
Abstract
Objectives
Purposeful design of physical settings, including sensorial elements, may enhance participant engagement in psychosocial interventions. Yet, consideration of these settings remains limited. This review mapped evidence on whether and how purposeful physical settings are reported in protocols for group-based psychosocial interventions for older adults.
Methods
Using Arksey and O'Malley’s framework, we searched four databases for protocols of group-based psychosocial interventions for older adults involving in-person sessions.
Results
Of the seventy-five included protocols, only six (8%) explicitly reported physical settings. Author consultation identified an additional 16 protocols, totaling 22 (29%) considering settings such as layout, acoustics, lighting, and thermal comfort. Physical activity interventions in community settings with smaller groups were more likely to report these elements.
Discussion
Underreporting and limited detail on physical settings highlight room for improvement. Intentionally integrating and thoroughly reporting these settings could enhance intervention designs, potentially improving outcomes and replicability of psychosocial interventions for older adults.
• Presents the first systematic review of how purposeful physical settings (i.e., room layout, auditory settings, lighting conditions, and thermal comfort) are reported in published protocols of group-based psychosocial interventions targeting older adults. • Identifies a significant reporting gap: only 8% of protocols explicitly describe purposeful physical settings, increasing to 29% after author consultations, highlighting an overlooked factor important for methodological rigor and replicability. • Reveals that room layout, auditory considerations, and thermal comfort are the most frequently considered purposeful physical settings, yet these aspects are inconsistently and inadequately detailed in protocols, with authors often reporting having considered them despite omitting details from their published protocols.
• Recommends the explicit inclusion of purposeful physical settings in standardized reporting guidelines (e.g., SPIRIT and CONSORT) to improve transparency, facilitate replication, and clarify intervention mechanisms. • Encourages researchers to systematically assess, modify, or isolate physical environmental factors before delivering interventions to enhance older adults’ engagement, attendance, and overall effectiveness. • Advises researchers and policymakers to prioritize detailed documentation of environmental settings in intervention protocols, aligning gerontological research practices with evidence-based environmental gerontology principles.What This Paper Adds
Applications of Study Findings
Introduction
Sensory stimuli provided by physical settings shape how individuals interpret and interact with their environments. Within the servicescape framework, physical settings comprise the immediate, multisensory environment that elicits cognitive and affective responses (Bitner, 1992). We define purposeful physical settings as servicescapes intentionally tailored to the needs, abilities, and preferences of specific user groups, with the explicit aim of supporting desired experiences and behaviors. This perspective aligns with the competence–press view and person–environment (P–E) fit theory, which argues that outcomes are optimized when environmental demands are calibrated to individuals’ abilities and needs; misfit elevates strain and undermines engagement (Edwards et al., 1998). Within this lens, we posit that age-sensitive design choices (e.g., lighting, acoustics, and space layout) reduce press and cognitive/sensory load, and increase perceived fit and comfort, thereby enhancing engagement. In long-term care facilities for residents with dementia, for example, adjustments to spatial layout, wayfinding cues, and sensory stimulation can influence residents’ behaviors and emotional responses, illustrating how thoughtfully designed, age-sensitive servicescapes can modulate engagement and well-being (Chaudhury et al., 2018).
As older adults are projected to constitute nearly one-fifth of the global population by 2050, meeting their complex healthcare and well-being needs is a priority (World Health Organization, 2022). In response, gerontological research has increasingly emphasized psychosocial interventions to extend healthy life years and improve quality of life. When participants are actively engaged, interventions are more likely to produce the intended effects, enhancing the validity and reliability of study outcomes (Treweek et al., 2013). Engagement is often measured through retention rates, session attendance, intervention completion, and adherence to intervention protocols (Amagai et al., 2022).
Participant engagement strategies have largely been behavioral, as summarized by Wong et al. (2021), who grouped 14 strategies into four categories: attitude change via social or individual motivators, burden reduction, and incentives. Facilitator characteristics also support engagement: higher facilitative interpersonal skills (e.g., empathy and rapport) predict better, particularly short-term, outcomes (Anderson et al., 2016).
While these behavioral and interpersonal approaches are well documented, incorporating purposeful physical settings hold promise especially for older adults, who often experience age-related alterations in their senses, mobility and cognition that alter how they interact with their environments (Davis et al., 2016). Older adults may have different sensory thresholds and responsiveness to environmental cues than younger people; therefore, age-sensitive adjustments could optimize engagement in psychosocial interventions (Wahl et al., 2012). Adjusting features such as lighting, acoustics, and spatial layout could help reduce sensory strain, accommodate mobility constraints, and create more inclusive environments, ultimately supporting greater engagement (Day et al., 2000).
