
Abstract
Background
Home-like models in long-term care (LTC) aim to improve residents’ well-being, autonomy, and daily life experience. However, its implementation is inconsistent with variation in adoption and sustainability across settings.
Objective
To systematically identify and explain the multilevel barriers and facilitators that shape implementation of home-like models in LTC.
Methods
A scoping review of 36 peer-reviewed studies and 13 Canadian grey literature documents was conducted. Implementation factors were extracted and mapped to the updated Consolidated Framework for Implementation Research (CFIR 2022).
Results
Fifty-two implementation factors emerged (23 barriers, 29 facilitators). Inner Setting, including staffing instability, organizational culture, leadership, and resource availability, was the most influential but constrained by Outer Setting determinants (regulatory rigidity and funding). Among facilitators, adaptive leadership and staff engagement were most consistently identified, followed by supportive organizational culture and flexible regulatory approaches. Homes employing incremental or pilot-based strategies manage implementation complexity and sustain culture change over time.
• This review demonstrates that home-like models rarely fail due to staff or organizational resistance. Rather, system-level constraints in regulation, funding structures, and workforce instability are the primary barriers to culture change. • It reveals how Inner Setting factors, particularly leadership approaches, workforce instability, organizational culture, and resource availability, interact with Outer Setting policies and nested layers of governance to shape real-world implementation capacity and sustainability. • The review establishes that home-like care represents a cultural transformation within implementing organizations rather than a purely physical design change, requiring alignment across conditions of work, governance structures, and organizational climate.
• Gerontological practitioners can use these findings to prioritize staff engagement, supportive supervision, and consistent assignment models that strengthen person-centred and relational care delivery in LTC settings. • Policy makers can reform rigid regulatory and funding structures through principle-based regulations and sustainable staffing that support home-like care. • Researchers can use the CFIR-aligned synthesis to design implementation studies, develop context-sensitive interventions, and evaluate culture change efforts more systematically.What This Paper Adds
Applications of Study Findings
Introduction
Long-term care (LTC) systems in Canada have long faced persistent workforce shortages, complex regulatory environments, and outdated institutional infrastructure (Goring & Loshak, 2021; Longstaff et al., 2022; Rochon et al., 2022). These persistent issues are being amplified by demographic pressures associated with the aging of the baby boomer generation, projected to double the population of adults aged 75 and older by 2040 (Hallman et al., 2022). This shift will place unprecedented demand on LTC services. Increased demand coincides with the rising prevalence of age-related conditions such as dementia and frailty, which require more complex, resource-intensive care (Baines & Armstrong, 2019; Hsu et al., 2020; Rochon et al., 2022).
The combination of structural problems and growing demands has exposed Canada’s LTC sector to intense scrutiny, most notably during the COVID-19 pandemic. During this crisis, structural failures in overcrowded facilities contributed to a devastating loss of life (Clarke, 2021), with mortality rates in Canada reaching nearly twice the Organization for Economic Co-operation and Development (OECD) average (Akhtar-Danesh et al., 2022; Clarke, 2021; Iyamu et al., 2023; Lucia, 2020; Oldenburger et al., 2022). Several inquiries called for an urgent system transformation toward more dignified, Person-centred care (PCC) models (Koren, 2010; Maccourt, 2021; Oldenburger et al., 2022; Wright, 2020).
Ontario’s existing LTC infrastructure, dominated by hospital-like environments, remains misaligned with the preferences of residents, families, and frontline staff for more home-like environments and PCC that support autonomy, dignity, and a sense of belonging (de Boer et al., 2018; Fishman et al., 2016; Kok et al., 2018). PCC is defined as an approach to care that prioritizes the individual’s preferences, needs, and values, positioning the person at the centre of care to fulfill their desires (McCormack et al., 2011).
