
Abstract
The Strengths and Difficulties Questionnaire (SDQ) is a brief instrument developed primarily for screening children and adolescents for social-emotional learning. The SDQ contains four factors related to socio-emotional difficulties and one factor related to prosocial behaviour. However, studies of its factor structure have produced mixed results. The present study examined whether the original five-factor model of the SDQ could be replicated with children in India. The sample consisted of 407 children aged 4–8 years with neurotypical development who were recruited across the states of North India. Parents and teachers were recruited through purposive sampling and completed the SDQ online. Confirmatory factor analysis (CFA) was conducted to assess the factor structure of the SDQ. The results showed that the five-factor model was a good fit for parents and an adequate fit for teachers. The results from this study provide evidence for the construct validity of the SDQ with children in India. Hence, these findings provide support for its use in screening the social-emotional functioning of children living in India.
Introduction
Social-emotional learning is the ability to engage appropriately in social interactions and regulate emotions effectively (Xie et al., 2019). Social-emotional learning contributes to early childhood school readiness and classroom and school adjustment (Denham & Brown, 2010). Increased attention to social-emotional problems in children has resulted in more awareness among clinicians and parents of the escalated risk of associated adverse outcomes, such as poor academic performance and psychiatric disorders (Briggs-Gowan & Carter, 2008).
However, the use of social-emotional screening tools can be restricted due to concerns such as the lack of appropriate training available to paediatricians to perform the screenings. This often results in clinicians relying only on their clinical impressions when evaluating this important aspect of a child’s development. Moreover, failing to utilize screening measures in schools and clinics can lead to delayed identification of social-emotional problems, resulting in late formal placements in programmes for children with social emotional disturbances (Muzzolon et al., 2013; Squires et al., 2001).