Most research examining the impact of physical settings on behavior has been conducted in commercial and economic contexts (e.g., consumer behavior and marketing) (Petit et al., 2016), excluding the lived experience of older adults who are often retired. The spatial arrangement and design of physical objects can impact behavior, particularly for individuals with reduced mobility (Donovan et al., 1994). Air quality and temperature in indoor spaces affect absenteeism, work performance, and job satisfaction (Seppänen & Fisk, 2006). Ambient odors can impact consumers’ purchasing decisions, increase time spent in retail spaces, and enhance brand recall and recognition (Morrin & Ratneshwar, 2003). Casinos often play high-volume, slow-tempo music to create the perception that patrons have spent less time gambling, so that they will gamble for longer (Ali et al., 2016), while hospital patients with natural daylight access have been shown to have shorter stays (Park et al., 2018).
Despite this, investigation of purposefully designed physical settings in psychosocial interventions for older adults has received limited attention. Tailoring environments to older adults’ needs could enhance engagement and intervention effectiveness. Accordingly, this review summarizes evidence on the use of purposeful physical settings in group-based psychosocial interventions for older adults.
Methods
Given the limited literature on purposeful physical settings in psychosocial interventions for older adults, we conducted a scoping review to map and characterize existing evidence and highlight research gaps. We followed the six-stage framework developed by Arksey and O’Malley (2005), while aligning our reporting with the PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews).
Review Questions
The review was guided by two operationalized research questions: (1) To what extent are physical settings reported in protocol papers of psychosocial interventions for older adults? (2) What specific physical setting characteristics are described in these protocols?
Search Strategy
We focused on published protocol papers as these offer detailed information about study context, rationale, objectives, and methods, including the design and settings of the intervention (Moher et al., 2015).
We searched Ovid MEDLINE, PubMed, Web of Science, and Scopus (initial search on 13 Aug 2021; updated on 02 Jul 2024) with no date limits. Search strings combined terms for publication type, intervention, study type, and population. Supplemental Table 3 contains a detailed search strategy description.
Eligibility Criteria and Study Selection
We included protocol papers describing non-pharmacological interventions for adults aged ≥55 years that incorporated at least one facilitated, face-to-face group session. Eligible interventions could involve psychosocial activities (e.g., social engagement and mindfulness), cognitive training, physical activities (e.g., yoga and exercise), or multi-domain programs. We excluded protocols whose primary target population was defined by a specific sensory impairment or neurological/cognitive disorder, and protocols involving pharmacological agents or brain stimulation to focus the review on mainstream psychosocial interventions for older adults delivered in non-specialist environments,. These exclusions were applied to avoid conflating servicescapes in generic psychosocial settings with those in highly specialized clinical or neurorehabilitation environments, where extensive condition-specific environmental adaptations are routinely embedded in care models. After de-duplication, all citations were imported into Covidence (Veritas Health Innovation, nd) for screening. BH screened all titles/abstracts; AW independently screened a random 20%. Both authors then assessed every full text, and disagreements were resolved through discussion, with a third reviewer (PR or NLM) consulted as needed.
Data Charting
We developed a standardized data extraction form based on the PRISMA-ScR guidelines. Two reviewers (BH and AW) independently extracted data from 20% of included studies using the form, refining it through discussion. BH then extracted data from the remaining studies.
Extracted items included the intended population (e.g., gender and health condition), recruitment information, eligibility criteria, intervention type and duration, location, information about group sessions, description of physical settings, planned outcomes, planned strategies to promote engagement, and intervention facilitator information. Regarding physical settings, we extracted information on room layout, ambient temperature, sensory stimuli (e.g., olfactory cues), lighting (e.g., daylight exposure), visual elements (color schemes, materials), aesthetics (art or decorative objects), and auditory factors (noise levels, ambient sounds, music).
Quality Appraisal
Although methodological quality assessment is not required in scoping reviews, we conducted an exploratory appraisal of the included protocols using the 11-item CASP Randomised Controlled Trial (RCT) (Critical Appraisal Skills Programme, 2023). The purpose of this appraisal was to explore, in an indicative way, whether protocols with higher CASP scores were more likely to consider physical settings.
Synthesis of Results
We narratively synthesized findings, combining a quantitative descriptive overview of study characteristics with a qualitative thematic analysis of how physical settings were reported in the included protocols.
Consultation
To extend our mapping and support knowledge translation, we contacted corresponding authors of included protocols to ask whether they had intentionally considered elements such as lighting, noise/music, room layout, or ambient conditions in their interventions and invited them to explain omissions. This aligns with Levac et al.’s (2010) recommendation that consultation should be an integral part of scoping review methodology and allowed us to capture unreported contextual information.
