
Abstract
The capability of people to engage in meaningful activities declines with the progression of major neurocognitive disorders. Cognitive strategies can help them pursue such activities, thus maintaining their dignity. They build on procedural memory and implicit retrieval, both preserves abilities, to automate the correct action sequences during learning, with repetition and while providing cues. However, few studies have implemented cognitive strategies especially in seniors’ residences. Thus, the feasibility of their implementation remains unknown. This study aims to document the facilitators and barriers to the implementation of cognitive strategies with people living with neurocognitive disorders housed in a private seniors’ residence. This participatory action research included training and coaching to allow care staff to integrate personalized cognitive strategies with nine residents. Qualitative interviews with 20 care staff and a focus group with 2 managers were conducted. Key facilitators identified included personalized approach rooted in life history, team awareness and engagement, alignment with organizational values, and a calm, home-like environment. Barriers included the rapid progression of neurocognitive disorder symptoms related to comorbidities, staff shortages and turnover, and disparities between organizational decisions and clinical practice. The results showed encouraging avenues to integrate cognitive strategies in long-term care settings when the care team is supported by adequate training and coaching.
Keywords
• Although cognitive strategies are promising for improving the autonomy and quality of life of people living with neurocognitive disorders, they remain poorly implemented in residential resources such as seniors’ residences. This study paves the way for the application of cognitive strategies in such contexts. • The participatory action research methodology is an important strength as interventions were carried out in co-construction with the team and implemented directly by the staff. This approach made it possible to anticipate challenges and adjust the process as they arose, based on lived experience, thereby improving the interventions accordingly.
• These results highlight the relevance of implementing cognitive strategies in residential care settings and emphasize the importance of supporting staff throughout the process, particularly in personalizing strategies to each resident. With effective training, the presence of a local champion, and regular coaching, the care team can successfully integrate cognitive strategies into daily practice, even when occupational therapists provide support only remotely. • Methods adapted to the realities of care providers working in residential care, including personalized tools such as brief and simple posters summarizing the steps associated to the use of cognitive strategies in a specific activity with a resident, must be prioritized to support the successful implementation of cognitive strategies in current work environments.What This Paper Adds
Applications of Study Findings
Introduction
Major neurocognitive disorders (MNCDs) are among leading causes of loss of autonomy (INSPQ, 2017). According to the Alzheimer Society of Société Alzheimer du Canada (2024), more than 650,000 Canadians were living with an MNCD in 2024, and this number is expected to reach more than one million by 2030. MNCDs, including Alzheimer’s disease, are characterized by impaired cognitive functions, notably memory and executive functions (American Psychiatric Association, 2013). These impairments significantly affect senior’s capability to carry out meaningful activities (Cipriani et al., 2020). Meaningful activities are based on the individual’s interests and skills, linked to their personal goals, which enable the expression of identity and dignity (Tierney & Beattie, 2020).
Current services, both in community settings and residential resources, are mainly compensatory in nature (OEQ, 2016) and offer few opportunities to maintain or enhance participation in meaningful activities (Nott et al., 2020). As a result, people living with MNCDs rarely can use their preserved cognitive capabilities to accomplish these activities that once were part of their routines (e.g., watering plants, playing cards, and setting the table). While participation in meaningful activities increases quality of life (Levasseur et al., 2014; Raymond et al., 2008; Townsend & Polatajko, 2007), deprivation decreases opportunities for social interaction (de Medeiros et al., 2020). Moreover, the limited quantity and quality of opportunities to perform meaningful activities can contribute to the development of reactive behaviors (Logsdon et al., 2007).
To prevent this restriction of opportunities to perform meaningful activities, four cognitive strategies (CSs) can support people living with MNCDs in learning or maintaining the performance of meaningful activities: (1) errorless learning, (2) motor encoding, (3) spaced retrieval, and (4) vanishing cues (Choi & Twamley, 2013; Crowe & Gabriel, 2013; Van der Linden & Juillerat Van der Linden, 2004). These CSs rely on the cognitive capabilities generally preserved in people living with MNCDs, namely, procedural memory and implicit retrieval processes (De Wit et al., 2021). These focus on the automation of correct action sequences during learning (errorless learning and motor encoding: Clare et al., 2000; De Werd et al., 2013), the gradually spaced repetition of these sequences (spaced retrieval: Bier et al., 2008; Lipinska & Bäckman, 1997), and the progressive reduction of motor, visual, and verbal cues provided during their performance (vanishing cues; Bier et al., 2006). For example, for a person living with an MNCD who forgets to take their medication after each meal, the application of cognitive strategies could look like this: (1) When the person finishes their meal, guide the person to the pill organizer while holding their hand (motor cue), show them the pill organizer (visual cue), and tell them to take their medication (verbal cue). (2) Repeat the action several times, immediately after each meal, increasing the interval between repetitions, while providing sufficient cues to help them successfully take the medication. (3) Gradually reduce the cues given as the person progresses in learning the correct sequence of action, until the person doesn’t need any more cues or until the satisfactory independence level has been consolidated. Several studies have demonstrated that these CSs can help maintain autonomy in targeted activities for several months after the end of interventions (Cherry et al., 2009; Clare et al., 2001; Clare & Woods, 2004; Déry et al., 2019; Thivierge et al., 2014).
Although CSs show promise
Objective of the Study
This study aims to document the facilitators and barriers to the use of CS with people living with MNCDs housed in SR from the perspective of care staff. The Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2022) was used to develop the interview guide to monitor the implementation of CS by the care staff, who were remotely coached by an occupational therapist from the research team.
Methods
Design
This study was conducted within a participatory action research design, using a descriptive exploratory qualitative approach (Creswell, 2018). Participation action research was chosen for its emphasis on collaboration and change, allowing the SR’s staff to actively participate in shaping the intervention and ensuring its feasibility (MacDonald, 2012). The descriptive exploratory qualitative approach enabled the capture of rich and in-depth understanding of participants’ experiences (Creswell, 2018). It was carried out between October 2021 and February 2023 in collaboration with an English-speaking SR located in Quebec. This SR is distinguished by its home-like environment and a mission focused on humanistic approach and personalized care. The facility accommodates a total of 120 residents in four units offering different levels of care to meet a wide range of needs. The study took place in one of these units, which specializes in services for people living with MNCDs.
The partnership between the research team and the SR originated from a request by the SR, which sought to ground its practices on evidenced-based approaches in order to offer the best possible care to its residents. Several meetings between the research team and the SR’s management led to the development of multiple research proposals, including the present participatory research project. Since then, bi-monthly meetings involving nurses and the care director have been ongoing. Occasionally, on-site visits are also conducted to support and participate in the implementation process. Throughout the project, the research team has continuously developed CS-related tools tailored to staff needs. A steering committee, including the physician, pharmacist, care director, and two family caregivers, was formed. The committee contributed to the project design, validated the interview guide, and assisted with the study planning.
