
Abstract
Background
Social disconnectedness, including isolation and loneliness, is a growing concern among older veterans, who are disproportionately affected and often less likely to seek assistance. Home-delivered meals offer opportunities to address social disconnectedness by combining nutritional support with routine interpersonal contact.
Objective
This study evaluates the feasibility and perceived impact of a veteran-adapted Meals on Wheels program integrating nutritional and social support.
Methods
Validated instruments assessed social isolation, loneliness, mental/physical health, and wellbeing at baseline, week 4, and week 8. Paired t-tests evaluated changes over time. Program delivery and engagement were assessed using the RE-AIM framework.
Results
Participants reported high baseline loneliness and social isolation. Loneliness declined significantly by weeks 4 and 8, with short-term gains in physical and mental health at week 4. No sustained changes were seen in isolation or overall wellbeing. Program retention (92%), adherence (74%), and acceptability (96%) were high, with strong fidelity and varied engagement.
Highlights the potential of home-delivered meal program to reduce loneliness among older homebound veterans, with modest improvements in physical and mental health Provides novel evidence on the feasibility of implementing a home-delivered meal program among older homebound veterans Integrating meal programs into veteran and community aging services can expand reach to underserved older adults, creating a practical bridge to more comprehensive interventions that support both nutrition and social connection
Enhance service delivery into VA and community-based aging services to address nutritional needs and social connection. High engagement suggests potential to reach underserved veterans using meal delivery programs as a bridge to more sustained interventionsWhat This Paper Adds?
Applications of Study Findings
Introduction
Older veterans face elevated risks of social disconnectedness, shaped by cumulative exposures to trauma, geographic separation from military networks, and transitions into civilian life that may disrupt social ties (Straus et al., 2022; US Department of Veterans Affairs [VA], 2018). These disruptions often manifest as both perceived loneliness, defined by subjective feelings of being alone, and social isolation, characterized by objective indicators such as limited social contact or small networks (National Academies of Sciences, Engineering, and Medicine [NASEM], 2020; Cudjoe et al., 2020; Wright et al., 2019). Social disconnectedness has been linked to depressive symptoms, reduced engagement in health-promoting behaviors, diminished wellbeing, and mortality, and is increasingly recognized as an important social determinant of health in later life (Prohaska et al., 2020; Wang et al., 2015; Wright et al., 2019).
Social connectedness is considered important to the physical, mental and cognitive health and is often described as multidimensional, encompassing physical functioning, psychological resilience, social participation, and perceived life satisfaction (Holt-Lunstad, 2021; NASEM, 2020; Prohaska et al., 2020). Wellbeing reflects both subjective experiences (life satisfaction) and objective indicators (functional ability and social connectedness) (Prohaska et al., 2020). Within this framework, connectedness can be understood as both a determinant and an outcome of wellbeing, reinforcing the need for interventions that address social and structural barriers simultaneously. Researchers have identified four forms of social connection
Despite growing recognition of social disconnectedness as a social determinant of health, intervention research remains limited, particularly for older veterans. Evaluating these efforts requires attention not only to effectiveness but also to reach, adoption, and implementation domains, emphasized in the RE-AIM framework. Most studies describe prevalence rather than testing approaches to reduce isolation or loneliness. A few intervention studies have linked home-delivered meals with reduced loneliness (Thomas et al., 2015) and behavioral activation with modest social gains among veterans (Juang et al., 2021). Training resources for meal delivery drivers have also been developed to support social connection (Bunker et al., 2025). These initiatives point to possible directions but remain short in duration and scope, with little attention to integration into broader veteran services. In addition, intersections with structural vulnerabilities such as food insecurity and disability are underexplored, despite evidence that these factors compound isolation, reduce engagement and increase feelings of loneliness (National Council on Aging [NCOA], 2024; Wright et al., 2019).
Food insecurity represents a related challenge to social disconnection, reflecting limited access not only to nutrition and health maintenance but also to opportunities for social participation (NASEM, 2020; Suntai & White, 2022). Among older adults, especially veterans, limited access to nutritious food is linked to poorer physical and mental wellbeing, psychological distress, reduced community engagement (Cudjoe et al., 2020; NCOA, 2024; Wang et al., 2015). These challenges are compounded by fixed incomes, disability-related limitations, and underutilization of veteran-specific services (Wright et al., 2019). Nutrition is a modifiable determinant of wellbeing: inadequate intake impairs functioning, while shared meals and food programs foster routine, interpersonal contact, and perceived support (Choi et al., 2020; NASEM, 2020). For older veterans, who often face compounded risks of isolation and food insecurity, interventions that integrate nutritional support with opportunities for social connection may provide a practical pathway to strengthen wellbeing across multiple domains (NASEM, 2020; Suntai & White, 2022).
