
Abstract
Background
Loneliness and subjective age in later life have been examined extensively as separate constructs, yet surprisingly little research has explored how they are linked.
Objective
To examine: (1) the cross-sectional relationship between loneliness and subjective age, with depressive/anxiety symptoms as a potential mediator; and (2) the association between changes in loneliness and subjective age.
Methods
Data came from the 2023 (T1) and 2024 (T2) National Health and Aging Trends Study. We used descriptive statistics and path and logistic regression models.
Results & Conclusions
Higher scores in loneliness were associated with feeling less young or feeling older than actual age, with depressive/anxiety symptoms as a significant mediator. Increased loneliness from T1 to T2 and depressive/anxiety symptoms were associated with feeling less younger or older at T2, whereas physical health variables were not associated with changes in the subjective–chronological age difference. The findings underscore that self-perceived age reflects psychosocial well-being more than physical health.
• Greater loneliness is associated with reporting an older subjective age relative to chronological age, with depressive/anxiety symptoms mediating the relationship. • Increases in loneliness over time are associated with longitudinal increases in subjective age, controlling for depressive/anxiety symptoms and other covariates.
• Loneliness and depressive/anxiety symptoms in later life are modifiable factors. It is important to provide services that can alleviate loneliness and depressive symptoms in later life. • Subjective age in later life reflects psychosocial experiences of aging. It is important to provide opportunities for positive aging experiences to enhance physical and mental health and health behaviors among older adults.What This Paper Adds
Applications of Study Findings
Introduction
Most older adults worldwide report feeling younger than their chronological age (Wettstein et al., 2023). Subjective or felt age reflects a variety of biological, psychological, and social aging processes, and younger subjective age has been associated with better current and future physical, functional, mental, and cognitive health statuses as well as greater longevity, although the overall effect sizes are typically small (Alonso Debreczeni et al., 2021; Petashnick et al., 2022; Westerhof et al., 2023). In contrast, older subjective age tends to predict worse health outcomes, including frailty, falls, hospitalization, and mortality (Fundenberger et al., 2022; Li et al., 2021; Stephan et al., 2016, 2018).
Research has identified both objective health indicators and subjective health perceptions as important contributors to, and correlates of, subjective age. For example, impairment in performance on the physical and cognitive tests, activities of daily living (ADL) limitations, urinal incontinence, poor sensory health, poor self-rated health, stressful life events, and depressive/anxiety symptoms were all associated with older subjective age (Aftab et al., 2022; Choi et al., 2014; Ihira et al., 2015; Liu et al., 2025; Xie & Wang, 2023). On the other hand, common self-reported reasons for younger subjective age included staying active, good self-rated health, positive attitudes, exercise or dancing, independence, interpersonal/intimate relationships, faith/spirituality, volunteering, family, driving or traveling, and mental acuity (Choi et al., 2021).
A limited number of studies have also examined the links between subjective age and loneliness, often defined as “the unpleasant experience that occurs when a person’s network of social relationships is significantly deficient in either quality or quantity” (Perlman & Peplau, 1984, p.15). A longitudinal study of individuals aged 18-93 found that higher loneliness was associated with older subjective age cross-sectionally and a steeper increase in subjective age over time (Kornadt et al., 2025). Among U.S. older adults (age 65+), reductions in loneliness over 4 years were associated with feeling five or more years younger, while increases in depressive symptoms predicted feeling five or more years older, but changes in objective social indicators or medical conditions did not predict changes in subjective age (Ayalon et al., 2016). As a psychosocial stressor exerting negative effects on multiple health domains and behaviors (Hawkley & Cacioppo, 2010), it is not surprising that loneliness is significantly associated with perceptions of and attitudes toward one’s own aging, as individuals construct, hold, and reconstruct awareness and knowledge of their own aging process (Diehl et al., 2014).
Loneliness in later life often arises from decreased social connections, disrupted social or community participation, and major life transitions such as bereavement or retirement, and is also compounded by physical limitations and a reduced sense of purpose in later life (Hajek et al., 2025; Hawkley et al., 2019; Puyané et al., 2025; Tomida et al., 2024). Extensive research shows that loneliness is associated with the onset and worsening of depression/anxiety and overall poor mental health outcomes (Cacioppo et al., 2010; Holt-Lunstad, 2024; Lee et al., 2021; Wan et al., 2025), as well as subjective and objective cognitive declines, cancer, cardiovascular disease, and premature death (Luchetti et al., 2025; Oken et al., 2024; Paul et al., 2020; Wang et al., 2023). A systematic review of prospective studies of loneliness trajectories among individuals aged 60 and older also found that loneliness fluctuates over time; however, the most common trajectory is an ascending one, that is, a significant upward trend in loneliness levels, and both the ascending and stable-high trajectories were consistently associated with adverse health outcomes, including greater depressive symptom severity and accelerated cognitive decline (Li et al., 2025).
