
Abstract
This study examines nativity differences in the relationship between living arrangement (living alone, with one other, or with two or more people) and cognitive impairment in older Mexican Americans (≥75 years) with moderate to high cognitive function at baseline. Using 12-year longitudinal data from 1,026 participants in the Hispanic Established Population for the Epidemiological Study of the Elderly, generalized estimating equation models revealed that US-born participants living with one other or two or more individuals had significantly higher odds of developing cognitive impairment than those living alone, whereas no significant association was observed among foreign-born participants, after adjusting for all covariates. These findings indicate that cognitive change over time for older adults in different living arrangements differs by nativity. These results emphasize the importance of considering both nativity and household structure when developing interventions to preserve cognitive function among diverse older adult populations.
• This paper investigated nativity differences in the relationship between living arrangement and cognitive impairment in older Mexican Americans. • This study highlights that living with others, compared to living alone, is linked to a heightened odds of cognitive impairment specifically among US-born older adults, pointing to nativity as a critical determinant. • This study emphasizes the importance of considering socio-cultural factors when examining the interplay between household composition and cognitive health in diverse aging populations.
• These findings can help clinicians and community practitioners employ tailored strategies that consider both nativity and living arrangement to better support cognitive health in older adults. • The results support the development of policy initiatives that promote tailored community-based support services for aging populations with diverse cultural backgrounds and household structures. • This study encourages further research to explore the role of nativity and its interplay with other social factors that influence cognitive trajectories among older adults.What This Paper Adds
Applications of Study Findings
Introduction
Mexican Americans represent approximately 57.7% of all Hispanic/Latino in the United States (Peña et al., 2023). In 2023, the Hispanic/Latino population accounted for 19.5% of the U.S. population. It is projected to increase from 19.1% in 2022 to 26.9% in 2060, while the Non-Hispanic White population is projected to decrease from 58.9% on 2022 to 44.9% in 2026 (U.S. Census Bureau, 2023). Despite the strides made in healthcare accessibility and quality in the United States, disparities in morbidity and mortality rates persist, revealing a complex interplay of factors that influence health across racial and ethnic groups (Hummer & Gutin, 2018; Moon et al., 2021; Shariff-Marco et al., 2020; To, 2017; Weden et al., 2017). The health of the Mexican American population carries significant public health implications, particularly in light of research pointing to a higher prevalence of cognitive impairment and dementia among older Hispanics/Latinos compared to their non-Hispanic/Latino white counterparts. For example, older Hispanics/Latinos are at 1.5 times greater risk for Alzheimer’s disease and other forms of dementia in late life than non-Hispanic/Latino whites, displaying symptoms of cognitive impairment 7 years earlier (Wu et al., 2019). Moreover, dementia prevalence rises steeply with age—about 13% among those 75–84 and 33% among those ≥85—underscoring the importance of studying cognitive health in the “oldest-old” (“2024 Alzheimer’s Disease Facts and Figures,” 2024). While genetic and behavioral factors contribute to these disparities, research has demonstrated the significant role of socioeconomic conditions in shaping cognitive health outcomes (Muhammad et al., 2022).
Living arrangements can shape cognitive aging through multiple pathways that operate both inside and outside the household. One important mechanism is social engagement, defined as the frequency and quality of interactions and participation in social activities, which has been linked to lower dementia risk; conversely, social isolation and loneliness have been associated with higher risk (Kuiper et al., 2015; Livingston et al., 2024). Although household size is often used as proxy for opportunities for social interaction, the relationship is not consistently positive. Larger household size may provide more interpersonal contact, emotional support, and shared daily activities that promote social engagement and contribute to the development of cognitive reserve, consistent with cognitive reserve theory (Bougea et al., 2022; Cardona & Andrés, 2023). However, household size alone does not ensure meaningful engagement. Loneliness and social isolation can persist even in larger or crowded households (Greenfield & Russell, 2010). Alternatively, the stress process model for individuals with dementia suggests that co-residential settings can introduce support burden and household strain through caregiving demands, role overload, conflict, crowding, and financial stress, which can elevate chronic stress and undermine cognition (Judge et al., 2010). Finally, the environmental press framework posits that outcomes depend on the fit between personal competence and environmental demands; both solitary and crowded households may present challenges (e.g., under-stimulation vs. over-demand), with implications for cognitive trajectory (Wolf et al., 2021).
Nativity can systemically shape these pathways. The convoy model of social relations emphasizes that the size, composition, and function of one’s social networks vary across the life course and across cultural contexts (Fuller et al., 2020). Immigrant older adults often maintain larger kin-oriented networks and are more likely to reside in multigenerational households, whereas US-born peers are more likely to live alone (Gubernskaya & Tang, 2017). In Mexican-origin families, familism and cultural norms of intergenerational caregiving can increase co-residence and reliance on family care, but these same norms can produce strain when expectations collide with resource constraints or acculturation pressures (Crist et al., 2009; Gelman, 2014). In short, nativity may moderate how living arrangements map onto social engagement and household strain, and therefore onto cognitive change.