Community-based organizations (CBOs) such as Meals on Wheels (MOW) may help address social disconnectedness by combining nutritional support with routine personal contact (Interfaith Ministries for Greater Houston [IM], 2024; Morris et al., 2019). Interfaith Ministries for Greater Houston, which administers the region’s MOW program, trains drivers to deliver meals, conduct structured wellness checks, and engage clients in brief, informal, unstructured conversations as part of their routine service delivery (IM Houston, 2024). Similarly, regular contact with familiar volunteers can foster trust, emotional connection over time, particularly when volunteers remain on the same routes, and a sense of continuity (Morris et al., 2019). These relational dynamics, though brief, may contribute to meaningful perceived support and wellbeing. Emerging evidence further suggests that such programs may reduce loneliness by pairing nutrition with sustained interpersonal engagement among homebound older adults (Bunker et al., 2025; Ross et al., 2022). For older veterans, who often experience heightened risks of isolation and loneliness due to service-related transitions and structural barriers, these programs may offer a low-burden, community-based pathway to connection (Suntai & White, 2022; Thomas et al., 2024). However, given the limited research focused specifically on veterans, Wright et al. (2019) underscores the need to connect rural, low-income veterans with food and resource networks to address gaps in access and support. Complementing this, Tsai et al. (2025) observed that sustained social support is positively associated with improved mental health outcomes in veteran populations.
The current study explored whether participation in a home-delivered meal program, including routine interactions with delivery drivers, contributed to reduced loneliness. Building on observations that meal delivery may provide nutritional support and brief socially supportive contacts, the study also assessed factors influencing program reach, adoption, and implementation to inform broader use of meal delivery services and support study participation among older veterans.
Using the RE-AIM framework (Reach, Effectiveness, Adoption, Implementation, and Maintenance), the study evaluated program delivery and identified factors influencing reach and uptake among eligible veterans (Richman, 2018). As a pragmatic model, RE-AIM emphasizes who is served, how well the intervention works, the extent of organizational uptake, the fidelity of delivery, and the potential for long-term sustainability (Richman, 2018). Although process evaluations of meal delivery programs are well established in aging research, veteran-specific implementation studies remain limited (Morris et al., 2019; Thomas et al., 2015). This study sought to address that gap by exploring how home-delivered meals could reduce SIL and improve wellbeing in the underserved veteran population, while also identifying barriers to access and opportunities for broader dissemination.
Methods
Program Description
Interfaith Ministries’ Meals on Wheels for Greater Houston and Galveston County was the largest provider of home-delivered meals in Texas during this study (March-December 2024). The program served an average of 5,200 homebound older adults daily across Harris, Galveston, Montgomery, Liberty, and Chambers counties. Homebound status was defined as individual, typically adults over age 60, who are unable to leave their homes without significant difficulty and often require assistance from another person or a mobility aid (IM Houston, 2024). This status was further characterized by limited ability to prepare meals and insufficient support, making home-delivered meals an essential service for both nutritional needs and routine social contact (IM Houston, 2024). The program offered nutritional support and routine interpersonal engagement to promote independence, health, and wellbeing among vulnerable seniors (IM Houston, 2024).
Participants
Participants were drawn from a convenience sample of program assessments conducted by Interfaith Ministries for Greater Houston (IM) between spring and winter 2024. All clients underwent an initial in-home assessment followed by annual reassessments. The study targeted older veterans (≥65 years) who were homebound, medically stable, and newly enrolled in the program. IM serves approximately 2,300 older veterans across five counties, which collectively include an estimated 20,000 older veteran residents (IM Houston, 2024).
Demographic characteristics of the broader client population included 44% Black, 16% Latino, 24% White, and 1% Asian; 28% are aged 75-84, and 20% are aged 85 (IM Houston, 2024). These figures underscored the racial, ethnic, and age diversity of the client base and highlighted the importance of tailoring interventions to meet the needs of a heterogeneous veteran population.
Intervention
Veterans who requested social services through Interfaith Ministries underwent an in-home assessment by a program coordinator to determine eligibility for home-delivered meals as a new client. Approved clients, specifically eligible veterans aged 65 and older, received a home-delivered meal 5 days a week (Monday-Friday) from Meals on Wheels (MOW). Meals were delivered by trained drivers who confirmed receipt and used a mobile application to document observed changes in client health, safety, or wellbeing. Alerts generated through the application were routed to care coordinators for follow-up and linkage to health or community services as needed. Services continued per standard MOW protocols after study completion.