The Strengths and Difficulties Questionnaire (SDQ) is a brief instrument developed primarily for screening for social-emotional learning. The tool has been translated into more than 40 languages and meets the need for practical, cost-friendly, and easy-to-use instruments (Giannakopoulos et al., 2009). The SDQ is available in a range of formats, from a three-band categorization to a newer four-band categorization. For example, parent–teacher and child reports on a population-based UK survey indicated cut-off points such as 80% of children in the community are considered normal, 10% of children are in the borderline range, and 10% of children are in the abnormal range (Idris et al., 2019). The newer four-band categorization categorises children as close to average, slightly raised, high/low, and very high/very low. For example, scoring high on total difficulties would indicate that the child has social-emotional learning concerns. Goodman (2001) evaluated the psychometric properties of the SDQ by gathering data from parents and teachers of children aged 4–16 years in the United Kingdom. Factor analysis yielded a five-factor subscale solution (emotional problems, conduct problems, hyperactivity, peer problems, and prosocial behaviour) for parents’ and teachers’ reports (Chiorri et al., 2016; Goodman, 1997, 2001).
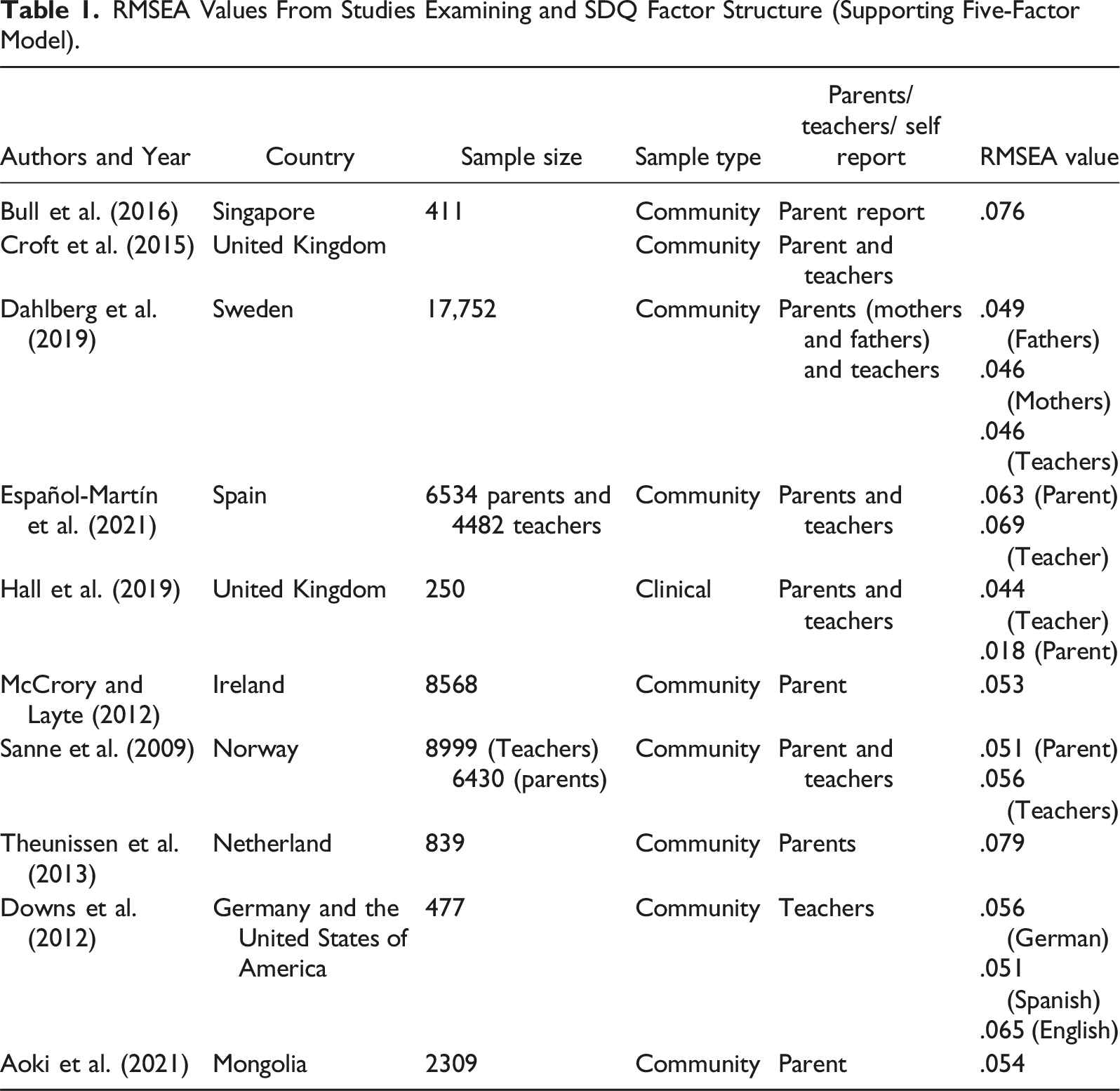
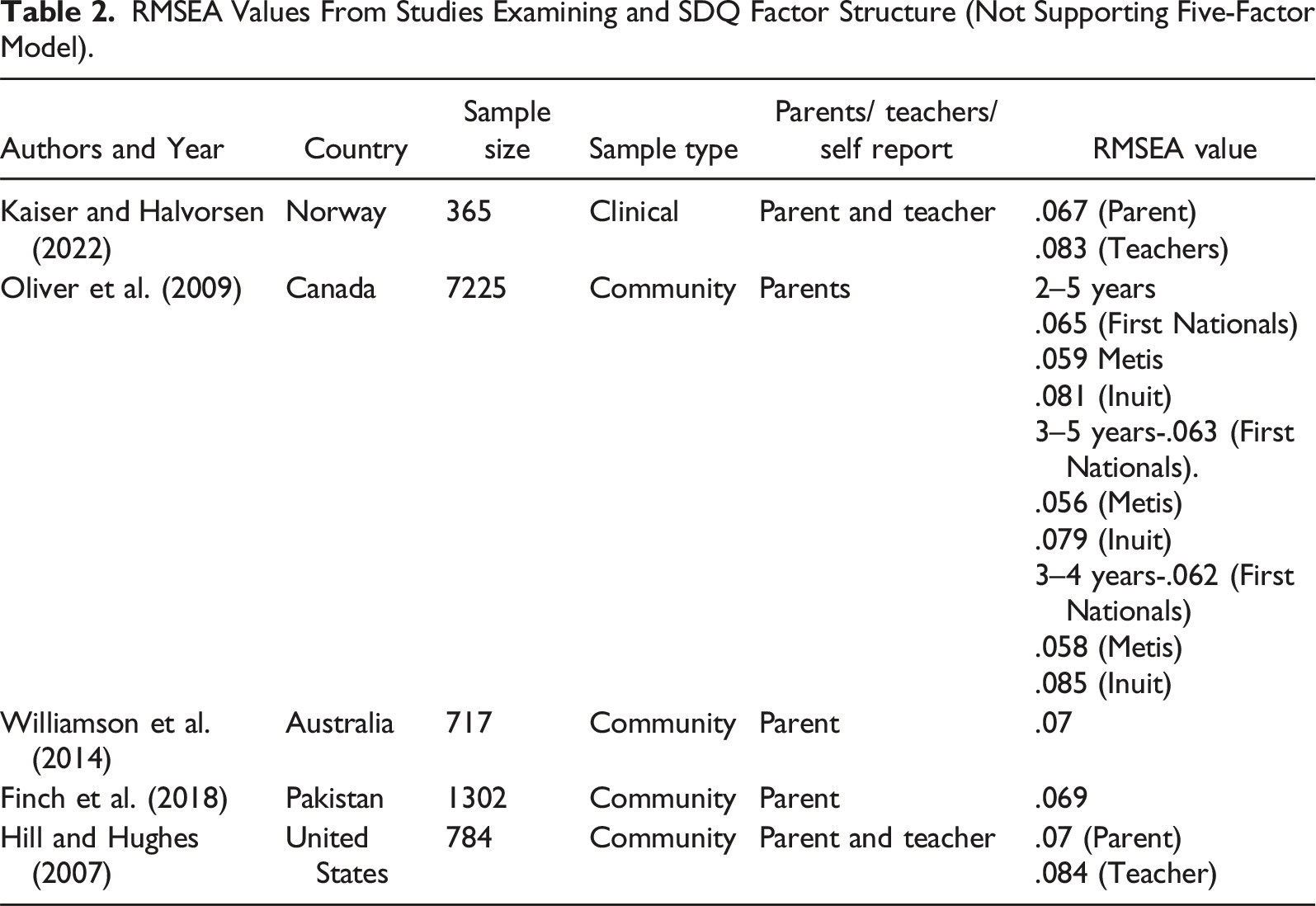
Studies in the past have reported that the parent and teacher SDQ five-factor model was a good fit for children aged 4–12 years with neurotypical development (Bull et al., 2016; Chiorri et al., 2016; Croft et al., 2015; Dahlberg et al., 2019; Goodman, 2001; Hall et al., 2019; Theunissen et al., 2013; Van Widenfelt et al., 2003) (Figure 1 & Table 1). However, some studies have also concluded