Home-like models are defined by their small-scale, residential-style design, typically housing 10-12 residents in private or semi-private rooms organized around a central kitchen and living area (Ausserhofer et al., 2016; Kok et al., 2018; Verbeek et al., 2014; Zwakhalen et al., 2018). These models prioritize autonomy, relational care, and resident choice in daily routines, aiming to recreate the physical, social, and emotional qualities of a real home. In contrast, traditional LTC models are institutional in nature, characterized by larger facilities, shared bedrooms, long corridors, centralized nursing stations, and rigid task-oriented schedules that prioritize efficiency and regulatory compliance over personalization. Examples of home-like models include the Green House Project, the Eden Alternative, and household models, all of which are grounded in PCC principles and represent alternatives for addressing residents’ needs and preferences (Fleming et al., 2017; Goring & Loshak, 2021; Kok et al., 2018). These models have demonstrated benefits including improved resident quality of life, staff satisfaction, and overall care outcomes (Ausserhofer et al., 2016; Kok et al., 2018; Verbeek et al., 2014; Zwakhalen et al., 2018)
The pandemic further highlighted these benefits by demonstrating how smaller, home-like settings achieved significantly better outcomes than traditional large facilities. An analysis of COVID-19 outcomes between January and July 2020 showed that Green House and other small LTC homes reported markedly better outcomes than traditional homes with 50 or more beds (Zimmerman et al., 2021). In this study, median COVID-19 case rates per 1000 resident-days were 0 in small homes compared with 0.06 in large facilities, and median mortality rates among infected residents were 0% versus 12.5%, respectively. Differences were most pronounced in the highest quartile, where large homes had case rates more than 9 times higher than those of small homes. The authors noted that these advantages may stem from ‘fewer people living, working, visiting, and being admitted to Green House/small nursing homes, and private rooms and bathrooms’ (p.489). These findings are consistent with a meta-analysis of data from 41 articles across 11 countries, including Canada and the United States, which found that care homes operating as smaller and detached buildings experienced significantly lower COVID-19 infection rates among residents (Samir & Naylor, 2025). However, despite this evidence, the adoption of home-like models in LTC remains limited and inconsistent across jurisdictions (Ausserhofer et al., 2016; Kok et al., 2018; Zimmerman et al., 2016).
Understanding this disconnect requires a systematic examination of the barriers and facilitators influencing the implementation of home-like models. It is also important to examine these factors without assuming that all barriers should be eliminated, recognizing that some regulatory requirements, while creating implementation challenges, serve essential protective functions for vulnerable residents. Accordingly, this scoping review examines factors affecting the implementation of home-like models without prejudging whether all barriers should be removed or whether home-like models are universally appropriate across LTC contexts.
Theoretical Framework
We used the Consolidated Framework for Implementation Research (CFIR) to guide the analysis and provide a structured taxonomy for identifying implementation factors. CFIR is an implementation framework that synthesizes constructs from multiple theories into a unified taxonomy to identify factors that influence implementation across settings (Damschroder et al., 2009, 2022). The 2022 update was specifically developed in response to user feedback to better capture the ‘why’ and ‘how’ of implementation by providing more granular subdomains, particularly within the Individuals and Inner Setting domains.
The CFIR framework organizes factors into five domains, each containing multiple constructs that represent more granular conceptual categories within that domain. For example, the Individuals domain contains constructs such as Motivation, Capability, and Need, while the Inner Setting domain contains constructs such as Culture, Leadership, and Available Resources. Importantly, not all constructs within a domain will be relevant to every study; researchers apply constructs selectively based on what emerges empirically from the data. In this review, inductively generated categories were mapped onto CFIR domains and their nested constructs during the analysis phase, with the full mapping provided in Appendix A.
Applied to this review, each domain is operationalized as follows. The Outer Setting refers to the broader environment surrounding LTC organizations and encompasses multiple interacting levels. At the broadest level, this includes federal policy frameworks and national funding structures. At an intermediate level, it includes provincial legislative and regulatory environments governing LTC. At a more proximate level, it may include regional health authorities, municipal governance structures, and, where applicable, the corporate or divisional structures of multi-site operators or nursing home chains whose system-level policies and resource decisions shape implementation capacity at the individual home level yet remain external to any single facility. The Inner Setting refers to the organizational context in which implementation occurs, with the primary Inner Setting in this review being the individual LTC home itself, such as a nursing home, a seniors’ residence, or a residential care facility, encompassing its leadership, culture, workforce conditions, and physical infrastructure. Where a home is part of a larger governing structure, such as a for-profit chain, a non-profit operator, or a municipally operated organization, that entity constitutes a nested layer within the Inner Setting, since operator-level decisions regarding funding allocation, staffing models, and organizational priorities directly shape conditions at the individual home level. The Individuals domain captures the roles and characteristics of those involved in or affected by implementation, including organizational leaders at all levels, frontline and direct care staff, and residents and families as recipients of care. The Innovation domain refers to the specific intervention being implemented, in this review, the home-like model of LTC itself, including its key design features, adaptability, perceived complexity, and evidence base. The Process domain describes the activities and strategies used to drive implementation, including planning, engaging, tailoring, and reflecting.
The updated 2022 CFIR emphasizes the importance of understanding how factors at different levels, such as individual behavior, organizational priorities, and system-level regulations, interact and shape one another. This perspective is particularly relevant for home-like models, where coordinated changes across all levels are essential for success. Appendix A provides a complete mapping of the CFIR domains and their nested constructs, including descriptions from the 2022 update, along with the specific barriers and facilitators identified in this review.