Study Design
Veteran clients with approved assessments were screened for eligibility and contacted by phone to schedule an in-person consent visit prior to meal delivery initiation. The study aimed to enroll 25 participants, a target selected to reflect feasibility within program resources and to provide preliminary data for future, larger-scale evaluations. Structured assessments were administered by trained research staff during hour-long home visits at baseline, midpoint (week 4), and endpoint (week 8). In addition, weekly interviewer-administered phone surveys monitored changes in health status, loneliness, pain, and meal-related concerns. Upon study completion, participants received a $25 HEB grocery store gift card. Primary outcomes included social isolation and loneliness, while secondary outcomes assessed physical and mental health, and life satisfaction. The study was approved by the University of Texas Health Science Center Institutional Review Board (HSC-SPH-23-0895
Outcome Measures
Social isolation was assessed using the 6-item Lubben Social Network Scale (LSNS-6), which evaluates perceived social engagement with family (items 1–3) and friends (items 4–6) (Buckley et al., 2022). Each item is scored from 0 (low engagement) to 5 (high engagement), yielding a total score of 0–30, with scores below 12 indicating risk for social isolation. All items were equally weighted, and the six scores were summed to produce the total. Higher scores indicate lower social isolation; a score below 12 is a suggested cutoff (Buckley et al., 2022). The LSNS-6 has demonstrated associations with mortality, hospitalization, health behaviors, and depressive symptoms, with reported internal consistency (α = 0.74) (Brown et al., 2022).
Loneliness was measured using the 20-item UCLA Loneliness Scale (LS-20), which captures subjective feelings of social disconnection (Russell et al., 1978). Items are rated on a 4-point Likert scale (1 = Never to 4 = Always), with reverse coding applied where appropriate. Total scores range from 20 to 80, with higher scores indicating greater loneliness (Russell et al., 1978). The LS-20 has demonstrated strong internal reliability (α = 0.89–0.94) and test-retest stability over one year (r = 0.73) (Hughes et al., 2004).
Secondary outcomes included mental and physical health, assessed via the 12-item Short Form Health Survey (SF-12). The SF-12 yields two composite scores: the Physical Component Summary (PCS-12) and Mental Component Summary (MCS-12), each ranging from 0 to 100, with a normative mean of 50 (Farivar et al., 2007). Internal consistency for PCS-12 and MCS-12 has been reported as α = 0.72 and α = 0.73, respectively (Arovah & Heesch, 2021; Ware et al., 1996). Scores were calculated using the Awell Online SF-12 survey (Awell Health, 2025).
Wellbeing was operationalized through subjective life satisfaction, assessed using the Life Satisfaction Index-Z (LSI-Z), a validated instrument used in gerontological research to capture cognitive evaluations of overall wellbeing in later life (Liang, 1984). The LSI-Z is a 13-item scale comprising positively and negatively worded statements. Responses were scored using a three-point format: “Agree,” “Disagree,” and “Don’t know,” with total scores ranging from 0 to 26, with higher scores reflecting grater life satisfaction (Papi & Cheraghifard, 2019). Score ≤12 indicated low satisfaction, 13-21 average satisfaction, and ≥22 high satisfaction. The LSI-Z has demonstrated adequate internal consistency (α = 0.78) (Cheraghifard et al., 2021).
Evaluation Design and Data Collection
Definitions and Data Sources for RE-AIM Domains in the Program Evaluation
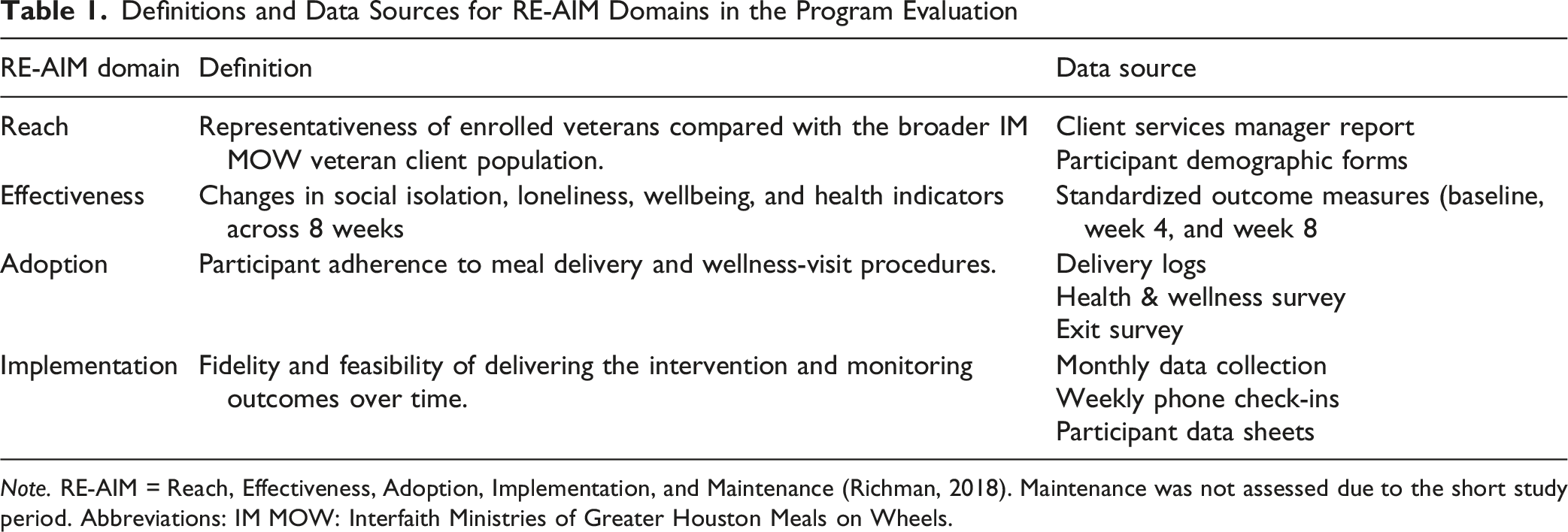
Note. RE-AIM = Reach, Effectiveness, Adoption, Implementation, and Maintenance (Richman, 2018). Maintenance was not assessed due to the short study period. Abbreviations: IM MOW: Interfaith Ministries of Greater Houston Meals on Wheels.
