
Abstract
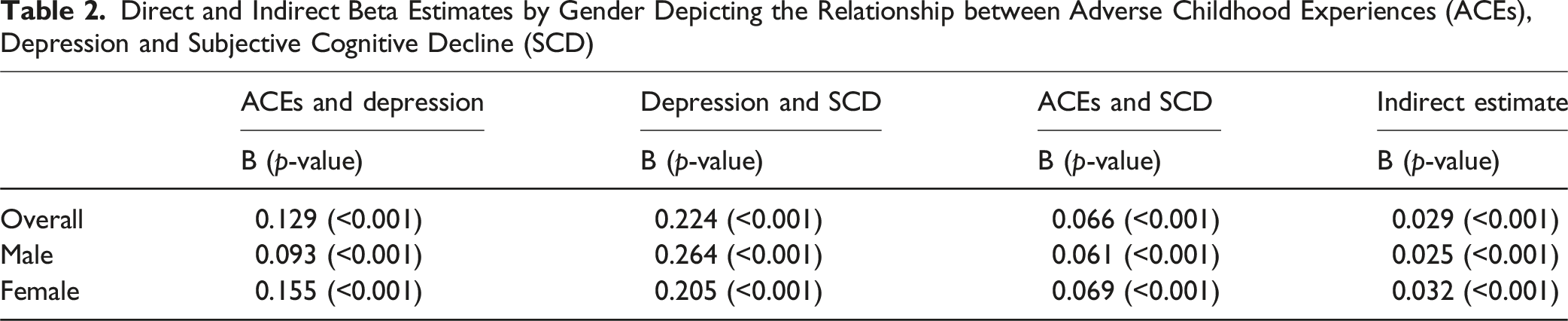
Studies assessing depression as a mediating factor between adverse childhood experiences (ACEs) and subjective cognitive decline (SCD) are lacking. Therefore, the aims of this study were to: (1) determine the mediating role of depression in the association between ACEs and SCD; and (2) assess the moderating role of gender. Data were obtained from the 2023 Behavioral Risk Factor Surveillance Study (BRFSS) survey (N = 38,600). Crude and adjusted path analyses were used to determine the mediating role of depression between ACEs and SCD. Adjusted analyses controlled for sociodemographic confounders. ACEs were positively associated with depression (B = 0.129, p < 0.001), depression was positively associated with SCD (B = 0.224, p < 0.001), and ACEs were positively associated with SCD (B = 0.066, p < 0.001). Depression mediated the association between ACEs and SCD in the overall population (B = 0.029, p < 0.001), and for men (B = 0.025, p < 0.001) and women (B = 0.032, p < 0.001). Intervention programs addressing ACEs may reduce depression and help with cognition for men and women.
• Depression plays a mediating role between adverse childhood experiences and subjective cognitive decline. • This mediating role of depression between ACEs and SCD does not differ significantly for men and women.
• Trauma-informed interventions may reduce depression and help with cognition for men and women. • Interventions addressing depression may also help with cognitive decline.What this paper adds
Applications of study findings
Introduction
Adverse childhood experiences (ACEs) constitute a paradigm-shifting framework within the field of developmental psychopathology, shedding light on the enduring impact of early-life adversity on subsequent health outcomes. ACEs encapsulate a range of traumatic experiences, including but not limited to abuse, neglect, and household dysfunction, that individuals may encounter during their formative years (Anda et al., 1999; Boullier, 2018; Felitti et al., 1998). As a multifaceted construct, ACEs acknowledges the intricate interplay between social, environmental, and biological factors, positing that cumulative exposure to adversity during childhood can significantly influence physical and mental health trajectories across the lifespan (Kalmakis & Chandler, 2015). The burgeoning body of research on ACEs has underscored their pervasive influence on various health outcomes, including mental health disorders and cognitive decline (Halpin et al., 2022; Mwachofi et al., 2020; Nelson et al., 2020).
Prior studies have demonstrated that individuals exposed to childhood adversities are more likely to experience depressive symptoms or develop clinical depression as adults. The enduring impact of ACEs on mental health is often attributed to various factors, including alterations in neurobiological pathways (Hakamata et al., 2022), disruptions in stress response systems (Dempster et al., 2021), and enduring changes in cognitive and emotional processing (Kalia & Knauft, 2020). Moreover, the cumulative effect of multiple ACEs appears to contribute to a dose-response relationship, where a higher number of adverse experiences correlates with an increased risk of depression in adulthood (Chapman et al., 2004; Lu et al., 2008; Stern & Thayer, 2019).