Objective and Research Questions
This scoping review addresses the persistent gap between evidence and practice in LTC by examining how home-like models are implemented in real-world settings. It synthesizes peer-reviewed and Canadian grey literature to identify the contextual factors that enable or hinder adoption and sustainability. The review is guided by the following research questions: (1) What barriers and facilitators influence the implementation of home-like models in LTC homes? (2) How do these barriers and facilitators align with the five domains of CFIR? (3) What contextual or systemic conditions contribute to the persistence of implementation barriers?
Methods
Study Design
A scoping review methodology was chosen to systematically map the existing evidence on how home-like models are implemented, to identify research gaps, and to synthesize findings from both peer-reviewed and grey literature sources. This design was appropriate because the research questions sought to capture the breadth and diversity of implementation factors rather than assess intervention effectiveness, aligning with the exploratory nature of scoping reviews. The inclusion of both peer-reviewed and grey literature sources was intended to capture the broad range of implementation evidence, encompassing both empirical research as well as practical insights from policy and organizational reports that directly shape implementation in the Canadian LTC system. However, grey literature can vary in quality and may lack the methodological detail of peer-reviewed studies.
This scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews (PRISMA-ScR) guidelines (Tricco et al., 2018) and Arksey and O'Malley’s five-stage methodological framework: (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, and (5) collating, summarizing, and reporting results (Arksey & O’Malley, 2005).
Search Strategy
The search strategy was developed in collaboration with a health sciences librarian and focused on three core concepts: (1) long-term care, (2) home-like or culture change models, and (3) implementation. Culture change was included because home-like models represent shifts in the environment, care philosophy, staff roles, and organizational culture. Searches were conducted in PubMed, CINAHL, PsycINFO, Embase, Scopus, Web of Science, and EuropePMC in July 2024 and updated in February 2025. Search terms and Boolean operators were adopted for each database (Appendix B).
Grey literature was retrieved via Google searches using combinations of terms including long-term care, home-like models, small home models, household models, PCC, and implementation paired with policy, report, government, and Canada. The first 10 pages of results were reviewed, as prior studies indicate that relevant grey literature typically appears in the early search results, with few additional relevant sources beyond this threshold. We also conducted targeted searches of organizational websites relevant to LTC. Relevant organizations were identified through references in peer-reviewed studies, Canadian government health department websites, and professional associations in LTC literature.
Canadian grey literature (2017-2025) was included if it reflected regulatory, political, or system-level contexts in LTC. This timeframe captured documents produced under consistent policy environments. Eligible sources included government and policy reports, strategy documents, evaluations, and position statements from established organizations. Editorials, blogs, news articles, and non-Canadian sources were excluded.
Documents from peer-reviewed and grey literature sources were included when they addressed system-level factors such as funding, regulation, staffing, or physical design relevant to home-like implementation, even without explicit reference to specific models such as Green House or Eden Alternative.
Study Selection
Citations were imported into Covidence for management. After removing duplicates, four trained members of the research team independently screened titles and abstracts using inclusion and exclusion criteria. Discrepancies were resolved through discussion, with unresolved cases referred to the supervising author for adjudication. To ensure consistency, a pilot screen of 10% of citations was conducted. Inclusion criteria were refined based on discrepancies identified in the pilot. Inter-rater reliability was assessed using Cohen’s kappa (k = 0.85), indicating strong agreement among reviewers.
Data Charting
Data from both peer-reviewed studies and Canadian grey literature sources were extracted and charted using a standardized data extraction form. For peer-reviewed studies, Table 2 summarizes study characteristics (author, year, country, design), model type, and all reported barriers and facilitators. For grey literature, Table 3 captures organizational, system-level, and policy-level implementation factors derived from government reports, policy briefs, position statements, and evaluations. Pilot testing of the extraction form on a subset of sources refined the extraction categories and ensured consistent capture of implementation factors across formats. Two trained members of the research team independently extracted and verified data from both peer-reviewed and grey literature sources, with discrepancies resolved through discussion and consensus. Consistent with scoping review methodology and PRISMA-ScR guidelines, no formal quality appraisal was undertaken, as the objective was to map the breadth and nature of implementation evidence rather than to assess methodological rigour.
Data Analysis
Summative content analysis (Hsieh & Shannon, 2005) was used to categorize barriers and facilitators from peer-reviewed studies and grey literature. First, extracted terms were categorized inductively from the source texts to capture the raw data. Second, these categories were deductively mapped to the specific domains, subdomains, and constructs of the updated CFIR framework (Damschroder et al., 2022). Two trained members of the research team independently assessed the alignment between the extracted categories and the CFIR constructs, resolving any discrepancies through discussion to enhance analytic rigour.
