
Abstract
Camera-based active and assisted living (AAL) technologies offer a promising solution to the challenges of population ageing but are not widely accepted by older adults. One possible reason for this resistance is a lack of identification with one’s future self, who is the primary beneficiary of such technologies. This study investigated the extent to which future self-continuity – the sense of psychological connectedness between present and future selves – influences older adults’ acceptance of camera-based AAL technologies. Results from an online sample of older adults (n = 183) demonstrated that greater future self-continuity was associated with increased acceptance. This relationship was mediated by perceived usefulness: older adults with more vivid and positive views of their future selves exhibited stronger recognition of the technology’s long-term benefits, which in turn increased acceptance. These findings highlight future self-continuity as a promising psychological target for interventions aimed at enhancing older adults’ acceptance of camera-based AAL technologies.
• Introduces future self-continuity as a novel psychological determinant of older adults’ acceptance of camera-based active and assisted living (AAL) technologies, extending beyond traditional utilitarian models of technology acceptance. • Demonstrates that lower future self-continuity is associated with underweighting the long-term benefits of camera-based AAL technologies, offering a mechanistic explanation for older adults’ tendency to postpone acceptance of the technology.
• Suggests that interventions that enhance older adults’ psychological connectedness with their future selves – specifically, those that encourage more vivid and positive views of their future selves – may increase acceptance of camera-based AAL technologies. • Provides evidence to support the strategic integration of psychological insights into the implementation of camera-based AAL technologies, extending beyond a focus on practical barriers to acceptance such as usability and ease of use.What This Paper Adds
Applications of Study Findings
Background
The global number of older adults – defined as individuals aged 60 and above – is expected to double between 2015 and 2050 (United Nations Department of Economic and Social Affairs Population Division, 2015). This rapid ageing poses social and economic challenges, including rising pension costs, healthcare strain, and economic stagnation (Bloom et al., 2015). Policies promoting ageing in place – enabling older adults to live independently at home rather than in acute or institutional care settings – are framed as a means of mitigating these pressures (Sixsmith & Sixsmith, 2008). Such approaches are believed not only to alleviate demands on health and social care systems but also to enhance older adults’ quality of life by upholding their well-chronicled preferences to remain in their own homes as they age (Bechtold et al., 2022).
Camera-based active and assisted living (AAL) technologies have emerged as promising tools for supporting ageing in place. By leveraging techniques in computer vision and artificial intelligence, these technologies can passively sense and proactively react to older adults’ various needs at home, such as by intervening in falls or wandering (Bhola & Vishwakarma, 2024; Fleck & Straßer, 2010), issuing medication reminders (Villacorta et al., 2011), and instrumenting more comfortable living environments for greater ease of daily living (Marques et al., 2019). More advanced systems can even predict risks and trigger preventive actions, including making timely behaviour change suggestions to target morbidity upstream (Andreu et al., 2016).
Despite these advantages, older adults often resist using camera-based AAL technologies, expressing willingness to trial such technologies only later in life. One study found that only 15.5% of surveyed older adults were willing to use the technology immediately, compared to 82.4% in later life (Claes et al., 2015). Similarly, older adults have reported preferences to use camera-based AAL technologies only ‘in the future when required’ (Elers et al., 2018), ‘at a later point’ (Demiris et al., 2008), or at ‘a later time, when they were older’ or ‘really needed the technology’ (Dermody et al., 2021).
The temporal asymmetry in older adults’ acceptance of camera-based AAL technologies, where acceptance is skewed toward future rather than present use, may be explained by differences in future self-continuity – the perceived psychological connectedness between one’s present and future selves (Ersner-Hershfield et al., 2009). Individuals typically feel greater affinity with temporally closer selves and weaker connection to distant future selves, whose consideration activates brain regions similar to those used when thinking about strangers (Ersner-Hershfield et al., 2009). Recent theoretical developments have established a three-factor substructure of future self-continuity, suggesting that future selves are experienced as more tenuously linked when seen as dissimilar to the current self, poorly imagined, or viewed negatively (Bixter et al., 2020; Sokol & Serper, 2020).
Future self-continuity has important implications for intertemporal choices – decisions involving costs and benefits that occur at different points in time (Hershfield, 2011). This is because the future self is often the beneficiary of such decisions, as exemplified by the choice to accept camera-based AAL technologies in present day: immediate costs such as privacy invasion accrue now, while benefits such as improved health, independence, and longevity typically manifest later. Although models of rational choice dictate favouring delayed, higher-value outcomes to maximise lifetime utility, people often discount the future, devaluing outcomes as their delay from the present increases, and prioritising immediate comfort or the avoidance of short-term costs instead (Bartels & Rips, 2010). This tendency is particularly pronounced among individuals with lower future self-continuity, who have been shown to deprioritise long-term welfare and concede to shortsighted behaviours such as procrastinating, failing to save for retirement, and forgoing exercise (Blouin-Hudon & Pychyl, 2015; Hershfield, 2011; Rutchick et al., 2018).
Applying this lens to technology acceptance, variations in future self-continuity may underpin the temporal asymmetry observed in older adults’ acceptance of camera-based AAL technologies. Older adults with lower future self-continuity may discount the technology’s long-term benefits as these accrue to a psychologically distant future self. Conversely, they may place greater weight on its immediate costs, such as its privacy implications, as these disproportionately impact the present self. This imbalanced valuation of costs and benefits may ultimately lead to rejection of the technology (Offermann et al., 2023). Indeed, if future selves are experienced as psychologically akin to strangers (Ersner-Hershfield et al., 2009), this may explain why older adults often attribute the need for AAL technologies to strangers they perceive as ‘older’, ‘more infirm’, and altogether ‘worse off’ than themselves (Grace et al., 2017), describing these technologies as useful innovations ‘but obviously not for me’ (Neven, 2010).