Recruitment
The principal investigator (female occupational therapist, PhD) and an occupational therapist with expertise in the application of CS working in the research team collaborated with the SR’s care director and recreation manager for the recruitment of residents. The SR’s care director and recreation manager often knew the resident for multiple years and were often in contact with the resident’s family, so they had a good understanding of the person’s preserved cognitive capabilities, their current cognitive difficulties or behavioral challenges, and their lifestory, including possible meaningful activities. With this information, the four researchers and SR’s team members used a purposive sampling method to identify which residents were likely to benefit from the CS intervention and to determine a meaningful activity for each resident. Ten seniors living with a major MNCD and facing challenges in engaging in meaningful activities (e.g., playing the piano, using the radio to listen to music, eating, and dressing) were identified. Because meaningful activities can sometimes prevent reactive behaviors, each case was reviewed jointly by the care and research teams to determine whether including a specific resident might help reduce such behaviors. Therefore, reactive behaviors (e.g., aggressivity) were not used as a systematic exclusion criterion. The SR’s care director would explain briefly the study to the resident and the family members (if they were involved), and then a member of the research team would contact them to sign the consent form at the SR.
The Course of the Study
For each selected resident, all staff members involved in their care were invited to a personalized training session of approximately 90 minutes. The initial training, delivered by the research team’s occupational therapist, addressed the following elements: (1) MNCD and its evolution; (2) the basic approach (Rey, 2017; Voyer et al., 2009) to adopt with people living with MNCDs (e.g., communication, validation, and diversion strategies); (3) the approach in the event of refusal of care; (4) principles of CS application (errorless learning, motor encoding, spaced retrieval, vanishing cues); and (5) operationalization of CS for each resident’s specific objective. The personalization of the training was based on discussion about the residents’ life history (i.e., is the objective associated to past interests, happy memories, and habits?) and daily routine (i.e., when was the activity usually performed? With whom?). The SR’s care director had previously explained the study to the staff members and invited them to the training. The occupational therapist giving the training explained the study in more detail and had them sign the consent form.
After the first three residents’ training sessions, subsequent sessions were shorter (the last ones lasted about 45 minutes) as the staff had gained familiarity with the CS. Thus, the focus shifted mainly to the last element, tailoring their application to each resident’s specific objective. The initial version of the training was first delivered to the staff and adjustments were made progressively to personalize the operationalization of the CS to each selected resident, ensuring applicability. This iterative process also allowed the training to be continuously refined based on staff feedback and questions during meetings. This way, the training was developed collaboratively, with the research team providing expertise and the staff contributing with practical experience and contextual knowledge.
With few exceptions due to illness or personal events, nearly all staff involved in direct care for the selected residents participated. As a result, the subgroup of trained care staff varied slightly between residents, approximatively ten staff members, from eight to sixteen. Most of them were involved in multiple training sessions. To facilitate participation of staff members, the training was given in person, at their place of work, and was strategically timed between work shifts so staff members could either participate before or after their usual tasks.
The form and frequency of staff involvement varied according to the targeted clinical objective (e.g., at mealtimes and during hygiene care), and the intervention plan was built accordingly. The implementation period for each resident ranged from 26 to 154 days, with some interventions interrupted due to COVID-19 isolation, hospitalization, or intercurrent illness. This period encompassed identifying the resident and their meaningful activity objective, scheduling and delivering training sessions and interventions to maximize staff attendance, integrating CS into the daily routine to learn the meaningful activity, adjusting strategies to daily routine and to include life history elements, and conducting staff interviews to assess facilitators and barriers. Although care staff members were expected to complete logs of intervention frequency and duration, these logs were not consistently maintained. Staff reported that staffing shortages and turnover constrained their schedules. However, the care director and recreation manager reported that day staff typically applied CS during nearly every interaction related to the selected objective, whereas evening and night staff rarely did. Therefore, unlike typical research projects where space retrieval is implemented systematically, in this study, space retrieval was rarely implemented; CSs were integrated only during the times when the meaningful activity usually occurred. Consequently, frequency varied by activity, ranging from once a day (e.g., CD sorting each morning waiting for husband to get up) to several times a day (e.g., playing piano after each meal).
Both the SR’s care director and recreation manager participated to bimonthly 30 minutes support meetings throughout the study. They first informally consulted the staff on their needs and challenges associated with trainings, intervention, or data collection, which were then addressed during the meeting with the principal investigator and the occupational therapist. The research team also provided video capsules (Laboratoire d’optimisation cognitive de l'Université de Sherbrooke (LOPCUS) - Université de Sherbrooke) accompanied by communication sheets summarizing key information about CS (cf. Appendix 1). The communication sheets were available in a binder at the nursing station, where staff members could read the full description on how to apply personalized CS for each resident. These videos were sent by email and shown twice in the workplace during sessions open to all staff involved. To help disseminate the intervention plan among team members, the research team developed a follow-up grid for each resident, which included a synthetic reminder of the objective and interventions examples. A designated staff member was appointed to ensure continuity of the intervention, proactively address challenges, and motivate the team. This person collaborated with the research team to develop new tools to support CS implementation.
For each resident, once the objective related to his or her meaningful activity was achieved, meaning they had learned, integrated, and automatized the sequence of actions for the chosen meaningful activity, as confirmed by the care team working with that resident, the care director invited care staff to participate in individual interviews. Participants were informed of the researcher’s professional role and the aims of the study. Only staff members who had worked directly with the selected residents were eligible. A purposive sampling strategy ensured representation by role (e.g., nursing staff, beneficiary attendants, and recreation workers) and work shift (day, evening). Care director and recreation manager also considered staff attitudes toward CS, inviting both those generally receptive and those more reticent, based on observations and staff comments during team meetings. No staff members refused to participate or withdrew from the study.
To facilitate implementation, comments and suggestions from interviews were used throughout the study to develop tools supporting staff. For example, if a staff member suggested modifications to address a specific barrier, the team created a corresponding tool, resulting in enhanced training and more tailored resources for care staff during the project. For example, to address a barrier related to the dissemination of the training to all staff members, we developed the training capsules and a synthetic memory aid for the application of personalized CS for each resident which was printed and placed in a common work desk for consultation.
Data Collection
As the study progressed, the 20 care staff involved participated in semi-structured individual interviews lasting approximately 30 minutes. Each participant was interviewed once; interviews were conducted either in person at the residence or via Microsoft Teams. An interview guide, developed by the research team based on the CFIR, had been pilot tested and validated by the steering committee. Following individual interviews with the care staff, a group interview was conducted with the care director and recreation manager to obtain an in-depth perspective on facilitators and barriers, including those related to work organization and the SR’s care context. Individual and group interviews were conducted by three research assistants who were not involved in the training or in the intervention process. They were all research students, so their interest in the research topic was acknowledged, and reflexive strategies were employed to address potential biases. All interviews were recorded and transcribed verbatim. Field notes were also taken during the group interview. The transcripts were not returned to the participants.