Study Selection
Of 4702 records identified through database searches, 634 were removed as duplicates, leaving 4068 citations for title and abstract screening. After this stage, 4019 records were excluded because they did not meet the inclusion criteria (i.e. wrong setting, intervention, or outcomes). This resulted in 75 full-text articles and documents assessed for eligibility, of which 36 peer-reviewed studies and 13 grey literature documents met the inclusion criteria. The PRISMA-ScR flow diagram summarizing identification, screening, and inclusion is presented in Figure 1. PRISMA flow diagram of study identification and selection
Results
Study Characteristics
Data Chart of Articles Included in the Scoping Review (n = 36)

Canadian Grey Literature (n = 13)

Analysis of Findings
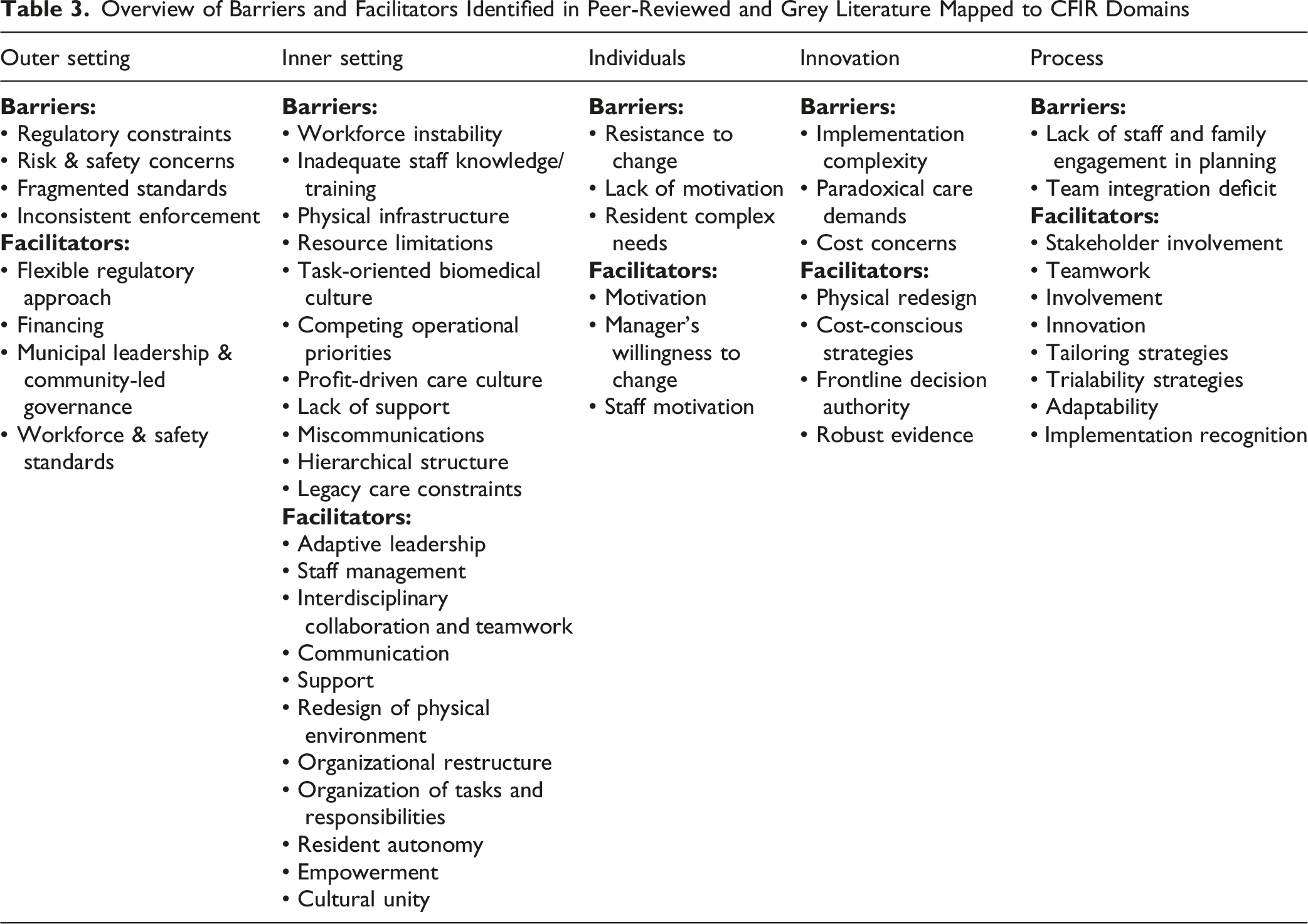
Overview of Barriers and Facilitators Identified in Peer-Reviewed and Grey Literature Mapped to CFIR Domains
Outer Setting
Barriers
Regulatory rigidity emerged as one of the most influential barriers across both peer-reviewed and grey literature sources. Licensing requirements, inspection practices, and prescriptive safety rules consistently reinforced institutional routines and limited flexibility in daily living practices. Staff described feeling obligated to prioritize regulatory compliance even when requirements conflicted with person-centred values, including restrictions on décor, communal cooking, meal service, or resident movement. These constraints reduced staff autonomy, increased administrative burden, and signalled that institutional order mattered more than resident choice. Health and safety policies further intensified the tension between autonomy and risk, placing frontline staff in difficult ethical positions when resident preferences did not fully align with prescriptive rules. In addition, fragmented and siloed oversight systems created inconsistent expectations across ministries and agencies, making it challenging for homes to implement culture change in a stable and coordinated way. Inconsistent enforcement of existing regulations further contributes to organizational uncertainty and a default toward risk-averse institutional care.