Further, persistent depressive symptoms may contribute to cognitive decline and can influence how individuals perceive and report cognitive functioning. Individuals with depression often report subjective cognitive impairments, such as difficulties with memory and concentration (Hill et al., 2016). Also, individuals with depression may be more likely to perceive cognitive decline even in the absence of objective impairment (Molinuevo et al., 2017). While the relationship between depressive symptoms and cognitive decline may be bidirectional (Jiang & Jiang, 2025; Ma et al., 2025; Yin et al., 2024), the current study examines depressive symptoms as a mediator and subjective cognitive decline (SCD) as the outcome to build on previous work linking depressive symptoms as the predictor of SCD (Brown, Hill, & Haider, 2022). The combination of ACEs, depression, and SCD suggests a cumulative effect on cognitive and mental health outcomes. Individuals with a history of ACEs may be at a higher risk of developing depression, and this, in turn, may contribute to self-reported cognitive decline.
There may also be a direct association between ACEs and SCD (self-reported cognitive decline) among older adults. Previous research has examined the relationship between ACEs and SCD and has shown that individuals who experienced ACEs have a higher likelihood of reporting SCD in the past year (Brown, Kaur, et al., 2022) and objective cognitive decline across the life course (Brown et al., 2021).
Over the years, various moderating factors, including gender differences, have been linked to ACEs, depression, and SCD. Studies indicate that the prevalence and impact of ACEs can vary between genders, with women often reporting higher rates of certain adversities, such as sexual abuse (Brown et al., 2015; Haahr-Pedersen et al., 2020; Merrick et al., 2018), while men may be more likely to experience adversities such as physical abuse (Brown et al., 2015; Merrick et al., 2018). These gender-specific patterns in ACEs are associated with distinct trajectories in mental health outcomes. There are also gender differences in both the prevalence and manifestation of depressive symptoms following exposure to ACEs. Women who have experienced ACEs, especially interpersonal traumas, may be more susceptible to developing depression in adulthood compared to men (Whitaker et al., 2021). However, gender differences were not observed in the link between depression and SCD. Both men and women with depression are more likely to report subjective cognitive impairments (Brown, Hill, & Haider, 2022; Brown, Joseph, et al., 2022). The interplay between depression, gender-specific stressors, and cognitive perceptions underscores the complexity of these associations.
The literature shows that ACEs are associated with depression (Chapman et al., 2004; Lu et al., 2008; Stern & Thayer, 2019); and depression is linked to SCD (Hill et al., 2016; Molinuevo et al., 2017). Therefore, due to these relationships, depression may play a mediating role in the association between ACEs and SCD. In addition, due to gender differences in the experience of ACEs (Brown et al., 2015; Haahr-Pedersen et al., 2020; Merrick et al., 2018), depressive symptoms (Whitaker et al., 2021), and SCD (Brown & Patterson, 2020), gender disparities may occur in the mediating relationship between ACEs, depression and SCD.
Understanding the interplay between ACEs, depression, and SCD in middle-aged and older adults is crucial for holistic mental health interventions. The literature illuminates the importance of understanding the long-term consequences of childhood adversity. It emphasizes the need for tailored interventions and preventive strategies to mitigate the risk of depression among individuals with a history of ACEs. As scholars and practitioners increasingly recognize the far-reaching implications of ACEs, the present study seeks to examine the moderating role of gender on the associations between ACEs, depression, and SCD among older adults and contribute to the evolving discourse on the long-term consequences of childhood adversity. Additionally, we aim to add to the emphasis on adopting a life-course perspective to comprehend the nuanced pathways through which ACEs contribute to the risk of depression in mid- and late-life, thereby informing more comprehensive and effective mental health interventions for middle-aged and older adults.
Methods
Data Source and Study Population
Data for the current study were obtained from the 2023 Behavioral Risk Factor Surveillance Study (BRFSS) survey. This survey is implemented by the Centers for Disease Control and Prevention (CDC) and is nationally representative of the US non-institutionalized population. Questions on health behaviors and conditions, and preventive services use are asked of participants. Data are collected in 50 states, Washington, DC, and three US territories with approximately 400,000 interviews every year (Centers for Disease Control and Prevention, 2024). Studies using deidentified publicly available data are deemed exempt by the University of South Carolina Institutional Review Board (Pro00144211).
