
Abstract
Code Status Discussions (CSDs), CPR understanding, and health literacy is understudied in traumatically injured older adults. We hypothesized that traumatically injured older adults and their families would have limited understanding of CPR and code status, and that lower health literacy would be associated with reduced advance care planning knowledge. We surveyed injured adults ≥65 or their surrogates to assess baseline code status, health literacy, and CPR discussions. Univariate and multivariable analyses were conducted. Among 201 respondents 55% had low health literacy. Only 38% had discussions about CPR, and 21% were asked about code status during admission. Surrogates similarly overestimated CPR success and were unaware of code status when compared to patients (p > 0.05). Lower health literacy was associated with decreased odds of seeking additional CPR information and less confidence in CPR effectiveness knowledge (p < 0.05). Older adults admitted after injury and surrogates for those incapacitated had an overall poor understanding of code status, CPR, and had low health literacy.
Traumatically injured older adults and their surrogates had poor understanding of both CPR and code status utilizing a comprehensive survey highlighting a critical communication gap in advanced care planning. Although low health literacy was not associated with knowledge of CPR effectiveness or code status, it was associated with reduced confidence in CPR understanding and lower likelihood of seeking additional information. Interventions targeting health literacy may improve the effectiveness of CSDs. The assessment of low health literacy in traumatically injured older adults and their surrogates is understudied, and this study showed that low health literacy was prevalent amongst all respondents.
These findings support the need for development of more effective CSDs strategies that are tailored to low health literacy, and future studies at our institution will utilize these findings to inform an intervention for a randomized control trial.What This Paper Adds
Applications of Study Findings
Introduction
More than 950,000 adults over 65 years of age are hospitalized each year after injury (Moreland et al., 2020). Recommended care for this vulnerable patient population includes discussions regarding goals for life-sustaining care and code status upon admission. Code status is typically comprised of three categories, full code, a full code with subsequent limitations, and do not resuscitate and do not intubate (DNR/DNI). Strictly defined, a DNR/DNI status indicates that a patient does not want to receive CPR or be intubated in the event of a cardiopulmonary arrest. Full code indicates that a patient would receive both CPR and intubation if medically indicated, and this is the default code Status in the United States.
The American College of Surgeons recommends that providers hold code status discussions (CSDs) with traumatically injured older adults at time of admission to provide high-quality patient care, uphold patient autonomy, and facilitate early advance care planning (TQIP, 2017). However, the majority of older patients do not have CSDs during their admissions which can place them at greater risk for receiving treatments that do not align with their preferences (González-González et al., 2020). Including patients in the shared decision-making process can prioritize their preferences, values, and goals regarding end-of-life care (Jordan et al., 2016; Kaldjian et al., 2009; Kon et al., 2016). With trauma as a leading cause of death in the United States and a rapid increase in geriatric trauma patients, it is imperative to identify effective methods of communicating code status in this population (Ahmad et al., 2023; Jiang et al., 2020).
Multiple barriers to productive CSDs between doctors and patients have been identified in non-trauma populations, but CSDs remain understudied among traumatically injured older adults. Previous studies have shown that patients and family members lack knowledge regarding end-of-life care interventions and often have preconceived unrealistic expectations of CPR (Gehlbach et al., 2011; Heyland et al., 2006; Kaldjian et al., 2009; Murphy et al., 1994). Health literacy is defined as an individual’s ability to obtain and understand health-related knowledge and history in order to maintain and improve their own health (Liu et al., 2020). Additionally, low health literacy is a known barrier to medical knowledge and decision making (Mancuso C, 2006; Seo et al., 2016). These barriers can prevent patients from choosing care that aligns with their preferences.
In this study we aimed to obtain a baseline assessment of health literacy and CSDs between traumatically injured older adults or surrogate decision makers and the healthcare team. We hypothesized that traumatically injured older adults and their families would demonstrate variable levels of understanding of CPR and code status, and that lower health literacy would be associated with reduced advance care planning knowledge. As this was an exploratory preliminary survey, these estimates were intended to characterize the distribution and variability of these outcomes to inform the design of a future randomized controlled trial.