Results
After removing duplicates and conducting title/abstract and full-text screening, a total of 75 study protocols were retained for the final synthesis. A list of the included studies, along with key characteristics and relevant citations, is provided in the supplementary materials. Inter-rater reliability was high (99% during title/abstract screening; 94% during full-text screening). The PRISMA diagram (Figure 1) details the study selection process. PRISMA flow diagram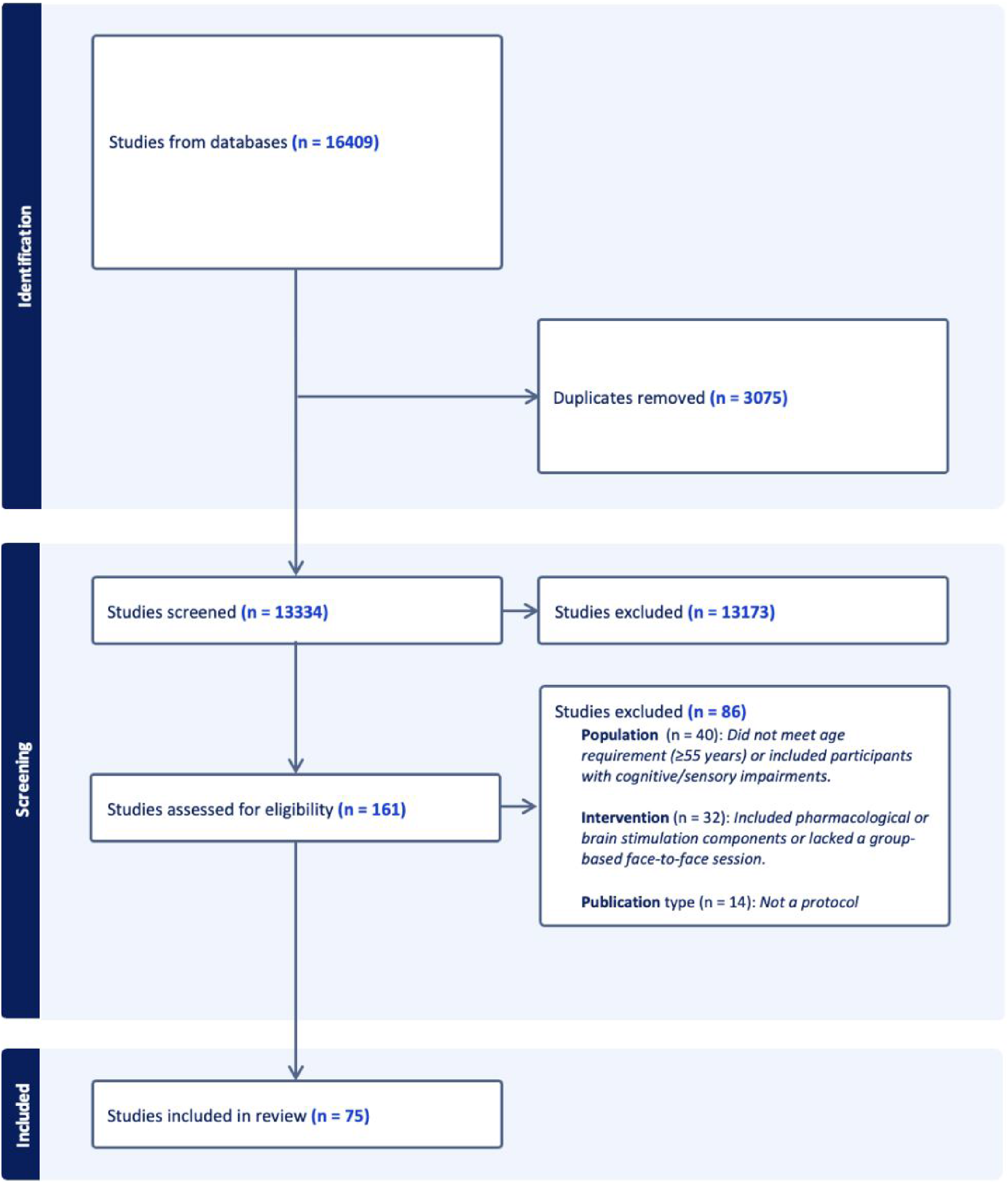
Study Characteristics
Planned Study Characteristics
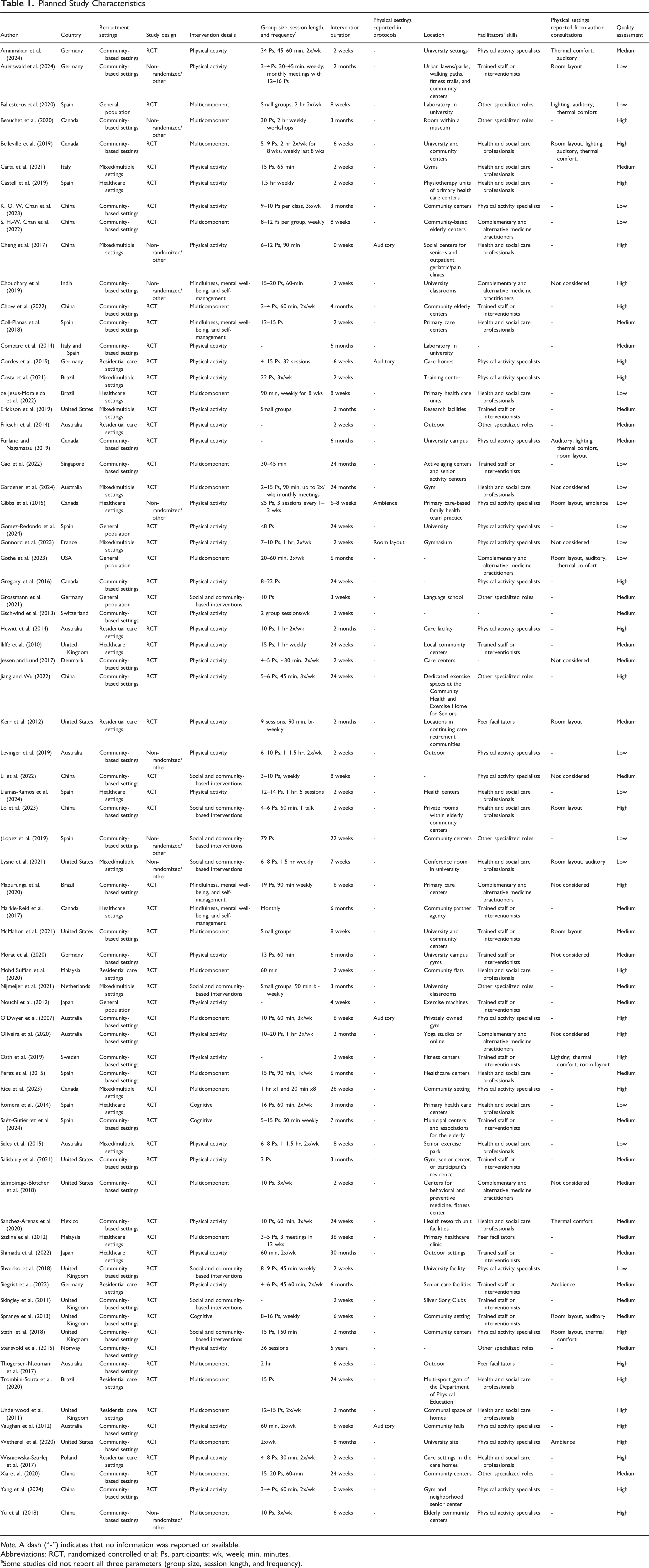
Note. A dash (“-”) indicates that no information was reported or available.
Abbreviations: RCT, randomized controlled trial; Ps, participants; wk, week; min, minutes.
aSome studies did not report all three parameters (group size, session length, and frequency).
Geographical Distribution
Studies were distributed across four continents, spanning 21 countries: Europe (k = 30, 40.0%), Asia (k = 16, 21.3%), the Americas (k = 20, 26.7%), and Oceania (k = 9, 12.0%).
Recruitment Settings
Studies planned to recruit participants from various settings: the community (k = 43, 57.3%), including local community centers and senior activity centers; healthcare settings (k = 9, 12%), such as primary healthcare centers and clinics; residential care settings (k = 7, 9.3%), including nursing homes and retirement villages; general population settings (k = 5, 6.7%), targeting a broad public audience through media or public notices; and mixed/multiple settings (k = 11, 14.7%), which combined community, healthcare, and online sources.
Study Design
