
Abstract
Objectives
In Czechia and Slovakia, nursing homes provide care for older adults with reduced independence due to aging. While specialized facilities exist for individuals with Alzheimer’s and dementia, those with other forms of mental distress lack adequate support. This study aims to explore the experiences of caregivers in nursing homes, focusing on their strategies for recognizing, managing, and addressing mental distress among older adults.
Design
A qualitative design study, adhering to the COREQ checklist, was conducted. Semi-structured interviews were performed with professional caregivers from nursing homes in Czechia and Slovakia.
Setting and Participants
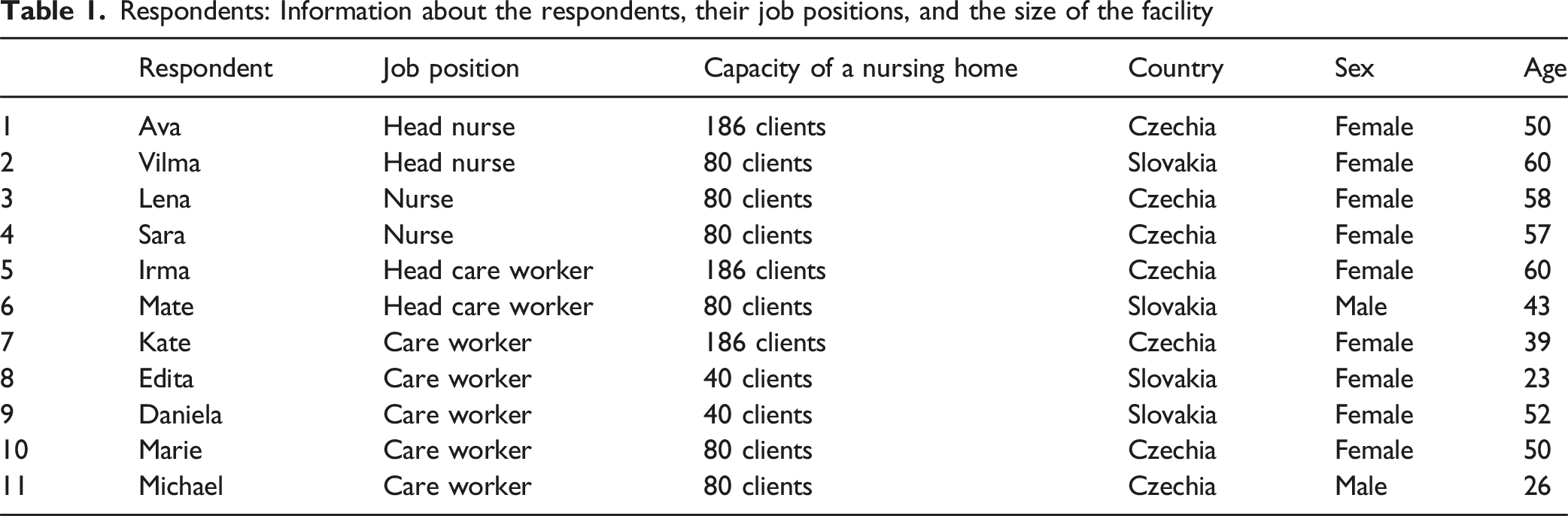
The study involved 11 professional caregivers working in nursing homes located in Czechia and Slovakia.
Methods
Thematic analysis was applied to data obtained through semi-structured interviews to identify key themes related to the research question: “What is the experience of professionals in nursing homes when caring for older adults with mental distress other than dementia?”.
