
Abstract
Healthcare generates large amounts of waste, harming both environmental and human health. Waste audits are the standard method for measuring and characterizing waste. This is a systematic review of healthcare waste audits, describing their methods and informing more standardized auditing and reporting. Using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we searched MEDLINE, Embase, Inspec, Scopus and Web of Science Core Collection databases for published studies involving direct measurement of waste in medical facilities. We screened 2398 studies, identifying 156 studies for inclusion from 37 countries. Most were conducted to improve local waste sorting policies or practices, with fewer to inform policy development, increase waste diversion or reduce costs. Measurement was quantified mostly by weighing waste, with many also counting items or using interviews or surveys to compile data. Studies spanned single procedures, departments and hospitals, and multiple hospitals or health systems. Waste categories varied, with most including municipal solid waste or biohazardous waste, and others including sharps, recycling and other wastes. There were significant differences in methods and results between high- and low-income countries. The number of healthcare waste audits published has been increasing, with variable quality and general methodologic inconsistency. A greater emphasis on consistent performance and reporting standards would improve the quality, comparability and usefulness of healthcare waste audits.
Keywords
Introduction
The healthcare sector of the United States represents nearly 18% of the domestic economy, and costs are only growing (Papanicolas et al., 2018). In addition to spending the most on healthcare relative to other countries, the U.S. healthcare sector generates the most pollution of any national health sector – 547 MtCO2e or 1.72 tCO2e/person per year – without attaining better health outcomes (Karliner et al., 2019; Minoglou et al., 2017; Papanicolas et al., 2018). Healthcare continues to contribute 9%–10% of U.S. greenhouse gas emissions and 9% of criteria air pollutants (Eckelman and Sherman, 2016) including ground-level ozone, particulate matter, carbon monoxide, lead, sulphur dioxide and nitrogen dioxide (US EPA, 2014), which leads to the loss of 388,000 disability-adjusted life years of human life annually (Eckelman et al., 2020). A large portion of these emissions are generated from the manufacturing and procurement of medical supplies and pharmaceuticals, most of which are disposable. With the holistic charge to ‘Do No Harm’, medical providers and the healthcare facilities where they work must quantify their generation of waste and take steps to mitigate threats to the environment and public health (Practice Greenhealth, 2021b; WHO, 2018).
Each year, at least 7 million premature deaths worldwide are tied to air pollution (WHO, 2014a), which is similar to the amount of deaths that have occurred due to COVID-19, but healthcare institutions continue to exacerbate this threat (Dong et al., 2020). We must address the significant environmental impact of the healthcare sector to tackle preventable health conditions (Landrigan et al., 2018; WHO, 2018). In addition to air pollution and carbon emissions, healthcare produces huge quantities of solid waste, estimated at 5 million tonnes/year (Practice Greenhealth, 2021b). These substantial amounts of infectious, sharps, pathological and hazardous waste (WHO, 2018) can be dangerous to waste management staff, surrounding communities (Babanyara et al., 2013), and in some contexts scavengers, or civilians who search through discarded waste in search of recyclable or profitable materials (Alam et al., 2008; Ali et al., 2016b; Asante et al., 2014; Azage and Kumie, 2010; Bassey et al., 2006; Hassan et al., 2008; Idowu et al., 2013; Mesdaghinia et al., 2009; Sawalem et al., 2009). Improperly treated medical waste could lead to various infections and diseases (WHO, 2014b). Physical hospital waste can also contaminate water supplies if quantities exceed the capabilities of regulated waste management or if water treatment processes are not in place. Landfill leachate into groundwater sources can be hazardous to human health, containing a variety of pollutants including heavy metals and toxins (Kumari et al., 2017).
Medical professionals already have a strong interest in reducing healthcare waste (Ryan et al., 2020; Thiel et al., 2017a); however, robust quantitative data, cost and environmental analysis are needed to effectively implement waste reduction strategies. Quantifying healthcare waste generation helps to allocate sufficient financial, logistical and legal resources to dispose of infectious or biohazardous waste safely. Only through understanding our waste generation and waste streams we can control and prevent downstream harms.
The most precise tool for measuring medical waste is likely a physical or manual waste audit, where individuals collect and measure medical waste using weigh scales (US EPA, 2016). Many entities – healthcare institutions, government agencies, universities and others – have conducted waste audits with highly variable objectives, timeframes, waste subsets and reporting schemes. In short, there is no widely accepted, standardized method to perform a healthcare waste audit. We sought to systematically review all published physical waste audits in healthcare settings to assess trends in methodology, data collection and reporting, with findings incorporated into a proposed guideline for an ideal physical waste audit in the healthcare setting.
Methods
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009), a systematic review was conducted using available published studies on waste audits conducted in healthcare settings. During July 2020 and again in September 2021, a trained medical librarian (Timothy Roberts) performed searches for studies in the MEDLINE, Embase, Inspec, Scopus and Web of Science Core Collection databases without language or date restrictions (Ovid MEDLINE available in Supplemental Appendix). References within studies from the data extraction stage were also screened for possible inclusion.
Included articles reported conducting a physical measurement of waste, manually or through an automated process, within a medical facility for the purposes of quantifying waste generation or identifying characteristics of the waste produced. Articles were included if any of the following waste types were measured: municipal solid waste/general landfill, regulated medical bio-hazard or infectious waste, recyclables, hazardous or radiological waste, pharmaceutical waste, linens, food waste and sharps. Medical facilities were defined as hospitals, clinical labs (including academic, commercial and governmental labs where medical waste is generated), medical clinics and dental practices. Studies were included from any country as long as the article was written in the English language.
Exclusion criteria are listed in Figure 1. The exclusion criterion of ‘Lax or Incorrect Methods’ includes the following:
Studies that only report aggregate results for more than one hospital (i.e. national or multi-system studies that do not report individual institutions’ data).
Studies that analyze the waste treatment pathways exclusively (rather than waste generation or sorting activities).
Studies that only use financial methods to ‘audit’ waste (without directly measuring waste).
Questionnaire-based studies (without physically measuring the waste).
Audits exclusively of food waste or clinical wastewater.
Studies focused on veterinary services and research laboratories (animal labs).
