
Abstract
Homebound status increasingly emerges as a critical social and health concern among older adults. Recognized as a “hard-to-reach” group, there is a need to better understand how to define and identify homebound older adults. Using the Arksey and O’Malley framework (2005), we searched eight databases with a librarian-guided strategy. Two authors independently screened titles, abstracts, and full texts, and extracted data based on set criteria. We included 19 studies that define homebound status through factors such as the duration and frequency of confinement; consequences of physical, social, or cognitive impairments; and those needing assistance. Researchers identify homebound individuals through health records, outpatient clinics, reports from family, neighbors, or community agencies like Meals on Wheels. Challenges include over-reliance on convenience and snowball sampling, as well as time constraints that limit the ability of researchers and clinicians to systematically identify those missing clinical appointments. A framework is needed to guide a formal identification.
• Provides strategies used to identify homebound older adults globally • Highlights the practical challenges in identifying homebound individuals, emphasizing the need for a standardized framework.
• Findings can inform clinicians, researchers, and policymakers in developing a framework to consistently identify homebound older adults. • Supports improved targeting of services and interventions (e.g., home care, community programs, and outreach) for this “hard-to-reach” population.What This Paper Adds
Applications of Study Findings
Introduction
The World Health Organisation forecasts a global demographic shift in which more than 20% of the world’s population will surpass the age of 65 by 2050 (Rudnicka et al., 2020). Concurrently with this projected increase in the proportion of older adults, there will be increased age-related conditions, such as reduced muscle mass leading to mobility limitations, or social factors, such as social isolation leading to a higher risk of prolonged confinement indoors (Schirghuber & Schrems, 2021a). Evidence from a systematic review indicates that factors such as climate change and mobility limitations among older adults worldwide contribute to prolonged periods of home confinement, a term coined as homebound (Engberg et al., 2001).
Homebound status has been defined differently across the literature. Collectively, the definitions of homebound status have been broadly grouped into two conceptual categories: (1) confinement, which refers to limited ability to leave the home and/or insufficient resources or assistance to do so (Engberg et al., 2001; Ko & Noh, 2021); and (2) infrequent going outside the house, which reflects reduced out-of-home activity shaped by physical, social, psychological, and environmental factors (Umegaki et al., 2015). For example, Lee et al. (2022) defined homebound status as individuals who consistently stay home for a certain period (such as a week or month) without leaving home for specific purposes such as shopping, leisure walking, medical appointments, community engagements, or attending work and social activities. Furthermore, other studies have defined homebound status as situations where individuals have limited out-of-home visits, such as once a month, week, or cannot leave their home independently (Soones et al., 2017; Xiang et al., 2020). Other studies have described homebound status as individuals facing mobility limitations and chronic diseases that make it difficult to leave their home (Schirghuber & Schrems, 2021b; Zhao et al., 2019).
Discrepancies and inconsistencies in the definition of homebound status have led to varied prevalence rates globally. In countries such as Japan, the United States, Israel, Spain, France, the United Kingdom, and China reported prevalence estimates ranged from 3.5% to 39.8% (Lee et al., 2022). Ko and Noh (2021), in a review of 47 studies, reported a prevalence of 5.6% when evaluating the frequency of leaving the home and a rate of 19.6% when considering functional disability as a reason for staying at home. Similar trajectories of prevalence have been documented in Canada, specifically within the long-term care system, with a prevalence of 30% in the span of 4–12 months period (Lapointe-Shaw et al., 2022). Therefore, one of the aims of our review is to reconceptualize the definition of homebound status and provide additional guidance or a framework to develop a more comprehensive understanding of this population.
Reviews on homebound status among older adults exist, most focusing on multidimensional factors affecting homebound older adults (Lee et al., 2022), social issues, such as loneliness (Ezeokonkwo et al., 2021), and the use of technological interventions to reduce social isolation among older adults who are homebound (Tan et al., 2024). Other reviews have focused on outcomes of home-based primary care programs (Sabetfakhri, 2023) and access to non-primary healthcare services (Ezeokonkwo et al., 2021; Tan et al., 2024) in the homebound population. However, despite this rich body of literature, none have specifically addressed the challenges of identifying homebound individuals or the methods used to do so. This gap is significant because the inability to systematically identify homebound older adults hampers efforts to address their needs, making it a critical social issue with far-reaching health and social consequences. Without a clear understanding of how to properly identify this population, efforts to mitigate their risks and improve their quality of life remain limited.
We conducted a preliminary search of OVID MEDLINE® and the Open Science Framework, a free, open-source platform for the preregistration of studies, including scoping reviews. We found no evidence of existing systematic or in-progress scoping reviews that address how to identify homebound older adults or the challenges associated with their identification. We chose a scoping review over other reviews, such as a systematic review, to identify the types of available evidence and the key features of strategies employed globally for identifying/recruiting homebound older adults. Our review aims to reconceptualize how homebound status is defined within the aging population and to describe the methods used to identify homebound older adults, including the challenges associated with this process.