Most studies (k = 66, 88%) intended to conduct a randomized controlled trial (RCT), while other studies (k = 9, 12%) proposed diverse trial designs that included non-randomized trials, quasi-experimental designs, mixed methods, and sequential approaches.
Intervention Details
Interventions fell into five primary domains: physical activity (k = 37, 49.3%), social and community-based (k = 9, 12%), mindfulness, mental health, and self-management (k = 4, 5.3%), cognitive (k = 3, 4%), and multicomponent (k = 22, 29.3%). Physical-activity interventions typically combined aerobic, strength, balance, and flexibility exercises (e.g., supervised resistance training, yoga, and community-based programs). Social and community-based interventions used group activities to promote social engagement and reduce isolation (e.g., social clubs, support groups, and participatory art). Mindfulness, mental health, and self-management interventions applied mindfulness-based and cognitive-behavioral techniques and self-management strategies, often in combination with physical or social components. Cognitive interventions used structured tasks targeting memory, attention, and related abilities, whereas multicomponent interventions explicitly integrated elements from two or more of these domains.
Intervention Location
Interventions were intended to take place in various settings, categorized into eight primary types: Community settings (k = 23, 30.7%), academic and research settings (k = 13, 17.3%), healthcare facilities (k = 9, 12%), outdoor spaces (k = 7, 9.3%), other specialized settings (k = 5, 6.7%), gym or fitness centers (k = 3, 4%), care facilities (k = 2, 2.7%), and residential settings (k = 2, 2.7%). The remaining studies (k = 11, 14.7%) did not provide information about the intended intervention location (see Supplemental Table 2 for details).