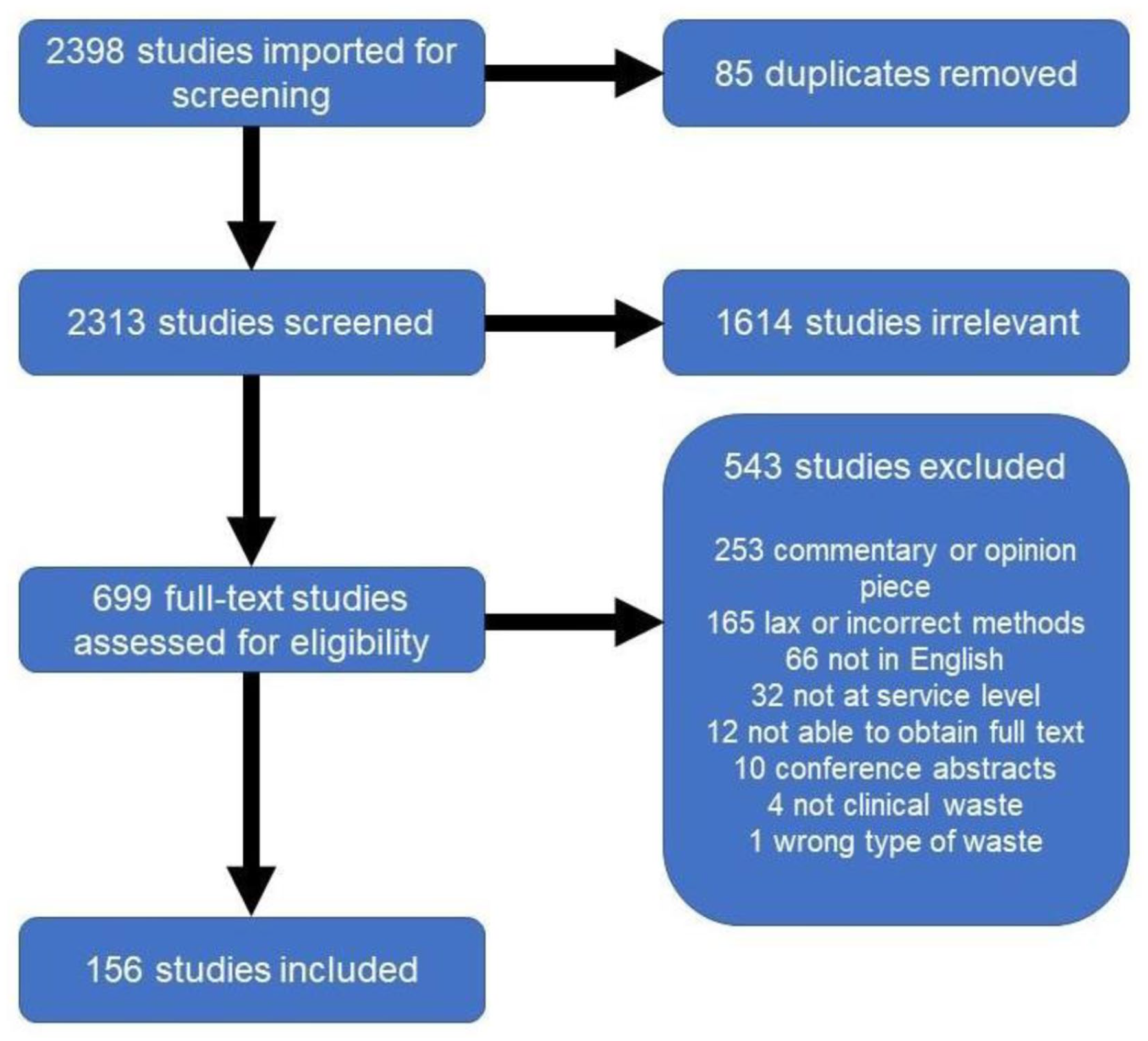
PRISMA diagram showing number of studies screened and included.
Following training on the protocol, all titles and abstracts were screened by Sarah Hsu, Michelle Lam, Jonathan E Slutzman, Ilyssa O Gordon and Cassandra L Thiel. The full texts of approved studies were then assessed by the same group of reviewers. Each study required two individual approvals to pass into the next stage of screening, and all conflicts were resolved through consensus. The final set of studies resulting from both stages of screening was then used for data extraction.
An online data extraction form was created to collect the following information from each study in a number of categories: publication meta-data, year, country, facility details, audit details (including dates, quantities and types of waste), audit methodology, reasons for the audit, data quality metrics and additional possible references. Two researchers independently extracted data from each paper, blinded to previous responses for that study. A custom-written Python script then consolidated identical responses. One individual examined each dissimilar data point, revisited each study and resolved conflicts to develop a consolidated data spreadsheet for analysis. Descriptive statistics are reported, with chi-squared tests for comparisons between groups.
Results
Study demographics
As shown in Figure 1, database searches and other sources identified 2398 studies and an additional 46 through other sources. After removing duplicates, 2313 studies were screened by title and abstract, yielding 699 articles for full-text review. From that set, ultimately 156 studies were eligible for inclusion in the qualitative synthesis (Supplemental Table S1) (Abd El-Salam, 2010; Abu Qdais et al., 2007; Alam et al., 2008; Al-Dhawailie, 2011; Alhumoud and Alhumoud, 2007; Ali, 2019; Ali and Geng, 2018; Ali et al., 2016a, 2016b; Al-Khatib et al., 2019; Almeida et al., 2016; Almuneef and Memish, 2003; Altin et al., 2003; Alves et al., 2014; Al-Zahrani et al., 2000; Andrade et al., 2014; Asante et al., 2014; Askarian et al., 2010; Awad et al., 2004; Azage and Kumie, 2010; Babu et al., 2019; Barbario et al., 2021; Bassey et al., 2006; Bazrafshan and Mostafapoor, 2011; Bdour et al., 2007; Caniato et al., 2016; Carr et al., 2019; Chiang et al., 2006; Chitnis et al., 2005; Chua et al., 2021; Conrardy et al., 2010; Debere et al., 2013; Debita et al., 2017; Dehghani et al., 2008, 2019; Denny et al., 2019; de Sa et al., 2016; De Sousa et al., 2014; Dewi et al., 2019; Dias et al., 2017; Diehl et al.,1992; Dietrich et al., 2004; Doiphode et al., 2016; Dumitrescu et al., 1998; Farmer et al., 1997; Farzadkiaet al., 2009; Fasola et al., 2008; Ferdowsi et al., 2012; Ferreira and Veiga, 2003; Ferreira et al., 2012; Figgins et al., 2019; Fraifeld et al., 2021; Francis et al., 1997; Furukawa et al., 2016a, 2016b; Gai et al., 2009; Garcia, 1999; Gargano et al., 2019; Ghafuri and Nabizadeh, 2017; Ghersin et al., 2020; Gilman, 2007; Gowrie et al., 2015; Graikos et al., 2010; Grimmond and Reiner, 2012; Guirguis, 2010; Hadipour et al., 2014; Hames, 2013; Hamoda et al., 2005; Hasan and Rahman, 2018; Hassan et al., 2008; Haylamicheal et al., 2011; Heitmiller et al., 2010; Hoenich and Pearce, 2002; Hoenich et al., 2005; Hsu et al., 2020; Hubbard et al., 2017; Idowu et al., 2013; James, 2010; Kalogiannidou et al., 2018; Khademinasab et al., 2017; Khan et al., 2019; Khor et al., 2020; Komilis et al., 2011, 2017; Kooner et al., 2020; Kron et al., 2021; Kubicki et al., 2015; Lawlor, 2014; Lee and Mears, 2012; Leissner and Ryan-Fogarty, 2019; Li and Jenq, 1993; Lima Barbosa and Gomes Mol, 2018; Lourenço et al., 2020; Majid and Umrani, 2006; Makofsky and Cone, 1993; Mandalidis et al., 2018; Manga et al., 2011; Manzi et al., 2014; Mattoso and Schalch, 2001; Mazloomi et al., 2019; McGain et al., 2009a, 2009b, 2015; Mekonnen et al., 2021; Meleko et al., 2018; Mendes et al., 2015; Mesdaghinia et al., 2009; Mohamed et al., 2009; Mohee, 2005; Moreira and Gunther, 2013, 2016; Mosquera et al., 2014; Mugambe et al., 2012; Namburar et al., 2018; Nandwani, 2010; Nemathaga et al., 2008; Niyongabo et al., 2019; Park and LaMattina, 2020; Pathak et al., 2021; Patil and Pokhrel, 2005; Paudel and Pradhan, 2010; Pereira et al., 2013; Phengxay et al., 2005; Piccoli et al., 2015; Rahmani et al., 2020; Reed et al., 2013; Richardson et al., 2016; Sanida et al., 2010; Santos et al., 2019; Sawalem et al., 2009; Senel et al., 2015; Shinee et al., 2008; Shum et al., 2020; Soroceanu et al., 2011; Stall et al., 2013; Stringer et al., 2011; Studnicki, 1992a, 1992b; Tadesse and Kumie, 2014; Tauber et al., 2019; Thiel et al., 2015, 2017b; Tieszen and Gruenberg, 1992; Tisdall et al., 2019; Tsakona et al., 2007; Tudor, 2007; Tudor et al., 2005, 2008; Vaccari et al., 2017; Vieira et al., 2009; Voudrias et al., 2012; Walker et al., 1994; Wiafe et al., 2015; Yurtseven et al., 2010; Zafar and Butler, 2000; Zhang et al., 2009).