that the SDQ five-factor model was not a good fit for reports from parents and teachers (Finch et al., 2018; Hill & Hughes, 2007; Kaiser & Halvorsen, 2022; Oliver et al., 2009; Thabet et al., 2000; Williamson et al., 2014) (Table 2). Proposed five-factor-model of parents and teachers SDQ data to be tested. RMSEA Values From Studies Examining and SDQ Factor Structure (Supporting Five-Factor Model). RMSEA Values From Studies Examining and SDQ Factor Structure (Not Supporting Five-Factor Model).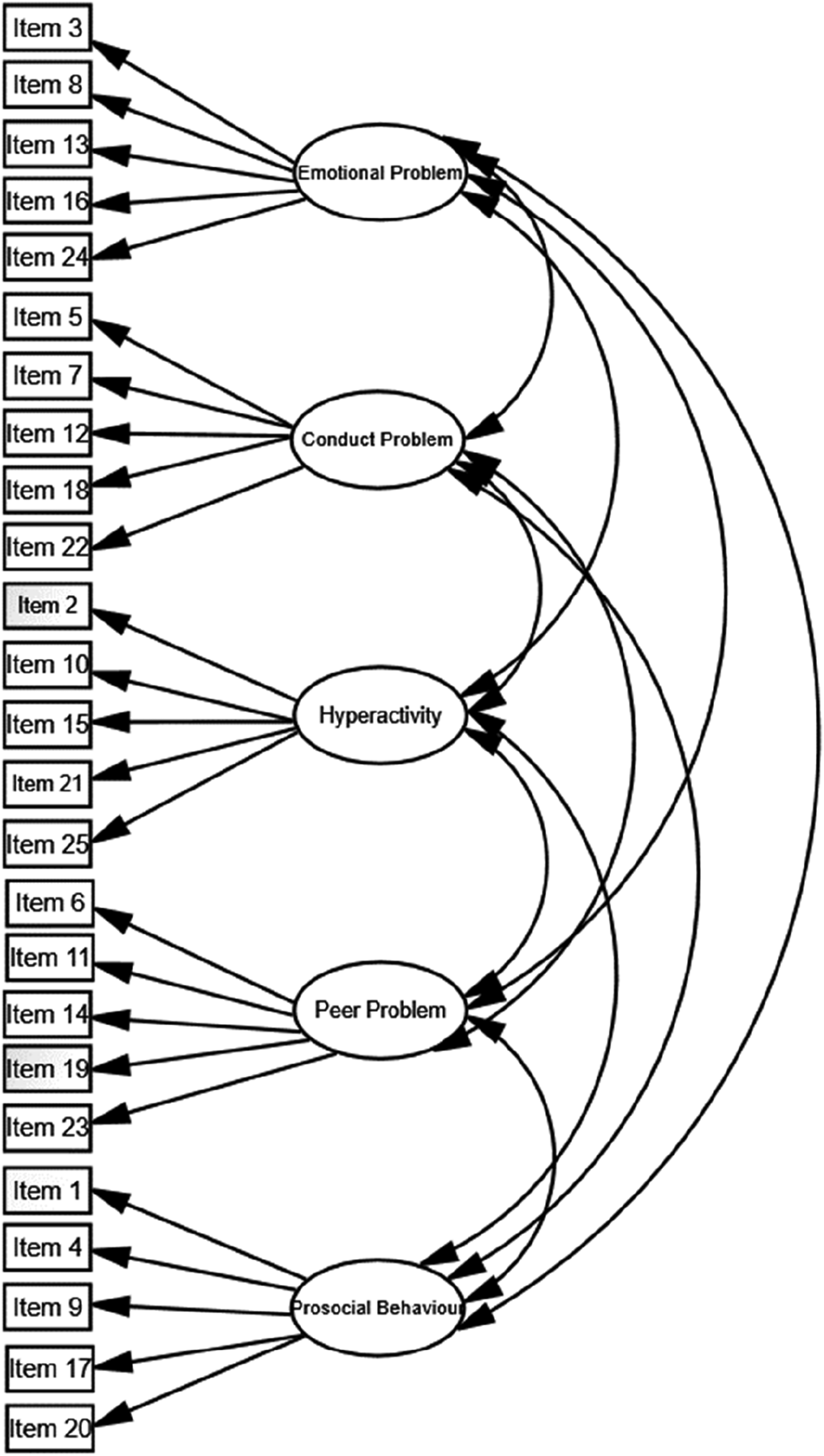
In India, existing literature reports a two-factor model consisting of the two factors of total difficulties and prosocial behaviour for adolescents aged 12–19 years from northern states of India. But the five-factor model of the English, Hindi, and Malayalam language versions of the SDQ has also been validated for assessing adolescents with typical development (TD), with an average to good fit for both self and parent’s reports (Singh et al., 2015; Stevanovic et al., 2015). The SDQ is suitable for a low- and medium-income country like India because it is free of cost, easy to use, easily accessible, and requires no training for administration. However, studies have yet to evaluate whether the five-factor model is a good fit for the reports from parents and teachers of children aged 4–8 years in India.
In the current study, the SDQ was administered to parents and teachers of children with neurotypical development in India. These data were used to determine whether the original five-factor model of the SDQ was suitable for use in India. Therefore, the hypothesis for this study is that the internal structure validity of the SDQ will be demonstrated by finding the five factors (emotional problems, conduct problems, hyperactivity, peer problems, and prosocial behaviour) previously reported in the literature for parents and teachers of children with neurotypical development (Chiorri et al., 2016; Goodman, 2001).
Method
Participants
Sociodemographic Characteristics of participants (parents).