Methods
This scoping review was guided by the methodological framework proposed by Arksey & O’Malley (2005) and was reported following the Preferred Reporting Items for Systematic Review and Meta-Analyses extension for scoping reviews (PRISMA-Scr) (Tricco et al., 2018). The five stages included: (1) identifying the research question, (2) identifying the relevant studies, (3) selecting studies, (4) charting the data, and (5) summarizing and reporting the findings (Arksey & O’Malley, 2005). The study protocol was preregistered at Open Science Framework (Kumapayi et al., 2024).
Stage 1—Identifying the Research Question
This review is guided by three research questions: (a) How has homebound status been defined in the literature concerning the aging population? (b) What methods are used to identify homebound older adults? (c) What are the challenges associated with the process of identifying homebound older adults?
Stage 2—Identifying Relevant Studies and Study Selection
Search Strategy
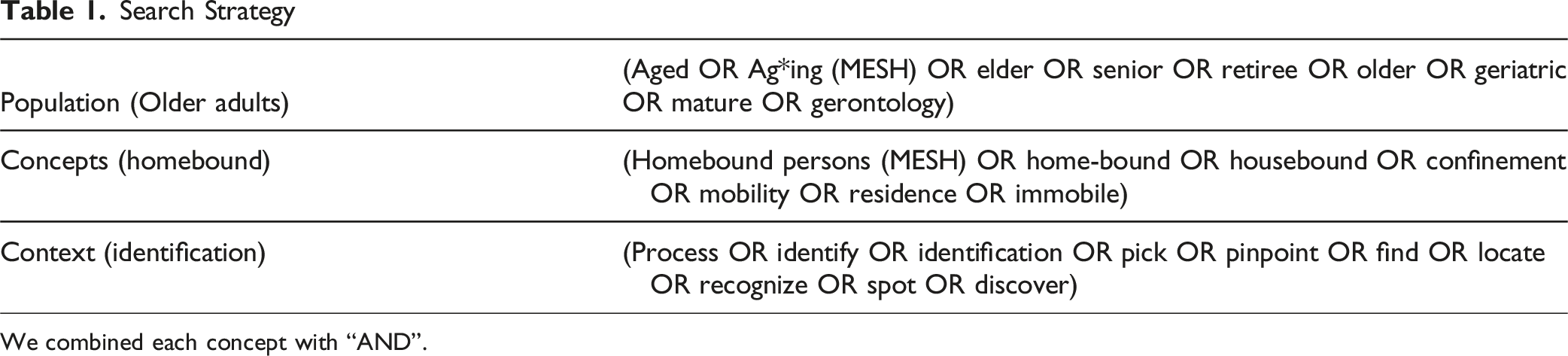
We combined each concept with “AND”.
Stage 3 - Selecting Studies
All citations were exported into Covidence©, a platform designed to streamline systematic review processes by enhancing efficiency and maintaining transparency. Covidence facilitates the removal of duplicate citations, ensuring a clean dataset for study selection. The study selection process was conducted in two stages: initial screening of titles and abstracts, followed by full-text review. Each screening stage was done with predefined inclusion and exclusion criteria in Box 1. Each stage was pilot tested to ensure every individual understood the inclusion and exclusion criteria. Four authors piloted the first 50 articles of the title and abstract screening. We calculated the inter-reliability with a Kappa of 0.70, indicating moderate agreement (DeVellis, 2005). As a result of the agreement, title/abstract screening and full-text screenings were done in pairs; any disagreement was