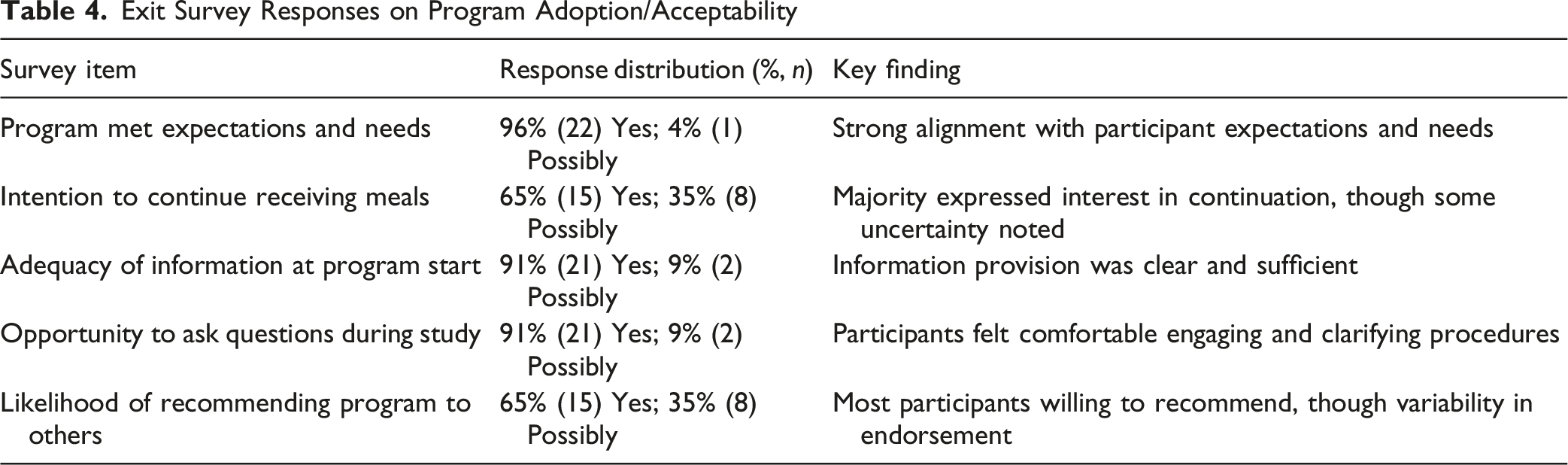
Adoption was evaluated through participant adherence to the MOW intervention protocol, including scheduled meal delivery and wellness visits. Delivery-related challenges were captured using one item from the health and wellness survey (“Have you had any issues with eating your delivered meals?”), which included binary response options and space for elaboration (Appendix A). The exit survey included four yes/no items assessing program fit and participant engagement: whether the meal delivery met expectations and needs, intent to continue receiving meals, adequacy of program information provided at enrollment, and likelihood of recommending the program to others (Appendix B).
Implementation was assessed at the study level as an ongoing process to evaluate the feasibility of monitoring program outcomes over time. Participant adherence to research protocols, including monthly home-based data collection visits and weekly phone check-ins, was tracked to ensure fidelity and consistency. Follow-up outcomes measures related to social disconnectedness were administered every four weeks across the eight-week study period, providing repeated assessments of change. Adherence was documented using participant data sheets, which captured completion of assessments, responsiveness to weekly phone calls, and overall retention. This structured monitoring approach allowed for evaluation of both participant engagement and the feasibility of sustaining outcome measurement in a community-based intervention.