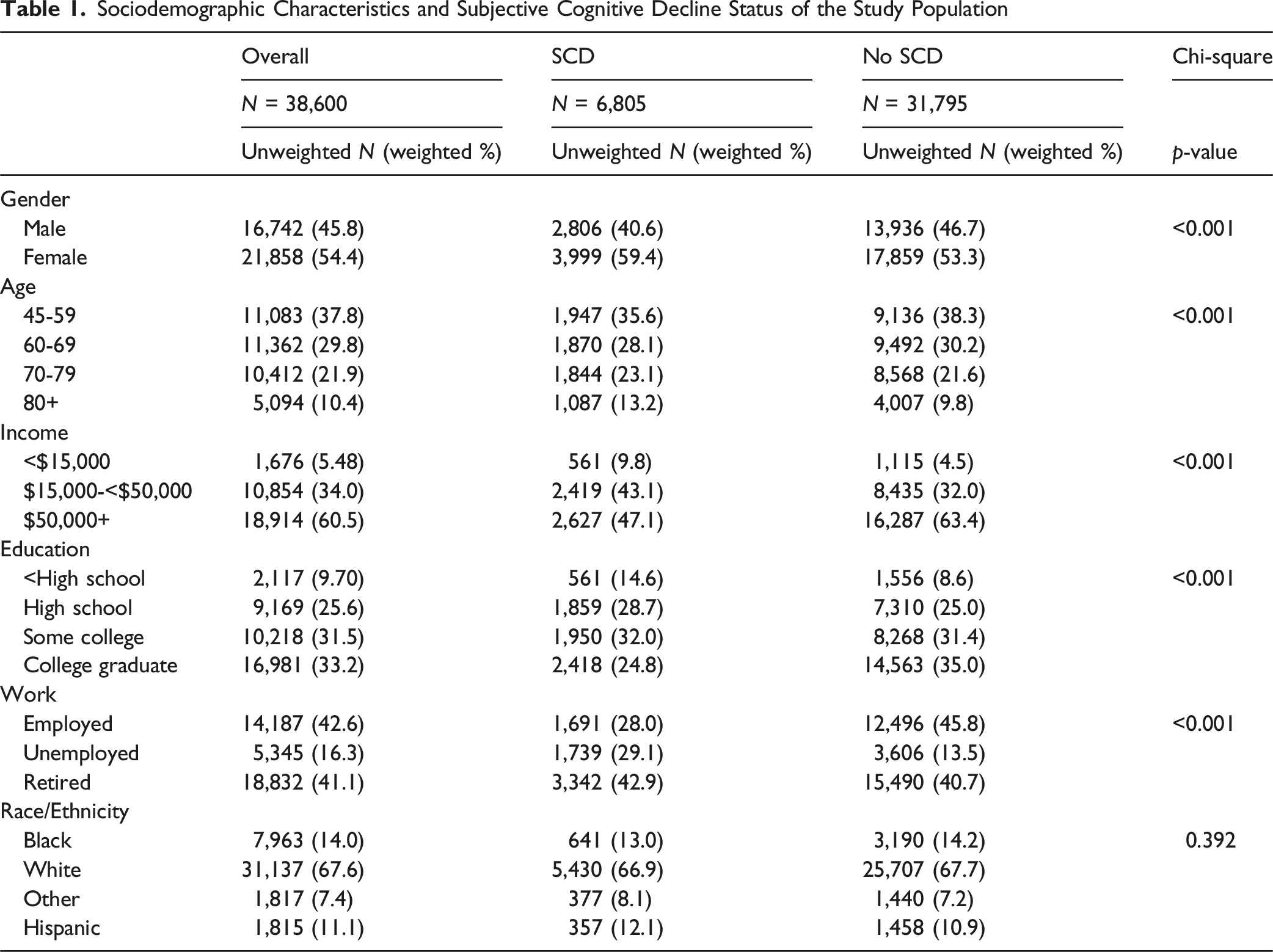
Sociodemographic Characteristics and Subjective Cognitive Decline Status of the Study Population
Primary Variables
Adverse childhood experiences (ACEs) are an optional module in the BRFSS. Data on ten ACEs were used in the current study: if the participant lived with anyone who had mental health challenges, or was a problem drinker, or used drugs, or was incarcerated, if their parents were separated or divorced, if they witnessed domestic violence, if they experience physical, emotional or sexual abuse (being touched sexually, made to touch someone else sexually, or forced to have sex).