Results
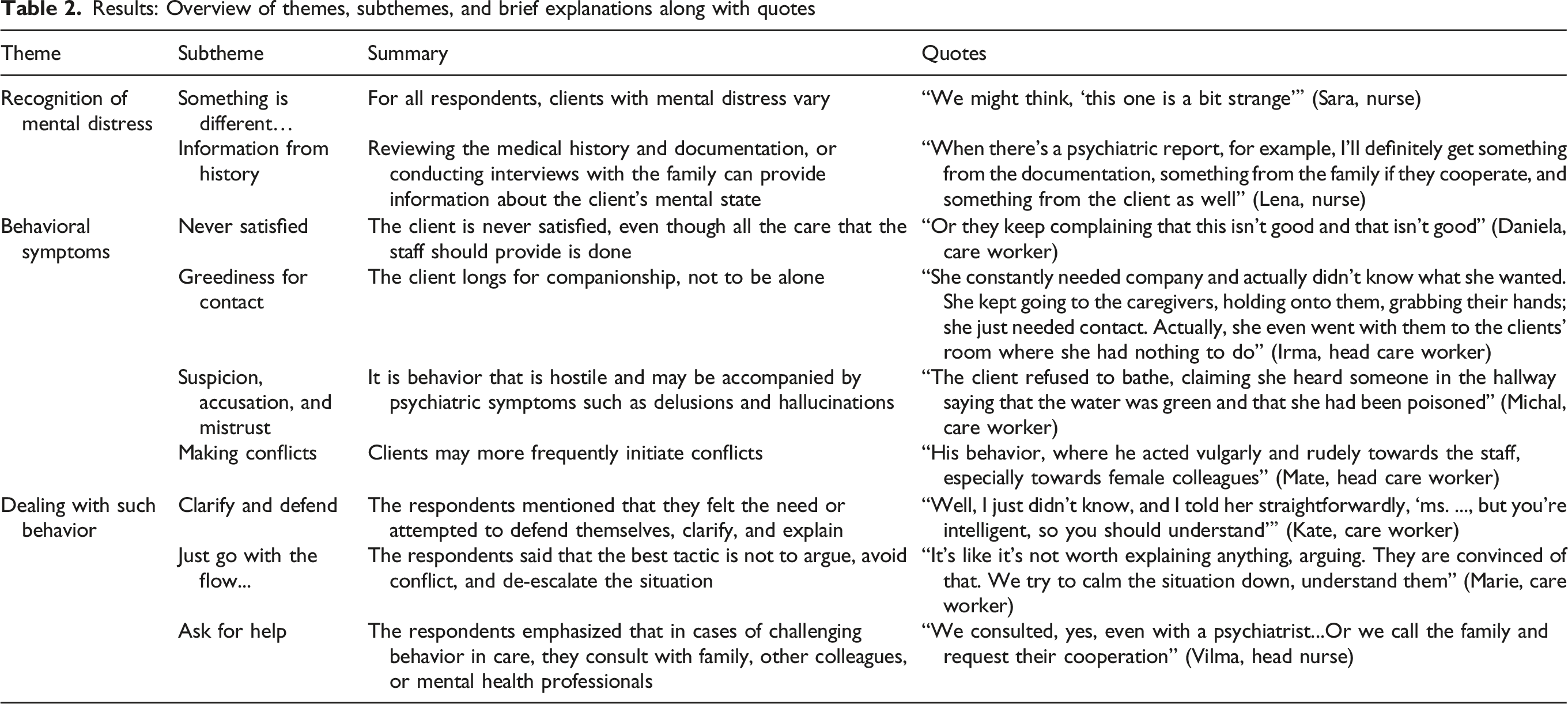
Three main themes and nine sub-themes were identified. The first theme focused on how caregivers recognize mental distress, either through subjective assessments or information provided by other sources, such as relatives or medical records. The second theme addressed the challenges posed by behavioral symptoms, categorized into four sub-themes: never satisfied; greediness for contact; suspicion, accusation, and mistrust; and making conflicts. The third theme examined the strategies used by caregivers to manage these behaviors, including advocacy, empathetic listening, and seeking support from colleagues or mental health professionals.
Conclusions and Implications
Systemic challenges, including under-diagnosis and stigmatization of mental health conditions, hinder the quality of care for clients with mental distress in nursing homes in Czechia and Slovakia. Recommendations include integrating psychologists into nursing homes, centralizing medical records, improving training programs, and using behavioral symptoms as diagnostic cues. Implementing these measures could enhance care quality and outcomes for both caregivers and clients.