These earlier studies suggest that loneliness may influence subjective age, an internalized perception of one’s own aging, in part through depressive/anxiety symptoms. Psychosocial perspectives on subjective aging propose that negative affective states shape self-perceptions by heightening attention to age-related losses, reducing perceived vitality, and activating internalized age stereotypes and negative attitudes toward aging, thereby contributing to an older subjective age (Kotter-Grühn & Hess, 2012; Montepare, 2009). However, additional work is needed to clarify not only whether loneliness relates to subjective age but also the psychological mechanisms through which this association unfolds. Understanding the interrelated pathways among subjective age, loneliness, and depressive/anxiety symptoms is essential because both loneliness and depression/anxiety are modifiable, and subjective age is a meaningful predictor of health and health behaviors in later life. Examining whether short-term changes in loneliness correspond to short-term changes in subjective age will further elucidate how psychosocial experiences of loneliness may be associated with subjective aging. Such insights can ultimately inform intervention strategies aimed at reducing loneliness and promoting healthier psychological aging among older adults.
In the present study, we used two waves (2023 [T1] and 2024 [T2]) of panel data from a nationally representative sample of U.S. Medicare beneficiaries aged 65 and older. We first examined the distribution of subjective age relative to chronological age (i.e., subjective–chronological age difference or SCD) and loneliness at each wave, as well as the changes in subjective age and loneliness from T1 to T2. We then tested three hypotheses: (H1) higher levels of loneliness and depressive/anxiety symptoms would be significantly associated with smaller negative SCD (i.e., subjective age closer to chronological age) or positive SCD (i.e., subjective age older than chronological age) at T1; (H2) the T1 relationship between loneliness and SCD would be mediated by depressive/anxiety symptoms; and (H3) increases in loneliness from T1 to T2 would be significantly associated with changes in SCD at T2. Covariates included chronological age, sociodemographic factors, social network size, and physical, cognitive, and sensory health statuses. Importantly, subjective age in this study is conceptualized not as a preference for youthfulness or a devaluation of chronological age, but as a psychosocial marker reflecting how social and emotional experiences shape individuals’ perceptions of aging. The findings from this study contribute to a deeper understanding of how loneliness and depressive/anxiety symptoms interact to influence subjective age in later life.
Methods
Data and Sample
Data came from the 2023 and 2024 National Health and Aging Trends Study (NHATS; https://www.nhats.org/). The 2024 NHATS data were collected from those who continued from 2023. We focused on 7,316 and 6,198 sample persons in 2023 (T1) and 2024 (T2), respectively, who lived in their own homes or residential care communities (but not in nursing homes) and self-reported data (i.e., no proxy interview) on loneliness and subjective age. The NHATS did not ask proxy interviewees (n = 390 at T1and n = 321 at T2) about the sample persons’ loneliness and subjective age. Of the self-respondents, 231 at T1 and 178 at T2 who did not provide data (refused or “do not know”) on subjective age were excluded from the study. Compared to those who reported subjective age at T1, those who did not were older (by 3 years; p < .001) and expressed higher loneliness (p = .015) but did not differ on depressive/anxiety symptoms and chronic medical conditions. They also included more women and those who lived alone, but did not differ significantly by race/ethnicity. Participants who did not report subjective age at T2 did not differ significantly from those who did on loneliness, depressive/anxiety symptoms, or chronic medical conditions. The NHATS administrators approved the use of a “sensitive” data file containing chronological age in years in this study. This study was based on de-identified, publicly available NHATS data and was therefore exempt from the authors’ institutional review board review.
Measures
Chronological and subjective age: Chronological age at each wave was measured in years. Subjective age refers to felt age and was assessed in NHATS using the following question: “Sometimes people feel older or younger than their age. During the last month, what age did you feel most of the time?”
The subjective–chronological age difference (SCD) at T1 was calculated by subtracting chronological age from subjective age (i.e., subjective age minus chronological age). Negative values indicate a subjective age younger than chronological age, zero indicates no difference, and positive values indicate a subjective age older than chronological age.
Change in subjective age from T1 to T2 was calculated by subtracting subjective age at T1 from subjective age at T2 (i.e., T2 subjective age minus T1 subjective age). Negative values indicate a younger subjective age at T2 relative to T1, zero indicates no change, and positive values indicate an older subjective age at T2 relative to T1. This measure captures within-person change in felt age across the two study waves.
Loneliness and change from T1 to T2: Loneliness was assessed with a question, “During the last month, how often did you feel lonely?” The response categories were every day (=5), most days (5–6 days a week) (=4), some days (2–4 days a week) (=3), rarely (once a week or less) (=2), and never (=1). We treated it as a continuous variable, with higher scores representing greater loneliness. For descriptive purposes, we also grouped them into three categories (never/rarely, some days, and five or more days). The change in loneliness from T1 to T2 was calculated by subtracting T1 loneliness from T2 loneliness scores; thus, higher values indicate greater loneliness in T2. For descriptive purposes, we also reported changes in categories (no change, decreased loneliness, and increased loneliness from T1 to T2).