Depression was operationalized using the question “(Ever told) (you had) a depressive disorder (including depression, major depression, dysthymia, or minor depression)? (Yes vs. No).” This question has been used in previous research (Brown, Hill, & Haider, 2022; Brown, Joseph, et al., 2022).
Subjective cognitive decline (SCD) in the past year was operationalized using the question “During the past 12 months, have you experienced confusion or memory loss that is happening more often or is getting worse?” This question has also been used in previous studies (Brown et al., 2023; Brown, Hill, & Haider, 2022; Brown, Joseph, et al., 2022; Komalasari et al., 2024; Schroeder et al., 2024).
Analytic Approach
Descriptive statistics were used to describe the study population and SCD status. Mediation analysis using PROC CAUSALMED was used to determine the mediating role of depression between ACEs and SCD. Adjusted analyses controlled for age, income, education, employment, and race/ethnicity. We tested for interaction between ACEs*gender on SCD, and between depression*gender on SCD. Stratified path analysis by gender was also conducted. Statistical significance was set at p < 0.05. All analyses were performed in SAS version 9.4.
Results
Table 1 shows the sociodemographic characteristics and SCD status of the study population. Statistically significant differences existed in SCD by gender, age, income, education, and work status where women, older participants, those with lower income and lower educational status, and those who were unemployed or retired tended to have SCD compared to those who were younger, had higher income and higher educational status, and those who were employed, respectively. There were no statistically significant differences in SCD by race/ethnicity.
Direct and Indirect Beta Estimates by Gender Depicting the Relationship between Adverse Childhood Experiences (ACEs), Depression and Subjective Cognitive Decline (SCD)

Mediational Models Showing the Relationship Between Adverse Childhood Experiences (ACEs), Depression and Subjective Cognitive Decline Overall, and by Gender
Discussion
While trauma has been linked to adverse mental health outcomes, the mechanisms by which traumatic incidents and experiences result in these outcomes remain unclear. Here, using data collected from the Behavioral Risk Factor Surveillance Study (BRFSS), the relationships between trauma, depression, gender, and subjective cognitive decline were studied. Results from pathway analyses demonstrate that depression mediated the association between ACEs and SCD in the overall population. SCD measures have been shown to increase the risk of neurocognitive disorders like dementia in longitudinal studies of older patients and has been nominated as a transition phase in the continuum from normal cognition to early stages of dementia (Jack et al., 2018; Liew, 2019).
The relationship between depression and dementia is complex, with depression in early life increasing an individual’s risk for developing dementia. On the other hand, depression in late life can indicate a prodromal condition for dementia, a comorbid condition, or develop as a result of cognitive decline (Bennett & Thomas, 2014). This study sheds light on this complex relationship by demonstrating that the depression resulting from ACEs can be linked to SCD, and both in combination lead to a higher risk of developing cognitive decline. These findings also further explain previous empirical findings that demonstrated that childhood trauma is associated with poorer cognitive performance, higher levels of anxiety, and greater rates of depression in older adulthood (Petkus et al., 2018; Van Assche et al., 2020).
The current study found that gender moderated the relationship between depression and SCD. However, depression exacerbated the effects of ACEs on cognitive decline in both men and women. These data are in line with a previous study that demonstrated that men and women meet the criteria for depression in equal proportions in a nationally representative sample, even though the expression of depressive symptoms differ between the genders (Martin et al., 2013). Other studies have demonstrated sex differences in the transcriptional profile and molecular signatures in the brains of individuals with depression (Labonté et al., 2017; Seney et al., 2018). This is further complicated by the fact that depressive disorders themselves form a spectrum with various subtypes (Benazzi, 2006). Since the BRFSS questionnaire does not capture this subtlety, it is possible that other differential effects of gender may be masked in our analysis and further investigations with other datasets are required to fully elucidate the role that gender plays in late-life cognitive decline arising due to early-life adversity.