To date, most studies have explained technology acceptance through utilitarian lenses focused on the usefulness and ease of use of technology (Davis, 1989), leaving psychological mechanisms such as future self-continuity underexplored. This oversight is significant as psychological influences on behaviour are typically malleable and responsive to intervention (Michie et al., 2014). Indeed, future self-continuity has be experimentally manipulated to encourage farsighted behaviours such as exercising (Rutchick et al., 2018) and saving for retirement (Shah et al., 2022). As such, establishing its role in older adults’ acceptance of camera-based AAL technologies could inform the design of interventions aimed at fostering acceptance, benefitting the technology’s broader adoption and strengthening its capacity to support ageing-in-place objectives.
Objective
This study aimed to examine the association between future self-continuity and older adults’ acceptance of camera-based AAL technologies. Drawing on the premise that low future self-continuity leads to the devaluation of future welfare, it was hypothesised that this diminished concern would result in an underweighting of the technology’s long-term benefits and an overweighting of its immediate costs, resulting in rejection of the technology.
Using a cross-sectional online survey, we tested three hypotheses: (H1) Future self-continuity – operationalised as perceived similarity to, vividness of, and positivity towards the future self (Bixter et al., 2020; Sokol & Serper, 2020) – will be positively associated with acceptance; The positive impact of future self-continuity on acceptance will be mediated by (H2) reduced privacy concerns and (H3) enhanced perceptions of the technology’s usefulness.
Methods
Participants and Procedure
Community-dwelling older adults aged 60–80 were recruited via Amazon Mechanical Turk (MTurk) to complete an online Qualtrics survey. MTurk samples have shown strong comparability to conventionally recruited offline samples of older adult (Lemaster et al., 2015). The lower age limit of 60 years aligns with the United Nations’ (2015) definition of older adults, while the upper limit excluded the ‘oldest old’ (≥80 years) due to anticipated difficulties envisioning one’s future self over a 10-year horizon in the Future Self-Continuity Questionnaire (described below). All participants provided informed consent and took 10.9 min on average to complete the survey. Participants received $0.50 for completing the survey, consistent with average reimbursement rates on MTurk (Hara et al., 2018).
Materials
Measures are listed below in the order in which they were presented in the survey.
Demographics
Participants reported their age, year of birth, gender, race/ethnicity, education, employment, income, and chronic disease status (self-reported diagnosis of diabetes, chronic obstructive pulmonary disease, chronic heart disease, or congestive heart failure). These conditions were selected due to their status as the leading global causes of chronic disease-related mortality (World Health Organisation, 2020).
Future Self-Continuity
Future self-continuity was assessed using the 10-item future self-continuity questionnaire (FSCQ; Sokol & Serper, 2020). Participants were asked to imagine themselves 10 years in the future and respond to items assessing three components of future self-continuity: similarity to (6-point Likert scale; 1 = completely different, 6 = exactly the same), vividness of (1 = not at all, 6 = perfectly), and positivity toward (1 = not at all, 6 = perfectly) the future self. Responses on the FSCQ yield an overall score as well as subscale scores corresponding to each component. The FSCQ demonstrated good internal reliability both in its validation study (Cronbach’s α = .850, subscales, subscales α = .790–.900) and in the present study (Cronbach’s α = .882, subscales α = .745–.790). Higher scores on the measure indicated greater future self-continuity.
Identification With Home Living Scenario
In line with previous studies examining older adults’ acceptance of AAL technologies (Offermann-van Heek et al., 2019), participants were presented with a descriptive paragraph asking them to imagine living alone while managing chronic disease and declining function. Thereafter, they read information on camera-based AAL technologies and their potential benefits for improving safety, health, longevity, and independence over the long term.
Given that stronger identification with such scenarios is positively correlated with acceptance of AAL technologies (Offermann-van Heek et al., 2019), participants’ identification with the home living scenario was assessed using a single item (6-point Likert; 1 = not at all; 6 = perfectly) and included as a covariate in the main analysis to control for potential confounding. Higher scores indicated greater identification with the scenario.
Privacy Concerns
Privacy concerns surrounding camera-based AAL technologies were assessed using a validated 6-item measure adapted from Jaschinski et al. (2021). Sample items included the statements: ‘If I use the camera-based technology, I am concerned that others might use my personal information to harm me’ and ‘If I use the camera-based technology, I worry about being constantly monitored’ (5-point Likert scale; 1 = strongly disagree, 5 = strongly agree; Cronbach’s α = .839). Higher scores reflected stronger privacy concerns.
Perceived Usefulness
Perceived usefulness of camera-based AAL technologies was measured using seven items, also adapted from Jaschinski et al. (2021). Sample items included the statements: ‘Using the camera-based technology will allow me to age in my home environment’ and ‘If I use the camera-based technology, I can keep doing things on my own’ (5-point Likert scale; 1 = strongly disagree, 5 = strongly agree; Cronbach’s α = .838). Higher scores indicated stronger perceptions of the technology’s usefulness.
Acceptance
Technology acceptance was assessed using a single item measuring participants’ willingness to install camera-based AAL technologies in their homes today (5-point Likert scale; 1 = not willing at all, 5 = perfectly willing). Willingness to install technology in one’s home has been used as a proxy for acceptance in prior research on older adults’ acceptance of in-home monitoring technologies (Mihailidis et al., 2008). Participants’ responses were dichotomised into two categories: ‘unaccepting’ (not willing at all, unwilling, neither willing nor unwilling) and ‘accepting’ (willing, perfectly willing). This binary categorisation reflects the practical nature of technology adoption decisions and supports clearer identification of factors that differentiate accepters from non-accepters.
Statistical Analysis
Continuous variables exhibited non-normal distributions (with standardised skewness and kurtosis values exceeding ±3.29; Kim, 2013) and were therefore analysed using non-parametric tests. Continuous data were summarised using medians and interquartile ranges and categorical data presented as frequencies and percentages. Correlations between continuous variables were assessed using Spearman’s rank correlation coefficient (r s ).
Differences between accepters and non-accepters of camera-based AAL technologies were assessed using Fisher’s exact tests for categorical demographic variables (gender, race/ethnicity, education, employment, income, chronic disease status) and Mann-Whitney U-tests for continuous (age) and ordinal (scenario identification) variables. Univariable logistic regression models assessed associations between acceptance and the individual predictor variables: FSCQ, FSCQ-similarity, FSCQ-vividness, FSCQ-positivity, privacy concerns, and perceived usefulness. Subsequently, multivariable logistic regression models were computed to control for demographic differences between accepters and non-accepters, and scenario identification. The strength of the associations between predictor variables and acceptance was expressed using the odds ratios (ORs) and 95% confidence intervals (CIs) for a unit increase in scores on each predictor variable.