In this framework, living arrangement is a time-varying structural context that influences social engagement and support burden/household strain, both of which in turn affect cognitive reserve. The objective of this study was to determine nativity differences in the relationship between living arrangement and cognitive impairment among Mexican American older adults over 12 years of follow-up among those with moderate to high cognitive function at baseline. We hypothesize that an increased number of household members will be associated with increased odds of cognitive impairment over time, and that this association will vary by nativity status, reflecting differences in the social and cultural context of co-residence.
Materials and Methods
Sample
The data used in this study were drawn from the Hispanic Established Population for the Epidemiological Study of the Elderly (H-EPESE), a longitudinal cohort study of non-institutionalized Mexican American older adults who resided in Arizona, California, Colorado, New Mexico, and Texas. The initial H-EPESE cohort study included 3,050 Mexican Americans aged 65 years and older interviewed in 1993/94. In 2004/05, an additional cohort of 902 participants aged 75 years and older were added to those who survived from the original cohort (N = 1,167) aged 75 years and older (total N = 2,069). This new cohort was recruited to replenish and maintain the representativeness of this population, particularly those reaching older ages after the original baseline. Interviews in English or Spanish were conducted every 2 or 3 years by trained interviewers to gather information on participant socio-demographics, health conditions, and psychosocial characteristics. Information on the survey contents and datasets is available at the National Archive of Computerized Data on Aging (K. Markides et al., 2016).
The present analysis used data from Waves 5–9 (2004/2005–2016). Appendix Figure 1 shows the process of cohort selection. As we were interested in examining the effect of living arrangement and nativity on changes in cognitive function in those with moderate or high cognitive function at baseline, we excluded those who scored less than 21 in the Mini Mental State Examination (MMSE) at baseline (N = 441). Of the 2,069 participants interviewed at Wave 5, we also excluded 602 with missing information on any of the variables included in the analyses. Compared to those included, excluded participants were significantly more likely at baseline to be older, widowed, foreign-born; to have a lower level of education; to report more falls; to report more depressive symptoms; to have multimorbidity; and to score lower on the Short Physical Performance Battery (SPPB) and handgrip strength (Appendix Table 1). Oral informed consent was obtained from all participants at each wave of interview, and the study protocol was approved by the University of Texas Medical Branch Institutional Review Board (IRB#16-0014).
Measures
Predictor Variables
Living arrangement was assessed by asking participants: “How many people live in this household?” and participants were categorized as living alone, living with one other person, or living with 2 or more people. Living arrangement was measured at each wave and modeled as a time-varying exposure. Participants could transition across categories between interviews.
Nativity was assessed by asking participants: “Where were you born? City, State, Country” and categorized as US-born vs foreign-born.
Outcome Variable
Cognitive function was assessed with the MMSE, a 30-item examination concentrating on the cognitive aspects of mental functions (Folstein et al., 1975). The examination was administered by interviewers who were trained through workshops and videotaped instructions. The Spanish version of the MMSE meets standardized criteria for translated tests, which includes formal translation, back-translation, and committee consensus approval of the finalized content (Bird et al., 1987). MMSE scores range from 0 to 30, with higher scores indicating better cognitive performance. We defined cognitive impairment as an MMSE score <21, a cut-off previously found to be appropriate for samples of older adults with low education and one previously used with the H-EPESE (Crum et al., 1993; Raji et al., 2010).
Covariates
Selected covariates for analysis included age, sex, years of education, marital status (married, separated, divorced, never married, and widow), language of interview (English vs. Spanish), multimorbidity (two or more of the following: hypertension, arthritis, diabetes, heart failure, heart attack, stroke, cancer, hip fracture, anemia, kidney disease, chronic obstructive pulmonary disease, and thyroid disease), pain on weightbearing, number of falls in the prior year (one or more), depressive symptoms (measured with Center for Epidemiological Studies Depression Scale [CES-D ≥ 16]) (Radloff, 1977), scores on the Short Physical Performance Battery (SPPB) (Guralnik et al., 1995), and hand grip strength test (Al Snih et al., 2002). Covariates were selected based on prior literature linking them to both the exposure and the outcome and thus were treated as potential confounders (Handing et al., 2020; Raji et al., 2010; Saenz et al., 2018; Ventura et al., 2023; Zhang et al., 2024).