resolved by a third reviewer or discussion in a research meeting every week. An article is included if a. It provided detailed descriptions of recruitment strategies that would enable us to understand how homebound older adults can be identified. b. The mean age of the study population was 60 years and above, residing in the community in their home, assisted living, senior housing, retirement home, or any home without 24-hour medical care. c. It was a peer-reviewed publication, including qualitative, quantitative, mixed-methods studies, or other forms such as co-creation or opinion papers. We included opinion papers because, in this emerging area of research, insights from expert perspectives can offer valuable context and help explain why this topic is rarely studied. d. It was published in the English language Articles were excluded if the a. Participant resides in a nursing home or long-term care facility with 24-hour medical care, or those admitted to the hospital. There was no year restriction during the database searches (i.e., each database was searched from inception till September 2025), and in selecting the included articles provided they meet the criteria.Box 1. Inclusion and Exclusion Criteria
Stage 4—Charting the Data and Synthesis
Results
Of the 24518 citations retrieved from databases and websites, 3,945 duplicates were removed. After screening titles and abstracts, 20532 articles were excluded, leaving 39 for full-text review. Ultimately, 19 articles were included in the review (see Figure 1). PRISMA Chart of the Scoping Review Process obtained from Covidence©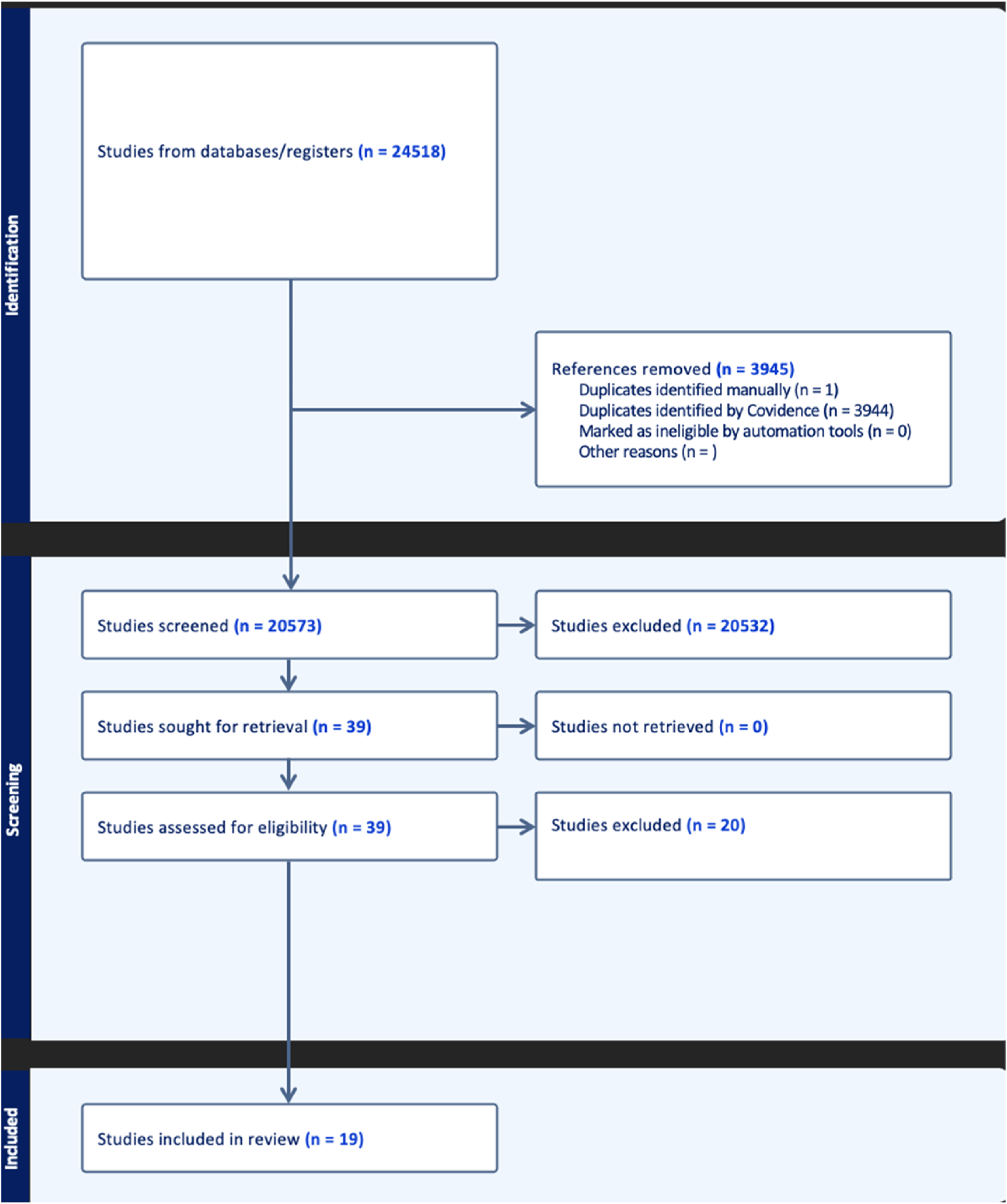
Characteristics of the Articles Included
Study Characteristics
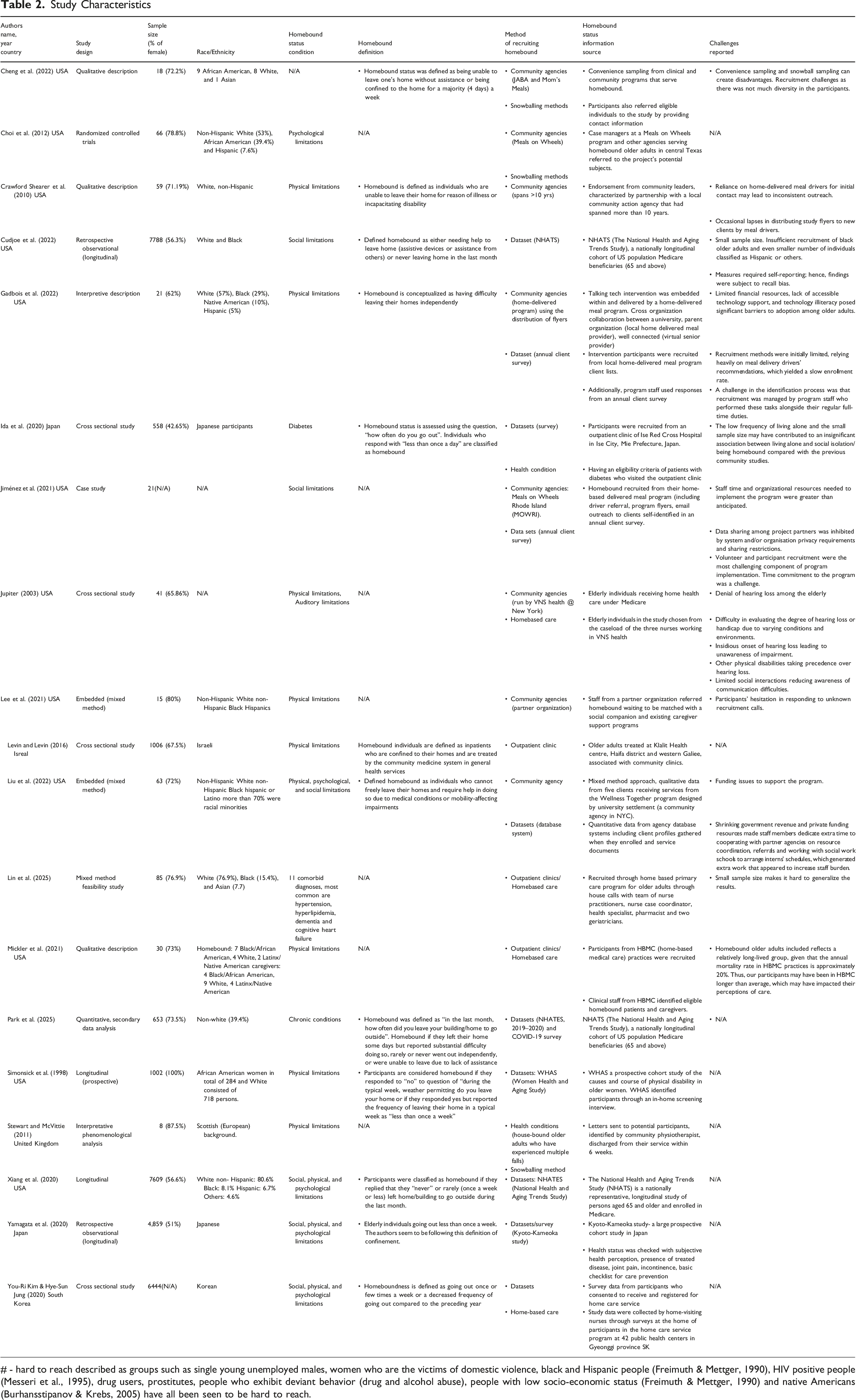
# - hard to reach described as groups such as single young unemployed males, women who are the victims of domestic violence, black and Hispanic people (Freimuth & Mettger, 1990), HIV positive people (Messeri et al., 1995), drug users, prostitutes, people who exhibit deviant behavior (drug and alcohol abuse), people with low socio-economic status (Freimuth & Mettger, 1990) and native Americans (Burhansstipanov & Krebs, 2005) have all been seen to be hard to reach.
Study Design