Analysis
Thematic analysis was conducted on the transcripts using an iterative process (Ritchie & Lewis, 2014). A coding tree was constructed using both deductive and inductive approaches and based on CFIR. This coding tree was also informed by the structure of the individual interview guide as well as the content of the interviews (e.g., external context, internal context, individuals, innovation, facilitators, barriers, and perceived effects of CS). Additional themes were added inductively as they emerged from the data. Through several iterative loops, the coding tree was revised to incorporate and group new themes as the analysis progressed. Microsoft Word tables were used for thematic coding, which facilitated blind co-coding, comparison, and validation of the codes. To ensure validity and credibility, all interviews were independently coded by three research team members, who then met to compare results, resolve discrepancies, and clarify specific codes. Data saturation was deemed sufficient as no new themes were identified in the final stages of analysis.
Results
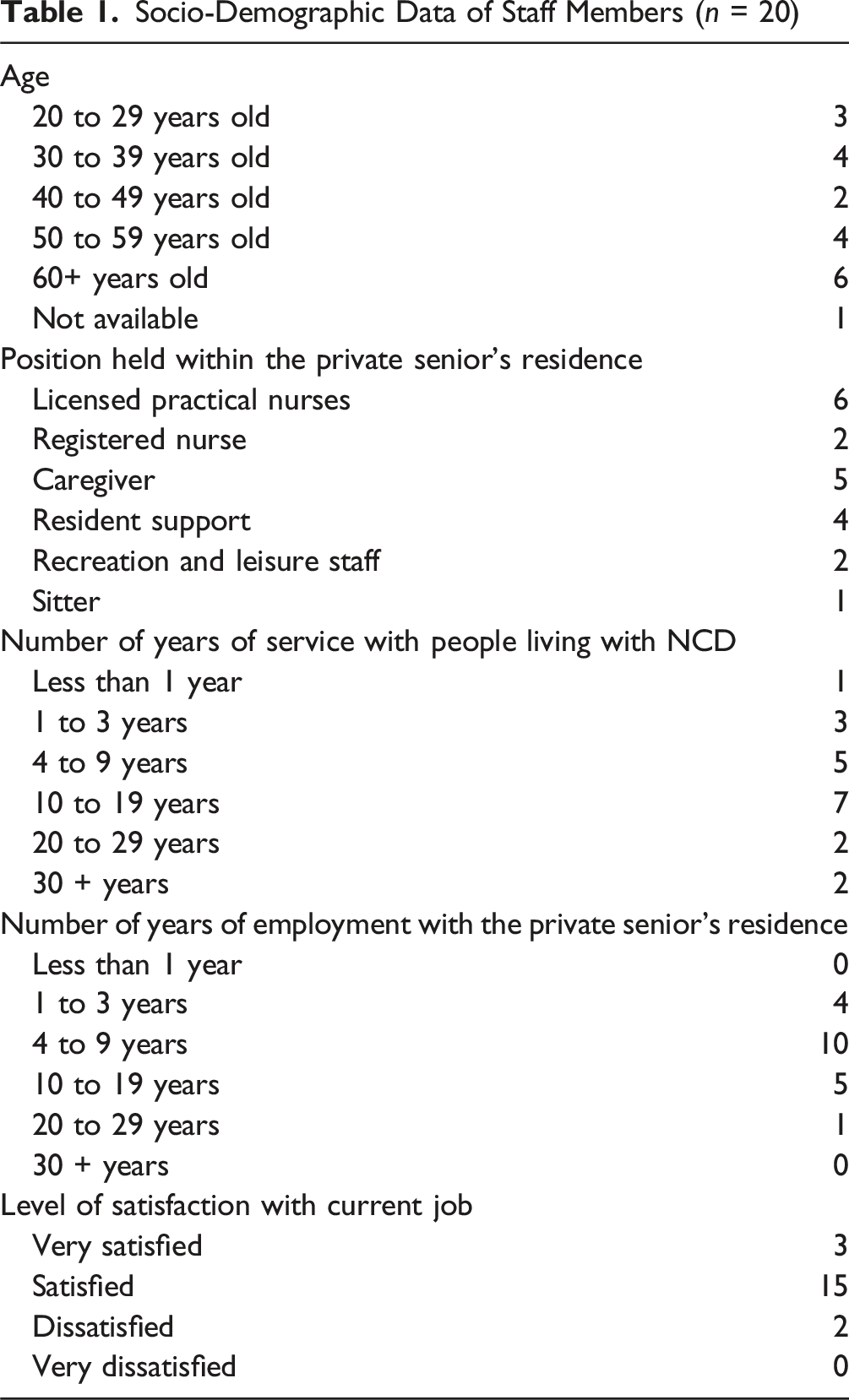
Participants
Socio-Demographic Data of Staff Members (n = 20)
Facilitators and Barriers
The facilitators relating to the use of CS reported by the care staff corresponded to four main themes: (1) personalized approach anchored in the life history of the person living with an MNCD; (2) awareness, concertation, and commitment within the team of care staff; (3) congruence with organizational values; and (4) calm, familiar environment, reminiscent of the feeling of being “at home.” The main themes relating to barriers reported from the care staff’s point of view were (1) deteriorating health and rapid progression of the MNCD; (2) inconsistent application of CS due to staff shortages and turnover; and (3) disparity between organizational decisions and clinical realities.