• This paper provides novel qualitative insights into how care professionals perceive and respond to non-dementia-related mental distress among older adults in nursing homes. By highlighting overlooked aspects of psychological and emotional care, it contributes to a more nuanced understanding of residents’ needs and identifies gaps in staff training and systemic support within long-term care facilities.
• The findings can inform staff training programs aimed at recognizing and managing non-dementia-relatedmental distress in nursing home residents. Insights highlight the need for integrating psychologists and establishing emotional support and supervision forcaregivers to reduce burnout. Results support the development of centralized medical records and interdisciplinary collaboration to improvecoordination and quality of care.What this paper Adds
Applications of study findings
Bullet Points
• Identifies key areas for improving care, including communication, mental health literacy, and interdisciplinary collaboration. Offers recommendations based on first-hand experiences of staff working with older adults with psychiatric histories. • Informs the need for targeted training to help caregivers recognize and respond to mental distress in older adults, improving diagnostic and care outcomes. • Supports the integration of centralized medical records to enhance continuity and coordination of care in nursing homes. Encourages provision of emotional support and supervision for caregivers to reduce burnout and enhance long-term quality of care.
Introduction
Relocation into long-term care facilities is a stressor for older adults and a significant risk factor for anxiety and/or depression in aged care residents (Polacsek & Woolford, 2022). Approximately 30% of residents in nursing homes live with depression (Seitz et al., 2010). After dementia, depression and anxiety are the most prevalent mental health conditions among the older adult population (Seitz et al., 2010). A study from the Czech environment in 2006 revealed that mild depression was found in 40% of the sample members, severe depression in 15%, and 34% showed no signs of depression among older adults. In the remaining 11%, a depression score corresponding to the norm was detected; however, these older adults were currently being treated with antidepressants. Therefore, a diagnosis of depression can be assumed for them (Holmerová et al., 2006).
In Czechia and Slovakia nursing homes (homes for seniors) are categorized as social service facilities, either operated by local or regional authority private entities. They provide care for older adults who have reduced self-sufficiency due to aging. Older adults with Alzheimer’s disease and other forms of dementia are in facilities called Homes with special regimes. In Czechia, there were 526 nursing homes for older adults with a capacity of 38,500 beds in 2021 (Czech Statistical Office, 2022). In Slovakia, there are approximately 406 nursing homes for older adults (DATAcube, 2018).
The political and historical development in both countries, specifically the transition to democracy in the 1990s, brought shifts in psychiatric services towards outpatient care and improved human rights for individuals with mental illness. Despite these changes, economic limitations hinder the widespread adoption of new treatment options, while challenges such as brain drain and care drain persist (Füredi et al., 2006). Both countries’ psychiatric care systems are undergoing reforms aimed at transitioning from institutional inpatient treatment to community-based and outpatient services. These reforms focus on increasing the number of specialists, promoting interdisciplinary collaboration, and enhancing professional education and training. However, the pace of this transition has slowed, and currently, only a small portion of those in need have access to quality community-based services in Czechia and Slovakia (Izáková et al., 2022; Winkler et al., 2017). Amid these systemic challenges, many individuals experiencing mental distress remain undiagnosed and untreated (Brazinova et al., 2019; Formánek et al., 2019). In this less-than-functional psychiatric care system, older adults become an even more vulnerable group.
The under-diagnosis itself is one of the reasons why we use the term “mental distress” instead of “mental illness” or “mental disorder” in the article. The second rationale for avoiding the term “mental illness” is the persistently high level of stigmatization. Although the public’s attitude towards people with mental illness has shown positive progress over the past decade, there still exists reluctance among people to interact with those who have mental health conditions (Winkler et al., 2021). During the interviews, we endeavored to avoid such stigma. The term “mental distress” is more socially acceptable. During data collection, we kept in mind that the respondents care for such people, and we intended to influence their perception of these clients as little as possible. The reason why the study does not focus on older adults with dementia symptoms is that in Czechia and Slovakia, we have long-term care facilities specifically tailored to their needs. However, the same cannot be said for clients with other mental distress.