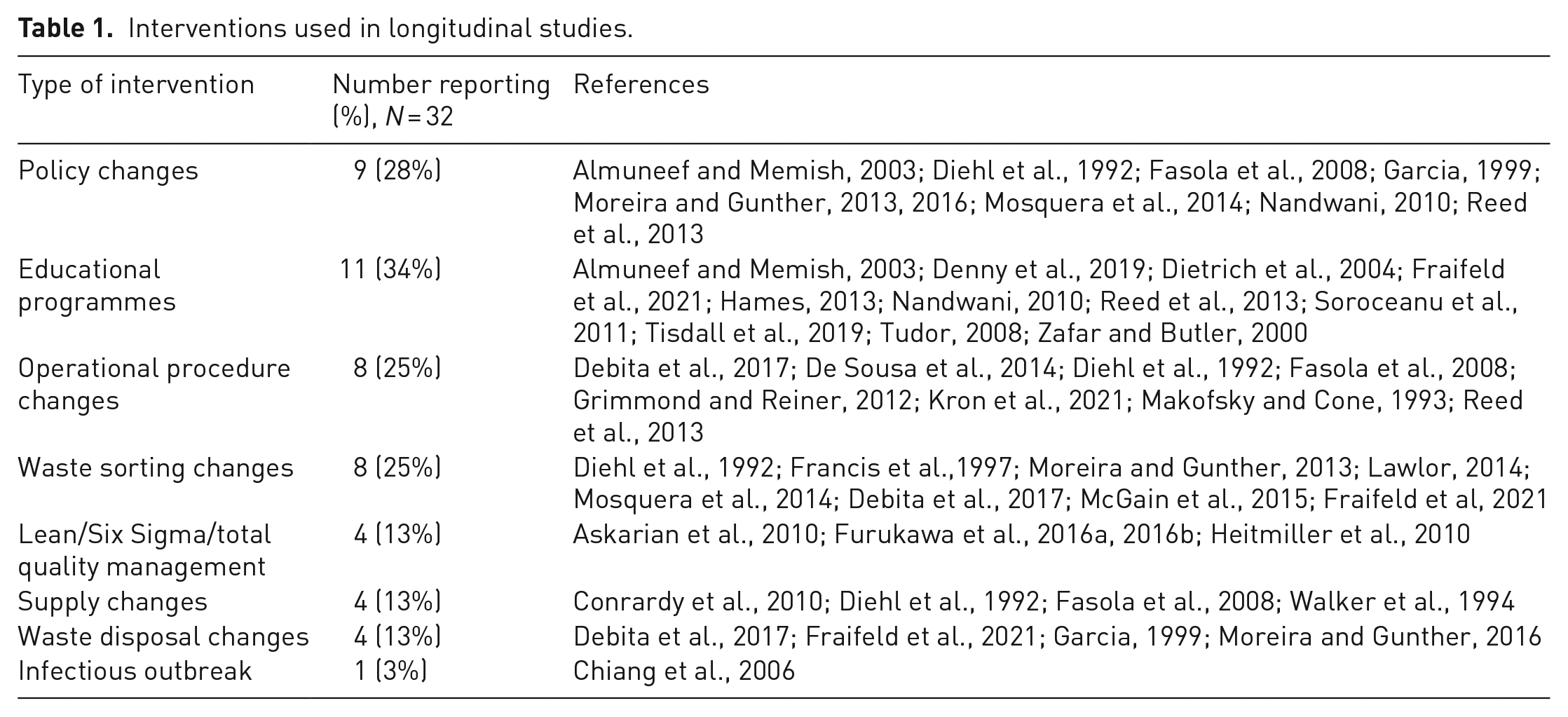
Interventions used in longitudinal studies.
All included studies were published in the year 1992 or later despite no date restrictions on the literature search, with an arithmetic average of 5.6 publications per year. The publication rate increased from 1.8 studies per year in the 1990s to 4.2 per year in the 2000s, 8.9 per year in the 2010s and 8.8 per year in the 2020s (only including the full year 2020 and the year 2021 through September as that was when the query was run again).
A plurality of studies was reported on waste audits that were conducted in the United States (27 of 156, 17%), followed by Brazil (17, 11%), United Kingdom (13, 8%), Iran (12, 8%), Australia (10, 6%) and Greece (8, 5%). The remaining 78 studies originated from 32 other countries, with no single nation being responsible for more than six studies. Studies were predominantly performed in high-income countries (78, 50%), followed by 40 (26%) in lower-middle-income countries, 31 (20%) in upper-middle-income countries and 8 (5%) in low-income countries (Figure 2) as defined by the World Bank (2022).
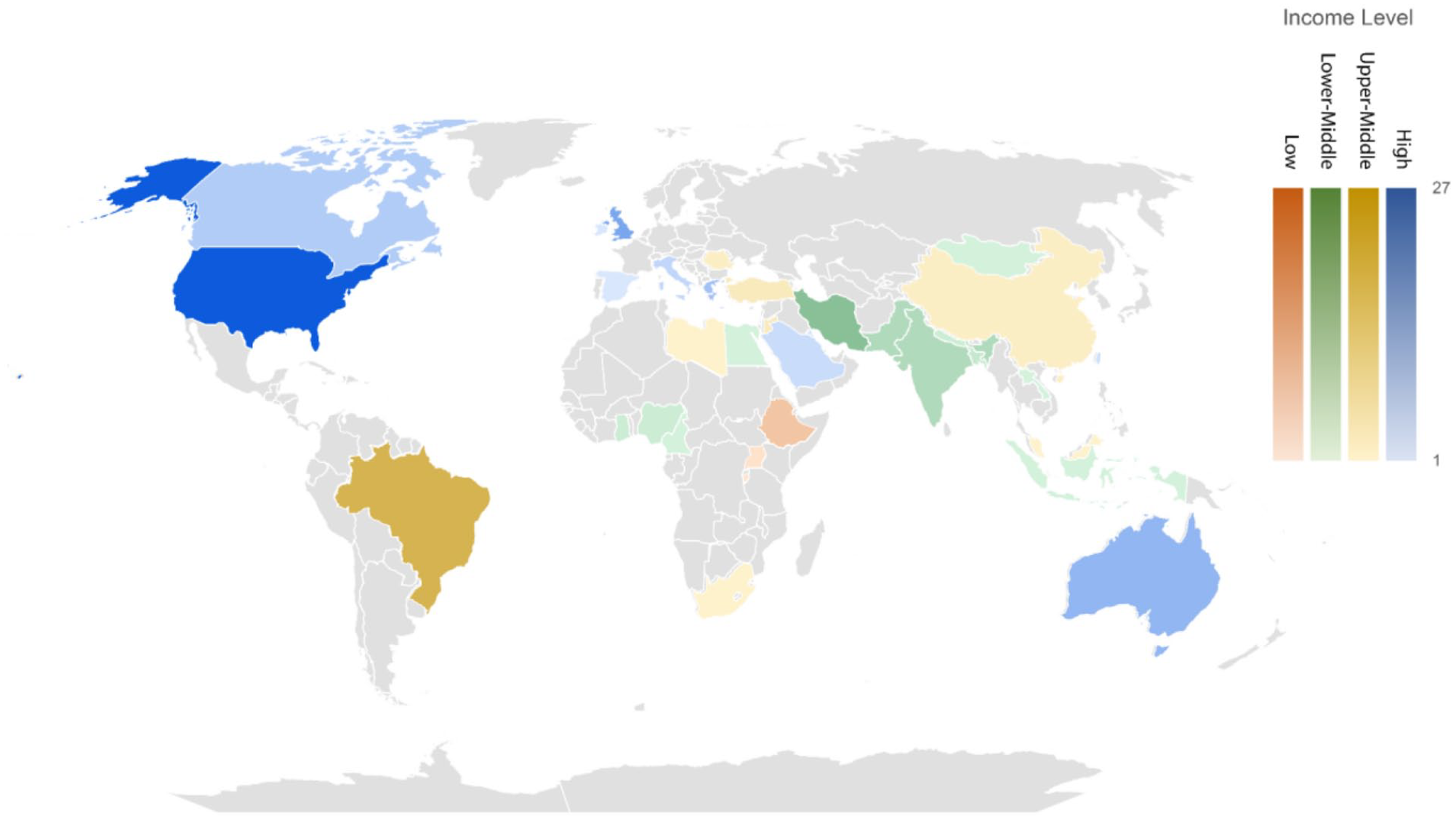
Number of papers published by country where the medical waste audit was conducted. Number of papers ranged from 1 to 27.
