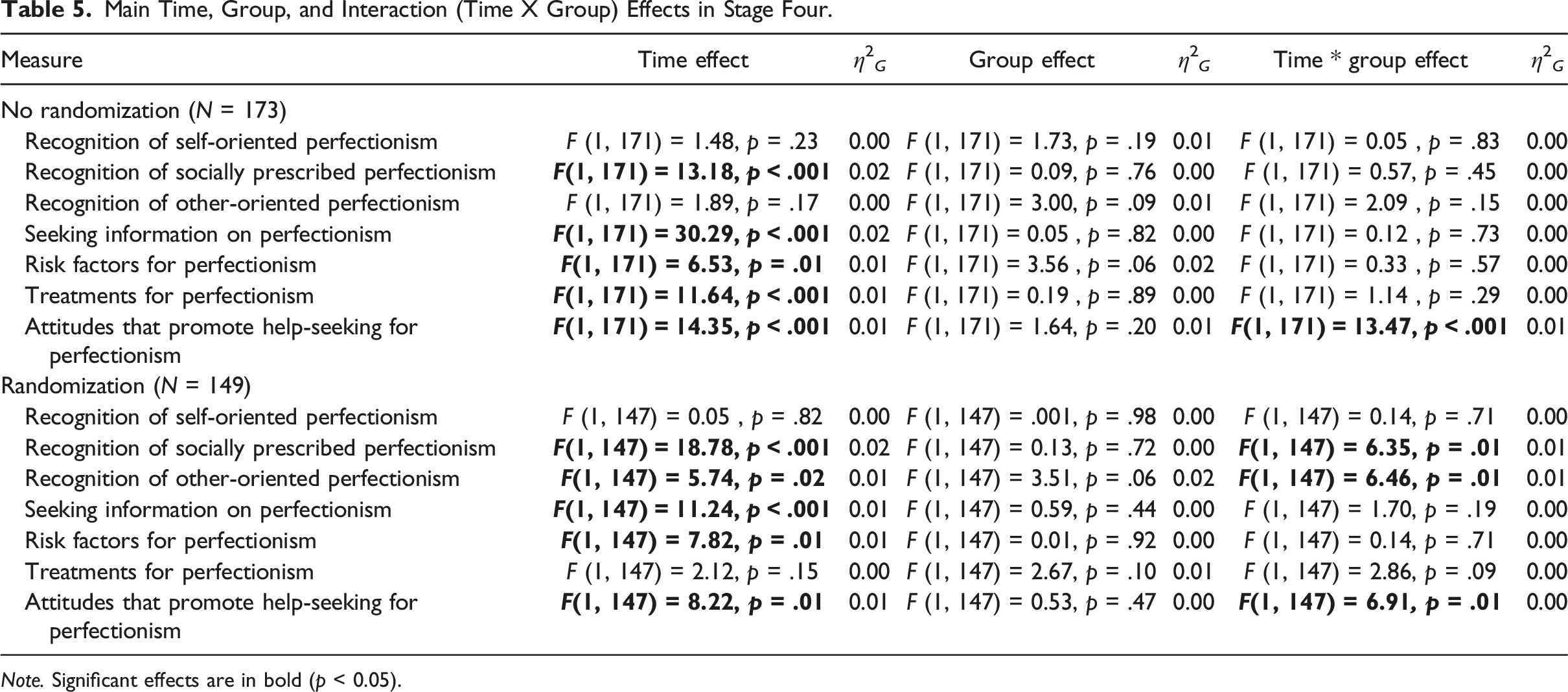
Note. Significant effects are in bold (p < 0.05).