In this study, the term “mental distress” refers to residents without evident or diagnosed dementia who were nonetheless perceived by formal caregivers as experiencing psychological difficulties, including possible signs of anxiety or depression. We deliberately use this broader term to reflect the way caregivers themselves described these clients, rather than to impose a strict diagnostic category. At the same time, it acknowledges that many older adults living in nursing homes, even when they might meet the diagnostic criteria for a mental disorder, are often not adequately diagnosed or treated (Holmerová et al., 2006). Consequently, the care provided is not tailored to their needs. The article aims to explore the experiences of formal caregivers with older adults with mental distress in nursing homes. The research question is: “What is the experience of professionals in nursing homes when caring for older adults with mental distress other than dementia?” We believe that through the perspectives and experiences of professional care workers and nurses, we can better describe how to provide care for these clients, identify the challenges that caregiving entails, and highlight examples of good practices or suggestions for improvement. Therefore, conducting research in this area is essential to improve care practices and address the specific needs of older adults with mental distress who are currently a neglected group in the long-term care system and also psychiatry.
Methods
Design
A qualitative design study adhering to the COREQ checklist (Tong et al., 2007) was used for this article. No pilot testing was conducted. We conducted 11 in-depth semi-structured interviews with care professionals working in 4 nursing homes in Czechia and Slovakia. Data collection took place from June 2023 to December 2023. Data collection concluded once participants’ accounts began to repeat and no new relevant information emerged, indicating saturation. Interviews were recorded and transcribed manually by the first author without the use of transcription software. Thematic analyses (Braun & Clarke, 2012) were used to identify themes. The established research question is as follows: “What is the experience of professionals in nursing homes when caring for older adults with mental distress other than dementia?ˮ
Data Collection
The interviews were conducted by the main researcher J.Č., a female psychologist. Respondents were aware of her professional background before the interview began.
Respondents are employees at nursing homes, where residents face challenges in self-care and have health issues unrelated to dementia. The care in these facilities, including the support provided by care workers and nurses, is available 24 hours a day. There were 4 facilities included in the study in Czechia (2) and Slovakia (2). Moreover, the first author completed a research stay in Slovakia as part of the PhD project, which facilitated access to the Slovak facilities. The study forms part of a broader doctoral research project, but the present article addresses a specific research question and constitutes an independent contribution. All respondents worked in the facility for at least 1 year. In Czechia and Slovakia, two main professions in nursing homes provide direct care: a nurse and a care worker. The nurse is someone with medical education who performs healthcare tasks and communicates with doctors. A care worker takes care of the hygiene, nutrition, and other daily needs of the clients. The study includes both of these professions, which in practice function as a unified whole, and their work directly interconnects.
Approval for participation in the research was always sought from the facility management. Based on this, contact was made with the supervisory staff, who determined who would be able to give an interview on any given day. The nursing home management approached employees at the workplace when the researcher was also present. Given the supervisor’s familiarity with the employees, they specifically approached individuals who were already known to be open to participating in research interviews. We acknowledge that the involvement of the supervisor in recommending potential respondents who were likely to be open to participation could have introduced a selection bias. Nevertheless, the possibility of selection bias is recognized as a limitation of the study, and the findings should be interpreted with this consideration in mind. As a result, none of those approached refused to participate in the study. This context makes the selection of respondents purposive. The interviews varied in length, ranging from 30 to 90 minutes.
The interviews were semi-structured, and some questions were prepared in advance; however, the interviewer asked follow-up questions based on how the conversation progressed. The interviews were conducted in Czech and Slovak languages. These languages are similar, so there was no problem with mutual understanding. In cases where the researcher was unsure about the exact meaning of a term, she asked for clarification. The transcripts were not returned to the respondents for feedback, and no formal respondent validation (member checking) was conducted. We assessed that this procedure could be burdensome for the participants, given their circumstances. Instead, trustworthiness was enhanced through iterative discussions of the emerging themes among the authors and by examining recurring patterns across participants.