Depression/anxiety symptoms in the past month at T1 and T2: In NHATS, depression/anxiety symptoms were assessed with the Patient Health Questionnaire-4 (PHQ-4) (Kroenke et al., 2009). The PHQ-4 includes the first two items (PHQ-2; had little interest or pleasure in doing things, and felt down, depressed, or hopeless) from the 9-item PHQ-9 for depression (Kroenke et al., 2003) and the first two items (GAD-2; felt nervous, anxious, or on edge, and have been unable to stop or control worrying) from the 7-item Generalized Anxiety Disorder Scale (Spitzer et al., 2006). Responses to each PHQ-4 item were based on a 4-point scale (0 = not at all; 1 = several days; 2 = more than half the days; 3 = nearly every day), with the total score ranging from 0 to 12. The unweighted Cronbach’s alphas for the PHQ-4 for the study samples were .77 in 2023 and .76 in 2024. For descriptive purposes, the symptom severity was also categorized into no symptom (0-2), mild symptoms (3-5), and moderate/severe symptoms (6-12) (Kroenke et al., 2009).
Sociodemographic factors and social network size. Sociodemographic factors included: gender (female vs. male); race/ethnicity (non-Hispanic White [reference category], non-Hispanic Black, Hispanic, all other); education (bachelor’s degree or higher vs. no degree); income (low-income [<$43,000] vs. all other categories) at each wave; living arrangement (living alone vs. living with spouse and/or other) at each wave; and residential type (care community vs. own home) at each wave. Social network size at T1 and T2 was defined as the number (0–5) of people with whom the sample person spoke about important matters in life, including positive or negative events and problems or concerns they may have had. Social network size was included as a covariate as it may influence social engagement and help decrease loneliness among older adults.
Physical/functional and sensory health at T1 and T2 was measured with (a) the number of chronic medical conditions (0–8: arthritis, cancer, hypertension, heart disease, stroke, diabetes, lung disease, osteoporosis); (b) activity-limiting chronic pain (yes or no); (c) vision impairment (i.e., cannot see well across the street with or without glasses); and (d) any hearing impairment (with or without hearing aid). We also included past-month exercise as a health indicator. NHATS includes two exercise variables: walking for exercise, and spending time on vigorous activities (working out, swimming, running, or biking, or playing a sport). We created a variable indicating engagement versus no engagement in any of these activities.
Cognitive health at T1 and T2 was measured with dementia status (no dementia, possible dementia, and probable dementia) determined using the NHATS dementia classification algorithm (https://nhats.org/researcher/nhats/methods-documentation?id=technical-papers) based on two types of information for self-respondents: (1) doctor diagnosis of dementia or AD (yes or no); and (2) scores from cognitive tests evaluating the sample person in the following three domains: memory (immediate and delayed 10-word