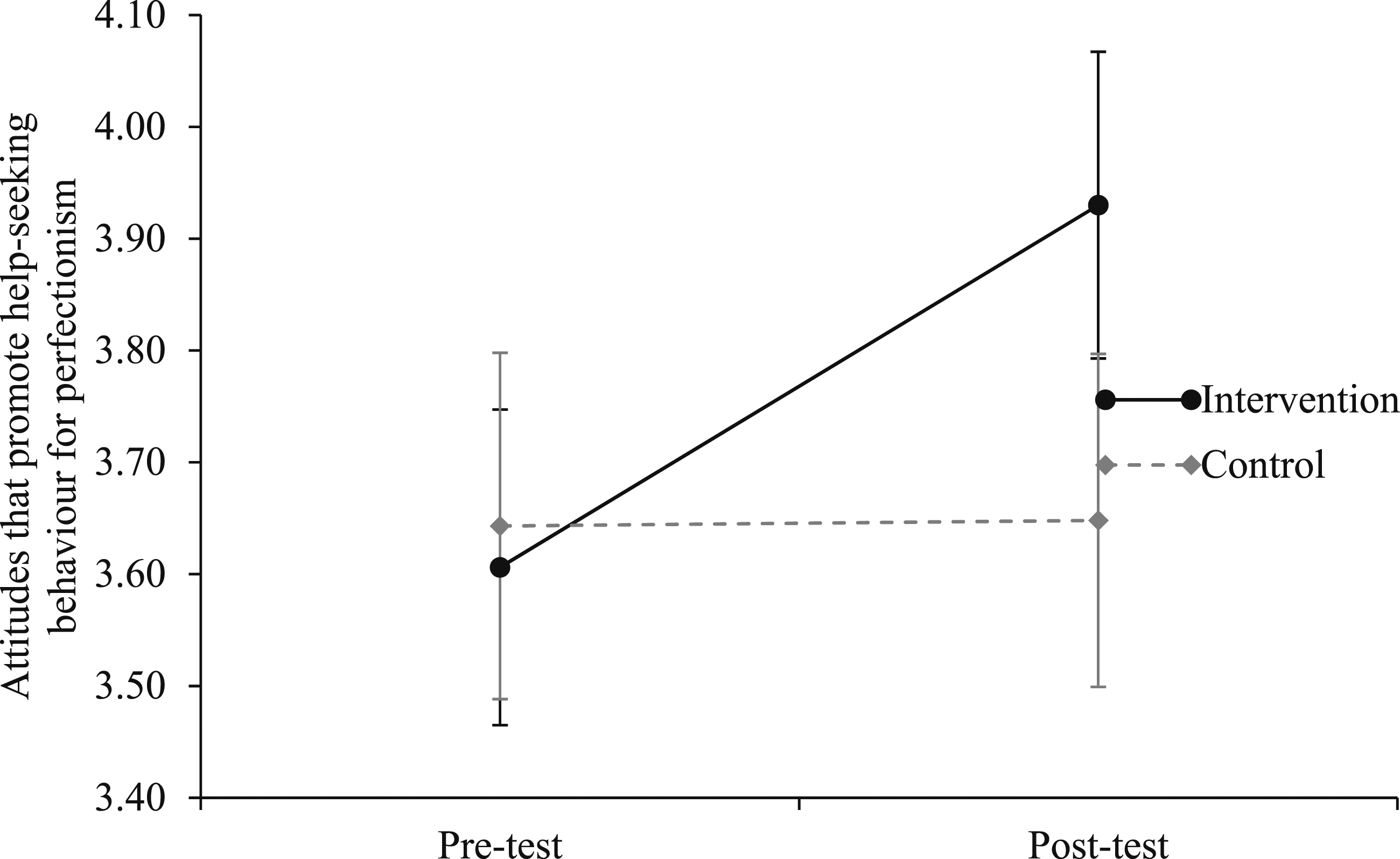
The interaction of attitudes that promote help-seeking behaviour for perfectionism in the sample without randomization.
Sample with Randomization
In analyzing the experimental design data with randomization, we found significant interaction effects in three models (see Tables 4 and 5).