Reason for audit
Waste audits were conducted for a variety of reasons, and more than one was cited in all but 21 publications (of which one did not specify a reason for their audit). The most common objective was to improve local (hospital or health system) waste sorting policies or practices (116 studies, 74%). The next most common objectives were to reduce waste generation (70 studies, 45%) and to inform regulatory policy development (65 studies, 42%). Increasing or implementing waste diversion (recycling, composting, etc.) was a motivation in 53 studies (34%), whereas a financial motivation to save money on waste costs was the fifth most common objective (48 studies, 31%). Over 30 additional reasons for conducting waste audits were identified in a total of 37 studies, such as quantifying greenhouse gas emissions, generating inputs for life cycle assessments, creating a waste prediction model and simply quantifying the total amounts of wastes.
Looking at the reason for performing the waste audit as related to the country of study, 85% of the studies with financial objectives (41 out of 48) were done in high-income countries, whereas only 9% (7 of 78) of studies in non-high-income countries cited financial reasons (p < 0.01). In contrast, audits performed in non-high-income countries were much more likely to cite improving local waste sorting policies or practices as the primary reason, with 91% of studies in those countries specifying these reasons compared to 58% in high-income countries (p < 0.01). Similarly, informing regulatory policy development was a primary objective in 50% of studies done in low-income countries and 70% of studies done in lower-middle-income countries, compared to 52% in upper-middle countries and only 22% in high-income countries (p < 0.01 for high-income vs non-high-income countries, high- vs lower-middle-income countries and high- vs upper-middle-income countries).
Audit methodology
A number of methods were used to quantify wastes under study. Of the 156 studies, 134 (86%) directly weighed waste, 3 (2%) counted items to obtain a weight, 26 (17%) counted items without obtaining weights and 25 (16%) used interviews, questionnaires or surveys to document waste amounts. A total of 37 studies (24%) used more than one method in their research.
Methods used by investigators also appeared to differ by location. Waste audits completed in non-high-income countries were more likely to use interviews, questionnaires or surveys to gather data: 21 of 78 studies (27%) in non-high-income countries compared to 4 of 78 studies (5%) in high-income countries (p < 0.01). In contrast, waste audits in high-income countries were more likely to use counting to quantify waste, being listed as a method in 27 of 78 studies (35%), compared with 2 of 78 studies (3%) in non-high-income countries (p < 0.01). Studies completed in non-high-income countries also almost all used weighing as a collection method (74 of 78 studies, 95%), compared to being used by 60 of 78 studies (77%) in high-income countries (p < 0.01).
Of the 156 studies, 72 (46%) audited waste at multiple hospitals or at the health system level, 41 (26%) investigated a single hospital, 27 (17%) studied a single department and 20 (13%) audited a single care pathway or procedure (Figure 3). There was one waste audit of an ambulance service and one of a clinical research institution.
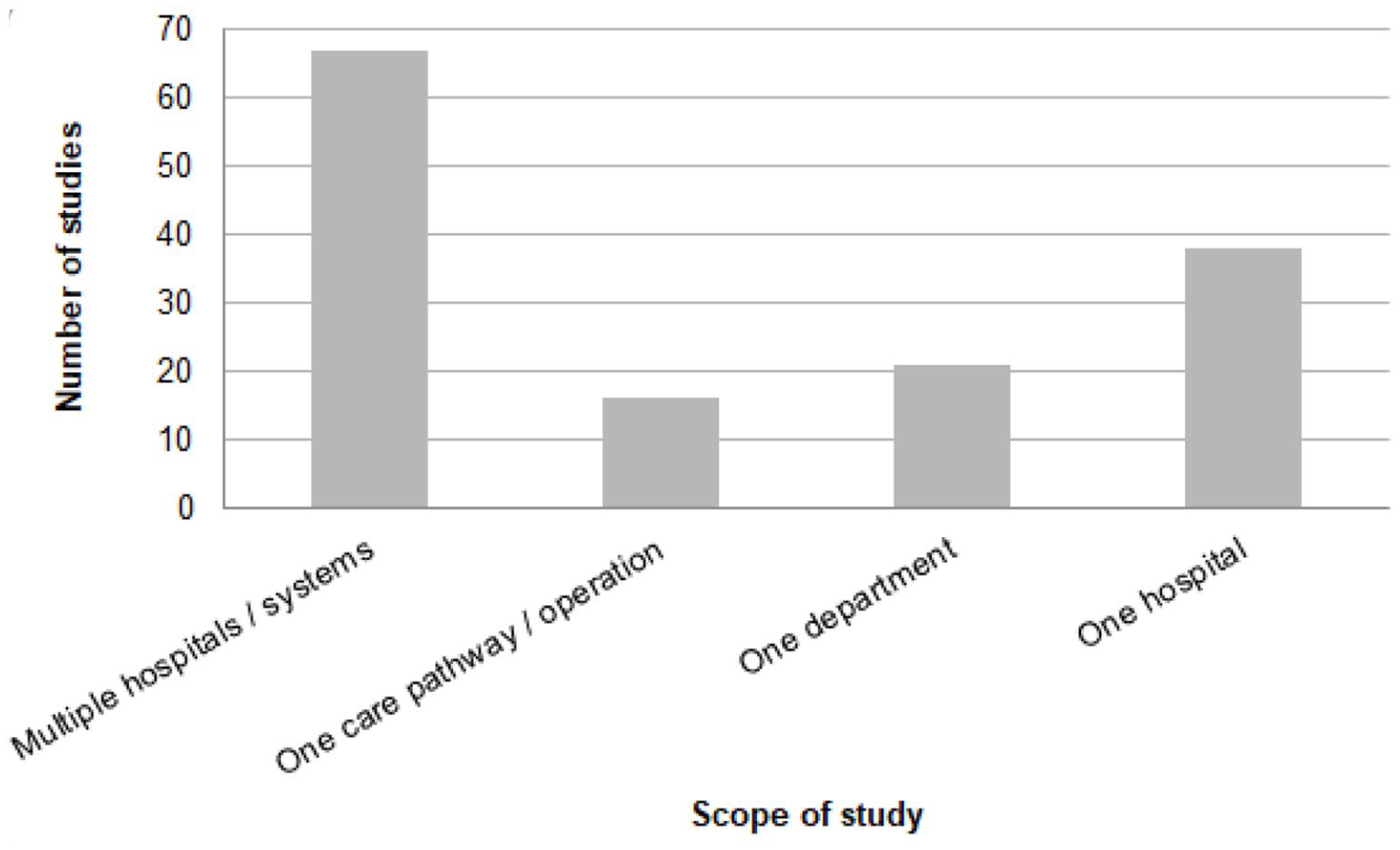
Number of medical waste audits by scope or audit boundaries.