Statistical Analysis
Descriptive statistics are presented as mean ± standard deviation (SD) for normally distributed continuous variables. The distribution of normality was tested using the Shapiro–Wilk test. The frequency distributions of categorical variables are presented as numbers and percentages. We used Chi Square and ANOVA tests to compare the baseline characteristics of the sample by living arrangement and nativity status. Generalized estimating equation (GEE) models using the GENMOD procedure in SAS were used to estimate the odds ratio (OR) and 95% confidence interval (CI) of cognitive impairment (MMSE < 21) over 12 years as a function of living arrangement by nativity status. The models used a logit-linked binomial distribution and autoregressive order correlation structure to account for repeated measures of participants (Wedderburn, 1974). In choosing the covariance matrix for GEE, we used Quasi-likelihood (QIC) estimation values. All variables were treated as time-varying, with the potential to change from interview to interview, except for sex, education, and nativity. Participants were classified at each time point based on living arrangement category. For example, a participant who reported living alone at baseline but reported living with another person at the next interview would be reclassified into the corresponding living arrangement category at each time point. The GEE model minimizes selection bias from missing data by using all available information from follow-up interviews, even when follow-up durations vary among participants. It uses all non-missing data pairs to estimate the working correlation structure based on repeated measures for the same participants over time. With these procedures, only the specific missing observations are excluded, instead of removing all measurements from participants with incomplete data (Liang & Zeger, 1986). Participants who refused to participate, died, or were lost to follow-up were included until their last interview date over the 12 years of follow-up. Statistical analyses were performed using the SAS System for Windows version 9.4 (SAS Institute, Inc., Cary, NC).
Results
Characteristics of Study Participants
Baseline Descriptive Characteristics of the Sample by Living Arrangement and Nativity Among Mexican American Older Adults With Moderate to High Cognitive Function at Baseline (N = 1,026)
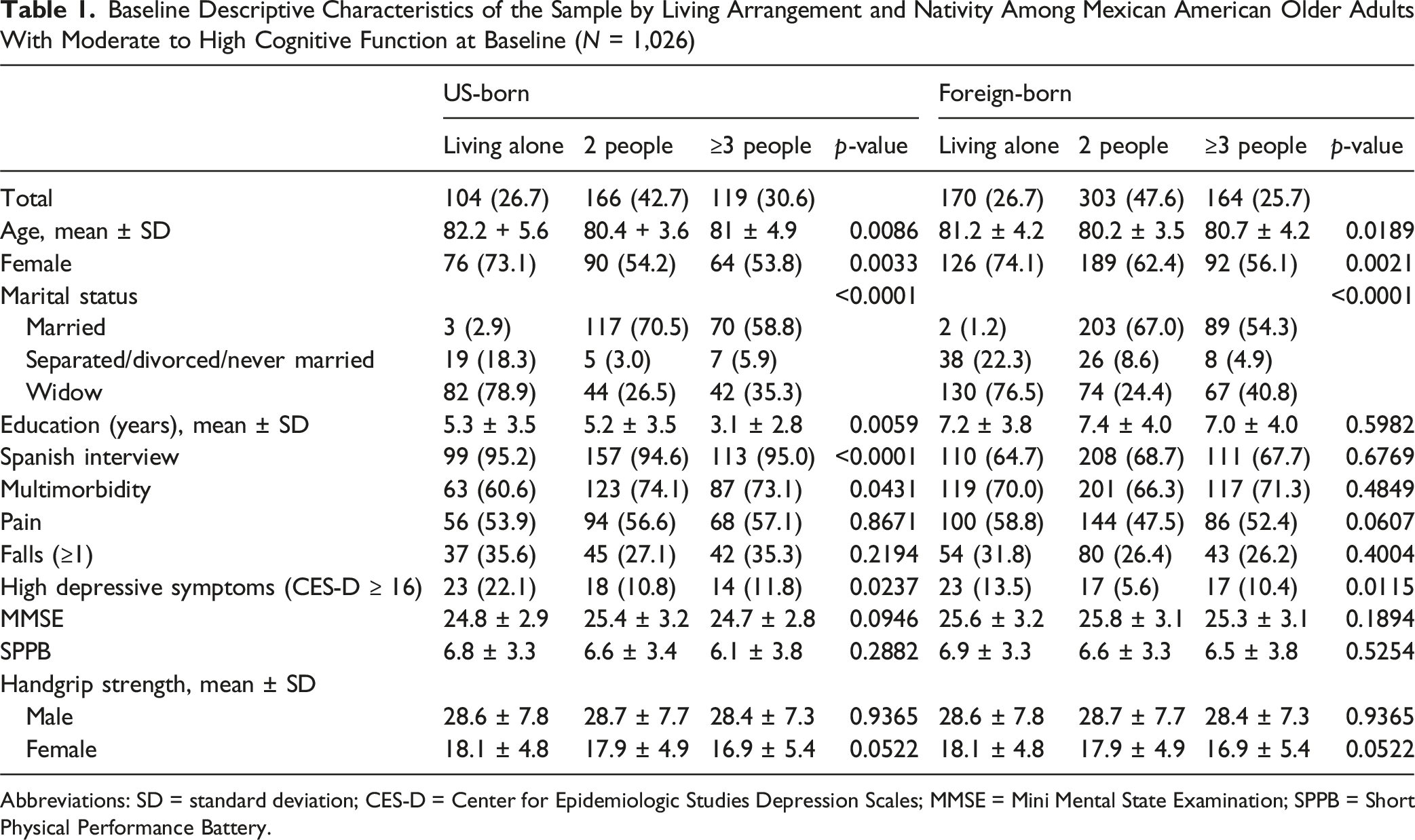
Abbreviations: SD = standard deviation; CES-D = Center for Epidemiologic Studies Depression Scales; MMSE = Mini Mental State Examination; SPPB = Short Physical Performance Battery.