The first interaction was in the model examining recognition of socially prescribed perfectionism (see Figure 3). In this model, the main effect for measurement occasion was small and significant (F (1, 147) = 18.78, p < .001, η2
G
= .02), while the main effect for group status was negligible and non-significant (F (1, 147) = .13, p = .72, η2
G
= 0.00). The interaction effect for recognition of socially prescribed perfectionism was small and significant (F (1, 147) = 6.35, p = .01, η2
G
= 0.01). The post-intervention between-group difference in means was statistically non-significant (t (147) = 0.88, p = .38) and small (∆M = 0.10, g* = −0.15 [−0.47, 0.17]). The interaction of socially prescribed perfectionism in the sample with randomization.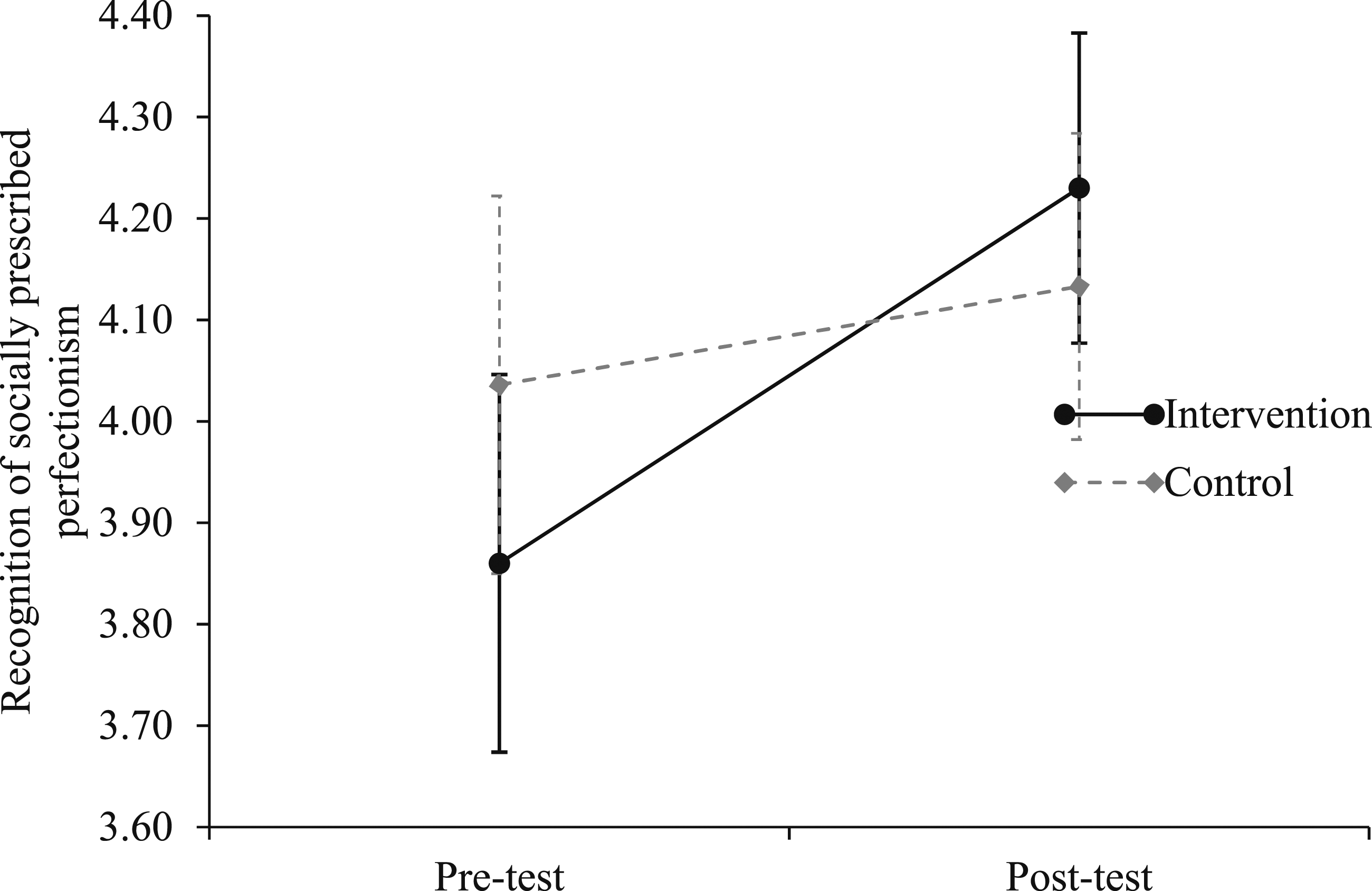
The second interaction was in the model examining recognition of other-oriented perfectionism (see Figure 4). In this model, the main effect for measurement occasion was small and significant (F (1, 147) = 5.74, p = .02, η2
G