Mediation models were computed to examine whether an imbalance in outcome valuation – specifically, heightened valuations of the technology’s benefits and/or reduced valuations of its privacy costs – explains the relationship between future self-continuity and acceptance. Mediation analysis was performed using Model 4 of the PROCESS macro for SPSS (Hayes, 2013). Covariates included scenario identification and demographic variables significantly associated with the predictor, outcome, or both (Lee et al., 2021). Bootstrapping procedures were used to generate 95% bias-corrected CIs for the magnitude of direct and indirect effects based on 5,000 resamples. Bootstrapped indirect effects were considered statistically significant if the 95% CI did not include zero (Hayes, 2013). All statistical tests were two-tailed, with p < .05 indicating statistical significance. All analyses were performed using SPSS Version 28.0.
Power Analyses
An a priori power analysis was undertaken using G*Power Version 3.1.9.6 (Faul et al., 2007). Considering a baseline acceptance rate of approximately 60% (Claes et al., 2015), a minimum sample of n = 84 participants was required to detect an odds ratio of at least two (representing a medium effect size; Rosenthal, 1996) – indicating that the odds of acceptance double for every one-unit increase in scores on the FSCQ – at 80% power with a 5% significance level. Additionally, a minimum sample size of n = 71 participants was required to detect medium effect sizes for each pathway of the planned mediation analyses using bias-corrected bootstrapping (Fritz & MacKinnon, 2007).
Results
Of the n = 293 participants who completed the survey, n = 110 were excluded: n = 53 provided inconsistent year-of-birth information at different points in the survey (suggesting potential falsification of age; Chu et al., 2016), n = 40 failed attention checks, n = 12 responded identically across consecutive Likert scale items, and n = 5 took less than 40% of the median time to complete the survey, indicating inattentive responding (Greszki et al., 2015). The final analytic sample (n = 183) exceeded the recommended sample size, suggesting sufficient statistical power.
Demographic Summary of the Study Sample (n = 183) Categorised by Acceptance of Camera-Based AAL Technologies (Willing Versus Unwilling to Accept)
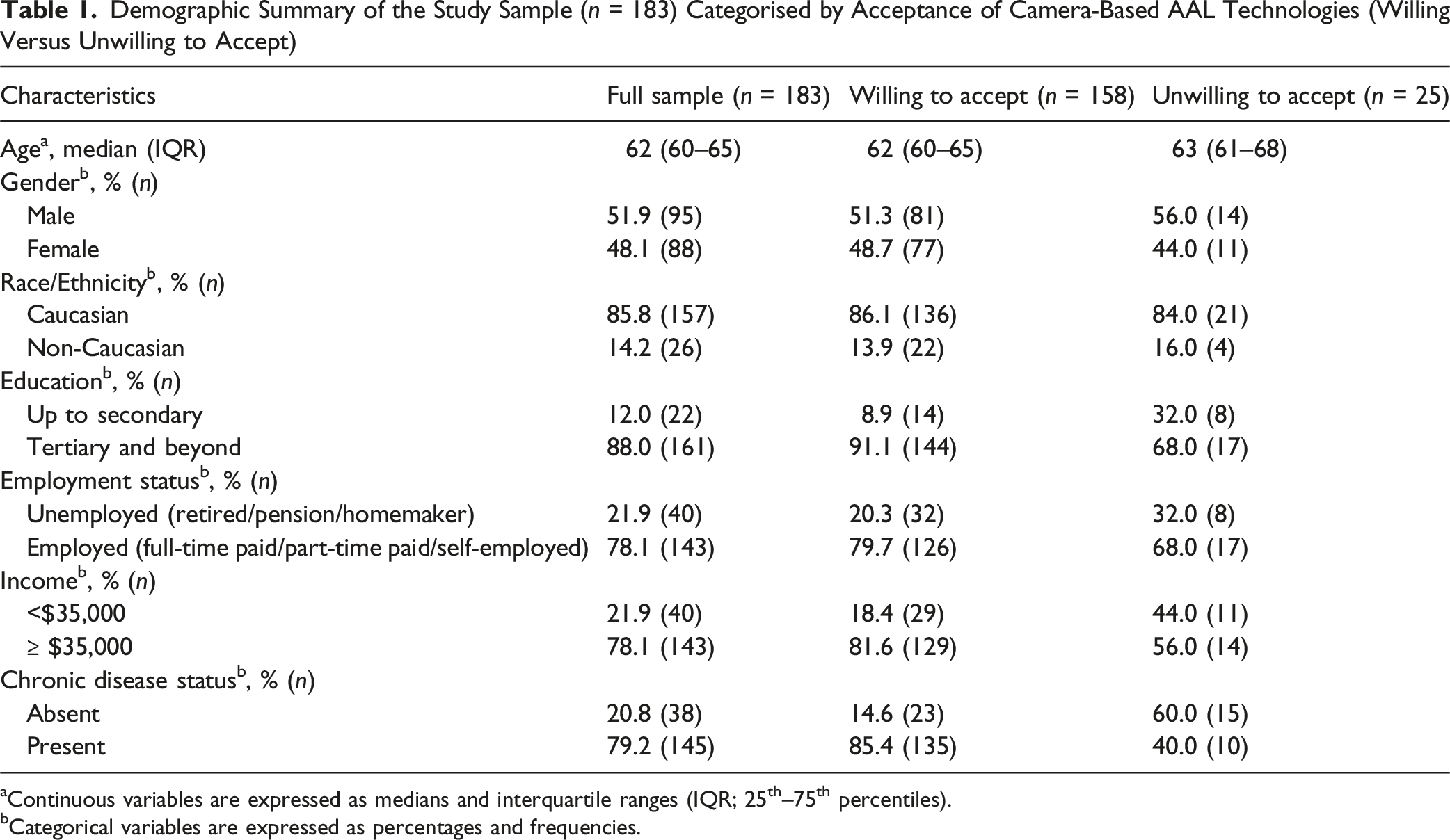
aContinuous variables are expressed as medians and interquartile ranges (IQR; 25th–75th percentiles).
bCategorical variables are expressed as percentages and frequencies.