Among US-born participants, 26.7% lived alone, 42.7% lived with one other person, and 30.6% lived with two or more people. Compared to those living alone, those living with two or more people were significantly more likely to be younger (mean age 81 ± 4.9 years vs. 82.2 ± 5.6 years), less likely to be female (53.8% vs. 73.1%), more likely to be married (58.8% vs. 2.9%), have few years of education (mean 3.1 ± 2.8 years vs. 5.3 ± 3.5 years), have more multimorbidity (73.1% vs. 60.6%), and report fewer depressive symptoms (11.8% vs. 22.1%). Similarly, compared to those living alone, those living with one other person were significantly more likely to be younger (mean age 80.4 ± 3.6 years vs. 82.2 ± 5.6 years), less likely to be female (54.2% vs. 73.1%), more likely to be married (70.5% vs. 2.9%), have a comparable level of education (mean 5.2 ± 3.5 years vs. 5.3 ± 3.5 years), be interview in English, and report fewer depressive symptoms (10.8% vs. 22.1%) (Table 1).
Among foreign-born participants, 26.7% lived alone, 47.6% lived with one other person, and 25.7% lived with three or more people. Compared to those living alone, those living with two or more people were significantly more likely to be younger (mean age 80.7 ± 4.2 years vs. 81.2 ± 4.2 years), less likely to be female (56.1% vs. 74.1%), more likely to be married (54.3% vs. 1.2%), and report fewer depressive symptoms (10.4% vs. 13.5%). Similarly, compared to those living alone, those living with one other person were significantly more likely to be younger (mean age 80.2 ± 3.5 years vs. 81.2 ± 4.2 years), less likely to be female (62.4% vs. 74.1%), more likely to be married (67.0% vs. 1.2%), and report fewer depressive symptoms (5.6% vs. 13.5%) (Table 1).
Figure 1 presents the percent distribution by living arrangement (living alone, living with one other person, or living with two or more people) among US-born and foreign-born participants over the study period. We observed that the most common living arrangement category for both US-born and foreign-born was living with one other person. Percent distribution of living arrangements over time among US-born (A) and foreign-born (B) participants over the study period (N = 1,026)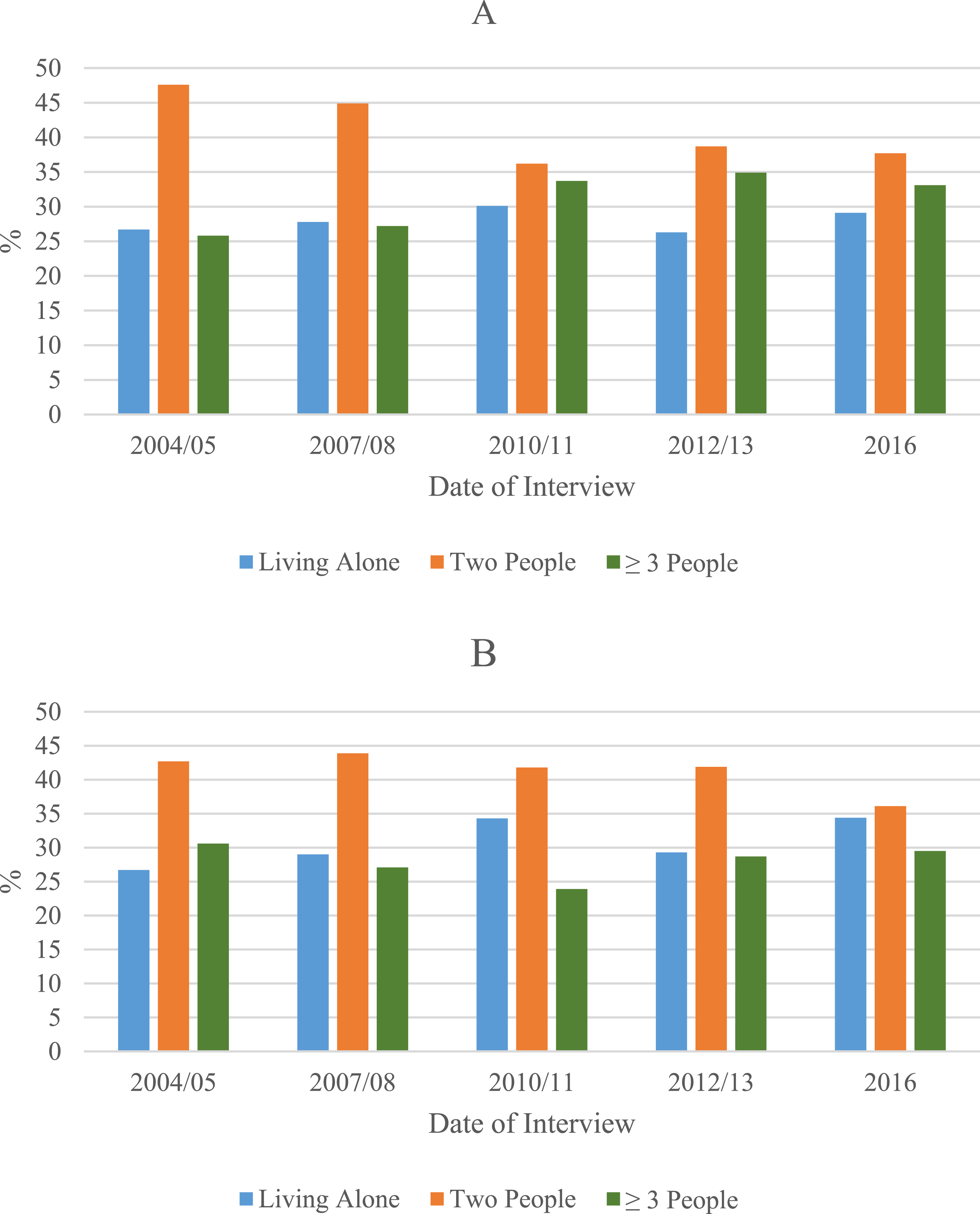