= 0.01), while the main effect for group status was small and non-significant (F (1, 147) = 3.51, p = .06, η2
G
= 0.02). The interaction effect for the two independent variables on recognition of other-oriented perfectionism was small and significant (F (1, 147) = 6.46, p = .01, η2
G
= .01). The post-intervention between-group difference in means was statistically significant (t (147) = 2.96, p < .01) and medium (∆M = 0.39, g* = −0.49 [−0.82, −0.17]). The interaction of other-oriented perfectionism in the sample with randomization.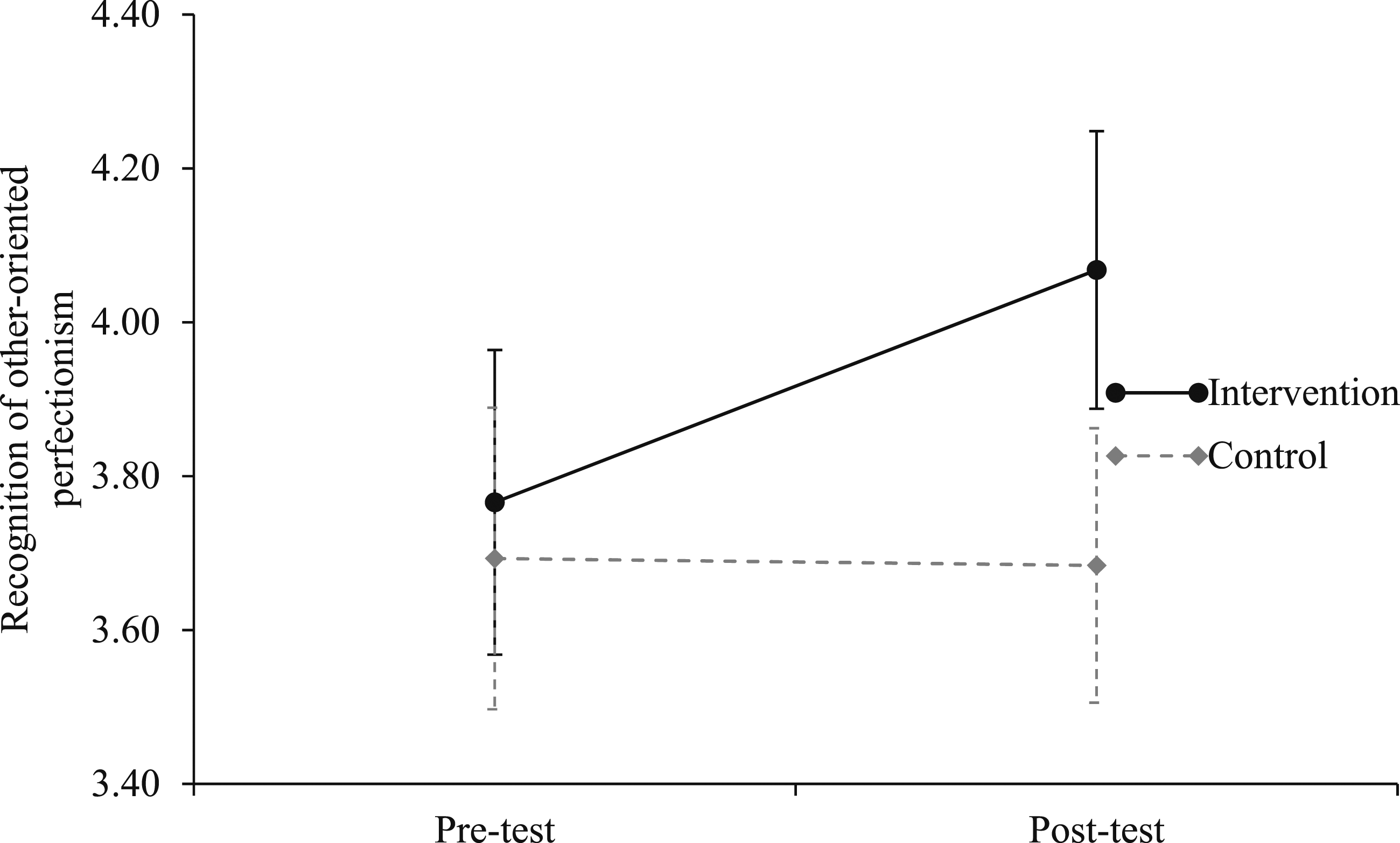
The third interaction was in the model examining attitudes that promote help-seeking behaviour for perfectionism (see Figure 5). In this model, the main effect for measurement occasion was small and significant (F (1, 147) = 8.22, p = .01, η2
G
= 0.01), while the main effect for group status was negligible and non-significant (F (1, 147) = .53, p = .47, η2
G
= .00). The interaction effect for the two independent variables on attitudes that promote help-seeking behaviour for perfectionism was negligible but statistically significant (F (1, 147) = 6.91, p = .01, η2