Fisher’s exact tests indicated significant differences in acceptance by chronic disease status (93.1% accepted the technology among those with chronic disease versus 60.5% without, p < .001), income (90.2% accepted among those earning ≥ $35,000 versus 72.5% among those earning < $35,000, p = .008), and education (89.4% accepted among those with at least a tertiary education versus 63.6% among those with up to secondary education, p = .004). Additionally, Mann-Whitney U test results indicated that participants who accepted the technology identified significantly more with the home living scenario than those who did not accept the technology (U = 577.0, p < .001). The median scenario identification score was 3 (somewhat identify) for non-accepters, compared to 5 (very strongly identify) for accepters. Chronic disease status, income, education, and scenario identification were therefore entered as covariates in multivariable logistic regression models examining the relationship between future self-continuity and acceptance.
Zero-Order Correlations Among the Key Study Variables FSCQ, FSCQ Subscales, Privacy Concerns, Perceived Usefulness, and Acceptance
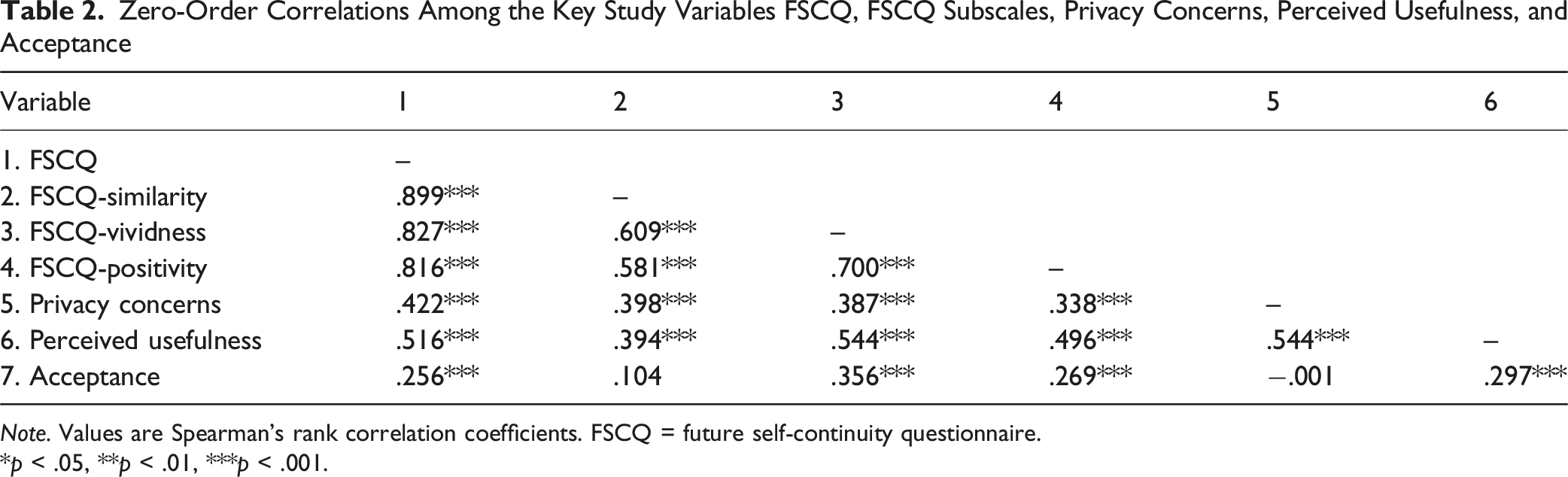
Note. Values are Spearman’s rank correlation coefficients. FSCQ = future self-continuity questionnaire.
*p < .05, **p < .01, ***p < .001.
Next, the association between future self-continuity and acceptance of camera-based AAL technologies was examined using logistic regression. Supporting H1, an unadjusted model revealed a significant and positive association between FSCQ and acceptance, with each unit increase in FSCQ score nearly tripling the odds of acceptance (OR = 2.99, 95% CI [1.67, 5.35], p < .001). To isolate the unique effects of the similarity, vividness, and positivity components of future self-continuity on acceptance, separate univariable logistic regression models were run for each FSCQ subscale. These revealed that the odds of acceptance were heightened when participants perceived their future selves more vividly (OR = 3.21, 95% CI [1.94, 5.31], p < .001) or positively (OR = 3.09, 95% CI [1.76, 5.43], p < .001) but not when they felt more similar to their future selves (OR = 1.52, 95% CI [1.00, 2.31], p = .050).
Summary of Unadjusted and Adjusted Logistic Regression Models Predicting Acceptance From Individual Predictor Variables FSCQ, FSCQ-Similarity, FSCQ-Vividness, and FSCQ-Positivity
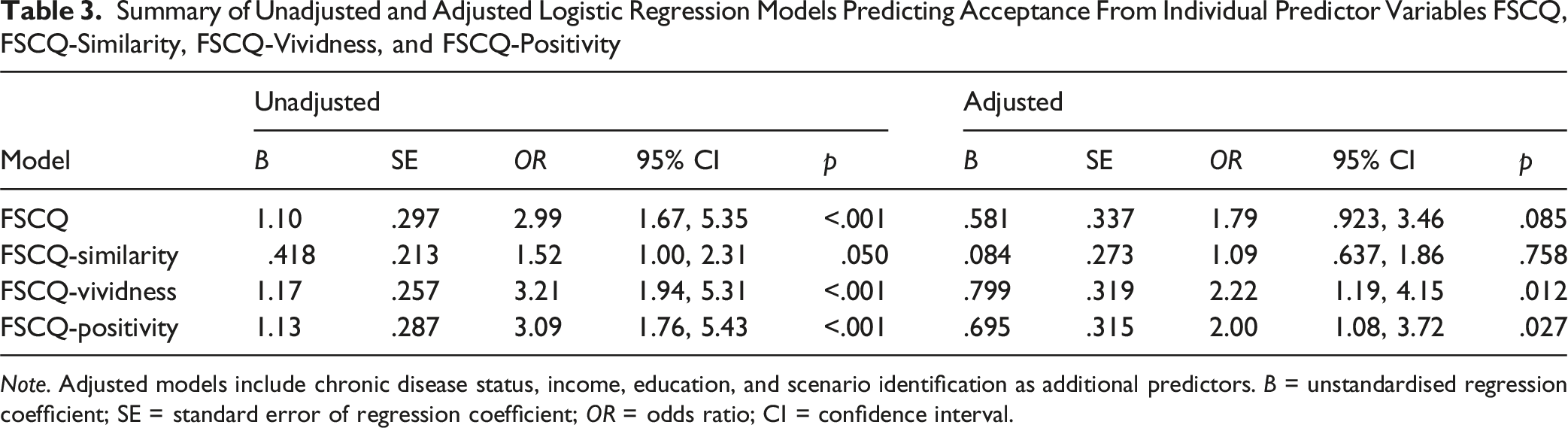
Note. Adjusted models include chronic disease status, income, education, and scenario identification as additional predictors. B = unstandardised regression coefficient; SE = standard error of regression coefficient; OR = odds ratio; CI = confidence interval.