Data Analysis
Descriptive statistics were used to summarize participant sociodemographic characteristics. Paired t-tests compared baseline, week 4, and week 8 assessments for all measures. Effect sizes (Cohen’s d) were calculated using G*Power 3.1 to estimate the magnitude of change and inform future sample size planning (Faul et al., 2009; StataCorp, 2023). The Cronbach’s alpha coefficients reported for each measure reflect internal consistency estimates calculated from the current sample. Analyses were conducted using STATA 18 SE, with statistical significance set at p < .05 (StataCorp, 2023). Twenty-three participants completed the full study protocol, ensuring compete case analysis.
Results
Participant Profile and Social Context
Participant Characteristics at Baseline (N = 23)
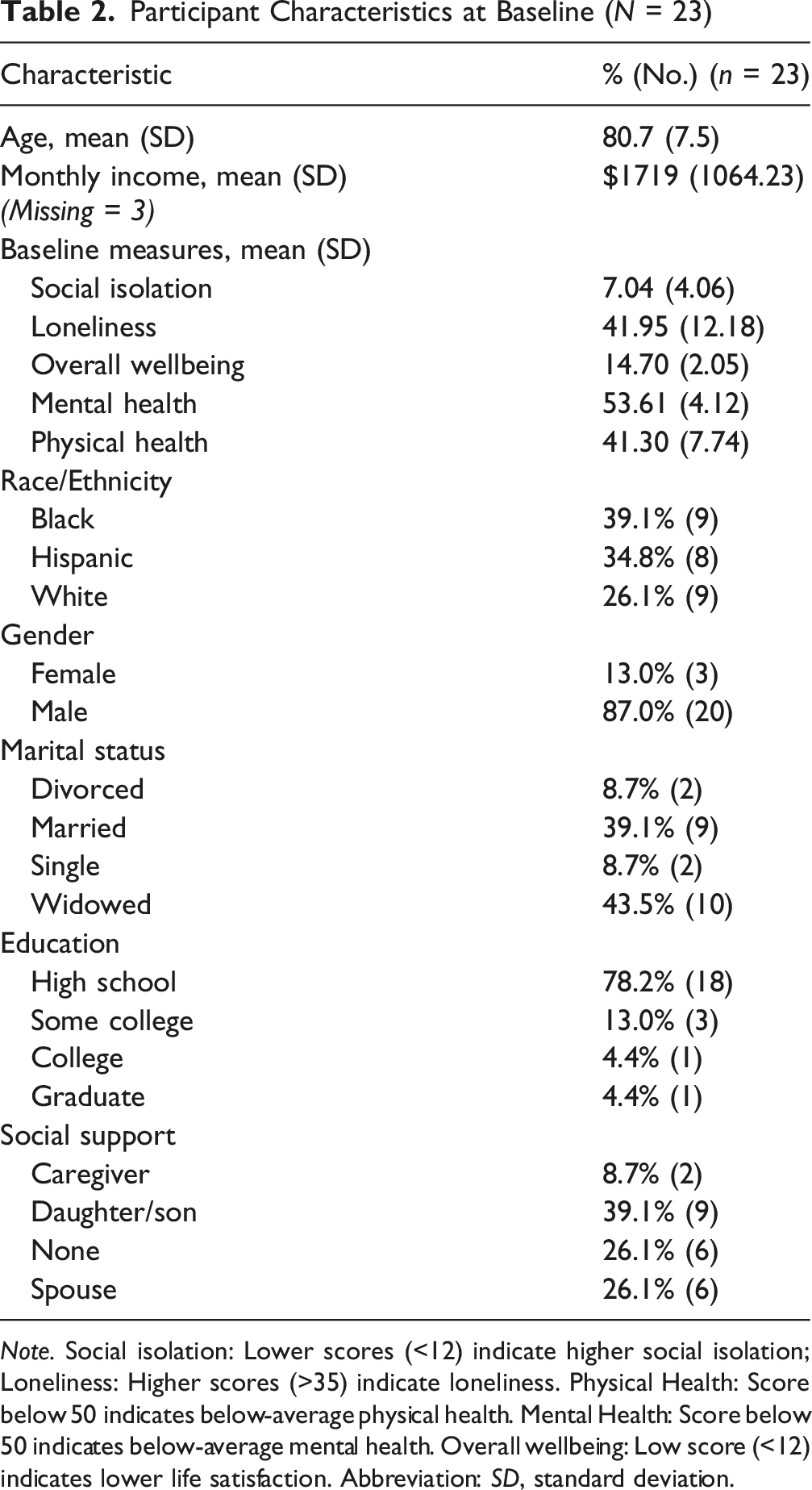
Note. Social isolation: Lower scores (<12) indicate higher social isolation; Loneliness: Higher scores (>35) indicate loneliness. Physical Health: Score below 50 indicates below-average physical health. Mental Health: Score below 50 indicates below-average mental health. Overall wellbeing: Low score (<12) indicates lower life satisfaction. Abbreviation: SD, standard deviation.