Study designs were quantitative (n = 11), qualitative (n = 4), mixed methods (n = 3), and a case study (Crawford Shearer et al., 2010). The quantitative studies comprised eight cross-sectional and three longitudinal designs. The qualitative studies included three descriptive and one phenomenological, while the three mixed-method studies employed a convergent parallel design. Sample sizes in qualitative studies ranged from 8 (Stewart & McVittie, 2011) to 59 (Crawford Shearer et al., 2010), whereas quantitative and mixed-method studies ranged from 15 (Lee et al., 2021) to 7788 (Cudjoe et al., 2022).
Study Settings
Most articles (n = 14) recruited participants from their homes, while others (n = 5) recruited from settings including
Study Population
Eighteen studies included older adults with diverse health conditions, such as physical impairments (Cheng et al., 2022; Crawford Shearer et al., 2010; Lee et al., 2021; Levin & Levin, 2016; Liu et al., 2022), cognitive, and psychological issues including depressive symptoms (Cheng et al., 2022; Choi et al., 2012; Gadbois et al., 2022; Kim & Jung, 2022; Mickler et al., 2021; Xiang et al., 2020) and dementia (Lee et al., 2021; Simonsick et al., 1998; Xiang et al., 2020). Additional conditions encompassed heart disease (Lin et al., 2025; Mickler et al., 2021), diabetes (Ida et al., 2020; Mickler et al., 2021), lung disease (Mickler et al., 2021), vision impairment (Mickler et al., 2021), hearing problems (Jupiter, 2003; Mickler et al., 2021), bowel incontinence (Mickler et al., 2021; Yamagata et al., 2020), hypertension, and hyperlipidemia (Lin et al., 2025). Four articles reported participants experiencing social isolation (Cudjoe et al., 2022; Gadbois et al., 2022; Jiménez et al., 2021; Liu et al., 2022).