Facilitators
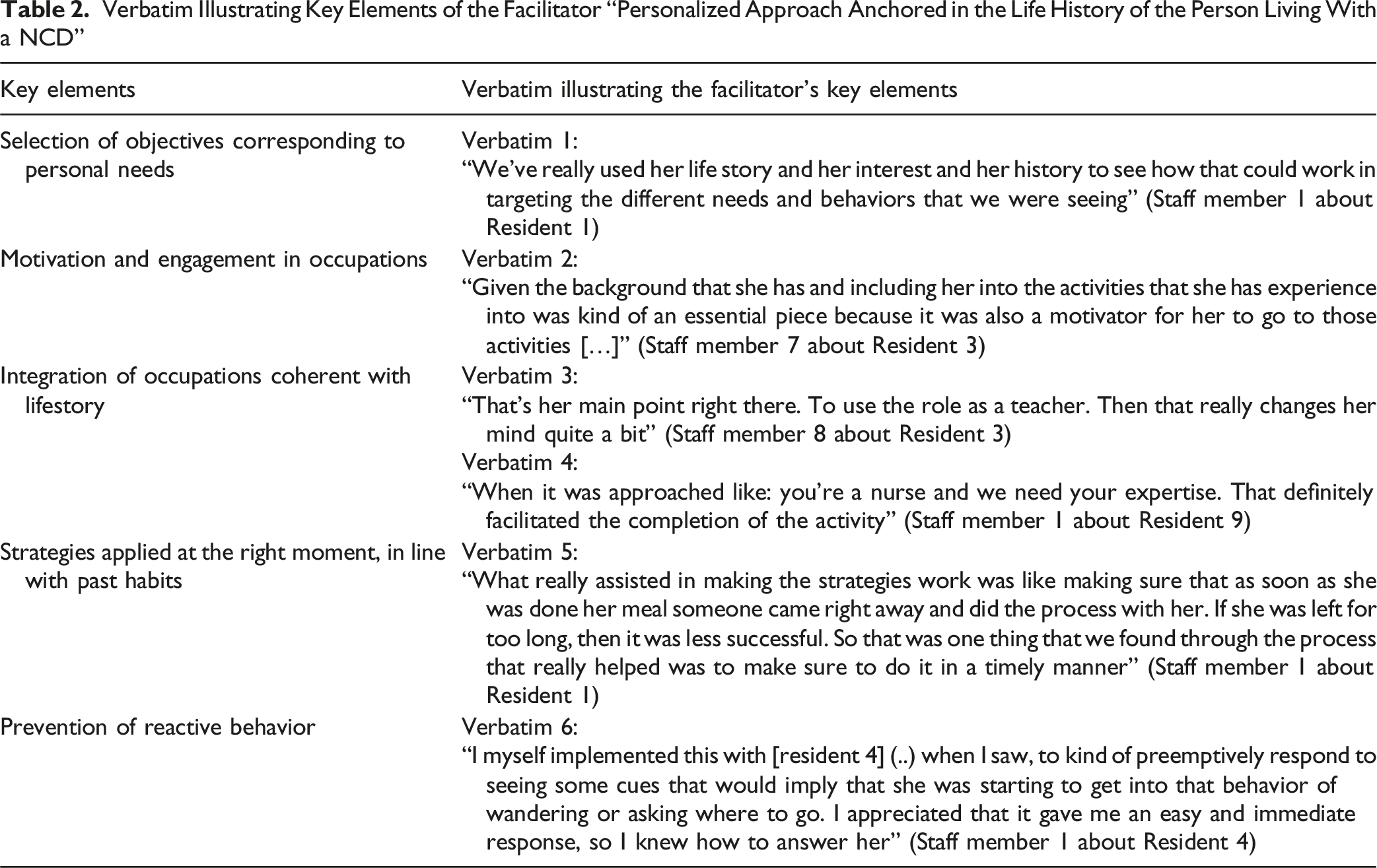
Personalized Approach Anchored in the Life History of the Person Living with an MNCD
Verbatim Illustrating Key Elements of the Facilitator “Personalized Approach Anchored in the Life History of the Person Living With a NCD”
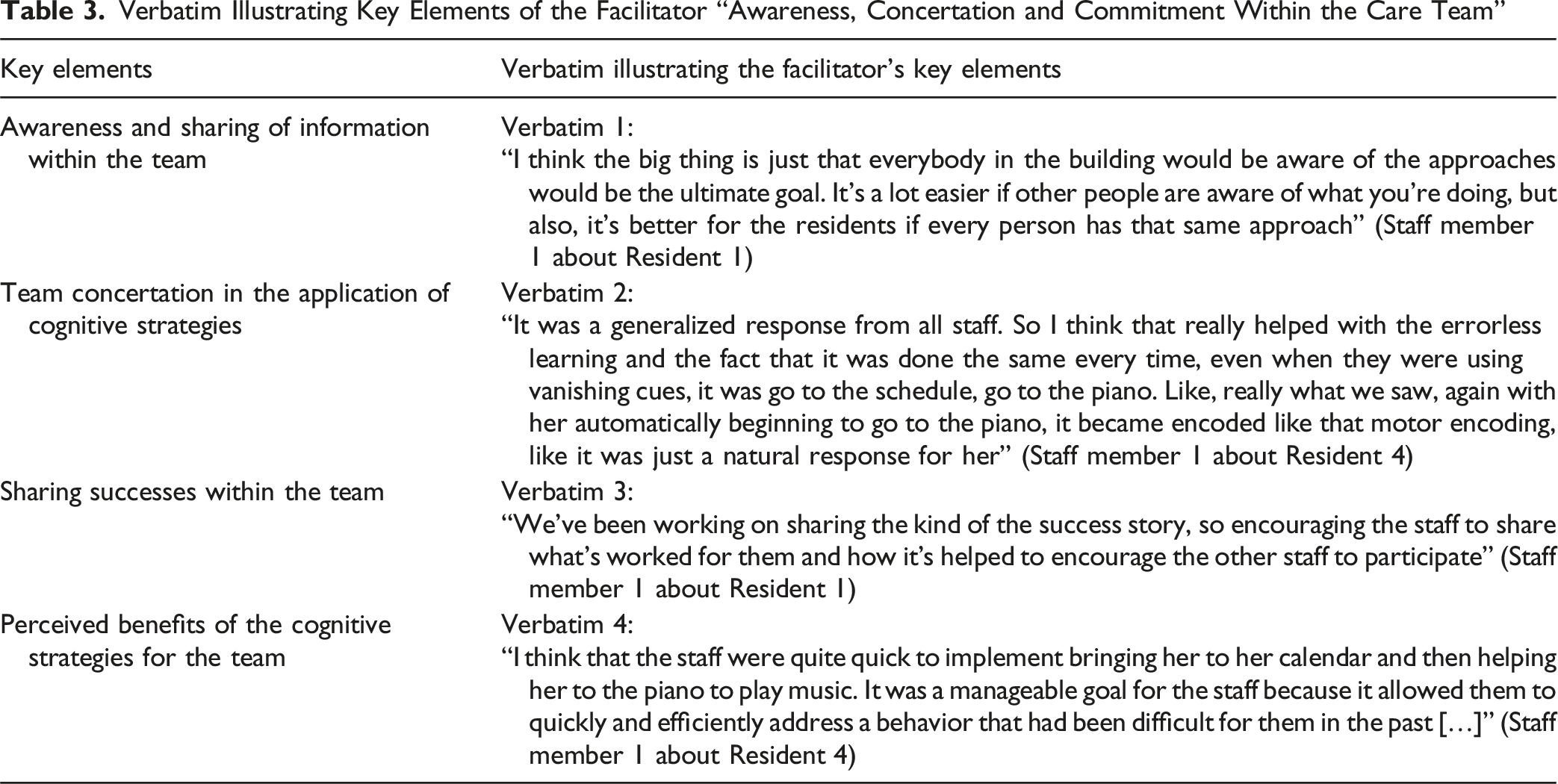
Awareness, Consultation, and Commitment within the Care Team
Verbatim Illustrating Key Elements of the Facilitator “Awareness, Concertation and Commitment Within the Care Team”
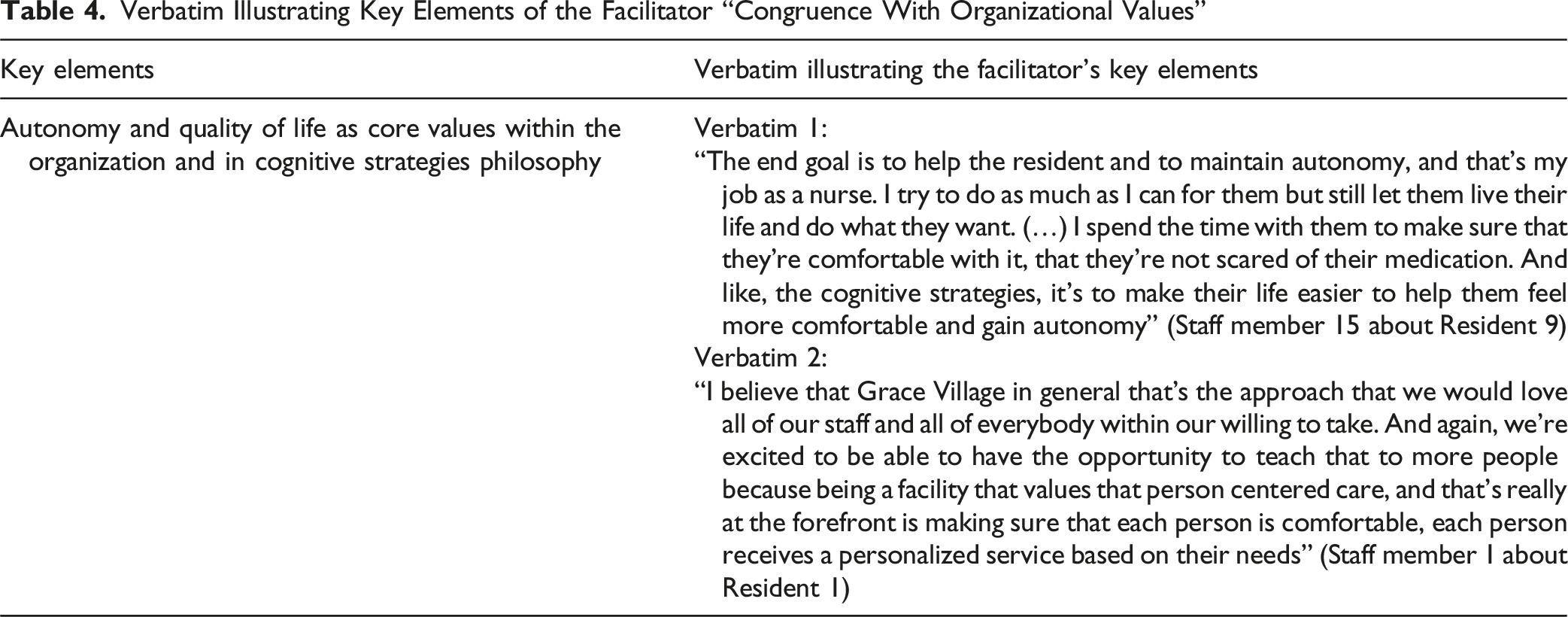