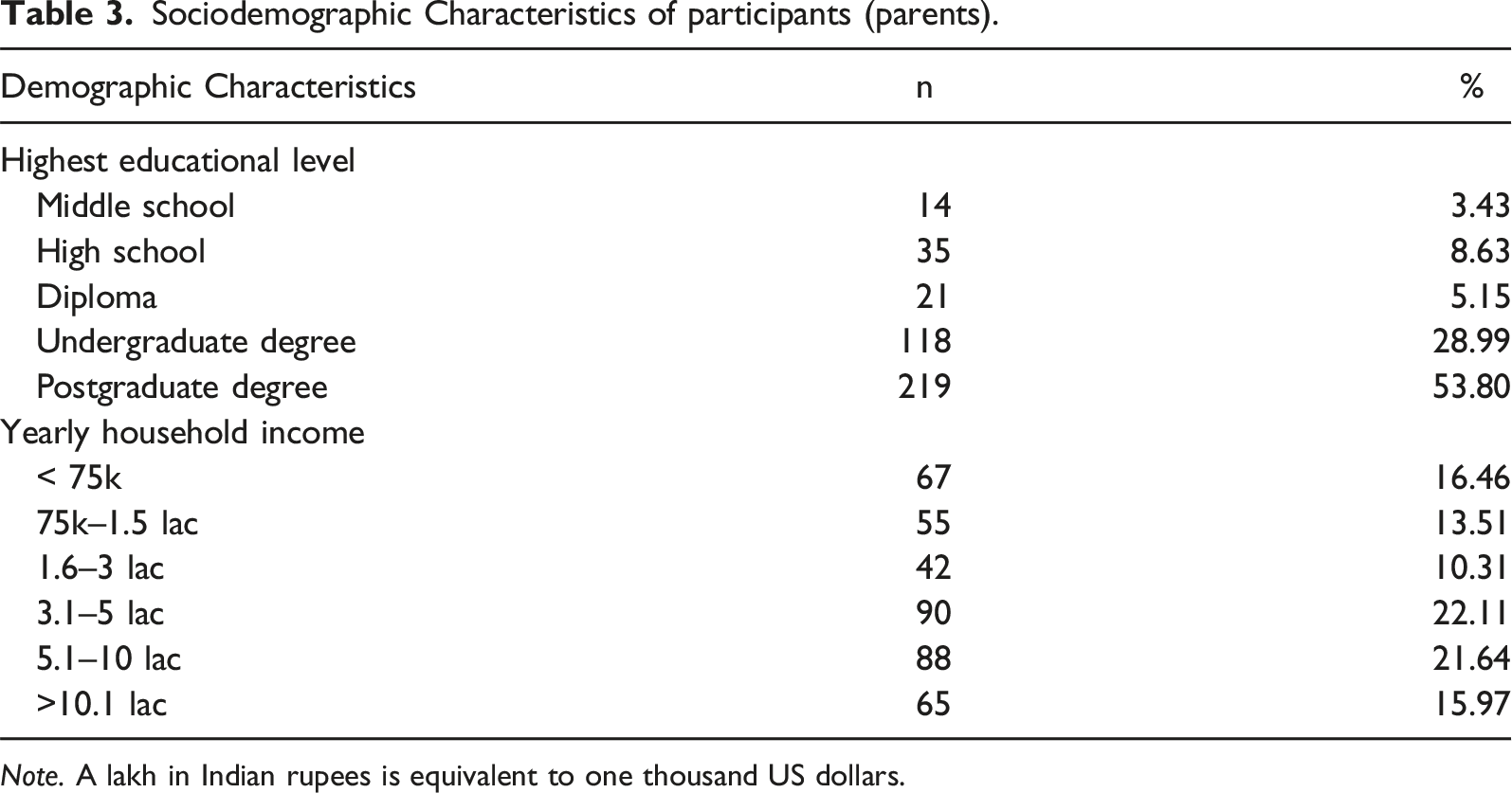
Note. A lakh in Indian rupees is equivalent to one thousand US dollars.
Inclusion criteria for participants were parents and teachers of children in the age range of 4–8 years who were citizens of India and were able to read, write, and speak at least to Primary 6 level in either English or Hindi. Exclusion criteria were parents whose child was not currently attending school.
Measures
Demographic Questionnaire
A demographic questionnaire was designed for this study to collect information from the parents on the child’s age, gender, and class; parent’s gender, level of education, age, and yearly family income; and whether the child had a disability.
Strengths and Difficulties Questionnaire (SDQ; Goodman, 2001).The SDQ was developed in the United Kingdom. This screening measure evaluates social-emotional functioning in children aged 2–17 years (Goodman, 2001). It comprises 25 questions under five domains: (a) emotional symptoms, (b) conduct problems, (c) hyperactivity/inattention, (d) peer-relation problems, and (e) prosocial behaviour. For children, the measure can be completed by both parents and teachers, while for adolescents there is also a self-report version (Goodman, 1997). This screening tool includes a 3-point rating scale: not true, somewhat true, and certainly true. The scoring for the SDQ comprises the total difficulty score, which is obtained by summing the scores for all four problem scales, excluding the prosocial scale. The total score ranges from 0 to 40. The cut-off scores for the SDQ scores are ‘normal’, ‘borderline’, and ‘abnormal’ (Goodman, 2001).
The SDQ has found to have sound psychometric properties, with an adequate internal consistency (Cronbach’s alpha = .73) and a high test–retest reliability of r = .62 (Brown, 2006; as cited in Sheel et al., 2023a). The discriminative comparing clinical and community samples and convergent validity assessed using the Child Behaviour Checklist (CBCL) were also strong, r = .80 and r = .50, respectively, and the specificity and sensitivity were excellent, above 70% assessed on British children aged 5–15 years (Goodman, 2001; Kresten et al., 2016) Although the developers of the SDQ offer the option of a Hindi-language version on their Web site, an examination of this found there to be errors in translation. Hence, a further translation was undertaken for the purposes of this study (Sheel et al., 2023b).
Procedure
The study received a Human Research Ethics Committee approval (H8285) to administer the screening questionnaires to parents and teachers of children ages 4–8. Data collection was conducted online between August and December 2021 using Qualtrics and purposive sampling. Data was collected from Chandigarh, Himachal Pradesh, Punjab, Haryana, and National Capital Region in India. Parents were given a choice of either the English-language or the Hindi-language version of the measure. Parents clicked on the language in which they were most comfortable answering the questions. All participants were provided with a Participant Information Sheet describing the study and the type of information that would be requested from them. Parents were informed that they were free to withdraw from the study at any given period of time. If participants had any questions about the study, they could email the researcher to receive answers to their queries. After providing informed consent, parents filled out the demographic questionnaire and SDQ.
Parents were also asked whether they would consent for their child’s class teacher to fill out the SDQ questionnaire on their child. If parents agreed, the English and Hindi versions of the SDQ were emailed to teachers. The teachers clicked on the language in which they were most comfortable answering. The total time to complete the form was 5–10 minutes.
Design and Data Analysis
Gomez and Stavropoulos (2019) reported that only 3 out of 13 studies that have validated the SDQ have CFI and TLI values of .90 and above, and all studies have RMSEA values of below .08 with 10 studies having a value of less than .06. Most studies have used RMSEA to determine model fit compared to CLI and TLI (Gomez & Stavropoulos, 2019). Therefore, in the current study, the model fit for the five-factor model was determined by RMSEA values.
In carrying out the CFA, the comparative fit index (CFI) and the Tucker–Lewis index (TLI) were employed to determine the model fit. A cut-off value greater than .90 on these two fit indices is considered acceptable, and a cut-off value greater than .95 indicates a good fit (Brown et al., 2006). The root mean square error of approximation (RMSEA) was also employed. The guidelines by Hu and Bentler (1998) indicate that values close to .06 or below are considered a good fit, close to .07 and less than .08 as a moderate fit, close to .08 to .10 as a marginal fit, and above .10 as a poor fit.