Figure 2 shows the rates of cognitive impairment (MMSE ≤ 21) among US-born and foreign-born participants by living arrangement (living alone, living with one other person, or living with two or more people) over the study period. Among US-born participants, we observed a linear increase of the percent of cognitive impairment as the number of people living in the household increased. Among foreign-born participants, those living alone and those living with two or more people showed a higher percent of cognitive impairment until 2012/2013. In 2016, those living with one other person had the highest percent of cognitive impairment among the three living arrangement groups. Percent of participants with cognitive impairment (MMSE ≤ 21) among US-born (A) and foreign-born (B) participants by living arrangement over the study period (N = 1,026). Abbreviation: MMSE = Mini Mental State Examination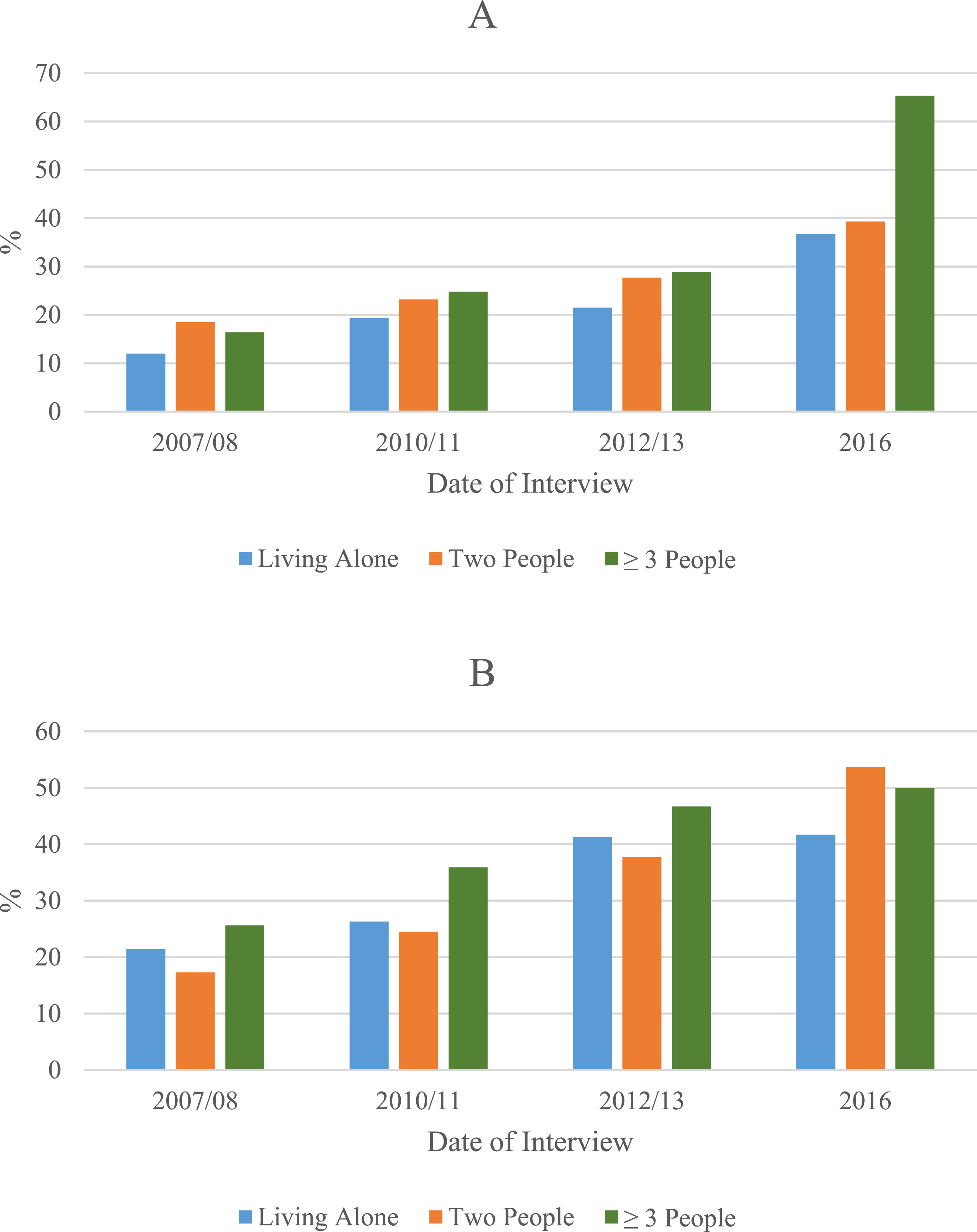
Generalized Estimation Equation Model Results
Generalized Estimation Equation Models for Cognitive Impairment as a Function of Living Arrangement by Nativity Among Mexican American Older Adults With Moderate to High Cognitive Function at Baseline (N = 1,026)
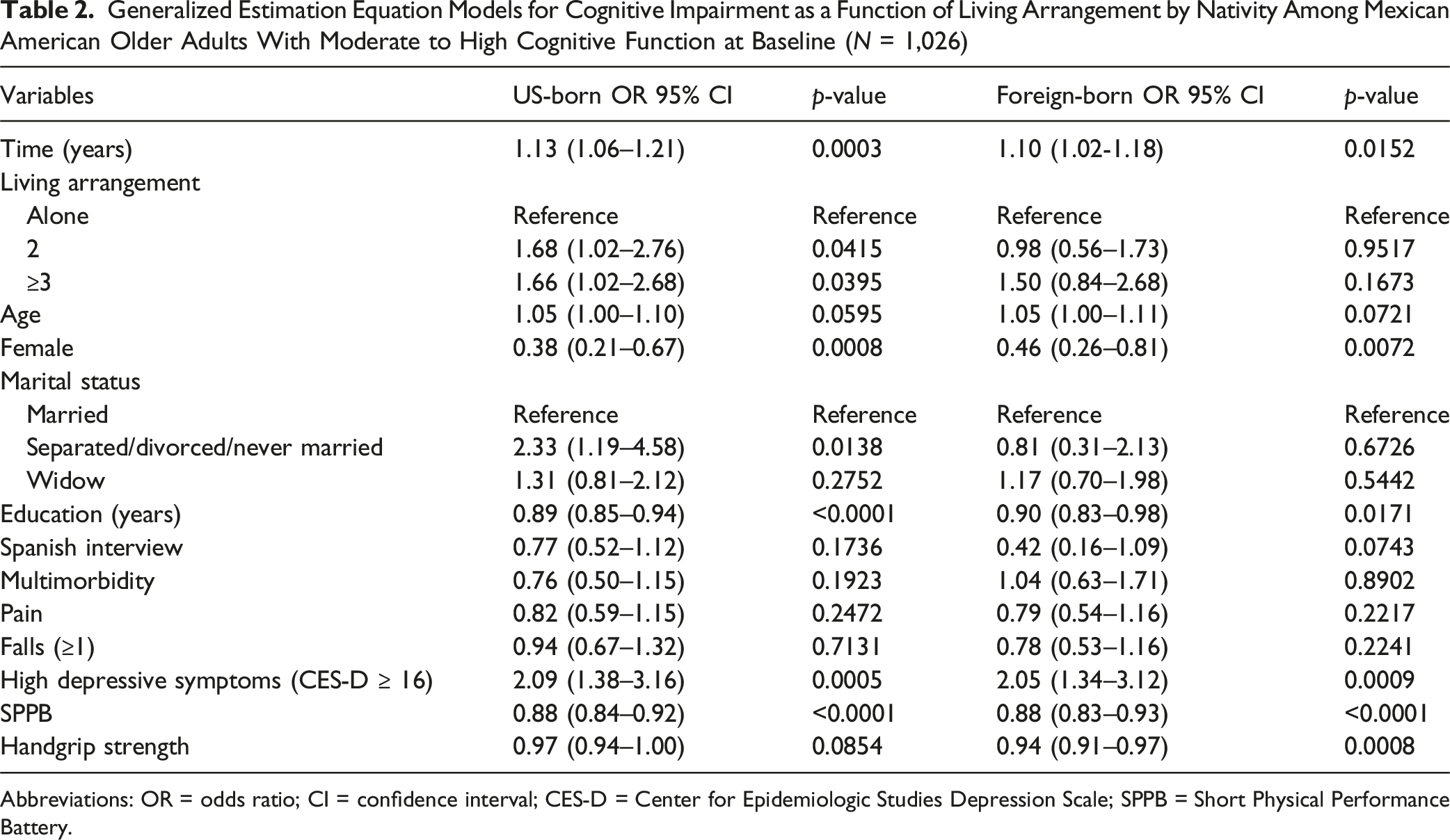
Abbreviations: OR = odds ratio; CI = confidence interval; CES-D = Center for Epidemiologic Studies Depression Scale; SPPB = Short Physical Performance Battery.