Congruence With Organizational Values
Verbatim Illustrating Key Elements of the Facilitator “Congruence With Organizational Values”
Calm and Familiar Environment, Reminiscent of the Feeling of Being “at Home”
Verbatim Illustrating Key Elements of the Facilitator “Calm and Familiar Environment, Reminiscent of The Feeling of Being ‘at Home’”
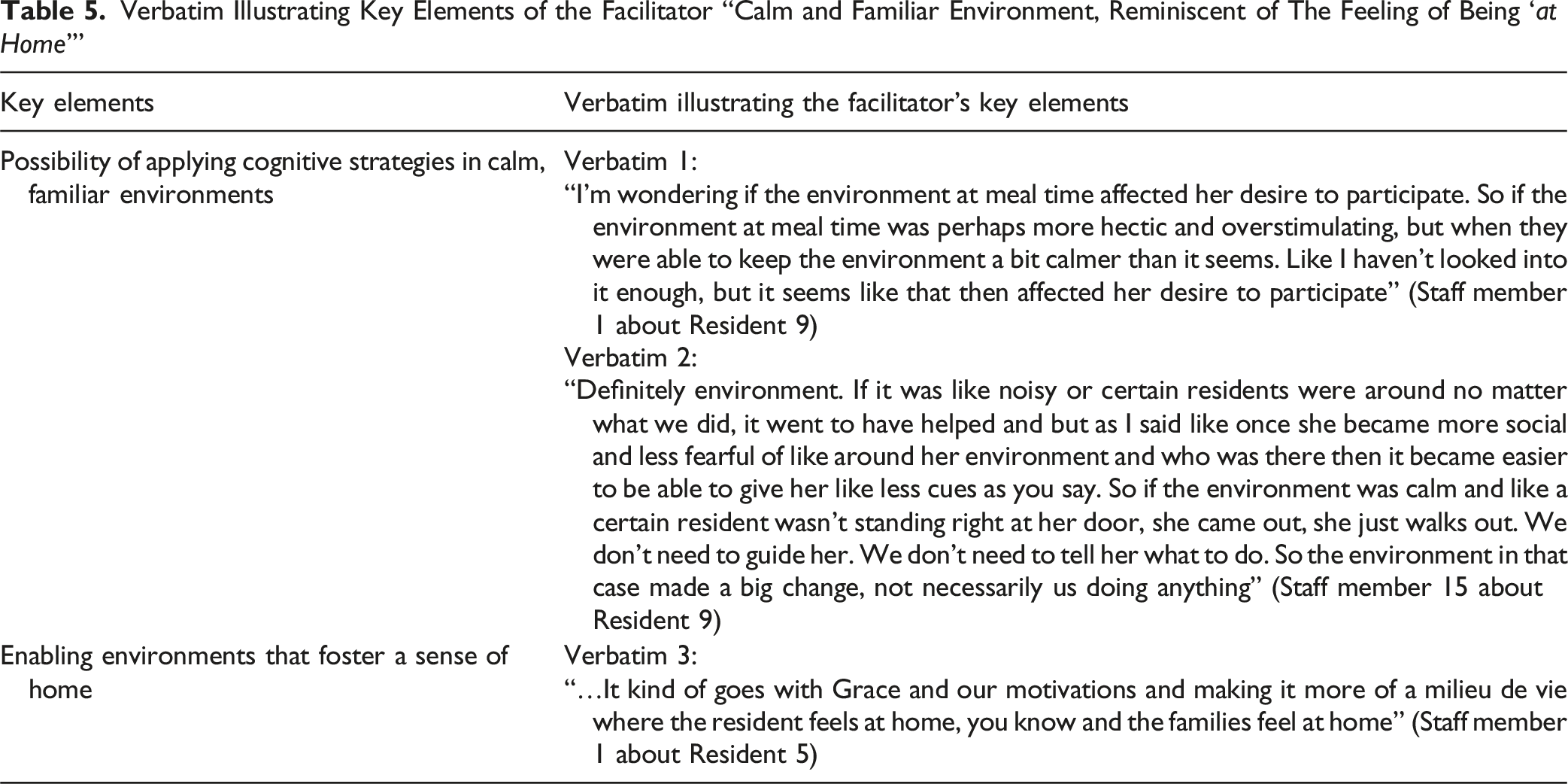
Although not directly mentioned, the facilitators mentioned by the staff seem to refer to the work organization in this residential facility.