A secondary goal of the study was to examine whether future self-continuity influenced older adults’ acceptance of camera-based AAL technologies by reducing privacy concerns and/or increasing the perceived usefulness of the technology. To this end, mediation analysis was conducted to assess the potential mediating roles of privacy concerns and perceived usefulness in the relationship between future self-continuity and acceptance.
To obtain unbiased estimates of mediation effects, the following assumptions must be met: (i) the predictor variable must be significantly associated with the dependent variable; (ii) the predictor variable must be significantly associated with the mediator; and (iii) the mediator must be significantly associated with the dependent variable (Baron & Kenny, 1986). Given the non-significant association between FSCQ-similarity and acceptance (OR = 1.52, p = .05, 95% CI [1.00, 2.31]), FSCQ-similarity did not meet criterion (i) and was excluded from further analyses. However, both FSCQ-vividness (OR = 3.21, p < .001, 95% CI [1.94, 5.31]) and FSCQ-positivity (OR = 3.09, p < .001, 95% CI [1.76, 5.42]) were positively associated with acceptance. Consequently, a composite FSCQ-vividness-positivity (FSCQ-VP; Cronbach’s α = .882) score was constructed for predicting acceptance. Criterion (ii) was met, as significant correlations were found between FSCQ-VP and both the proposed mediators perceived usefulness (r s = .569, p < .001) and privacy concerns (r s = .387, p < .001). Upon examining criterion (iii), only perceived usefulness emerged as a candidate mediator, showing a strong positive association with acceptance (OR = 5.14, p < .001, 95% CI [2.58, 10.2]). In contrast, privacy concerns was not associated with acceptance (OR = 1.33, p = .299, 95% CI [.776, 2.28]), leading to its exclusion as a mediator. Therefore, it was not possible to test H2, which posited that the positive effect of future self-continuity on acceptance would be mediated by reduced concerns about the technology’s privacy implications.
The final mediation model included FSCQ-VP as the predictor variable, perceived usefulness as the mediator, and acceptance as a dichotomous dependent variable. Results revealed a significant indirect path from FSCQ-VP to acceptance through perceived usefulness. Specifically, participants with higher FSCQ-VP scores perceived camera-based AAL technologies as more useful than those with lower FSCQ-VP scores (B = .461, 95% CI [.362, .560]), p < .001), which in turn led to greater acceptance of the technology (B = 1.31, 95% CI [.524, 2.09]), p = .001). Mediation was confirmed since bias-corrected bootstrapped 95% CIs for the indirect effect through FSCQ-VP did not contain zero (95% CI [.166, 1.07]). The direct effect of FSCQ-VP on acceptance remained significant after accounting for indirect effects (B = 1.05, 95% CI [.356, 1.74], p = .003), suggesting that perceived usefulness partially mediated the relationship between FSCQ-VP and acceptance.
A separate mediation model was computed to adjust for variables significantly associated with FSCQ-VP (employment) or acceptance (chronic disease status, income, education, scenario identification). In the adjusted model, the predictor-mediator path (B = .395, 95% CI [.281, .511]), p < .001) and the mediator-outcome path (B = 1.19, 95% CI [.220, 2.15]), p = .016) were consistent with those in the unadjusted model. However, the direct effect of FSCQ-VP on acceptance, when controlling for perceived usefulness, was no longer significant in the adjusted model (B = .460, 95% CI [–.344, 1.26], p = .262), suggesting that perceived usefulness fully mediated the relationship between FSCQ-VP and acceptance.