recall), orientation (date, month, year, and day of the week; naming the President and Vice President), and executive function (clock drawing test). A possible dementia classification was assigned when the person scored ≤1.5 SD below the mean in one domain of the cognitive test. A probable dementia classification was assigned when the person was diagnosed with dementia or scored ≤1.5 standard deviations (SD) below the mean in at least two domains of the cognitive tests.
Analysis
All analyses were conducted with Stata/MP 19.5’s svy function (College Station, TX) to account for NHATS’s stratified, multistage sampling design. All statistics are weighted except for the sample size. First, we used univariate frequencies to describe characteristics of the T1 sample and the T1-T2 continued sample. Second, we fitted a path model (see Figure 1) to test H1 and H2 regarding the direct effects of loneliness and depressive/anxiety symptoms on SCD at T1, as well as the mediating role of depressive/anxiety symptoms in the relationship between loneliness and SCD. Because most older adults reported feeling younger than their chronological age, the distribution of SCD was markedly left-skewed (ranging from −78 to +35). To address this skewness and retain information about directionality, we applied a signed log transformation to SCD. In the transformed variable, negative values indicate a subjective age younger than chronological age (with values closer to zero indicating a smaller difference), and positive values indicate a subjective age older than chronological age; the transformation compresses extreme values toward greater symmetry. Sensitivity analysis showed that the results were substantively similar to those obtained with the untransformed SCD, supporting the robustness of our findings. Path coefficients (B) and linearized standard errors (SE) with 95% confidence intervals (CIs) were estimated using the survey-adjusted SEM framework. Mediation model showing the indirect and direct associations among loneliness, depressive/anxiety symptoms, and subjective–chronological age difference (SCD). Note. Covariates (not shown in diagram): age, sex, race/ethnicity, education, income, living arrangement, residence type, social network size, and physical, cognitive, and sensory health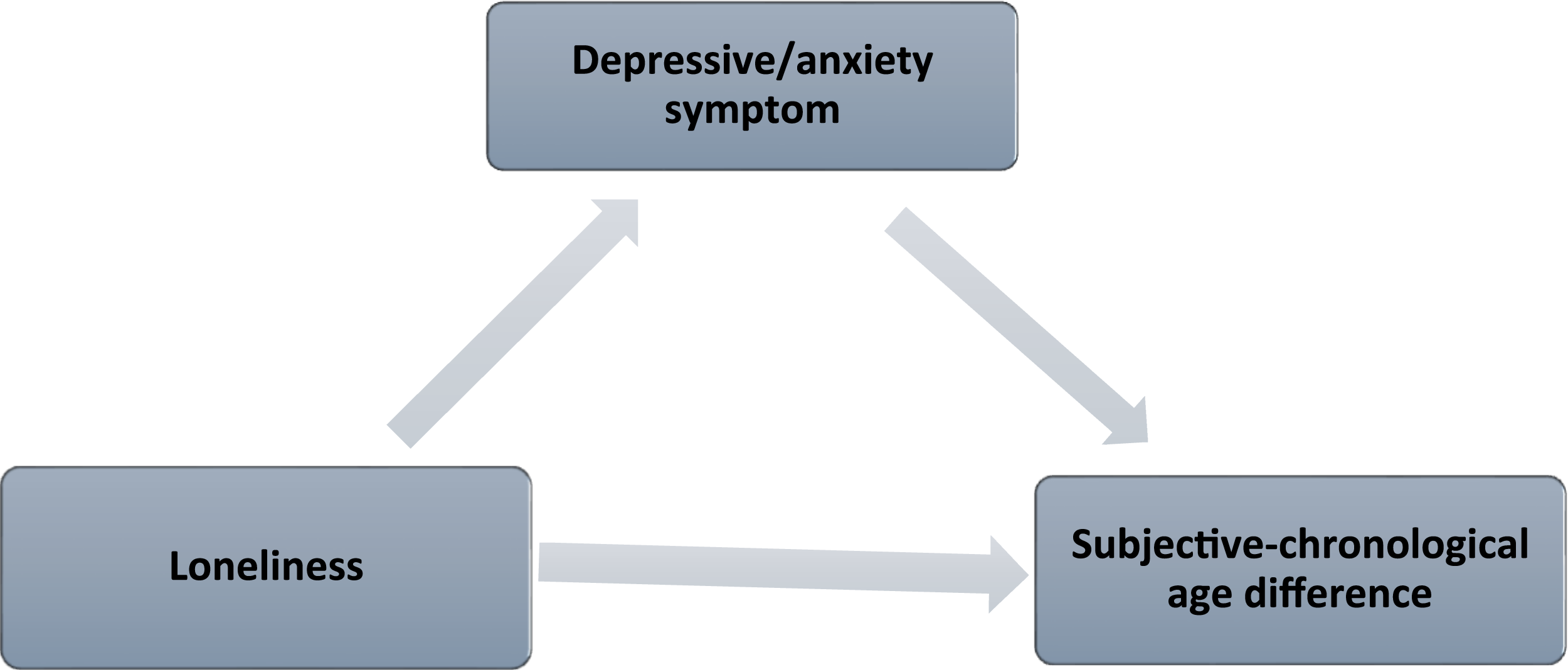
To assess mediation, we computed the indirect effect and its 95% CIs of depressive/anxiety symptoms on SCD using bootstrapping with 10,000 replications. In addition, we calculated the proportion of the total effect that was mediated (indirect effect divided by the sum of direct and indirect effects) and the ratio of indirect to direct effects. Note that, given the cross-sectional data, while we use terms such as direct and indirect effects from the mediation literature, we do not infer causal relationships, but the findings reflect associations.