Among foreign-born participants, living with one other person or with two or more people was not significantly associated with cognitive impairment over time compared to living alone. After adjusting for all covariates, the odds ratios were 0.98 (95% CI = 0.56–1.73, p = 0.9517) for living with one person and 1.50 (95% CI = 0.84–2.68, p = 0.1673) for living with two or more people. Factors associated with cognitive impairment were the length of follow-up (years), older age, and high depressive symptoms. Female sex, higher levels of education, and higher scores on the SPPB and handgrip strength were associated with lower odds of cognitive impairment over time (Table 2).
Discussion
This 12-year longitudinal study of Mexican American older adults examined the association between living arrangement and cognitive impairment by nativity (US-born vs. foreign-born). The findings revealed that, among US-born participants, those living with one other person or those living with two or more people had 62.7% and 62.4% greater odds of developing cognitive impairment over time, respectively, compared to those living alone, after controlling for all covariates. In contrast, no significant association between living arrangement and cognitive impairment was observed over time among foreign-born participants, after controlling for all covariates. Interpreted through complementary frameworks of cognitive reserve, stress and household strain, and person–environment fit, these results suggest that nativity may moderate how living arrangements influence opportunities for social engagement and the distribution of support burdens, ultimately influencing cognitive trajectories over time.
Our US-born results diverge from work that link living alone with increased odds of cognitive decline (Desai et al., 2020; Grande et al., 2018; Portacolone et al., 2019). Living alone does not necessarily imply social isolation as many older adults who live alone maintain active extra-household networks and active community participation (Cardona & Andrés, 2023; Guarnera et al., 2023; Perissinotto & Covinsky, 2014). A plausible explanation for our findings is that healthier, cognitively intact older adults are more likely to sustain independent living and socially engaged routines, whereas cognitive or functional decline can precipitate moves into co-residence to meet rising care needs. Such moves may increase or intensify household strain including caregiver burden, role overload, and interpersonal stress, which can adversely affect cognition (Choi et al., 2015; Gilbert et al., 2018; Sheehan et al., 2020). From a person–environment fit perspective, both solitary and crowded settings can become misaligned when individual competence and demands are not well aligned; for some US-born older adults, co-residence may reflect a response to worsening health rather than a setting that fosters cognitive resilience (Wolf et al., 2021).
Among foreign-born Mexican American older adults, the null association between co-residence and cognitive impairment may reflect nativity-patterned household structures, health selection, and acculturation dynamics. Foreign-born individuals generally exhibit more favorable health profiles than their US-born counterparts (the “healthy immigrant” effect) and are more likely to reside in larger multigenerational households and to rely on family assistance, which can provide instrumental and emotional support. Such support may buffer cognitive decline through greater day-to-day engagement and practical help (Angel et al., 2014; Kritz et al., 2000; Landale et al., 2006; Markides & Rote, 2019). However, these benefits are unlikely to be uniform. When household resources are constrained or role expectations clash, crowding, conflict, and caregiver strain may offset advantages, suggesting that the cognitive impact of household size is contingent on within-household dynamics rather than representing a universal risk or protection (Villa et al., 2021; Zhou et al., 2018). Acculturation processes further shape these pathways, through changes in family structure and norms, as well as exposure to acculturative stress, which may differentially influence cognitive aging across immigrant cohorts (Muñoz et al., 2019; Smokowski et al., 2008; Verdaguer et al., 2023).