Methods
Study Design
This was a single-center prospective cohort survey study of older injured patients admitted to a level 1 trauma center. Patients were surveyed at time of discharge from June 14th, 2024, to December 14th 2024 at a single-institution urban academic center, and this study was approved as a quality improvement study aimed at improving clinical care processes and posing minimal harm to patients. Therefore this study was exempt from IRB approval. Verbal consent was received from patients or their surrogates prior to administration of the CSD survey. Results were reported according to the STROBE checklist. This cross-sectional survey served as a preliminary study to inform the design and power calculations of a future randomized controlled trial. Because the objective of this phase was exploratory focused on the distributions of key outcomes such as confidence in CPR decision-making, recall of prior CPR discussions, and requests for additional information. No power calculation was performed. A convenience sample of 200 participants was targeted to generate preliminary estimates for the subsequent trial.
Patients
Traumatically injured older adults (>65) or their surrogate decision-makers admitted to the hospital at any level of care, with English or Spanish as their preferred primary language, were included. Exclusion criteria were prisoners, patients with existing do-not-resuscitate (DNR) or do-not-intubate (DNI) orders, patients admitted while on hospice, and patients not expected to survive beyond 24–48 hours.
Data and Survey Collection
Eligible patients were approached by research assistants to complete a survey prior to discharge. Completed surveys were stored via Qualtrics software. Questions investigated if patients received discussions to determine acceptance of life sustaining care during hospitalization, presence of a prehospital advanced directive, knowledge of CPR and code status, and desire for more information regarding code status. All survey responses were graded using a Likert scale, and were self-reported. Over-estimation of CPR success was based on in-hospital CPR survival rates. Demographic variables were also collected within the survey including age, race/ethnicity, sex, and highest level of education. These variables were self-reported by patients, and race/ethnicity was a combined variable.
Health Literacy Assessment
For the purposes of this study, health literacy was assessed using the BRIEF Health Literacy Assessment Tool. Patients self-assessed their health literacy with the BRIEF validated four-item survey using a Likert scale; total scores can range from 4–20 (Haun et al., 2012). Inadequate literacy is a score of 4–12, marginal literacy 13–16, and adequate literacy 17–20 (Haun et al., 2012). For this study, low health literacy was defined as those with marginal or inadequate literacy scores. Prior literature has shown that those with low or marginal health literacy scores often have poor self-care behavior, receive fewer preventative measures, and have increased all-cause mortality (Hwang et al., 2023).
Outcomes
The primary outcome was the percentage of patients who received discussions to determine life-sustaining care during hospitalization. Secondary outcomes included health literacy level, presence of a prehospital advance directive, knowledge of CPR, and code status (assessed using a Likert scale), and desire for more information regarding code status.
Statistical Analysis
Statistical analysis was conducted using R (version 4.4.3) (Team, 2023). Descriptive statistics were performed. Univariate analyses were performed based on both the respondent group and on health literacy score (low or adequate). Demographics were compared between the respondent groups and 2 health literacy groups (low and adequate). Categorical variables were compared using Chi-squared or Fisher’s exact tests. Continuous variables were compared using the Wilcoxon Rank Sum test. Categorical and continuous variables were presented as the median (interquartile range [IQR]) and as counts (percent). Multivariable analysis with binomial or multinomial logistic regression was performed adjusting for age, sex, education level, hospitalization in the past year, and race/ethnicity.