To test H3 (associations between changes in loneliness and changes in subjective age from T1 to T2), we used linear regression analysis. Because the distribution of subjective age change values was highly skewed, with long negative and positive tails (range: −78 to +74), we also used signed log-transformed difference scores, with negative values indicating a decrease in subjective age from T1 to T2 (with values closer to zero indicating a smaller change), and positive values indicate an increase in subjective age over time. The results were substantively similar to those obtained using the untransformed difference scores, supporting the robustness of our findings. Linear regression results are presented as unstandardized coefficients (B) and linearized SE with 95% CIs.
Results
Sample Characteristics at T1 and T2
Weighted Descriptive Characteristics of the Study Sample at 2023 (T1) and 2024 (T2), and Changes in Loneliness and Subjective Age
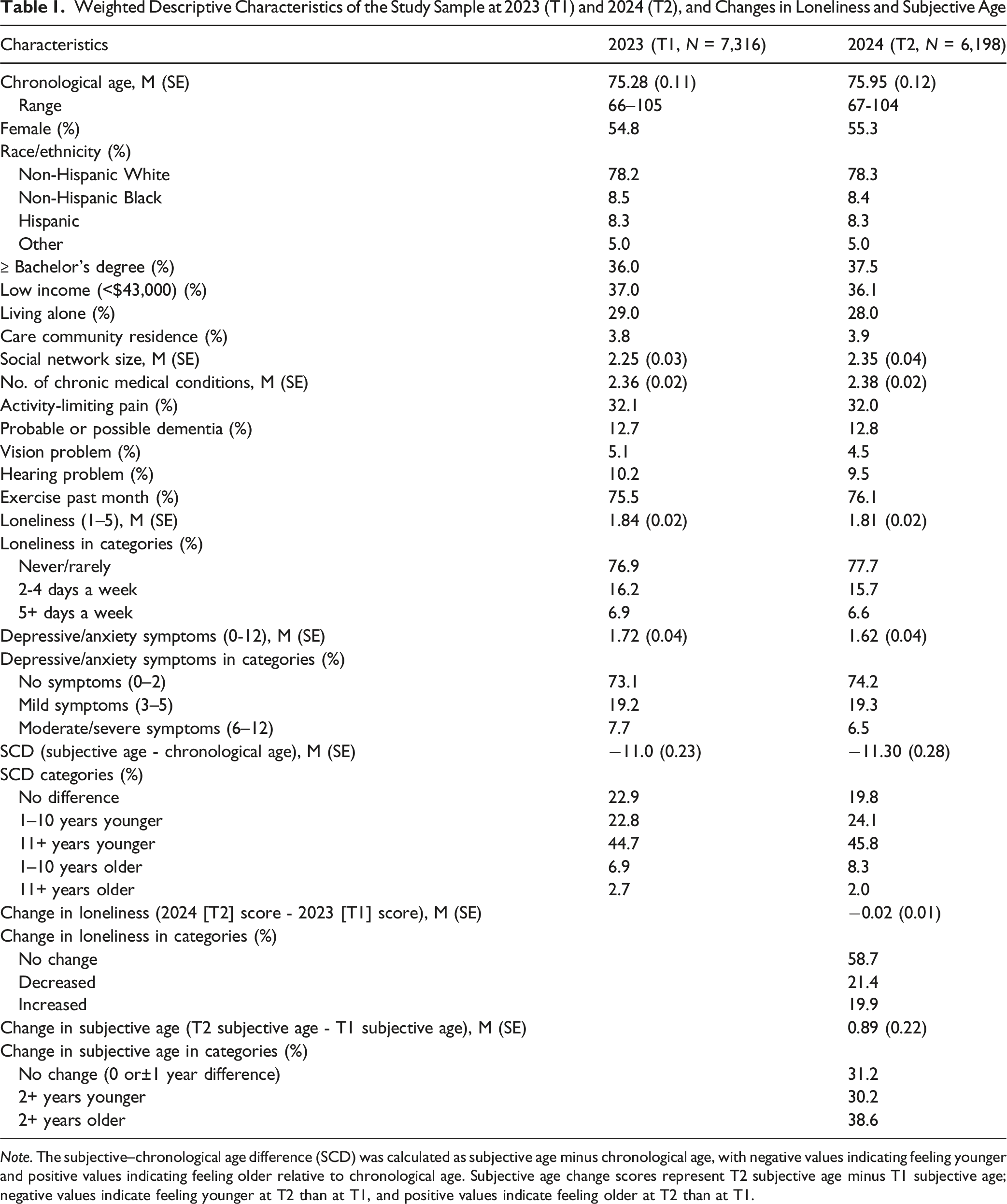
Note. The subjective–chronological age difference (SCD) was calculated as subjective age minus chronological age, with negative values indicating feeling younger and positive values indicating feeling older relative to chronological age. Subjective age change scores represent T2 subjective age minus T1 subjective age; negative values indicate feeling younger at T2 than at T1, and positive values indicate feeling older at T2 than at T1.
Regarding loneliness, 23.1% at T1 and 22.3% at T2 reported feeling lonely at least 2 days a week. Between T1 and T2, 58.7% showed no change in loneliness, whereas 21.4% and 19.9% reported decreased and increased loneliness, respectively. The mean change score was −0.02 (SE = 0.01). Regarding depressive/anxiety symptoms, 7.7% at T1 and 6.5% at T2 reported moderate/severe symptoms.
Table 1 also shows that, on average, subjective age was 11 years younger than chronological age at both T1 and T2. At T1, 67.5% reported a younger subjective age, 22.9% reported the same subjective and chronological age, and 9.6% reported an older subjective age. At T2, the corresponding percentages were 69.9%, 19.8%, and 10.3%. Additional analysis showed that SCD was −17.5 (SE = 0.23) years among those who reported a younger subjective age, and 8.4 (SE = 0.41) years among those who reported an older subjective age at T1. There was also a significant difference in T1 SCD by age group (F [4,53] = 9.97, p < .001) and race/ethnicity (F [3.54] = 8.99, p < .001). SCD was larger among the older age groups (i.e., −12.4 and −13.1 years in the 80–84 and 85+ groups, respectively, compared to −9.4 years in the 65–69 group) and among Blacks (−13.1) and Hispanics (−12.7), compared to non-Hispanic whites (−10.5).
On average, T2 subjective age was 0.9 years older than T1 subjective age; 30.2% reported T2 subjective age that was 2+ years younger than T1 subjective age, 31.2% reported the same (i.e., <2-year difference) subjective age at both T1 and T2, and 38.6% reported T2 subjective age that was 2+ years older than T1 subjective age. Additional analysis showed no significant differences in subjective age changes from T1 to T2 across age groups and sex; however, compared with non-Hispanic white older adults, Black older adults were more likely to report a younger subjective age at T2 than at T1 (t = 2.65, p = .01).