Barriers
Deteriorating Health and Rapid Progression of the MNCD
Verbatim Illustrating Key Elements of the Barrier “Deteriorating Health and Rapid Progression of the NCD”
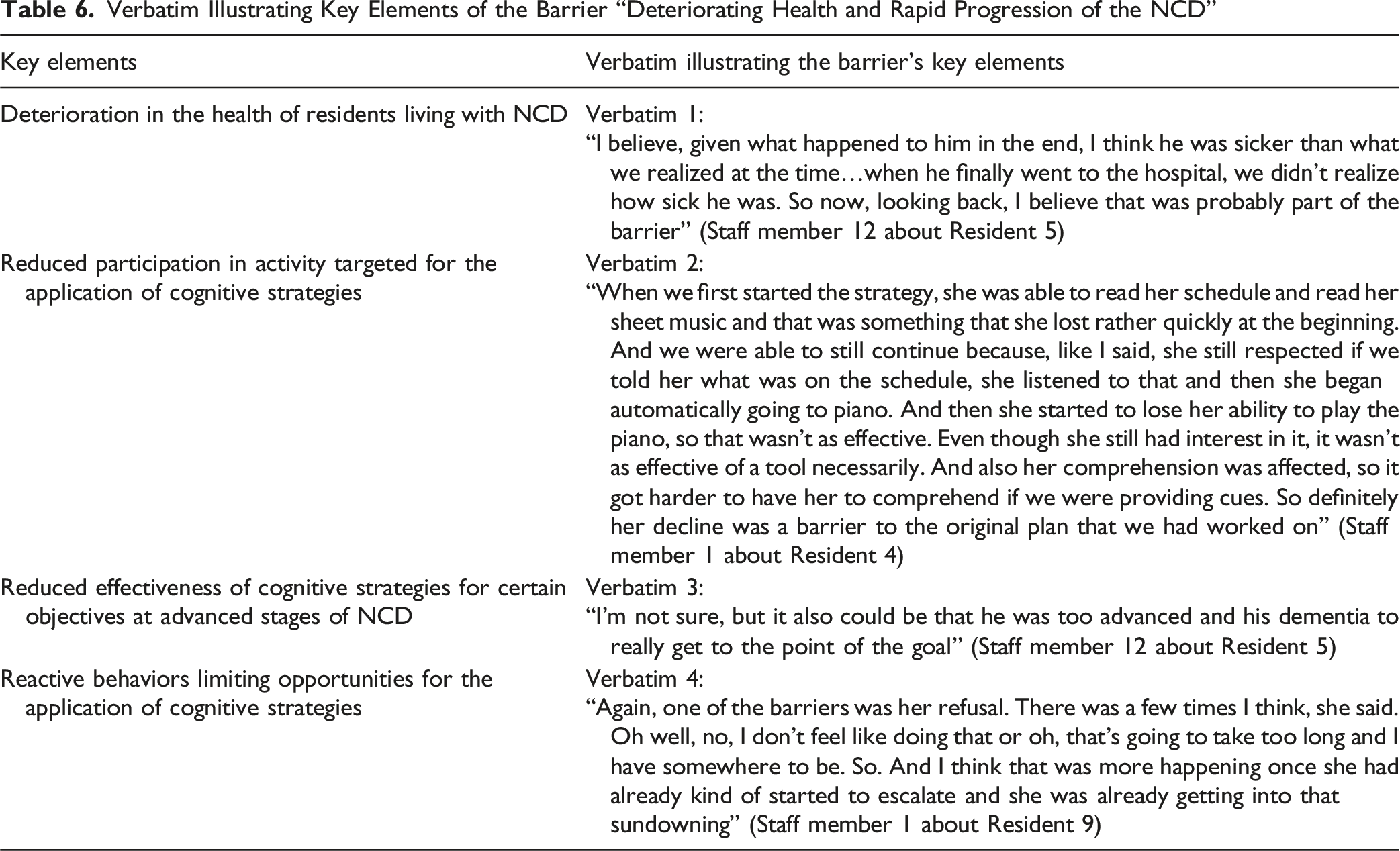
Although coaching was available on request and provided during bimonthly meetings, staff sometimes had already ceased an intervention with a resident before adjustments could be discussed. When MNCD progression reaches more advanced stages, it seems that the effectiveness of CS is further compromised if the activity is not sufficiently simple (see Table 6, verbatim 3). In addition, the progression of MNCDs frequently occurs at the same time as an increase in reactive behaviors, including a reduction in collaboration during interventions, which may reduce the opportunities for applying CS for certain types of goals, or even diminish their scope. This situation illustrates this barrier: “Again, one of the barriers was her refusal. There was a few times I think, she said. Oh well, no, I don’t feel like doing that (…). I think that that was more happening once she had already kind of started to escalate and she was already getting into that sundowning” (Staff member 1 about Resident 9).
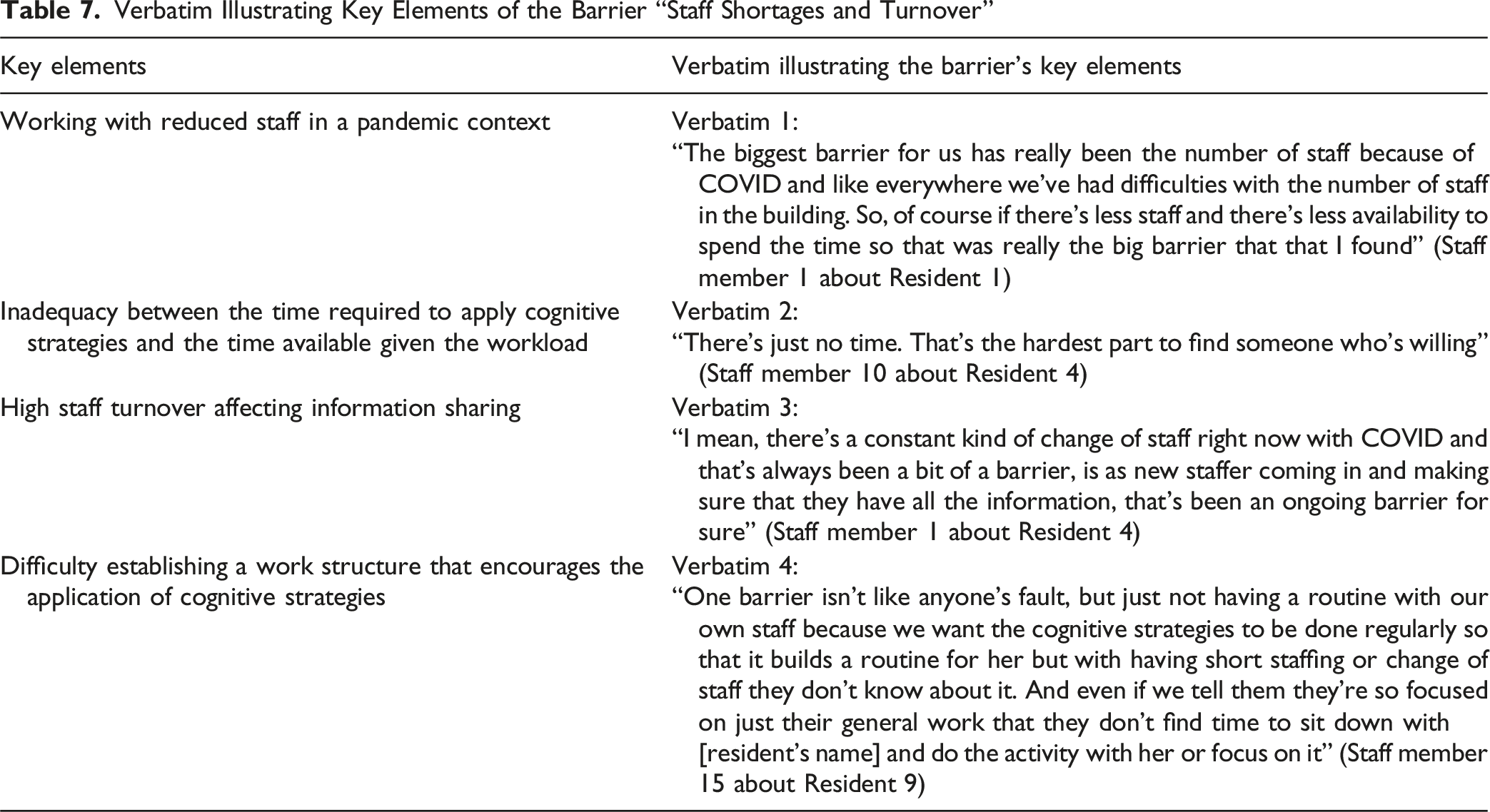
Inconsistency in the Application of CS Related to Staff Shortages and Turnover
Verbatim Illustrating Key Elements of the Barrier “Staff Shortages and Turnover”
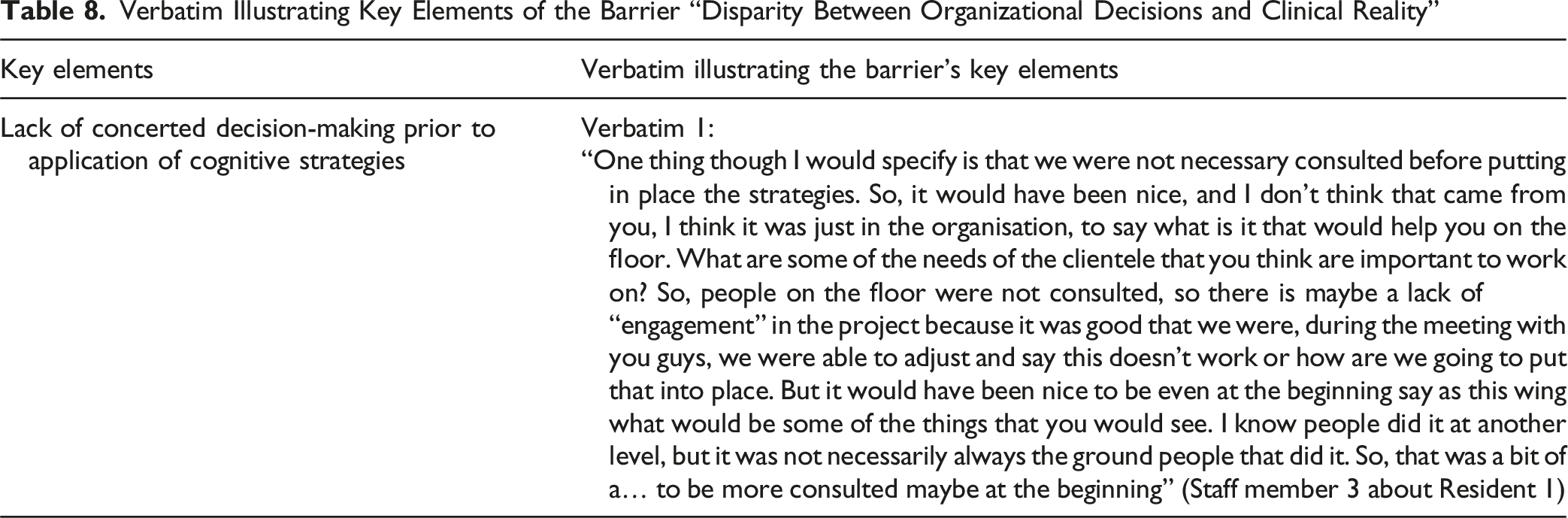
Disparity Between Organizational Decisions and Clinical Reality
Verbatim Illustrating Key Elements of the Barrier “Disparity Between Organizational Decisions and Clinical Reality”
Discussion
The present study documented the facilitators and barriers to the application of CS with people living with MNCDs in an SR. The main results indicate that the adoption of a person-centered approach facilitates the selection of relevant personal objectives related to the engagement in meaningful activities and commitment to the interventions offered. However, sometimes, a rapid evolution of a health condition or the presence of reactive behaviors (e.g., wandering and aggressivity) may compromise the achievement of targeted goals
One approach that optimizes success in achieving the target objective with CS is to personalize it for the person living with an MNCD. This requires setting objectives adapted to preserved capabilities, as the progression of MNCDs leads to a gradual decline in cognitive functions and autonomy in daily activities (Dubbelman et al., 2020). Consequently, care staff applying these CSs must be attentive to this evolution, to adjust the initial objective when it becomes incompatible with the person’s preserved capabilities. This finding is consistent with Khayum and Wynn’s (2015) study, which indicates that CS used with people living with MNCDs must continually be adapted as the disease progresses and needs change. Furthermore, based on our results/one of the