Outcome Patterns Over Time
Outcomes at Baseline, Week 4, and Week 8 With Paired Comparisons
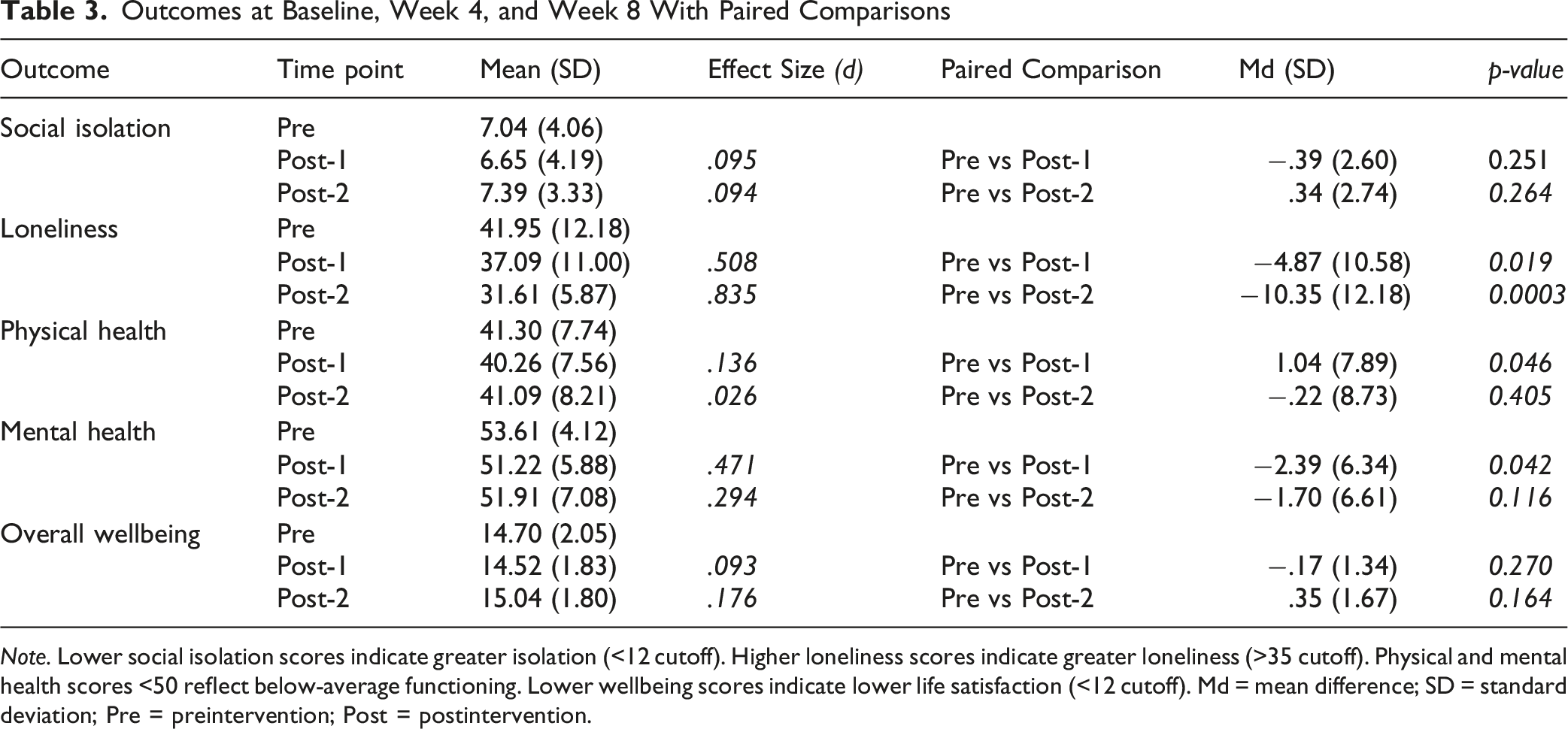
Note. Lower social isolation scores indicate greater isolation (<12 cutoff). Higher loneliness scores indicate greater loneliness (>35 cutoff). Physical and mental health scores <50 reflect below-average functioning. Lower wellbeing scores indicate lower life satisfaction (<12 cutoff). Md = mean difference; SD = standard deviation; Pre = preintervention; Post = postintervention.
Mental health showed modest fluctuation, decreasing from 53.61 (SD = 4.12) at baseline to 51.22 (SD = 5.88) at week 4 (d = .47). This decline was statistically significant (Md = −2.39, SD = 6.34, p = .042), but scores stabilized by week 8 at (51.91, SD = 7.08; Md = −1.70, SD = 6.61, p = .116), suggesting a temporary fluctuation rather than sustained change.