Direct Effects of Loneliness and Depressive/Anxiety Symptoms on SCD at T1
Effects of Depressive/Anxiety Symptoms on the Association Between Loneliness and SCD (Subjective–Chronological Age Difference) at T1: Parameters from the Mediation Model Using Path Analyses
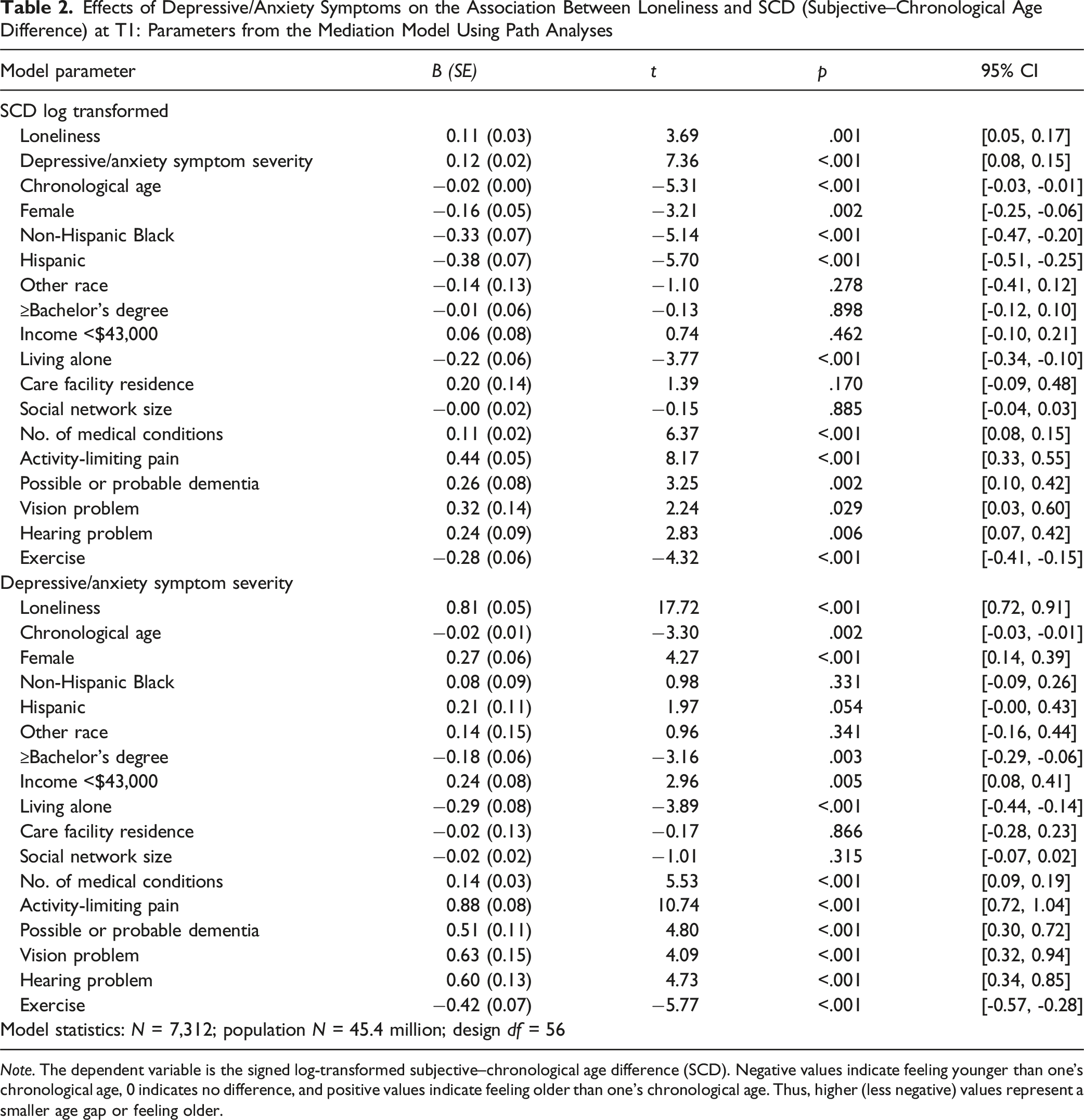
Note. The dependent variable is the signed log-transformed subjective–chronological age difference (SCD). Negative values indicate feeling younger than one’s chronological age, 0 indicates no difference, and positive values indicate feeling older than one’s chronological age. Thus, higher (less negative) values represent a smaller age gap or feeling older.
Among the covariates, a greater number of chronic medical conditions, activity-limiting pain, possible or probable dementia, and vision or hearing problems were also positively associated with the log-transformed SCD, indicating smaller subjective–chronological age gaps. In contrast, older chronological age, female sex, Black or Hispanic race/ethnicity, living alone, and engaging in regular exercise were negatively associated with the transformed SCD, that is, larger negative SCDs, indicating feeling younger than one’s chronological age.
As shown in the lower portion of Table 2, depressive/anxiety symptoms were strongly and positively associated with loneliness (B = 0.81, SE = 0.05, t = 17.72, p < .001). Depressive/anxiety symptoms were also positively associated with female sex, lower income (<$43,000), greater numbers of chronic medical conditions, activity-limiting pain, possible or probable dementia, and sensory (vision or hearing) problems. Conversely, they were negatively associated with older age, college education, living alone, and regular exercise.
Indirect Effects of Depressive/Anxiety Symptoms on SCD
Bootstrapped results indicated a significant indirect effect of loneliness on the signed log-transformed SCD through depressive/anxiety symptoms (indirect effect = 0.09, 95% CI [0.07, 0.12], z = 6.81, p < .001). The ratio of this indirect effect (0.09) to the total effect of loneliness on SCD (indirect + direct = 0.20) was 0.45, indicating that nearly half of the total association between loneliness and SCD operated through depressive/anxiety symptoms. The ratio of the indirect to the direct effect was 0.82, further underscoring the substantial mediating role of depressive/anxiety symptoms. These results fully supported H1 and H2.