Facilitators
When system-level environments supported culture change, they enabled organizational efforts to take root. Policy flexibility and principle-based regulatory approaches allowed leaders and inspectors to interpret safety rules, thereby upholding resident autonomy while maintaining compliance. In Principle-based regulatory systems, governments specify desired outcomes rather than prescribe the specific structural or procedural means of achieving them, leaving organizations discretion in how they meet regulatory intent. Ontario’s Fixing Long-Term Care Act (2021) illustrates this approach through its Fundamental Principle (s. 1), which requires the entire Act to be interpreted with reference to resident dignity, comfort, and met needs, without mandating how homes must operationalize these outcomes (Fixing Long-Term Care Act, 2021). At the sector level, the Ontario Long Term Care Association (2019) has similarly called for funding flexibility that allows homes to allocate government resources toward different categories of support staff based on resident needs, rather than following prescribed staffing arrangements, reflecting the same principle-based logic applied to workforce funding (Ontario Long Term Care Association, 2019). Stable financing and workforce investments provided the conditions for homes to experiment with home-like redesign, relational care routines, and decentralized decision-making. Several grey literature sources emphasized that non-profit operators may be well-positioned to support home-like care, prioritizing public accountability and resident well-being over financial performance. Further, it was noted that municipally operated homes governed by community-led, locally accountable structures share these advantages and offer comparable potential to sustain home-like care (Armstrong et al., 2023). These system-level facilitators not only empowered organizations to adopt home-like models but also strengthened the conditions across Inner Setting, Individuals, Innovation, and Process domains. When regulations, funding, and governance structures aligned with home-like principles, organizations were better able to sustain leadership continuity, invest in training, support staff autonomy, and implement the day-to-day relational practices that define home-like care. Finally, the adoption of clear workforce and safety standards, such as improved infection control protocols, provides a structured environment that supports the sustainability of home-like environments.
Inner Setting
Barriers
Workforce instability emerged as the most pervasive challenge to implementing home-like care models, encompassing staff turnover, inconsistent staffing assignments, chronic absenteeism, and frequent leadership transitions. These destabilizing patterns systematically undermined continuity of care relationships, disrupted relationship-building processes essential to PCC, and fragmented the sustained organizational attention required to shift daily routines toward home-like care. Homes faced substantial gaps in staff knowledge and training regarding resident-directed care, perpetuating reliance on task-oriented, biomedical routines that prioritized operational efficiency and clinical procedures over relational interactions.
Physical infrastructure presented another major obstacle, because legacy ward-style layouts made it difficult to implement household-style living arrangements. Resource constraints manifested as inadequate time allocations, insufficient staffing levels, limited access to training, scarce funding, and outdated technology. These limitations, combined with competing operational priorities, miscommunication across organizational levels, and rigid hierarchical control structures that concentrated decision-making away from frontline staff, thereby reinforcing institutional care patterns. Additionally, profit-driven organizational models created financial pressures that constrained empowerment initiatives, limited collaboration, and undermined continuity through cost-reduction strategies.
Facilitators
Homes that successfully implemented home-like models demonstrated distinctive organizational characteristics. Among these, adaptive leadership and staff management that modelled PCC values and supported reflective practice emerged as the most consistently identified facilitators. Rather than isolated educational sessions, successful homes invested in ongoing, embedded training programs integrated into daily routines to manage gradual shifts in staff beliefs and practices. Robust interdisciplinary collaboration supported by regular communication and consistent staff assignment strengthened continuity and collective problem-solving capacity. Physical redesign through new construction or incremental renovation created shared environments supporting social interaction and household rhythms. Homes that decentralized decision-making authority to frontline staff and residents and aligned daily routines with household life proved substantially more likely to sustain transformation. Communication strategies that emphasize shared goals and resident voice further strengthened the team’s commitment to culture change.