While RMSEA is considered an absolute fit index, as the fitted model is not directly compared with a baseline model, CFI and TLI are global model fit indices, each of which compares the fit of the target model with that of a baseline model in which no underlying factor structure is posited (Finch, 2020; Montoya & Edwards, 2021). RMSEA and CFI carry the assumption that the implicit model is correct in the target population. However, CFI carries an additional assumption that the baseline model is also correct. This is problematic because of the predominant use of null models as the base line. Therefore, to confirm which model fits well, the RMSEA is better suited that CFI.
The current study employed a cross-sectional research design. Data analysis was conducted using Analysis of Moment Structures (AMOS 18). The Confirmatory Factor Analysis (CFA) technique used was maximum likelihood estimation. Each SDQ item was specified to load on only one latent factor. The five latent factors, emotional symptoms (ES), conduct problem (CP), hyperactivity/inattention (HI), peer problem (PP), and prosocial behaviour (PB), were allowed to correlate with one another. All measurement errors were assumed to be uncorrelated (Figure 1; Goodman, 2001). The study followed the recommendation of Gomez and Stavropoulos (2019) and used the RMSEA value to determine whether the five-factor model was a good fit for the reports of parents and teachers of children with typical development in India.
Results
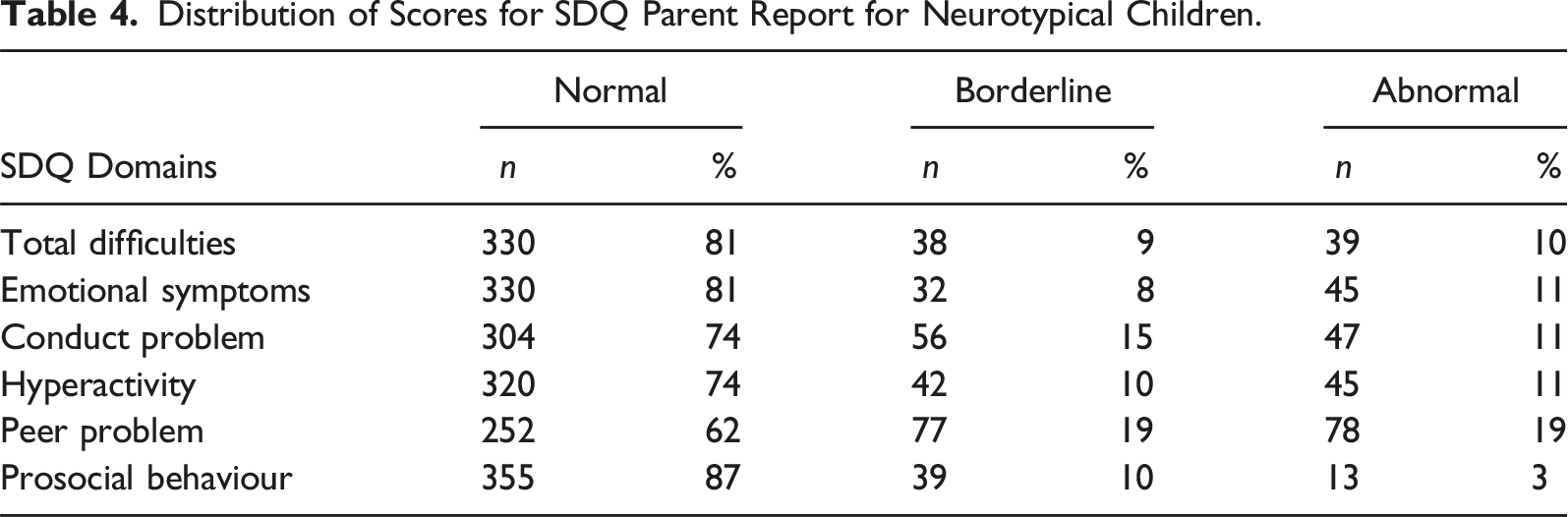
Distribution of Scores for SDQ Parent Report for Neurotypical Children.
Results from the CFA
There were no missing values for the SDQ ratings used in the current study. Results of the CFA performed on 25 items of the five-factor SDQ model using the responses from parents suggested a good fit on the RMSEA value (RMSEA = .060; χ2 = 650.501) but a poor fit using CFI and TLI indices (CFI = .699; TLI = .659). The RMSEA value for teachers of children with TD suggested a marginal fit (RMSEA = .090; χ2 = 988.80 ) and a poor fit using CFI and TLI values (CFI = .738; TLI = .704).
Results of the CFA for Parents on the SDQ.