Associations Between Changes in Subjective Age and Changes in Loneliness from T1 to T2
Associations Between Changes in Loneliness and Changes in Subjective Age from T1 to T2: Results from a Linear Regression Model
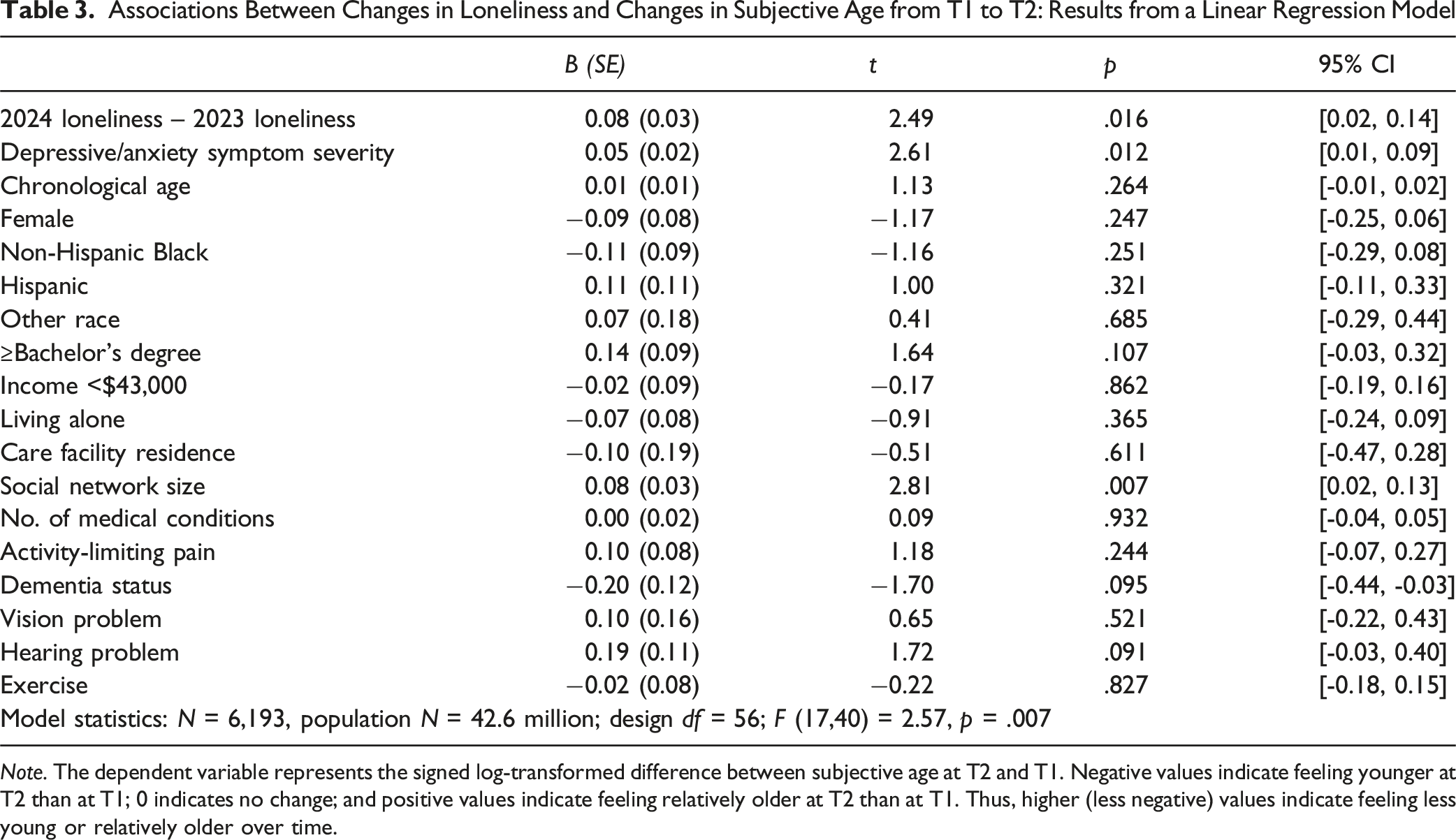
Note. The dependent variable represents the signed log-transformed difference between subjective age at T2 and T1. Negative values indicate feeling younger at T2 than at T1; 0 indicates no change; and positive values indicate feeling relatively older at T2 than at T1. Thus, higher (less negative) values indicate feeling less young or relatively older over time.
Discussion
This study examined the relationship between loneliness and subjective age, with depressive/anxiety symptoms as a mediator, among U.S. older adults. Consistent with previous research (Choi et al., 2014; Li et al., 2021), two-thirds or more of older adults in this study felt younger, and about 10% felt older than their chronological age. Loneliness and depressive/anxiety symptoms were significantly associated with the subjective age and chronological age difference, or SCD, with higher scores being associated with feeling less young or feeling older than actual age. The mediation model showed that depressive/anxiety symptoms mediated nearly half of the relationship between loneliness and SCD.