Large-scale audits of health systems or multiple hospitals were completed disproportionately more in non-high-income countries compared to high-income countries. Of the 78 studies done in non-high-income countries, 51 (65%) were at the health system or multiple hospital level, compared to 21 of 78 studies (27%) completed in high-income countries (p < 0.01).
Most studies (134, 86%) reported the duration of the audit in time, with a range of 1 day to multiple years. Five studies (3%) did not specify the duration of the audit. The remainder (17, 11%) reported lengths of studies in terms of numbers of procedures or numbers of items reviewed. These data are presented in Figure 4.
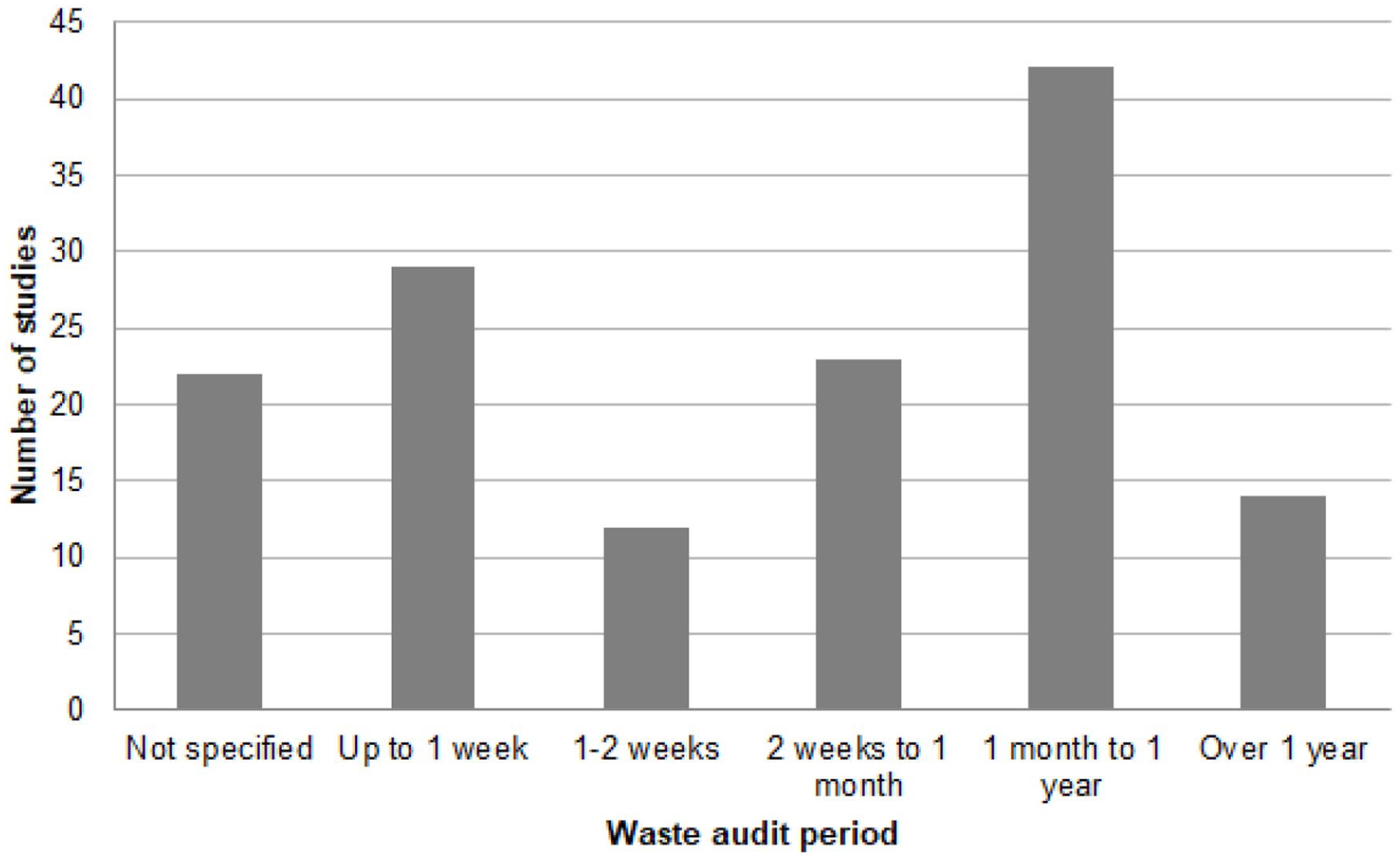
Length of waste audit period.
Longitudinal or interventional studies
Thirty-two articles (21%) described longitudinal studies, reporting two sequential medical waste audits before and after a specified intervention, such as an educational module (Table 1). Of these, 23 articles (72%) were aimed at increasing local waste sorting, 21 articles (66%) for reducing waste generation, 20 articles (63%) for financial reasons, 11 articles (34%) for increasing waste diversion and 1 article (3%) for regulatory policy development. Intervention-based audits were predominantly performed in high-income countries (25, 78%) compared to upper-middle-income (5, 16%) and lower-middle-income (2, 6%) countries (p < 0.01). Regarding measurement methods used in these particular studies to quantify wastes, 22 studies (69%) weighed with a scale, 11 studies (34%) counted without weight, 1 study (3%) counted to obtain a weight and 2 studies (6%) used questionnaires, interviews or surveys.
Waste categories
Formal definitions of the waste categories used in the audit were provided in 111 (71%) studies. Most of those studies (75, 48%) specified regulatory or other bodies as the sources of waste definitions. National governmental statutes or regulations were cited by 46 studies (29%), international agencies (e.g. World Health Organization or United Nations) by 33 studies (21%), state or provincial statutes or regulations by 4 studies (3%), industry groups by 3 studies (2%), non-governmental organizations by 2 studies (1%) and other sources of definitions by 4 studies (3%).
These audits most frequently assessed biohazardous and infectious waste (137, 88%), as well as general landfill waste, also called municipal solid waste (107, 69%). Additional categories of waste assessed included sharps (85, 54%), pharmaceutical (37, 24%), recycling (26, 17%), hazardous or radiologic (21, 13%), linen (19, 12%), food (16, 10%) and chemical (16, 10%), as well as 19 other categories listed in 36 studies. Studies done in high-income countries compared to non-high-income countries were significantly different with respect to waste categories included (p = 0.02). Categories with significant differences based on income level were: general landfill, which was included in 61 of 78 studies in non-high-income countries (78%) and only 46 of 78 studies in high-income countries (59%) (p < 0.01); biohazardous and infectious waste, included in 75 (96%) non-high-income country studies compared to 62 (63%) high-income country studies (p < 0.01); sharps, included in 49 (63%) non-high-income country studies and 36 (46%) high-income country studies (p = 0.04); recycling, included in 8 (10%) non-high-income country studies and 18 (23%) high-income country studies (p = 0.03); chemical waste, included in 14 (18%) non-high-income country studies and 2 (3%) high-income country studies; and pathologic waste, included in 8 (10%) of non-high-income country studies and 0 (0%) high-income country studies (p < 0.01).