Overall, mediation results confirmed H3, demonstrating that the positive effect of future self-continuity – specifically, its vividness and positivity components – on acceptance was mediated by increased perceptions of the technology’s usefulness. Mediation results are summarised in Figure 1. Path coefficients for mediation models predicting acceptance from FSCQ-VP through perceived usefulness (A) without and (B) with adjustment for chronic disease status, income, education, employment, and scenario identification. The a path coefficient represents the estimated association between FSCQ-VP and perceived usefulness; The b path coefficient represents the estimated association between perceived usefulness and acceptance; The c’ path coefficient represents the estimated association between FSCQ-VP on acceptance controlling for perceived usefulness (the direct effect). Coefficients for continuous outcomes (path a) represent unstandardised regression weights. Coefficients for binary outcomes (paths b and c’) represent log-odds [odds ratios]. FSCQ-VP = Future Self-Continuity Questionnaire Vividness-Positivity subscale. *p < .05, **p < .01, ***p < .001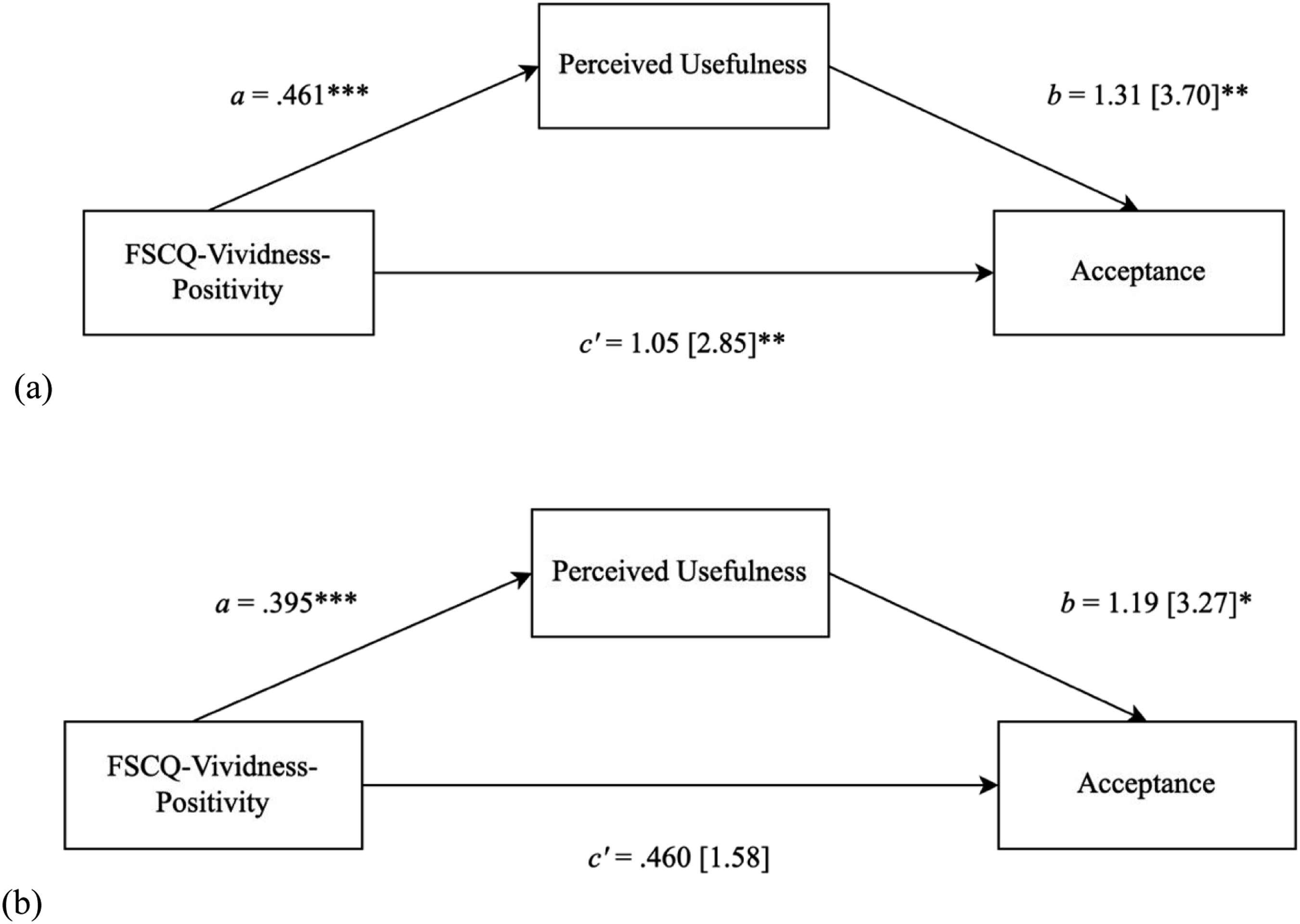
Discussion
To the best of our knowledge, this study is the first to examine the effect of future self-continuity on older adults’ acceptance of camera-based AAL technologies, and is also the first to examine the role of future self-continuity in individuals’ technology acceptance decisions more broadly. The results provide preliminary evidence that older adults’ resistance to camera-based AAL technologies is partly attributable to a diminished sense of subjective connectedness to their future selves. Specifically, older adults who experienced their future selves in less (versus more) vivid and positive terms were significantly less likely to be willing to install the technology in their homes today. Notably, acceptance was not influenced by older adults’ perceived similarity to their future selves.
The finding that acceptance of camera-based AAL technologies was higher among older adults with more positive conceptions of their future selves accords with the literature on the adaptive functional value of positive future self-views. Research has demonstrated that positive views of the future self are predictive of various positive outcomes, including better health, improved physical function, and increased longevity (Levy et al., 2002; Sargent-Cox et al., 2012). This phenomenon is thought to occur because positively envisaged future selves serve as motivating beacons that individuals are driven to emulate, thus propelling adaptive behaviours in pursuit of these positively appraised future selves (Cross & Markus, 1991; Markus & Nurius, 1986). For instance, positive views of ageing have been shown to predict increased engagement in preventive health behaviours such as maintaining a healthy diet, avoiding alcohol and smoking, exercising regularly, and adhering to medication regimens (Levy & Myers, 2004). Similarly, Kornadt et al. (2015) found that older adults who held more (versus less) positive views of their future selves were more likely to engage in ageing-related preparation behaviours, such as maintaining social relationships and increasing participation in leisure and community activities. Therefore, to the extent that the present-day acceptance of camera-based AAL technologies can be construed as a form of preventive health behaviour aimed at achieving a positively envisioned future self, our results attest to the motivational value of positive future self-imagery and extend this concept to the domain of camera-based AAL technology acceptance.
Another perspective suggests that, given that individuals are more likely to prioritise the interests of those they like over those they dislike (Fiske & Taylor, 2013), individuals who view their future selves more favourably may be more inclined to act in their future selves’ best interests (Burum et al., 2016). This could explain why older adults who viewed their future selves more positively were more willing to accept camera-based AAL technologies, presumably because such acceptance maximises the interests of their future selves rather than solely those of their present selves.