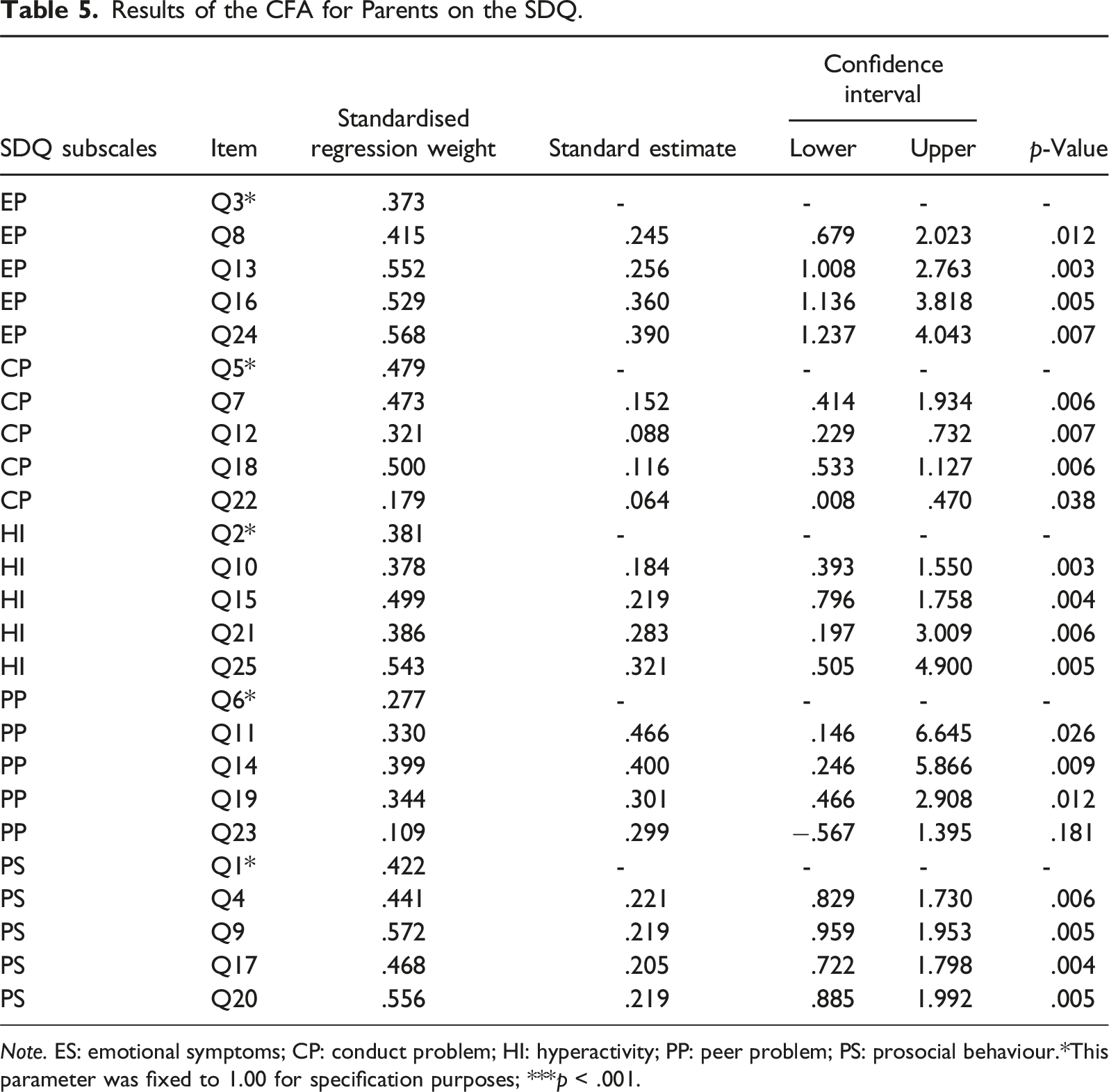
Note. ES: emotional symptoms; CP: conduct problem; HI: hyperactivity; PP: peer problem; PS: prosocial behaviour.*This parameter was fixed to 1.00 for specification purposes; ***p < .001.
Results of the CFA for Teachers on the SDQ.
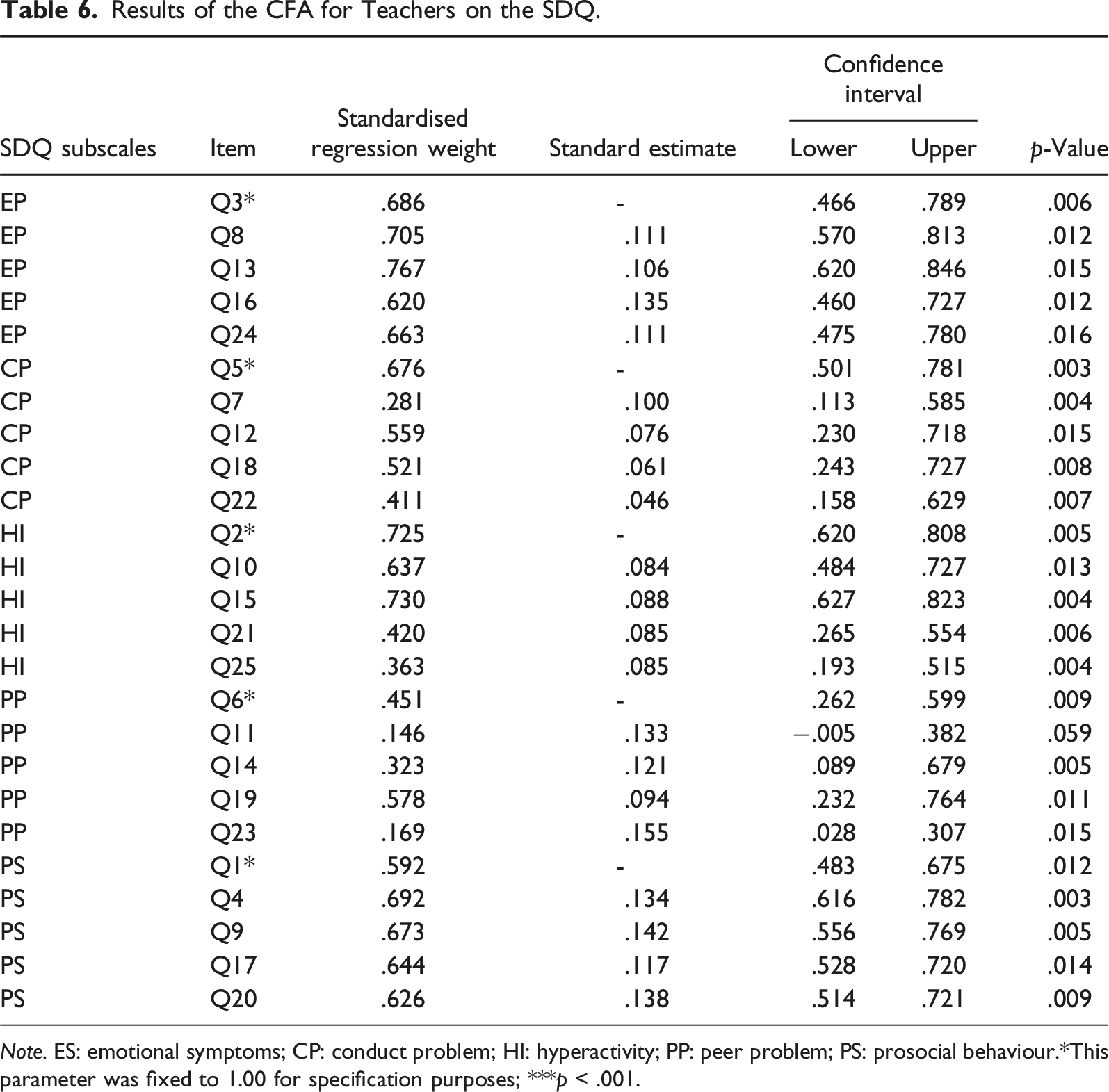
Note. ES: emotional symptoms; CP: conduct problem; HI: hyperactivity; PP: peer problem; PS: prosocial behaviour.*This parameter was fixed to 1.00 for specification purposes; ***p < .001.