Planned Outcomes
Intended outcomes of the studies included improving cognitive function (k = 17, 22.7%), physical function and activity (k = 16, 21.3%), mental health, well-being and quality of life (k = 10, 13.3%), or a combination of factors, including physical activity, mental health, and/or quality of life (k = 18, 24%). The remaining studies’ (k = 14, 18.7%) outcomes focused on feasibility and implementation, frailty and falls, cardiovascular health, sleep, pain, mortality, oral health, or social factors.
Purposeful Physical Settings
Six studies (8%) provided information about the planned intervention’s physical settings. Among these, four studies reported auditory considerations. Cheng et al. (2017) specified that interventions would be “conducted in a quiet room,” and O’Dwyer et al. (2007) mentioned using a “quiet room away from the main gym area.” Vaughan et al. (2012) reported that the intervention would involve “freestyle aerobics set to music.” Cordes et al. (2019) reported, “Multicolour equipment and music will be used in an effort to provide a stimulating environment” The other two studies reported on the environment: Gibbs et al. (2015) mentioned the creation of a “home-like environment,” and Gonnord et al. (2023) reported that the group sessions would take place in enriched environments with spatial modifications designed to enhance social interactions and well-being. These environments were created by two specialist associations with expertise in providing stimulating and enriched settings. The remaining 69 protocols (92%) did not provide any information about purposeful physical settings.
Of the 75 authors contacted during the consultation process, 26 (34.7%) responded. Two were authors from the six studies that had explicitly reported purposeful physical settings in their published protocols. One of these authors (Gibbs et al., 2015) confirmed that they had indeed incorporated purposeful physical settings, aligning with their published protocol, whereas the other (Gonnord et al., 2023) stated that purposeful physical settings were not considered, despite being mentioned in the published protocol.
17 of the 26 respondents indicated that they had incorporated purposeful physical settings in their intervention designs. These comprised spatial arrangements, including room layout, encompassing furniture arrangement, spatial considerations for participants, and accessibility features (n = 12); thermal comfort factors, such as temperature and ventilation (n = 8); auditory factors, including noise levels and the use of music (n = 7); lighting conditions (n = 4); and aesthetics and ambiance (n = 3). Some authors indicated that they considered more than one type of physical setting leading to a total greater than 17. These authors agreed that purposeful physical settings might enhance participant engagement, attendance, and retention and influence trial outcomes.
Nine authors clarified that they did not consider purposeful physical settings. Reasons stated for their exclusion comprised unfamiliarity with the concept (n = 6), uncertainty regarding the impact of such settings on trial outcomes (n = 2), belief that these settings would not yield significant differences (n = 1), the notion that the protocol stage was too early for considering such settings (n = 2), unnecessary complexity in the trial caused by purposeful physical settings (n = 4), lack of authority to alter the intervention settings (n = 3), and irrelevance to specific trial objectives (n = 5). Taken together, these reasons portray the physical environment as background context—conceptually unclear, methodologically burdensome, or outside the investigators’ control—contrasting with the view of those authors who treated settings as an active lever for engagement and feasibility.
Combining information from the six protocol papers that mentioned purposeful physical settings with responses from the 17 authors who confirmed such considerations (including one overlap between both sources), 22 out of 75 studies (29.3%) incorporated such settings. Room layout considerations were the most common (13 studies, 59.1%), followed by auditory elements (11 studies, 50%), thermal comfort (8 studies, 36.4%), and both lighting conditions and aesthetics/ambiance (each with 4 studies, 18.2%).
Across the 22 studies that considered physical settings, physical activity interventions predominated: 18 studies (82%) included a physical activity element, encompassing all 6 protocols that explicitly described physical setting considerations and 75% of those clarified via author consultation. Cognitive training components were included in six studies (27%) and educational components in three studies (14%). Most interventions were planned as randomized controlled trials (18/22), with only four using non-randomized designs.
Among the 75 included studies, the proportion reporting physical settings varied by region: the Americas (9/20; 45.0%), Europe (9/30; 30.0%), Asia (2/16; 12.5%), and Oceania (2/9; 22.2%). Within this sample, studies conducted in the Americas were roughly 3.5 times more likely to report physical settings than those conducted in Asia.