Respondents: Information about the respondents, their job positions, and the size of the facility
Data Analyses
Thematic analysis was utilized for analyzing transcribed interviews, which proved suitable due to its flexibility. This process unfolded in six steps, following Braun and Clarke’s recommendations (Braun & Clarke, 2012).
Familiarization with the dataset began during transcription by the main researcher, who also conducted the initial coding and identification of broader themes. These themes were then discussed with the co-authors, who provided feedback and helped refine the analysis. This consensus-building process strengthened the trustworthiness of the findings, although formal inter-rater reliability was not calculated. Themes offered insights into the research question. In this phase, the themes were introduced to the other authors of the article. Together, we delved into the interview transcripts, subjecting the themes to further analysis. The themes that emerged from the analysis were reviewed and refined by all the authors of the article. Subsequently, their names were defined. Finally, the themes are presented as the study’s outcomes, as showcased in this article.
Ethical Considerations
The study was approved by the Ethics Committee at the Faculty of Humanities, Charles University as part of a doctoral dissertation project. Respondents signed informed consent forms, where they were informed about handling the data. Transcriptions of the interviews were conducted by the researcher J.Č. Names and exact locations of the facilities were not disclosed, nor were the real names of the respondents. Respondents were assured that the interview was confidential and its content would be presented only anonymously in scientific publications.
Results
Results: Overview of themes, subthemes, and brief explanations along with quotes
Recognition of Mental Distress
When asked how respondents recognize that a client is experiencing mental distress, most of the respondents answered that these clients are different. “Probably from different behavior than usual” (Irma, head care worker). “One simply somehow recognizes it. Or simply says to oneself, ‘that person is acting strange’ˮ (Sara, nurse). “He simply behaves differently, just as during the care” (Edita, care worker). The distinctiveness is apparent in their behavior, which is another theme.
Furthermore, they noted that these clients struggle to adapt to the rhythm of care established in the facility or have difficulty integrating into the collective of other clients. “How do they manage to integrate themselves into the collective with the other clients here. How do they engage in conversations with them. You simply see it” (Ava, head nurse).
Information about whether a client is experiencing mental distress can sometimes be obtained by the staff from medical records, medical history, or conversations with the client’s close relatives. “We gather this information from medical history, then through conversations with family members, or possibly with staff from another facility, either healthcare or social, from which the client comes” (Mate, head care worker). “Either they already have a psychiatric diagnosis when they come in, or we simply see it during the adaptation process, that it's different” (Vilma, head nurse).
Behavioral Symptoms
After further inquiry into what makes these clients different from others, it became apparent that it is predominantly behavior that requires increased care and attention. The behavior frequently mentioned by respondents is persistent dissatisfaction. This means that, despite having everything necessary in the eyes of the staff and trying to meet their demands, it was never enough and never sufficient. “I’m trying to do my utmost for her. But for her, it’s not sufficient. Or she always seems to find some issue, even when everything is fine” (Kate, care worker).
Another behavior that respondents described was a desire for contact. Clients may be insistent, demanding frequent staff contact, and pressing the call button even when respondents deem it unnecessary. Or they follow the staff around, which prevents them from performing other tasks. “For instance, they keep ringing the bell incessantly, demanding something. Even though they already have everything they need for that day” (Irma, head care worker).
Respondents also described behaviors involving suspicion and accusation. Such behavior takes various forms. For example, suspecting that staff stole something from them, or accusing staff of persecuting the client or neglecting care, “He started saying that I want to kill him, that I tried to kill him” (Edita, care worker).
All the above-mentioned examples of behavioral symptoms can escalate to frequent conflict provocation, which may take the form of verbal aggression, cursing, and swearing. “She then walks down the hallway, shouting that we are mean to her and wishing death upon us and even our children” (Kate, care worker).
Dealing with Such Behavior
The respondents described several approaches they chose in the case of behavioral symptoms. They also assessed from their experience what appeared to them as functional and dysfunctional reactions. The respondents felt the need to justify, explain, persuade, or actively defend themselves. “I felt the need to defend myself. Confronting the client, questioning why they said that when it wasn’t true” (Vilma, head nurse). Respondents engaged in lengthy debates with clients. However, in most cases, this proved to be an ineffective and exhausting approach. “We tried various reactions, attempted to debunk that belief, and found that it doesn’t make sense. It’s better to accept it. Individual approach, we try to respect clients just as they are” (Marie, care worker).