While this study is unique in probing the relationship between trauma, depression, and adverse mental health outcomes, the study has a few limitations. First, path analysis is based on several assumptions of the underlying data and is not effective at elucidating non-linear relationships between the variables (Lleras, 2005). As discussed in our key findings, however, the relationships between these variables are not always linear. In addition, using a cross-sectional design does not establish the temporal sequence between ACEs, depression, and SCD. However, the temporal sequence is established between ACEs (occurring before age 18) and SCD (occurring in the past year). Nevertheless, individual differences in genetic predispositions to these conditions exist, including those due to biological sex, which complicate the modeling of these variables to predict outcomes (Das, 2019; Gardner et al., 2001; Wurtman, 2005). In addition, survey data were collected by phone, which may exclude important demographic groups. The survey only captures data on the U.S. non-institutionalized population. As mentioned above, the BRFSS questionnaire does not capture the complexity of depressive symptoms that can manifest in men and women as a result of traumatic experiences. For example, other multiple-item measures, such as the Patient Health Questionnaire-9 (Kroenke et al., 2001) or the Centers for Epidemiologic Studies Depression-20 (Miller et al., 2008) measures may be able to capture subclinical depressive symptoms. In addition, the single-item SCD measure is also a limitation. SCD-plus, which includes a multi-pronged approach to the determination of SCD, including worry about the decline, change in the last 2 years, age greater than 60, confirmation by informant and APOE ɛ4 carrier status (Sanchez-Benavides et al., 2018) may be crucial to the assessment of SCD in future studies.
Despite these limitations, this study contributes to the body of work trying to understand the complex multifactorial pathways that connect traumatic experiences to cognitive decline. Given the global health, economic, and caregiver burden of cognitive decline in older age, it is imperative to find interventions that address the underlying causal mechanisms to improve the lives of millions of individuals. While significant strides have been made in elucidating disease etiology, especially in non-Hispanic White populations, mechanisms by which social, environmental, and systemic lived experiences influence the risk and resilience towards developing dementias are poorly understood (Adkins-Jackson et al., 2023). Some of these risk factors, such as poverty, neighborhood disadvantage, and others can exacerbate the toll of adverse events on the development of a child’s normal physical, behavioral, and cognitive development. Recognizing the pressing need to understand these relationships, studies to capture the exposome—or the sum of exposures on our bodies—are also being conducted to understand the mechanisms by which social, lifestyle, and physical factors affect health (Vermeulen et al., 2020). Traumatic experiences are folded into the rubric of psychological and mental stress under the framework of the exposome, however, it is well-established that the type, frequency, intensity, duration, and age at the experience of trauma all differentially affect individuals and their metabolic responses to these events. The impact of traumatic experiences in childhood have been shown to be particularly harmful to an individual’s development, well-being, and has long-term consequences (Mooren & Kleber, 2013). Childhood trauma has been associated with failure of the circuits underlying emotional regulation (Grant et al., 2014; Hart & Rubia, 2012), and has been shown to sensitize individuals to stressors by decreasing their resilience to psychological events later in life (Grasso et al., 2013).
Conclusion
Despite the well-established evidence of the severe consequences of ACEs on individuals, the development of health care and interventions for trauma-related disorders is underdeveloped. In a focused review, five important steps were recommended for the development of public health strategies for trauma care—preventing adversity, creating awareness and recognition, strengthening resilience, providing counseling, and making policies (Kleber, 2019). Studies such as ours investigating the causal links between variables in nationally representative datasets directly inform many of these strategies. An individual’s race and ethnicity, gender, culture, religious and spiritual attitudes, age, and a multitude of other factors affect their resilience or vulnerability to traumatic events. More studies that investigate the underlying relationships between ACEs, depression, gender, and cognitive health are essential to develop effective therapeutic and lifestyle interventions.
Footnotes
Acknowledgments
This manuscript was facilitated by the Alzheimer’s Association International Society to Advance Alzheimer’s Research and Treatment (ISTAART), through the Diversity and Disparities Professional Interest Area (PIA) Sex and Gender Differences Special Interest Group (SIG).
Ethical Consideration
The current study used deidentified publicly available data and these studies are deemed exempt by the University of South Carolina Institutional Review Board (Pro00144211).
Consent for Publication
The views and opinions expressed by authors in this publication represent those of the authors and do not necessarily reflect those of the PIA membership, ISTAART or the Alzheimer’s Association.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant K01MH115794 and R34MH137775 from the National Institute of Mental Health to Dr Brown and K99AG078286 from the National Institute on Aging to Dr Esiaka. Dr Viswanathan is an independent researcher without financial conflicts who contributed to this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.