Facilitators
Seventy-two studies (96%) provided information on the qualifications and backgrounds of the intervention facilitators. Facilitators often fulfilled multiple roles; therefore, some were classified into multiple role-categories and the sum of categories exceeds the total number of studies. Involvement of physical activity specialists was planned in 27 studies (36%), including exercise instructors, physiotherapists, sports scientists, and personal trainers, many with experience working with older adults. Health and social care professionals were planned in 28 studies (37.3%), including psychologists, occupational therapists, nurses, dietitians, and gerontologists. Trained staff, such as research assistants or personnel explicitly trained for the study, were reported in 16 studies (21.3%). Complementary and alternative medicine practitioners, including yoga instructors, mindfulness teachers, Tai Chi masters, and traditional Chinese medicine practitioners, were planned in seven studies (9.3%). Peer facilitators, such as peer mentors and resident ambassadors, were included in three studies (4%). Other specialized roles, like cultural mediators and language trainers, were reported in four studies (5.3%). Specific training or certification for facilitators was mentioned in 34 studies (45.3%).
Additional Strategies to Enhance Engagement or Behavioral Change
Sixty-six studies (88%) planned strategies intended to enhance engagement or behavioral change in the interventions. The most common approach, reported in 24 studies (32%), was fostering a supportive group environment, which involved promoting group dynamics, social activities, and mutual assistance. Tracking participant progress and providing feedback were planned in 20 studies (26.7%), followed by regular communication, such as reminder and follow-up messages, in 13 studies (17.3%). Intervention personalization, including tailored activity plans and culturally adapted materials, was highlighted in 10 studies (13.3%), as was the provision of educational materials and resources (10 studies, 13.3%). Nine studies (12%) mentioned offering incentives and rewards, such as vouchers or small gifts, while addressing convenience and accessibility was emphasized in nine studies (12%). Varied activities tailored to participant preferences were reported in seven studies (9.3%) and incorporating home-based components in six studies (8%).
Quality Assessment
Twenty-seven studies (36%) were rated as high, 30 (40%) as medium, and 18 (24%) as low quality (Table 1). No association was observed between study quality and reporting or consideration of physical settings.
Discussion
Summary of Key Findings
This scoping review examined how often purposeful physical settings are reported in protocol papers of group-based psychosocial interventions targeting older adults. From 75 protocol papers, we found that only six (8%) mentioned the physical settings of their intended interventions, and this information was limited. In contrast, facilitator qualifications (96%) and engagement strategies (88%) were routinely reported. Through author consultations, we identified additional studies that had considered but not reported purposeful physical settings, bringing the total to 22 studies (29.3%), demonstrating a further gap between the consideration of physical settings and their documentation in protocol papers. Studies from the Americas were more likely to report physical settings as compared to Asia; however, no corresponding pattern was observed with respect to study quality. Studies planning physical activity interventions were more likely to consider physical settings. One possible explanation is the perceived direct link between setting and primary outcomes (e.g., music to enhance motivation) (Karageorghis & Priest, 2012). Physical setting considerations such as room layout, thermal comfort, and lighting conditions were more frequently omitted in published protocols but mentioned during author consultations. Consistent with scoping review objectives, we did not extract or analyze participant outcomes and did not examine correlations between physical-setting parameters and engagement or endpoints.
Consideration and Reporting of Physical Settings
Among the 22 studies that considered purposeful physical settings, room layout was most common, followed by auditory elements, thermal comfort, lighting, and aesthetics/ambiance. While broader literature has shown that these elements influence engagement, behavior, and well-being (Ulrich et al., 2008), none of the protocol papers explicitly provided a rationale for why these design elements were included or excluded. The discrepancy noted in Gonnord et al. (2023), where the published protocol suggested spatial modifications but subsequent author clarification indicated these were not conceived as “purposeful physical settings,” suggests a gap in how authors conceptualize, implement, and report these factors. Furthermore, descriptions of physical settings were brief and lacked details (e.g., music tempo or room acoustics).
Overall, these elements clustered around three overlapping themes: spatial layout and accessibility, sensory comfort, and social atmosphere. This pattern suggests that, when researchers do attend to the physical environment, they tend to prioritize safety and mobility (through layout and space), sensory comfort (temperature, noise, and light), and an inviting social atmosphere (through aesthetics and music), even though these rationales are rarely made explicit in the published protocols.
Why Underreporting Persists
Despite items requiring “settings and locations” in CONSORT and SPIRIT and “where” in TIDieR, widely used templates prioritize human resources and activities over environmental parameters. This is reflected in our findings: facilitator qualifications were almost universally reported, whereas physical settings were not. Physical (e.g., multi-site variation and differences in access to facilities) and pragmatic (e.g., journal word limits) barriers to reporting likely reinforce a perception that the environment is ancillary rather than constitutive of the intervention. Clearer expectations and concise, parameter-based templates may shift this norm.
Importance of Detailed Reporting of Physical Settings
Detailed descriptions of factors such as room layout, auditory conditions, lighting, and temperature in protocol papers might facilitate more accurate replication of interventions by other researchers. SPIRIT items 9 and 11 already require setting and intervention details; applying them fully would improve transparency (Malmivaara, 2019).