Results
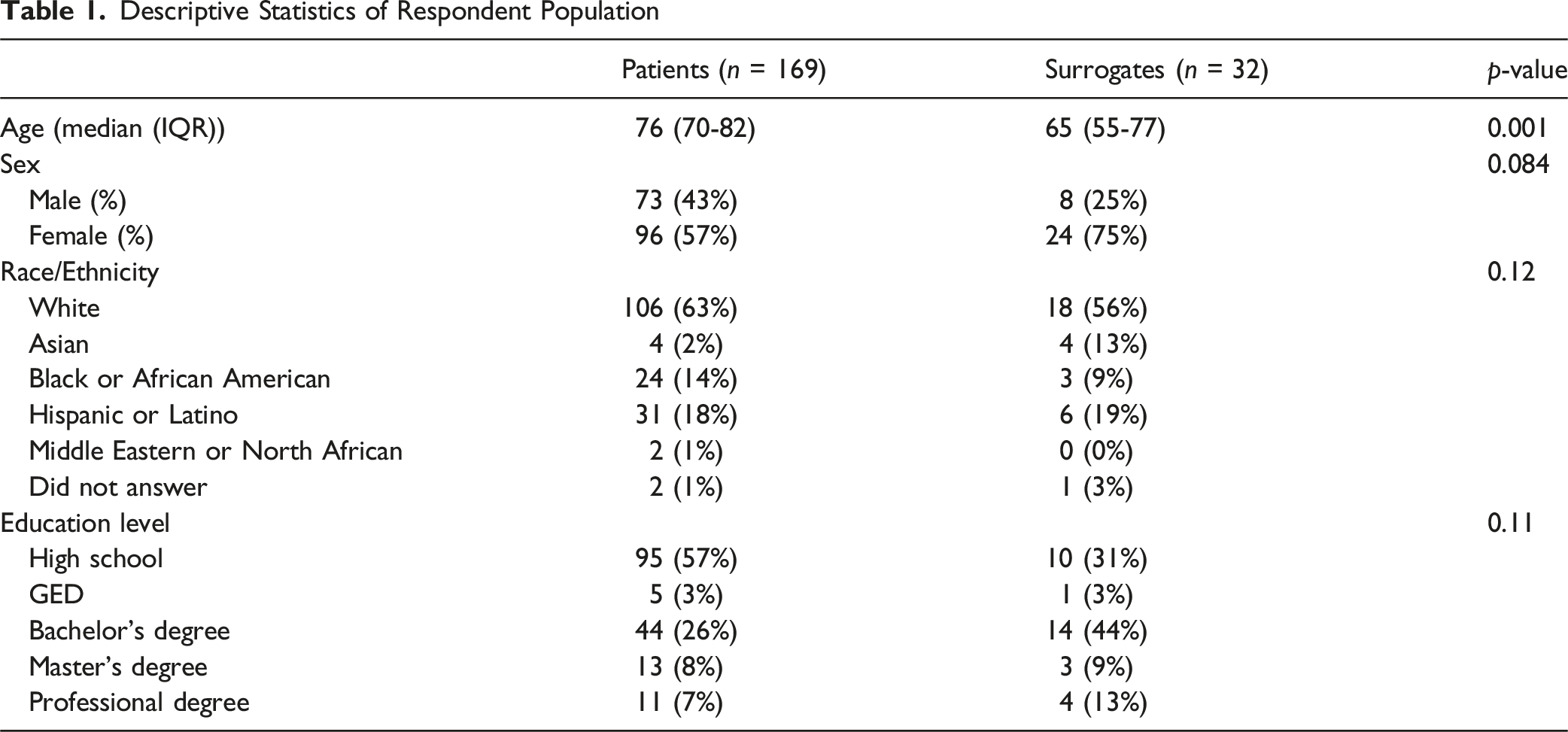
Patient Population
Descriptive Statistics of Respondent Population
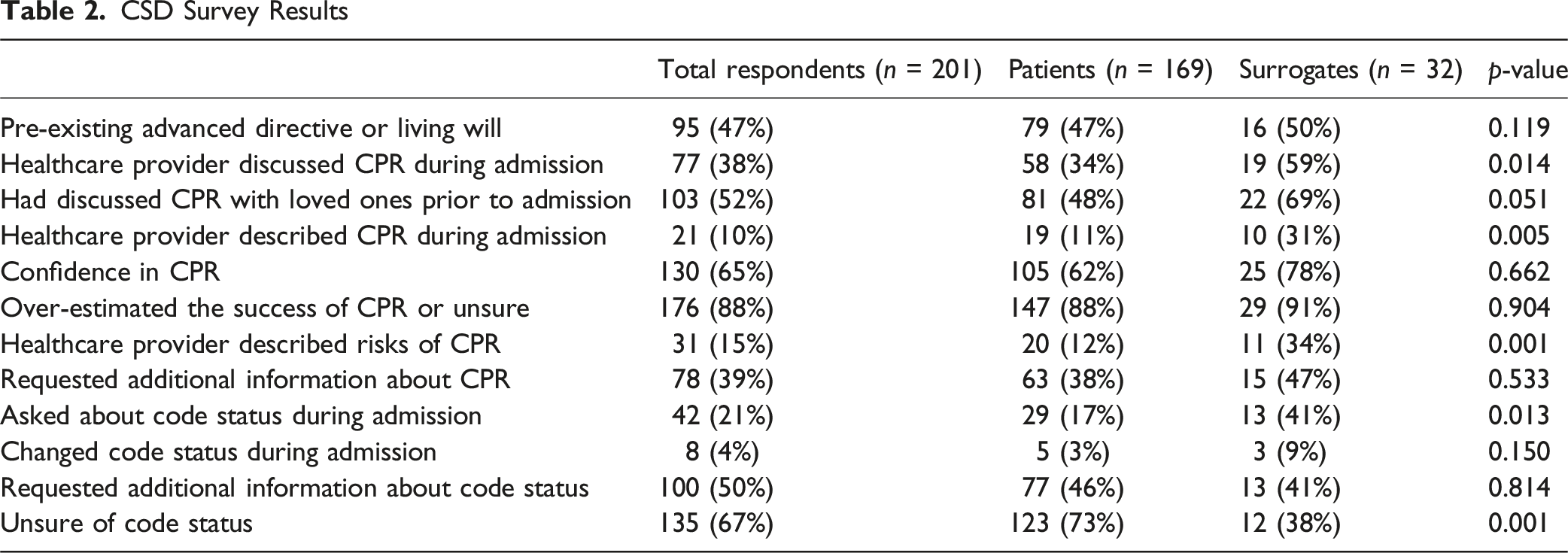
CSD Surveys
CSD Survey Results
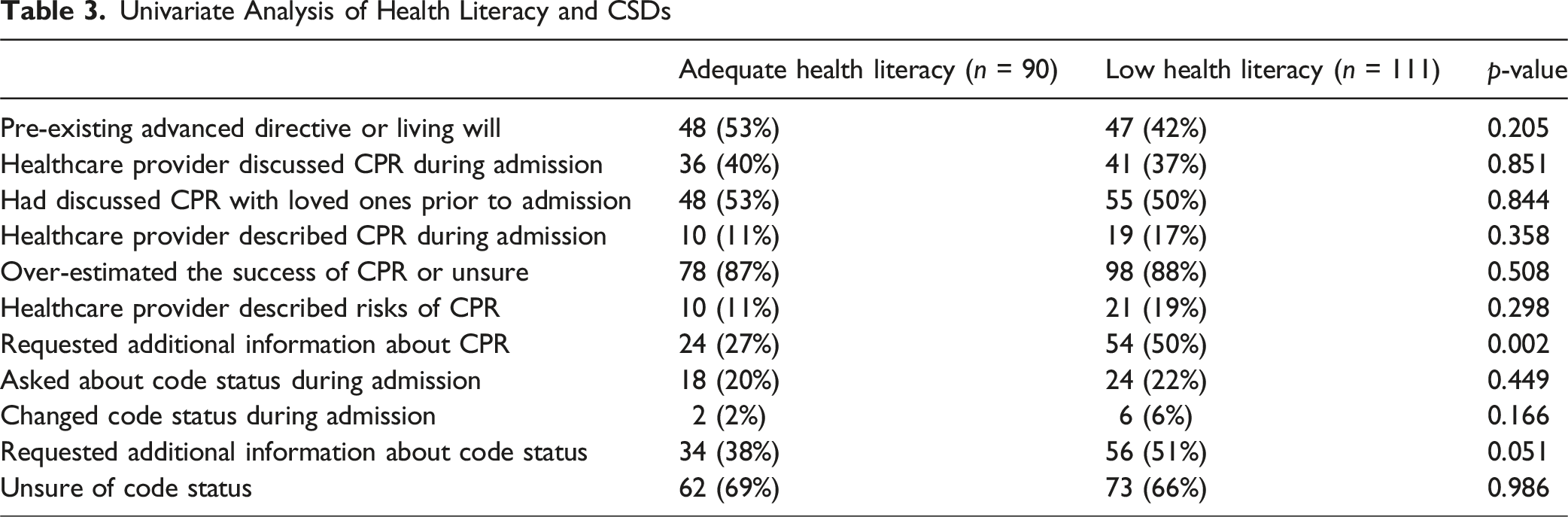
Association Between Health Literacy and CSD Results
Univariate Analysis of Health Literacy and CSDs
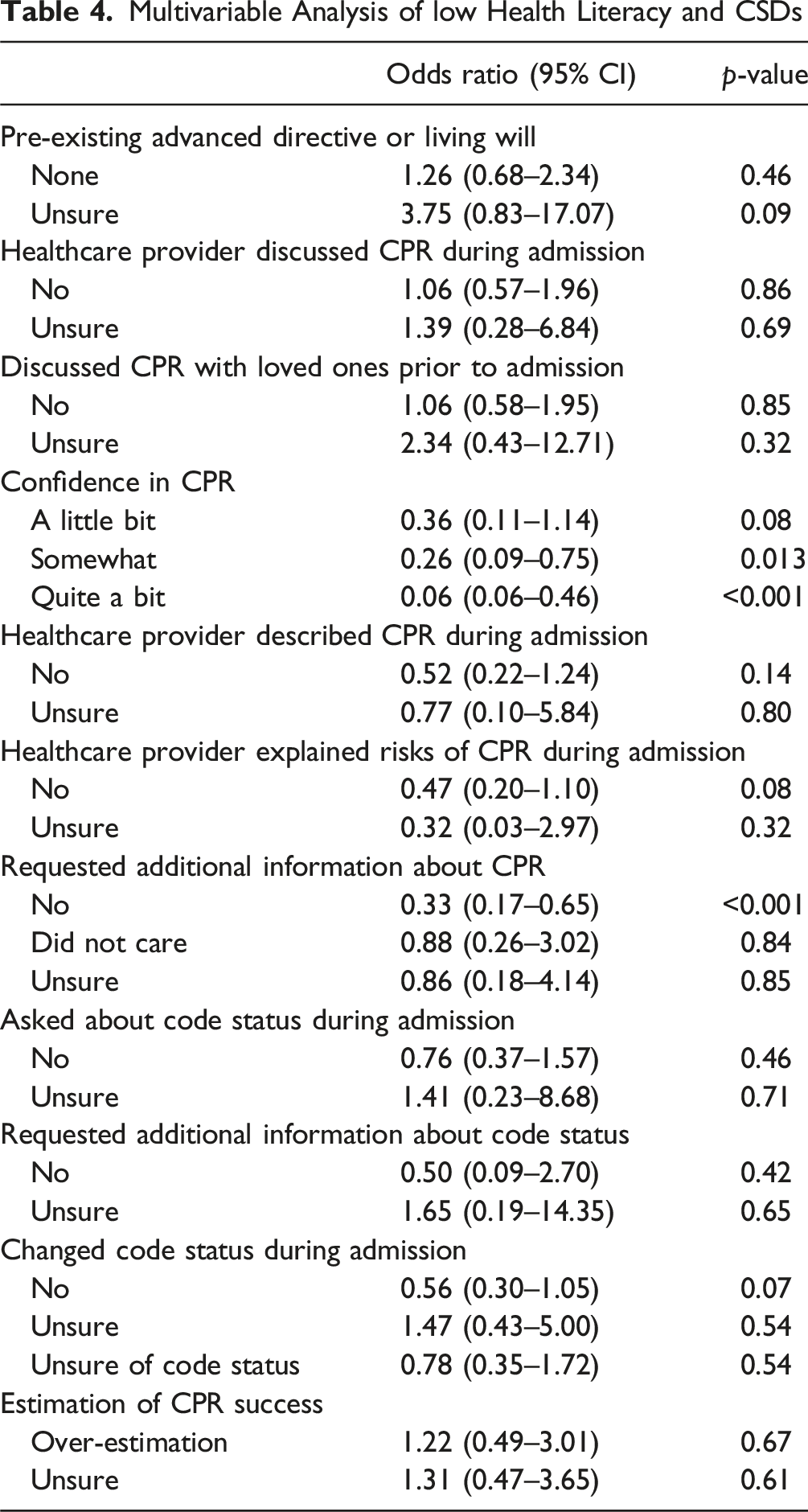
Multivariable Analysis of low Health Literacy and CSDs
Discussion
We conducted a single-center prospective survey study to assess CSDs, health literacy, and their association in older injured adults at our Level 1 trauma center. The results of the CSD surveys indicated an overall poor understanding of both code status and CPR, with a majority of patients overestimating the success rate of CPR and reporting a significant lack of CSDs with medical providers. Most respondents also had low health literacy, as defined by the BRIEF assessment. After adjustment, low health literacy was associated with decreased confidence in CPR effectiveness knowledge and increased requests for