Among the nineteen studies, one featured exclusively female participant (Simonsick et al., 1998), fifteen had a higher proportion of females than males (Cheng et al., 2022; Choi et al., 2012; Crawford Shearer et al., 2010; Cudjoe et al., 2022; Gadbois et al., 2022; Jupiter, 2003; Lee et al., 2021; Levin & Levin, 2016; Lin et al., 2025; Liu et al., 2022; Mickler et al., 2021; Park et al., 2025; Stewart & McVittie, 2011; Xiang et al., 2020; Yamagata et al., 2020), one had more males (Ida et al., 2020), and two did not report sex distribution (Jiménez et al., 2021; Kim & Jung, 2022). Racially, eight studies predominantly included Non-Hispanic White participants (Choi et al., 2012; Gadbois et al., 2022; Lee et al., 2021; Lin et al., 2025; Liu et al., 2022; Park et al., 2025; Simonsick et al., 1998; Xiang et al., 2020), or only Non-Hispanic Whites (Crawford Shearer et al., 2010), with three having more Black participants (Cheng et al., 2022; Cudjoe et al., 2022; Mickler et al., 2021). Participants from diverse ethnic backgrounds were recruited in five studies, including Japanese, Scottish, Israeli, and Korean populations (Ida et al., 2020; Kim & Jung, 2022; Levin & Levin, 2016; Stewart & McVittie, 2011; Yamagata et al., 2020), whereas two studies did not specify race or ethnicity (Jiménez et al., 2021; Jupiter, 2003).
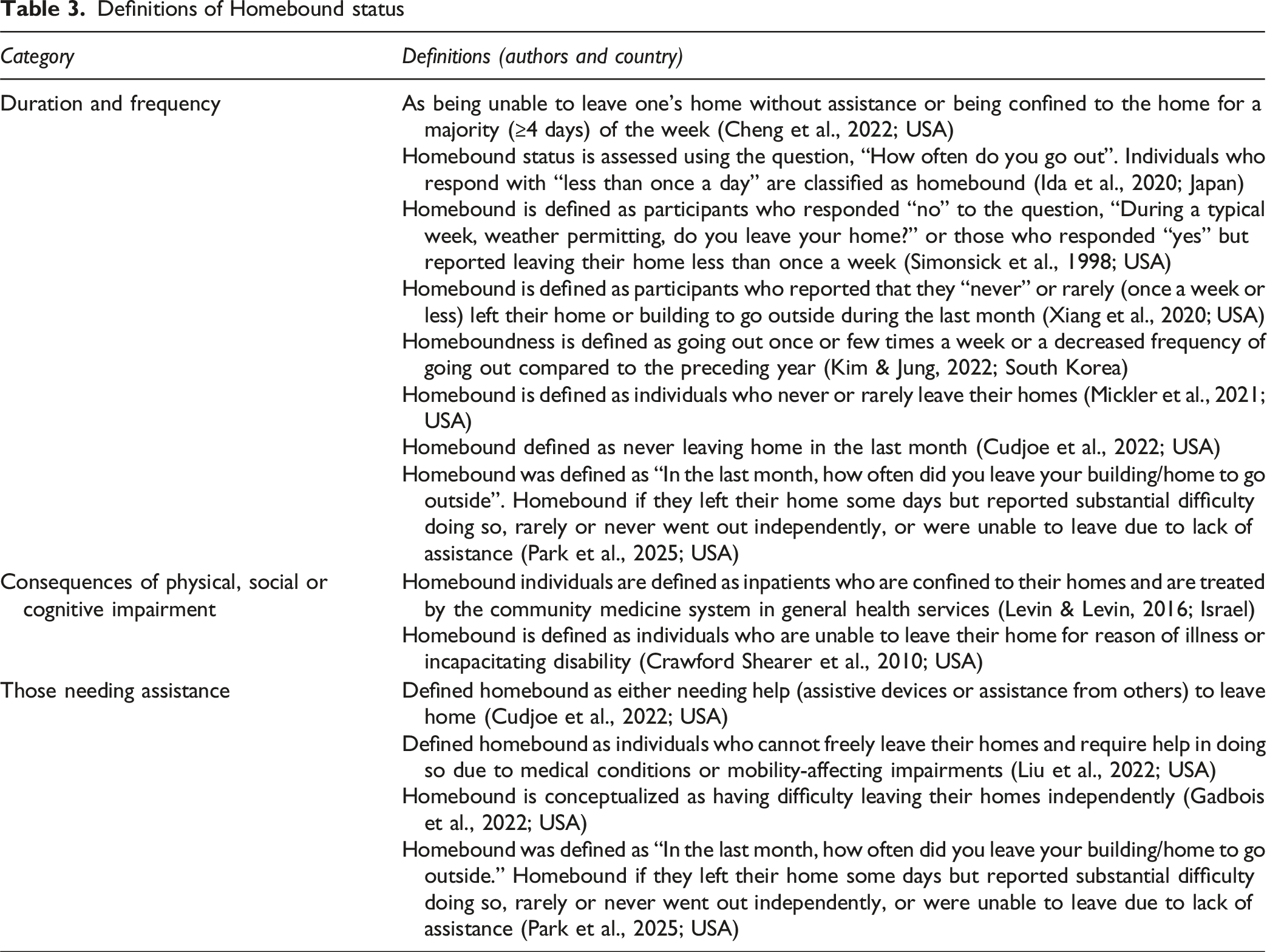
Definition of Homebound (what)
Definitions of Homebound status
Identification Process (How)
Our analysis found that homebound older adults were identified through: (a) community agencies (eight studies—Cheng et al., 2022; Choi et al., 2012; Crawford Shearer et al., 2010; Gadbois et al., 2022; Jiménez et al., 2021; Jupiter, 2003; Lee et al., 2021; and Liu et al., 2022); (b) outpatient clinics (five studies—(Jupiter, 2003; Kim & Jung, 2022; Levin & Levin, 2016; Lin et al., 2025; and Mickler et al., 2021); (c) snowball sampling techniques (three studies—Cheng et al., 2022; Choi et al., 2012; Stewart & McVittie, 2011); (d) assessment of health conditions (two studies—Ida et al., 2020; Stewart & McVittie, 2011); and use of dataset (ten studies (Cudjoe et al., 2022; Gadbois et al., 2022; Ida et al., 2020; Jiménez et al., 2021; Kim & Jung, 2022; Liu et al., 2022; Park et al., 2025; Simonsick et al., 1998; Xiang et al., 2020; Yamagata et al., 2020). It is important to note that some studies utilized more than one of these strategies.