Beyond transparency for replicability, reporting physical-setting parameters, as integral components of the intervention servicescape, could inform the mechanisms through which environments influence engagement and outcomes. For example, older adults—particularly those with age-related hearing loss—would benefit from reduced background noise to understand and participate in group interactions (Goossens et al., 2017). Evidence from environmental gerontology and dementia care shows that older adults benefit from higher levels of illuminance and more uniform light distribution than younger adults to support safe mobility, task performance, and visual comfort (Day et al., 2000). Where feasible, protocols should also specify the intended use—or absence—of daylight, which can affect mood, alertness, and readiness to engage in activities (Chaudhury et al., 2018). Thermal preferences likewise shift with age: the neutral temperature for many older adults is higher than that assumed in standard comfort models (Seppänen & Fisk, 2006).
The planned use of a quiet room by Cheng et al. (2017) and O’Dwyer et al. (2007) aligns with research indicating that reduced noise and vibration can enhance cognitive task performance by aiding participant focus (Ljungberg et al., 2004). Additionally, the intervention involving freestyle aerobics set to music by Vaughan et al. (2012) is consistent with findings demonstrating the positive effects of music tempo and loudness on exercise performance (Edworthy & Waring, 2006), and the benefits of motivational music in optimizing arousal, reducing perceived exertion, and improving performance in repetitive, endurance-based exercises (Karageorghis & Priest, 2012). Music tempo also influences physical activity levels and heart rate, which could particularly benefit older adults engaging in physical exercise (Terry et al., 2012). However, no information was provided about the music tempo in the protocol paper, limiting replicability of these conditions.
Gibbs et al. (2015), Cordes et al. (2019), and Gonnord et al. (2023) each reported they would create environments that were “home-like,” stimulating, or designed to promote social interaction and well-being. These adaptations are supported by previous literature suggesting that the design and layout of spaces, such as furniture arrangement and the strategic use of space, can significantly influence how individuals interact. For instance, spatial proximity in group interactions can enhance comfort and willingness to engage, particularly when the layout encourages closer distances among participants (Novelli et al., 2010), music can play a critical role in social bonding by evoking attachment-related emotions, which are crucial for group dynamics (Koelsch, 2014), and warmer temperatures could increase group conformity and a sense of closeness, facilitating better social interactions among participants (Huang et al., 2014).
Implications for Reproducibility and Interpretation
The lack of detail about physical settings limits the ability to accurately replicate intervention environments, which could potentially affect the validity and reliability of outcomes. This observation aligns with findings from Lorusso and Bosch (2018), who emphasized the importance of detailed reporting in environmental interventions. They highlighted that inconsistent documentation of sensory elements such as lighting, auditory stimuli, and tactile components compromises the replicability of findings and limits the broader understanding of how these elements contribute to intervention outcomes. Their review of multisensory environments demonstrated that controlled and purposefully designed physical settings, when accurately documented and applied, have the potential to significantly improve mood, alleviate behavioral symptoms, and enhance participant engagement.
Strengths and Limitations
This review presents, to our knowledge, the first systematic investigation of purposeful physical settings in group-based psychosocial interventions targeting older adults. A strength of our approach is the focus on setting characteristics as an explicit design dimension often overlooked in intervention protocols.
Protocol-Based Evidence and Author Consultation
Reliance on protocol papers may introduce inaccuracies if actual implementation deviates from planned procedures (e.g., due to space availability, recruitment constraints, or resource changes). We attempted to mitigate this by contacting study authors; however, only approximately one-third responded. Because nonresponse can bias estimates, our observed prevalence of explicit setting consideration (29.3%) should be interpreted as a cautious upper bound.
Search Coverage and Gray Literature
Our search was limited to four multidisciplinary databases (Ovid MEDLINE, PubMed, Web of Science, and Scopus). We did not search AgeLine, PsycINFO, or CINAHL, nor did we systematically search grey literature (e.g., trial registries, governmental/community reports, theses, and conference proceedings). Methodological standards for scoping reviews recommend broad database coverage and targeted grey-literature searches to reduce selection and publication bias. These omissions may have led us to miss protocols that describe practical aspects of physical settings, potentially underestimating real-world attention to setting design.
Scope of Populations and Generalizability
We excluded protocols focused primarily on older adults with major sensory impairments (e.g., severe hearing or vision loss) or cognitive/neurological disorders (e.g., dementia, stroke, and Parkinson’s disease), and trials in which pharmacological agents or brain stimulation were the main interventions, to maintain focus on psychosocial programs delivered in non-specialist environments. This decision limits external validity. Many older adults experience sensory impairment and people living with dementia often benefit from systematic environmental adaptations (e.g., enhanced wayfinding cues, optimized lighting and acoustics, and simplified layouts) that are standard in specialized servicescapes. A complementary review focused on specialist dementia and neurorehabilitation settings is warranted.