The reactions that have proven effective for respondents stem from an individual approach to the client. However, the foundation lies in listening to the client, refraining from arguing, and attempting to de-escalate the situation whenever possible. “I mainly try not to argue, not to refute them. I attempt to accommodate, to appease or just be quit” (Michael, care worker).
The respondents evaluated that another effective way to deal with behavioral symptoms is to ask for assistance or consultation. The respondents had the option to seek consultation or assistance from family members, colleagues, psychologists, or psychiatrists. Together, they could then seek a way to ensure proper care. “We simply contact a psychologist, outline the problem, and if a solution is found, the psychologist starts working with the client over time…we contact the family, as we usually learn the most from them” (Ava, head nurse).
Discussion
The study allows us to look at the experience of professional caregivers with clients who are experiencing mental distress, which may or may not be clearly recognized, described, or diagnosed, but in some way affects the proper care. Thematic analysis of data derived from semi-structured interviews revealed 3 main themes and 9 sub-themes that correspond to the research question: “What is the experience of professionals in nursing homes when caring for older adults with mental distress other than dementia?”
The first theme concerns how the staff even recognizes that the client is experiencing mental distress. This theme relates to two sub-themes. The first stems from the experience and overall feeling of the respondents. Based on their subjective assessment, the client appears different to them than other clients. It became evident that these professionals rely on their experience, perceptions, and preconceptions about mental distress. The second sub-theme relates to more objective findings, such as medical reports or information from relatives. It should be noted that in Czechia and Slovakia, clients are obliged to provide long-term care facilities with medical reports from general practitioners, but not from other specialists. Among the 28 European countries, Czechia ranks as the second-worst in healthcare digitalization. Slovakia holds the fourth-worst score but made progress between 2022 and 2023, gaining 24 points. This advancement allowed Slovakia to surpass Czechia, which only gained 5 points in the same period. At the top of the rankings is Belgium, followed by Denmark, Estonia, and Lithuania (European Commission, 2023). Nursing homes may not even know that a client has been or is being treated psychiatrically. In addition, there is still an under-diagnosis of mental illness, especially among older people. The under-diagnosis and subsequent under-treatment of mental illness in homes for older people is shown by a study of depression in clients of these institutions, which showed that only 44% of older adults showed severe depression and 16% of older adults with mild and moderate depressive symptoms were treated with antidepressants (Holmerová et al., 2006).
The apparent distinctiveness mainly manifests itself in behavior, which is the second theme. These behavioral symptoms are perceived by caregivers as impeding their ability to provide care and healthcare in accordance with the established daily schedule. The caregivers attributed these behavioral symptoms to the mental distress of the clients. The observed behavioral symptoms were classified into four subthemes: constant dissatisfaction; desire for contact; suspicion and accusation; and provoking conflict. Although caregivers spoke of clients without evident or diagnosed dementia. The prevalence of behavioral and psychological symptoms increases with cognitive decline, subjective memory problems, and reduced functional ability (van der Linde et al., 2010). Behavioral symptoms could thus serve as a guide for caregivers to further diagnostic considerations to provide appropriate treatment or support. And, as a result, reduce the caregiver burden associated with caring for these clients. At the same time, interpreting persistent dissatisfaction as a sign of mental distress may risk pathologizing residents’ genuine experiences and thereby limiting their voice and agency.