G
= 0.00). The post-intervention between-group difference in means was statistically non-significant (t (147) = 0.10, p = .92) and negligible (∆M = 0.01, g* = −0.01 [−0.33, 0.31]). The interaction of attitudes that promote help-seeking behaviour for perfectionism in the sample with randomization.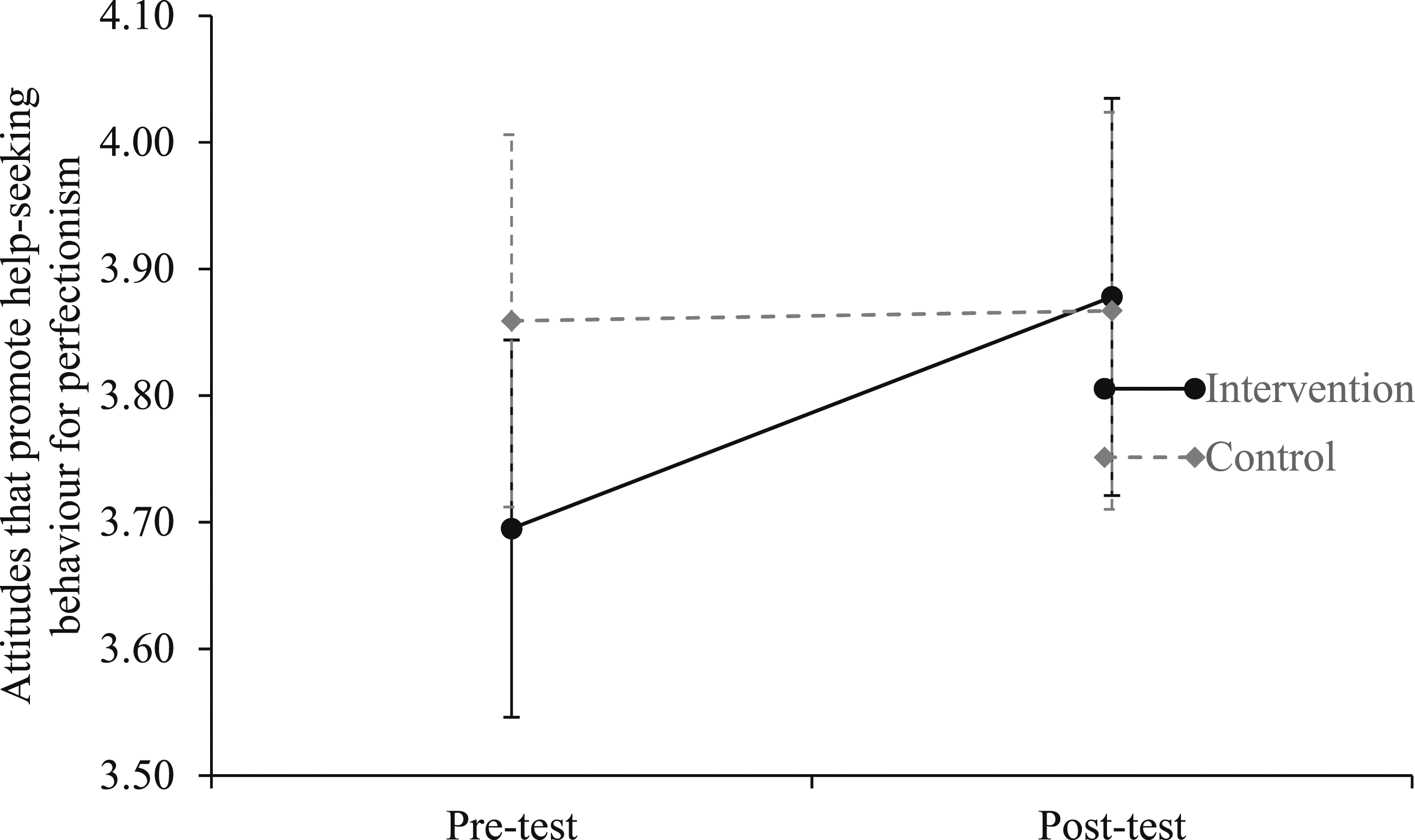
Discussion
The current study sought to develop the first measure of perfectionism literacy. To do so, we used a multi-stage process. Stage one involved the generation and refinement of PLQ items. Stage two examined the structure of the PLQ items using exploratory and confirmatory analyses. Stage three examined the construct validity of the PLQ with measures of multidimensional perfectionism and attitudes towards help-seeking. The result of this work is a seven-factor 29-item measure with strong evidence for its reliability and validity. Stage four showed some changes in perfectionism literacy following a short video alluding to the possible utility of the instrument for education and prevention work.