Future Directions
Experimental evidence on how specific physical-setting parameters affect engagement and outcomes in psychosocial interventions for older adults is limited. This scoping review, and the practice-oriented recommendations that follow, are a preliminary step toward an evidence-informed framework for designing and reporting purposeful physical settings. We propose that purposeful physical settings be treated as a prespecified design dimension of psychosocial interventions for older adults. For example, a brief, field-tested checklist aligned with SPIRIT/TIDieR could specify measurable parameters—acoustics (e.g., LAeq and RT60/SNR strategy), lighting/daylight (horizontal and vertical illuminance, glare control), thermal conditions (temperature range, stability), layout/visibility, accessibility, and sensory cues (e.g., music tempo (bpm) and level (dB)). At a minimum, protocols should report planned background sound levels and reverberation control, target illuminance (horizontal and vertical) and daylight strategy, and the intended temperature range and means of ensuring thermal stability, particularly when facilities are intended for general public use (e.g., community halls or outpatient clinics). For each checklist item, authors would indicate whether it is (a) standardized, (b) deliberately varied, or (c) uncontrolled but documented and outline minimal site-level monitoring. A qualitative investigation of barriers and enablers of environmental reporting in psychosocial interventions could facilitate adoption and use of such a checklist.
As interventions increasingly occur online, the home environment and digital interface function as an extended servicescape that can be purposefully shaped. In these cases a brief, standardized “environment check” could be incorporated to help participants and facilitators optimize basic conditions—for example, sitting in a well-lit position facing the light (rather than backlit), using headphones or participating in a quiet room with doors closed to reduce background noise, confirming thermal comfort, and ensuring a stable chair with clear floor space when movement is involved (Rodrigues et al., 2022). Integrating these simple steps into protocol templates could improve fidelity and participant safety while acknowledging variability in home settings.
Beyond reporting, experimental studies should estimate the causal contribution of key environmental features while holding psychosocial content constant. Randomized controlled trials (RCTs) could manipulate, for example, background noise (quiet vs. moderate), illuminance (higher vs. lower), or seating layout (circle vs. classroom). Primary outcomes should target participant engagement (attendance, active participation, validated engagement scales), with secondary endpoints for adherence, listening effort, affect, and safety; environmental fidelity should be prespecified. These trials would extend person–environment fit, where behavior and well-being reflect the interaction between personal competence and environmental press.
Finally, future research should (i) develop pragmatic protocols for routine measurement and documentation of environmental conditions within process evaluations, coupled with participant-reported comfort, and (ii) conduct a qualitative study with stakeholders to investigate barriers and enablers of environmental reporting. Embedding these insights into reporting standards will enhance transparency, reduce confounding, and strengthen replicability and generalizability.
Conclusion
In psychosocial interventions for older adults, the physical setting is not a backdrop; it is a designed input that shapes engagement and outcomes through identifiable psychological mechanisms and age-linked moderators. Our findings suggest that intentional consideration and thorough documentation of these settings can enhance engagement, replicability, and outcomes. Future protocols and studies should integrate these elements more explicitly, thereby strengthening both the transparency and the overall impact of gerontological intervention research.
Supplemental Material
Supplemental Material - The Use of Purposeful Physical Settings in Group-Based Psychosocial Interventions for Older Adults: A Scoping Review of Study Protocols
Supplemental Material for The Use of Purposeful Physical Settings in Group-Based Psychosocial Interventions for Older Adults: A Scoping Review of Study Protocols by Bilal Hassan, Andrew Waterhouse, Penny Rapaport, and Natalie L. Marchant in Journal of Applied Gerontology.
Footnotes
Acknowledgments
We thank study authors for their helpful communication about the studies. We thank Dr. Marcella Ucci, Dr. Kristina Niedderer, and Dr. Nuriye Kupeli for their contributions to this work. We also extend our appreciation to Harriet Demnitz-King, Tim Whitfield, and Yolanda Lau for their generous support and collaboration.
Ethical Considerations
Not applicable. The present work is a scoping review and does not involve direct human participants.
Author Contributions
All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BH is employed by Les Roches, a Swiss University of Applied Sciences, as a senior lecturer. Les Roches provided no financial support, resources, or directives in this research. Although the findings may have future academic applications in healthcare education, no current initiatives would directly benefit from these results. BH declares no other potential financial or institutional conflicts of interest. Prof. Penny Rapaport reports grants from the National Institute for Health and Care Research (NIHR) Academy (NIHR300844) and NIHR Programme Grants for Applied Research (PGfAR; NIHR200120, and NIHR203670); and support from the University College London (UCL) Hospitals NIHR Biomedical Research Centre with no conflict of interest with the present work. Andrew Waterhouse and Dr. Natalie L. Marchant report no conflicts of interest.
Data Availability Statement
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Supplemental Material
Supplemental material for this article is available online.