Another topic is how caregivers address situations related to behavioral symptoms. Three approaches to responding have been described: advocating, not reacting to the situation, and requesting assistance. The need for advocacy points to the fact that caregivers take such behavior personally, which is a high risk for burnout syndrome (Kandelman et al., 2018). Although caregivers knew from experience that it was best not to react or to listen empathetically to the client, they mentioned that when there is an attack that the caregiver perceives as an injustice, they still feel the need to defend themselves, which creates more space for conflict. Seeking help proved to be another tool for effectively dealing with the challenging situation. Respondents seek help from colleagues, family, or institutions where a psychologist is present; they seek crisis intervention or consultation. Although only one facility in the study had a psychologist, it was evident that respondents felt very supported in this facility and praised the fact that they could intervene directly in the situation, provide consultation, and possibly educate on mental health and communication. A psychologist in a long-term care facility has several roles, primarily diagnosis, advocacy, crisis intervention, consultation, and education (Hyerstay, 1979). All of these roles in the system of care for clients with psychological distress can be used to improve the well-being of clients and also to support staff.
Based on the results, we recommend further research. Further research should focus on the long-term effects of caregiving on professional caregivers’ mental health and job satisfaction. Additionally, studies should investigate the effectiveness of various training programs aimed at improving caregivers’ ability to manage mental distress and behavioral symptoms. Research on integrating psychologists into long-term care facilities and the impact of centralized medical records on care quality and diagnostic accuracy would also be valuable. Finally, exploring the satisfaction and well-being of older adults themselves, particularly those experiencing mental distress, can provide insights into improving their care and overall quality of life.
Conclusion and Implications
This study reveals that professional caregivers in nursing homes face significant challenges when caring for older adults with mental distress beyond apparent dementia. Caregivers emphasized difficulties in managing behavioral symptoms that disrupted care routines and relied heavily on subjective assessments when formal medical information was lacking. These experiences highlight the considerable emotional burden placed on staff and the need for psychological support to help them cope effectively and prevent burnout.
From a practice perspective, it is important to recognize behavioral expressions as meaningful signals of possible psychological or cognitive difficulties, while at the same time equipping caregivers with training in empathetic listening, non-reactive techniques, and stress management. Increased supervision, continuous education, and access to supportive resources could help caregivers respond more effectively to residents’ needs without personalizing their challenging behaviors. Employing a psychologist within the nursing home would further strengthen the system by offering direct intervention, consultation, crisis management, and staff education.
At the policy level, systemic barriers—such as under-diagnosis of mental health conditions and the lack of accessible medical records—impede the timely recognition of residents’ needs and the development of appropriate care plans. Establishing clearer diagnostic pathways and centralized medical record systems could improve coordination of care and reduce caregiver burden.
For future research, several avenues are important. Studies should include the perspectives of residents themselves to complement caregiver accounts and avoid the risk of pathologizing dissatisfaction or distress. Intervention studies are needed to evaluate the effectiveness of staff training programs and the integration of psychological support within nursing homes. Comparative and multicenter studies across facilities and countries could also help identify best practices and scalable models of care.
Taken together, these implications underscore the need for a systemic response that combines staff education, clinical support, and policy reform to ensure that the growing mental health needs of nursing home residents are met effectively and compassionately.
Limitations
The inclusion of two countries in the study might initially appear limiting. However, Czechia and Slovakia share a unique historical context, having been one country until 1993, and remain linguistically and culturally similar. The systems of elderly care in facilities are likewise comparable, which justifies a comprehensive approach. Ultimately, the study can offer valuable insights into both Czech and Slovak nursing homes.
This study is limited to the perspectives of formal caregivers, which narrows the scope of the findings, and one of its limitations is that the supervisor recommended participants who were likely to be open to interviews, which may have introduced a selection bias. Future research should include the perspectives of older adults themselves, as well as their family members, to provide a more holistic understanding of the caregiving experience and the impact of mental distress.
Footnotes
Ethical Considerations
The study was approved by the Ethics Committee at the Faculty of Humanities, Charles University (Č.j: UKFHS/292431/2023, Decision Number: 032023/Wil) as part of a doctoral dissertation project.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Alzheimer Nadační Fond, Scholarship for Mother Scientists J.Č. and the Agentura Pro Zdravotnický Výzkum České Republiky Project AZV MZ NV18-09-00587 and NU22-09-0044.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Brief Summary
This study explores how nursing home professionals in Czechia and Slovakia recognize and manage mental distress in residents without dementia, offering practical insights to improve care.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used ChatGPT to correct the language. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the publication’s content.