In much the same way that positive future selves serve as motivating models for behaviour, vividly imagined future selves also possess similar motivational power. This is thought to occur because vividly envisioned future selves – and the costs and benefits that accrue to these future selves – are often experienced as more proximate, as though they were happening in the present (Hershfield et al., 2018). Individuals with vivid conceptions of their future selves may thus be better able to ‘pre-experience’ the outcomes that will accrue to their future selves, facilitating more accurate estimations of how their present choices might affect their future wellbeing (Boyer, 2008). On this reading, the potential health and wellbeing benefits of camera-based AAL technologies, which largely accrue to the future self, are likely to be given considerable weight by older adults who vividly conceptualise their future selves. Conversely, if potential future pains due to be endured by the future self are imagined less vividly and perceived as ‘less real, or less painful’ (Parfit, 1984), the potential long-term costs of rejecting the technology today, such as deteriorated health and wellbeing for one’s future self, may be underestimated. This underestimation may in turn lead to rejection of the technology.
Consistent with this theorising, the results of the mediation analyses demonstrated an indirect path from FSCQ-VP scores to acceptance through perceived usefulness. This suggests that the positive effect of vivid and positive conceptions of the future self on acceptance was transmitted through heightened perceptions of the technology’s usefulness. In other words, older adults who envisioned their future selves more vividly and positively were more likely to endorse the technology’s benefits – benefits that largely accrue to their future selves rather than their present selves – which in turn increased their likelihood of accepting the technology. These findings underscore the putative behaviour change efficacy of interventions aimed at enhancing vivid and positive future self-views among older adults, as such interventions may facilitate greater acceptance of camera-based AAL technologies.
Interestingly, the converse mediational pathway – specifically, that future self-continuity increases acceptance by reducing concerns about the technology’s immediate privacy costs – could not be established. This limitation arose because privacy concerns were not significantly associated with acceptance, thereby restricting examination of the proposed mediational path. Although this finding is perplexing given the well-documented dampening effect of privacy concerns on older adults’ acceptance of camera-based AAL technologies (Courtney et al., 2008; Jaschinski & Allouch, 2015), these findings cohere with prior evidence indicating null effects of privacy considerations on AAL technology acceptance (Charness et al., 2016; Steele et al., 2009). It is possible that other unmeasured near-term costs, such as the loss of cherished human contact or the infantilising stigma associated with AAL (Jaschinski et al., 2021), may have had effects on acceptance beyond the effects of privacy concerns alone. Accordingly, the non-significant indirect effect of future self-continuity on acceptance through privacy concerns may reflect a failure to account for a comprehensive set of immediately costly barriers to acceptance.
The finding that acceptance was influenced by positive and vivid future self-views but not by future self-similarity is challenging to interpret, particularly given the dearth of research on how future self-continuity influences older adults’ technology acceptance decisions. Nonetheless, insights from research on age-related changes in future self-views may provide some explanatory context. Research has documented that individuals tend to feel more similar to their future selves (Löckenhoff & Rutt, 2017) but often conceive their future selves with notably less vividness and positivity as they grow older (Chessell et al., 2014; Schacter et al., 2013). This general decline in future self-positivity and vividness with age may mean that even small increases in these constructs may have surprising potency for incentivising farsighted behaviour, such as the acceptance of camera-based AAL technologies. In contrast, if older adults already perceive sufficient likeness between their current and future selves, relative increases in future self-similarity may have minimal impact on acceptance.
Strengths and Limitations
This study represents the first known attempt to theorise and empirically substantiate the association between future self-continuity and older adults’ acceptance of camera-based AAL technologies. By exploring this relatively uncharted territory, the study contributes to the existing literature on the determinants of said acceptance among older adults, shedding light on psychological factors that have been understudied in this context.
A key strength of this study is its robust methodological framework, with a cross-sectional design and substantial sample size (n = 183) that enhance the validity of its findings. The results have significant practical implications for the implementation of camera-based AAL technologies. Understanding that enhancing future self-continuity may increase acceptance can guide developers and policymakers in creating interventions that foster this psychological connection, ultimately leading to greater acceptance and adoption of the technology.
Several limitations nonetheless warrant consideration. Notably, acceptance was measured as older adults’ self-reported intention to have camera-based AAL technologies installed in their homes, rather than their actual use of the technology. While the assumption that usage intentions lead to actual usage is common in the technology acceptance literature (Davis, 1989), the intention-usage link is tenuous and particularly flimsy in older cohorts (Ojiako, 2018). For example, participants’ self-reported acceptance in this study may have been optimistically biased due to social desirability (Bhattacherjee & Sanford, 2009). Participants may have felt pressure to appear open to technologies that could enhance their health and independence or may have wished to avoid appearing technophobic or resistant to change. Additionally, the desire to be helpful to researchers and the lack of real-world consequences for indicating (non-)acceptance in a hypothetical research scenario may have led to inflated acceptance rates. Indeed, given the extensive documentation of older adults’ resistance to camera-based AAL technologies (Demiris et al., 2008, 2009; Jaschinski & Allouch, 2015; Sánchez et al., 2019), the elevated rates of acceptance in this study (86.3% accepted) may reflect acquiescent, socially desirable responding. This potential bias may overestimate participants’ actual acceptance rates and mask their true privacy concerns surrounding the technology, constraining the validity of the results. Consequently, the non-significant link between privacy concerns and acceptance may be an artefact of this bias rather than a true reflection of participants’ attitudes.
However, the high rate of acceptance among participants may also be attributed to the use of a descriptive home living scenario in the present study, where participants were asked to imagine living alone whilst grappling with deteriorating health. Consistent with previous research demonstrating that older adults are more accepting of camera-based AAL technologies when they perceive a need for in-home care (Offermann-van Heek et al., 2019), our results indicated that acceptance was heightened among those who identified more strongly with the home living scenario. It is possible that, rather than reflecting older adults’ ‘true’ levels of technology acceptance based on their current circumstances, self-reported acceptance was inflated due to identification with and empathy for the home living scenario. Nonetheless, the findings regarding the association between future self-continuity and acceptance remain robust against this potential confound, as the results of the main analyses were statistically similar both with and without controlling for scenario identification.