Quality metrics
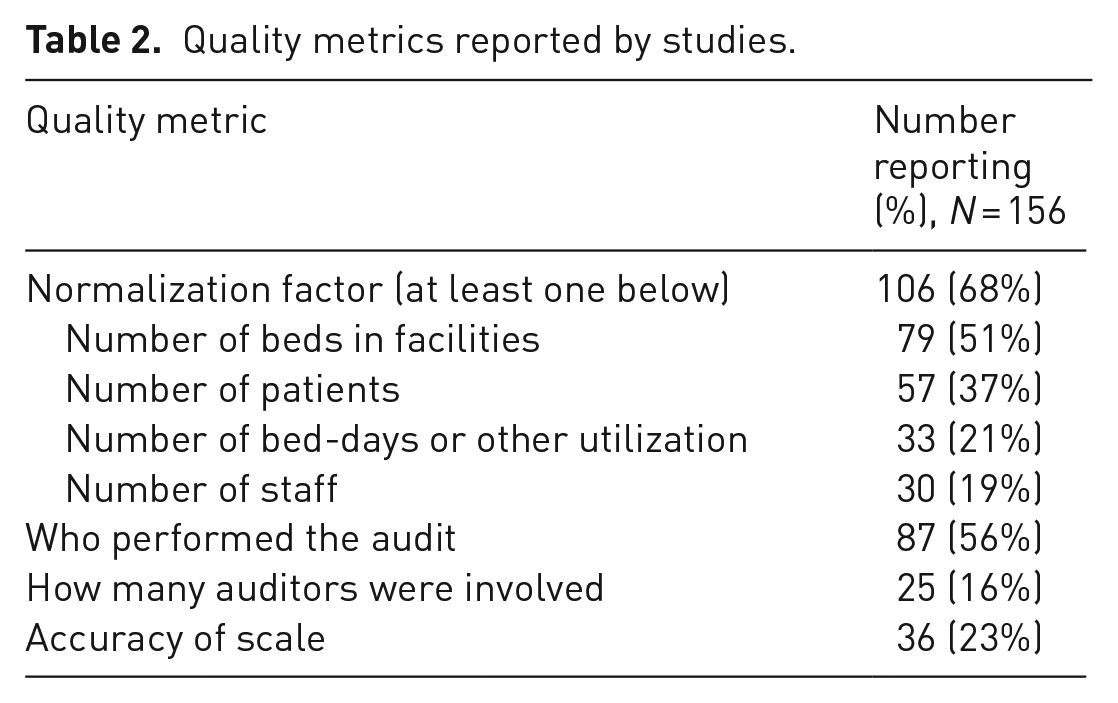
We considered a number of factors that may indicate the detail with which study authors may have conducted their waste audits and that contribute to the ability to compare results from one facility to another. Study quality metrics, including specifying details of the facility size and occupancy, description of the auditors and accuracy of the weigh scale are listed in Table 2.
Quality metrics reported by studies.
Discussion
The number of medical waste audit publications has been increasing over time, suggesting broader recognition of the value of waste generation data, greater attention to environmental issues in healthcare or both. As more healthcare organizations set plausible waste reduction goals, waste audits will continue to hold value as a tool to inform waste reduction strategies in the healthcare setting. Overall, we found that studies of solid waste audits in the healthcare setting spanned a wide range of locations, purposes, durations and techniques.
Waste audits have been published in both higher- and lower-income countries, demonstrating that healthcare waste is a problem faced by all health systems worldwide. Lower-income countries were more likely to cite regulatory policy development as the reason for their waste audits, suggesting that lower-income countries are still working to create effective healthcare waste management infrastructure.
Lower-income countries were more likely to use indirect methods to obtain data (i.e. interviews, questionnaires or surveys) compared to those in higher-income countries. Although all included audits from lower-income countries also used direct-weight measurement for at least a portion of their study, their reliance on indirect methods may be due to constrained resources, with direct measurement taking more effort, personnel and time. On the other hand, higher-income countries were more likely to conduct audits in which waste items were counted, rather than weighed. This may be because higher-income countries generate much more total waste, making direct measurement more challenging and possibly less feasible for investigators. In addition, more studies in higher-income countries focused on particular care pathways (e.g. single-surgical procedures), lending themselves more to counting waste items, whereas waste audits in lower-income countries were more commonly broader in scope, measuring waste generation across whole health systems.
The majority of studies (110, 77%) evaluated waste with the purpose of improving local (hospital or health system) waste sorting policy or practices. Improved sorting practices can reduce biohazardous waste, increase recycling and potentially reduce overall waste, all of which can save labour time, optimize waste treatment expenses and reduce environmental impacts from waste over-treatment (Sherman and Hopf, 2018). If general or landfill waste is improperly sorted as biohazardous material, it often undergoes unnecessary decontamination and treatment, with associated higher financial and environmental costs. Additionally, improving sorting protects communities, staff and patients from dangerous hazardous materials and sharps (Babanyara et al., 2013).
The underlying data sources used in waste audits varied widely across studies, with some measuring volume and others measuring weight. In some cases, the ultimate sources informing these additional data were waste management records or invoices. Obtaining either weight or volume data may be easiest by reviewing waste management invoices; however, using invoice data is an imperfect method of auditing waste. Firstly, treatment vendors may charge by the load, by volume or by container volumes. These data would not necessarily answer how much waste, by mass, a facility is generating. Furthermore, once wastes are commingled for hauling, it is not possible to further characterize the waste to help determine what is driving waste generation. For example, it would remain unknown if waste generation rates are driven more by plastics versus textiles, and future practices could not be informed by knowing whether wastes are appropriately separated or contaminated (e.g. recyclable metal cans in municipal solid waste or reasonably clean plastics in regulated medical waste).
As stated earlier, waste categorization varies greatly among locations and is not standardized. Most studies included general landfill and biohazardous/infectious waste, which is an important distinction in waste streams for determining hazard level and safe disposal methods. Not all studies included sharps, recycling, hazardous or radiologic, pharmaceutical, food, chemical or linen wastes, which is likely due to the variety of departments and sites being audited. Surprisingly, only 17% of studies included recycling as a waste category, indicating a missed opportunity because of the relative feasibility of large-scale hospital recycling. According to the Healthcare Plastics Recycling Council, it is estimated that one-fourth of hospital waste in the United States is composed of plastic packaging and products, and 85% of that waste is non-hazardous and therefore easily recyclable (Sparrow, 2020). With ongoing issues facing recycling markets, the unpredictable variability of single-stream recycling collected from domestic settings complicates recycling, whereas hospitals contribute large quantities of uniform disposable materials that hold higher market value (HPRC, 2020).
Safe management of medical waste can be extremely expensive, but in the United States, up to 85% of waste from hospitals does not need to be treated as infectious according to regulatory definitions (WHO, 2018). Physical waste audits in which components are measured can unveil issues in waste segregation, reducing the financial burden that infectious waste pathways would otherwise cost.
Of the studies, 32 (21%) measured waste, performed an intervention, and then measured waste again to see if the intervention was successful. The variety of interventions employed in these longitudinal studies not only reflects the diversity of reasons for performing the audit but also supports the need for more uniform waste audit methodology and structure. When resources permit, performing a baseline and a post-intervention audit can be useful to compare the effectiveness of various waste management practices.
Examining the complete lifespan of waste can inform more comprehensive policy development, as demonstrated by studies that monitored waste from creation to disposal (Sawalem et al., 2009). Indicating whether waste is sent to an incinerator, landfill or dump outside of the hospital may emphasize the importance of proper waste management. Such distinctions also can contribute to modelling broader environmental impacts of waste disposal, such as downstream pollutant generation from waste treatment activities.