Changes in loneliness between T1 (2023) and T2 (2024) were associated with changes in subjective age. As hypothesized, greater loneliness at T2 relative to T1 was associated with reporting an older subjective age at T2 compared with T1. In other words, increases in loneliness were associated with longitudinal increases in subjective age, even after adjusting for depressive/anxiety symptoms, chronological age, and other covariates. Notably, only loneliness, depressive/anxiety symptoms, and social network size emerged as significant correlates of 1-year change in subjective age; physical, functional, and cognitive health indicators were not associated with these changes. Interestingly, although loneliness remained stable for nearly 60% of older adults, even relatively small fluctuations in loneliness were meaningfully associated with shifts in subjective age, underscoring the sensitivity of subjective age to changes in psychosocial experience.
The links between loneliness and subjective age observed in this study and prior research (Ayalon et al., 2016; Kornadt et al., 2025) suggest that lonelier older adults may conflate their perceived social disconnection with the experience of aging itself. The mediating role of depressive/anxiety symptoms between loneliness and subjective age aligns with evidence that negative affect and stress amplify feelings of accelerated aging and more negative self-perceptions of aging (Kotter-Grühn & Hess, 2012; Montepare, 2009). In sum, our findings clarify the cross-sectional and short-term longitudinal dynamics linking psychosocial well-being and subjective age.
Subjective–chronological age difference or SCD was also greater among older age groups, consistent with the notion that subjective age becomes increasingly psychologically and socially constructed over time. An earlier study found that objective health indicators were significantly associated with felt-chronological age discrepancy only in the 70–79 age group, whereas subjective health perceptions and psychological well-being were significantly associated with age discrepancy across all older adult age groups (Choi et al., 2014). In this context, the larger SCD among older adults in our study may reflect resilience and positive affect despite health challenges. After adjusting for other covariates, SCD was also higher among Black and Hispanic older adults, those living alone, and those who reported exercising regularly. In a qualitative study of felt age (Choi et al., 2021), Black and Hispanic older adults who reported younger felt age often described downward social comparisons with less healthy peers, gratitude for social connectedness and leisure activities such as dancing and exercise, and pride in maintaining independence after a lifetime of hardship. Thus, the positive association between living alone and higher SCD in our study may reflect the social value placed on independence and self-reliance in later life, which can shape how individuals perceive their age relative to chronological time.
Interestingly, social network size was not associated with SCD or depressive symptoms cross-sectionally; however, a larger network predicted shifts toward a smaller SCD. Given that the NHATS measure captures emotionally meaningful confidants rather than casual contacts, one plausible explanation of this counterintuitive finding is that older adults with more supportive people around have more positive self-perceptions of aging (Ingrand et al., 2018) and thus feel more comfortable with and accepting of their aging. Another possibility is that older adults facing more emotional or health challenges, and therefore experiencing greater aging-related strain, may expand or maintain more supportive ties as a coping or compensatory response to perceived losses. Previous studies have shown that social networks can serve both protective and compensatory functions, depending on individuals’ psychological states and perceived needs (Meyer-Wyk & Wurm, 2024; Vos et al., 2020). In this sense, network size may reflect not only social resources but also social demands and emotional investments that influence how individuals experience aging.
This study has a few limitations. NHATS included only a single item assessing felt age, precluding more nuanced assessments of subjective aging. Loneliness and depressive/anxiety symptoms were also measured with brief scales (one and four items, respectively), limiting construct precision. The use of cross-sectional and two-wave data limits causal inference and examination of potential bidirectional associations between loneliness and depressive/anxiety symptoms or between loneliness and subjective age. Self-reports may be subject to recall bias or social desirability bias. Longer observation periods and richer measures of psychosocial functioning would strengthen future analyses.
Despite these limitations, this study’s findings underscore the importance of alleviating loneliness in late life, given its role in depressive/anxiety symptoms and subjective age. Evidence-based interventions, such as community engagement initiatives, social prescribing, peer-delivered behavioral activation, and technology-supported befriending, have demonstrated effectiveness in reducing loneliness among older adults (Fakoya et al., 2020; Hoang et al., 2022; Paquet et al., 2023). Implementing such interventions at individual, interpersonal, and community levels could enhance both psychological well-being and subjective vitality in late life. Future research should further integrate psychological constructs such as personality traits, internal locus of control, generativity, resilience, and self-perceptions of aging, as well as contextual and cultural factors, to deepen our understanding of how older adults interpret and internalize their sense of age. Longitudinal analyses capturing longer-term patterns of stability and change in subjective age will also provide valuable insight into the mechanisms of adaptive aging and emotional resilience.
Footnotes
Author Contributions
Study concept and design: Namkee G. Choi & Nathan Marti. Acquisition of data: Namkee G. Choi. Data analysis: Namkee G. Choi. Interpretation: Namkee G. Choi & C. Nathan Marti. Drafting of the paper: Namkee G. Choi. Final editing: Namkee G. Choi & C. Nathan Marti.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant P30AG066614, awarded to the Center on Aging and Population Sciences at The University of Texas at Austin by the National Institute on Aging.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study (The National Aging and Health Trends Study) are in the public domain.
Research Ethics
The University of Texas at Austin’s Institutional Review Board exempted this study based on de-identified public-domain data.