It is worth noting that more objective measures of acceptance, such as actual technology use, can be impractical and may even be unfeasible in the case of novel innovations such as camera-based AAL technologies. Still, it may profit future work to implement alternative proxies for acceptance to improve the validity of the results. For example, studies could assess older adults’ implicit (i.e. subconscious) attitudes towards camera-based AAL technologies using well-established implicit association tests. These tests measure the strength of automatic associations between concepts by presenting participants with pairs of categories, such as camera-based AAL technologies and various positive attributes (e.g. ‘helpful’ and ‘beneficial’) alongside negative attributes (e.g. ‘intrusive’ and ‘unsafe’). Participants are tasked with quickly categorising words or images from these pairs, and their response times would indicate the strength of their implicit associations (Greenwald et al., 1998). Implicit attitudes are thought to better approximate actual technology acceptance and usage behaviour compared to explicit measures of attitude or intention (Belletier et al., 2018) and may therefore offer more valid approximations of acceptance.
Another limitation is that the study’s cross-sectional design precludes establishing a definitive causal pathway from future self-continuity to acceptance. While it may be that older adults were more likely to accept the technology due to heightened future self-positivity and vividness, it is also conceivable that anticipated use of the technology promoted self-continuity. For instance, older adults who imagined using the technology might have envisioned their healthier, more independent technologically assisted future selves in more vivid and positive terms. Causal investigations of the impact of future self-continuity on acceptance, such as through experimental manipulations of future self-continuity, should therefore be prioritised in future work.
Methodological decisions made during analysis should also be taken into consideration when interpreting the findings. While separate regression models were run for each of the FSCQ subscales to avoid multicollinearity issues arising from their high intercorrelations, this approach may have inflated the risk of Type I errors (i.e., false positives) by failing to account for shared variance among the subscales. Employing a multivariable approach that includes all three similarity, vividness, and positivity subscales as predictors in a single model would better control for their intercorrelations and provide a more comprehensive understanding of their combined and unique contributions to acceptance. Future work should explore such multivariable approaches to more effectively disentangle the relative influences of these closely related constructs.
Finally, these findings should be interpreted in light of the substantial heterogeneity that characterises later life. Cumulative experiences of education, employment, health, and technology exposure over earlier life stages – experiences more commonly available to socioeconomically advantaged individuals (Elder et al., 2003) – may shape individual characteristics such as future self-continuity. Studies have established positive links between future self-continuity and both educational attainment and income (Lu et al., 2023), possibly reflecting how socioeconomic privilege supports long-term planning, reduces uncertainty about the future, and enables more vivid and positive future self-views. Indeed, these same socioeconomic affordances, as reflected in the present results, may also promote greater access to and familiarity with technology, increasing the likelihood of accepting AAL technologies in later life. Conversely, older adults whose life courses have been marked by socioeconomic disadvantage may hold less positive views of their future selves, potentially due to cognitive constraints on long-term planning (Sheehy-Skeffington & Rea, 2017).
These life-course dynamics warrant cautious extrapolation from the present results. Participants were disproportionately White, highly educated, and employed – characteristics associated with systematically higher future self-continuity (Lu et al., 2023) – limiting the generalisability of the findings to other older populations, particularly those with histories of cumulative disadvantage. Future research should therefore examine whether the patterns identified here – particularly the finding whereby more vivid and positive future self-views promote acceptance via perceived usefulness – operates similarly across more socioeconomically diverse populations of older adults.
Implications
The present findings implicate future self-continuity as a promising target for interventions aimed at increasing older adults’ acceptance of camera-based AAL technologies. Results stand to inform the development of targeted acceptance-facilitating interventions, suggesting that to be effective, such interventions should focus on increasing the vividness and positivity with which future selves are envisaged rather than targeting felt similarity to the future self. Promisingly, studies have demonstrated that future self-vividness and positivity are amenable to manipulation and can be augmented through such techniques as viewing age-progressed images of oneself (Hershfield et al., 2011), interacting with age-progressed avatars in virtual reality (van Gelder et al., 2022; Şenel & Slater, 2020), and evoking mental imagery of one’s future self (Blouin-Hudon & Pychyl, 2017), with resultant gains in future-orientated action such as increased retirement savings behaviour (Hershfield et al., 2011) and lowered propensities to procrastinate (Blouin-Hudon & Pychyl, 2017). Given the intertemporal nature of AAL technology acceptance decisions, future studies would do well to examine the potential utility of such intervention strategies for enhancing older adults’ acceptance of camera-based AAL technologies or indeed on AAL technologies in general. Additionally, given the privacy-sensitive nature of imaged data captured by such technologies, interventions that enhance future self-continuity may be fruitfully used as an adjunct to more pragmatic but cost-intensive means of promoting acceptance, such as the use of privacy filters that redact identifying information from camera recordings (Padilla-López et al., 2015). Importantly, as highlighted above, evaluating whether interventions operate effectively across diverse older adult populations is essential to ensure that efforts to enhance future self-continuity do not inadvertently exacerbate existing inequalities in acceptance of AAL technologies. Such considerations will help guide the development of equity-sensitive, targeted interventions that are both effective and broadly applicable (Berkman et al., 2011).
Conclusion
The present findings lend preliminary support to the role of future self-continuity in older adults’ acceptance of camera-based AAL technologies. Results suggest that future selves that are imbued with more vividness and positivity inspire greater acceptance of camera-based AAL technologies by increasing older adults’ valuation of the technology’s long-run benefits. These findings implicate future self-vividness and positivity as plausible targets for interventions aimed at enhancing older adults’ acceptance of camera-based AAL technologies. Future work might profitably explore the effects of targeting these vividness and positivity constructs in acceptance-facilitating interventions.
Footnotes
Ethical Considerations
This study was approved by the Research Ethics Committee at the School of Nursing and Midwifery, Trinity College Dublin (approval number: COM_21_21.22).
Consent to Participate
All participants provided written informed consent.
Author Contributions
Conceptualisation: NAQT
Data collection and analysis: NAQT
Writing – Original draft: NAQT
Writing – Review and editing: All authors
Supervision: JD, AMB
Funding acquisition: JD
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the European Union’s Horizon 2020 research and innovation programme under grant agreement visuAAL Project Grant No. 861091. This document reflects the views only of the authors, and the European Union cannot be held responsible for any use which may be made of the information contained therein.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.