facilitators, personalizing intervention also involves selecting meaningful goals that will be consistent with the person’s values and interests. For this reason, it is essential for care staff to be sensitive to the habits, activities enjoyed, and roles occupied throughout life, so that they can be considered when setting treatment goals (Jogie et al., 2021). Using life history elements is essential both for setting relevant goals and for determining the appropriate moments to implement them. In fact, incorporating life history fosters positive interactions and should be prioritized when working with people living with MNCDs (Cooney & O’Shea, 2019). In a residential setting, the daily involvement of care staff with residents encourages the acquisition of such life history knowledge. More specifically, the SR in which the study took place is part of a small community where care staff have sometimes known the residents for many years, prior to their arrival at the SR. This closeness gave staff deep knowledge of residents’ family, careers, hobbies, and personality traits, which likely facilitated the adoption of a person-centered approach rooted in life history and the establishment of personalized, meaningful goals. In contexts where staff do not have this prior knowledge, it is essential to develop systematic ways of gathering life history (Davies et al., 2022).
To ensure the consistent application of CS, the sustained and concerted involvement of care staff is essential. Indeed, close support during the early learning phases is critical to proactively prevent errors, as their occurrence may compromise intervention success (Clare et al., 2000; De Werd et al., 2013). In a residential environment such as an SR, care staff are always on hand to respond to the needs of residents, which is an asset for the regular and timely application of CS. Compared with the home environment, the person may be alone for part, or even all, of the day, and so may not always have access to the support needed to apply the CS properly. This distinct advantage of the residential setting may also explain why many of the residents targeted in this study were able to achieve the intervention objectives initially set to engage in meaningful activities, or at least partially, even though they were in moderate to advanced stages of the disease. The constant presence of a team ensures that the sequence of actions required to learn a meaningful activity is consistently followed, which aligns with the principles of errorless learning (Clare et al., 2000), and this supervision in the first phases of learning is a great advantage in this type of residential setting. However, to be effective, CS must not only be applied regularly but also consistently by all team members. Indeed, frequent staff changes across shifts and high turnover rates remain significant barriers to successful implementation of new interventions (Coffey et al., 2021).