Factorial Structure of the Teacher Completed SDQ for Typically Developing Children in India.
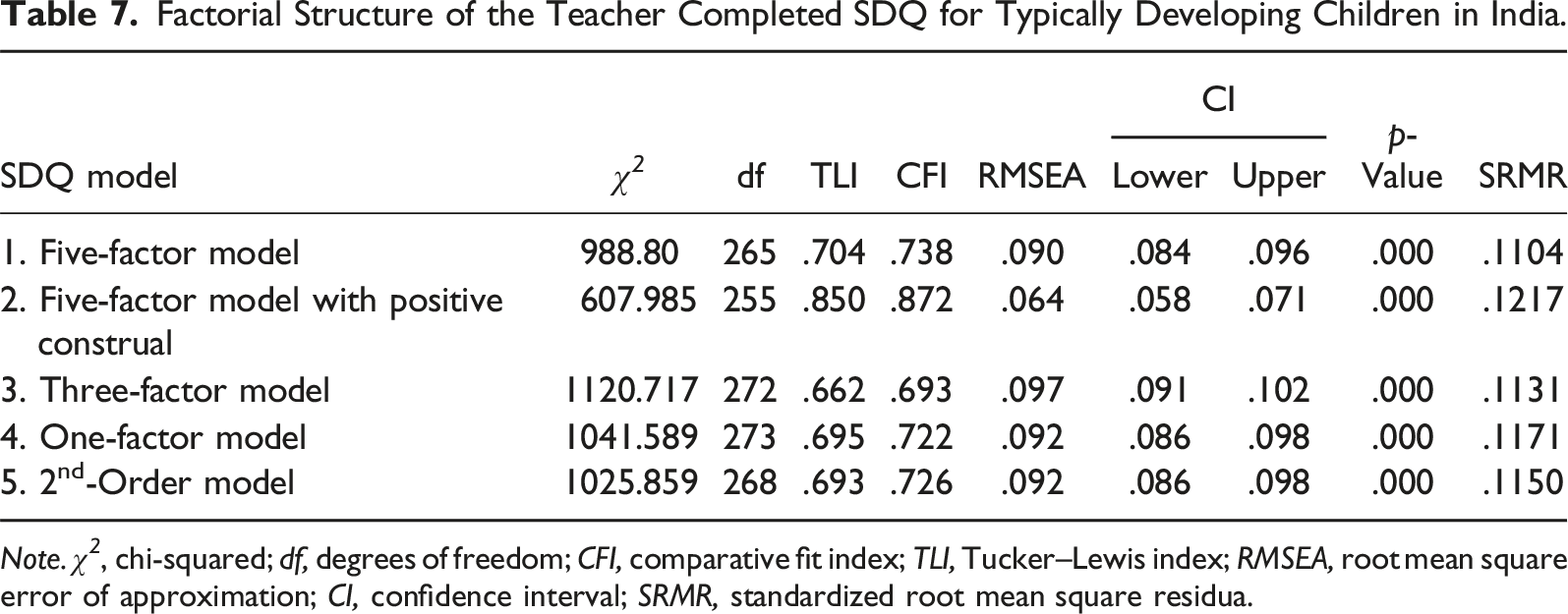
Note. χ 2 , chi-squared; df, degrees of freedom; CFI, comparative fit index; TLI, Tucker–Lewis index; RMSEA, root mean square error of approximation; CI, confidence interval; SRMR, standardized root mean square residua.
Factorial Structure of the Parent Completed SDQ for Typically Developing Children in India.
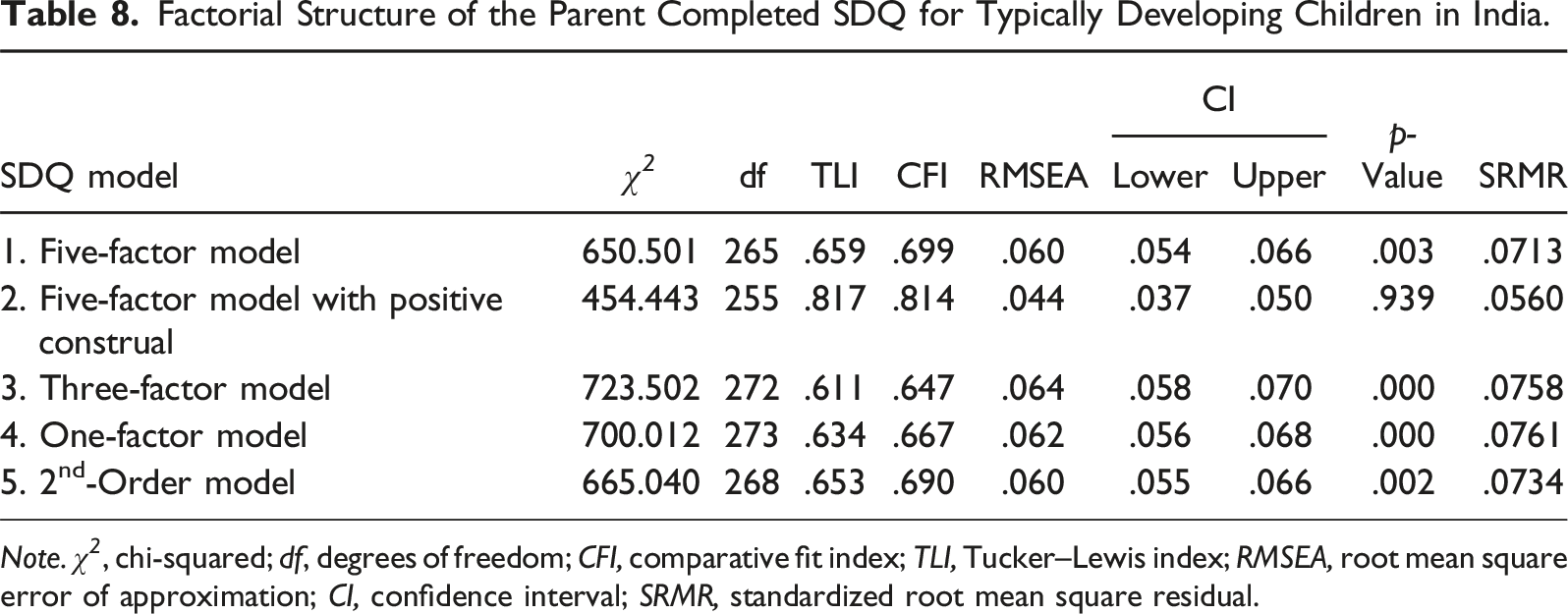
Note. χ 2 , chi-squared; df, degrees of freedom; CFI, comparative fit index; TLI, Tucker–Lewis index; RMSEA, root mean square error of approximation; CI, confidence interval; SRMR, standardized root mean square residual.