Our findings both mirror and contrast findings from other cross-national studies conducted in other racial and ethnic groups, where living with others was found to be associated with better cognitive outcomes. For example, among European older adults, those living with family members experienced a slower rate of cognitive decline than those living alone (Mazzuco et al., 2017). Similarly, a study in Singapore reported that older adults residing with family had better cognitive abilities than those living alone (Roystonn et al., 2020). However, in a study conducted among Chinese older adults found that those experiencing family conflict while co-residing had a higher chance of cognitive impairment (Yu et al., 2022). Findings from the United Kingdom found that living alone was not associated with greater cognitive decline, emphasizing that social engagement outside of the household can mitigate the risks associated with solitary living (Evans et al., 2019). Together with our findings, these studies indicate that the social ecology surrounding the household—including network quality, caregiving strain, opportunities for meaningful arrangement, and the broader cultural environment inside and outside of the household—rather than household size alone, is central to cognitive outcomes.
Our study also observed lower odds of cognitive impairment in females in both nativity groups. These findings may be reflect a combined mechanisms, including greater cognitive reserve at baseline, slower rate of decline, selective survival, and difference in cognitive function assessment performance (LaPlume et al., 2022; Levine et al., 2021; McCarrey et al., 2017; Shireen et al., 2021). In addition, socioeconomic status, acculturation, and immigration experiences each may influence living arrangements and cognitive functioning. We captured aspects of these processes using measures of educational attainment and language of interview.
This study has some limitations. First, living arrangements and cognition co-evolve; bidirectionality is possible and estimates should be interpreted as associations, not causal effects. However, to minimize reverse causality, we excluded participants with significant cognitive impairment at baseline (MMSE < 21), ensuring that we captured changes in cognitive function among those with moderate or high cognitive functioning at study entry. Second, survival and attrition biases are also possible, given the ≥75 baseline age. However, the addition of the new cohort helps reduce survivor bias by including older adults who were newly eligible due to age and thus had not previously been subject to selection through survival or attrition. Their inclusion enhances the representativeness of our sample and allows us to better capture variation in cognitive and functional health at older ages. The availability of a new cohort allows us to better examine longitudinal associations at a similar age without relying solely on long-term survivors. Third, excluded participants may have underestimated our findings, especially among those with poorer outcomes. Fourth, the assessment of cognitive impairment using the MMSE also has some limitations, as it is used primarily as a screening assessment for cognitive function, limiting the sensitivity to changes over time, particularly in specialized areas of cognition. Fifth, participant self-reports of medical conditions may also not be accurate, and the study team had no access to medical records, biomarkers, or diagnostic images to confirm these self-reported conditions. Lastly, the H-EPESE is also not fully representative of the broader older Hispanic/Latino population in the U.S., which constrains the generalizability of these findings to the Mexican American population in study regions. Taking together, these limitations reinforce a cautious interpretation: our results identify nativity-specific associations consistent with theory, but they do not establish causality. Despite these limitations, the study has several strengths, including the use of longitudinal data with 12 years of follow-up from a large, representative Mexican American cohort, with a focus on the very old group of 75 years and older, one of the fastest growing groups of older adults in the U.S.
In conclusion, this study found significant differences in cognitive impairment among Mexican American older adults based on living arrangement and nativity, underscoring the unique challenges faced by these groups. US-born older adults residing with others exhibited higher odds of cognitive impairment over time, while foreign-born older adults in households with one or more people did not exhibit increased odds relative to those living alone. These findings suggest that neither co-residence nor living alone should be treated as uniformly detrimental or protective. Instead, clinicians and community practitioners should screen for modifiable social mechanisms across all household types, including social isolation and engagement, caregiver burden and conflict, and gaps between functional capacity and household demands, while also targeting interventions that consider household composition and cultural heritage when addressing cognitive health in older adults. Further investigation into cultural expectations and the role of family and community members in caregiving, particularly in foreign-born populations, may provide valuable insights into protective factors associated with multigeneration living arrangements to better support cognitive health in this population.
Supplemental Material
Supplemental Material - Living Arrangements and Cognitive Impairment Among Mexican American Older Adults: Nativity Differences
Supplemental Material for Living Arrangements and Cognitive Impairment Among Mexican American Older Adults: Nativity Differences by Vedant Agrawal and Soham Al Snih in Journal of Applied Gerontology
Footnotes
Acknowledgments
The authors acknowledge the assistance of Sarah Toombs Smith, PhD, ELS, in article preparation.
Ethical Considerations
The University’s Institutional Review Board (IRB # 16-0014) approved the study protocol.
Author’s Contributions
Funding
This work was supported by the National Institute on Aging (R01 AG010939 and 1P30 AG059301-01) the National Institute on Minority Health and Health Disparities (R01 MD010355). This project was partially funded by the Department of Health and Human Services, HRSA, UTMB Center of Excellence for Professional Advancement and Research 1 D34HP49234-01-00.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.