Individuals
Barriers
Within the updated CFIR 2022 framework, individual-level barriers are primarily mapped to the Characteristics subdomain, specifically the constructs of Motivation, Capability, and Needs. Resistance to change was identified across multiple roles, including frontline staff, leadership, and families, reflecting legitimate concerns regarding increased workloads and uncertainty about evolving role expectations rather than personal opposition to person-centred principles. This resistance is often a rational response to systemic pressures: staff questioned the long-term sustainability of culture change given persistent constraints on staffing ratios, time allocations, and institutional support, leading to skepticism that extended beyond the initial implementation. Without meaningful recognition, professional development opportunities, or tangible rewards, staff lacked compelling reasons to invest in transformation, resulting in passive compliance rather than authentic commitment. Barriers related to Capability include not only limited confidence in embracing new practices but also a lack of the conceptual frameworks and practical skills needed to recognize and respond effectively to residents’ individualized preferences and needs, thereby constraining the capacity to deliver relational and personalized care. Barriers related to Need involve the challenges of managing increased resident complexity, which strains the well-being and capacity of those delivering care.
Facilitators
Within the Individual domain, includes a supportive organizational culture aligned with home-like approaches. These are managers’ willingness to adopt new practices and intrinsic staff motivation that match the core reasons staff work in LTC. The intrinsic motivation lasted longer than compliance driven by external mandates. Recognition systems that acknowledged staff contributions increased commitment and showed organizational investment in the transformation.
Innovation
Barriers
Home-like care models were consistently described as complex innovations requiring coordinated changes across multiple dimensions, including daily routines, professional roles, physical environments, and organizational culture. This complexity contributed to inconsistent implementation and elevated staff stress. Persistent tensions between resident autonomy principles and organizational safety expectations created ongoing dilemmas, particularly regarding infection-control protocols and risk-management procedures. Significantly higher labour costs associated with necessary staffing ratios and substantial capital costs for physical redesign created formidable financial barriers to adoption and scale-up, particularly for organizations operating under tight margins.
Facilitators
Strategic environmental redesign through small-home construction, unit clustering, or modification of existing spaces effectively supported everyday interaction and reduced institutional scale. Cost-conscious strategies, including phased renovations and strategic procurement, enabled homes to make meaningful changes despite budget constraints. Deliberate empowerment of frontline staff with decision-making authority enhanced responsiveness while supporting PCC principles. A robust evidence base demonstrating psychosocial benefits and quality-of-life improvements helped secure stakeholder buy-in and strengthened support for long-term implementation.
Process
Barriers
Implementation was significantly hindered when staff and families were not meaningfully engaged early in the planning process, resulting in weak ownership, limited contextual fit, and subsequent resistance. Insufficient coordination across disciplines and unclear role expectations systematically disrupted implementation processes and weakened sustainability by undermining collective accountability.
Facilitators
Effective implementation was consistently supported by early and continuing involvement from residents, families, frontline staff, and management. Team-based approaches incorporating interdisciplinary discussions and clarified responsibilities strengthened coordination and collective accountability. Opportunities to test changes on a small scale enabled staff to adapt innovations to local needs and build confidence through manageable successes. Tailoring implementation strategies and maintaining flexibility helped ensure alignment with existing routines and organizational culture. Structured reflection on progress and formal recognition of successes reinforced momentum and helped systematically embed new practices into routine operations over time.
These findings illuminate the interdependence of barriers and facilitators to implementing the home-like models. Although factors were organized by the CFIR domain for analytic clarity, the reality within LTC homes is much more interconnected. Challenges in the Inner Setting, such as workload pressures, competing priorities, and reliance on biomedical routines, are fundamentally shaped by Outer Setting forces. These include restrictive funding sources, prescriptive inspection requirements, and inflexible staffing regulations. This dynamic between external system pressures and internal capacity was evident throughout the studies, especially in homes trying to implement household or home-like models within regulatory frameworks that limited culture change.
Leadership is a central cross-domain factor. While formally part of the Inner Setting, leadership affects all domains. Leaders can mediate regulatory demands, direct resources, influence culture, and support staff adaptation. Adaptive leadership can buffer external constraints and connect system demands with organizational change. In contrast, hierarchical leadership increases external pressures and reduces readiness for change.
Interactions also occur between Individuals and Innovation. Staff motivation and readiness are influenced by model design, training, workload, and the level of autonomy supported. The complexity of home-like models means even motivated staff may struggle without sufficient adaptation, time, or clear processes. Successful homes use incremental strategies so innovation can evolve with feedback and changing needs.
Finally, Process factors integrate all domains. Engagement of families, residents, and staff builds shared understanding and challenges institutional norms. Trialability, reflection, and evaluation help address tensions between autonomy and safety or PCC and compliance. Implementation is not linear or sequential but a continuous process of adaptation and collective sense-making.
Overall, the distribution and interconnectedness of the 52 factors in this review show that home-like models require alignment at all levels. Without such alignment, even strong facilitators cannot overcome fundamental structural barriers.