Overall wellbeing (life satisfaction) increased slightly over time, rising from 14.70 (SD = 2.05) at baseline to 15.04 (SD = 1.80) at week 8. Effect sizes were small (d = .09 at week 4; d = .18 at week 8) and paired comparisons indicated no statistically significant changes (week 4: Md = −.17, SD = 1.34, p = .270; week 8: Md = 0.35, SD = 1.67, p = .164), though a modest upward trend was observed.
In contrast, social isolation and physical health remained largely stable. Social isolation scores showed minimal fluctuations (Pre: 7.04, Post-1: 6.65, Post-2: 7.39), with negligible effect sizes (d = .095 and .094) and non-significant paired difference at both week 4 (
Reach (Intervention)
Twenty-five older veterans were initially enrolled: two declined study participation following the first scheduled phone contact. Among the 23 study participants, the demographic profile (mean age = 80.7; 87% male) aligned with the broader population served by IMGH (mean age = 81.5; 96% male), though the proportion of Black veterans was lower in the study sample (39% vs. 65%). Recruitment relied on an assessment list developed in coordination with the Meals on Wheels Client Services manager and approved assessors, highlighting the feasibility of integration into existing service workflows.
Adoption (Intervention)
Exit Survey Responses on Program Adoption/Acceptability
Implementation (Study)
All consenting participants completed outcome measures at both week 4 and week 8. Minor gaps in weekly survey completion were noted, most often due to health events or phone access issues. One participant missed multiple surveys due to hospitalization, loss of a cell phone, and medical appointments. Notably, one individual reported increased loneliness over the study period, distinct from broader trends, and experienced persistent survey nonresponse. These patterns point to variability in engagement and response trajectories within a generally high-fidelity implementation process.
Discussion
This study observed a home-delivered meal program implemented among older homebound veterans, with particular attention to its potential association with perceived loneliness and feasibility across the RE-AIM domains. Decreases in loneliness scores during the 8-week period suggest a possible link between participation in the program and reductions in subjective feelings of disconnection. The program demonstrated high retention and adherence, and quantitative data on reach, adoption, and implementation indicated broad engagement among veterans not previously receiving meals. Exit surveys further reflected satisfaction, with most participants reporting that the program met their expectations and needs.
Taken together, these findings highlight both the promise and the limitations of meal delivery programs in addressing social disconnectedness. While reductions in loneliness were observed, the absence of change in broader indicators such as life satisfaction underscores the need to consider how brief, routine interactions can be enhanced to produce more sustained benefits. One potential pathway is to design these conversations around strengths-based and positive psychology strategies, which emphasize resilience and wellbeing rather than deficit correction (Holt-Lunstad, 2021; Prohaska et al., 2020). Evidence suggests that behavioral activation, when delivered by non-clinicians, can improve mental and physical health outcomes among older adults (Choi et al., 2020). Within the context of home-delivered meals, drivers could be trained to incorporate simple prompts that reinforce engagement in meaningful activities or highlight resilience in daily routines. These strategies may help translate short-term improvements into longer-lasting gains, particularly if paired with extended follow-up periods that allow cumulative benefits to emerge (Campbell et al., 2021; Juang et al., 2021).
Evaluations using frameworks such as RE-AIM emphasize the importance of reach and adoption in advancing population-level benefit (Berkowitz et al., 2018; Dondanville et al., 2022; Juckett et al., 2024; LoSavio et al., 2024). The current study demonstrates that meal-based support can be feasibly delivered within established service channels, with procedural flexibility that allows for pauses and re-engagement based on participants’ health needs. Implementation processes were generally consistent, reflected high survey completion and low attrition, confirming that longitudinal assessment may be achievable in this population. At the same time, variability in engagement was observed, with one participant reporting increased loneliness and repeated survey nonresponse, underscoring the need for tailored approaches and monitoring differential trajectories.
By reaching more than 2,300 older veterans, IM’s Meals on Wheels program demonstrated substantial penetration into the local veteran community; however, many older veterans in the region remain outside the program’s reach. This disparity reflects broader challenges in connecting veterans to community-based services, particularly those who are rural, low-income, or socially isolated (Wright et al., 2019). National data reinforce these concerns: nearly half of U.S. veterans are aged 65 or older, and older veterans experience higher rates of disability, chronic illness, and food insecurity compared to non-veterans (Campbell et al., 2021; NASEM, 2020). These patterns highlight the need for targeted outreach strategies and cross-sector partnerships to ensure that community-based nutritional and social supports reach the veterans most likely to benefit.
Finally, broader efforts to sustain intervention impact may benefit from alignment with training and implementation strategies that foster accessibility, cultural responsiveness, and long-term scalability (LoSavio et al., 2024; Relyea et al., 2024). Prior literature underscores the relevance of provider education, coordinated service delivery, and client-centered design in maintaining program fidelity and reach (Dondanville et al., 2022). Participant feedback in the current study highlighted program acceptability, with most indicating comfort, comprehension, and interest in continued engagement. Taken together, these findings point to the need for scalable, equity-oriented interventions that support sustained improvements in loneliness and other indicators of wellbeing among older veterans.