Community Agencies
Identification through community agencies was one of the most prevalent methods for recognizing homebound older adults. These agencies were primarily private nonprofit organizations in the United States that offer services such as Meals on Wheels (Cheng et al., 2022; Choi et al., 2012; Crawford Shearer et al., 2010; Gadbois et al., 2022; Jiménez et al., 2021; Liu et al., 2022) or Medicaid-funded visiting nursing programs (Jupiter, 2003; Lee et al., 2021). These organizations, for example, Meals on Wheels delivers nutritious meals tailored to older adults’ needs, requiring recipients to be aged 65 or older, disabled, needing assistance with grocery shopping, and enrolled in a Medicaid Advantage plan. These organizations often inform healthcare professionals or researchers about older adults who are homebound.
Outpatient Clinics and Home Care Visits
Outpatient clinics and home care visits were common methods for recruiting homebound older adults. In Israel (Levin & Levin, 2016), older adults visiting hospitals were asked to self-identify as homebound during consultations, procedures, or treatments. In the USA, studies (Jupiter, 2003; Lin et al., 2025; Mickler et al., 2021) reported identifying homebound individuals through home care visits in which physicians or healthcare providers visit patients’ homes to provide social or healthcare services. One study conducted in South Korea (Kim & Jung, 2022) recruited homebound older adults through home-visiting nurses who provided care as part of a home care service program.
Snowballing Method
Snowballing method, defined as a recruitment technique where existing study participants refer or recruit other eligible individuals, was one of the approaches used to identify homebound older adults. Some studies reported that older adults were referred by peers who also identified as homebound (Cheng et al., 2022), while healthcare professionals providing care observed and reported the likelihood of certain individuals being homebound (Cheng et al., 2022; Choi et al., 2012; Stewart & McVittie, 2011).