additional information about CPR (Table 4). Our study also found that healthcare providers were more likely to discuss and describe CPR and ask about code status with caregivers than with patients (59% vs. 34% and 41% versus 17%). Additionally, patients were more likely to be unsure of their code status when compared to surrogates (73% compared to 38%). One potential explanation is that our institution’s surgical trauma ICU frequently conducts code status discussions (CSDs) with traumatically injured older adults who may be unable to make their own medical decisions while critically ill. As a result, these conversations often occur with caregivers during the ICU phase and may not be repeated once the patient is downgraded to a lower level of care. However, low health literacy was not associated with CPR and code status knowledge or perceptions of CPR effectiveness.
Geriatric trauma patients represent a vulnerable population with an increased risk of mortality. Despite this, there is a lack of literature regarding CSDs in this population. Our study aligns with prior literature showing a lack of CSDs. One study found that in their geriatric trauma population less than 20% of patients had documented CSDs (Hwang et al., 2023). Another study documented CSDs occurring in only 5.3% of their geriatric trauma population (Southerland et al., 2017). In our study, documented CSDs were identified for 11% of patients, and 21% of respondents recalled having CSDs performed. While this represents an improvement compared to prior literature, only a minority of patients had CSDs. CPR effectiveness knowledge is also not well studied in older injured adults. However, a separate survey study of older adults found that 84% of patients over-estimated the successfulness of CPR, which is comparable to our finding of 88% (Zijlstra et al., 2016).
A 2003 study found that only 59% of adults aged greater than 65 had basic or below basic level of health literacy (Kutner et al., 2006). Age-related changes, such as physical impairments in hearing and vision, as well as cognitive decline, can contribute to lower health literacy (Chesser et al., 2016). A cross-sectional study of over 1,300 older adult outpatients in Europe, utilizing the Survey on Health, Aging and Retirement in Europe, showed that those with higher health literacy had better advance care planning knowledge, were more likely to have discussed their end-of-life wishes with loved ones, had a documented advanced directive, and had a designated surrogate decision-maker (Meier et al., 2024). Nouri et al. performed a cross-sectional study of 1,400 Veterans Affairs patients to identify predictors of knowledge about advance care planning. They reported that health literacy and sociodemographics were more important than prior experience with advance care planning, suggesting that easy-to-understand advance care planning materials should be provided to address low health literacy and to improve knowledge. Low health literacy and the complexity of language used in CSDs may explain why our results did not demonstrate an association between CSD and knowledge of CPR (Nouri et al., 2019).