In addition to ensuring consistency in the application of CS to meaningful activities, to ensure effective implementation and long-term sustainability, a new clinical or organizational practice must offer appropriate training to members of the care team (Shanbhag et al., 2018). Given the presence of several barriers, participatory action research is particularly relevant, as it allows for continuous adjustment of tools to reduce these barriers through concrete and simple means, such as four-step cue sheets to operationalize CS according to each resident’s personal objective. The involvement of all stakeholders is essential to foster organizational structure that supports the integration of innovative practices (Massuard, 2023).
The COVID-19 pandemic exacerbated the already known phenomena of absenteeism among care workers (Statistique Canada, 2023), creating difficulties in training all staff, including new care staffs, and in ensuring efficient communication. Guidelines for implementing innovative clinical and organizational practices stress the importance of identifying communication strategies and involving champions throughout the process (Massuard, 2023). The designation of a resource person was identified as an effective method for ensuring continuity of intervention, proactively resolving challenges, and motivating the team during the intervention process. This promising solution would certainly benefit from further experimentation.
Even though no “champion” was designated within the team, the care staff who took part in this study benefited from ongoing support of an occupational therapist with expertise in the application of CS. Occupational therapists are professionals who may be called upon to use these CSs to maintain skills and compensate for disabilities, to promote optimal autonomy (OEQ, 2020). Given that occupational therapy services across Canada are expected to fall short of demand by 2028 (Employment and Social Development Canada, 2020), it seems unrealistic that these professionals should be systematically deployed in residential settings to apply CS to people living with MNCDs. However, this study has shown the feasibility of applying CS by non-therapeutic staff, mainly care staff and nursing assistants. In fact, through individual or group support meetings with the occupational therapist, the care staff were able to apply CS appropriately and resolve the difficulties experienced during the intervention.
At first glance, CS interventions may appear as an additional burden on the already demanding daily workload of care staff. Indeed, this type of intervention requires increased intensity and considerable mobilization of care staff during the early phases of learning. As a result, in some cases, an impression of overload may be felt. However, in some cases, such as demonstrated in various studies, the application of CS maintains the autonomy of people living with MNCDs (Cherry et al., 2009; Clare et al., 2001; Clare & Woods, 2004; Déry et al., 2019; Thivierge et al., 2014). Improved independence in certain daily activities could ultimately reduce the number and duration of care staff interventions. A systematic review of economic evaluation of cost-effectiveness of non-pharmacological interventions including cognitive, multicomponent, and occupational therapy interventions for mild cognitive impairment and dementia realized by Eaglestone and colleagues (2023) in community settings and residential care settings shows good evidence of cost-effectiveness. Thus, the time initially invested in applying CS could translate into future time savings. Moreover, engaging residents in meaningful activities tailored to their preserved capabilities can reduce reactive behaviors, such as agitation (Klinedinst et al., 2024), which are associated with emotional distress, injuries, absenteeism, and burnout among staff (Lyons & Champion, 2022). In a context of staff shortages, this argument may be persuasive to managers and care staff who question the feasibility of integrating CS into their daily responsibilities.
To the best of our knowledge, this study is the first to explore the facilitators and barriers to the application of CS in a residential care context, laying the groundwork for their current use and relevance. One of the study’s strengths is its participatory action research methodology, which allowed the team to anticipate challenges and adapt the process in real time based on the lived experiences of staff and managers. Another strength is the rigorous process used for thematic analysis involving codification of qualitative data. However, this study also includes some limitations. First, the implementation of CS in real-life setting, especially during the pandemic, impacts the planed data collection. Although staff were initially expected to complete grids tracking intervention frequency, duration, and progression, this was not feasible; instead, the occupational therapist from the research team recorded estimated times during meetings with care staff according to the description they gave. Another limit was the inconsistency in the implementation phase, partly due to staff turnover. This inconsistency, often present in real clinical settings, impacts the principles of CS. Finally, the planed quantitative grid to follow the evolution of behaviors was not completed by staff. Thus, only qualitative data were available to document the changes in residents’ mood and behaviors. Further studies in diverse care contexts, such as hospitals or community settings, would be relevant to provide a better understanding of how the application of CS is operationalized (e.g., types of goals and people involved in application) and to compare factors facilitating or limiting the implementation of CS (e.g., profile of people living with MNCDs and available resources) in several contexts.
Conclusion
In context of implementing CS in SRs, this study identified several facilitators, including the concerted selection of meaningful objectives for the resident, the collaboration and shared knowledge of the interventions among care staff, and the alignment between the values advocated by the SR and those underlying the CS. Conversely, the resident’s rapid deterioration, inconsistency in the sequence of action in the learning phase related to high turnover, and lack of staff were identified as barriers to the implementation of CS. The results therefore show that it could be possible to apply CS in long-term care settings when the care team is supported by adequate training and coaching, even without the constant presence of an occupational therapist at the SR. This finding is encouraging, as it paves the way for the democratization of CS. Indeed, if they were applied by those providing day-to-day care, this would enable a greater proportion of people living with MNCDs to benefit from them. Future research should explore the implementation and factors essential to foster sustainability of CS in other contexts along the continuum of care and their cost-effectiveness.
Supplemental Material
Supplemental Material - Building on Preserved Capabilities of People Living With a Neurocognitive Disorder: Participatory Action Research for the Implementation of Cognitive Strategies in a Seniors’ Residence
Supplemental Material for Building on Preserved Capabilities of People Living With a Neurocognitive Disorder: Participatory Action Research for the Implementation of Cognitive Strategies in a Seniors’ Residence by Chantal Viscogliosi, Sarah Rahimaly, Romane Laplante-Duquette, Khalilah Anderson, Marianne Larin, Claudia Beaudin, Hélène Carbonneau, Yves Couturier, Nathalie Delli-Colli, Jessica Déry, Dominique Giroux, Ariane Grenier, Véronique Provencher, and Sandra Klinck in Journal of Applied Gerontology.
Footnotes
Acknowledgments
We would like to thank the residents and the senior resident’s care team for taking part in this study and Eve Thibeault for the translation of this paper.
Ethical Considerations
This study was approved by the Comité d’éthique du Centre intégré universitaire de santé et de services sociaux de l'Estrie - Centre hospitalier universitaire de Sherbrooke’ (CIUSSS de l'Estrie – CHUS) (approval no. 2021-3822) on September 14th, 2020.
Consent to Participate
All participants provided written informed consent prior to participating.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Partnership Engage Grants from the Social Sciences and Humanities Research Council of Canada (grant number 892-2020-0043).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.