Discussion
The pattern of parents’ categorisation of children according to the SDQ’s three bands of ‘normal’, ‘borderline’, and ‘normal’ were similar to those reported for studies conducted in Germany (Becker et al., 2015), the United Kingdom (Glazebrook et al., 2003), and the Netherlands (Vugteveen et al., 2021), where most parents of children with typical development reported their children to be ‘normal’ on the five domains of the SDQ. Furthermore, existing literature also indicates that parents of children with typical development report relatively fewer concerns than parents of children with a developmental disability (Becker et al., 2004; Emerson, 2005; Strømme & Diseth, 2000).
An examination of whether the SDQ five-factor model was a good fit for the sample from India was conducted. Data from 407 parents and 102 teachers of children with neurotypical development aged 4–8 years were used in this study. The results showed that the five-factor model was a good fit for parent. However, it was a marginal fit for teachers, partially supporting the hypothesis. The current findings, of an average to good fit for parent-reported SDQ responses, were similar to those reported from studies conducted in countries like the Netherlands, Singapore, Sweden, and the United Kingdom, comprising children from clinical and community samples. Furthermore, results from multicultural assessments conducted in low- and medium-income countries like Mongolia also demonstrated that the five-factor model was a moderate to good fit (Table 1). In contrast, CFA studies carried out in Australia, Canada, the United States (parent), Pakistan, and Norway indicated that the five-factor model was a poor fit for parents and teachers. Consistent with the current findings, in the United States, the five-factor model was better suited for parents than teachers (Table 2).
The five-factor model for teachers reported a marginal fit. Multiple factors could be responsible for the plausible result. First, it may be due to the difference in understanding of the underlying factors, the difference in settings (home vs. school), and the normative expectations of the raters (Hill & Hughes, 2007). Second, parents often tend to rate a child more independently than teachers, who tend to rate children in comparison with one another (Hill & Hughes, 2007). Third, the current study was conducted during the COVID-19 pandemic. Online education was the only mode of teaching children. Teachers rated children on their online interaction and not in face-to-face physical interaction. Identifying children for any social-emotional learning concerns requires consideration of their body language, and nonverbal communication is essential. Furthermore, the regression weight for items 11, 22, and 23 was relatively low. However, keeping the items within their factors is essential because each item theoretically assesses the factor. For example, item 11, ‘has at least one good friend’, assesses peer problems among children.
Tables 7 and 8 report that the five factor with positive construal is better suited than the five factor alone (Goleman, 1998; Kaiser & Halvorsen, 2022; Lee, 2018; Palmieri & Smith, 2007; Vugteveen et al., 2021). The five-factor model with positive construal comprises five items from Prosocial Behaviour (PB) and five reverse-keyed problem-oriented items (Gomez & Stavropoulos, 2019).
Although the five-factor model with positive construal was a better fit than the five-factor model alone, the original model is still an adequate fit and by keeping this model it is possible to compare our results with those of other studies, thus providing an opportunity for a direct comparison with findings from previous research (Bull et al., 2016; Chiorri et al., 2016; Croft et al., 2015; Dahlberg et al., 2019; Goodman, 2001; Hall et al., 2019; Hawes & Dadds, 2004; Theunissen et al., 2013; Van Widenfelt et al., 2003).
Limitations and Recommendations
The current study was conducted during the COVID-19 pandemic. Online learning may make it difficult for parents and teachers to assess children properly. Caution is recommended in generalizing the results for a non-pandemic environment where physical attendance at school is the norm. Furthermore, the generalisability of the current results may be limited because the study comprised only children aged 4–8 years, and the sample was collected from a few states in North India; this is not a national representation of India, which comprises 28 states and multiple languages.
Future studies of the SDQ should prioritise a larger and more heterogenous sample. The tool is suitable for parents and teachers of children and adolescents in the broader age range and from diverse backgrounds, especially since pediatricians and physicians have limited time and resources to conduct such psychosocial assessments. The SDQ is low-cost, easily accessible, and uses reports from others. It can help practitioners and schools across India reliably determine whether a child needs further assessments and requires early intervention.
Contribution and Conclusion
This study is the first to examine whether the five-factor model was a good fit for interpreting the reports from parents and teachers of children aged 4–8 years in India. These results can be used to initiate using this tool for screening children across clinics and schools in India.
The findings from the present study provide further support for Goodman’s (2001) recommendation of the five-factor model for parents’ reports. The five-factor model was also found to be adequate for teachers’ reports, based on the RMSEA value. Therefore, the SDQ can be used with parents and teachers to screen children in the community. This replication of the factor structure validates the continuing use of the SDQ across schools and clinical practices and affirms the value of assessing parents’ and teachers' concerns regarding a child’s development (Shekhawat et al., 2022).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.