Measuring Perfectionism Literacy
Our work on developing a measure of perfectionism literacy was guided by Hewitt and Flett’s (1991) multidimensional model of perfectionism and Jorm et al.’s (1997) conceptualization of mental health literacy. The findings of stages one and two provided strong support for our approach. Notably, the EFA and CFA derived a seven-factor structure that aligned with the five overarching components of perfectionism literacy but also included the ability to recognize the distinct features of the three trait dimensions of perfectionism. With the exception of a focus on the availability of general professional treatments, rather than self-treatments, the item content of the PLQ also closely matches components of mental health literacy. Overall, then, the structure of our measure of perfectionism literacy appears as intended and is analogous to other measures of mental health literacy.
In support of the construct validity, stage three found components of the PLQ to be largely distinct from measures of trait perfectionism and general attitudes towards help-seeking. In other words, we are confident that knowledge about perfectionism should not be conflated with being perfectionistic. We can, therefore, expect people who are perfectionistic to have both higher and lower levels of knowledge about the features, risks, and interventions associated with perfectionism. This was also the case for general attitudes toward help-seeking, except for a link between a general indifference towards stigma and a lower propensity for help-seeking for perfectionism. It is also noteworthy that the PLQ appears to include two larger components – recognition and development of perfectionism along with knowledge of support and propensity to seek support. As such, these two components may themselves be discernible in regard to what people know about perfectionism versus the likelihood of engaging in behaviours to help themselves or others. The distinction between these two clusters may be relevant in practical settings and should be explored further in future work.
In the final stage, we found some evidence that the PLQ is responsive to change following a short educational video. Specifically, recognition of other-oriented perfectionism and attitudes that promote help-seeking behaviour for perfectionism both increased in a significant and non-trivial manner. This is consistent with research suggesting that mental health literacy can be increased using short interventions (e.g. Ueda et al., 2021). There were other instances of changes (e.g. recognition of socially prescribed perfectionism), which were more mixed (significant interaction but effect size estimates including zero). In addition, of the two effects that were moderate in size, one was found when randomization was not used, hence is less robust and should be interpreted with caution. Although promising, given the nature of the intervention (and lack of randomization in one sample), the findings are best considered tentative until additional research can take place. We are mindful that the nature of these changes could reflect either features of the educational video or the responsiveness of the PLQ. Testing the impact of other interventions on the PLQ is therefore also essential prior to wider use of the instrument.
Limitations and Future Directions
There are limitations of the study. First, we adopted Hewitt and Flett’s (1991) conceptualization of perfectionism as the basis for the instrument and focused on trait perfectionism. Our model therefore does not include reference to other approaches or aspects of perfectionism (e.g. perfectionistic self-presentation). Second, our samples were community-based middle-aged adults. Confirmation of the validity and reliability of the instrument in other samples (e.g. students, teachers, health care professionals) is required. This would also enable comparisons between groups and testing for presumed differences in perfectionism literacy (e.g. community samples vs. clinical psychologists). Third, while we were able to establish construct validity in relation to measures of perfectionism and general attitudes towards help-seeking, future work of this kind is needed to further establish convergent and predictive ability (e.g. does perfectionism literacy predict actual help-seeking behaviour for perfectionism). Fourth, in the randomized intervention, although we instructed participants not to access any information on perfectionism prior to completing the PLQ on the second occasion, we were unable to control for this. Thus, it is possible that changes in levels of perfectionism literacy were due to factors other than the perfectionism animation intervention. Finally, while the intervention was somewhat effective in increasing levels of perfectionism literacy, the time lag between measurement occasions was short (i.e. three days). To examine longer lasting effects on perfectionism literacy, longer follow-up measurement is required (see Freţian et al., 2021).
Conclusion
We provide the first measure of perfectionism literacy – the PLQ. The PLQ has good factorial validity and construct validity. There was tentative evidence that it is responsive to an educational intervention. Therefore, the measure could be useful in improving recognition and prevention of mental health issues linked to perfectionism.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.