Supplementary Quantitative Findings
Quantitative studies provided outcome data demonstrating the benefits of home-like models. Across survey, pre–post, and comparative designs, home-like environments were associated with higher PCC scores, greater resident quality of life, and improved staff job satisfaction. For example, units with smaller household structures and engaged leadership reported higher PCC scores (Backman et al., 2021), and residents in small-scale homes demonstrated better quality of life, and staff reported greater satisfaction compared to traditional units (Bergman, 2004). Pre- and post-renovation studies also showed improvements in resident autonomy and relational care practices (Chaudhury et al., 2017). Adoption of culture-change models such as the Eden Alternative was associated with reduced depressive symptoms and stronger staff–resident relationships (Duan et al., 2022).
Distribution of Barriers and Facilitators Across CFIR Domains
Across CFIR domains, the Inner Setting accounted for the most barriers and facilitators (22/52; 42.3%), followed by Process (9/52; 17.3%), Outer Setting (8/52; 15.4%), Innovation (7/52; 13.5%), and Individuals (6/52; 11.5%). When examined separately, Inner Setting was predominant for both barriers (11/23; 47.8%) and facilitators (11/29; 37.9%), while the Outer Setting, Innovation, and Individuals domains showed similar proportions for both barriers and facilitators. Process factors were more frequently facilitators (7/29; 24.1%) than barriers (2/23; 8.7%). Overall, barriers and facilitators spanned all CFIR domains, rather than being concentrated in any single domain. Additionally, we identified interactions between domains, including between Inner and Outer Setting for barriers and between Individuals and Innovation for facilitators.
Discussion
Home-like models have been promoted internationally as a promising alternative to traditional institutional LTC environments, yet adoption across jurisdictions remains uneven. This scoping review shows that implementation challenges arise not from a lack of willingness among staff or organizations to provide relational, resident-directed care, but from misalignment among system, organizational, and workforce conditions. By synthesizing evidence from peer-reviewed research and Canadian grey literature and mapping factors to the updated 2022 CFIR, our findings reveal a multi-level pattern in which Inner Setting conditions carry the greatest weight in shaping implementation, yet these challenges should not be interpreted as local deficiencies but rather as downstream effects of the broader policy and financing environment that the Outer Setting establishes.
Workforce instability illustrates this pattern concretely. Although it manifests as an organizational challenge within the Inner Setting, its roots lie in system-level forces, including funding shortfalls, legislative gaps, sector-wide staffing shortages, and regulatory pressures (Bhattacharyya et al., 2022; Government of Canada, 2023; Ontario Long Term Care Association, 2019). Apparent organizational failures in implementation are therefore more understood as manifestations of structural conditions, including inadequate funding, fragmented policy, and chronic workforce shortages, that exceed the capacity of any individual facility to resolve. The same logic extends to the individual level: barriers such as low motivation, limited capability, and unmet needs among staff are less a reflection of personal deficiency and more a predictable response to systemic under-resourcing, role uncertainty, and inadequate support structures. Resistance to change was not a simple reluctance; instead, it reflected concerns about workload and staffing instability (Ploeg et al., 2007; Tyler et al., 2014). These findings reinforce that changing individual practice requires concurrent organizational and system support, rather than isolated training or motivational interventions.
Regulation further demonstrates how Outer and Inner Setting factors interact. Rigid interpretations of compliance requirements often conflicted with resident autonomy, causing staff to default to institutional routines even when these routines contradicted PCC values. Evidence suggests that regulatory flexibility, when framed as principle-based rather than prescriptive, can reconcile safety with autonomy (Ontario Long Term Care Association, 2019). However, such flexibility was frequently temporary, confined to pilot projects, or dependent on local leadership discretion, limiting scalability across the sector.
Within the Inner Setting, leadership and staff management were
Findings within the Innovation domain highlighted a fundamental tension: home-like models require simultaneous changes to the physical environment, staff autonomy, and everyday routines, yet existing regulatory and funding structures were designed toward standardization, efficiency, and risk minimization, not relational care (Longstaff et al., 2022). Successful innovation required adaptive fidelity, maintaining core PCC principles while tailoring implementation to local contexts (Zimmerman et al., 2016). Incremental environmental modifications and phased workflow changes were more feasible and sustainable than large-scale redesigns (Shield et al., 2014). These findings underscore that home-like models are not plug-and-play interventions; they require iterative adaptation supported by flexible governance and stable resources.
The Process domain contained the highest proportion of facilitators, particularly stakeholder engagement, team collaboration, and trialability. These factors offered practical entry points for initiating culture change and created opportunities to learn and adjust during implementation. However, their success depended on organizational capacity, especially staffing stability and protected time for relational care (Baines & Armstrong, 2019; Bangerter et al., 2016). Sustainable change occurred when process strategies were aligned with structural supports, enabling continuity, teamwork, and staff autonomy (Shield et al., 2014; Tappen et al., 2017).