Waste audit quality
We identified several data categories that speak to the quality of a medical waste audit. These can be considered sentinel details that, when provided, show that the auditors considered even small data points important and fully understood the value of sharing specific points about their facilities that enable normalization and comparison with other studies. The least commonly reported quality metrics were the number of auditors involved in the study and the number of staff at the facility. More than two-thirds of the studies reported at least one facility occupancy metric, with the most common being the number of hospital beds. At least in a clinical research setting, facility staff size has been shown to correlate with waste more strongly than the number of patients (Sanida et al., 2010). Furthermore, as with other data categories we studied, there was no uniform reporting unit for facility utilization, occupancy or staffing. These metrics are of substantial value for interpreting the scale and scope of an audited facility and are certainly necessary when considering pooling data for meta-analysis. They are typically already collected for other facility purposes and should be readily available.
Waste audit reporting guidelines
Overall, there was no established or uniform protocol for performing or reporting a waste audit in the healthcare context. Similar to other scientific fields, a minimal objective is to enable comparison of results across settings and time. This requires establishing and reporting clear definitions of waste categories, units of potential allocation (like occupancy) and methods of data collection to gauge the quality of the study.
Practice Greenhealth, the healthcare institution membership arm of Health Care Without Harm, emphasizes the importance of waste audits (HCWH, 2013) but does not specify protocols for completing them. The Healthier Hospitals Initiative (Practice Greenhealth, 2021a), which is now a programme of Practice Greenhealth, has rudimentary waste auditing tools, but they (1) advocate using waste vendor invoicing as a means of measuring waste and (2) break waste into only four categories: municipal solid waste, regulated medical waste, hazardous waste and recycling. As noted above, there are additional waste categories that could be important to any particular health care facility, such as pharmaceutical, linens, food and chemical. The studies in this review did not describe specific international standards for the audits performed, and Internet searches for existing waste audit standards in healthcare did not identify any such specifications. Without consistent and accepted detailed standards, comparisons across waste audits remain a challenge.
Other industries with waste audit standards include commercial kitchens and cafeterias, drug manufacturing and general manufacturing. Many industrial and commercial business operations, including retail shopping, office buildings, restaurants, hotels/motels, educational institutions (STARS, 2021; Terry et al., 2017) and large manufacturing establishments are covered by general standards set forth by UNIDO (UNEP and UNIDO, 1991), the US Environmental Protection Agency (US EPA, 1998), local Ministries of the Environment (Ontario Ministry of the Environment, 2008) and the US Department of Agriculture (Terry et al., 2017). The standards with the most specific step-by-step instructions – including materials, timelines and definitions of waste – are those provided by Seven Generations Ahead (2019) and US EPA in application to cafeteria waste in primary and secondary schools (Terry et al., 2017), and Green Tourism in Canada (Green Step Tourism, 2021) (Table 3). These standards generally require creating a team, using proper personal protective equipment (PPE), defining categories of waste, and the process of physically separating the waste into different categories, but do not provide guidelines for what is considered a sufficient audit time period or statistically appropriate quantity or proportion of waste to be audited. These standards are not precise enough to compare between audits and apply findings in their most useful sense. With specific reference to healthcare, the WHO waste management standard (Chartier et al., 2014) recommends using audits to ensure compliance, but it does not provide guidelines or instructions for how to perform an audit.
Existing waste auditing guidelines and steps from other sectors.
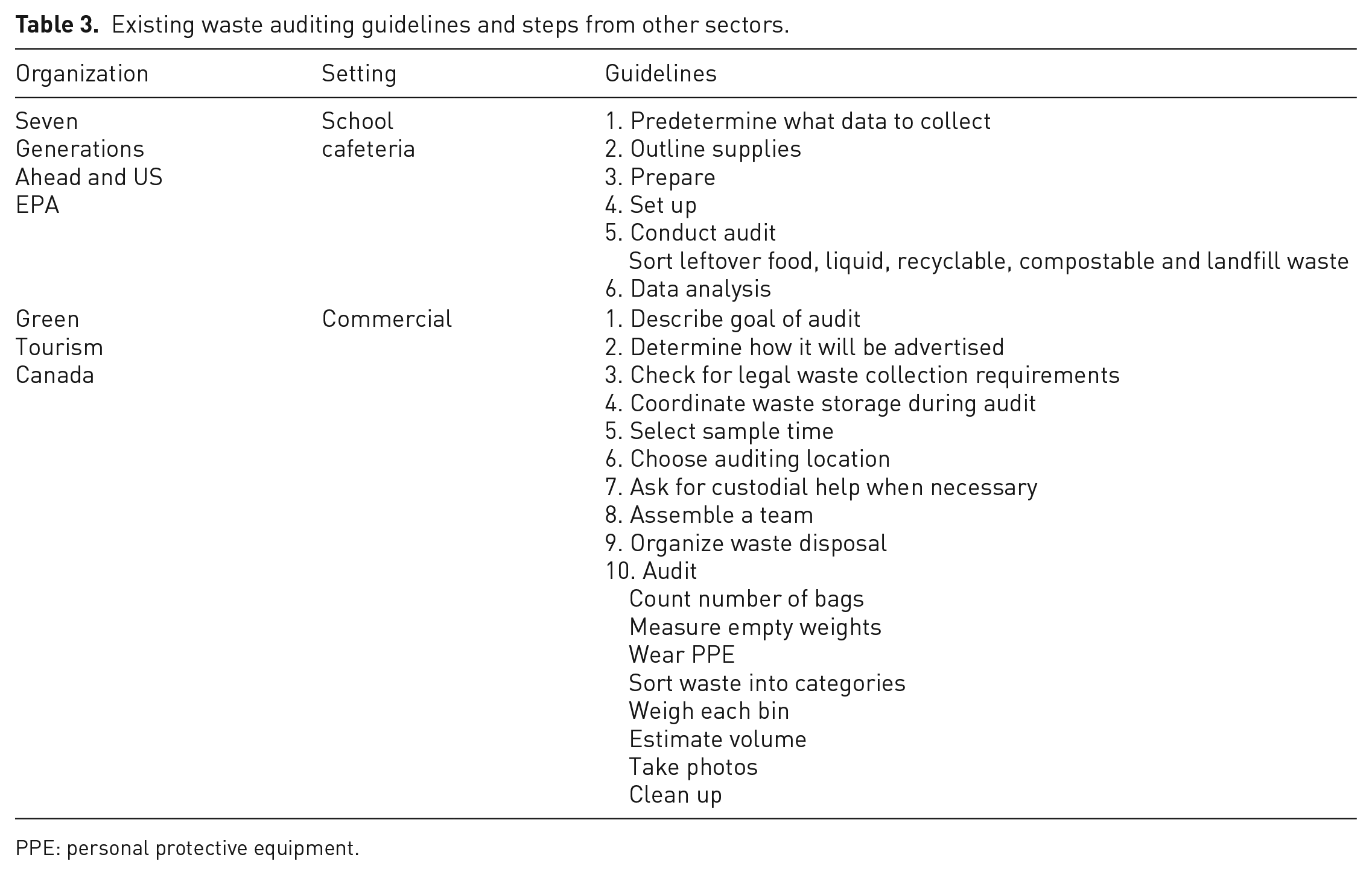
PPE: personal protective equipment.
We propose that waste auditing in healthcare be performed under a set of quality standards, both in performance and in reporting. Performance standards should address the representativeness of the sampling strategy, the fraction of the population that needs to be sampled to be considered sufficiently rigorous (e.g. minimum number of days or individual procedures out of a total of interest), the definitions of waste classifications and how to assign individual wastes to accurate categories. They should also stress the benefit of direct weight measurements, but be flexible enough to accommodate circumstances where counting or counting and calculating weight would be appropriate. These procedural standards should account for different objectives, including differences between large and small facilities and more or less detailed needs. Finally, standards must address the safety of auditing staff given the possibility of exposure to dangerous materials in healthcare waste.