Use of Dataset
The use of large, often longitudinal datasets, including the National Health and Aging Study (Cudjoe et al., 2022; Park et al., 2025; Xiang et al., 2020), Kyoto-Kameoka study (Yamagata et al., 2020), and the Women’s Health and Aging Study (Xiang et al., 2020), was common for identifying homebound older adults. These datasets facilitated population-level analyses to derive indicators and predictors of homebound status. Cudjoe et al. (2022) utilized a representative sample of 7,788 Medicare beneficiaries aged 65+ from 2011 to 2019, assessing the odds of becoming homebound based on social isolation, and found that socially isolated older adults were more likely to become homebound both at baseline and over time. Similarly, Xiang et al. (2020) utilized a representative sample of 7,607 Medicare beneficiaries aged 65+ from 2011 to 2017, examining the trajectories of homebound status and shaping risk factors. They identified three trajectories: never, onset, and chronic. Most participants remained non-homebound (never, 65.5%); a smaller group was persistently homebound (chronic, 8.3%); and the onset group (26.2%) showed a rapid rise in homebound risk over 7 years. Compared with the never group, a higher risk of onset/chronic status was associated with older age, Hispanic ethnicity, social isolation, past/current smoking, IADL limitations, probable dementia, and use of a walker or wheelchair. Park et al. (2025) utilized public-use data files from the NHATES main surveys for 2019–2020, supplemented with the 2020 COVID-19 survey, with a sample of 3961, to highlight that providing information and communication technology (ICT) is not sufficient to reduce e-health disparities among homebound older adults.
Simonsick et al. (1998) utilized the Women’s Health and Aging study, a prospective cohort study consisting of 1002 moderately to severely disabled community-dwelling Medicare beneficiaries women age 65 +, assessing association of disability and social interaction, and found that older age, lower levels of education attainment, driver at home, hearing difficulties, incontinence and African American race were related to home confinement and low social contact. Lastly, Yamagata et al. (2020) utilized the Kyoto-Kameoka study, a prospective cohort study of 6,696 community-dwelling adults aged 65 years and older in Japan, to examine 2-year changes in confinement and related factors. Among 375 participants, most (86.9%) remained in the non-confinement group. Low social role was associated with a higher likelihood of becoming confined, whereas improvements were observed among those with no medical conditions and higher intellectual activity. In addition to large datasets such as NHATS and WHAS, several studies (Gadbois et al., 2022; Ida et al., 2020; Jiménez et al., 2021; Kim & Jung, 2022; Liu et al., 2022) used annual client surveys containing client-profile information as a supplementary approach to identify homebound older adults enrolled in programs or services.
Health Conditions
Findings from 2 studies were mapped based on health conditions, as they all involved recruitment of homebound older adults with various limitations (Ida et al., 2020; Stewart & McVittie, 2011). Stewart and McVittie (2011) recruited participants through a community physiotherapy service, targeting individuals recently discharged after experiencing multiple falls due to physical disability. In contrast, Ida et al. (2020) recruited homebound older adults diagnosed with diabetes, including classifications of type 1, type 2, and prediabetes.
Challenges in Identifying Homebound Older Adults
Sampling and recruitment challenges were prevalent in studies included in this review. Cheng et al. (2022) noted that their reliance on convenience and snowball sampling methods resulted in limited participant diversity, potentially undermining the generalizability of their findings. This limitation may stem from the nature of snowball sampling, which relies on participant referrals. Such referrals often lead to the recruitment of individuals with similar characteristics, thus introducing sampling bias (Cheng et al., 2022). Some studies also depended on meal delivery services for recruitment, which created inconsistent outreach and delays in the distribution of recruitment flyers to potential participants, ultimately slowing enrollment rates (Liu et al., 2022; Gadbois et al., 2022). Additionally, programs requiring meal delivery drivers, such as Meals-on-Wheels, demanded increased staff time and resources (Liu et al., 2022; Mickler et al., 2021). Also, it is important to realize that there were no specific studies on the identification of homebound older adults; however, the included articles reported the recruitment process in their methods section.
Discussion
To the best of the authors’ knowledge, this is the first review to explore existing literature on the identification process of homebound older adults globally. This review specifically explored the “what” (definitions associated with homebound status), the “how” (identification processes employed), and the challenges associated with the recruitment process.
We noted a pattern in the homebound status definition that varies significantly across different healthcare systems. In studies conducted in the United States, the definition is primarily centered on the duration of an individual’s indoor confinement, as well as any physical incapacities that hinder their ability to leave home and necessitate care (Musich et al., 2015). This aligns closely with the Medicare Home Care Benefit Criteria, which emphasizes that the homebound older adults must be under the care of a physician, need skilled services, and have physical limitations that prevent exit from their home (Ornstein et al., 2015). Conversely, research from countries with universal healthcare, such as Japan, Israel, and South Korea, expands the definition of homebound status to encompass not only physical abilities but also social, environmental and cognitive factors that reduces the frequencies a person leave their home (Ida et al., 2020; Kim & Jung, 2022; Levin & Levin, 2016; Yamagata et al., 2020). These studies suggest that an individual may be classified as homebound even if they possess the physical capability to leave their home, indicating a more nuanced understanding of the concept that accounts for psychological and social influences. This disparity in definitions underscores the varying approaches to addressing homebound needs across different healthcare systems. Such variations may serve as potential reasons for the challenges in identifying individuals who qualify as homebound. Moreover, the absence of a standardized definition presents significant hurdles in accurately understanding the relationship between these definitions and the recruitment processes for homebound older adults. Therefore, researchers, clinicians, older adults at risk of becoming homebound, and their families must engage in collaborative discussions. Through this exchange, stakeholders can work towards establishing a cohesive global definition or set of criteria for homebound status, which is essential for addressing the needs of an aging population worldwide.