Although the evidence base is predominantly qualitative, supplementary quantitative findings reinforce the positive psychosocial impacts of home-like models, including improved quality of life, enhanced PCC, reduced depressive symptoms, and stronger staff satisfaction (Backman et al., 2021; Bergman, 2004; Duan et al., 2022). Importantly, measurable benefits often required stable staffing and supportive organizational conditions, and system-level constraints remained barriers to scale and sustainability (Chaudhury et al., 2017; Miller et al., 2010). These findings underscore the importance of aligning demonstrated benefits with structural reforms to enable the widespread, equitable, and enduring implementation of home-like models.
Strengths and Limitations
A major strength of this scoping review is the integration of peer-reviewed research with Canadian grey literature, enabling a comprehensive synthesis of empirical findings and system-level insights that are often absent from academic studies. The use of the 2022 CFIR provided a rigorous, theory-informed structure for organizing the 52 implementation factors and clarifying how barriers and facilitators interact across system, organizational, individual, innovation, and process levels. The inclusion of diverse care models strengthens the applicability of the findings across different home-like philosophies. Rigorous screening, double extraction, and consensus-based CFIR mapping enhanced reliability.
However, limitations must also be acknowledged. The evidence base was weighted toward qualitative studies, limiting the ability to estimate the magnitudes of outcomes or to statistically compare models. Grey literature varied in methodological detail, which may affect the depth of reported implementation processes. Differences in terminology across studies necessitated interpretive synthesis during CFIR categorization, which may introduce subjectivity in classification despite consensus procedures. Finally, most included studies were conducted in North America, limiting generalizability to other LTC systems.
Implications for Policy, Practice, and Research
The findings demonstrate that home-like care cannot be sustained without organizational conditions that support relationship-based work. LTC leaders should prioritize relational training, interdisciplinary teamwork, and participatory decision-making to create environments where home-like principles can be enacted. Emotional support, reflective practice, and coaching can help staff manage the complexities of resident-directed care, particularly in settings with high turnover or changing resident needs.
System-level reforms are also essential for making home-like models viable. Flexible, principle-based regulatory frameworks, staffing legislation, and funding arrangements that reward continuity over task completion are required for home-like care to thrive. Policymakers should shift from compliance-driven inspections toward outcome-oriented standards that reinforce autonomy, meaningful engagement, and the conditions of relational care. Infrastructure planning should prioritize small-scale, clustered units and accessible common spaces that align with home-like principles and reduce the institutional scale.
Further research can include longitudinal evaluation of how homes adapt and how system-level policies affect sustainability. Quantitative assessment can complement qualitative evidence to evaluate quality of life, psychosocial outcomes, and workforce stability. Hybrid implementation-effectiveness designs informed by CFIR can provide evidence to support scale-up, guide policy, and inform practice across LTC contexts.
Conclusions
This scoping review demonstrates that implementing home-like models in LTC is a multi-level challenge that depends on the alignment of system, organizational, individual, and process factors. While Inner Setting conditions, especially workforce instability, leadership, workplace culture, and the physical environment, play a central role, they are fundamentally shaped by Outer Setting structures such as regulation, funding, and staffing policies. Successful implementation requires coordinated action across the CFIR domains, with adaptive leadership, training, stakeholder engagement, and regulatory flexibility to support autonomy-driven care.
Implementing home-like models demands cultural transformation within organizations, extending well beyond physical redesign or programmatic change. Long-term sustainability, however, depends on system-level reforms that remain largely misaligned with the requirements of home-like care, particularly the shift toward principle-based regulatory frameworks and funding models that reward relational, PCC-oriented service delivery over task-based service delivery. Organizational readiness can be meaningfully strengthened through adaptive leadership, consistent staff engagement, relational training, and recognition systems that align staff values with care philosophy. Ultimately, sustainable implementation requires coherence between the work environment and the underlying care philosophy, ensuring that staff are genuinely supported in terms of time, resources, role clarity, and organizational culture to enact home-like principles in their everyday practice rather than merely complying with them.
Supplemental Material
Supplemental Material - Barriers and Facilitators to Implementing Homelike Models in Long-Term Care: A Scoping Review Using the Updated Consolidated Framework for Implementation Research
Supplemental Material for Barriers and Facilitators to Implementing Homelike Models in Long-Term Care: A Scoping Review Using the Updated Consolidated Framework for Implementation Research by Denise Bedard, Marie Savundranayagam, Maxwell Smith, and Afshin Vafaei in Journal of Applied Gerontology
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This study is based entirely on published peer-reviewed articles and publicly accessible grey literature documents. No new data were created, and therefore no datasets are available for sharing.
IRB Protocol
This study is a scoping review of publicly available literature and did not involve human participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.