Reporting standards should stress clearly defining study methodology. Reproducibility is essential for any scientific endeavour, and a reader should understand clearly how a particular waste audit was completed. Reports should answer what was done, who did it, how often and for how long. Readers should be able to understand from an audit report or manuscript the scope and scale of a particular study, including some metric of healthcare service utilization or occupancy during the audit period, ensuring that best practices for appropriate waste reduction can be gleaned and applied appropriately.
Based on our review of the literature, we have developed guidelines for performing waste audits in healthcare (Table 4). We additionally utilized the framework for Environmental Life Cycle Assessment under ISO 14040 and ISO 14044 (ISO 2006), which set the standard for comprehensive environmental reviews of products or processes. Waste is often one component of these environmental assessments, and therefore the ISO framework lends itself nicely to a widely accepted protocol for waste auditing in the healthcare setting. Published reports resulting from audits completed using these guidelines should still clearly describe the details of their methodology. Of note, these recommended steps may at times be done out of the order presented when local conditions or objectives warrant.
Suggested healthcare waste auditing guidelines.
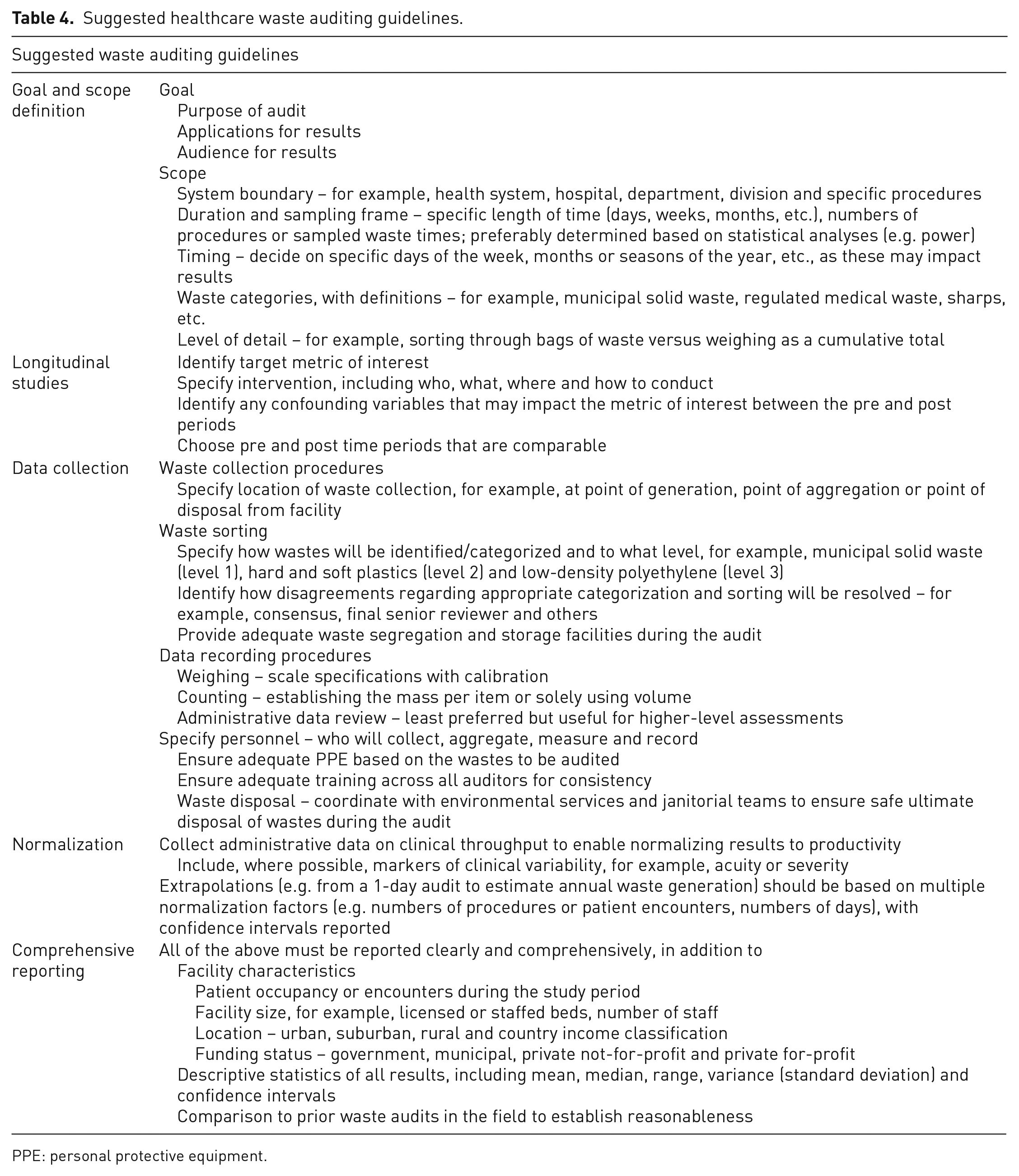
PPE: personal protective equipment.
Study limitations
This review has a number of limitations, which we do not expect to impact the results materially. Our systematic review is limited to studies published in English, resulting in the removal of 66 studies from the screening pool of 2398. Globally, researchers and institutional staff may have internally conducted any number of unpublished waste audits, to which we would not have had access. Additionally, data published solely on independent websites would not have been captured. We also excluded studies that were based solely on questionnaires (i.e. researchers did not physically audit waste). However, some methodologies were not entirely clear or mixed questionnaires with physical measurement of wastes. We acknowledge that there is a literature of audits based on waste questionnaires that we did not include, but which could provide additional insight. By restricting our review to studies that included a physical waste audit, we remained focused on assessing the methodology in order to identify the necessary parameters for our guidelines. Finally, during data collection, we used a uniform data extraction form for manual extraction, which may not have captured the reported study data in its entirety.
To inform the sustainable development of global public health, future studies should examine the rates of waste production relative to the cost of a given procedure and compare across national development levels. Future analyses should examine the association between clinical outcomes and waste production to determine whether higher use of single-use disposable instruments actually increase procedural success, or could encourage the use of reusable instruments to optimize environmentally sustainable healthcare practices (Thiel et al., 2017a).
Conclusions
Waste auditing is a common tool in healthcare to understand the waste generation and disposal practices of a health system or hospital. We have described the breadth of published reports, finding 156 applicable studies, all of which were published in 1992 and later. An increasing number of healthcare waste audits have been published over the last 30 years, with variable quality. These studies have predominantly been conducted to improve local waste practices, inform regulatory and policy development, and to identify ways to save money. Waste auditing can continue to fill these roles, as well as others, such as reducing the generation of waste by informing better purchasing practices and increasing waste diversion from landfills through reuse, reprocessing, recycling and composting, and we therefore recommend a greater emphasis on consistent performance and reporting standards to ensure high-quality results and to improve the ability to compare healthcare waste across different settings.
Supplemental Material
sj-docx-1-wmr-10.1177_0734242X221101531 – Supplemental material for Waste audits in healthcare: A systematic review and description of best practices
Supplemental material, sj-docx-1-wmr-10.1177_0734242X221101531 for Waste audits in healthcare: A systematic review and description of best practices by Jonathan E Slutzman, Hannah Bockius, Ilyssa O Gordon, Hannah C Greene, Sarah Hsu, Yiming Huang, Michelle H Lam, Timothy Roberts and Cassandra L Thiel in Waste Management & Research
Footnotes
Acknowledgements
The authors thank Health Care Without Harm for bringing them together and encouraging this work to be completed. The authors thank Riya Patel and Pranav Jayaraman for their assistance in responding to reviewers’ comments. The authors thank Amy Weiss of Amy Weiss Design for assistance in the creation of ![]() .
.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.