Limitations
This study contributes novel evidence on the feasibility of a home-delivered meal program for older veterans, using validated measures and the RE-AIM framework to assess implementation. High retention, adherence, and acceptability strengthen confidence in program feasibility and relevance. However, several limitations should be noted. The small convenience sample, short follow-up period, and reliance on self-reported outcomes limit generalizability and preclude conclusions about long-term impact. The absence of a comparison group further constrains causal inference, underscoring the need for larger, longitudinal studies to clarify mechanisms and sustained effects. It should be noted that participants received a $25 HEB grocery store gift card upon study completion, which may have influenced adherence and engagement; future research should examine retention patterns with and without incentives to better isolate program effects. In addition, the hour-long home visits required for structured assessments may have introduced measurement reactivity, as extended interaction with research staff could provide additional social contact beyond usual conditions. This potential influence on perceived social connectedness should be considered when interpreting findings and designing future studies.
Implications for Future Research and Practice
Findings from this formative evaluation suggest that home-delivered meal programs may offer a feasible, low-burden approach to reducing loneliness among older veterans, while also supporting nutritional needs and routine wellness monitoring. Future research should examine longer trajectories of social engagement, health, and program sustainability, including subgroup analyses by age, functional status, and structural barriers such as food insecurity or disability.
Given the veteran focus, the Department of Veterans Affairs may consider partnering with community-based organizations or piloting similar home-delivered meal and wellness-check models within existing geriatric, primary care, or social work services to expand reach to homebound veterans and strengthen coordination with community aging networks. Evaluating cost, scalability, and integration with VA care pathways would further inform policy decisions.
For practice, integrating meal programs into veteran and community aging services may enhance reach to underserved populations and provide a bridge to more comprehensive supports. High retention and acceptability observed here underscore the potential for scaling such programs, particularly when aligned with culturally responsive training, coordinated service delivery, and strategies that promote continuity of social contact.
Conclusion
Findings suggest that home-delivered meal programs may be associated with reduced perceived loneliness among older, homebound veterans. While objective indicators of social isolation remained unchanged, the introduction of structured social interaction through meal delivery, facilitated by participants’ daily presence at home to receive meals, appeared to support subjective improvements in connection and perceived care. These results underscore the potential of such programs to extend impact beyond nutritional support, particularly through low-burden, relationship-oriented interventions. Evaluation through the RE-AIM framework demonstrated strong reach, adoption, and implementation within the Houston region, with sample characteristics aligning closely with the broader target population. Retention and participant satisfaction were notably high, reinforcing feasibility. These outcomes support the relevance of meal delivery programs as scalable, community-based strategies that can complement broader efforts to address social determinants of health.
Further research is needed to explore long-term trajectories of social engagement and health among recipients, including subgroup analyses that capture variation by age, functional status, and contextual barriers. Expanding measurement strategies to include both structural and quality domains may enhance future evaluations of social connection in this population.
Supplemental Material
Supplemental Material - Formative Evaluation of a Home-Delivered Meal Program to Enhance Social Connection Among Homebound Veterans
Supplemental Material for Formative Evaluation of a Home-Delivered Meal Program to Enhance Social Connection Among Homebound Veterans by Melissa R. Cruz, Aanand D. Naik, Jason Burnett, Jack Tsai, Vanessa Schick in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Formative Evaluation of a Home-Delivered Meal Program to Enhance Social Connection Among Homebound Veterans
Supplemental Material for Formative Evaluation of a Home-Delivered Meal Program to Enhance Social Connection Among Homebound Veterans by Melissa R. Cruz, Aanand D. Naik, Jason Burnett, Jack Tsai, Vanessa Schick in Journal of Applied Gerontology
Footnotes
Acknowledgments
We would like to thank Interfaith Ministries of Greater Houston Meals on Wheels Program staff, especially Liz Vallette and Heidi Toft. This manuscript was prepared in partial fulfillment of the requirements for the DrPH in Community Health Practice at UTHealth School of Public Health. I am deeply grateful to my dissertation committee and collaborators for their guidance throughout this process.
Ethical Considerations
The study was approved by University of Texas Health Science Center Institutional Review Board (HSC-SPH-23-0895
Consent to Participate
Respondents gave written informed consent following review and signature procedures prior to survey administration.
Author Contributions
MC conceptualized and led the study, conducted data analysis and interpretation, and drafted the manuscript. AN, JT, VS. and JB provided critical revisions and substantive intellectual content during the manuscript development. All authors reviewed and approved the final version of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to ethical considerations involving human subjects. Requests for access may be considered by the corresponding author in accordance with institutional guidelines.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.