An objective of the review was to describe the “how” or process of identifying homebound older adults. However, to date, there is a lack of empirical studies in this area. Consequently, we shifted our focus to examining how existing studies have recruited participants identified as homebound. Among the strategies employed, endorsements from community-based leaders, organizations, and the use of datasets emerged as the most prominent method for recruiting homebound older adults. This is largely due to the established trust and rapport that these leaders and organizations have within their communities, which can significantly enhance their outreach to individuals with homebound status (Spencer et al., 2018). These organizations are typically well-aware of the specific needs and preferences of residents, allowing them to craft tailored messages that resonate with the homebound audience, thereby driving collective action (Kaholokula, 2024). These findings underscore the wealth of knowledge that community-based organizations and leaders possess regarding the identification of homebound status, making them the ideal first point of contact. The absence of empirical evidence outlining the process for identifying homebound status highlights the necessity for such studies, with involvement of community-based organizations and leaders serving as a promising starting point.
Themes of over-reliance on meal delivery drivers and potential recall bias among participants emerged as potential challenges when recruiting “hard to reach” populations. These findings may reflect the labor-intensive and time-consuming nature of recruiting homebound older adults, as meal delivery drivers spend considerable time traveling between visits and distributing flyers (Cohen-Mansfield et al., 2010; Ritchie & Dennis, 1999). Additionally, meal delivery drivers often need to take a proactive approach to build rapport and ensure that homebound individuals feel comfortable allowing them into their homes; this process can be stressful (Cohen-Mansfield et al., 2012). As such, meal delivery drivers can become overwhelmed with the tasks of both delivering meals and intentionally identifying those who are homebound. There is an ethical concern regarding the use of meal delivery drivers as champions of identifying homebound individuals, as it may be seen as a breach of privacy. We emphasize the importance of ensuring that meal delivery drivers understand these ethical considerations; drivers can be trained to obtain informed consent from older adults whom they perceive as homebound. Further research is needed to determine how the use of meal delivery drivers would be beneficial in identifying homebound older adults.
Study Limitations
While our review has expanded the evidence on the phenomenon of homebound among older adults, there are some limitations. First, although we ensured that all eligible studies that passed the inclusion criteria were included in the review, we could still have omitted some articles as a result of search engines utilized that might not include articles from regions like Africa. Also, by limiting the inclusion criteria to only homebound older adults residing at home, we may have excluded articles that combine homebound older adults residing at home and long-term care. Lastly, overlap among identification methods across studies may have increased the risk of misclassification. To mitigate this, we assigned each article to a recruitment category (e.g., endorsement from community agencies) based on the recruitment details reported in the manuscript and a content analysis conducted by a senior researcher. Although some interpretive judgment was unavoidable given variation in reporting and the use of multiple approaches within some studies, we believe our categorizations are consistent with the available evidence. Readers are nevertheless encouraged to consider this when interpreting the review findings.
Conclusion
We identified multiple factors for each category of what, how, and challenges of identifying homebound older adults (60 and above) globally. The review showed the disparity in definitions of “homebound” across healthcare systems, with some countries adopting broader criteria that allow for more inclusive identification. Factors contributing to the identification of homebound older adults were categorized into five domains: health conditions, endorsements from community agencies, snowballing methods involving family members or caregivers, referrals from outpatient clinics, and datasets. These variations in definitions create significant barriers to accurately identifying homebound individuals, ultimately hindering the delivery of appropriate services and support. Therefore, establishing a consensus definition of homebound status is essential for ensuring consistency in identifying and addressing the needs of this population.
Supplemental Material
Supplemental material - How Are Homebound Older Adults Identified? Definitions, Approaches, and Challenges—A Scoping Review
Supplemental material for How Are Homebound Older Adults Identified? Definitions, Approaches, and Challenges—A Scoping Review by Peace Kumapayi, Blessing Ugochi Ojembe, Amanda Grenier, Ethan Chan, Prince Onyekere, Benita Ugwu, Ravjyot Ughra, and Michael E Kalu in Journal of Applied Gerontology.
Footnotes
Acknowledgments
We want to acknowledge Emerging Research and Professionals in Aging-African Network (ERPANN) for their support and for allowing us to involve some of their members in this research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by Social Science Humanities Research Council (SSHRC) Insight Development Grant (430-2024-0110); SSHRC Undergraduate Student Research Award; and York University Black Seed Grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.