Houlihan et al. performed a systematic review of randomized trials addressing low health literacy in advance care planning. Strategies that were evaluated included writing text at lower reading levels, adding images to educational materials, and using video. Although there were methodological limitations identified with the trials, the strategies did appear to improve knowledge and to increase the preference for comfort care (Houlihan et al., 2022). Nair et al. conducted a randomized controlled trial involving over 200 adult inpatients, comparing a video decision tool for advance care planning to a verbal description (Nair & Kohen, 2019). They found that patients who received the video intervention had increased knowledge of advance care planning, more documented CSDs, and better concordance between their end-of-life care goals and chart documentation (Nair & Kohen, 2019). Volandes et al. assessed a video-intervention compared to a verbal description in over 100 older patients admitted to a skilled nursing facility. They found those who received the video intervention were more likely to opt for comfort care compared to their counterparts (Volandes et al., 2023). Both of these studies suggest that video support tools may improve understanding, and support informed-decision making.
Limitations
Our study had several limitations. First the study was susceptible to selection bias. However, all older injured adults were approached at our hospital for inclusion, and surrogates were utilized to improve patient representation. Second, the results may not be generalizable. Recall bias may have influenced respondents’ responses as their ability to accurately remember CSDs may vary, leading to either underestimations or overestimations of these discussions. Additionally, social desirability bias could potentially affect the honesty of responses amongst participants, as they may provide responses they deem more ethically or socially appropriate. Additionally, although our hypothesis focused on the association between health literacy and CSD knowledge, the outcomes measured in this cross-sectional survey served as proxies instead of direct assessments of CSD knowledge. Future studies should focus on direct measures of CSD knowledge.
Regarding health literacy, patients may have also overestimated their health literacy due to the self-administered nature of the BRIEF survey, which also makes it difficult to determine the extent to which patient understanding influences perceptions or engagement during CSDs, given the lack of objective measures. The BRIEF also does not assess functional or interactive health literacy which may be more relevant in CSDs. Although few objective measures for health literacy exist. There is no single standardized measure for the quality of CSDs, as a result variations in communication style and clinician approach could not be quantified or compared for this study, and therefore we may not have captured all aspects of which health literacy affects CSD engagement. Future studies could incorporate an additional health literacy tool, such as the Short Test of Functional Health Literacy in Adults (S-TOFHLA) to provide a more objective measure of literacy performance. Nonetheless, if the incidence of low health literacy was underestimated, then there is an even greater need to develop easy-to-understand materials to aid in CSDs.
Conclusion
In conclusion, older injured adults and their surrogates had an overall poor understanding of code status and CPR, and more than half of respondents had low health literacy. However, low health literacy was not associated with code status knowledge or CPR effectiveness. Future strategies to enhance the effectiveness of CSDs should consider incorporation of video interventions, visual aids, and simplified language to better account for varying health literacy levels in advance care planning.
Footnotes
Acknowledgments
The authors have no acknowledgements.
Ethical Considerations
This study was approved by the institutional IRB.
Consent to Participate
The requirement for informed consent was waived due to the minimal risk posed to participants.
Author Contributions
Conception and Study Design: TJP, LSK, MOF, ASK. Literature Review: TJP, ASK, MOF. Data Acquisition: ASK, MOF, SMU. Data Analysis and Interpretation: MOF, TJP. Drafting of the manuscript: TJP, MOF, ASK. Critical Revision: MOF, ASK, SMU, MLB, GK, SS, JLL, LSK, TJP, KMM, GEH, AN.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Fajemisin, and Dr Rieger are supported by the National Institute of General Medical Sciences of the National Institutes of Health under award number 2T32GM008792. The remaining authors have nothing to disclose.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available from the corresponding author upon reasonable request.
Meetings Presentation
Previously presented in part at the 20th Annual Academic Surgical Congress Conference, February 12th, 2025, Las Vegas, NV, 2025 South Texas Chapter Annual Meeting of the American College of Surgeons, February 20th, 2025, Houston, TX, and Southwestern Surgical Society Conference, April 8th, 2025 Sonoma, CA.